Reflections on Retention or The World of Connectivity in HIV Ambulatory Care
41
Reflections on Retention or The World of Connectivity in HIV Ambulatory Care Bruce D. Agins, MD MPH Medical Director, NYSDOH AIDS Institute
description
Reflections on Retention or The World of Connectivity in HIV Ambulatory Care. Bruce D. Agins, MD MPH Medical Director, NYSDOH AIDS Institute. Overview of the Talk. Defining Retention Rationale for Focusing on Retention Measurement QI Strategies The Next Frontier: Revisiting Taxonomy. - PowerPoint PPT Presentation
Transcript of Reflections on Retention or The World of Connectivity in HIV Ambulatory Care

Reflections on Retention or The World of Connectivity in
HIV Ambulatory Care
Bruce D. Agins, MD MPHMedical Director, NYSDOH AIDS Institute

Overview of the Talk
• Defining Retention
• Rationale for Focusing on Retention
• Measurement
• QI Strategies
• The Next Frontier: Revisiting Taxonomy

Defining Retention
• The act of keeping or holding in one’s possession
• To keep in a particular place, condition or position

Why is Retention Important?
• Medical care:
– The heart of the patient-doctor
relationship:
• The patient identifies the doctor (clinic) as
his or her provider
• The doctor identifies the individual as his or
her patient

Why is Retention Important?
• The Primary Care Model– Access– Coordination– Continuity – Comprehensiveness– Quality
• Perfectly suited to system-level interventions and quality improvement

Why is Retention Important?
• Revenue
– If patient’s keep coming to clinic, more
bills can be generated in the fee-for-
service system.

Why is Retention Important?
• Healthcare Costs
– If patients are retained in care, they are
more likely to receive preventive care,
use emergency services less and keep
overall healthcare costs lower.

Why is Retention Important?
• Public Health
– Keeping patients retained in healthcare
achieves the overall goal of keeping the
population healthy, increasing the
likelihood of preventing chronic disease
and reducing morbidity and premature
mortality.

Why is Retention Important for People Living with HIV?
• Hypothesis: – Retention in care promotes improved
adherence to treatment which results in lower viral loads, prevention of drug-resistance and improved health outcomes.
• Is there evidence to support the hypothesis?

Why is Retention Important for People Living with HIV?
• The Evidence Base:– Rastegar, AIDS Care 2003: Missed appointments associated with
detectable viral load. Chart review 1997-99.
– Lucas, Ann Intern Med 1999: Missed appointments associated with failure of suppression. JHU. 1996-8.
– Valdez, Arch Intern Med 1999: Missing <2 appts per year associated with virologic success defined as <400 copies.
– Sethi, Clin Infect Dis 2003: Missed appointments associated with viral rebound and clinically significant resistance at JHU 2000-1.
– Nemes, AIDS 2004: Missing 2 appointments associated with decreased adherence among >1900 patients in Brasil.

Why is Retention Important for People Living with HIV?
• The Evidence Base:
– We still don’t know
which comes first:
• Viral load elevation
or
• The missed
appointment

Measurement
• What is the extent of the problem?
– No-shows
– Retention rates
– Sources of data
– Unmet need
• But, why??

No-Show Rates: aka “DNKA”
• No-show rates range from 25% to >40% in published studies
• Limitations: – Patients may be counted for multiple visits– Type of clinic visit not uniform – Time frame accepted for prior cancellation– Rescheduling: does it count?– What about walk-ins and open access?

Retention Rates
• Require precise definitions of expected number of
visits during a specified time interval
• Eligible population required for the denominator
which requires determination of visit type and
determination of active caseload of the clinic

Retention Rates
• Examples:# of unique clients with at least 1 visit in past 4 months# of unique clients with at least one visit in past 12 months
# pts with at least 1 visit during 3 month interval after 12 month period
# pts with 3 or more visits in the 12 mo. period (*1 in last 6 months)
# pts with 2+ visits during the defined 12-month period# pts in the clinic registry during the defined period
# pts with no visit during the past 4 months# pts with at least 1 visit during past 12 mos

Current NYS Retention Measure
• Number of unique clients with at least 2 or more visits during the past 12 months, one in each 6-month period
Number of unique clients with at least 1 visit during the past 12 months

Data Sources• In the Clinic
– Administrative databases in clinic
– Medical record review required to ascertain
reasons for not keeping appointments – may
include case management notes

Unmet Need
• During a 12-month interval, the
number of patients who have had
either a viral load or CD4 count
measured or who have been
prescribed antiretroviral therapy

Why Don’t Patients Come?
• Which patients are more likely to miss their appointments*:– Patients from minority communities, especially African-Americans– Younger age– Heterosexual – Education level lower than high school – Lack of health insurance– Lower income– Higher CD4 count– No AIDS diagnosis– History of IDU or current IDU– Lower perceived social support– Shorter follow-up since baseline– Less engagement with health care provider
*Numerous studies; bibliography available upon request

Why Don’t Patients Come?
• HIV Literature:– Norris abstract 1990: conflict with work, no child care, no
transportation, family illness– Palacio J Acquir Immune Defic Syndr 1999: among
women: forgetting, conflicts, too sick.
• Non-HIV Literature:– Multiple sources: forgetting, feeling too ill, symptom
resolution.– Lacy, Ann Fam Med 2004: negative emotions about
seeing doctor; perceived disrespect of beliefs and time; distrust; lack of understanding about the scheduling system.
• Patient Satisfaction Surveys

Why Don’t Patients Come?
• One-Visit Study – Queens Hospital Center*– Exclude those who moved, transferred or died– 15 patients not “retained”:
• Unable to contact 7• Contacted 8:
– 2 reported active substance abuse, 1 returned to care– 1 fear of recognition, referred to other HIV clinic– 1 psychiatric history, attends multiple HIV clinics– 1 looking for a job, returned to care– 1 refused outpatient treatment despite extensive
outreach efforts (frequent QHC hospitalizations)– 2 feeling well, are early in HIV and refused frequent
medical visits
Jazila Mantis, MD, Jean Fleischman, MD, Kathleen Aratoon, NP, Maria Szczupak,
RPh, Diana Jefferson, RN, Terri Davis, MSW, Maria Bucellato

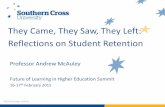
Percentage of Visits that were Missed because the Client failed to keep scheduled appointment with provider or social worker
(N=1500) < 25% > 25%
Clinical Outcomes
Using HAART 78% 64%*
Viral Load suppressed (< 400 copies/ml)
65% 31%*
Change in CD4 from Baseline
+68 cells/mm3 -36 cells/mm3*
Health Resource Utilization
Hospital Admissions per year(mean)
2.2 days 3.2 days*
ED visits per year (mean) 3.2 6.8*
*All comparisons are significant with p <0.01 Johns Hopkins AIDS Service Data Base 1999-2004
Clinical Outcomes and Health Resource Utilization Stratified by Percentage of Missed Visits

Improving Retention
• QI is perfectly suited to improve retention in the clinic
• Improvement strategies– Clinic operation & information systems– Consumer involvement to identify barriers &
solutions– Increasing staff & patient awareness– Focused case management (internal & external)

Clinic Operation and Information System Strategies
Clinic Organization
• Ensure coverage for provider vacations and time-off to avoid canceling or re-
scheduling appointments
• Establish patient database to track adherence with appointments
Pre-Appointment
• Reminder cards with date/time/location of visit mailed to patients
• Reminder calls made 48 hrs prior to appointment to allow patient time to
make arrangements, if needed
• Reminder calls to patients made by providers, case managers or other staff
closely involved w/ patient's care
• Schedule labs to be done prior to visits to maximize time spent w/ provider

Consumer Involvement
• Convene focus group of established patients to provide
feedback on retaining new patients
• Survey patients who have missed appointments to identify
common reasons and barriers
• Routinely share results of patient satisfaction surveys w/
Consumer Advisory groups to elicit feedback
• Survey new patients immediately following initial visit for
satisfaction w/ services
• Develop patient satisfaction surveys targeted to patient
groups w/ different levels of experience - patients w/ less
than 3 visits, patients w/ more than three clinic visits, etc.

Increasing Patient and Staff Awareness
• Conduct new patient orientation sessions and
include discussion of staying in care
• Schedule one-to-one sessions for new patients
unable to attend group orientations
• Develop written patient materials on the
importance of staying in care
• Staff education - routinely discuss patient
retention w/ all staff

Focused Case Management Strategies: Internal (facility) and External (community)
• Create “patient profile” sheet to summarize patient’s
appointment history
• Medical records of patients who missed appointments given to
providers at end of session-provider determines priority for follow-
up
• Multidisciplinary case conferencing includes plans for retaining
individual patients in care
• Develop categories of patients requiring more intensive follow-up
and develop specific protocols for each group
• Refer patients w/ two consecutive broken appointments to case
manager

Focused Case Management Strategies: Internal (facility) and External (community)
• Assess new patients for adherence barriers and make early,
proactive referrals to services
• Community liaison workers utilized to re-engage patients
lost to care

Improvement Processes
• “One of the best strategies leading to
success has been strong clinical and
administrative leadership in the
retention initiative.”

Improvements: Current Status
• Patient Factors
– May or may not be amenable to change
– Supportive services may be beneficial
– Outreach programs effective but expensive
• System Factors
– Amenable to change
– Do changes result in improvement?
– QI methods well-suited to improving retention and testing strategies

Setting Policy
• When can we stop making calls?
• How much effort should we make to
physically locate patients, especially when
contact information is incorrect?
• What are the legal responsibilities involved?
• Should certain patients be sought more
aggressively than others?

Looking Beyond the Clinic
• Patients may seek care from multiple
providers in different locations.
• Is a patient who receives care from
another provider “retained”?
• How should we define quality of care in
the context of retention when a patient
receives care outside of the clinic?

Why is Retention Important?
• Public Health
– Keeping patients retained in healthcare
achieves the overall goal of keeping the
population healthy, increasing the
likelihood of preventing chronic disease
and reducing morbidity and premature
mortality.

ContinuumEngagement in Care
Unaware of HIV Status (not tested or never received results)
Know HIV Status (not referred to care; didn’t keep referral)
May Be Receiving Other Medical Care But Not HIV Care
Entered HIV Primary Medical Care But Dropped Out (lost to follow-up)
In and Out of HIV Care or Infrequent User
Fully Engaged in HIV Primary Medical Care
Not inCare
Fully Engaged

A New Taxonomy
• Retention• Engagement?
-the act of obtaining and holding the attention of; engrossing
-the act of pleasing or attracting; winning
-the act of entangling, involving

A New Taxonomy
• Connection
– the act of joining;
union
– an association,
alliance, or relation
– anything that joins,
relates, or connects;
a bond; a link

Connecting to Care: 17 Strategies
• Adherence and self-management
• Inter-agency networking
• Support retreat: peer to peer
education
• Teen peer outreach: peer
education
• Primary care liaison
• Zip code mapping: targeting
activities
• Snapshot viral load testing
• Deployed case management
• Heartline hotline
• Aftercare plan
• Support groups
• Early intervention nurse
• Woman to woman support
• Financial advocacy
• Clinicians reaching out
• Intake housing coordinator-
– Linkage to care
• HIV care coordinator

Continuity of Care• The state or quality of being unceasing,
extending or prolonged without interruption [American Heritage Dictionary]
• An uninterrupted succession, unbroken course
• The extent to which services are coordinated an uninterrupted succession of events concordant with the patient’s clinical requirements. [Roos 1980; Shortell 1975]
• Both the provider and patient expect an enduring relationship. [Carmichael 1976]

Continuity of Care
• “Continuity of care may be provided by the same provider, the same care team or practitioners within the same group, or providers linked by referral.”
» Adapted from Hidalgo: “Measuring Continuity of Care in HIV Special Needs Plans”. NYSDOH AIDS Institute. 1998.

Current Retention Activities
• In New York State Focus of improvement projects for several Quality
Learning Networks, including HHC and substance use providers
NYS Quality of Care Advisory Committee retention workgroup - addressing retention statewide
Internal AIDS Institute Continuity of Care workgroup
Ongoing review of journals and other publications

Acknowledgments
• Elizabeth Horstmann• The HHC HIV Quality Learning
Network