RACS coordination meeting 29 May 2008 Brussels. Review of the functioning of the RACs.

0
Regional Advisory Council (RAC)

1
TABLE OF CONTENTS
EXECUTIVE SUMMARY ................................................................................................................................................... 3
INTRODUCTION ............................................................................................................................................................. 4
BACKGROUND ............................................................................................................................................................... 4
STROKE IN TEXAS ........................................................................................................................................................... 4
METHODOLOGY ............................................................................................................................................................. 5
Figure 1. The method of collection and analysis process of the regional stroke data reported. .......................... 6
EVALUATING THE REGIONAL STROKE SYSTEM OF CARE ............................................................................................... 7
Table 1. Number of hospitals reporting per data collection period and participation type. ................................ 7
STROKE CASES REPORTED ......................................................................................................................................... 8
Figure 2. Percentage of stroke cases reported by data collection method. ......................................................... 8
Figure 3. Total number of stroke cases reported by participation type, July 2015-June 2016. ............................ 8
Table 2. Total number of stroke cases reported by participation type, July 2015-June 2016. RAC Data Survey;
Item 14. ................................................................................................................................................................. 9
Figure 4. Total number of stroke cases by RAC, Texas, July 2015-June 2016. .................................................... 10
CLASSIFICATION OF STROKE CASES ......................................................................................................................... 11
Figure 5a. Classification of stroke cases, July 2015-June 2016. ........................................................................... 11
Table 3a. Classification of stroke cases, July 2015-June 2016. RAC Data Survey, Item 15. ................................. 12
Table 3b. Classification of stroke cases, July 2015-June 2016. RAC Data Survey, Item 15. ................................. 13
Figure 5b. Total number of ischemic stroke cases by RAC, Texas, July 2015-June 2016..................................... 14
ARRIVAL METHOD OF STROKE CASES...................................................................................................................... 15
Figure 6a. Percent of EMS from home or scene, July 2015-June 2016. .............................................................. 16
Figure 6b. Percent of private transportation from home or scene, July 2015-June 2016. ................................. 16
Figure 6c. Percent of transfer from other hospital, July 2015-June 2016. .......................................................... 16
Figure 6d. Percent of arrival via EMS from home or scene by RAC, Texas, July 2015-June 2016. ...................... 17
Table 4. Arrival method of stroke cases, July 2015-June 2016. RAC Data Survey; Item 16................................. 18
NATIONAL INSTITUTES OF HEALTH STROKE SCALE (NIHSS) PERFORMED ............................................................... 19
Figure 7. Percent of ischemic stroke cases with an NIH Stroke Scale (NIHSS) performed, July 2015-June 2016.
............................................................................................................................................................................. 20
Table 5. Ischemic stroke cases with an NIH Stroke Scale (NIHSS) performed, July 2015-June 2016. RAC Data
Survey, Item 17. .................................................................................................................................................. 20
INTRAVENOUS THROMBOLYTIC THERAPY (IV t-PA) ................................................................................................ 21
Figure 8. Percent of ischemic stroke cases that received IV t-PA, July 2015-June 2016. .................................... 21
Table 6. Ischemic stroke cases that received IV t-PA, July 2015-June 2016. RAC Data Survey, Item 18. ............ 22
IV t-PA WITHIN 60 MINUTES OF ARRIVAL ............................................................................................................... 23

2
Figure 9. Percent of ischemic stroke cases that received IV t-PA within 60 minutes or less from time of hospital
arrival, July 2015-June 2016. ............................................................................................................................... 23
Table 7. Ischemic stroke cases that received IV t-PA within 60 minutes or less from time of hospital arrival, July
2015-June 2016. RAC Data Survey, Item 19. ....................................................................................................... 24
ENDOVASCULAR THERAPY ...................................................................................................................................... 25
Figure 10. Percent of ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion),
July 2015-June 2016. ........................................................................................................................................... 25
Table 8. Ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion), July 2015-
June 2016. RAC Data Survey, Item 21. ................................................................................................................ 26
PICTURE-TO-PUNCTURE WITHIN 60 MINUTES ........................................................................................................ 27
Figure 11. Percent of ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion)
within 60 minutes or less of time of initial brain imaging, July 2015-June 2016. ............................................... 27
Table 9. Ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion) within 60
minutes or less of time of initial brain imaging, July 2015-June 2016. RAC Data Survey, Item 22. .................... 28
DISCHARGE DISPOSITION OF ISCHEMIC STROKE CASES .......................................................................................... 29
Figure 12. Discharge disposition of ischemic stroke cases, July 2015-June 2016. .............................................. 29
Table 10a. Discharge disposition of ischemic stroke cases, July 2015-June 2016. RAC Data Survey, Item 23. ... 30
Table 10b. Discharge disposition of ischemic stroke cases, July 2015-June 2016. RAC Data Survey, Item 23.... 31
HEALTH INSURANCE STATUS OF ISCHEMIC STROKE CASES .................................................................................... 32
Figure 13. Health insurance status of ischemic stroke cases, July 2015-June 2016. ........................................... 32
Table 11. Health insurance status of ischemic stroke cases, July 2015-June 2016. RAC Data Survey, Item 20. . 33
Figure 14. Percent of ischemic stroke cases with any health insurance by RAC, Texas, July 2015-June2016. ... 34
LIMITATIONS ................................................................................................................................................................ 35
REFERENCES ................................................................................................................................................................. 36
APPENDICES ................................................................................................................................................................. 37

3
EXECUTIVE SUMMARY
This report describes the findings from the regional data collection effort and reflects the care of stroke
patients reported from July 1, 2015 to June 30, 2016 for the 22 regions in Texas.
Regional stroke care findings, July 2015 – June 2016:
220 hospitals provided stroke data for the first collection period (July - December 2015) and 235
hospitals provided data for the second (January - June 2016) (Table 1).
Strokes cases occurred in all 22 regions (Figure 4).
44,044 stroke cases were reported; 83.2% of which was collected through the RAC Data Surveys and
16.8% GWTG-Stroke (Table 2).
Emergency Medical Service (EMS) was the most common arrival method for 13 out of the 20 regions
included (Figure 6d). Private transportation was the most common for the remaining seven regions
(Figure 6b).
42.4% (n=18,655) reported were classified as ischemic (Figure 5b).
Nearly half, seven of the 15 regions included, reported more than 90% of ischemic stroke patients had
a NIHSS performed (Figure 7).
12.8% of the ischemic stroke patients received intravenous thrombolytic therapy (IV t-PA) (Figure 8).
The average percent of patients that received IV t-PA within 60 minutes of arrival was 59.5%.
4.0% of ischemic stroke patients received endovascular therapy (Figure 10). More than half, six of the
11 regions included, reported 0.0% receiving therapy within 60 minutes of imaging (Figure 11).
Home was the most common discharge disposition for eight of the reporting regions (Figure 12).
21.2% of ischemic patients had some form of health insurance documented (Figure 14).

4
INTRODUCTION
Heart disease and stroke are the number one and number three leading causes of death in Texas in 2014.1
In order to reduce heart disease and stroke related death and disability, it is important to evaluate the
current state of systems of care in the state for both conditions by collecting and analyzing data.
During the 83rd Regular Texas Legislative Session, the Legislature appropriated funds to advance heart
attack and stroke reduction efforts throughout Texas. To inform such efforts, the Texas Department of
State Health Services (DSHS) has launched a heart attack and stroke data collection initiative. The initiative
focuses on pre-hospital and hospital heart attack and stroke measures. The data elements are collected
from multiple sources for the comprehensive assessment of the systems of care.
Regional Advisory Councils (RACs) play a key role in data collection by enhancing the surveillance of the
heart attack, with a particular focus on ST-segment elevation myocardial infarction (STEMI), and stroke
systems of care in Texas. This report describes the findings for the regional stroke system of care measures
in Texas. Survey findings will be used to assess practices regarding delivery of heart attack and stroke care
across the state and identify areas of opportunity for quality improvement.
BACKGROUND
With guidance from the Texas Council on Cardiovascular Disease and Stroke, Governor’s EMS and Trauma
Advisory Council (GETAC), and DSHS Office of Surveillance, Evaluation and Research (OSER), the Texas
Heart Disease and Stroke Program developed an online survey using Survey Monkey
(https://www.surveymonkey.com) to gather regional pre-hospital and hospital STEMI and stroke data.
The 22 Regional Advisory Councils (RACs) were surveyed and asked to report STEMI and stroke data
elements for their regions, also known as Trauma Service Areas (TSA), that occurred between July 1, 2015
and June 30, 2016. RACs collected and reported data to the Health Promotion and Chronic Disease
Prevention Section (HPCDPS) of DSHS. OSER analyzed the data and created this report to inform RACs and
the Texas Council on Cardiovascular Disease and Stroke, as well as other stakeholders.
Appendix A displays the geographic coverage of the 22 RACs in Texas, all of which are represented in the
report.
STROKE IN TEXAS
In 2015, the prevalence of stroke among Texans, 18 years of age and older, was 3.0% (95% CI: 2.5-3.5).2
In 2014, age-adjusted stroke death rate among Texans of all ages, was 43.3 (95% CI: 42.4-44.1) per 100,000
people.1 When stratified by race/ethnicity, the age-adjusted stroke death rate was significantly higher
among black, (59.2, 95%CI: 56.0-62.5), than white (43.7, 95% CI: 42.7-44.8) and Hispanic (36.4, 95%CI:
34.8-38.0) subgroups.1
In 2014, the age-adjusted hospitalization rate due to stroke among Texans of all ages, was 20.3 (95% CI:
20.1-20.4) per 10,000 people.3

5
METHODOLOGY
This report includes the de-identified, aggregate RAC-level data collected from hospitals who agreed to
share hospital-level data through 1.) Semi-annual Surveys and 2.) Get With The Guidelines® (GWTG)-
Stroke data with DSHS. All data is protected under Health Insurance Portability Accountability Act (HIPAA)
guidelines. No hospital-level data will be distributed, nor will any hospital name be identified in the report.
There were a total of 24 questions in the survey, consisting of the following elements:
RAC leadership and contact information, and pre-hospital and hospital elements of STEMI and
stroke (Appendix B).
RAC Data Survey 1, collected data on cases that occurred between July 1, 2015 and December 31,
2015.
RAC Data Survey 2, collected data on cases that occurred between January 1, 2016 and June 30,
2016.
The surveys’ RAC-level data submitted to OSER was subsequently combined for analysis and includes data
reported from July 1, 2015 through June 30, 2016.
OSER identified hospitals participating in the GWTG-Stroke registry that did not provide hospital-level data
through the RAC Data Surveys. These hospitals’ data from July 1, 2015 to June 30, 2016 were analyzed at
the regional level and aggregate data were added to the RAC-level data collected through the RAC Data
Surveys.
Figure 1 on the following page explains the data collection method and analysis process used for the
evaluation of the stroke system of care at the regional level.

6
Figure 1. The method of collection and analysis process of the regional stroke data reported.
DATA ANALYSIS
OSER removed duplicate entries before analyzing the data. OSER followed up with the RACs when
clarification was needed. Data from the RAC Data Surveys was analyzed using Microsoft Excel 2010, and
GWTG-stroke data was analyzed using SAS 9.4.
RAC Data Collection (via semi-annual survey)
Hospitals participating in GWTG-stroke
and DSHS
Hospitals participating in GWTG-stroke but not with
DSHS
Hospitals NOT participating in either GWTG-stroke or DSHS
Aggregate data from the hospitals will be collected by each RAC. The list of hospitals that submitted data to RACs will be available
along with the aggregate data.
RACs submit aggregate data to DSHS
2016 Texas Regional Stroke System of Care Report
Identify hospitals from GWTG-stroke registry that are not included in the RAC Data
Surveys by each RAC
Pull data for these hospitals at the RAC-level
Analyze data from the above subset for the measures included in the RAC Data Survey
following the same definitions given to RACs
Add aggregate data to the data submitted by the RACs
Regional Data Reports
Method and Process

7
EVALUATING THE REGIONAL STROKE SYSTEM OF CARE
Overall, there were 220 hospitals that provided data on stroke cases that occurred between July 1, 2015
and December 31, 2015, and 235 hospitals provided data on stroke cases that occurred between January
1, 2016 and June 30, 2016 (Table 1).
21 RACs reported regional hospital stroke data for RAC Data Survey 1 (Table 1).
22 RACs reported regional hospital stroke data for RAC Data Survey 2 (Table 1).
The number of hospitals participating through the RAC Data Survey increased from 197 for Survey 1
to 212 for Survey 2 (Table 1).
Data from an additional 31 hospitals that participated through the GWTG-stroke registry was
combined with the regional stroke data submitted through the RAC Data Surveys.
Hospitals participating through the GWTG-stroke registry for Survey 1 are located in eight regions
(RACs C, E, G, H, K, L, O, and P).
Hospitals participating through the GWTG-stroke registry for Survey 2 are located in five regions (RACs
E, H, O, P, and V).
Table 1 displays the hospital participation totals for each participation type by RAC for July-December
2015 and January-June 2016.
Table 1. Number of hospitals reporting per data collection period and participation type.
TOTAL NUMBER OF REPORTING HOSPITALS
RAC
July - December 2015 January - June 2016
RAC Data Survey GWTG-stroke RAC Data Survey GWTG-stroke
Total 197 23 212 23 A 12 0 11 0 B 17 0 16 0 C 2 1 6 0 D 16 0 8 0 E 20 13 26 15 F 3 0 6 0 G 8 1 11 0 H 5 1 5 2 I 6 0 6 0 J 13 0 11 0 K 10 1 10 0 L 0 1 7 0
M 7 0 8 0 N 8 0 8 0 O 10 2 1 3 P 2 3 9 2 Q 33 0 32 0 R 8 0 10 0 S 5 0 7 0 T 2 0 2 0 U 3 0 4 0 V 7 0 8 1

8
STROKE CASES REPORTED Guidance on inclusion and exclusion criteria was provided to the RACs in the RAC Data Surveys for each
question (Appendix B). For July 1, 2015 through June 30, 2016, a total of 44,044 stroke cases were
reported (Table 2); 83.2% was collected from the RAC Data Surveys and 16.8% collected from the GWTG-
stroke registry participating hospitals (Figure 2).
All 22 regions have reported stroke cases (Figure 4).
A total of 36,652 stroke cases were reported from the RAC Data Surveys (Table 2).
A total of 7,392 stroke cases were reported from GWTG-stroke (Table 2).
Nine regions (RACs C, E, G, H, K, L, O, P, and V) include data from both GWTG-stroke and the RAC Data
Surveys (Table 2).
For the majority of regions, the total number of reporting hospitals varied between the July-December
2015 and January-June 2016 collection periods (Table 2).
Figure 2. Percentage of stroke cases reported by data collection method.
Figure 3 and Table 2 display the number of stroke cases reported by participation type and the total number of stroke cases from July 2015 to June 2016 by RAC.
Figure 3. Total number of stroke cases reported by participation type, July 2015-June 2016.
83.2%
16.8%
RAC Data Surveys
GWTG-stroke registry
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
STR
OK
E C
ASE
S (N
)
RAC
TOTAL NUMBER OF STROKE CASES REPORTED BY DATA COLLECTION METHOD
RAC Data Surveys
GWTG-stroke registry

9
Table 2. Total number of stroke cases reported by participation type, July 2015-June 2016. RAC Data Survey; Item 14.
TOTAL STROKE CASES REPORTED
RAC
RAC Data Survey (n)
GWTG-stroke (n)
Total stroke cases reported (N)
Total number of reporting hospitals
Total number of eligible hospitals July-Dec 2015 Jan-June 2016
Total 36,652 7,392 44,044 220 235 412 A 608 -- 608 12 11 18 B 1,134 -- 1,134 17 16 18 C 36 192 228 3 6 13 D 391 -- 391 16 8 17 E 6,853 3,712 10,565 33 41 83 F 490 -- 490 3 6 6 G 2,065 93 2,158 9 11 21 H 230 400 630 6 7 8 I 1,430 -- 1,430 6 6 9 J 949 -- 949 13 11 17 K 345 115 460 11 10 10 L 596 373 969 1 7 10
M 1,395 -- 1,395 7 8 7 N 1,000 -- 1,000 8 8 8 O 3,049 645 3,694 12 4 26 P 1,072 1,624 2,696 5 11 36 Q 9,304 -- 9,304 33 32 54 R 1,250 -- 1,250 8 10 18 S 397 -- 397 5 7 7 T 580 -- 580 2 2 2 U 1,430 -- 1,430 3 4 11 V 2,048 238 2,286 7 9 13
(--) missing; no additional data from GWTG-stroke participating hospitals.

10
Figure 4. Total number of stroke cases by RAC, Texas, July 2015-June 2016.

11
CLASSIFICATION OF STROKE CASES The stroke classification was reported as follows; 18,655 (42.4%) ischemic stroke, 4,082 (9.3%) transient
ischemic attack <24 hours (TIA), 3,180 (7.2%) intracerebral hemorrhage, 1,046 (2.4%) subarachnoid
hemorrhage, and 755 (1.7%) stroke not otherwise specified (Figure 5a).
▪ 17 regions reported stroke classification data.
▪ Stroke classification data was missing for five regions (RACs A, E, J, P, and T).
▪ Seven regions (RACs C, G, H, K, L, O, and V) included stroke classifications data from GWTG-stroke and
the RAC Data Surveys.
Figures 5a below and Tables 3a-b on the following pages display the classification of the stroke cases
reported from July 1, 2015 through June 30, 2016 by RAC.
Figure 5a. Classification of stroke cases, July 2015-June 2016.
0
20
40
60
80
100
Total B C D F G H I K L M N O Q R S U V
TO
TAL P
ERCEN
T (
%)
RAC
CLASSIFICATION OF STROKE CASES
Ischemic Stroke Transient Ischemic Attack (TIA) Intracerebral Hemorrhage
Subarachnoid Hemorrhage Stroke Not Otherwise Specified

12
Table 3a. Classification of stroke cases, July 2015-June 2016. RAC Data Survey, Item 15.
RAC
Total stroke cases (N)
Ischemic Stroke Transient Ischemic Attack (<24 hours) (TIA) Intracerebral Hemorrhage
RAC Survey (n)
GWTG-Stroke (n)
Total (n)
Total %
RAC Survey (n)
GWTG-Stroke (n)
Total (n)
Total %
RAC Survey (n)
GWTG-Stroke (n)
Total (n)
Total %
Total 44,044 17,398 1,257 18,655 42.4 3,607 475 4,082 9.3 3,010 170 3,180 7.2 A 608 -- -- -- -- -- -- -- -- -- -- -- -- B 1,134 638 -- 638 56.2 247 -- 247 21.8 137 -- 137 12.1 C 228 11 138 149 65.4 5 30 35 15.4 2 21 23 10.1 D 391 204 -- 204 52.2 86 -- 86 22.0 27 -- 27 6.9 E 10,565 -- -- -- -- -- -- -- -- -- -- -- -- F 490 276 -- 276 56.3 75 -- 75 15.3 84 -- 84 17.1 G 2,158 1,087 47 1,134 52.5 429 47 476 22.1 197 10 207 9.6 H 630 65 211 276 43.8 81 104 185 29.4 19 29 48 7.6 I 1,430 910 -- 910 63.6 258 -- 258 18.0 185 -- 185 12.9 J 949 -- -- -- -- -- -- -- -- -- -- -- -- K 460 212 99 311 67.6 61 0 61 13.3 42 11 53 11.5 L 969 333 224 557 57.5 118 70 188 19.4 61 44 105 10.8
M 1,395 793 -- 793 56.8 461 -- 461 33.0 134* -- 134* 9.6* N 1,000 523 -- 523 52.3 310 -- 310 31.0 82 -- 82 8.2 O 3,694 1,939 383 2,322 62.9 675 159 834 22.6 296 42 338 9.1 P 2,696 -- -- -- -- -- -- -- -- -- -- -- -- Q 9,304 7,465 -- 7,465 80.2 0 -- 0 0.0 1,404 -- 1,404 15.1 R 1,250 1,031 -- 1,031 82.5 0 -- 0 0.0 177 -- 177 14.2 S 397 230 -- 230 57.9 106 -- 106 26.7 34 -- 34 8.6 T 580 -- -- -- -- -- -- -- -- -- -- -- -- U 1,430 630 -- 630 44.1 302 -- 302 21.1 147 -- 147 10.3 V 2,286 1,051 155 1,206 52.8 393 65 458 20.0 116 13 129 5.6
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 15a-e that are invalid. *RAC M for RAC Data Survey 2 reported Intracerebral Hemorrhage (n=75) as a combined total including both Intracerebral and Subarachnoid Hemorrhages. The total number (n) and total percent (%) reported as Intracerebral Hemorrhage (n=134, 9.6%) includes both Intracerebral Hemorrhage and Subarachnoid Hemorrhage classifications.

13
Table 3b. Classification of stroke cases, July 2015-June 2016. RAC Data Survey, Item 15.
RAC
Total stroke cases (N)
Subarachnoid Hemorrhage Stroke Not Otherwise Specified Total number of
reporting hospitals Total
number of eligible
hospitals RAC Survey (n)
GWTG-Stroke (n)
Total (n)
Total %
RAC Survey (n)
GWTG-Stroke (n)
Total (n)
Total %
July-Dec 2015
Jan-June 2016
Total 44,044 983 63 1,046 2.4 644 111 755 1.7 155 159 256 A 608 -- -- -- -- -- -- -- -- -- -- -- B 1,134 80 -- 80 7.1 25 -- 25 2.2 17 16 18 C 228 1 3 4 1.8 17 0 17 7.5 3 6 13 D 391 11 -- 11 2.8 34 -- 34 8.7 16 8 17 E 10,565 -- -- -- -- -- -- -- -- -- -- -- F 490 22 -- 22 4.5 0 -- 0 0.0 3 6 6 G 2,158 51 2 53 2.5 39 8 47 2.2 9 11 21 H 630 2 3 5 0.8 63 53 116 18.4 6 7 8 I 1,430 77 -- 77 5.4 0 -- 0 0.0 6 6 9 J 949 -- -- -- -- -- -- -- -- -- -- -- K 460 11 5 16 3.5 19 0 19 4.1 11 10 10 L 969 46 29 75 7.7 22 6 28 2.9 1 7 10
M 1,395 --* -- -- -- 0 -- 0 0.0 7 8 7 N 1,000 19 -- 19 1.9 66 -- 66 6.6 8 8 8 O 3,694 123 16 139 3.8 16 44 60 1.6 12 4 26 P 2,696 -- -- -- -- -- -- -- -- -- -- -- Q 9,304 435 -- 435 4.7 0 -- 0 0.0 33 32 54 R 1,250 42 -- 42 3.4 0 -- 0 0.0 8 10 18 S 397 9 -- 9 2.3 18 -- 18 4.5 5 7 7 T 580 -- -- -- -- -- -- -- -- -- -- -- U 1,430 28 -- 28 2.0 323 -- 323 22.6 3 4 11 V 2,286 26 5 31 1.4 2 0 2 0.1 7 9 13
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 15a-e that are invalid. *RAC M for RAC Data Survey 2 reported Intracerebral Hemorrhage (n=75) as a combined total including both Intracerebral and Subarachnoid Hemorrhages. The total number (n) and total percent (%) reported as Intracerebral Hemorrhage (n=134, 9.6%) includes both Intracerebral Hemorrhage and Subarachnoid Hemorrhage classifications.

14
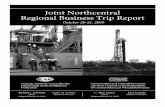
Figure 5b below displays the total number of cases classified as ischemic stroke for each region.
Figure 5b. Total number of ischemic stroke cases by RAC, Texas, July 2015-June 2016. RACs MISSING STROKE CLASSIFICATION DATA In the RAC Data Survey, guidance was provided that the sum of Item 15; Ischemic Stroke, Intracerebral Hemorrhage, Subarachnoid Hemorrhage, Transient Ischemic Attack (<24 hours), and Stroke Not Otherwise Specified, must be less than or equal to the number reported for Item 14.
▪ RAC J, Survey 1; the sum of stroke classifications reported for Item 15 was greater than the total number of stroke cases, Item 14.
▪ RACs E, P, and T, Survey 2; the sum of stroke classifications reported for Item 15 was greater than the total number of stroke cases, Item 14.
▪ RAC A, Survey 1 and 2; the sum of stroke classifications reported for Item 15 was greater than the total number of stroke cases, Item 14.

15
ARRIVAL METHOD OF STROKE CASES
According to the 2013 Texas Behavioral Risk Factor Surveillance System (BRFSS) survey, an estimated
86.9% of adults in Texas said they would call 911 if they thought someone was having a heart attack or
stroke. The remaining 13.1% of adults said they would take other action, such as take the person to the
hospital, tell the person to call their doctor, call a spouse or family member, or do something else.
The arrival method of stroke cases was reported as follows; 12,841 (29.2%) EMS from home or scene,
11,554 (26.2%) private transport/taxi/other from home or scene, 4,732 (10.7%) transferred from other
hospital, and 1,030 (2.3%) mode of arrival was not documented or unknown (Table 4).
▪ 20 regions reported arrival method data.
▪ Arrival method data was missing for two regions (RACs A and Q).
▪ Nine regions (RACs C, E, G, H, K, L, O, P, and V) included data from GWTG-stroke and the RAC Data
Surveys.
▪ EMS from home or scene was the most common arrival method in 13 regions (RACs B, E, F, G, I, J, L,
N, O, P, R, T, and U) (Figure 6a).
▪ RAC F reported the highest regional percentage of stroke cases arriving via EMS from home or scene;
51.8% (n=254).
▪ Private transport from home or scene was the most common arrival method in seven regions (RACs
C, D, H, K, M, S, and V) (Figure 6b).
▪ RAC I reported the highest regional percentage of stroke cases arriving via private transportation from
home or scene; 41.8% (n=598).
▪ Transferred from a hospital was the least common arrival method among stroke cases in all 20 regions
(Figure 6c).
Figures 6a-d and Table 4 on the following pages display the arrival methods of the reported stroke cases
from July 1, 2015 through June 30, 2016 by RAC.

16
Figure 6a. Percent of EMS from home or scene, July 2015-June 2016.
Figure 6b. Percent of private transportation from home or scene, July 2015-June 2016.
Figure 6c. Percent of transfer from other hospital, July 2015-June 2016.
26.2 26.8
43.0 40.2
31.6 32.7 33.5
43.8 41.837.0
49.8
36.2 38.334.0 34.9
31.3 31.938.0
6.4
34.938.3
0
20
40
60
80
Total B C D E F G H I J K L M N O P R S T U V
TOTA
L P
ERC
ENT
(%)
RAC
PRIVATE TRANSPORTATION
10.7
26.3
17.5 19.9 17.1
5.912.8 16.0 14.1
10.2 10.0
17.6
1.1
16.0 16.0 18.811.0 10.3
0.05.3 2.5
0
20
40
60
80
Total B C D E F G H I J K L M N O P R S T U V
TOTA
L P
ERC
ENT
(%)
RAC
HOSPITAL TRANSFER
29.2
43.638.2 37.1 35.6
51.8
36.5 38.442.2
46.7
37.442.8
32.3
41.438.1
46.442.2
36.8
12.6
36.1
28.3
0
20
40
60
80
Total B C D E F G H I J K L M N O P R S T U V
TOTA
L P
ERC
ENT
(%)
RAC
EMS FROM HOME OR SCENE

17
Figure 6d below displays the percentage of stroke patients that arrive at the hospital by EMS from home
or scene for each region.
Figure 6d. Percent of arrival via EMS from home or scene by RAC, Texas, July 2015-June 2016.

18
Table 4. Arrival method of stroke cases, July 2015-June 2016. RAC Data Survey; Item 16.
RAC
Total stroke cases (N)
EMS from Home/Scene Private Transport/taxi/other Transfer from other hospital Not documented or Unknown Total number of reported
hospitals Total
number of
eligible hospitals
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total %
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total %
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total %
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total %
July-Dec 2015
Jan-June 2016
Total 44,044 9,582 3,259 12,841 29.2 8,841
2,713 11,554 26.2 3,355 1,377 4,732 10.7 989 41 1,030 2.3 175 192 340
A 608 -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
B 1,134 494 -- 494 43.6 304 -- 304 26.8 298 -- 298 26.3 31 -- 31 2.7 17 16 18
C 228 14 73 87 38.2 22 76 98 43.0 0 40 40 17.5 0 3 3 1.3 3 6 13
D 391 145 -- 145 37.1 157 -- 157 40.2 78 -- 78 19.9 3 -- 3 0.8 16 8 17
E 10,565 2,119 1,647 3,766 35.6 1,924 1,414 3,338 31.6 1,169 640 1,809 17.1 75 9 84 0.8 33 41 83
F 490 254 -- 254 51.8 160 -- 160 32.7 29 -- 29 5.9 0 -- 0 0.0 3 6 6
G 2,158 752 36 788 36.5 666 57 723 33.5 276 0 276 12.8 122 0 122 5.7 9 11 21
H 630 101 141 242 38.4 119 157 276 43.8 0 101 101 16.0 3 1 4 0.6 6 7 8
I 1,430 603 -- 603 42.2 598 -- 598 41.8 202 -- 202 14.1 27 -- 27 1.9 6 6 9
J 949 443 -- 443 46.7 351 -- 351 37.0 97 -- 97 10.2 34 -- 34 3.6 13 11 17
K 460 128 44 172 37.4 182 47 229 49.8 22 24 46 10.0 13 0 13 2.8 11 10 10
L 969 253 162 415 42.8 228 123 351 36.2 84 87 171 17.6 1 1 2 0.2 1 7 10
M 1,395 450 -- 450 32.3 534 -- 534 38.3 16 -- 16 1.1 395 -- 395 28.3 7 8 7
N 1,000 414 -- 414 41.4 340 -- 340 34.0 160 -- 160 16.0 5 -- 5 0.5 8 8 8
O 3,694 1,149 259 1,408 38.1 1,035 254 1,289 34.9 483 107 590 16.0 19 25 44 1.2 12 4 26
P 2,696 463 789 1,252 46.4 387 457 844 31.3 130 377 507 18.8 22 1 23 0.9 5 11 36
Q 9,304 -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
R 1,250 527 -- 527 42.2 399 -- 399 31.9 137 -- 137 11.0 5 -- 5 0.4 8 10 18
S 397 146 -- 146 36.8 151 -- 151 38.0 41 -- 41 10.3 8 -- 8 2.0 5 7 7
T 580 73 -- 73 12.6 37 -- 37 6.4 0 -- 0 0.0 0 -- 0 0.0 2 2 2
U 1,430 516 -- 516 36.1 499 -- 499 34.9 76 -- 76 5.3 218 -- 218 15.2 3 4 11
V 2,286 538 108 646 28.3 748 128 876 38.3 57 1 58 2.5 8 1 9 0.4 7 9 13
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 16a-d that are invalid.

19
RACs MISSING ARRIVAL METHOD DATA In the RAC Data Survey, guidance was provided that the sum of Item 16; EMS from home/scene, Private transport/taxi/other from home/scene, Transfer from other hospital, and Mode not documented or unknown, must be less than or equal to the number reported for Item 14. ▪ RAC Q, Survey 1; the sum of arrival modes reported for Item 16a-d was greater than the total number
of stroke cases, Item 14. ▪ RAC A, Survey 2; the sum of arrival modes reported for Item 16a-d was greater than the total number
of stroke cases, Item 14.
NATIONAL INSTITUTES OF HEALTH STROKE SCALE (NIHSS) PERFORMED
When a potential stroke patient arrives at a hospital, an initial neurological examination should be
conducted as a component for determining diagnosis of stroke and further care. The NIHSS is a
standardized neurologic examination tool commonly used to evaluate and document the patient’s status.
The NIHSS allows healthcare providers to easily quantify the degree of neurological deficits and severity,
and identify the most appropriate treatment and level of care.
Of the total number of ischemic stroke cases reported (n=18,655), 7,798 (41.8%) had a NIHSS performed
(Figure 7).
▪ 15 regions reported NIHSS data.
▪ NIHSS data was missing for seven regions (RACs A, E, G, J, P, S, and T).
▪ Six regions (RACs C, H, K, L, O, and V) included data from GWTG-stroke and the RAC Data Surveys.
▪ The median percent of NIHSS performed among the 15 regions is 86.1%.
▪ RAC D reported the highest regional percentage; 100% (n=204) of ischemic stroke cases had a NIHSS
performed.
▪ Nearly half, seven out of the 15 regions, reported that more than 90% of ischemic stroke cases had a
NIHSS performed.
▪ RAC R reported the lowest regional percentage; 30.8% (n=318) of ischemic stroke cases had a NIHSS
performed.
Figure 7 and Table 5 on the following page display the number and percent of Ischemic stroke cases with
a NIHSS reported from July 1, 2015 through June 30, 2016 by RAC.

20
Figure 7. Percent of ischemic stroke cases with an NIH Stroke Scale (NIHSS) performed, July 2015-June 2016.
Table 5. Ischemic stroke cases with an NIH Stroke Scale (NIHSS) performed, July 2015-June 2016. RAC Data Survey, Item 17.
ISCHEMIC STROKE CASES WITH NIHSS PERFORMED
RAC
Total ischemic stroke cases (n)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
Total number of reporting hospitals Total
number of eligible hospitals
July-Dec 2015
Jan-June 2016
Total 18,655 6,685 1,113 7,798 41.8 141 140 228
A -- -- -- -- -- -- -- --
B 638 438 -- 438 68.7 17 16 18
C 149 0 136 136 91.3 3 6 13
D 204 204 -- 204 100.0 16 8 17
E -- -- -- -- -- -- -- --
F 276 253 -- 253 91.7 3 6 6
G 1,134 -- -- -- -- -- -- --
H 276 55 184 239 86.6 6 7 8
I 910 748 -- 748 82.2 6 6 9
J -- -- -- -- -- -- -- --
K 311 170 94 264 84.9 11 10 10
L 557 307 206 513 92.1 1 7 10
M 793 734 -- 734 92.6 7 8 7
N 523 516 -- 516 98.7 8 8 8
O 2,322 1,633 357 1,990 85.7 12 4 26
P -- -- -- -- -- -- -- --
Q 7,465 0 -- 0 0.0 33 32 54
R 1,031 318 -- 318 30.8 8 10 18
S 230 -- -- -- -- -- -- --
T -- -- -- -- -- -- -- --
U 630 621 -- 621 98.6 3 4 11
V 1,206 688 136 824 68.3 7 8 13
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 17 that are invalid.
41.8
68.7
91.3100
91.786.6
82.2 84.992.1 92.6
98.7
85.7
0.0
30.8
98.6
68.3
0
20
40
60
80
100
Total B C D F H I K L M N O Q R U V
TOTA
L P
ERC
ENT
(%)
RAC
ISCHEMIC STROKE CASES WITH NIHSS PERFORMED

21
RACs MISSING NIHSS PERFORMED DATA
In the RAC Data Survey, guidance was provided that the number of ischemic stroke cases with NIHSS performed reported for Item 17, must be less than or equal to the total number of ischemic stroke cases reported for Item 15a. ▪ RACs A, E, J, P, and T; missing Item 15a, number of ischemic stroke cases. ▪ RACs G and T, Survey 1; the ischemic stroke cases with NIHSS performed, Item 17 was greater than
the total number of ischemic stroke cases, Item 15a.
▪ RAC J, Survey 2; the ischemic stroke cases with NIHSS performed, Item 17 was greater than the total number of ischemic stroke cases, Item 15a.
INTRAVENOUS THROMBOLYTIC THERAPY (IV t-PA)
Of the total number of ischemic stroke cases reported (n=18,655), 12.8% (n=2,392) received intravenous
thrombolytic therapy (IV t-PA) (Figure 8).
17 regions reported IV t-PA data.
IV t-PA data was missing for five regions (RACs A, E, J, P, and T).
Seven regions (RACs C, G, H, K, L, O, and V) included data from GWTG-stroke and the RAC Data Surveys.
RAC F reported the highest regional IV t-PA percentage; 26.1% (n=72) of ischemic stroke cases (n=276)
received IV t-PA.
RAC M reported the lowest regional IV t-PA percentage; 5.8% (n=46) of ischemic stroke cases (n=793)
received IV t-PA.
Figure 8 and Table 6 display the number and percent of ischemic stroke cases that received IV t-PA from
July 1, 2015 through June 30, 2016 by RAC.
Figure 8. Percent of ischemic stroke cases that received IV t-PA, July 2015-June 2016.
12.8
7.212.1 11.8
26.1
13.0
7.611.1 9.3
13.1
5.89.6 11.0 12.8
17.7
25.222.4
14.7
0
20
40
60
Total B C D F G H I K L M N O Q R S U V
TOTA
L P
ERC
ENT
(%)
RAC
ISCHEMIC STROKE CASES THAT RECEIVED IV T-PA

22
Table 6. Ischemic stroke cases that received IV t-PA, July 2015-June 2016. RAC Data Survey, Item 18.
ISCHEMIC STROKE CASES THAT RECEIVED IV t-PA
RAC
Total ischemic stroke cases (n)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
Total number of reporting hospitals
Total number
of eligible hospitals
July-Dec 2015
Jan-June 2016
Total 18,655 2,285 107 2,392 12.8 153 159 256 A -- -- -- -- -- -- -- -- B 638 46 -- 46 7.2 17 16 18 C 149 1 17 18 12.1 3 6 13 D 204 24 -- 24 11.8 16 8 17 E -- -- -- -- -- -- -- -- F 276 72 -- 72 26.1 3 6 6 G 1,134 144 3 147 13.0 9 11 21 H 276 4 17 21 7.6 6 7 8 I 910 101 -- 101 11.1 6 6 9 J -- -- -- -- -- -- -- -- K 311 18 11 29 9.3 11 10 10 L 557 55 18 73 13.1 1 7 10
M 793 46 -- 46 5.8 7 8 7 N 523 50 -- 50 9.6 8 8 8 O 2,322 235 20 255 11.0 10 4 26 P -- -- -- -- -- -- -- -- Q 7,465 952 -- 952 12.8 33 32 54 R 1,031 182 -- 182 17.7 8 10 18 S 230 58 -- 58 25.2 5 7 7 T -- -- -- -- -- -- -- -- U 630 141 -- 141 22.4 3 4 11 V 1,206 156 21 177 14.7 7 9 13
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 18 that are invalid. RACs MISSING INTRAVENOUS THROMBOLYTIC THERAPY (IV t-PA) DATA In the RAC Data Survey, guidance was provided that the number of ischemic stroke cases that received IV t-PA reported for Item 18, must be less than or equal to the total number of ischemic stroke cases reported for Item 15a. ▪ RACs A, E, J, P, and T; missing Item 15a, number of ischemic stroke cases.

23
IV t-PA WITHIN 60 MINUTES OF ARRIVAL
Of the total number of ischemic stroke cases treated with intravenous thrombolytic therapy (IV t-PA) reported (n=2,392), 64.0% (n=1,532) received IV t-PA within 60 minutes or less from time of hospital arrival (Figure 9).
17 regions reported IV t-PA ≤ 60 minutes of arrival data.
IV t-PA within 60 minutes data was missing for five regions (RACs A, E, J, P, and T).
Seven regions (RACs C, G, H, K, L, O, and V) included data from GWTG-stroke and the RAC Data Surveys.
RAC F reported the highest regional IV t-PA ≤ 60 minutes percentage; 26.1% (n=72) of ischemic stroke
cases that received IV t-PA (n=276).
RAC M reported the lowest regional IV t-PA ≤ 60 minutes percentage; 5.8% (n=46) of ischemic stroke
cases that received IV t-PA (n=793).
The average among the 17 regional percentages reported was 59.5%.
The total number and percent of ischemic stroke cases that received IV t-PA within 60 minutes or less
from time of hospital arrival is displayed in Figure 9 and Table 7.
Figure 9. Percent of ischemic stroke cases that received IV t-PA within 60 minutes or less from time of hospital arrival, July 2015-June 2016.
64.0
28.3
66.7
58.3
66.760.5
57.1
48.5
31.0
61.6
69.666.0
71.866.0
62.6 63.8
56.7
75.7
0
20
40
60
80
100
Total B C D F G H I K L M N O Q R S U V
TOTA
L P
ERC
ENT
(%)
RAC
IV t-PA ≤ 60 MINUTES OF ARRIVAL

24
Table 7. Ischemic stroke cases that received IV t-PA within 60 minutes or less from time of hospital arrival, July 2015-June 2016. RAC Data Survey, Item 19.
IV t-PA ≤ 60 MINUTES OF ARRIVAL
RAC
Ischemic stroke cases that received IV t-PA (n)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
Total number of reporting hospitals Total
number of eligible hospitals
July-Dec 2015
Jan-June 2016
Total 2,392 1,449 83 1,532 64.0 153 159 256
A -- -- -- -- -- -- -- --
B 46 13 -- 13 28.3 17 16 18
C 18 0 12 12 66.7 3 6 13
D 24 14 -- 14 58.3 16 8 17
E -- -- -- -- -- -- -- --
F 72 48 -- 48 66.7 3 6 6
G 147 87 2 89 60.5 9 11 21
H 21 1 11 12 57.1 6 7 8
I 101 49 -- 49 48.5 6 6 9
J -- -- -- -- -- -- -- --
K 29 5 4 9 31.0 11 10 10
L 73 31 14 45 61.6 1 7 10
M 46 32 -- 32 69.6 7 8 7
N 50 33 -- 33 66.0 8 8 8
O 255 164 19 183 71.8 10 4 26
P -- -- -- -- -- -- -- --
Q 952 628 -- 628 66.0 33 32 54
R 182 114 -- 114 62.6 8 10 18
S 58 37 -- 37 63.8 5 7 7
T -- -- -- -- -- -- -- --
U 141 80 -- 80 56.7 3 4 11
V 177 113 21 134 75.7 7 9 13
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 19 that are invalid.
RACs MISSING IV t-PA WITHIN 60 MINUTES OF ARRIVAL DATA
In the RAC Data Survey, guidance was provided that the number of ischemic stroke cases that received IV t-PA within 60 minutes of less of hospital arrival reported for Item 19, must be less than or equal to the total number of ischemic stroke cases treated with IV t-PA reported for Item 18.
▪ RACs A, E, J, P, and T; missing Item 18, number of ischemic stroke cases treated with IV t-PA.

25
ENDOVASCULAR THERAPY
Of the total number of ischemic stroke cases reported (n=18,655), 4.0% (n=748) received endovascular
therapy (IA catheter-based reperfusion) (Figure 10).
17 regions reported endovascular therapy data.
Endovascular therapy data was missing for five regions (RACs A, E, J, P, and T).
Two regions (RACs L and O) included data from GWTG-stroke and the RAC Data Surveys.
Six regions (RACs C, D, H, K, S, and U) reported 0 (0.0%) ischemic stroke cases treated with
endovascular therapy.
RAC F reported the highest regional IA catheter-based reperfusion percentage; 11.2% (n=31) of
ischemic stroke cases (n=276).
The total number and percent of ischemic stroke cases that received IA catheter-based reperfusion
therapy from July 1, 2015 through June 30, 2016 by RAC is displayed in Figure 10 and Table 8.
Figure 10. Percent of ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion), July 2015-June 2016.
4.0
1.40.0 0.0
11.2
2.3
0.0
5.5
0.0 0.4 0.6 0.2
3.75.3
6.5
0.0 0.0
6.6
0
5
10
15
20
Total B C D F G H I K L M N O Q R S U V
TOTA
L P
ERC
ENT
(%)
RAC
ISCHEMIC STROKE CASES THAT RECEIVED ENDOVASCULAR THERAPY

26
Table 8. Ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion), July 2015-June 2016. RAC Data Survey, Item 21.
ISCHEMIC STROKE CASES THAT RECEIVED ENDOVASCULAR THERAPY
RAC
Total ischemic stroke cases (n)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
Total number of reporting hospitals Total
number of eligible hospitals
July-Dec 2015
Jan-June 2016
Total 18,655 739 9 748 4.0 149 153 256
A -- -- -- -- -- -- -- --
B 638 9 -- 9 1.4 17 16 18
C 149 0 -- 0 0.0 2 6 13
D 204 0 -- 0 0.0 16 8 17
E -- -- -- -- -- -- -- --
F 276 31 -- 31 11.2 3 6 6
G 1,134 26 -- 26 2.3 8 11 21
H 276 0 -- 0 0.0 5 5 8
I 910 50 -- 50 5.5 6 6 9
J -- -- -- -- -- -- -- --
K 311 0 -- 0 0.0 10 10 10
L 557 1 1 2 0.4 1 7 10
M 793 5 -- 5 0.6 7 8 7
N 523 1 -- 1 0.2 8 8 8
O 2,322 77 8 85 3.7 10 2 26
P -- -- -- -- -- -- -- --
Q 7,465 392 -- 392 5.3 33 31 54
R 1,031 67 -- 67 6.5 8 10 18
S 230 0 -- 0 0.0 5 7 7
T -- -- -- -- -- -- -- --
U 630 0 -- 0 0.0 3 4 11
V 1,206 80 -- 80 6.6 7 8 13
(--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 21 that are invalid.
RACs MISSING ENDOVASCULAR THERAPY DATA In the RAC Data Survey, guidance was provided that the number of ischemic stroke cases that received endovascular therapy reported for Item 21, must be less than or equal to the total number of ischemic stroke cases reported for Item 15a. ▪ RACs A, E, J, P, and T; missing Item 15a, number of ischemic stroke cases.

27
PICTURE-TO-PUNCTURE WITHIN 60 MINUTES
Of the total number of ischemic stroke cases that received endovascular therapy (IA catheter-based
reperfusion) reported (n=748), 6.6% (n=49) received IA catheter-based reperfusion within 60 minutes or
less from time of initial brain imaging (Figure 11).
11 regions reported picture-to-puncture time ≤ 60 minutes’ data.
Picture-to-puncture data was missing for five regions (RACs A, E, J, P, and T).
No GWTG-stroke data was included.
Six regions (RACs C, D, H, K, S, and U) reported no endovascular therapy.
More than half of the regions (RACs B, L, M, N, Q, and R) reported 0.0% picture-to-puncture time ≤60
minutes.
RAC G reported the highest regional picture-to-puncture time ≤60 minutes percentage; 69.2% (n=18)
of endovascular treatments (n=26).
The total number and percent of ischemic stroke cases that received IA catheter-based reperfusion within
60 minutes or less from time of initial brain imaging is displayed in Figure 11 and Table 9.
Figure 11. Percent of ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion) within 60 minutes or less of time of initial brain imaging, July 2015-June 2016.
6.6
0 NA NA
9.7
69.2
NA
18.0
NA 0 0 0
21.2
0 0 NA NA 1.3
0
20
40
60
80
Total B C D F G H I K L M N O Q R S U V
TOTA
L P
ERC
ENT
(%)
RAC
PICTURE-TO-PUNCTURE ≤ 60 MINUTES OF INITIAL BRAIN IMAGING

28
Table 9. Ischemic stroke cases that received endovascular therapy (IA catheter-based reperfusion) within 60 minutes or less of time of initial brain imaging, July 2015-June 2016. RAC Data Survey, Item 22.
PICTURE-TO-PUNCTURE ≤ 60 MINUTES OF INITIAL BRAIN IMAGING
RAC
Ischemic stroke cases that received endo-vascular therapy (n)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
Total number of reporting hospitals Total
number of eligible
hospitals July-Dec
2015 Jan-June
2016 Total 748 49 0 49 6.6 149 153 156
A -- -- -- -- -- -- -- --
B 9 0 -- 0 0.0 17 16 18
C 0 NA NA NA NA 2 6 13
D 0 NA NA NA NA 16 8 17
E -- -- -- -- -- -- -- --
F 31 3 -- 3 9.7 3 6 6
G 26 18 -- 18 69.2 8 11 21
H 0 NA NA NA NA 5 5 8
I 50 9 . 9 18.0 6 6 9
J -- -- -- -- -- -- -- --
K 0 NA NA NA NA 10 10 10
L 2 0 0 0 0.0 1 7 10
M 5 0 -- 0 0.0 7 8 7
N 1 0 -- 0 0.0 8 8 8
O 85 18 0 18 21.2 10 2 26
P -- -- -- -- -- -- -- --
Q 392 0 -- 0 0.0 33 31 54
R 67 0 -- 0 0.0 8 10 18
S 0 NA NA NA NA 5 7 7
T -- -- -- -- -- -- -- --
U 0 NA NA NA NA 3 4 11
V 80 1 -- 1 1.3 7 8 13 (--) missing; data is missing as a result of values submitted for RAC Data Survey; Item 22 that are invalid. (NA) not applicable to report a value.
RACs MISSING PICTURE-TO-PUNCTURE WITHIN 60 MINUTES DATA In the RAC Data Survey, guidance was provided that the number of ischemic stroke cases that received endovascular therapy within 60 minutes of initial brain imaging reported for Item 22, must be less than or equal to the total number reported for Item 21. ▪ RACs A, E, J, P, and T; missing Item 15a, number of ischemic stroke cases.

29
DISCHARGE DISPOSITION OF ISCHEMIC STROKE CASES
The discharge disposition of ischemic stroke cases was reported as follows; 3,176 (17.0%) home, 1,353
(7.3%) inpatient rehabilitation facility, 867 (4.6%) skilled nursing facility, 222 (1.2%) hospice, 307 (1.6%)
expired, and 4,881 (26.2%) other or not documented or unknown (Table 10a-b).
10 regions reported discharge disposition data.
Discharge disposition data was missing for 12 regions (RACs A, C, D, E, F, G, J, K, M, P, R, and T).
Four regions (RACs H, L, O, and V) included discharge disposition data from GWTG-stroke and the RAC
Data Surveys.
Discharged home was the most common disposition among eight regions (RACs B, H, L, N, O, S, U, and
V).
RAC L reported the highest regional percentage of ischemic stroke patients (n=557) discharged home;
53.7% (n=299).
The discharge disposition of ischemic stroke cases by RAC is displayed in Figure 12 and Tables 10a-b.
Figure 12. Discharge disposition of ischemic stroke cases, July 2015-June 2016.
0
20
40
60
Total B H I L N O Q S U V
TOTA
L P
ERC
ENT
(%)
RAC
DISCHARGE DISPOSITION OF ISCHEMIC STROKE CASES
Home Inpatient Rehabilitation Facility Skilled Nursing Facility
Hospice Expired Not Documented

30
Table 10a. Discharge disposition of ischemic stroke cases, July 2015-June 2016. RAC Data Survey, Item 23.
RAC
Total ischemic stroke cases (n)
Home Inpatient Rehabilitation Facility Skilled Nursing Facility
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
Total 18,655 2,691 485 3,176 17.0 1,116 237 1,353 7.3 743 114 867 4.6 A -- -- -- -- -- -- -- -- -- -- -- -- -- B 638 259 -- 259 40.6 74 -- 74 11.6 57 -- 57 8.9 C 149 -- -- -- -- -- -- -- -- -- -- -- -- D 204 -- -- -- -- -- -- -- -- -- -- -- -- E -- -- -- -- -- -- -- -- -- -- -- -- -- F 276 -- -- -- -- -- -- -- -- -- -- -- -- G 1,134 -- -- -- -- -- -- -- -- -- -- -- -- H 276 27 86 113 40.9 3 63 66 23.9 14 28 42 15.2 I 910 234 -- 234 25.7 88 -- 88 9.7 55 -- 55 6.0 J -- -- -- -- -- -- -- -- -- -- -- -- -- K 311 -- -- -- -- -- -- -- -- -- -- -- -- L 557 185 114 299 53.7 40 35 75 13.5 56 47 103 18.5
M 793 -- -- -- -- -- -- -- -- -- -- -- -- N 523 246 -- 246 47.0 86 -- 86 16.4 88 -- 88 16.8 O 2,322 961 197 1,158 49.9 472 104 576 24.8 198 30 238 10.2 P -- -- -- -- -- -- -- -- -- -- -- -- -- Q 7,465 -- -- -- -- -- -- -- -- -- -- -- -- R 1,031 -- -- -- -- -- -- -- -- -- -- -- -- S 230 94 -- 94 40.9 52 -- 52 22.6 18 -- 18 7.8 T -- -- -- -- -- -- -- -- -- -- -- -- -- U 630 309 -- 309 49.0 130 -- 130 20.6 191 -- 191 30.3
V 1,206 376 88 464 38.5 171 35 206 17.1 66 9 75 6.2
(--) missing; data is missing as a result of values submitted for RAC data survey; item 23a-f that are invalid.

31
Table 10b. Discharge disposition of ischemic stroke cases, July 2015-June 2016. RAC Data Survey, Item 23.
RAC
Total ischemic stroke cases (n)
Hospice (home or facility) Expired Other or Not Documented
Total number of reporting hospitals Total
number of eligible hospitals
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
July-Dec
2015
Jan-June 2016
Total 18,655 184 37 222 1.2 235 44 307 1.6 4,852 41 4,881 26.2 98 100 164
A -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
B 638 12 -- 12 1.9 21 -- 21 3.3 58 -- 58 9.1 17 16 18
C 149 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
D 204 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
E -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
F 276 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
G 1,134 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
H 276 3 15 18 6.5 2 5 7 2.5 16 9 25 9.1 6 7 8
I 910 28 -- 28 3.1 29 -- 29 3.2 476 14 490 53.8 6 6 9
J -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
K 311 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
L 557 8 5 13 2.3 16 14 30 5.4 28 5 33 5.9 1 7 10
M 793 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
N 523 23 -- 23 4.4 9 -- 9 1.7 51 -- 51 9.8 8 8 8
O 2,322 64 15 80 3.4 90 17 135 5.8 120 -- 108 4.7 12 4 26
P -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
Q 7,465 -- -- -- -- -- -- -- -- 4,001 -- 4,001 53.6 33 32 54
R 1,031 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
S 230 2 -- 2 0.9 9 -- 9 3.9 49 -- 49 21.3 5 7 7
T -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
U 630 23 -- 23 3.7 24 -- 24 3.8 22 -- 22 3.5 3 4 11
V 1,206 21 2 23 1.9 35 8 43 3.6 31 13 44 3.6 7 9 13
(--) missing; data is missing as a result of values submitted for RAC data survey; item 23a-f that are invalid.

32
RACs MISSING DISCHARGE DISPOSITION DATA In the RAC Data Surveys, guidance was provided that the discharge disposition of ischemic stroke cases reported in Item 23, must be less than or equal to the number of ischemic stroke cases reported. RACs A, E, J, P, and T; missing Item 15a, number of ischemic stroke cases. RACs K, P, and T, Survey 1; the sum of discharge dispositions reported for Item 23a-f was greater than
the number of ischemic stroke cases, Item 15a. RACs A, C, and J, Survey 2; the sum of discharge dispositions reported for Item 23a-f was greater than
the number of ischemic stroke cases, Item 15a. RACs E, F, G, and M, Survey 1 and Survey 2; the sum of discharge dispositions reported for Item 23a-f
was greater than the number of ischemic stroke cases, Item 15a. RAC R, Survey 1 and Survey 2; did not report data for Item 23.
HEALTH INSURANCE STATUS OF ISCHEMIC STROKE CASES
Of the total number of ischemic stroke cases (n=18,655), 21.2% (n=3,960) had a form of health insurance
documented, 3.4% (n=634) did not have health insurance, and 22.3% (n=4,163) health insurance status
was not documented or unknown (Figure 13).
Nine regions reported health insurance data.
Health insurance status was missing for 13 regions (RACs A, C, E, F, G, I, J, K, M, P, R, T, and U).
Four regions (RACs H, L, O, and V) included data from GWTG-stroke and the RAC Data Surveys.
RAC N reported the highest regional percentage of any health insurance; 88.3% (n=462) of ischemic
stroke cases (n=523).
RAC B reported the highest regional percentage of no health insurance; 18.2% (n=116) of ischemic
stroke cases (n=638).
The health insurance status of ischemic stroke cases by RAC is displayed in Figure 13-14 and Table 11.
Figure 13. Health insurance status of ischemic stroke cases, July 2015-June 2016.
21.2
67.1
11.3
71.0
50.1
88.3
78.3 80.4
47.3
3.4
18.211.8 12.7
6.611.7 10.4
15.2
7.0
22.3
4.21.0
8.32.3 0.0 3.5
53.6
4.3 0.40
20
40
60
80
100
Total B D H L N O Q S V
TOTA
L P
ERC
ENT
(%)
RAC
HEALTH INSURANCE STATUS OF ISCHEMIC STROKE CASES
Any Health Insurance No Health Insurance Not Documented

33
Table 11. Health insurance status of ischemic stroke cases, July 2015-June 2016. RAC Data Survey, Item 20.
RAC
Total ischemic stroke cases (n)
Any Health Insurance No Health Insurance Not Documented or Unknown Total number of reporting hospitals
Total number
of eligible
hospitals
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
RAC Survey (n)
GWTG-stroke (n)
Total (n)
Total Percent (%)
July-Dec 2015
Jan-June 2016
Total 18,655 3,165 795 3,960 21.2 543 91 634 3.4 4,076 87 4,163 22.3 105 98 161
A -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
B 638 428 -- 428 67.1 116 -- 116 18.2 27 -- 27 4.2 17 16 18
C 149 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
D 204 23 -- 23 11.3 24 -- 24 11.8 2 -- 2 1.0 16 8 17
E -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
F 276 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
G 1,134 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
H 276 38 158 196 71.0 5 30 35 12.7 0 23 23 8.3 6 7 8
I 910 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
J -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
K 311 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
L 557 84 195 279 50.1 17 20 37 6.6 4 9 13 2.3 1 7 10
M 793 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
N 523 462 -- 462 88.3 61 -- 61 11.7 0 -- 0 0.0 8 8 8
O 2,322 1,518 299 1,817 78.3 213 29 242 10.4 27 55 82 3.5 12 4 26
P -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
Q 7,465 -- -- -- -- -- -- -- -- 4,001 -- 4,001 53.6 33 32 54
R 1,031 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
S 230 185 -- 185 80.4 35 -- 35 15.2 10 -- 10 4.3 5 7 7
T -- -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
U 630 -- -- -- -- -- -- -- -- -- -- -- -- -- -- --
V 1,206 427 143 570 47.3 72 12 84 7.0 5 0 5 0.4 7 9 13
(--) missing; data is missing as a result of values submitted for RAC data survey; item 20 that are invalid.

34
Figure 14. Percent of ischemic stroke cases with any health insurance by RAC, Texas, July 2015-June2016.
RACs MISSING HEALTH INSURANCE STATUS DATA In the RAC Data Surveys, guidance was provided that the health insurance status of ischemic stroke cases reported in Item 20, must be less than or equal to the number of ischemic stroke cases reported. RACs A, E, J, P, and T; missing Item 15a, number of ischemic stroke cases. RACs G and I, Survey 1; the sum of health insurance status reported for Item 20 was greater than the
number of ischemic stroke cases, Item 15a. RACs U and C, Survey 2; the sum of health insurance status reported for Item 20 was greater than the
number of ischemic stroke cases, Item 15a. RACs F, J, K, and P, Survey 1 and Survey 2; the sum of health insurance status reported for Item 20
was greater than the number of ischemic stroke cases, Item 15a. RAC R, Survey 1 and Survey 2; did not report data for Item 20.

35
LIMITATIONS
The measures and values reported represent aggregate RAC-level data and do not represent
individual hospital performance.
Hospitals participation was voluntary however RACs were encouraged to gather data as much as
possible.
The accuracy of the hospital-level data collected by the RAC affects the accuracy of the final aggregate
RAC-level data submitted to DSHS. For example, for RACs A, E, J, P, and T the sum of reported stroke
cases by classification was larger than the reported total number of stroke cases. Thus, classification
of stroke for these RACs was set to missing (Table 3a-b).
Only the total number of hospitals reporting stroke data for each RAC is known. It cannot be assumed
that the same hospitals reported data for both data collection periods.
Only the total number of hospitals reporting stroke data for each RAC is known. The data received by
DSHS via the RAC Data Surveys were aggregated at the RAC-level. So it cannot be assumed that all
hospitals reported on all measures asked.
The number of hospitals reporting per region includes the number of hospitals reported for the RAC
Data Survey and hospitals reporting from GWTG-stroke.

36
REFERENCES
1. 2014 Texas Vital Statistics, Mortality Data. Texas Department of State Health Services, Austin, TX.
2. Texas Behavioral Risk Factor Surveillance System Public Use Data File, 2015. Texas Department of State
Health Services, Austin, TX.
3. Texas Hospital Inpatient Discharge Public Use Data File, 2014. Texas Department of State Health
Services, Austin, TX.

37
APPENDICES
APPENDIX A

38
APPENDIX B
Rider 97 RAC Data Survey #1 2016-03-01
Introduction
Stroke and STEMI Data Collection
The purpose of data collection among the Regional Advisory Councils (RACs) is to enhance surveillance
of the stroke and STEMI systems of care in Texas. RACs will collect and report data to the Health
Promotion and Chronic Disease Prevention Section (HPCDPS) of DSHS and HPCDPS will analyze the
data and report results of the analyses to RACs and the Texas Council on Cardiovascular Disease and
Stroke, as well as other stakeholders.
DSHS is asking RAC (leadership, RAC Chairs or RAC Directors and, if applicable, Stroke Committee
Chairs and Cardiac Committee Chairs, or others) to work with key stakeholders in their regions to
complete this survey. Information must be entered into every field to move forward to the next question.
If your response to a question is a zero (0), please enter "0" in the text box. If you are not able to provide
a response or compile the necessary data, please enter "NA" in the text box. Please provide the most
accurate and complete data as possible.
This survey is due March 1, 2016, and should only include data from July 1, 2015, through
December 31, 2015. If you have any questions about taking the survey, please contact Randy
Crutsinger at 512-776-6525 or [email protected].
Thank you in advance for your time.

39
Rider 97 RAC Data Survey #1 2016-03-01
RAC Information
1. RAC Information
RAC Name:
Trauma Service Area:
2. Person entering data
Name:
Email Address:
Phone Number:
3. Your Professional Title:
4. I am the:
RAC Chair
RAC Executive Director
Stroke Committee Chair
Cardiac Committee Chair
Other (please specify)

40
Rider 97 RAC Data Survey #1 2016-03-01
Regional Hospital Stroke Data
Please consult the hospitals in your Trauma Service Area to enter the following data.
INCLUSION CRITERIA (Questions 14-22): Stroke is defined as a case with a final clinical diagnosis
related to stroke regardless of time last known well that presented to the emergency department during
the corresponding months regardless of admission or transfer status. Exclude strokes that occurred
after hospital arrival (ED/observation/inpatient).
14. Total number of stroke cases from July 1, 2015 through December 31, 2015.
15. Classification of stroke cases reported in Item 14.
Logic: 15a + 15b + 15c + 15d + 15e must be less than or equal to Item 14.
15a. Number of ischemic
Strokes
15b. Number of Intracerebral
hemorrhages
15c. Number of
Subarachnoid
Hemorrhages
15d. Number of Transient
Ischemic Attack (< 24
hours) (TIA)
15e. Number of stroke not
otherwise specified

41
16. Arrival method for the stroke cases reported in Item 14.
Logic 16a +16b + 16c + 16d must be less than or equal to Item 14.
16a. Number arriving via
EMS from home/scene
16b. Number arriving via private
transport/taxi/other from
home/scene
16c. Number arriving via
transfer from other hospital
16d. Number with arrival mode
not documented or unknown
17. Of the ischemic stroke cases reported in Item 15a, how many had an NIH stroke scale performed?
Logic: Must be a number less than or equal to Item 15a.
18. Of the ischemic stroke cases reported in Item 15a, how many received t-PA therapy?
Logic: Must be a number less than or equal to Item 15a.
19. Of the cases reported in Item 18, how many received t-PA within 60 minutes or less from the time of
arrival?”
Logic: Must be a number less than or equal to Item 18.
20. Of the ischemic stroke cases reported in Item 15a, indicate the health insurance status for these cases.
Logic: 20a + 20b + 20c must be less than or equal to Item 15a
20a. Number with any health
insurance
20b. Number without health
insurance
20c. Number with health
insurance not documented or
unknown.

42
21. Of the ischemic stroke cases reported in Item 15a, how many received endovascular therapy? Logic:
Must be a number less than or equal to Item 15a.
22. Of the endovascular therapy cases reported in Item 21, how many received endovascular therapy within
60 minutes?
Definition: Number includes all cases that received IA catheter-based treatment within 60 minutes or less from
time of initial brain imaging (“picture to puncture” time ≤ 60 minutes). Time difference between pretreatment
neuroimaging (picture) and receiving IA catheter-based treatment (puncture) is equal or less than 60 minutes.
This is regardless of IV t-PA status.
EXCLUSION CRITERIA: patients where the time of IA catheter-based treatment was earlier than time for brain
imaging and patients where IA catheter-based treatment was done outside your hospital.
Logic: Must be a number less than or equal to item 21.
23. Of the total ischemic stroke cases reported in Item 15a, how many met the following disposition
categories?
Logic: 23a + 23b + 23c + 23d + 23e + 23f = Item 15a.
23a. Number discharged to
home
23b. Number discharged to
inpatient rehabilitation
23c. Number discharged to
skilled nursing facility
23d. Number discharged to
hospice care (home hospice or
facility hospice)
23e. Number expired
23f. Number discharged to
“other” or not known/reported

43
24. Please provide a list of individual hospital names that contributed to the STROKE data.
Please separate individual hospital names with a semicolon (;). If the individual hospital is part of a hospital system
please use the following naming convention: Hospital System name - individual hospital name or location.

44
Rider 97 RAC Data Survey #1 2016-03-01
Thank You For Your Time
Thank you for completing this assessment of the STEMI and stroke systems of care in your Trauma
Service Area. This information will assist Texas organizations in providing leadership, technical
assistance, training, and additional resources to areas where system building is needed.

45
Rider 67 RAC Data Survey #2 2016-08-31
Introduction
Stroke and STEMI Data Collection
The purpose of data collection among the Regional Advisory Councils (RACs) is to enhance surveillance
of the stroke and STEMI systems of care in Texas. RACs will collect and report data to the Health
Promotion and Chronic Disease Prevention Section (HPCDPS) of DSHS and HPCDPS will analyze the
data and report results of the analyses to RACs and the Texas Council on Cardiovascular Disease and
Stroke, as well as other stakeholders.
DSHS is asking RAC (leadership, RAC Chairs or RAC Directors and, if applicable, Stroke Committee
Chairs and Cardiac Committee Chairs, or others) to work with key stakeholders in their regions to
complete this survey. Information must be entered into every field to move forward to the next question.
If your response to a question is a zero (0), please enter "0" in the text box. If you are not able to provide
a response or compile the necessary data, please enter "NA" in the text box. Please provide the most
accurate and complete data as possible.
This survey is due August 31, 2016, and should only include data from January 1, 2016, through June
30, 2016. If you have any questions about taking the survey, please contact Randy Crutsinger at 512-
776-6525 or [email protected].
Thank you in advance for your time.

46
Rider 67 RAC Data Survey #2 2016-08-31
RAC Information
1. RAC Information
RAC Name:
Trauma Service Area:
2. Person entering data
Name:
Email Address:
Phone Number:
3. Your Professional Title:
4. I am the:
RAC Chair
RAC Executive Director
Stroke Committee Chair
Cardiac Committee Chair
Other (please specify)

47
Rider 67 RAC Data Survey #2 2016-08-31
Regional Hospital Stroke Data
Please consult the hospitals in your Trauma Service Area to enter the following data.
INCLUSION CRITERIA (Questions 14-22): Stroke is defined as a case with a final clinical diagnosis
related to stroke regardless of time last known well that presented to the emergency department during
the corresponding months regardless of admission or transfer status. Exclude strokes that occurred
after hospital arrival (ED/observation/inpatient).
14. Total number of stroke cases from January 1, 2016 through June 30, 2016.
15. Classification of stroke cases reported in Item 14.
Logic: 15a + 15b + 15c + 15d + 15e must be less than or equal to Item 14.
15a. Number of ischemic
Strokes
15b. Number of Intracerebral
hemorrhages
15c. Number of
Subarachnoid
Hemorrhages
15d. Number of Transient
Ischemic Attack (< 24 hours)
(TIA)
15e. Number of stroke not
otherwise specified

48
16. Arrival method for the stroke cases reported in Item 14.
Logic 16a +16b + 16c + 16d must be less than or equal to Item 14
16a. Number arriving via
EMS from home/scene
16b. Number arriving via private
transport/taxi/other from
home/scene
16c. Number arriving via
transfer from other hospital
16d. Number with arrival mode
not documented or unknown
17. Of the ischemic stroke cases reported in Item 15a, how many had an NIH stroke scale performed?
Logic: Must be a number less than or equal to Item 15a
18. Of the ischemic stroke cases reported in Item 15a, how many received t-PA therapy?
Logic: Must be a number less than or equal to Item 15a
19. Of the cases reported in Item 18, how many received t-PA within 60 minutes or less from the time of
arrival?”
Logic: Must be a number less than or equal to Item 18
20. Of the ischemic stroke cases reported in Item 15a, indicate the health insurance status for these cases.
Logic: 20a + 20b + 20c must be less than or equal to Item 15a
20a. Number with any health
insurance
20b. Number without health
insurance
20c. Number with health
insurance not documented or
unknown.

49
21. Of the ischemic stroke cases reported in Item 15a, how many received endovascular therapy?
Logic: Must be a number less than or equal to Item 15a
22. Of the endovascular therapy cases reported in Item 21, how many received endovascular therapy
within 60 minutes?
Definition: Number includes all cases that received IA catheter-based treatment within 60 minutes or
less from time of initial brain imaging (“picture to puncture” time ≤ 60 minutes). Time difference between
pretreatment neuroimaging (picture) and receiving IA catheter-based treatment (puncture) is equal or
less than 60 minutes. This is regardless of IV t-PA status.
EXCLUSION CRITERIA: patients where the time of IA catheter-based treatment was earlier than time for
brain imaging and patients where IA catheter-based treatment was done outside your hospital.
Logic: Must be a number less than or equal to item 21
23. Of the total ischemic stroke cases reported in Item 15a, how many met the following disposition
categories?
Logic: 23a + 23b + 23c + 23d + 23e + 23f = Item 15a
23a. Number discharged to
home
23b. Number discharged to
inpatient rehabilitation
23c. Number discharged to
skilled nursing facility
23d. Number discharged to
hospice care (home hospice or
facility hospice)
23e. Number transferred to
higher level of care
23e. Number expired
23g. Number discharged to
“other” or not known/reported

50
24. Please provide a list of individual hospital names that contributed to the STROKE data.
Please separate individual hospital names with a semicolon (;). If the individual hospital is part of a hospital system
please use the following naming convention: Hospital System name - individual hospital name or location.

51
Rider 67 RAC Data Survey #2 2016-08-31
Thank You For Your Time
Thank you for completing this assessment of the STEMI and stroke systems of care in your Trauma
Service Area. This information will assist Texas organizations in providing leadership, technical
assistance, training, and additional resources to areas where system building is needed.