Reference values of capillary blood volume and pulmonary membrane diffusing capacity in North...
11
ORIGINAL ARTICLE Reference values of capillary blood volume and pulmonary membrane diffusing capacity in North African boys aged 8 to 16 years Sonia Rouatbi a, * , Mehdi Khemis a , AbdelHamid Garrouch b , Helmi Ben Saad a a Laboratory of Physiology and Explorations, Faculty of Medicine Ibn El Jazzar, Sousse, Tunisia b Service of Pneumology, Farhat Hached Hospital, Sousse, Tunisia Received 6 February 2014; accepted 17 February 2014 KEYWORDS Reference values; Capillary blood volume; Pulmonary membrane dif- fusing capacity; Children Abstract Lung diffusing capacity estimated using nitric oxide (NO) as the tracer gas has been proposed as a direct measure of the pulmonary membrane diffusing capacity for NO (Dm) and the pulmonary capillary blood volume (Vc). Thus, the aims of this study were to identify the factors influencing Vc and Dm and to establish linear regression equations for predicting reference values for Vc and Dm in healthy Tunisian boys aged 8 to 16 years. Methods: It is a cross-sectional analytical study. The sample is formed of healthy Tunisian children aged 8 to 16 years. First, subjects responded to a questionnaire. Anthropometric and spirometric data were collected. DLNO and DLCO were measured and Dm and Vc were calculated simultaneously during a single breath maneuver using the double transfer technique for NO/CO. Statistical analyses were carried out using Statistica (Statistica Kernel version 6, StatSoft, 26 France). Significance was set at the 0.05 level. Abbreviations: ATS, American Thoracic Society; BMI, body mass index; BSA, body surface area; BTPS, body temperature and pressure saturated; CO, carbon monoxide; DL, lung diffusing capacity; DLCO, lung diffusing capacity for carbon monoxide; DLNO, lung diffusing capacity for nitric oxide; Dm, pulmonary membrane diffusing capacity; DmCO, pulmonary membrane diffusing capacity for CO; DmNO, pulmonary membrane diffusing capacity for nitric oxide; ERS, European Respiratory Society; FEV 1 , forced expiratory volume at the first second; FIO 2 , fraction of inspired oxygen; FVC, forced vital capacity; GAP, Global Academic Programs; Hb, hemoglobin; He, helium; IC, confidence limits; ISSAC, International Study of Asthma and Allergies in Childhood; KCO, DLCO/VA; LLN, lower limit of normal; MMEF, maximum mid expiratory flow; N 2 , nitrogen; NO, nitric oxide; NO 2 , nitrogen dioxide; O 2 , oxygen; PIO 2 , the inspiratory pressure of oxygen; ppm, parts per million; RSD, residual standard deviation; RV, residual volume; SD, standard deviation; SEL, socioeconomic level; ULN, the upper limit of normal; VA, alveolar volume; Vc, pulmonary capillary blood volume * Corresponding author. Tel.: +216 73 222 600; fax: +216 73 224 899. E-mail addresses: [email protected], [email protected] (S. Rouatbi), [email protected] (M. Khemis), abdelhamid.garrouch@ rns.tn (A. Garrouch), [email protected] (H. Ben Saad). Peer review under responsibility of The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier Egyptian Journal of Chest Diseases and Tuberculosis (2014) xxx, xxx–xxx The Egyptian Society of Chest Diseases and Tuberculosis Egyptian Journal of Chest Diseases and Tuberculosis www.elsevier.com/locate/ejcdt www.sciencedirect.com 0422-7638 ª 2014 The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.ejcdt.2014.02.007 Please cite this article in press as: S. Rouatbi et al., Reference values of capillary blood volume and pulmonary membrane diffusing capacity in North African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (2014), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007
Transcript of Reference values of capillary blood volume and pulmonary membrane diffusing capacity in North...

Egyptian Journal of Chest Diseases and Tuberculosis (2014) xxx, xxx–xxx
The Egyptian Society of Chest Diseases and Tuberculosis
Egyptian Journal of Chest Diseases and Tuberculosis
www.elsevier.com/locate/ejcdtwww.sciencedirect.com
ORIGINAL ARTICLE
Reference values of capillary blood volume
and pulmonary membrane diffusing capacity
in North African boys aged 8 to 16 years
Sonia Rouatbia,*, Mehdi Khemis
a, AbdelHamid Garrouch
b, Helmi Ben Saad
a
a Laboratory of Physiology and Explorations, Faculty of Medicine Ibn El Jazzar, Sousse, Tunisiab Service of Pneumology, Farhat Hached Hospital, Sousse, Tunisia
Received 6 February 2014; accepted 17 February 2014
A
C
ox
di
in
In
flo
re
vo*
E-
rn
Pe
04
ht
PN
KEYWORDS
Reference values;
Capillary blood volume;
Pulmonary membrane dif-
fusing capacity;
Children
bbreviations: ATS, American
O, carbon monoxide; DL, lun
ide; Dm, pulmonary membr
ffusing capacity for nitric ox
spired oxygen; FVC, forced
ternational Study of Asthma
w; N2, nitrogen; NO, nitric o
sidual standard deviation; RV
lume; Vc, pulmonary capillaCorresponding author. Tel.:
mail addresses: Sonia.rouatb
s.tn (A. Garrouch), helmi.be
er review under responsibilit
Production an
22-7638 ª 2014 The Egyptia
tp://dx.doi.org/10.1016/j.ejcd
lease cite this article in pressorth African boys aged 8 to
Thoracic
g diffusin
ane diffu
ide; ERS
vital cap
and All
xide; NO
, residua
ry blood+216 73
nsaad@r
y of The
d hostin
n Society
t.2014.02
as: S. Ro16 years,
Abstract Lung diffusing capacity estimated using nitric oxide (NO) as the tracer gas has been
proposed as a direct measure of the pulmonary membrane diffusing capacity for NO (Dm) and
the pulmonary capillary blood volume (Vc). Thus, the aims of this study were to identify the factors
influencing Vc and Dm and to establish linear regression equations for predicting reference values
for Vc and Dm in healthy Tunisian boys aged 8 to 16 years.
Methods: It is a cross-sectional analytical study. The sample is formed of healthy Tunisian
children aged 8 to 16 years. First, subjects responded to a questionnaire. Anthropometric and
spirometric data were collected. DLNO and DLCO were measured and Dm and Vc were calculated
simultaneously during a single breath maneuver using the double transfer technique for NO/CO.
Statistical analyses were carried out using Statistica (Statistica Kernel version 6, StatSoft, 26
France). Significance was set at the 0.05 level.
Society; BMI, body mass index; BSA, body surface area; BTPS, body temperature and pressure saturated;
g capacity; DLCO, lung diffusing capacity for carbon monoxide; DLNO, lung diffusing capacity for nitric
sing capacity; DmCO, pulmonary membrane diffusing capacity for CO; DmNO, pulmonary membrane
, European Respiratory Society; FEV1, forced expiratory volume at the first second; FIO2, fraction of
acity; GAP, Global Academic Programs; Hb, hemoglobin; He, helium; IC, confidence limits; ISSAC,
ergies in Childhood; KCO, DLCO/VA; LLN, lower limit of normal; MMEF, maximum mid expiratory
2, nitrogen dioxide; O2, oxygen; PIO2, the inspiratory pressure of oxygen; ppm, parts per million; RSD,
l volume; SD, standard deviation; SEL, socioeconomic level; ULN, the upper limit of normal; VA, alveolar
volume222 600; fax: +216 73 224 899.
, [email protected] (S. Rouatbi), [email protected] (M. Khemis), abdelhamid.garrouch@
ns.tn (H. Ben Saad).
Egyptian Society of Chest Diseases and Tuberculosis.
g by Elsevier
of Chest Diseases and Tuberculosis. Production and hosting by Elsevier B.V. All rights reserved.
.007
uatbi et al., Reference values of capillary blood volume and pulmonary membrane diffusing capacity inEgypt. J. Chest Dis. Tuberc. (2014), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

2 S. Rouatbi et al.
Please cite this article in press as: S. RoNorth African boys aged 8 to 16 years
Results: Eighty five boys were included to establish Vc and Dm reference values. Correlations
between the Vc or Dm of the 85 healthy boys and anthropometric data showed that only BMI
was not significantly correlated with Dm. The proposed Vc reference equation is: Vc (ml) =
11.3859 · age + 3.4613 · BMI � 117.0508. This model explains 45.7% of Vc variability. The
proposed Dm reference equation is as follows: Dm (ml/min/mmHg) = 0.6430 · height � 41.5854.
This model explains only 16.31% of Dm variability.
Conclusion: We have established a reliable and an available reference equation to interpret the
results of Dm and Vc in healthy North African boys aged 8 to 16 years.
ª 2014 The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier
B.V. All rights reserved.
Introduction
The measurement of gas transfer in the lung is one of the fewtests aimed at investigating deep lung function. According to
the classic model of pulmonary diffusion proposed by Rough-ton andForster [1] lung diffusing capacity (DL) for carbonmon-oxide (DLCO) is composed of two resistances arranged in series:
1=DLCO ¼ ð1=DmÞ þ ð1=HCO�VcÞ ð1Þ
where pulmonary membrane diffusing capacity (Dm) for CO(DmCO) is the CO conductance across the alveolar-capillarytissue membrane and plasma barrier; HCO is the rate of CO
uptaken by the whole blood and combination with hemoglobin(Hb) measured in vitro, and Vc is the pulmonary capillaryblood volume. In normal subjects, resistance of the membrane(1/DmCO) and erythrocytes [1/(HCO*Vc)] contribute almost
equally to the overall diffusive resistance across the lung.Lung diffusing capacity estimated using nitric oxide (NO) as
the tracer gas (DLNO) has been proposed as a direct measure
of the conductance of alveolar membrane (pulmonary mem-brane diffusing capacity for NO [Dm]) [2]. Because the reactionrate of NO binding to Hb is some 280 times faster than that of
CO [3], the rate of NO uptaken by blood (HNO) is extremelylarge and 1/(HNO*Vc) becomes negligible, i.e. DLNO isapproximately equal to Dm [2,3]. So the nitric oxide diffusingcapacity (DLNO) reflects the properties of the alveolo-capillary
membrane better than the DLCO [2]. Therefore DLNO can bedefined as the true alveolo-capillary membrane diffusing capac-ity [3]. This non-invasive technique, easy to perform and repeat,
could be of value in the diagnosis of many diseases. Howeverthe DLNO has been investigated by a small group of research-ers, and is still not implemented in clinical routine.
Several childhood diseases can be explained (pathophysiol-ogy) and explored by the measure of diffusing capacity, Vc andDmNO, for example: Cystic fibrosis [4], childhood systemic
diseases such as systemic lupus erythematosus [5], b-thalasse-mia [6] and childhood cancer [7]. These parameters can accu-rately locate the place of the anomaly: pulmonary capillaryor alveolar membrane. This non-invasive technique may be
useful in diagnosis, and during the follow-up of the diseaseas an early indicator of reactivation. Indeed, several childhooddiseases are accompanied by a change in Vc and/or Dm and
interpretation of these changes requires the knowledge of theirnormal values. In other words, we must have some ideas ofphysiological variations and reference values of these parame-
ters in order to properly interpret pathological changes.Regarding children, to our knowledge, no studies have beenmade to determine the predicted values for lung diffusing
capacity in healthy children.
uatbi et al., Reference values of ca, Egypt. J. Chest Dis. Tuberc. (20
Thus, we propose to study, for the first time, lung capillaryblood volume and alveolar membrane diffusing capacity, usingthe NO–CO method, in healthy North African boys. The aims
of this study are to: (1) identify the factors influencing Vc andDmNO in healthy North African boys aged 8 to 16 years. (2)Establish linear regression equations for predicting referencevalues for Vc and Dm in healthy North African boys aged 8
to 16 years.
Material and methods
Study design
This is a cross-sectional analytical study spread over eightmonths. It was conducted in the Department of Physiologyand Functional Explorations in the Public Health Institution,
Farhat HACHED Sousse (Tunisia) (altitude <100 m). Studydesign consists of a sample of healthy Tunisian children inthe region of Sousse, aged 8 to 16 years. Subjects were recruited
from the children of the hospital workers, and from public andprivate schools. Information letters, clarifying the aims of thestudy, were put up in the Medicine Faculty and in differentschools. When a subject was interesting, an appointment for
distributing a medical questionnaire and exploration was fixed.Data from each volunteer child included: gender, age, height,weight, birth height and weight, smoking history (child or par-
ents), medication use, medical history, physical examinationand pulmonary capillary blood volume data. All children re-ceived a copy of their exploration and when an unknown dys-
function was discovered, they were sent to a specialist. Studyapproval was obtained from the Ethics committee of the FarhatHached Public Institution of Health and written informed con-
sent was obtained from all children and their parents.
Sample size
A large number of subjects (i.e., n > 100) are needed to ensure
no significant difference between the published referenceequations and those from the local community [8]. Therefore,to determine the influencing factors and establish a reference
equation or normal values, we recruited an initial group of172 children.
Subjects
Volunteer healthy children aged from 8 to 16 years were in-cluded. The following non-inclusion criteria were applied:
chronic illnesses; history of pulmonary diseases or related
pillary blood volume and pulmonary membrane diffusing capacity in14), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

Capillary blood volume and pulmonary membrane diffusing capacity norms in North African boys 3
respiratory symptoms (history of asthma or medication asth-ma use, current or past symptoms of wheeze, chronic cough);abnormal lung function [8]; oto-rhino-laryngological diseases
or symptoms (allergic rhinitis); recent airway infection (cold,flu, and sore throat within the last 7 days); atopic dermatitisor eczema; regular medication use (especially steroids or
b-agonist, leukotriene receptor agonist. . .); heart disease;premature birth (i.e., birth before 36 weeks gestational age);active smoking; and imperfect realization of required respiratory
maneuvers or the inability to comply with the study procedure.The Vc measurements were performed after the inclusion/
exclusion criteria had been verified.
Medical questionnaire
Two medical questionnaires recommended for epidemiologicalresearch were combined and used to assess several children’s
characteristics [9].The questionnaire was written in Arabic. It was composed of
37 questions, mainly closed responses and usually dichotomous.
Questions were asked by an examiner with whom children orchildren–parents were not familiar. Children or parents of thesubjects answered questionnaires regarding demographic data,
general health information (especially birth weight, height andgestational age noted from the personal health records), ques-tions on clinical symptoms and diagnosis of allergic diseases.
Two subgroups of children were defined according to sports
activity (non-active and active) based on the response to thefollowing question [10]: do you practice any sport activity out-side school?
Two socio-economic levels (SEL) were distinguished basedon the ratio between the number of inhabited rooms andhousehold size (<1.5: unfavorable; P1.5: favorable) [11].
Physical examination
Anthropometric data were verified, measured or calculated:
age (year), height (cm), weight (kg), body mass index (BMI,kg/m2), and body surface area (BSA, m2).
The decimal age (accuracy to 0.1 years) was calculated fromthe date of measurement and the date of birth. Due to the fail-
ure of software to compute decimal age as the difference be-tween test date and birth date, age was taken as the numberof complete years from birth to the date of the study.
Height (cm) was measured with a height gauge, in a subjectwith shoes taken off; heels joined, and backwell straight.Weight(±1 kg) was measured in a subject without heavy clothes.
BMI (=weight/height2, kg m�2) was calculated. Over-weight and obesity were defined according to the criteria ofCole et al. [12] depending on age and BMI. Two groups of chil-
dren were identified (normal weight, overweight or obesity).BSA (m2) was calculated by using weight in kg and height
in cm [13]: BSA (m2) = 0.007184 · weight0.425 · height0.725.
Diffusion capacities, Dm and Vc measurements
Volume and gas calibrations of the Hyp’Air lung diffusion sys-tem (Medisoft, Dinant, Belgium) were performed prior to each
testing session.DLNO and DLCO were measured simultaneously during a
single breath maneuver using the automated apparatus. Dm
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (201
and Vc were then calculated according to the classic model ofpulmonary diffusion proposed by Roughton and Forster [1].
Subjects were in the sitting position, they wore a nose clip. A
mixture containing 0.28% CO, 14% helium (He), 21% O2 bal-anced with nitrogen (N2) was mixed with a NO/N2 mixture(450 ppm NO/N2, Air Liquide Sante, Tunisia). The final con-
centration of NO in the inspired bag was 40 ppm and that ofO2 was 19.1%. The apparatus was calibrated for gas fractionsusing automated procedures. The linearity of the analyzers
was factory checked. Linearity on site could be checked by dilu-tion procedures, i.e. dilution of the NO mixture with the CO/He/O2 mixture to check NO analyzer linearity, or dilution ofthe CO/He/O2 mixture with air to check CO analyzer linearity
[14,15]. The screen pneumotachograph was calibrated dailywith a 2 L syringe.
The subject breathed through a mouth-piece and a filter
connected to the pneumotachograph. When needed, subjectwas requested to make a deep expiration. Then at the onsetof the next inspiration, a valve opened allowing the subject
to inspire the mixture during a rapid deep inspiration. Abreath-hold of 4 s was then requested followed by a rapid expi-ration. The first 0.8 L of expired gas was rejected as the further
0.6 L was sampled in a bag which was automatically analyzedfor NO, CO and He. The delay to analyze the sample of ex-pired gas was constant, 35 s. The alveolar volume (VA) wasdetermined during the apnea; it was calculated using the He-
dilution technique. A breath-holding time of 4–5 s was chosen.As the recent international guidelines recommend a mini-
mum of 4 min between DLCOmeasurements [16], subjects per-
formed the single-breath maneuver with a minimum of 4.5 minbetween tests. Five sequential diffusion capacity tests were per-formed. Based on the recent international criteria [16], the aver-
age value of two trials whose difference in diffusing capacity iswithin 10% of each other is considered acceptable.
Values of Dm and Vc were calculated according to the
model of Roughton and Forster [1]. ‘‘1/HNO’’ was assumednegligible [17], therefore DLNO = DmNO. DmCO was calcu-lated as ‘‘DmNO/a’’ where ‘‘a’’ = 1.97 following Graham’slaw [1]. To calculate Vc, HCO reference values from Forster,
as he recommended, were chosen [18]. Mean capillary O2 pres-sure was estimated at 100 mmHg taking into account theslightly lower than normal O2 fraction in the inspired mixture.
So the measured parameters by the double transfer techniquewere: Vc, Dm, DLCO, DLNO, VA and residual volume (RV).
Statistical analysis
Data analysis
The Kolmogorov–Smirnov test was used to analyze variable
distribution [19]. When the distribution is normal and the vari-ances are equal, the results are expressed by theirmeans ± standards deviations (SD). If the distribution is not
normal, the results are expressed by their medians (1st–3rdquartiles).
Univariate and multiple regression analysis: Influencing factors
Pearson product-moment correlation coefficients (r) evaluatedthe associations between Vc or Dm and the continuous mea-sures: age, height, weight, BMI, BSA, RV (l) and VA (l).
The linearity of association between Vc or Dm and the con-tinuous measures was checked graphically by plotting each
pillary blood volume and pulmonary membrane diffusing capacity in4), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

4 S. Rouatbi et al.
regressor against the Vc or Dm. Only significantly and linearlyassociated variables were entered into the model. A linearregression model was used to evaluate the independent vari-
ables explaining the variance in Vc or Dm. Candidate variableswere stepped into the model with a stepwise selection method.To determine entry and removal from the model, significance
levels of 0.15 and 0.05 were used, respectively. No collinearitybetween predictors was detected with variance inflationfactors.
Vc and Dm simplified reference equations
As for the most published Vc or Dm adult’s reference equa-tions [20], we have established a simple Vc and Dm reference
equation using only significant anthropometric data age aspredictors of Vc or Dm in another stepwise linear regressionmodel. The model was evaluated by correlation (r) and deter-
mination (r2) coefficients and the standard error. The 95%confidence interval (95% CI) was calculated as follows [21]:95% IC = 1.64 · residual standard deviation (RSD).
A measured Vc or Dm lower than the upper limit of normal
(ULN = theoretical value � 1.64 · RSD) will be consideredabnormal.
Analyses were carried out using Statistica (Statistica Kernel
version 6, StatSoft, 26 France). Significance was set at the 0.05level.
Table 1 Applied non-inclusion and exclusion criteria.
Brief description
Recent airway infection (cold, flu, sore throat within the last 7 days)
Poor cooperation to achieve a standard spirometry or a correct FeNO m
Current smoker
Asthma or obstructive ventilator defect (FEV1/FVC ratio < LLN)
Allergy
Medication use (glucocorticoid)
Premature children
Unaccepted FVC maneuver
For abbreviations, see abbreviations list.
Table 2 Anthropometric and pulmonary diffusing capacities data i
[8–9] years (n = 11) [10–11] years (n = 49) [1
Anthropometric data
Age** (Yr) 9 (9–9) 11 (11–11)€ 12
Height* (m) 1.35 ± 0.07 1.49 ± 0.06€ 1.
Weight* (kg) 33 ± 7 40 ± 7€ 43
BMI* (kg.m�2) 18.0 ± 2.8 18.0 ± 2.7 17
BSA* (m2) 1.12 ± 0.15 1.29 ± 0.12€ 1.
Pulmonary diffusing capacities data
VA** (l) 2.72 (2.17–2.91) 3.47 (3.10–3.69)€ 3.
RV** (l) 0.79 (0.70–1.04) 1.19 (0.92–1.36) € 1.
DLNO* 86.66 ± 26.25 106.39 ± 24.53 € 12
DLCO* 18.10 ± 3.17 21.91 ± 3.81 € 22
Vc** (ml) 58.50 (46.30–66.10) 68.70 (57.20–79) 54
Dm* (ml/min/mmHg) 44.00 ± 13.32 53.77 ± 12.48€ 62
For abbreviation, see abbreviation list.* Data are mean ± SD.** Data are median (1st–3rd quartiles).€ p< 0.05: comparison from one range to the next.
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (20
Results
An initial sample of 172 voluntary children was examined.Non-inclusion criteria (Table 1) were found in 78 boys. 9 vol-
untary girls were examined and excluded from the study. Fi-nally, 85 boys were included to establish Vc and Dmreference values. All patients were not obese and had a favor-
able socio economic level (SEL) and qualified as active. Thenumber of boys in each age group, the anthropometric, lungvolumes and Vc and Dm data are given in Table 2. Fewer boysaged [14–16] years (9.4% of the total sample) were included.
Comparison from one range to the next, showed that Vc valuesincreased significantly from the [12–13] to the [14–16] ageranges (value is multiplied by three) and that Dm values in-
creased significantly from the [8–9] to the [10–11] age rangesand from the [10–11] to the [12–13] age ranges.
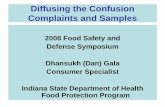
The Vc of the 85 healthy boys is shown in Fig. 1, according
to age, height and weight ranges (Fig. 1A–C, respectively). Sig-nificant Vc increases were found from the [12–13] to the [14–16] age ranges, from the [26–34] to the [35–40] weight ranges
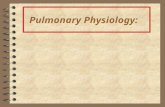
and from the [46–50] to the [51–69] weight ranges.The Dm of the 85 healthy boys is shown in Fig. 2, accord-
ing to age, height and weight ranges (Fig. 1A–C, respectively).Significant Dm increases were found from the [8–9] to the
[10–11] age ranges and from the [10–11] to the [12–13] age
Number
12
easure 21
2
3
7
2
1
30
n different age groups.
2–13] years (n= 17) [14–16] years (n= 8) Total sample (n= 85)
(12–13) € 16 (14–16) € 11 (10–12)
54 ± 0.08€ 1.64 ± 0.08€ 1.50 ± 0.10
± 8 56 ± 9€ 41 ± 9
.9 ± 2.0 20.80 ± 3.13€ 18.24 ± 2.74
35 ± 0.16 1.60 ± 0.16€ 1.31 ± 0.18
84 (3.45–4.01) € 6.41 (4.67–7.29) € 3.47 (2.96–3.99)
26 (1.11–1.44) 1.97 (1.72–2.87) € 1.20 (0.89–1.40)
3.98 ± 26.03 € 114.55 ± 54.12 108.12 ± 30.26
.20 ± 5.60 33.22 ± 6.97 € 22.54 ± 5.76
.40 (45.90–71.30) 151.25 (108–180.5) € 67 (53.30–81.30)
.92 ± 13.22€ 58.13 ± 27.49 54.75 ± 15.39
pillary blood volume and pulmonary membrane diffusing capacity in14), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

Figure 1 The pulmonary capillary blood volume in subgroups of children, according to age (A), height (B) and weight (C) ranges.
n= number of children. Data are shown as box-and-whiskers-plots illustrating the median (s), 25%75% (h) and minimum–maximum
( ). *p< 0.05: Comparison (T-test) from one range to the next. NS: not significant.
Capillary blood volume and pulmonary membrane diffusing capacity norms in North African boys 5
ranges. A significant Dm decrease was found from the [41–45]to the [46–50] weight ranges.
Univariate Spearman correlation coefficients (r) betweenthe Vc or Dm of the 85 healthy boys data are shown in Table 3.Only BMI was not significantly correlated with Dm.
Table 4 presents the cumulative r2 of the independentinfluencing factors included in the Vc and Dm forward linearstepwise multiple regressions. VA, BMI, height, age, weight
and BSA explain 60.8% of Vc variability. The forward linearstepwise multiple regression Vc model is as follows: Vc (ml) =0.000041 · VA (l) + 0.720789 · BMI (kg m�2) + 0.407270 ·height (cm) + 0.046601 · age (Yr) + 0.047680 · Weight (kg) +0.095710 · BSA (m2) + 0.989652. VA, RV, age and heightexplain 25.6% of Dm variability. The forward linearstepwise multiple regression Dm model is as follows: Dm (ml/
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (201
min/mmHg) = 0.004469 · VA+ 0.097675 · VR+ 0.031998 ·age + 0.066044 · height + 0.838455.
The proposed Vc reference equation (Table 5) is asfollows: Vc (ml) = 11.3859 · age + 3.4613 · BMI � 117.0508.This model explains 45.7% of the Vc variability. To calculate
the lower limit of normal value subtract 42.48778 from the Vccalculated reference value.
The proposed Dm reference equation (Table 5) is as
follows: Dm (ml/min/mmHg) = 0.6430 · height � 41.5854.This model explains only 16.31% of the Dm variability. Tocalculate the lower limit of normal value subtract 23.22076
from the Dm calculated reference value.In the 85 boys of our study, the calculated Vc corresponded
to 102 ± 36% (95%IC: 94–110%) of the predicted Vc. andthe calculated Dm corresponded to 100 ± 25% (95%IC:
pillary blood volume and pulmonary membrane diffusing capacity in4), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

Figure 2 The pulmonary membrane diffusing capacity in subgroups of children, according to age (A), height (B) and weight (C) ranges.
n= number of children. Data are shown as box-and-whiskers-plots illustrating the mean (h) and standard deviation ( ). *p< 0.05:
Comparison (T-test) from one range to the next. NS: not significant.
6 S. Rouatbi et al.
95–105%) of the predicted Dm. The difference between thecalculated and predicted Vc of the 85 boys was not significant(73.88 ± 34.74 ml vs. 73.88 ± 23.49 ml, p= 0.99) and the
correlation was significant (r = 0.68; p= 0.0001). In addition,only 1 boy (1.17%) showed a measured Vc lower than theLLN of the predicted Vc.
The difference between the measured and predicted Dm ofthe 85 boys was not significant (54.75 ± 15.38 ml/min/mmHgvs. 54.75 ± 6.21 ml/min/mmHg, p = 0.99) and the correlation
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (20
was significant (r = 0.40; p = 0.0001). In addition, only 2 boys(2.35) showed a measured Dm lower than the LLN of thepredicted Dm.
Discussion
The aims of this study were to identify the factors influencing
Vc and Dm and to establish linear regression equations for
pillary blood volume and pulmonary membrane diffusing capacity in14), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

Table 3 Univariate Spearman correlation coefficients (r)
between the pulmonary diffusing capacities and the 85 healthy
boys’ data.
Vc Dm DLNO DLCO
Age (Yr) 0.62* 0.24* 0.24* 0.64*
Height (m) 0.46* 0.40* 0.40* 0.61*
Weight (kg) 0.59* 0.30* 0.30* 0.60*
BMI (kg m�2) 0.42* 0.11 0.11 0.34*
BSA (m2) 0.58* 0.35* 0.34* 0.63*
VA (l) 0.71* 0.41* 0.41* 0.82*
RV (l) 0.60* 0.26* 0.25* 0.76*
For abbreviations, see abbreviation list.* p< 0.05.
Capillary blood volume and pulmonary membrane diffusing capacity norms in North African boys 7
predicting reference values for Vc and Dm in healthy Tunisianboys aged 8 to 16 years.
Most children above the age of 7–8 years can perform the
full range of tests available for older individuals, using similarprotocols to those described elsewhere in this Monograph. Bycontrast, assessments in young children have generally been re-
stricted to specialized research establishments, due to the lackof suitable equipment and the complexity of undertaking suchmeasurements [22].
Table 5 Pulmonary capillary blood volume and pulmonary membra
Independent variables B P level
Vc (ml)
Constant �117.0508 0.000005
Age (Yr) 11.3859 0.000000
BMI (kg m�2) 3.4613 0.001773
Dm (ml/min/mmHg)
Constant �41,5854 0.08687
Height (cm) 0.6430 0.00013
For abbreviations, see abbreviations list. 95% CI: 95% confidence interv
Table 4 Independent variables included in the forward linear stepw
volume and pulmonary membrane diffusing capacity of the 85 healt
Independent variables B P level
Vc (ml)
Constant �4.138 0.98965
VA (l) 18.043 0.00004
BMI (kg.m�2) 3.189 0.72078
Height (cm) 3.325 0.40727
Age (Yr) 5.224 0.04660
Weight (kg) 13.898 0.04768
BSA (m2) �901.322 0.09571
Dm (ml/min/mmHg)
Constant �6.262 0.83845
VA (l) 9.733 0.00446
RV (l) �7.954 0.09767
Age (Yr) �3.340 0.03199
Height (cm) 0.487 0.06604
For abbreviations, see abbreviations list. 95% CI: 95% confidence interv
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (201
Healthy subjects were selected by including all children whorespond to inclusion criteria. These different criteria describedpreviously have been inspired by similar studies according to
ATS/ERS guidelines [23]. 78 boys were excluded from thegroup suffering from respiratory diseases or with a recent his-tory of respiratory infections. Therefore 94 subjects remained
with 85 boys and 9 girls. Due to the low number of girls, wehave eliminated the female gender of our study. Thus, theremaining 85 boys (age range, 8–16 years) were coded as being
well and were included in the final study population. Ideally,reference values are calculated with equations derived frommeasurements observed in a representative sample of healthysubjects in a general population. A large number of subjects
(i.e., n> 100) are needed to ensure no significant differencebetween the published reference equations and those fromthe local community [8]. Because, it is the first work establish-
ing reference values of Vc and Dm for healthy children, thissample size (n= 85) can be considered as acceptable.
Two questionnaires were combined and used to evaluate
the characteristics of several children: the ATS-DLD-78-Cand ISSAC children’s questionnaire [9]. Some modificationswere established to fit the socio-cultural needs. There were
medical questionnaires most recommended for epidemiologi-cal research. The questionnaire was written in Arabic andwas composed of 37 questions, mainly closed response andusually dichotomous. Questions were asked by an examiner
ne diffusing capacity reference equations for the 85 healthy boys.
95% CI Cumulative r2 1.64 RSD
�156.2042 to �77.89738.5211–14,2507 0.3880 42.48778
1.7047–5,2178 0.4571
�80.9470 to �2.2238 23.22076
0.3808–0.9052 0.1631
al around each B.
ise multiple regression model for the pulmonary capillary blood
hy boys.
95% CI Cumulative r2
2 305.319–941.401
1 �3.982–12.278 0.513
9 �8.534–26.313 0.547
0 �3.831–11.812 0.559
1 �2.480–7.647 0.587
0 �6.632–20.447 0.594
0 �513.079–1581.994 0.608
5 �29.390–90.6189 �3.193–9.846 0.172
5 �4.557–14.050 0.201
8 �1.469–4.528 0.224
4 �0.251–0.774 0.256
al around each B.
pillary blood volume and pulmonary membrane diffusing capacity in4), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

8 S. Rouatbi et al.
with whom children or children-parents were not familiar. Thisquestionnaire was validated for the Arabic language.
In this study, Dm and Vc were calculated at rest among
healthy children aged from 8 to 16 years. We used a techniqueof double transfer of NO–CO. Roughton and Forster demon-strated that CO diffusion measured by the diffusing capacity of
the lung for CO reflected both Dm and reaction with Vc [1,15].The diffusion capacity test was performed by children after acalibration of the analysers and the pneumotachograph of
the hyp’air Compact Medisoft device.This technique is suitable for measuring the simultaneous
transfer of two gases NO and CO known by their reactivitywith Hb. A correlation between DLCO and the Hb concentra-
tion was demonstrated by several authors [2,17,24–28]. In ourstudy, we investigated the notion of anemia in the question-naire and the medical files of children. All subjects in our sam-
ple did not present anemia (Hb between 12 and 14 g/100 ml).Corrections of Vc values based on Hb were not made. In fact,Stam et al. [26] demonstrated that in healthy subjects, the cor-
rection of Hb levels had no effect on the values of DLNO,DLCO, Dm and Vc.
This method was also characterized by ease of implementa-
tion since the breath-holding time of 4–5 s was chosen. In fact,it has been shown that DLCO values were not different with 3or 5 s [2,17,27–29]. In normal subjects, an apnea time of threeseconds instead of 10 s produced no change in measured
DLCO [17,27,29]. Apart from considerations of NO oxidationand detection, breathless patients may have difficulty holdingtheir breath for 10 s [14,15]. The main methodological advan-
tage was that it was a one-time technique reducing greatly theintra-individual dispersion of measurements [28]. The coeffi-cients of variation of Dm and Vc for a given subject were much
smaller than with the conventional technique in two times [28].Initial works showed no significant difference in mean valuesof Dm and Vc calculated with the conventional method in
two times and those calculated by this new technique of doubletransfer of NO and CO [17,27,29].
Since the development of this technique, the specific prob-lem was due to the use of NO as a test gas. Zavorsky and Mur-
ias [30] showed that the inhalation of repeated inhalations of40–50 ppm of NO during single breath-hold maneuvers didnot increase DLNO, DLCO, Dm and Vc. In fact, five sequen-
tial breath-hold maneuvers did not change DLNO and thusDm.
NO is theoretically an ideal gas to study the function of the
alveolar-capillary membrane [31]. The heme structure ofhemoglobin has great affinity for NO, and we believe that in-haled NO is inactivated by hemoglobin, thereby restricting itsvasodilator activity in the lung [32]. NO is combined with
hemoglobin forming nitrosyl hemoglobin with an affinity1500 times higher than that measured for carbon monoxide[33].
It is therefore reasonable to assume that 40 ppm inhaledNO for three consecutive tests of a single respiratory cycle ap-nea time relatively short (3 s) cannot have direct toxic effect on
the lungs of our subjects [2].We designed the present study with the aim of establishing
a reference equation for Vc and Dm in a healthy North Afri-
can child population. To our knowledge, these are the first re-ported data on reference values of Vc and Dm for healthy boysaged from 8 to 16 years.
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (20
The most important determinants of lung volume are bodysize, sex and age, and the usual approach is to use some com-binations of these attributes when predicting lung volume
[34–36]. However, during recent years, there has been increas-ing evidence of ethnic [35,37,38] and environmental influences(e.g. passive smoking, SEL), which also need to be borne in
mind, together with the potential effects of puberty.All patients of the present study had a favorable SEL and
qualified as active. Several studies were conducted on school-
children to predict lung functions using SEL [39–41]. Studiesfrom the United Kingdom [42] China [43] and Malaysia [44]did not find any relationship between SEL and lung functionsin children contrary to the Canadian [40] and the Indian [41]
studies where they found a significant impact of the SELregarding pulmonary functions. In the present study, the im-pact of SEL and physical activity on diffusing variables cannot
be studied because there is no variability of these two param-eters in our children sample.
Comparison from one range age to the next, showed that
DLCO and Vc values increased significantly from the{12–13} to the {14–16} age ranges (value is multiplied by three)and DLNO and Dm values increased significantly from the
{8–9} to the {10–11} age ranges and from the {10–11} to the{12–13} age ranges. These results can be explained by the effectof puberty. Indeed, the beginning of puberty in boys occurredat the age of 11.5 to 14.5 [45]. Indeed, at puberty children
increase in height. This anthropometric parameter is consideredas the most important determinant of functional respiratoryparameters [15].
Since the work of Krogh N. in 1914 [46] which showed thatDLCO/body surface area does not depend on age in adults,several other studies [47,48] were interested in studying the ef-
fect of age on the different functions of the deep lung and inparticular the DLCO. The influence of age on the Dm andVc has not been well studied. These works have often focused
on a small number of subjects; and no children were includedin the samples. In our study where the sample included onlychildren, it was found that the VA, the Dm, the Vc, the DLNOand the DLCO increased with age, this increase was related to
growth in height and weight. Significant DLNO, DLCO andVc increases were found from the {26–34} to the {35–40}weight ranges and from the {46–50} to the {51–69} weight
ranges. A significant Dm decrease was found from the {41–45}to the {46–50} weight ranges. This result was confirmed by Cotes[38], Zanen [49], and Rouatbi [50].
For the total sample, DLCO, DLNO, Vc and Dm were sig-nificantly correlated to age, height, weight, BSA, VA and RV.DLCO and Vc were significantly correlated to BMI (r = 0.42).Several studies show the positive correlation of lung function
with anthropometric data in children [51,52]. Height had thesame effects in all approaches: Vc and Dm values increasedwith increasing height [15]. Van Der Lee et al. [55] found that
the DLNO which was considered as the Dm was much stron-ger related to the VA than Dm. In fact, lung size seems to be adeterminant factor: larger lungs show a stronger NO uptake
and therefore the DLNO is dependent on VA. In agreementwith our results Dm was not significantly correlated withBMI in males [53]. It is the physiological lung growth which
depends essentially on height. Keifer et al. [54] showed thatthe associations of age and height with lung function were sim-ilar across the 3 major ethnic groups.
pillary blood volume and pulmonary membrane diffusing capacity in14), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

Capillary blood volume and pulmonary membrane diffusing capacity norms in North African boys 9
Reference equations were determined using anthropometricand spirometric data as predictors of Vc or Dm in a stepwiselinear regression model. VA, BMI, height, age, weight and
BSA explained 60.8% of Vc variability. The forward linearstepwise multiple regression Vc model is as follows:Vc(ml) = 0.000041 · VA (l) + 0.720789 · BMI (kg m�2) +
0.407270 · height (cm) + 0.046601 · age (Yr) + 0.047680 ·Weight (kg) + 0.095710 · BSA (m2) + 0.989652.
VA, RV, age and height explained 25.6% of Dm variability.
The forward linear stepwise multiple regression Dm model isas follows:
Dm(ml/min/mmHg) = 0.004469 · VA+ 0.097675 · VR+0.031998 · age + 0.066044 · height + 0.838455. A measured
Vc or Dm lower than the lower limit of the normal range(LLN = predicted value � 1.64 · RSD) is considered asabnormal.
Zanen et al. [49] showed that VA played an important role,although the exact influence on DLCO is still under debate[56,57]. It, therefore, seems plausible that when a sample of
short subjects is selected, lower Dm and Vc values will bemeasured and another set of regression equations will follow.Because VA played an important role, the diffusing capacity
makes it an attractive covariate to include in reference equa-tions. Chinn et al. [56] showed that the inclusion of VA dividedby height (H) squared (VA.H�2) lowers RSD considerably.However, when a VA term appears in a reference equation,
the diffusion parameters are corrected for VA, which resultsin obtaining Dm or Vc per liter VA. The first of the twoparameters serves the same purpose as the well-known KCO
(=DLCO/VA). It is not so much a question of whether VAis a better parameter than height or age, but if its inclusionwould result in a new and different parameter. Dm/VA,
Vc/VA or Dm/VA.H�2, Vc/VA.H�2 are not, at present,routinely used. More research is needed to select the bestparameter and to design a proper evaluation scheme
(especially for Vc) [49]. The same logic can be applied withthe VR and its influence on Dm.
Of pure and simple practical interest we established refer-ence equations by including, as independent variables, only
anthropometric data: height for Dm; age and BMI for Vc.Inclusion of only anthropometric data in reference equationsis justified by their easy use to assess their association with
dependent variables. Although VA and RV showed strongrelationships with Dm and Vc in univariate analysis, they werenot included in the reference equations [23]. Indeed, VA and
RV were not found in published reference equations for Vcand Dm [39,50,51]. So the proposed Vc reference equation isas follows: Vc (ml) = 11.3859 · age+ 3.4613 · BMI� 117.0508.This model explains 45.7% of the Vc variability. To calculate
the lower limit of normal value subtract 42.48778 from the Vccalculated reference value.
The proposed Dm reference equation is as follows: Dm
(ml/min/mmHg) = 0.6430 · height � 41.5854. This model ex-plains only 16.31% of the Dm variability. Other factors, asthe length of the upper part of the body, body circumference,
nutritional comportment and air pollution could explain therest of the Dm variability. To calculate the lower limit of nor-mal value subtract 23.22076 from the Dm calculated reference
value.The difference between the measured and predicted Vc of
the 85 boys was not significant (73.88 ± 34.74 ml vs.73.88 ± 23.49 ml, p = 0.99) and the correlation was
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (201
significant (r = 0.68; p= 0.0001). In addition, only 1 boy(1.17%) showed a measured Vc lower than the LLN of thepredicted Vc.
The difference between the measured and predicted Dm ofthe 85 boys was not significant (54.75 ± 15.38 ml/min/mmHgvs. 54.75 ± 6.21 ml/min/mmHg, p = 0.99) and the correlation
was significant (r= 0.40; p= 0.0001). In addition, only 2 boys(2.35) showed a measured Dm lower than the LLN of thepredicted Dm.
Because of the lack of published reference values of Dmand Vc in children, comparison of Vc and Dm referencesfound in our study with published references could not beperformed.
In conclusion, we have established a reliable reference equa-tion to interpret the results of Vc and Dm in healthy NorthAfrican children subjects. Vc and Dm can easily be predicted
by anthropometric parameters. Our Vc and Dm referenceequations enrich the world bank of reference equations, inwhich the physician could choose according to their regional
localization or patient ethnic composition.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
The authors wish to thank Drs. Ahmed Sahloul Essoussi and
Imed Laatiri for their invaluable contribution in the prepara-tion of the manuscript.
References
[1] F.J.W. Roughton, R.E. Forster, Relative importance of
diffusion and chemical reaction rates in determining the rate
of exchange of gases in the human lung, with special reference to
true diffusing capacity of the pulmonary membrane and volume
of blood in lung capillaries, J. Appl. Physiol. 11 (1957) 290–302.
[2] C.D.R. Borland, T.W. Higenbottam, A simultaneous single
breath measurement of pulmonary diffusing capacity with nitric
oxide and carbon monoxide, Eur. Respir. J. 2 (1989) 56–63.
[3] R.M. Tamhane, R.L. Johnson Jr, C.C.W. Hsia, Pulmonary
membrane diffusing capacity and capillary blood volume
measured during exercise from nitric oxide uptake, Chest 120
(2001) 1850–1856.
[4] P.J. Merkus, E.S. Govaere, W.H. Hop, H. Stam, H.A. Tiddens,
J.C. de Jongste, Preserved diffusion capacity in children with
cystic fibrosis, Pediatr. Pulmonol. 37 (1) (2004) 56–60.
[5] E. Abdulla, I. Al-Zakwani, S. Baddar, R. Abdwani, Extent of
subclinical pulmonary involvement in childhood onset systemic
lupus erythematosus in the sultanate of oman, Oman Med. J. 27
(1) (2012) 36–39.
[6] E. Bourli, M. Dimitriadou, M. Economou, E. Vlachaki, A.
Christoforidis, E. Maratou, I. Stanopoulos, P. Argyropoulou,
V. Aivazis, Restrictive pulmonary dysfunction and its predictors
in young patients with b-thalassaemia major, Pediatr. Pulmonol.
47 (8) (2012) 801–807.
[7] R.L. Mulder, N.M. Thonissen, H.J. van der Pal, P. Bresser, W.
Hanselaar, C.C. Koning, F. Oldenburger, H.A. Heij, H.N.
Caron, L.C. Kremer, Pulmonary function impairment measured
by pulmonary function tests in long-term survivors of childhood
cancer, Thorax 66 (12) (2011) 1065–1071.
[8] R. Pellegrino, G. Viegi, V. Brusasco, R.O. Crapo, F. Burgos, R.
Casaburi, et al, ATS/ERS Task Force: standardisation of lung
pillary blood volume and pulmonary membrane diffusing capacity in4), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

10 S. Rouatbi et al.
function testing. Interpretative strategies for lung function tests,
Eur. Respir. J. 26 (2005) 948–968.
[9] B.G. Ferris, Epidemiology standardization project II:
recommended respiratory disease questionnaire for use with
adults and children in epidemiological research, Am. Rev.
Respir. Dis. 118 (1978) 7–52.
[10] G. Pouessel, C. Santos, C. Thumerelle, V. Neve, A. Sardet, N.
Wizla, et al, Reproductibilite du test de marche en navette chez
des enfants atteints de mucoviscidose, Rev. Mal. Respir. 20
(2003) 711–718.
[11] F. Lazreg, A. Ben Abdelaziz, R. Gaha, A. Ghedira, A.
Boussaadia, H. Ghannem, Behaviours and needs for health of
secondary-school-adolescents in Sousse (Tunisia), Tunis Med.
83 (2005) 731–738.
[12] T.J. Cole, M.C. Bellizzi, K.M. Flegal, W.H. Dietz, Establishing
a standard definition for child overweight and obesity
worldwide: international survey, BMJ 320 (2000) 1240–1243.
[13] D. Dubois, E.F. Dubois, A formula to estimate the appropriate
surface area if height and weight be known, Arch. Intern. Med.
17 (1916) 863–871.
[14] Y. Trabelsi, H. Ben Saad, Z. Tabka, N. Gharbi, A. Bouchez
Buvry, J.P. Richalet, et al, Spirometric reference values in
Tunisian children, Respiration 71 (2004) 508–511.
[15] C. Borland, A place for T(L, NO) with T(L, CO)?, Eur Respir. J.
31 (5) (2008) 918–919.
[16] B. Aguilaniu, J. Maitre, S. Glenet, A. Gegout-Petit, H. Guenard,
European reference equations for CO and NO lung transfer,
Eur. Respir. J. 31 (5) (2008) 1091–1097.
[17] N. Macintyre, R.O. Crapo, G. Viegi, D.C. Johnson, C.P. van
der Grinten, V. Brusasco, et al, Standardisation of the single-
breath determination of carbon monoxide uptake in the lung,
Eur. Respir. J. 26 (2005) 720–735.
[18] H. Guenard, N. Varene, P. Vaida, Determination of lung
capillary blood volume and membrane diffusing capacity in man
by the measurements of NO and CO transfer, Respir. Physiol. 70
(1987) 113–120.
[19] R.E. Forster, Diffusion of gases across the alveolar membrane,
in: L.E. Fahri, S.M. Tenney (Eds.), Handbook of Physiology.
The Respiratory Systazem, Gas Exchange, American
Physiological Society, Washington, D.C., 1987, pp. 71–88.
[20] H. Ben Saad, C. Prefaut, R. Missaoui, I. Hadj Mohamed, Z.
Tabka, M. Hayot, Reference equation for 6-min walk distance
in healthy North African children 6–16 years old, Pediatr.
Pulmonol. 44 (2009) 316–324.
[21] S. Rouatbi, H. Ben Saad, I. Latiri, Z. Tabka, H. Guenard,
North African references of alveolar membrane diffusion
capacity and pulmonary capillary blood volume, Respiration
80 (2010) 301–312.
[22] M. Jenicek, R. Cleroux, Clinical epidemiology: its evolution and
role in clinical practice and research, Union Med. Can. 114
(1985) 625–632.
[23] P.J.F.M. Merkus, J.C. de Jongste, J. Stocks, Respiratory
function measurements in infants and children, Eur. Res. Soc.
Monogr. 31 (2005) 166–194.
[24] N. MacIntyre, R.O. Crapo, G. Viegi, D.C. Johnson, C.P.M. van
der Grinten, V. Brusasco, et al, Standardisation of the single-
breath determination of carbon monoxide uptake in the lung,
Eur. Respir. J. 26 (2005) 720–735.
[25] P. Dinakara, W.S. Blumenthal, R.F. Johnston, L.A. Kaufmann,
P.B. Solnick, The effect of anemia on pulmonary diffusing
capacity with derivate of a correction equation, Am. Rev.
Respir. Dis. 102 (1970) 965–969.
[26] J.S. Guliera, J.N. Pande, M.M. Markose, R.G. Gupta, B.P.
Jain, Pulmonary function in chronic severe anemia, Clin. Sci. 40
(1971) 317–325.
[27] H. Stam, F.J. Kreuzer, A. Versprille, Effect of lung volume and
positional changes on pulmonary diffusing capacity and its
components, J. Appl. Physiol. 71 (4) (1991) 1477–1488.
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (20
[28] J. Moinard, H. Guenard, Membrane diffusion of the lungs in
patients with chronic renal failure, Eur. Respir. J. 6 (1993) 225–
230.
[29] J. Moinard, G. Manier, O. Pillet, Y. Castaing, Effect of inhaled
nitric oxide on hemodynamics and VA/Q inqualities in patients
with chronic obstructive lung disease, Am. J. Respir. Crit. Care
Med. 149 (1994) 1482–1487.
[30] P. Vaida, C. Kays, D. l Riviere, P. Techoueyres, Lachaud JL:
Pulmonary diffusing capacity and pulmonary capillary blood
volume during parabolic flights, J. Appl. Physiol. 82 (1997)
1091–1097.
[31] G.S. Zavorsky, J.M. Murias, A small amount of inhaled nitric
oxide does not increase lung diffusing capacity, Eur. Respir. J.
27 (6) (2006) 1251–1257.
[32] M. Meyer, J. Piiper, Nitric oxide (NO), a new gas for study of
alveolar-capillary diffusion, Eur. Respir. J. 2 (1989) 294–496.
[33] C. Frostell, M.D. Fratacci, J.C. Wain, R. Jones, W.M. Zapol, A
selective pulmonary vasodilator reversing hypoxic pulmonary
vasoconstriction, Circulation 84 (5) (1991) 2212.
[34] Q.H. Gibson, F.J.W. Roughton, The kinetics of equilibria of the
reactions of nitric oxide with sheep haemoglobin, J. Physiol. 136
(1957) 507–526.
[35] Ph.H. Quanjer, J. Stocks, G. Polgar, M. Wise, J. Karlberg, G.
Borsboom, Compilation of reference values for lung function
measurements in children, Eur. Respir. J. 2 (Suppl 4) (1989)
184s–261s.
[36] Ph.H. Quanjer, G.J. Tammeling, J.E. Cotes, O.F. Pedersen, R.
Peslin, J.C. Yemault, Lung volumes and ventilator flows. Report
Working Party ‘‘Standardization of Lung Function Tests’’,
European Community for Steel and Coal and European
Respiratory Society, Eur. Respir. J. 6 (Suppl. 16) (1993)
5–40.
[37] A.S. Buist, Evaluation of lung function: concepts of normality,
in: D.H. Simmons (Ed.), Current Pulmonology, vol. 4,
Houghton Mifflin, Boston, 1982, Chapter 7.
[38] G.J. Miller, M.J. Saunders, R.J.C. Gilson, M.T. Ashcroft, Lung
function of healthy boys and girls in Jamaica in relation to
ethnic composition and habitual physical activity, Thorax 32
(1977) 486–496.
[39] J.E. Cotes, Lung function: assessment and application in
medicine, fifth ed., Blackwell Scientific Publications, Oxford,
1993.
[40] R.J. Rona, D. Mahabir, B. Rocke, S. Chinn, M.C. Gulliford,
Social inequalities and children’s height in Trinidad and
Tobago, Eur. J. Clin. Nutr. 57 (2003) 143–150.
[41] K. Demissie, P. Ernst, J.A. Hanley, U. Locher, D. Menzies,
M.R. Becklake, Socioeconomic status and lung function among
primary school children in Canada, Am. J. Respir. Crit. Care
Med. 156 (1996) 719–723.
[42] P.S. Raju, K.V. Prasad, Y.V. Ramana, N. Balakrishna, K.J.
Murthy, Influence of socioeconomic status on lung function and
prediction equations in Indian children, Pediatr. Pulmonol. 39
(6) (2005) 528–536.
[43] J.E. Lunn, J. Knowelden, A.J. Handyside, Patterns of
respiratory illness in Sheffield infant school children, Br. J.
Prev. Soc. Med. 21 (1967) 7–16.
[44] Y. Chen, W.X. Li, The effect of passive smoking on children’s
pulmonary function in Shanghai, Am. J. Public Health 76 (1986)
515–518.
[45] B.H.O. Azizi, R.L. Henry, Effects of indoor air pollution on
lung function of primary school children in Kaulalampur,
Pediatr. Pulmonol. 9 (1990) 24–29.
[46] N.A. Matveeva, L.V. Nazarova, N.G. Chekalova, M.V. Ashina,
E.O. Maksimenko, M.V. Shaposhnikova, The characteristics of
morphofunctional status of rural schoolchildren, Gig. Sanit. 4
(2011) 62–64.
[47] M. Krogh, The diffusion of gases through the lungs of man, J.
Physiol. 49 (1914) 271.
pillary blood volume and pulmonary membrane diffusing capacity in14), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007

Capillary blood volume and pulmonary membrane diffusing capacity norms in North African boys 11
[48] G. Viegi, D.L. Sherrill, L. Carozzi, F. Di Pede, S. Baldacci, F.
Pistelle, P. Enright, An 8-year follow-up of carbon monoxide
diffusing capacity in a general population sample of northern
Italy, Chest 120 (2001) 74–80.
[49] T. Ueda, G. Cheng, Y. Kuroki, H. Sano, K. Sugiyama, S.
Motojima, T. Fukuda, Effects of aging on surfactant forms in
rats, Eur. Respir. J. 15 (1) (2000) 80–84.
[50] P. Zanen, I. Van der Lee, T. Van der Mark, J.M.M. Van der
Bosch, Reference values for alveolar membrane diffusion
capacity and pulmonary capillary blood volume, Eur. Respir.
J. 18 (2001) 764–769.
[51] S. Rouatbi, Y.F. Ouahchi, C. Ben Salah, H. Ben Saad, I.
Harrabi, Z. Tabka, H. Guenard, Physiological factors
influencing pulmonary capillary volume and membrane
diffusion, Rev. Mal. Respir. 23 (2006) 211–218.
[52] Rajkapoor, K.K. Mahajan, A. Mahajan, Ventilatory lung
function tests in school children of 6–13 years, Indian J. Chest
Dis. Allied Sci. 39 (2) (1997) 97–105.
[53] R.V. Chowgule, V.M. Shetye, J.R. Parmar, Lung function tests
in normal Indian children, Indian Pediatr. 32 (2) (1995) 185–191.
Please cite this article in press as: S. Rouatbi et al., Reference values of caNorth African boys aged 8 to 16 years, Egypt. J. Chest Dis. Tuberc. (201
[54] G. Von Nieding, H.M. Wagner, H. Kreheler, Investigation of
the acute effects of nitrogen monoxide on lung function in man,
Proceedings of the 3 Intemational Clean Air Congress,
Dusseldorf, October 8–12, 1973 Dusseldorf. VDI-Verlag: A14–
A16.
[55] E.M. Kiefer, J.L. Hankinson, R.G. Barr, Similar relation of age
and height to lung function among Whites, African Americans,
and Hispanics, Am. J. Epidemiol. 173 (4) (2011) 376–387.
[56] I. Van der Lee, P. Zanen, N. Stigter, J.M. van den Bosch, J.W.
Lammers, Diffusing capacity for nitric oxide: reference values
and dependence on alveolar volume, Respir. Med. 101 (7) (2007)
1579–1584.
[57] D.J. Chinn, J.E. Cotes, R. Flowers, A.-M. Marks, J.W. Reed,
Transfer factor (diffusing capacity) standardized for alveolar
volume: validation, reference values and applications of a new
linear model to replace KCO (TL/VA), Eur. Respir. J. 9 (1996)
1269–1277.
pillary blood volume and pulmonary membrane diffusing capacity in4), http://dx.doi.org/10.1016/j.ejcdt.2014.02.007