
Refractory Ascites: TIPS vs non-TIPS ascites • Definition- complication of portal hypertension;...
28
Refractory Refractory Ascites Ascites : TIPS : TIPS vs vs non non - - TIPS TIPS Jayer Jayer Chung, MD Chung, MD Department of Surgery Department of Surgery University of Colorado Health Sciences Center University of Colorado Health Sciences Center
Transcript of Refractory Ascites: TIPS vs non-TIPS ascites • Definition- complication of portal hypertension;...

Refractory Refractory AscitesAscites: TIPS : TIPS vsvs nonnon--TIPSTIPS
JayerJayer Chung, MDChung, MDDepartment of SurgeryDepartment of Surgery
University of Colorado Health Sciences CenterUniversity of Colorado Health Sciences Center
• Definition and epidemiology of refractory ascites(RA)
• Pathophysiology of ascites• Description of the treatments for RA• Why are other therapies better than TIPS?
– Transplant– TIPS vs LVP- encephalopathy, QOL, cost, frequent
occlusions– TIPS vs peritoneovenous shunts
• Conclusion
OverviewOverview
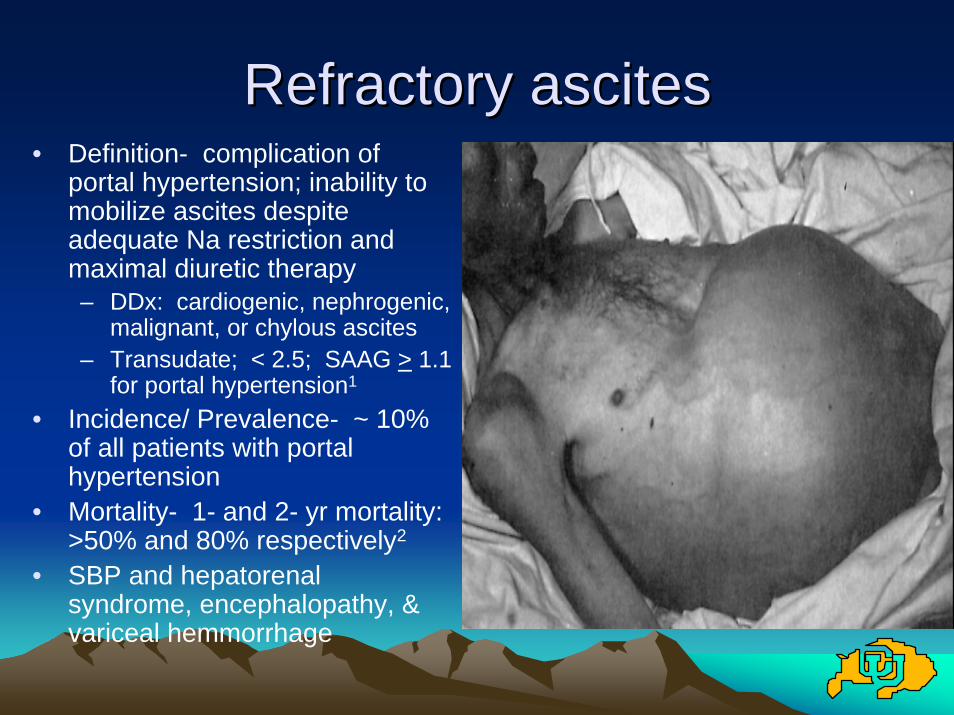
Refractory Refractory ascitesascites• Definition- complication of
portal hypertension; inability to mobilize ascites despite adequate Na restriction and maximal diuretic therapy– DDx: cardiogenic, nephrogenic,
malignant, or chylous ascites– Transudate; < 2.5; SAAG > 1.1
for portal hypertension1
• Incidence/ Prevalence- ~ 10% of all patients with portal hypertension
• Mortality- 1- and 2- yr mortality: >50% and 80% respectively2
• SBP and hepatorenalsyndrome, encephalopathy, & variceal hemmorrhage
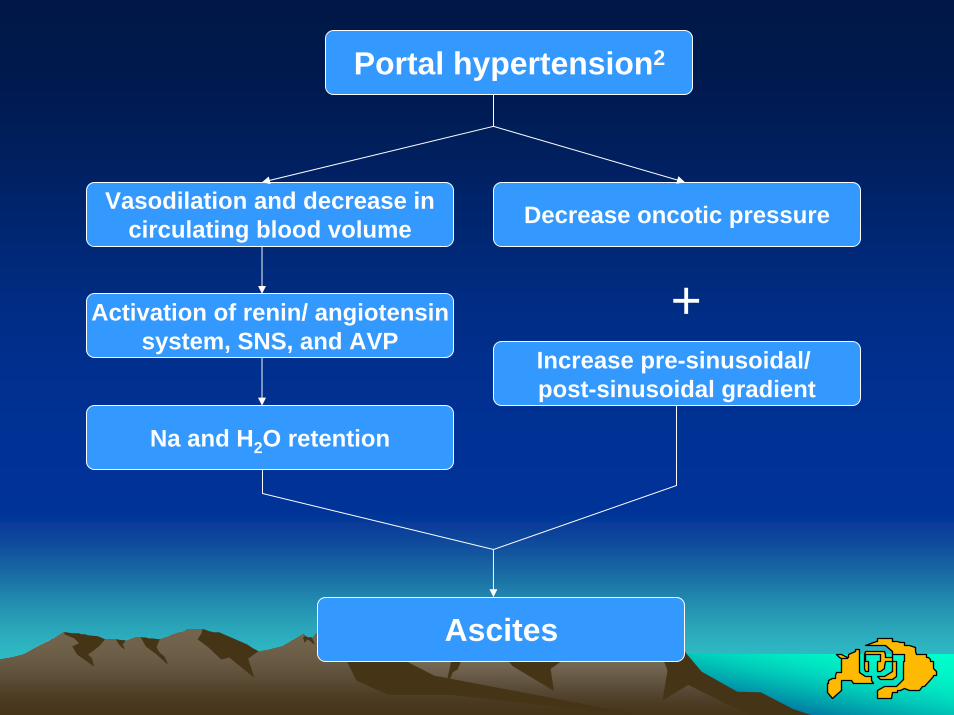
Portal hypertension2
Vasodilation and decrease incirculating blood volume
Activation of renin/ angiotensinsystem, SNS, and AVP
Na and H2O retention
Decrease oncotic pressure
Increase pre-sinusoidal/ post-sinusoidal gradient
+
Ascites
TreatmentsTreatments• Transplant• Transjugular Intrahepatic Portosystemic
Shunt (TIPS)• Large Volume Paracentesis (LVP; >5L)• Peritoneovenous shunt (LaVeen, and
Denver)• Open portosystemic shunts
Large Volume Large Volume ParacentesisParacentesis (LVP)(LVP)22
• Indications– Tense ascites
• Complications– Repeated complement and protein depletion,
SBP, hypotension– Colloid replacement (albumin) if > 5L removed

TransplantTransplant44
• Indications- Acute or chronic liver failure of any cause (Child’s > 7, MELD > 10)
• Contraindications– Morbid obesity, active extrahepatic malignancy, active
sepsis, HIV, non-compliance, cholangiocarcinoma, HCC > 6cm

3
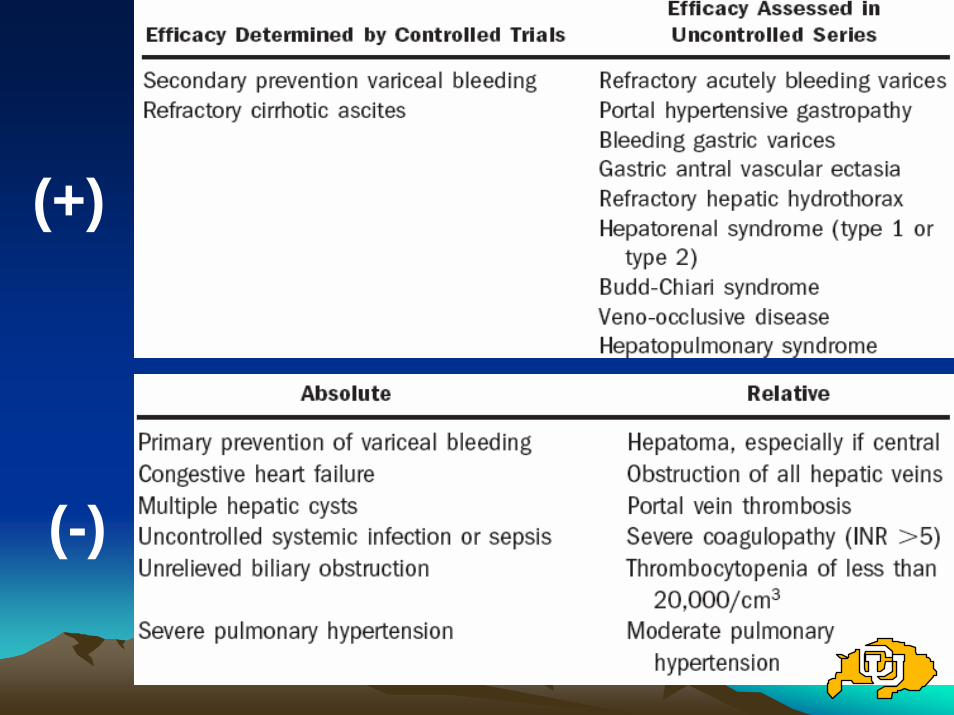
(+)
(-)
4
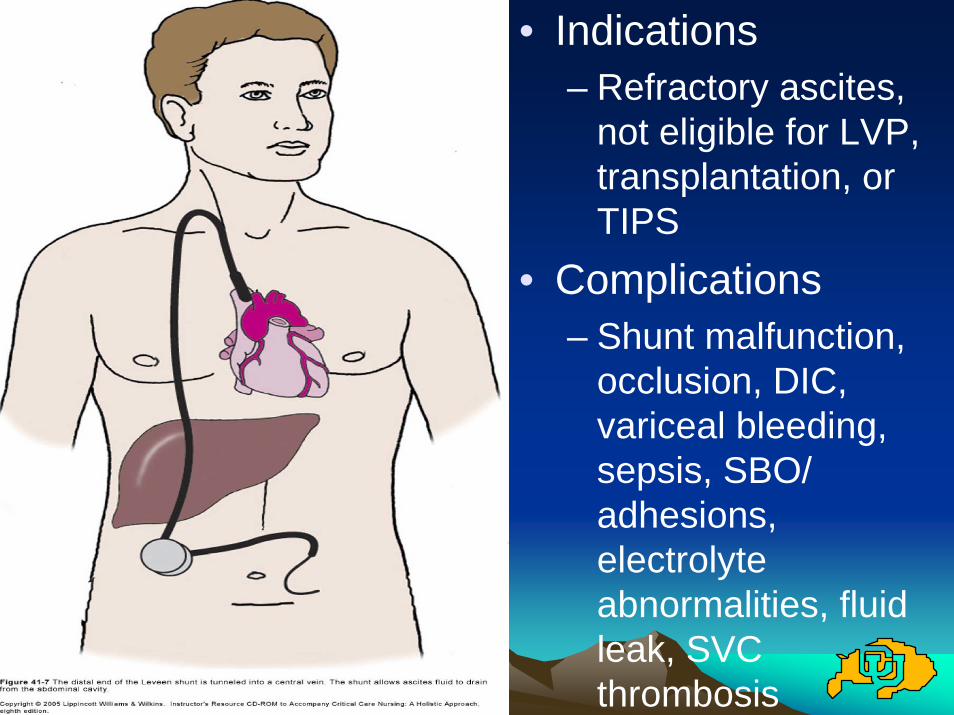
• Indications– Refractory ascites,
not eligible for LVP, transplantation, or TIPS
• Complications– Shunt malfunction,
occlusion, DIC, variceal bleeding, sepsis, SBO/ adhesions, electrolyte abnormalities, fluid leak, SVC thrombosis
Transplant is #1 therapy for RATransplant is #1 therapy for RA
• Gold standard- 1-, 5-, 10-yr survival of 81%, 72% and 68% respectively5
• Only curative therapy for refractory ascites• Improve health-related quality of life6
• Only problem is organ shortage– 1991-1999: Candidacy by 8x, organs only by
2x3
– 17,269 candidates on wait list, and only 5,906 donors for 20057
Why is TIPS the same or worse Why is TIPS the same or worse than LVP?than LVP?
• No overall change in survival vs LVP• Complications- frequent stenoses/
occlusions, hepatic encephalopathy• QOL• Cost

Authors N
Lebrec9 25
Rossle10 60
Gines11 70
Sanyal12 109
Salerno13 66Lower with paracentesisLower with TIPS
10.5 2 3
8
No survival benefit No survival benefit vsvs LVPLVP
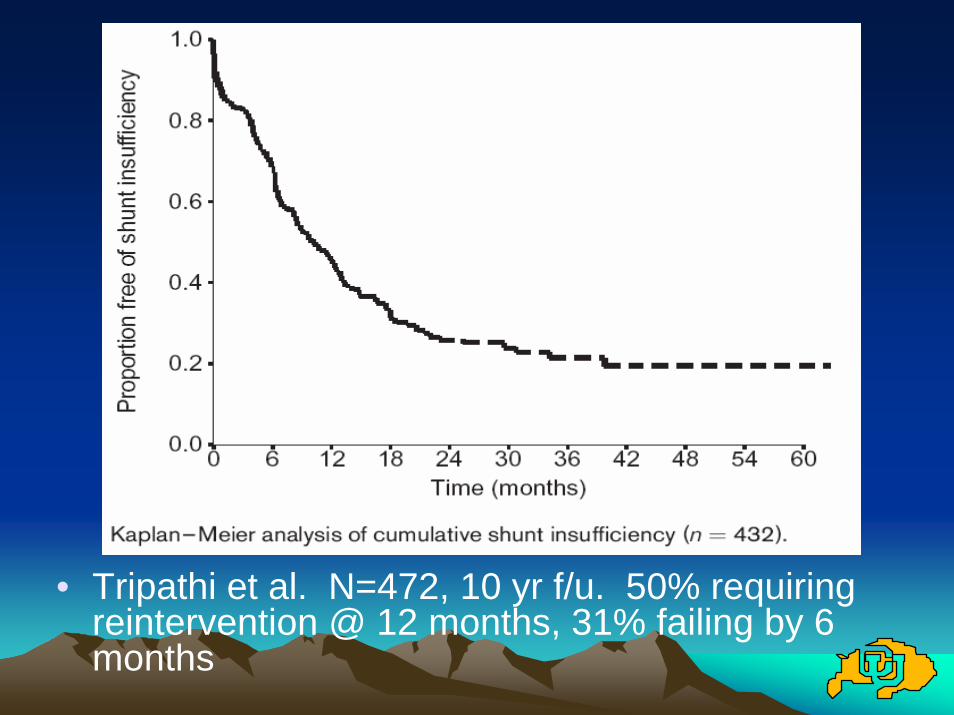
• Tripathi et al. N=472, 10 yr f/u. 50% requiring reintervention @ 12 months, 31% failing by 6 months
9
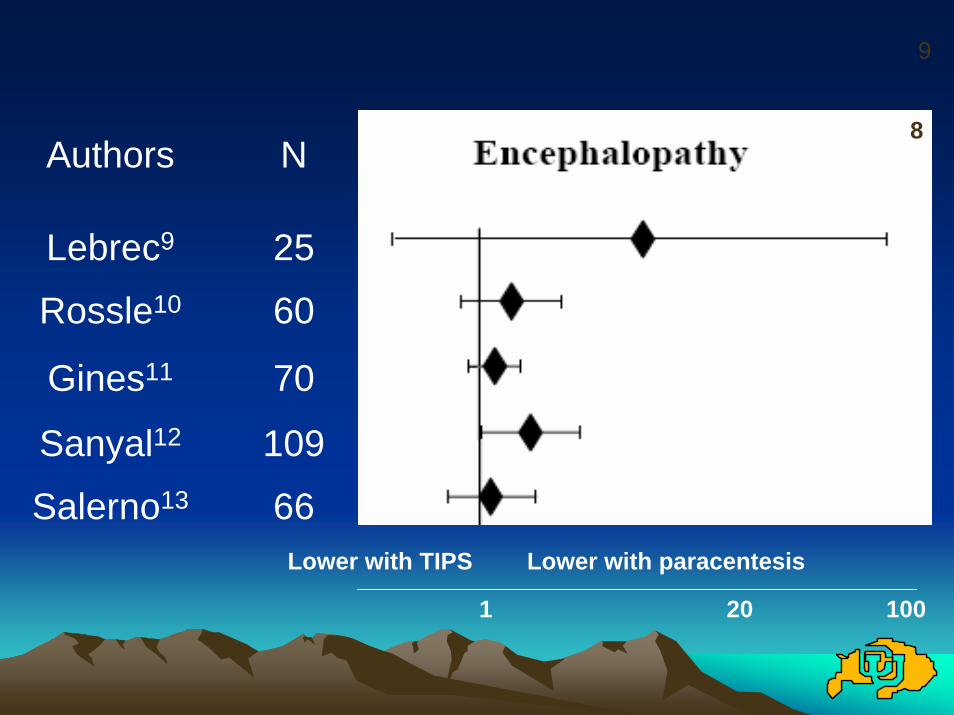
Authors N
Lebrec9 25
Rossle10 60
Gines11 70
Sanyal12 109
Salerno13 66Lower with paracentesisLower with TIPS
8
1 20 100
QOLQOL
• Campbell MS et al. 109 pts (52/57), PRCT, 1 yr f/u15
– 21 pts (57%) in TIPS arm vs 8 pts (24%) in LVP arm required re-hospitalization (p=0.006)
– SF-36 questionnaire showed no change, largely due to the increase in encephalopathy in the TIPS arm (49% vs 21% @ 6 months)
Due to the increased frequency of hospitalizations (secondary to further interventional procedures) and increased frequency of encephalopathy, there is no overall improvement in QOL despite improvements in ascites control.
CostCost1111
• Gines 2002- PRCT, N=70 (35/35)• TIPS 103% more expensive than repeated
LVP ($19,813 vs $9,765)• Analysis of the cost of procedures only;
hence, this analysis likely underestimates the cost of TIPS vs LVP
TIPS TIPS vsvs PeritoneovenousPeritoneovenous shuntsshunts
• Rosemurgy 2004. N=32(16/16), PRCT, 3 yr f/u16 Denver shunts only– Mortality
• 28.7 months vs 16.1 months median survival– Ascites
• 54% control vs 80% control @ 1 month• 80% control vs 54% control @ 1 yr
– Patency• Median primary patency of 4.4 months vs 4 months, though
assisted patency of 31.1 months vs 13.1 months
Short term results comparable, though TIPS better long-term
ConclusionsConclusions
• Transplant the gold standard, but organ shortage
• Short term results of TIPS and peritoneovenousshunts comparable
• TIPS only superior to LVP with respect to removal of ascites– Similar or worse QOL
• Frequent hospitalizations and increased rates of encephalopathy
– No change in overall mortality– Much more expensive $$$$

ReferencesReferences1. Townsend CE, et al. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical
Practice. 17th edition, 2004.2. Zervos EE, et al. Management of medically refractory ascites. The American Journal of
Surgery. 2001; 181: 256-264.3. Trotter JF, et al. Adult-to-Adult Transplantation of the Right Hepatic Lobe from a Living Donor.
NEJM. 2002; 346(14): 1074-1082.4. Murray KF, et al. AASLD Practice Guidelines: Evaluation of the Patient for Liver
Transplantation. Hepatology. 2005; 41: 1-26.5. Boyer T, et al. AASLD Practice Guideline: The Role of Transjugular Intrahepatic Shunt in the
Management of Portal Hypertension. Hepatology. 2005; 41: 1-15.6. Orsi F, et al. Percutaneous Peritoneovenous Shunt Positioning: Technique and Preliminary
Results. Eur Radiol. 2002; 12: 188-1192.7. Busuttil RW, et al. Analysis of Long-term Outcomes of 3200 Liver Transplantations Over Two
Decades: A Single-Center Experience. Annals of Surgery. 2005; 241(6): 905-918.8. Sainz-Barriga M, et al. Quality-of-Life-Assessment Before and After Liver Transplantation.
Transplantation Proceedings. 2005; 37: 2601-2604.9. United Network for Organ Sharing (UNOS): Data Resources Page. Retrieved January 25,
2006 from the UNOS website: http://www.unos.org/data/data_resources.asp10. Abillos A, et al. A meta-analysis of transjugular intrahepatic portosystemic shunt versus
paracentesis for refractory ascites. Journal of Hepatology. 2005; 42: 990-996.11. Lebrec, D et al. Transjugular intrahepatic portosystemic shunts: comparison with
paracentesis in patients with cirrhosis and refractory ascites: a randomized trial. Journal of Hepatology. 1996; 25: 135-144.

10. Rossle M, et al. A Comparison of Paracentesis and Transjugular Intrahepatic PortosystemicShunting in Patients with Ascites. NEJM. 2005; 342(23): 1701-1707.
11. Gines P, et al. Transjugular Intrahepatic Portosystemic Shunting Versus Paracentesis Plus Albumin for Refractory Ascites in Cirrhosis. Gastroenterology. 2002; 123: 1839-1847.
12. Sanyal AJ, et al. The North American study for the Treatment of Refractory Ascites. Gastroenterology. 2003; 124: 634-641.
13. Salerno F, et al. Randomized Controlled Study of TIPS Versus Paracentesis Plus Albumin in Cirrhosis With Severe Ascites. Hepatology. 2004; 40: 629-635.
14. Tripathi D, et al. Ten Years’ follow-up of 472 patients following transjugular intrahepaticportosystemic stent-shunt insertion at a single centre. European Journal of Gastroenterology & Hepatology. 2004; 16: 9-18.
15. Campbell MS, et al. Quality of Life in Refractory Ascites: Transjugular Intrahepatic Portal-Systemic Shunting Versus Medical Therapy. Hepatology. 2005; 42: 635-640.
16. Rosemurgy A, et al. TIPS Versus Peritoneovenous Shunt in the Treatment of Medically Intractable Ascites: A Prospective Randomized Trial. Ann Surg. 2004; 239: 883-891.
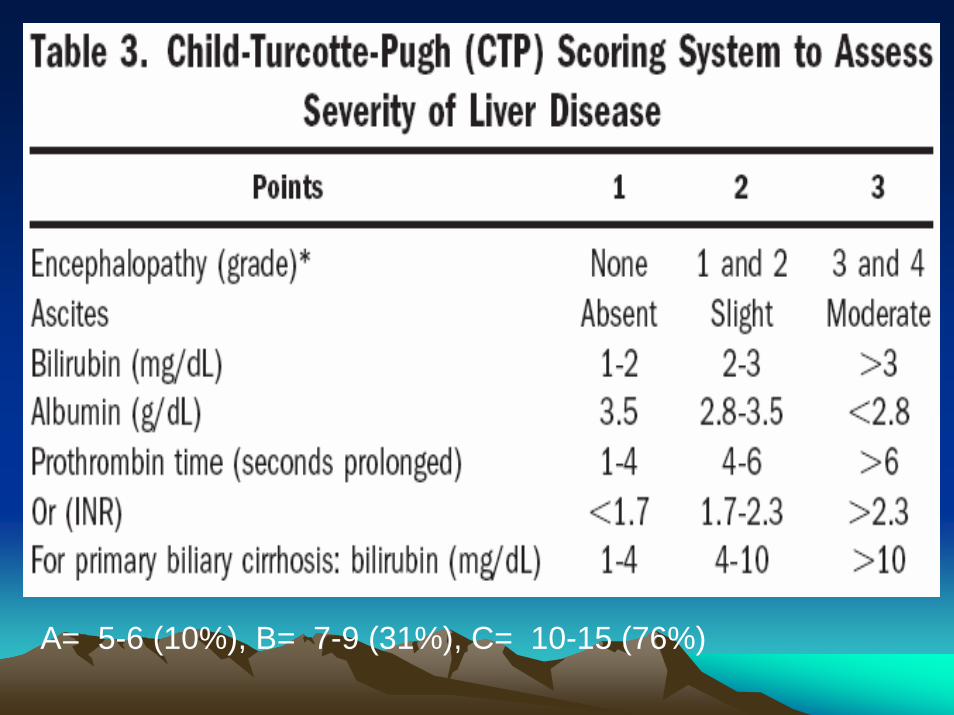
A= 5-6 (10%), B= 7-9 (31%), C= 10-15 (76%)

• Non-selective– Completely divert portal flow– End-side (Eck’s fistula) &side-side
portacaval, mesocaval, and mesorenal, H-graft (8mm PTFE), splenorenal shunt
• Selective– Distal spleno-renal (Warren)

• Odds Ratio- probability of disease among exposed subjects/ probability of disease in unexposed subjects (ad/bc)
• Hepatorenal syndrome– High M&M; avid Na retention, UNa<5mmol
• Hepatopulmonary syndrome– R to L intrapulmonary shunt through dilated
intrapulmonary vessels + ascites leads to hypoxia


















