Refractory ascites
94
CHAIR PERSON : PROF.DR.RAVI .K CO CHAIR PERSON:ASSOC.PROF.DR.KAVYA PRESENTER:DR.ASHOKVARDHANREDDY.T
-
Upload
ashok-t -
Category
Health & Medicine
-
view
292 -
download
1
Transcript of Refractory ascites

CHAIR PERSON : PROF.DR.RAVI .K
CO CHAIR PERSON:ASSOC.PROF.DR.KAVYA
PRESENTER:DR.ASHOKVARDHANREDDY.T

PATHOPHYSIOLOGY OF ASCITES
REFRACTORY ASCITES
DEFINITION,
CAUSES
PATHOPHYSIOLOGY
TREATMENT

Ascites is the most common complication
in patients with cirrhosis.
It develops as a consequence of a severe
impairment of liver function and portal
hypertension.

PORTAL HYPERTENSION
Nitric oxide
SPLANCHNIC VASO
DILATATION

RENAL SODIUM
RETENTION
OVERFILL OF
INTRA VASCULAR
VOLUME
ASCITES
Sympathetic
Activity,
RAAS

The central event of ascites formation in
cirrhosis is a splanchnic arterial vasodilatation
secondary to portal hypertension.
1 Backward theory :pressure due to resistance in
liver
2 Forward theory :splanchnic bed vaso
dilatation.
3 Overflow theory-Increased plasma volume
increases hepatic lymph formation.
4 Underfilling theory – Arterial under filling

Clinical examination
Usg abdomen- liver size
portal vein
homogenous – transudate
multiple echogenic shadows –exudate
Fluid collects first in flanks,right upper quadrant ,para colic gutter , and around liver
Multiple echos ,septations ,fibrous strands indicates ascites unrelated to portal hypertension.

Grade 1-Detectable by ULTRASOUND
abdomen.
Grade 2-symmetrical distension of
abdomen.shifting dullness present.
Grade 3 :Marked abdominal distension.
fluid thrill present

Total ascitic fluid protein is inversely
related to portal hypertension.
As the disease severity increases ,protein
levels decrease
SBP develops in total ascitic fluid protein <1
g/dl
High concentration of macrophages is found
in ascitic fluid
Bloody ascites occurs in 2 % patients

In patients with cirrhosis a complex coagulation
process within the ascitic fluid results in intra
peritoneal coagulation and primary and
secondary fibrinolysis.
The macrophages of ascitic fluid synthesize
vasodilatatory substances (e.g., nitric oxide,
adreno medullin, vascular endothelial growth
factor). The pathophysiologic significance of this
finding is unknown.
The concentration of leptin and vascular
endothelial growth factor is higher in ascitic
fluid than in plasma .

Ascitic fluid has anti bacterial activity, which
correlates directly with the total ascitic fluid
protein concentration . Substances such as
complement, fibronectin, cytokines, and are
implicated in this effect.
Infusion of ascitic fluid within the general
circulation is associated with important biologic
effects, the most important being intravascular
coagulation and fever.

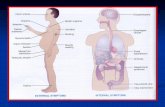
A single layer of mesothelial cells covers
the peritoneal surface of the diaphragm over
a connective tissue matrix with a very rich
plexus of terminal lymphatic vessels
(lymphatic lacunae) .
Lacunae are large enough to allow the
passage of erythrocytes, connect the
peritoneal cavity with the lumen of the
terminal lymphatics.

The submesothelial lymphatic plexus drains into
parasternal trunks on the ventral thoracic wall,
right lymphatic duct, and right subclavian or
internal jugular vein.
During inspiration, lacunae are emptied
During expiration, the gaps open and
communication is re established.
The estimated mean rate of ascitic fluid
reabsorption is 1.4 L/day, ranging from less than
0.5L to more than 4L.

Furosemide and spironolactone are the most
commonly used drugs

o Furosemide and spironolactone are most
commonly used drugs

Two different approaches for patients with cirrhosis and ascites-
1 step care approach –sodium restriction
spironolactone 100 mg/day
No response in 4 days
200 mg/day
no response in 4 days
400 mg/day

No response at 400 mg spironolactone /day
start furosemide 40 mg /day
Can be increased to 160 mg /day
Dose escalated by 40 mg every 2 days.

Simultaneous administration of Na
restriction ,
Spironolactone 100 mg/day
Furosemide 40 mg/day
4 days
dose increased to 200 spironolactone
+
80 mg furosemide

Complications of diuretics
Renal failure
Hyponatremia
Hepatic encephalopathy
Hypo/hyper kalemia
Hyper uricemia

Furosemide challenge test-
80 mg furosemide iv
urine collection for next 8 hrs
Urine sodium <50 m Eq for 8 hrs is indicative of resistance
Random urine Na/k ratio >1
Indicates 24 hr urine Na excretion >78 m Mol/day.
WORLD JOURNAL OF GASTRO ENTEROLOGY
SENOUSY ETAL , 2009 JANUARY

Once in 2 weeks
Check body weight
BP
Look for orthostatic symptoms
serum electrolytes
Blood urea ,serum creatinine
WORLD JOURNAL OF GASTRO ENTEROLOGY
JANUARY 2009


Refractory ascites applies to the ascites that
cannot be mobilized(minimal /no weight
loss)despite adherence to sodium
restriction(88 m eq/2000 mg/day) or the
early recurrence of which (i.e., after
therapeutic paracentesis) cannot be
prevented by medical therapy.
International ascites club
Arroyo V etal .Hepatology ,1996 .

1 DIURETIC RESISTANT ASCITES:
Loss of body weight <200 g /day after 4 days of treatment or recurrence cannot be prevented even after
dietary sodium restriction <50 m eq/day {<90 m Eq/day EASL}
Furosemide 160 mg/day AND
Spironolactone 400 mg/day { SCHIFFS DISEASES OF LIVER}/
600 mg /day {HARRISONS TEXT BOOK OF INTERNAL MEDICINE} for at least 1 week.
Recurs rapidly after therapeutic paracentesiswith in 4 weeks {AASLD}

2 DIURETIC INTRACTABLE ASCITES:
Ascites cannot be mobilised / recurrence
cannot be prevented due to diuretic induced
complications that precludes use of effective
diuretic dose.
Eg –Hepatic encephalopathy in absence of
any precipitating cause

Increase in creatinine levels >100% to a value
>2 mg %
Decrease in serum sodium level by >10
mEq/L to a concentration <125 mEq/L.
Decrease of serum potassiumlevel to <3
mEq/L or an increase to >6 mEq/L despite
appropriate measures to normalize potassium
concentration.

Most patients with cirrhosis and ascites with
serum creatinine >1.2 mg/dl reflects
decrease in renal blood flow and GFR by >50
% .

Renal hypo perfusion
Impairment of access of diuretics to
effective sites on the tubular cells
excessive reabsorption of Na + in PCT
Reduced delivery of sodium to ascending
limb of loop of henle and the distal nephron

Peritoneo venous shunt.
TIPS(Trans jugular Intrahepatic Portosystemic
Shunt).
Therapeutic paracentesis .

Remove ascitic fluid before inserting prosthesis
To avoid massive passage of ascitic fluid in to circulation
Pulmonary edema ,
Variceal bleed,
Intravascular coagulation.

Prophylactic administration of anti
staphylococcal antibiotics is recommended
atleast for 3 days.

.


Passage of ascitic fluid from abdominal cavity to systemic circulation
Sustained expansion of circulating blood volume
Renin,nor epinephrine,ADH, response to diuretics
Its very good that patient feels better immediately,and it appears rational therapy for refractory ascites …….BUT

40 % obstruction of shunt with
in 1 yr
{Fibrin deposits in valve / catheter,thrombus
in venous limb of prosthesis, thrombus in SVC
causing obstruction}
10 % small bowel obstruction in
long term {intra peritoneal fibrosis}

Remove the prosthesis and insert new one

1 st described by CELSUS in 20 B.C
Ludvig van beethoven in 1827 received large
volume paracentesis ….2 days after which he
expired.


NECESSITY –
10-20 % of patients are diuretic resistant.
Complications are high with diuretics.
Diuretics take time to reduce ascites.

Therapeutic paracentesis is considered the
best therapy for tense ascites in cirrhosis .
It considerably shortens hospital stay ,the cost
of treatment, incidence of
complications during hospitalization than
among those treated with diuretics .

1-
Repeated large volume paracentesis.
Ascites can leak in to abdominal
wall/outside.
2-
Total paracentesis
Fluid is removed at once
Less complication rate


7 cm length
17 G
Blunt edged cannula with side holes
Left lower quadrant
To be connected to suction pump,30 – 60 mins( free flow of ascitic fluid is recommended now)
Precaution – patient should recline on opposite side for 2 hrs to prevent leakage of ascitic fluid


Few studies –no apparent major changes in
circulatory function
Arterial pressure
PR – No change
Ascites disappears
Creatinine and electrolytes –no change

Intra thoracic pressure
Circulatory function
Stroke volume,cardiac output
cardio pulmonary pressure , Renin

plasma renin levels which peaks on 6
th day of paracentesis leads to
angiotensin II,nor epinephrine
vaso constriction of intrahepatic
vessels-thereby resistance portal
pressure

Patients admitted for tense ascites and not on treatment and in 1 week hospital stay-16 %
Paracentesis induced circulatory dysfunction in patients not on plasma volume expansion -75 %
Patients on polygeline {8g/l ascitic fluid}-33-38 %
Patients on albumin {8g/l ascitic fluid}-11-18%

If amount drained is <5 l – incidence is 16%
with albumin vs 18 % with synthetic plasma
expander .
If 5-9 l- incidence 19% vs 30 %
>9 l 52 % with synthetic plasma expanders.

Risk of peritoneal bleeding 0.5-1 %
Leakage of ascitic fluid from tap
site…managed by z technique.
PICD (Paracentesis induced circulatory
dysfunction.)
Plasma renin increase > 50 % of pre
treatment value to above 4 ng/ml on 6 th
day after paracentesis.

Spontaneous bacterial peritonitis
Creatinine >3 mg/dl
Severe hepatic encephalopathy
Hypotension
Disseminated intra vascular coagulation
Caution in patients with abdominal adhesions

Albumin infusion
Incidence of Hyponatremia 3.8 %
renal impairment -0%
No plasma expander-
Hyponatremia – 17 %
Renal impairment 11 %

If we drain < 5 l ascitic fluid –
less expensive synthetic plasma expanders -8g/l ascitic fluid can be used
If > 5 l is drained albumin infusion is advised 8 g /l
50% immediately after paracentesis
6 hrs
50 % to be given
Diuretics to be continued If BUN and serum creatinine are normal –
200 mg / day spiranolactone or 40 mg /day furosemide + 100 mg /day spironolactone …..

paracentesis Leveen shunt
Ascites episodes 125 38
Lvs obstruction 40 % in 1 yr
Days in hospital 48 +/-6 44+/- 6
Survival 1 yr 57 % 44%

Innovative idea of usage of cvp catheter for
drainage of ascitic fluid was tried to reduce
the hospitalisation rate ,and so morbidity
Shahram agah,sahar tavakoli,Hajar nikbakth,Mehrdokht
Najafi,Abdolreza al agha
Colorectal research center ,IRAN UNIVERSITY OF MEDICAL
SCIENCES

Precise percussion and point of highest fluid
accumulation should be marked for puncture
site.
Local anesthesia with 5-10 ml of 2 %
lignocaine inj.
Punctured using 18 G needle
Perpendicular to skin

Guide wire passed through needle.
Remove the needle .
Pass the catheter through guide wire till wing meet the skin .
catheter outlet attached to urine bag .
Drainage started at the rate of 250 -500 ml/hr.
Vital signs checked every 15 mins once during procedure.
8 g Albumin is infused for 1 l of ascitic fluid drained.

After complete drainage of ascitic fluid
{< 100 ml fluid drained /day}.
All patients were prescribed diuretics ,low
sodium diet on followed up.

Re admission rate was 1.9 in 1 yr follow up
(2-4 times in routene paracentesis)
Serum sodium showed no significant change ,
Potassium – no significant change
Creatinine decreased with in 24 hrs.



Trans jugular intra hepaic portosystemicshunt
Endogenous vaso constrictor
system
Renal function , GFR,response to
diuretics
Lymph formation in liver and other
splanchnic organs

marked in renin, aldosterone with in 1
week
ADH and Nor epinephrine in 2
weeks
GFR increases ,
urinary excretion of Na increases in 1-2
weeks
Free water clearance

TIPS porto caval gradient
In 358 patients with refractory ascites with
TIPS
Porto caval gradient decreased from 20.9
10 mm Hg
Portal venous pressure 29.4 mm Hg
21.8 mm Hg
Ascites resolves in 1-3 months
10 % patients doesn’t respond to TIPS
Diuretics are required in >95 % cases

TOTAL BILIRUBIN >5 mg/dl
PT INR>2
CHILD PUGH SCORE>11
MELD SCORE >18
HEPATIC ENCEPHALOPATHY >/= 2
INFECTIONS
RENAL FAILURE
CARDIOPULMONARY DECOMPENSATION

Most common – hepatic encephalopathy
Occurs in > 40 % patients
Responds to standard therapy
May require to decrease the stent size
Early mortality {with in 30 days} occurs in 12
%
Late mortality in 40 %

Worsening of Liver function tests due to
liver ischemia due to diversion of portal
blood to systemic circulation
Cardiac failure
Migration of stent to right heart or lung
Endo tipssitis
Transient intra vascular hemolysis Reference –API Medicine update ..Aabha nagral

study Type of
ascites
Control of
ascites
Hepatic
encephalop
athy
survival
LEBREC etal
1994
Refractory
ascites
Better with
TIPS
NO
difference
Worse with
TIPS
ROSSLE etal Refractory
& recidivant
Better with
TIPS
No
difference
Better with
TIPS
GINES etal Refractory Better with
TIPS
Worse with
TIPS
No
difference
SANYAL etal Refractory Better with
TIPS
Worse with
TIPS
No
difference
SALERNO
etal2004
Refractory
& recidivant
Better with
TIPS
Worse with
TIPS
Better with
TIPS

TIPS changes course of cirrhosis from ascites
to hepatic encephalopathy without improving
overall results of paracentesis , in relation to
length of hospitalisation .

Medical therapy –
Beta blockers contra indicated ( hypotension)
Midodrine 7.5 mg tid can be started
urine output
urine sodium
mean arterial pressure
Diuretic resistant diuretic sensitive

Refractoriy ascites
discontinue betablockers,
add midodrine 7.5 mg
tid
If not responding
Consider 1 serial therapeutic paracentesis
2 liver transplant
3 TIPS
4 experimental medical treatment

Large volume therapeutic paracentesis-{
atleast 5 L}
Total paracentesis is recommended
Once in 2 weeks or once in 1 week
Colloid replacement- In a randomised
control study 105 patients with tense
ascites-
Albumin 1g/L vs without albumin infusion
was studied

Significant increase in renin ,
creatinine,
serum electrolytes are observed without
albumin infusion.
But no more clinical morbidity and mortality

o hr Terlpressin iv 1 mg starting of
paracentesis
8 hr iv 1 mg repeat +tab midodrine
5 mg tid
16 hr iv 1 mg repeat
EQUIVALENT to albumin in suppressing
renin

Chronic therapeutic paracentesis is reserved
for only 10 % patients who fail diuretics
As it causes hypo proteinemia,
Malnutrition
Increased infections
Prognosis of refractory ascites –
Bad.21 % die in 6 months

TIPS vs Large volume therapeutic paracentesis
Significant survival advantage
Better control of ascites
More chances of encephalopathy
Caution- patients with renal parenchymal
disease on dialysis may not respond well to TIPS
Do not with held diuretics after TIPS
New entry- poly tetra fluoro ethylene coated
Stent is better ,patency duration is
increased,greater survival;

Why?
Poor long term patency
Increased infections
No increased survival compared to medical therapy
Only in patients who are not candidates for TIPS/liver transplant/not fit for serial therapeutic paracentesis

1 retrospective study on efficacy of weekly
albumin infusion of 50 g in reducing weight in
patients with refractory ascites who are not
candidates for TIPS ….result awaited
Pilot Randomised control study -0.075 mg
oral clonidine bid vs placebo in patients with
cirrhosis ,with ascites and plasma nor
Epinephrine> 300 pg/ml--- more rapid
mobilisation of ascites with fewer
complications

3 pilot Randomised control studies
Paracentesis + albumin
Vs
Clondine + spironolactone
In patients with refractory ascites and
plasma nor epinephrine >300 pg/ml
Result – fewer hospitalisation in latter group
.


Device that drains ascitic fluid into urinary
bladder.
ALFA pump system (Automated low flow ascites
pump).
Flow : catheter in abdominal cavity
subcutaneously inserted battery powered
pump catheter connected to bladder.
Pump is recharged wirelessly through skin
Removes 5 L per charge.

Severe irritation in bladder
Recurrent urinary tract infections.
Pyelo nephritis
Not approved for practise.

Median survival period for refractory ascites
is 6 months
1 st best option is liver transplant
MELD score >18
Hyponatremia <130 mEq/l
LOW Mean arterial pressure
Low urine sodium <50 m eq/l
High child pughscore >11
All determine duration of survival

LVP is the 1 st line treatment
Diuretics must be discontinued if dyselectrolytemia/renal failure/hepatic encephalopathy occurs.Continue diuretics only when urine sodium >30 mMol/l
V2 receptor antagonists – satavaptan + fixed dose diuretics is under phase II trials
Improves Na levels,increases weight loss,decreases recurrence of ascites.
TIPS is recommended only if very frequent requirement of LVP/ineffective paracentesis(loculated)

Role of aquaretics
phase III clinical trials –satavaptan +
diuretics showed no further improvement in
control of ascites
Increased morbidity and mortality was also
observed
Recently Tolvaptan is approved for
management of refractory ascites..

Forty cirrhotic patients with refractory or
recurrent ascites were prospectively studied
after long term administration of midodrine
plus standard medical therapy (n = 20) or
standard medical therapy alone (n = 20) in a
randomized controlled trial at a tertiary
centre. Virendra singh etal …PGIMER

A significant increase in urinary volume,
urinary sodium excretion, mean arterial
pressure, and decrease in plasma renin
activity (p <0.05) was noted after 1 month of
midodrine administration.
There was also a significant decrease in
cardiac output and an increase in systemic
vascular resistance after midodrine therapy
at 3 months (p <0.05)

There was no change in glomerular filtration
rate and model for end-stage liver disease
(MELD) score.
Midodrine addition is superior to standard
medical therapy alone in the control of ascites
(p = 0.013) at 3 months. The mortality rate in
the standard medical therapy group was
significantly higher than the midodrine group
(p <0.046). There was no significant difference
in the frequency of various complications at
the end of follow-up.

ANNALS OF HEPATOLOGY ..Amarapurkar etal
Back ground- use of covered TIPS was shown
to improve the shunt patency rate over
uncovered TIPS.Retrospective analysis was
performed to assess efficacy of both
Methods-over 10 yr period,selected patients
who require LVP atleast 2 times in a
month,or intolrant to LVP,or unwilling to
undergo further LVP were treated with TIPS

12 PATIENTS 11 PATIENTS
Uncovered TIPS PTFE covered TIPS
Age 56.1+/_4.5 yrs 55.8+/_5.2 yrs
Male : female-5:1 male :female-8:3
Followed up with –clinical examination,USGabdomen,doppler examination ,every monthly for 3 months,and every 3 monthly thereafter.

Clinical success= disappearance of ascites in
1 month
Technical success =post TIPS reduction of
PPG (porto systemic pressure gradient) <12
mm Hg.
Appearance of encephalopathy
TIPS dysfunction= >50 %reduction in flow
velocity ,> 50 % shunt stenosis,or increase in
PPG> 12mm Hg

GROUP A GROUP B
CLINICAL SUCCESS 63.3% 81.8%
TECHNICAL SUCCESS 63.3% 81.8%
HEPATIC
NCEPHALOPATHY
60% 54.4%
MORTALITY AT 1 YR 70% 63.3%
TIPS DYSFUNCTION
REQUIRING RE
INTERVENTION 50% 0%

Harrisons text book of internal medicine 18th edition
Schiffs diseases of liver 11th edition.
Sherlock’s diseases of liver and biliary tract 12th edition
AASLD guide lines 2013
EASL guidelines of liver disease 2012
Indian journal of gastro enterology. .volume 33,isssue4 ,august 2014.
Clinical gastroenterology by Rajiv mehta 3rd
edition.

Thanks to
• Dr.RAVI .K professor of medicine
• Dr.SUSHRUTH Surgical gastro
enterologist. PMSSY