Reduced access block causes shorter emergency department waiting times: An historical control...
7
Emergency Medicine (2003) 15, 232–238 Blackwell Publishing Ltd. Original Research Access block and ED waiting times Reduced access block causes shorter emergency department waiting times: An historical control observational study Robert Dunn Emergency Department, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia, Australia Abstract Objective: To study the effect of changes in hospital occupancy and ED occupancy on ED waiting times during a 13-day period of improved bed access. Methods: A comparative, observational study of 1133 ED attendances in the study period and 2332 attendances in a historical control period. Results: During the study period, mean hospital occupancy decreased from 94.9% to 89.0% (P < 0.001), mean ED occupancy decreased from 19.1 to 14.8 patients (P < 0.001) and the mean ED waiting time decreased from 58.5 to 37.1 min (P < 0.001). There were statistically significant reductions in waiting times for patients in Australasian triage scale (ATS) categories 2–5. Departmental staffing levels, attendances and patient acuity were not significantly different during the study and control periods. Conclusions: Modest decreases in hospital occupancy resulted in highly significant reductions in ED waiting times. Emergency department overcrowding due to large numbers of admitted patients awaiting hospital admission is a major cause of ED dysfunction. Key words: crowding, emergency service, health service accessibility, hospital bed occupancy, length of stay. Introduction Emergency department overcrowding is recognized as a major and increasingly frequent cause of ED dysfunction in many parts of the world, 1–4 with 91% of 575 United States ED Directors reporting it to be a problem. 1 The extent of ED overcrowding has been less well quantified in Australia, however, overcrowding due to the lack of availability of hospital beds for emergency admissions (‘access block’) is widespread 5–7 and has been described by the President of the ACEM as ‘the single biggest impediment to delivery of adequate emergency care in Australasia’. 8 Despite the high frequency of ED overcrowding, there is little published data on this topic. Previous investigators have noted an association between ED overcrowding and the number of patients in the waiting area 9 and reduced overcrowding is associated with increased Correspondence: Associate Professor Robert Dunn, Director of Clinical and Academic Emergency Medicine, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia. Email: [email protected] Robert Dunn, MBBS, FACEM, Grad Cert Mgmt, Grad Cert Lang, Director of Clinical and Academic Emergency Medicine, Royal Adelaide Hospital.
-
Upload
robert-dunn -
Category
Documents
-
view
212 -
download
0
Transcript of Reduced access block causes shorter emergency department waiting times: An historical control...

Emergency Medicine (2003) 15, 232–238
Blackwell Publishing Ltd.Original ResearchAccess block and ED waiting times
Reduced access block causes shorter emergency department waiting times: An historical control observational studyRobert DunnEmergency Department, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia, Australia
Abstract
Objective: To study the effect of changes in hospital occupancy and ED occupancy on ED waitingtimes during a 13-day period of improved bed access.
Methods: A comparative, observational study of 1133 ED attendances in the study period and 2332attendances in a historical control period.
Results: During the study period, mean hospital occupancy decreased from 94.9% to 89.0%(P < 0.001), mean ED occupancy decreased from 19.1 to 14.8 patients (P < 0.001) andthe mean ED waiting time decreased from 58.5 to 37.1 min (P < 0.001). There werestatistically significant reductions in waiting times for patients in Australasian triagescale (ATS) categories 2–5. Departmental staffing levels, attendances and patient acuitywere not significantly different during the study and control periods.
Conclusions: Modest decreases in hospital occupancy resulted in highly significant reductions in EDwaiting times. Emergency department overcrowding due to large numbers of admittedpatients awaiting hospital admission is a major cause of ED dysfunction.
Key words: crowding, emergency service, health service accessibility, hospital bed occupancy, length of stay.
Introduction
Emergency department overcrowding is recognizedas a major and increasingly frequent cause of EDdysfunction in many parts of the world,1–4 with 91%of 575 United States ED Directors reporting it to be aproblem.1 The extent of ED overcrowding has beenless well quantified in Australia, however, overcrowdingdue to the lack of availability of hospital beds for
emergency admissions (‘access block’) is widespread5–7
and has been described by the President of the ACEMas ‘the single biggest impediment to delivery ofadequate emergency care in Australasia’.8 Despitethe high frequency of ED overcrowding, there is littlepublished data on this topic. Previous investigatorshave noted an association between ED overcrowdingand the number of patients in the waiting area9 andreduced overcrowding is associated with increased
Correspondence: Associate Professor Robert Dunn, Director of Clinical and Academic Emergency Medicine, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia. Email: [email protected]
Robert Dunn, MBBS, FACEM, Grad Cert Mgmt, Grad Cert Lang, Director of Clinical and Academic Emergency Medicine, Royal Adelaide Hospital.

Access block and ED waiting times
233
patient throughput and decreased numbers of patientswho do not wait for treatment (DNW).10 AlthoughDirectors of many US ED believe ED overcrowdingto be a significant cause for prolonged waitingtimes,1 there are no published studies in the Medlinereferenced literature that directly examine therelationship between bed access for ED admissionsand ED waiting times. The following study examinesthis relationship during a period of industrial actionthat significantly altered hospital bed availabilityfor patients requiring admission from the ED.
The aim of the study was to determine if changes inhospital occupancy would effect ED occupancy andED waiting time performance. It was hypothesizedthat, during the period of industrial action, hospitaloccupancy would decrease due to an increase in thenumber of cancellations of elective patient admissionsand this would in turn, decrease ED admission waitingtime. As a result of these changes, it was hypothesizedthat ED occupancy would decrease and ED waitingtime performance improve.
Methods
The study was a retrospective, observational studythat compared hospital and ED data during a period ofindustrial action with a control period when there wasno industrial action.
The Queen Elizabeth Hospital is a 365 bed publictertiary teaching hospital located in the north-westernsuburbs of Adelaide. It provides a full range of adultinpatient services for approximately 250 000 people.The ED has an annual patient census of approxi-mately 36 000 of which approximately 11 000 requirehospital admission.
During a 13-day period from Thursday 22February to Tuesday 6 March 2001 inclusive, industrialaction was taken by nursing staff employed in SouthAustralian public hospitals. The action resulted in thecancellation of all elective hospital admissions (exceptfor the highest urgency cases) at the study hospitalbut did not close hospital beds for admissions from theED. The action did not directly involve the ED, ICU,HDU (high dependency unit), CCU, maternity, hospitalin the home or diagnostic services. The action wasnot intended to affect the discharge of patients fromhospital or the provision of services to hospitaloutpatients.
The performance of the ED during the period ofindustrial action (study period) was compared with a
period when industrial action was not active (controlperiod). The study period consisted of all 13 daysduring which industrial action was active and thecontrol period consisted of one 13-day period prior tothe study period and another 13-day period followingit. To minimize possible transitional effects theindustrial action might have on hospital function,eight days separated the study period from each of thecontrol periods. The first control period was fromThursday 1 to Tuesday 13 February 2001 (inclusive)and the second from Thursday 15 to Tuesday 27March 2001 (inclusive). There were an equal number ofdays of the week in the study and control periods andthere were no public or school holidays during any ofthe periods. No planned changes were made to thenormal work practices of the ED during the study.The study and control groups consisted of all patientattendances to the ED during the study and controlperiods.
Variables measured and their definitions are shownin Table 1.
Data for each ED attendance was retrieved fromthe ED patient information database. Emergencydepartment staff collected data for each patient attend-ance at the time of occurrence. All non-derived studyvariables, except the time of admission request,required completion by staff for the computerizedpatient tracking system to function properly. The timeof admission request was recorded by ED clerical staffand usually followed completion of patient review bythe admitting service.
Following ED treatment, patients were eitherdischarged or admitted. The possible departuredestinations for admitted patients were as follows:admission to the study hospital (admissions); transferto another hospital (transfers); or discharge followinga short stay admission within the ED (ED admissions).As the ED did not have a specifically designatedobservation area, ED admissions remained in the EDuntil time of discharge. The ED admission group alsocontained some hospital admissions who improvedsufficiently whilst awaiting a hospital bed to allowdischarge directly from the ED without ever beingtransferred to a hospital bed. Patients who died inthe ED and those that did not wait for treatmentwere considered as having been discharged fromthe ED.
During the study and control periods the ED had32 treatment areas designed for patient care (thetotal capacity), with 25 of these able to accommodatepatients on trolleys (the bed capacity). The treatment

R Dunn
234
areas consisted of two resuscitation bays, eightacute monitored beds, nine general cubicles, six lowacuity cubicles, one mental health room and an opencare area (able to accommodate up to six ambulantpatients).
The number of elective hospital admissions cancelledand the occupancy of the hospital for each day of thestudy were collected by hospital management. Themean number of occurrences of access block eachday was also calculated. Access block was definedaccording to the ACEM definition, where an instanceof access block occurs when a patient requiringhospital admission spends > 8 h in the ED.
In addition to patient attendance data, the numberof hours of clinical care actually provided by medicaland nursing staff for each day of the study wascalculated from the appropriate rosters. Variations tothe normal roster due to changes in staff availability,sick leave and non-rostered additional shifts workedwere included in the analysis.
Analysis of occupancy was performed for eachhour of the study and control periods using MicrosoftAccess. This analysis determined the number ofpatients in the ED at fixed times of analysis (i.e. 15:00,16:00, etc.) rather than a mean occupancy figure for
each hourly period. The number of times the totalnumber of patients in the ED equalled or exceeded thebed capacity of the ED (25) and the total capacity ofthe ED (32) were counted for the study and controlperiods.
A number of other outcome measures wereanalysed. The admission waiting time was used toquantify the degree of hospital bed availability for EDpatients. The mean ED waiting times and the numberof patients who DNW were used to measure EDperformance. Patients in Australasian triage scale(ATS) category 1 were excluded from analysis ofwaiting times because all were attended to at timeof arrival. The discharged patient treatment time andthe time to bed request were selected as measuresof the operational efficiency of the ED that wereindependent of changes in inpatient bed availability.Analysis of contributors to ED occupancy accordingto patient disposition and the phase of care was alsoperformed.
Data were analysed on a personal computer usingUnistat 4.52 for Microsoft Excel statistical software.Results are described with 95% confidence intervals(CI) unless otherwise specified. Continuous variableswere analysed using the two-tailed unpaired students
Table 1. Definitions of study variables
Measured variables Definition
Patient age Age in yearsTime of arrival Time of arrival in the EDTime seen Time first attended to by a health professionalTime of discharge Time of discharge from the EDTime of admission request Time of request for hospital admissionTriage category Urgency category according to Australasian Triage Scale11
Discharge destination Site of discharge following ED treatmentDid not wait for treatment (DNW) Patients who did not wait to be seen by a health professionalCalculated variablesWaiting time Interval between time of arrival and time seenTreatment time Interval between time seen and time of dischargeTotal time in ED Interval between time of arrival and time of discharge from the EDTime to admission request Interval between time seen and time of admission requestAdmission waiting time Interval between time of admission request and time of discharge from the EDAdmission length of stay Mean time from arrival to discharge from the ED for all admitted patientsDischarge length of stay Mean time from arrival to discharge for discharged patientsAll admissions = admissions + ED admissions + transfersED occupancy Mean number of patients in the ED
= (mean length of stay (min) X number of patients/day)/1440Hospital occupancy = number of admitted patients/total number of hospital beds*,†
*Calculation performed at midnight; †Patients awaiting hospital admission in the ED at midnight were excluded from this calculation.

Access block and ED waiting times
235
t-test unless otherwise specified. Categorical variableswere analysed using the chi-squared test. Resultswere considered statistically significant at P-values of< 0.05 and highly significant at P-values < 0.01.
Results
There were 2332 patient attendances in the controlperiod and 1133 in the study period. Collection of datawas complete for all patient variables except for thetime of bed request, which was available for 780/824(95%) of admissions. The total admission rate for thecombined study and control periods was 31.5%.
The baseline characteristics of the study andcontrol periods are shown in Table 2.
Outcome measures
A comparison of the outcome measures in the studyand control periods is shown in Table 3. There was ahighly statistically significant increase in the numberof elective cancellations and a highly significantdecrease in hospital occupancy during the study period.There were significant reductions in the admissionwaiting time, ED waiting times and the proportionof DNW without significant change in the time toadmission request and treatment time for dischargedpatients during the study period.
The mean number of admitted patients in the EDdecreased during the study period by 2.9 (11.8 vs 8.9,
Table 2. Baseline characteristics of control and study periods
Table of means Control period n = 2332
Study period n = 1133
Admissions/day 20.8 (± 4.3) 21.7 (± 5.1)ED admissions/day 5.9 (± 2.1) 4.4 (± 2.0)Transfers/day 1.4 (± 0.9) 1.5 (± 1.4)Total admissions/day 28.2 (± 5.3) 27.6 (± 5.0)Age (years) 47.1 (± 23.7) 46.2 (± 23.2)Attendances/dayATS 1 0.73 (± 1.0) 0.77 (± 1.0)ATS 2 4.3 (± 2.6) 3.3 (± 1.9)ATS 3 21.2 (± 4.7) 20.4 (± 4.2)ATS 4 53.7 (± 10) 52.9 (± 8.1)ATS 5 9.7 (± 4.5) 9.9 (± 5.8)Total 89.8 (± 12.4) 87.2 (± 9.5)Medical staff hours/day 164.8 (± 18.1) 160.4 (± 16.8)Nursing staff hours/day 232.9 (± 12.1) 230.2 (± 16.2)
Data are the mean and standard deviation. ATS, AustralasianTriage Scale.
Table 3. A comparison of the outcome measures in the study and control periods
Table of means Control period Study period Absolute difference Relative difference P-value
Hospital measuresElective cancellations/day 2.8 (± 3.5) 18.2 (± 16.2) 15.4 (8.9–22.1) 550% (317–789) < 0.001Hospital occupancy (%) 94.9 (± 2.5) 89.0 (± 1.7) −5.9 (−4.3–7.4) −6.2% (−4.5–7.8) < 0.001Access blocks/day* 14 (11–17) 9 (5–12) –5 (−2–8) −36% (−14–57) 0.003ED efficiency measuresTime to admission request (min) 182 (± 133) 185 (± 143) 3 (23–18) 1.6% (13–10) 0.78Discharge treatment time (min) 109.3 (± 106) 104.5 (± 93) −4.81 (4.0–13.6) −4.4% (3.7–12.4) 0.26ED Occupancy measuresAdmission waiting time (min) 397 (± 1403) 250 (± 286) −147 (−92–202) −37% (−23–51) < 0.001Total time in ED (min) 601 (± 340) 462 (± 256) −139 (−90–188) −23% (−15–31) < 0.001ED occupancy (no. of patients) 19.1 (± 10.8) 14.7 (± 8.1) −4.4 (−1.4–7.5) −23% (−7.3–39.3) < 0.001ED Waiting time performanceWaiting time (min) 58.5 (± 62) 37.1 (± 37) −21.4 (−17.5–25.3) −37% (−30–43) < 0.001Patients who DNW/day 3.7 (± 2.9) 2.2 (± 2.1) −1.5 (−0.2–2.8) −41% (−5–76) 0.024ATS2 (min) 8.8 (± 8.7) 4.8 (± 4.5) −4.0 (−1.2–6.8) −45% (−14–77) 0.005ATS3 (min) 25.5 (± 22.3) 21.3 (± 20.1) −4.2 (−1.0–7.3) −16% (−4–29) 0.01ATS4 (min) 72.7 (± 65) 43.0 (± 38) −29.7 (−24.4–34.9) −41% (−34–48) < 0.001ATS5 (min) 78.6 (± 78) 51.0 (± 46) −27.6 (−13.0–42.3) −35% (−17–54) < 0.001
Data are the mean and standard deviation unless otherwise specified. *Data are the median and interquartile range, comparison withMann–Whitney U-test. Comparison of waiting times (in minutes) between the preindustrial action, industrial action and postindustrial actionperiods. ATS, Australasian triage scale; DNW, patients who did not wait to be seen.

R Dunn
236
95% CI 1.7–3.7, P < 0.001), which was 68% of the totalreduction in mean ED occupancy during this period.
The mean number of patients only awaitingadmission in the ED decreased during the studyperiod by 2.2 (5.6 vs 3.4, 95% CI 1.3–2.9, P < 0.001)which was 51% of the total reduction in mean EDoccupancy during this period. The mean number ofpatients waiting to be seen decreased during the studyperiod by 1.4 (3.6 vs 2.2, 95% CI 1.1–1.6, P < 0.001),which was 33% of the reduction in mean EDoccupancy during this period. The remaining 16%of the decrease in mean ED occupancy was due tonon-statistically significant changes in the meanoccupancy of ED admissions and transfers (P = 0.51and P = 0.16, respectively).
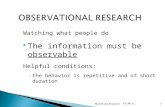
A comparison of the admission waiting time andmean ED waiting time during the study and each ofthe control periods is shown in Fig. 1. This showsthe admission waiting time and ED waiting time fellby 194 min (56%) (95% CI 131–257, P < 0.001) and29.7 min (44%) (95% CI 25.0–34.3. P < 0.001),respectively, during the period of industrial actionthen increased again by 101 min (40%) (95% CI 44–158, P = 0.0006) and 12.4 min (34%) (95% CI 8.8–16.1,P < 0.001), respectively, following the period ofindustrial action.
Occupancy
During the study period the percentage of timeED occupancy exceeded bed capacity decreased by13% (113 vs 16 occasions, 18% vs 5%, 95% CI 8.4–17.6,P < 0.001), and the percentage of time ED occupancyexceeded total ED capacity decreased by 3.7% (25 vsone occasion, 4.0% vs 0.3%, 95% CI 1.5–5.9, P < 0.001[Yates’ correction] ).
At the times when ED occupancy exceeded the bedcapacity of the ED, the mean number of admittedpatients awaiting a hospital bed was 9.8, representing39% of the bed capacity of the department. When thenumber of ED patients exceeded the total capacity ofthe ED, the mean number of admitted patients waitingfor a hospital bed was 13.5, representing 54% of thebed capacity of the department.
Discussion
This study has demonstrated that during a period ofindustrial action there was a significant reduction of5.9% in the mean hospital occupancy due to increasedcancellations of elective hospital admissions. Therewas a 37% reduction in the admission waiting time,which was the major contributor to a 23% reduction intotal ED occupancy. There was a 13% absolute and an72% relative reduction in the number of times patientnumbers exceeded the bed capacity of the department.As a result, there was a 37% reduction in the EDwaiting time and a 37% reduction in the number ofpatients who did not wait for treatment. As othercontributing factors to ED waiting time performancesuch as patient numbers and acuity, staffing numbersand work practices did not change significantlybetween study and control periods, this stronglysuggests a causal relationship between the admissionwaiting time and the ED waiting time in this model.The finding that the admission waiting time and theED waiting time both increased in the period followingcessation of the industrial action further supports thishypothesis.
During the control period, patient numbersexceeded the bed capacity of the ED 18% of the time,with 39% of the ED bed capacity devoted solely toadmitted patients awaiting a hospital bed. Duringthe study period, patient numbers exceeded the EDbed capacity only 4% of the time.
An important finding of this study is that the EDwaiting time was significantly reduced during thestudy period despite patient numbers and acuityremaining unchanged. This suggests that the EDwaiting time in this model is not primarily determinedby the demand of new attendances but is insteadlimited by the ability of the ED to discharge patientswho require hospital admission. This is importantfor the planning of optimum emergency care as itsuggests that improved bed access for ED patients isrequired if improvements in ED waiting times are to
Figure 1. Bed wait versus waiting time. (�), wait; (�), bed wait.

Access block and ED waiting times
237
occur. It also suggests that attempts to reduce thenumber of ED attendances are unlikely to improve EDwaiting times unless bed access also improves. Thisstudy also illustrates that emergency and electiveadmissions are in direct competition for hospital bedsand that there were inadequate resources in the studyhospital to accommodate the desired levels of bothelective and emergency admissions. This finding isconsistent with the results of a previous study ofbed modelling by Bagust et al. which predicts bedshortages for emergency admissions at hospitaloccupancy levels greater than 85% and regular bedcrises at occupancy levels greater than 90%.12 Duringthe control period the mean occupancy of the studyhospital was 94.9%. This further emphasizes thatED overcrowding and the dysfunction it causes arecaused by problems within the hospital, not ED. Itis important that this is acknowledged if solutions toED overcrowding are to be found. The resourcing ofhospitals, the activity of other competing hospitalservices for limited bed resources, and the prioritiesin allocation of such scarce resources need all beexamined if ED dysfunction due to overcrowding is tobe minimized.
The proposed mechanism by which the admissionwaiting time increases ED waiting time is by its effecton increasing ED occupancy. As ED occupancyincreases, the number of available treatment areasdecreases and it becomes increasingly difficult to findappropriate areas to treat new patients. In addition,the need for ED staff to provide care to admittedpatients unable to be discharged from the EDreduces staff availability to attend to new patients. Thisresults in increased ED waiting times which itselfsignificantly contributes to ED overcrowding. In thismodel, a decrease in mean hospital occupancy of only5.9% (equating to an additional 21 beds available forED patients) resulted in a 37% reduction in EDwaiting times.
The ED waiting time causes avoidable delays inpatient treatment and has the potential to significantlyalter ultimate patient outcomes for some patients. Thisis particularly of concern when waiting times becomeexcessively prolonged and affect high triage prioritycases. Given that there are approximately 36 000attendances to the study ED each year, a sustaineddecrease in the mean waiting time of 21.4 min (asoccurred during the study period) would reduce thetotal delay to patient care by approximately 13 000 heach year — the equivalent of 7.2 years of work forthe average Australian! Considering that relatives
or carers accompany many patients, the potentialsavings in time by modest improvements in accessblock must be even greater.
Although ED waiting times do not necessarycorrelate to the overall patient perception of thequality of care received this has previously beenreported as a significant factor, particularly for lessurgent cases.13,14 Apart from decreasing delays topatient care, decreasing ED occupancy is likely toalso improve the availability of staff to attend to theneeds of their patients and therefore improve otheraspects of patient care not measured by this study.
Apart from decreasing delays to treatment, shortertimes in the ED for admitted patients are associatedwith a decreased length of hospital stay and lowertotal cost of hospital treatment. Krochmal et al. foundthat patients who stayed in the ED for greater than24 h prior to hospital admission had a 10–13%increase in their hospital stay compared with other EDadmissions,15 whilst Sixsmith showed that patientswho waited for more that 18 h in the ED had anincreased length of hospital stay of between 0.7and 1.1 days.16 A more recent Australian study byRichardson has also demonstrated a 20% (4.9 vs 4.1days) increase in hospital length of stay of patientswho spend more than eight hours in the ED prior tohospital admission.17
Given the extent of access block across a largenumber of health systems, the social and economiccosts of access block must truly be massive.
The methodological limitations of this study relateprimarily to unmeasured variability in factors thatcould influence the waiting time performance of theED between the study and control periods. However,as the discharged patient treatment time and the timeto admission request did not change between the studyand control periods, this suggests that departmentalefficiency did not change significantly throughout thestudy. Also, as worsening bed access and ED waitingtimes recurred following the industrial action, it isunlikely that changes in work practices or otherunmeasured factors were responsible for the changein waiting time performance during the study period.
Despite the methodological limitations of thisobservational study, it is likely to be the highest levelof evidence achievable given the low probability thata randomized trial of differing levels of bed accesscould ever be conducted.
Although the author believes the characteristicsof the study ED to be typical of many other urbanteaching hospitals in Australia, the results of this

R Dunn
238
study may not be applicable to some other ED. Factorssuch as staffing profile, work practices and designconsiderations may be the prime determinants of EDfunction for some hospitals. However, in a surveyconducted by Derlet of Directors of USA teachinghospital ED, access block was rated as a factorcontributing to ED overcrowding by 88%, considereda major factor by 52% and occurred daily in 51% ofthe ED surveyed.18 Given that ED overcrowdinghas been reported to occur in 96% of ED that servepopulations of 250 000 or more,1 the findings of thisstudy are likely to be broadly applicable to otherteaching hospital ED.
It should also be noted that the study wasconducted during late summer when access blockis usually much less than during the winter months.Therefore, the effect of access block on ED waitingtimes may have been underestimated by this study.
Further work is required to determine if changesin bed access have similar effects in other models andto analyse which of the measures of access block andED overcrowding are the most useful in predictingED dysfunction.
Conclusions
During a period of industrial action there was 5.9%reduction in hospital occupancy, a 23% reduction inthe mean occupancy of the ED and a 72% reduction inthe frequency in which the ED was required to operatein excess of its bed capacity. Fifty-one per cent of thereduction in ED occupancy was due to decreasednumbers of patients awaiting admission from the ED.There was a 37% reduction in the mean waiting timeand improvements in waiting times for ATS categories2–5. As other factors expected to effect the ED waitingtime did not change during the study period, modestimprovements in bed access resulted in highlysignificant reductions in ED waiting times. Emergencydepartment overcrowding due to large numbers ofadmitted patients awaiting hospital admission is amajor cause of ED dysfunction.
Accepted 13 January 2003
References
1. Derlet R, Richards J, Kravitz R. Frequent overcrowding in USemergency departments. Acad. Emerg. Med. 2001; 8: 151–5.
2. Graff L. Overcrowding in the ED: an international symptom ofhealth care system failure. Am. J. Emerg. Med. 1999; 17: 208–9.
3. Shih FY, Ma MH, Chen SC et al. ED overcrowding in Taiwan:facts and strategies. Am. J. Emerg. Med. 1999; 17: 198–202.
4. Geraci E. [The overcrowding of the emergency room ofhospitals.] G. Ital. Cardiol. 1993; 23: 219.
5. Gaudry PL. Council highlights. Your Direction, September2000, Vol. 1, No. 2: p. 3.
6. Richardson D. Access block and emergency physician health — arecipe for early retirement. Proceedings of annual scientificmeeting of the ACEM and ASEM; Oct 2001, Blackwell, 2002.
7. Vinen J. Access block — strategies for measurement andresearch. Proceedings of annual scientific meeting of the ACEMand ASEM; Oct 2001, Blackwell, 2002.
8. Cameron P. Presidents message. Your Direction, April 2001,Vol. 2, No. 1: pp. 2–3.
9. Weiss SJ, Arndahl J, Ernst AA et al. Development of a sitesampling form for evaluation of ED overcrowding. Acad.Emerg. Med. 2001; 8: 577b–8b.
10. Bazarian JJ, Schneider SM, Newman VJ et al. Do admittedpatients held in the emergency department impact thethroughput of treat-and-release patients? Acad. Emerg. Med.1996; 3: 1113–18.
11. Australasian College for Emergency Medicine. TheAustralasian Triage Scale. Policy Document, PO 6 Nov, 1993.
12. Bagust A, Place M, Posnett JW. Dynamics of bed use inaccommodating emergency admissions: a stochastic simulationmodel. BMJ 1999; 319: 155–8.
13. Bursch B, Beezy J, Shaw R. Emergency departmentsatisfaction: what matters most? Ann. Emerg. Med. 1993;22: 586–91.
14. Holden D, Smart D. Adding value to the patient experience inemergency medicine: What features of the emergencydepartment visit are most important to patients? Emerg. Med.1999; 11: 3–8.
15. Krochmal P, Riley PA. Increased health care costs associatedwith ED overcrowding. Am. J. Emerg. Med. 1994; 12: 265–6.
16. Sixsmith DM, Rosenberg C, Silber S et al. Excess length of stayin the ED increases inpatient length of stay. Acad. Emerg. Med.2000; 7: 544. [Abstract].
17. Richardson DB. The access-block effect: relationship betweendelay to reaching an inpatient bed and inpatient length of stay.MJA 2002; 177: 492–5.
18. Derlet RW, Richards JR. Overcrowding in academic emergencydepartments Acad. Emerg. Med. 1999; 6: 404. [Abstract].