
Recurrent Clostridium difficile infection: A review of risk factors, treatments, and outcomes
8
REVIEW Recurrent Clostridium difficile infection: A review of risk factors, treatments, and outcomes Stuart Johnson a,b, * a Infectious Disease Section, Loyola University Medical Center, Stritch School of Medicine, Maywood, IL 60153, USA b Hines Veterans Affairs Hospital, Hines, IL, USA Accepted 24 March 2009 Available online 5 April 2009 KEYWORDS Clostridum difficile; Vancomycin; Metronidazole; Diarrhea Summary Episodes of recurrent Clostridium difficile infection (CDI) are difficult to treat for several reasons. Foremost, data are lacking to support any particular treatment strategy. In addition, treatment of recurrent episodes is not always successful, and repeated, prolonged treatment is often necessary. Identification of subgroups at risk for recurrent CDI may aid in diagnosing and treating these patients. Two likely mechanistic factors increasing the risk of re- current CDI are an inadequate immune response to C. difficile toxins and persistent disruption of the normal colonic flora. Important epidemiologic risk factors include advanced age, contin- uation of other antibiotics, and prolonged hospital stays. Current guidelines recommend that the first recurrent episode be treated with the same agent (i.e., metronidazole or vancomycin) used for the index episode. However, if the first recurrence is characterized as severe, vanco- mycin should be used. A reasonable strategy for managing a subsequent episode involves ta- pering followed by pulsed doses of vancomycin. Other potentially effective strategies for recurrent CDI include vancomycin with adjunctive treatments, such as Saccharomyces boular- dii, rifaximin ‘‘chaser’’ therapy after vancomycin, nitazoxanide, fecal transplantation, and in- travenous immunoglobulin. New treatment agents that are active against C. difficile, but spare critical components of the normal flora, may decrease the incidence of recurrent CDI. Published by Elsevier Ltd on behalf of The British Infection Society. Introduction A first episode of Clostridium difficile infection (CDI) is fol- lowed by a symptomatic recurrence in approximately 19e20% of patients affected, following the resolution of the initial infection. 1 In one study of 163 patients who already had at least one recurrence, the risk of a subse- quent recurrence was 45%. 2 Earlier, a small French study * Infectious Disease Section, Loyola University Medical Center, 2160 South First Avenue, Fahey Center (Bldg. 54), Room 149, Maywood, IL 60153, USA. Tel.: þ1 708 216 3232; fax: þ1 708 216 8198. E-mail address: [email protected] 0163-4453/$36 Published by Elsevier Ltd on behalf of The British Infection Society. doi:10.1016/j.jinf.2009.03.010 www.elsevierhealth.com/journals/jinf Journal of Infection (2009) 58, 403e410
-
Upload
stuart-johnson -
Category
Documents
-
view
218 -
download
2
Transcript of Recurrent Clostridium difficile infection: A review of risk factors, treatments, and outcomes

Journal of Infection (2009) 58, 403e410
www.elsevierhealth.com/journals/jinf
REVIEW
Recurrent Clostridium difficile infection: A reviewof risk factors, treatments, and outcomes
Stuart Johnson a,b,*
a Infectious Disease Section, Loyola University Medical Center, Stritch School of Medicine, Maywood, IL 60153, USAb Hines Veterans Affairs Hospital, Hines, IL, USA
Accepted 24 March 2009Available online 5 April 2009
KEYWORDSClostridum difficile;Vancomycin;Metronidazole;Diarrhea
* Infectious Disease Section, Loyola2160 South First Avenue, Fahey CeMaywood, IL 60153, USA. Tel.:þ1 708 2
E-mail address: [email protected]
0163-4453/$36 Published by Elsevier Ldoi:10.1016/j.jinf.2009.03.010
Summary Episodes of recurrent Clostridium difficile infection (CDI) are difficult to treat forseveral reasons. Foremost, data are lacking to support any particular treatment strategy. Inaddition, treatment of recurrent episodes is not always successful, and repeated, prolongedtreatment is often necessary. Identification of subgroups at risk for recurrent CDI may aid indiagnosing and treating these patients. Two likely mechanistic factors increasing the risk of re-current CDI are an inadequate immune response to C. difficile toxins and persistent disruptionof the normal colonic flora. Important epidemiologic risk factors include advanced age, contin-uation of other antibiotics, and prolonged hospital stays. Current guidelines recommend thatthe first recurrent episode be treated with the same agent (i.e., metronidazole or vancomycin)used for the index episode. However, if the first recurrence is characterized as severe, vanco-mycin should be used. A reasonable strategy for managing a subsequent episode involves ta-pering followed by pulsed doses of vancomycin. Other potentially effective strategies forrecurrent CDI include vancomycin with adjunctive treatments, such as Saccharomyces boular-dii, rifaximin ‘‘chaser’’ therapy after vancomycin, nitazoxanide, fecal transplantation, and in-travenous immunoglobulin. New treatment agents that are active against C. difficile, but sparecritical components of the normal flora, may decrease the incidence of recurrent CDI.Published by Elsevier Ltd on behalf of The British Infection Society.
University Medical Center,nter (Bldg. 54), Room 149,16 3232; fax:þ1 708 216 8198.u
td on behalf of The British Infect
Introduction
A first episode of Clostridium difficile infection (CDI) is fol-lowed by a symptomatic recurrence in approximately19e20% of patients affected, following the resolution ofthe initial infection.1 In one study of 163 patients whoalready had at least one recurrence, the risk of a subse-quent recurrence was 45%.2 Earlier, a small French study
ion Society.

Table 1 Important risk factors for the development ofrecurrent Clostridium difficile infection.
- Inadequate antitoxin antibody response- Persistent disruption of the colonic flora- Advanced age- Continuation of non-C. difficile antimicrobial therapy
following a first episode of CDI- Long hospital stays- Concomitant receipt of antacid medications
CDI, Clostridium difficile infection.
404 S. Johnson
of 93 patients with recurrent CDI found that 61% had a singlerecurrence, 27% had two subsequent recurrences, and 12%had more than two subsequent recurrences.3 Unfortu-nately, such episodes may continue to recur over severalmonths or years.
Recurrent CDI occurs either due to relapse (i.e., endog-enous persistence of the same strain of C. difficile) or rein-fection (i.e., acquisition of a new strain of C. difficile froman exogenous source). The relative frequency of eachmechanism of recurrence has not been well described;however, in five published reports, 33%e75% of cases of re-current CDI were attributed to infection with a newstrain.3e7 The mean time to relapse with the same strainis typically much shorter than the mean time to reoccur-rence with a new strain (i.e., reinfection). According toone study, the mean time between the end of therapy forthe prior episode and relapse was 14.5 days, whereastime to reinfection was 42.5 days.4 The impact of recurrentCDI on the healthcare system is significant because the de-velopment of recurrent CDI increases the average length ofhospitalization and cost of treatment.8 Furthermore, pa-tients often become frustrated by the consistent reappear-ance of symptoms and the repeated need for treatment.
Risk factors
The prompt diagnosis and treatment of patients with CDImay be facilitated by recognition of populations at risk.Traditionally, the major risk factors for developing health-care-associated CDI have included treatment with broad-spectrum antibiotics and the subsequent disruption ofnormal colonic microflora followed by exposure to C. diffi-cile spores from hospital environmental surfaces, infectedroommates, or hand carriage by hospital staff. Clindamycin,cephalosporins, and fluoroquinolones have been the antibi-otics most frequently implicated, but chemotherapeuticagents are also occasionally implicated. Proton pump inhib-itors have been implicated in some studies but not others,but these agents are most likely much less important thanantibiotics.9 In addition, several host factors are probablyimportant, including low antitoxin antibody levels, comor-bid conditions, and advanced age.10,11 However, new at-risk populations, including children and peripartum women,have been recognized.12e16 For example, in a study of 250children between 5 and 12 years of age who developed diar-rhea while they were hospitalized in India, 7.2% had stoolsamples that tested positive for C. difficile.14 Another studyof children with diarrhea who presented to a large pediatricemergency department in Seattle found C. difficile cyto-toxin in 6.7% of the 372 children tested; the mean age ofC. difficile-positive patients was 19 months, and there wasa strong association between the recent use of antibioticsand the presence of the toxin.17 In addition, a report fromthe US Centers for Disease Control and Prevention describedsevere CDI in 10 peripartum women from four states; 50% ofthese women experienced a relapse.12
The patient’s inability to develop an adequate immuneresponse may be one of the major reasons for the de-velopment of recurrent CDI.18e20 In one study of 40 patients,those who experienced relapsing disease had significantlylower levels of toxin A-specific IgG (p Z .033) and specificfecal IgA (p Z .025) than patients who did not experience
relapse.20 A later study found evidence suggesting an anam-nestic response in patients with asymptomatic carriage of C.difficile, based on high levels of toxin A-specific IgG and rap-idly increasing levels of specific IgG antibodies following col-onization.18 Later, the same group of investigators set out toconfirm if the host response to toxin A during the initial epi-sode of CDI could prevent the development of recurrent CDIand found that increased levels of toxin A-specific IgM andIgG were associated with a substantially reduced risk ofrecurrent CDI.19
Another likely mechanistic factor increasing the risk ofrecurrent CDI is persistent disruption of the normal colonicflora. A recent study reported that decreased overalldiversity of the gut microbiota was associated with re-current CDI.21 Compared with controls, the fecal micro-biome of patients with recurrent CDI was consistently andsignificantly decreased in phylotype richness.21
Other epidemiologic risk factors for recurrent CDI havealso been described. In a retrospective study of hospital-ized patients from Quebec, a group of Canadian investiga-tors reported that independent predictors of recurrenceincluded age of 65 years or older, acquisition of CDI duringa hospital stay, and, to a lesser degree, length of hospitalstay.22 McFarland et al. also found that increased age, aswell as decreased quality-of-life scores, were associatedwith a higher risk of recurrent CDI.23 Most recently, Gareyet al. conducted a meta-analysis of 12 studies that assessedrisk factors for CDI and found that continued use of non-C.difficile antibiotics after diagnosis, concomitant receipt ofantacid medication, and older age were significantly associ-ated with recurrent CDI.24 Important and consistently re-ported risk factors for recurrent CDI are summarized inTable 1.
In patients with recurrent CDI, the documentation ofreinfection as opposed to relapse may be of interestbecause the incidence of reinfection may be reduced onthe basis of several infection control procedures, such ashandwashing with soap and water, rigid environmentaldecontamination, and the use of prompt enteric isolationprecautions.4 To reduce the transmission of C. difficilespores, environmental disinfection with 10% sodium hypo-chlorite is recommended to remove spores from surfaces.25
Optimally, the reduction of CDI outbreaks involves theintegration of several distinct approaches that alsoinvolve restricting antimicrobial use, reducing exposure toC. difficile, and interrupting C. difficile transmission.26
Other strategies that may reduce recurrent CDI includeearly identification of recurrence and use of appropriatetreatments.27
Treatment of Recurrent Clostridium difficile Infection 405
McFarland et al. reported results from a referral study of209 patients with recurrent CDI (average 2.6� 1.9 prior ep-isodes at enrollment) conducted between 1993 and 1996,which found that the severity of recurrent CDI did not pro-gressively increase as the number of episodes increased.23
A more recent study conducted in the setting of a multiplehospital outbreak in Quebec caused by a hypervirulentstrain has shown that serious complications, includingshock, toxic megacolon, colectomy, and death, were asso-ciated with recurrent CDI in 11% of patients who experi-enced a first-time recurrence of CDI, a rate higher thanpreviously reported.28
Treatment
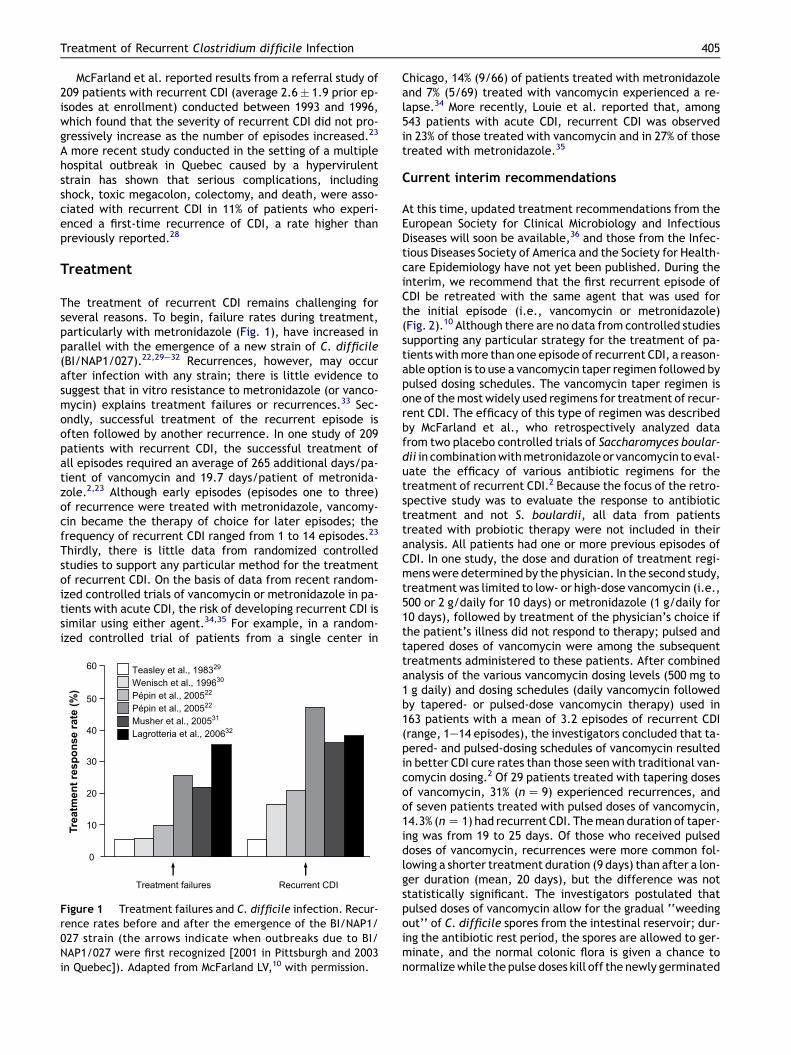
The treatment of recurrent CDI remains challenging forseveral reasons. To begin, failure rates during treatment,particularly with metronidazole (Fig. 1), have increased inparallel with the emergence of a new strain of C. difficile(BI/NAP1/027).22,29e32 Recurrences, however, may occurafter infection with any strain; there is little evidence tosuggest that in vitro resistance to metronidazole (or vanco-mycin) explains treatment failures or recurrences.33 Sec-ondly, successful treatment of the recurrent episode isoften followed by another recurrence. In one study of 209patients with recurrent CDI, the successful treatment ofall episodes required an average of 265 additional days/pa-tient of vancomycin and 19.7 days/patient of metronida-zole.2,23 Although early episodes (episodes one to three)of recurrence were treated with metronidazole, vancomy-cin became the therapy of choice for later episodes; thefrequency of recurrent CDI ranged from 1 to 14 episodes.23
Thirdly, there is little data from randomized controlledstudies to support any particular method for the treatmentof recurrent CDI. On the basis of data from recent random-ized controlled trials of vancomycin or metronidazole in pa-tients with acute CDI, the risk of developing recurrent CDI issimilar using either agent.34,35 For example, in a random-ized controlled trial of patients from a single center in
Treatment failures
Teasley et al., 198329
Wenisch et al., 199630
Pépin et al., 200522
Pépin et al., 200522
Musher et al., 200531
Lagrotteria et al., 200632
60
50
40
30
20
10
0
Recurrent CDI
Treatm
en
t resp
on
se rate (%
)
Figure 1 Treatment failures and C. difficile infection. Recur-rence rates before and after the emergence of the BI/NAP1/027 strain (the arrows indicate when outbreaks due to BI/NAP1/027 were first recognized [2001 in Pittsburgh and 2003in Quebec]). Adapted from McFarland LV,10 with permission.
Chicago, 14% (9/66) of patients treated with metronidazoleand 7% (5/69) treated with vancomycin experienced a re-lapse.34 More recently, Louie et al. reported that, among543 patients with acute CDI, recurrent CDI was observedin 23% of those treated with vancomycin and in 27% of thosetreated with metronidazole.35
Current interim recommendations
At this time, updated treatment recommendations from theEuropean Society for Clinical Microbiology and InfectiousDiseases will soon be available,36 and those from the Infec-tious Diseases Society of America and the Society for Health-care Epidemiology have not yet been published. During theinterim, we recommend that the first recurrent episode ofCDI be retreated with the same agent that was used forthe initial episode (i.e., vancomycin or metronidazole)(Fig. 2).10 Although there are no data from controlled studiessupporting any particular strategy for the treatment of pa-tients with more than one episode of recurrent CDI, a reason-able option is to use a vancomycin taper regimen followed bypulsed dosing schedules. The vancomycin taper regimen isone of the most widely used regimens for treatment of recur-rent CDI. The efficacy of this type of regimen was describedby McFarland et al., who retrospectively analyzed datafrom two placebo controlled trials of Saccharomyces boular-dii in combination with metronidazole or vancomycin to eval-uate the efficacy of various antibiotic regimens for thetreatment of recurrent CDI.2 Because the focus of the retro-spective study was to evaluate the response to antibiotictreatment and not S. boulardii, all data from patientstreated with probiotic therapy were not included in theiranalysis. All patients had one or more previous episodes ofCDI. In one study, the dose and duration of treatment regi-mens were determined by the physician. In the second study,treatment was limited to low- or high-dose vancomycin (i.e.,500 or 2 g/daily for 10 days) or metronidazole (1 g/daily for10 days), followed by treatment of the physician’s choice ifthe patient’s illness did not respond to therapy; pulsed andtapered doses of vancomycin were among the subsequenttreatments administered to these patients. After combinedanalysis of the various vancomycin dosing levels (500 mg to1 g daily) and dosing schedules (daily vancomycin followedby tapered- or pulsed-dose vancomycin therapy) used in163 patients with a mean of 3.2 episodes of recurrent CDI(range, 1e14 episodes), the investigators concluded that ta-pered- and pulsed-dosing schedules of vancomycin resultedin better CDI cure rates than those seen with traditional van-comycin dosing.2 Of 29 patients treated with tapering dosesof vancomycin, 31% (n Z 9) experienced recurrences, andof seven patients treated with pulsed doses of vancomycin,14.3% (n Z 1) had recurrent CDI. The mean duration of taper-ing was from 19 to 25 days. Of those who received pulseddoses of vancomycin, recurrences were more common fol-lowing a shorter treatment duration (9 days) than after a lon-ger duration (mean, 20 days), but the difference was notstatistically significant. The investigators postulated thatpulsed doses of vancomycin allow for the gradual ‘‘weedingout’’ of C. difficile spores from the intestinal reservoir; dur-ing the antibiotic rest period, the spores are allowed to ger-minate, and the normal colonic flora is given a chance tonormalize while the pulse doses kill off the newly germinated

Figure 2 Suggested approach to treatment of patients with recurrent Clostridium difficile infection (CDI). All regimens listed,with the exception of intravenous immunoglobulin (IVIG), are given orally. IVIG should be considered only if other options fail(see text). If CDI still recurs after all of the suggested approaches have been tried, consider a vancomycin maintenance regimenat the lowest dose possible (e.g., 125 mg daily or twice daily).
406 S. Johnson
vegetative cells.2 Repeated, prolonged courses of metroni-dazole are not recommended because of the increased riskof neurotoxicity.37
If episodes of recurrent CDI continue, other treatmentoptions include alternative antibiotics, probiotics, immu-nologic approaches, fecal reconstitution, and toxin-bindingagents (Fig. 2). Two other antibiotic options include rifax-min and nitazoxanide, which are approved in the UnitedStates for other indications but are still being evaluatedfor CDI treatment. Rifaximin, a poorly absorbed rifamycinderivative, has been found to reduce the risk of CDI relapsein hamsters infected with C. difficile.38 Hamsters weretreated for five days with either vancomycin or rifaximin24 h following infection with one of two strains of C. diffi-cile (a reference strain, VPI 10463 or an epidemic strain,BI17). Following one month of follow-up in animals infectedwith the VPI 10463 strain, significantly more vancomycin-treated animals developed recurrent CDI (75%) than didanimals who received rifaximin (0%) (p< 0.01). In one un-controlled clinical study, the use of a rifaximin ‘‘chaser’’was evaluated in eight female patients with four to eightprior episodes of CDI. Prior regimens included metronida-zole, vancomycin with or without rifampin or S. boulardii,and vancomycin administered in pulsed or tapering doses.Rifaximin was started following the completion of the lasttreatment for CDI but before the recurrence of symptoms.This strategy was highly effective in this very challenginggroup of patients; the use of a rifaximin ‘‘chaser’’ pre-vented recurrence in seven patients. Although one patient
had a symptomatic recurrence, the patient was successfullytreated with a second course of rifaximin.39 A C. difficileisolate with a high minimum inhibitory concentration to ri-faximin was recovered from the stool of this patient follow-ing the second rifaximin course; resistance to rifaximin atthe start of treatment is a potential concern for the effi-cacy of this approach. Because the systemic absorption ofrifaximin is very low, it is associated with very high fecalconcentrations and has an excellent safety profile.39,40 Fur-thermore, there are minimal changes in the fecal flora dur-ing treatment with rifaximin. Further randomized studies ofthis approach with susceptibility testing of C. difficileisolates are warranted. Resistance to rifaximin41 and therelated drug, rifampin,42 may be a limiting factor for thisapproach as increased rates of resistance to thesecompounds have recently been reported in vitro,41,42 par-ticularly among the BI/NAP1/027 epidemic strain.42 Nita-zoxanide is another clinically available agent that mayalso be useful for patients with recurrences after treatmentwith metronidazole.43 In addition, one small study of recur-rent CDI treatment advocated rifampin as adjunctive ther-apy with vancomycin.44 Rifampin as adjunctive therapywith metronidazole is not recommended.32
The best studied probiotic strategy for the treatment ofrecurrent CDI involves S. boulardii, a non-pathogenic yeast.The goal of using biotherapy with S. boulardii or other pro-biotics is to restore colonization resistance (i.e., the hostdefense mechanism of the normal flora). The combineduse of S. boulardii with vancomycin was evaluated during

Treatment of Recurrent Clostridium difficile Infection 407
an exploratory analysis of data from a double-blind, pla-cebo-controlled trial of patients with recurrent CDI.45,46 Pa-tients were randomly assigned to 28-day treatment with S.boulardii (1 g daily) or placebo on day 7 of antibiotic treat-ment with high-dose vancomycin, low-dose vancomycin, ormetronidazole. Neither the 10-day course of low-dose van-comycin nor metronidazole was effective, so the investiga-tors focused their analysis on the 32 patients who receivedhigh-dose vancomycin with or without S. boulardii. In thehigh-dose vancomycin patients, the recurrence rate de-creased from 50% (7/14) to 16.7% (3/18) with the additionof S. boulardii, and this result approached statistical signif-icance (p Z .05). The number of subsequent recurrenceswas lower as well; the seven patients who only receivedvancomycin experienced one to two subsequent recur-rences, whereas the three patients given S. boulardiieach had only one subsequent recurrence (p Z .03). Useof S. boulardii had no effect when combined with low-dose vancomycin or metronidazole. An earlier study foundthat standard antibiotic therapy (metronidazole or vanco-mycin) combined with S. boulardii for primary CDI resultedin a lower relative risk of recurrent CDI than that seen withstandard antibiotic therapy plus placebo, also suggestingthat combination antibiotic and S. boulardii therapy maybe more effective than standard therapy alone for the ini-tial episode of CDI.47 It has been postulated that S. boular-dii may exert its effect by inactivation of C. difficile toxinreceptor sites through binding of S. boulardii protease.45
One potential concern with S. boulardii, particularly in im-munocompromised patients, is the risk of fungemia.48 Lac-tobacillus spp. have also been evaluated for use inrecurrent CDI. A two-year, double-blind, placebo-con-trolled study of 21 patients with recurrent CDI comparedthe use of metronidazole alone (400 mg three times dailyfor 10 days) with the same course of 10-day metronidazolewith Lactobacillus spp. once daily for 38 days. Twenty pa-tients were considered cured clinically, and there was nosignificant difference between the lactobacilli group andthe placebo group with regard to bacteriological cure.49
There have been several small reports of the use ofpassive vaccination with intravenous immunoglobulin (IVIG)in subgroups of patients with multiple recurrences ofCDI.50,51 In one such study that reviewed all cases of pa-tients with recurrent CDI treated within a two-year periodat a university teaching hospital in Leeds, England, theuse of IVIG was found to be useful among patients with in-tractable, moderate to severe CDI. In this review of 580 pa-tients with protracted or recurrent CDI, five patients weregiven from one to six doses of IVIG 300e500 mg/kg (mostcommon dose was 400 mg/kg) after having diarrhea fora mean duration of 50 days (range, 45e64) and a medianof three therapeutic courses of antibiotics before IVIG.Treatments administered prior to IVIG included metronida-zole and vancomycin in four patients. Of these four pa-tients, one also received rifampin, and the other receivedS. boulardii. The fifth patient received vancomycin or an in-vestigational treatment (GT160-246 [tolevamer]). Althoughthree patients had no further recurrence within threemonths, one patient experienced recurrence of symptomsat six weeks, and one patient died of intractable CDI.50 Ear-lier, Beales reported that four patients with recurrent CDIwere successfully treated using two doses of IVIG
(400 mg/kg) and a tapering dose of vancomycin.51 In theo-retical support of this approach, it has been reported thatasymptomatic carriers of C. difficile have serum antibodylevels of IgG antitoxin A that are threefold higher thanthose in patients with CDI (p< 0.001), and patients withhigh serum IgG antitoxin A antibody levels during a first ep-isode of CDI are 48-fold less likely to develop recurrent CDIthan patients who have lower levels of serum antitoxin an-tibodies.18,19 Despite the lack of significant data supportingthe use of IVIG in patients with fulminant CDI, this treat-ment is often used in these patients. In summary, passiveimmunization, although theoretically attractive, is notwell studied. Until more data become available and a hy-per-immune preparation of IVIG becomes available, thisexpensive and resource-limited approach should only beconsidered if other options are not effective. An active vac-cination approach has also been explored. For example,three patients with recurrent CDI were administered a C.difficile vaccine, which included toxoid preparations ofboth toxin A and toxin B, while vancomycin was contin-ued.52 None of the patients had a subsequent CDI episodeafter the vancomycin was stopped, and two patients devel-oped serum neutralizing antibody responses. The C. diffi-cile vaccine is currently being studied further in clinicaltrials of healthy volunteers.
Fecal reconstitution is a novel alternative for recurrentCDI and appears to be a highly effective treatment. Ina case series of 18 patients treated with healthy donor stoolvia nasogastric tube at a single center in Minnesota, 15patients were recurrence-free at 90 days, two patients diedof unrelated causes, and one patient experienced a re-currence.53 Because the fundamental challenge in treatingCDI is not the presence of the pathogenic organism per sebut rather the absence of the healthy flora, the restorationof bacterial homeostasis was anticipated to resolve infec-tion caused by uncontrolled growth of C. difficile. The in-vestigators reported several advantages associated withstool transplantation, including breaking the cycle of re-peated antimicrobial use, preventing the emergence of re-sistant strains, avoiding the possibility of allergic reactions,and reducing drug-related treatment costs.53
Cholestyramine, an anion-exchange resin that wasthought to bind C. difficile toxins, has also been used as anadjunct to conventional antibiotic therapy for CDI. Althoughearly case studies54,55 found that extended courses ofcholestyramine were effective in controlling recurrent CDIin children and a cancer patient, the potential affinity ofcholestyramine for vancomycin and the relative lack of affin-ity for C. difficile toxins translate into limited clinical effi-cacy. During an early study comparing tolevamer withcholestyramine, tolevamer (a novel non-antibiotic toxinbinder) exhibited a 16-fold greater ability to block toxinAemediated enterotoxic activity in rats, and tolevamerwas also significantly more effective than cholestyraminein protecting hamsters from C. difficile-related death.56
Other ongoing studies are evaluating tolevamer, a newmacrocycle called OPT-80 (which appears to have a narrowspectrum of activity that may translate to fewer cases ofrecurrent CDI57), a human monoclonal antibody to C. diffi-cile toxins, and nitazoxanide (an antiparasitic agent). Ac-cording to data from a study of OPT-80 versus vancomycinin patients with CDI,58 the use of OPT-80 was not associated

Figure 3 Clinical course of recurrent Clostridium difficile infection in an 81-year-old woman.
408 S. Johnson
with significant deceases in fecal flora, whereas fecalcounts of Bacteroides fragilis were significantly (p Z .03)decreased at day 10 in patients treated with vancomycin.59
Clinical course of recurrent CDI: case study
The challenging nature of managing patients with recurrentCDI may be illustrated by this case study of an 81-year-oldfemale with atrial fibrillation and end-stage renal disease inwhom hemodialysis was recently initiated. In April, she wastreated with cephalexin for cellulitis at the site of herrecently placed arteriovenous fistula. She was hospitalizedon April 29 with her first CDI episode, and she received a10-day course of metronidazole (Fig. 3). Her symptomsimproved with metronidazole therapy, and she was dis-charged to home. On May 13, she was readmitted for con-gestive heart failure and pneumonia, for which shereceived treatment with moxifloxacin. She was hospitalizedagain on May 28 with 10e15 watery stools per day; despitea negative stool toxin assay, empiric treatment with metro-nidazole was started again with improvement in symptoms.
After completing a 14-day course of metronidazole, shehad another recurrence of symptoms and was hospitalizedfor a fourth time. She now had 15e16 watery stools per day,abdominal tenderness on examination, and a leukocytecount of 15,300 cells/mm3. Her stool toxin assay was posi-tive, and she was treated with oral vancomycin. Six days af-ter completing the vancomycin course (July 22), diarrheastarted again. She was seen in clinic on July 27, and a stoolspecimen was sent for toxin testing and anaerobic cultureon selective C. difficile agar. Vancomycin was resumed;when she was asymptomatic, vancomycin was stopped (Au-gust 24) and rifaximin was started per the empiric ‘‘chaser’’protocol.35 She was seen in clinic one week after finishing therifaximin course (September 14), and a stool specimen wassent for toxin and culture again. Less than one week afterthat visit, she had a large incontinent diarrheal episode;she called the clinic, and another two-week course of rifax-imin was started on September 19. She was seen in clinicagain on October 12, at which time she had no further diar-rhea.Two surveillance specimens sent from the dialysis clinicin December were negative, and she was not retreated.
This case demonstrates several important clinical pointswith recurrent CDI. First, recurrent episodes can be severeand require rehospitalization, as was the case for the first
three episodes. Secondly, the toxin immunoassays arerelatively insensitive (the toxin assay used at the timewas a toxin A immunoassay). The stool toxin assay wasnegative on several occasions when she had a clear symp-tomatic relapse. For instance, a stool specimen obtained atthe start of the fourth CDI episode was toxin-negative butshowed heavy growth of C. difficile when cultured in ourresearch laboratory. Finally, even though we obtaineda stool specimen following her last rifaximin episode, thiswas done for investigative purposes. As can be seen inFig. 3, the stool was both toxin- and culture-positive, yetshe did not experience a clinical relapse. It is likely that pa-tients will be colonized with C. difficile for some time aftersuccessful treatment; therefore, use of the so-called ‘‘test-of cure’’ assays is discouraged. Considering her history,a compulsive practitioner might have been tempted to re-treat the patient at this point (because of a positive post-treatment assay), but this would have been the wrongclinical decision.
Conclusion
In summary, recurrent CDI is a frustrating condition that isnot only difficult to treat but may affect patients formonths or even years. The selection of treatment for theinitial recurrent CDI episode should mirror that chosenduring the index episode. For multiple recurrences of CDI,tapering followed by pulsed doses of vancomycin is a rea-sonable strategy. Other options include antibiotics (such asrifaximin used as a post-vancomycin ‘‘chaser’’), nitazox-anide, probiotic therapy (employing S. boulardii), the useof IVIG, or fecal transplantation. Clearly, the disappointingefficacy of most treatments in patients with recurrent CDIsuggests there is an ongoing need for continued researchto improve outcomes for these patients.
Acknowledgments
Dr. Johnson receives grant support from the United StatesDepartment of Veterans Affairs Research Service andViroPharma Incorporated; Dr. Johnson has also served onthe advisory boards of Genzyme Corporation; Salix Phar-maceuticals, Inc.; Acambis; Optimer Pharmaceuticals, Inc.;Replidyne, Inc.; and BD DiagnosticseGeneOhm.

Treatment of Recurrent Clostridium difficile Infection 409
The author thanks Marie Bialek, PharmD, and RobertMichael Healthcare Alliance LLC for assistance in preparingthis article. This work was supported by a grant fromViroPharma Incorporated.
References
1. Aslam S, Hamill RJ, Musher DM. Treatment of Clostridium dif-ficile-associated disease: old therapies and new strategies.Lancet Infect Dis 2005;5:549e57.
2. McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle:treatment strategies for 163 cases of recurrent Clostridiumdifficile disease. Am J Gastroenterol 2002;97:1769e75.
3. BarbutF,RichardA,HamadiK,ChometteV,BurghofferB,Petit J-C.Epidemiologyof recurrenceor reinfectionsofClostridiumdifficile-associated diarrhea. J Clin Microbiol 2000;38:2386e8.
4. Johnson S, Adelmann A, Clabots CR, Peterson LR, Gerding DN.Recurrences of Clostridium difficile diarrhea not caused by theoriginal infecting organism. J Infect Dis 1989;159:340e3.
5. O’Neill GL, Beaman MH, Riley TV. Relapse versus reinfectionwith Clostridium difficile. Epidemiol Infect 1991;107:627e35.
6. Wilcox MH, Fawley WN, Settle CD, Davidson A. Recurrence ofsymptoms in Clostridium difficile infectionerelapse or reinfection?JHosp Infect1998;38:93e100.doi:10.1016/S0195-6701(98)90062-7.
7. Tang-Feldman Y, Mayo S, Silva Jr J, Cohen SH. Molecular anal-ysis of Clostridium difficile strains isolated from 18 cases ofrecurrent Clostridium difficile-associated diarrhea. J ClinMicrobiol 2003 Jul;41:3413e4.
8. Spencer RC. Clinical impact and associated costs of Clostridiumdifficile-associated disease. J Antimicrob Chemother 1998;41:5e12.
9. Pepin J, Saheb N, Coulombe MA, Alary ME, Corriveau MP,Authier S, et al. Emergence of fluoroquinolones as the predom-inant risk factor for Clostridium difficile-associated diarrhea:a cohort study during an epidemic in Quebec. Clin Infect Dis2005;41:1254e60.
10. McFarland LV. Update on the changing epidemiology of Clos-tridium difficile-associated disease. Nat Clin Pract Gastroen-terol Hepatol 2008;5:40e8.
11. Bartlett JG, Gerding DN. Clinical recognition and diagnosis ofClostridium difficile infection. Clin Infect Dis 2008;46(Suppl.1):S12e8.
12. Centers for Disease Control. Severe Clostridium difficile-asso-ciated disease in populations previously at low riskdfourstates, 2005. MMWR Morb Mortal Wkly Rep 2005;54:1201e5.
13. McFarland LV, Brandmarker SA, Guandalini S. Pediatric Clos-tridium difficile: a phantom menace or clinical reality? J Pe-diatr Gastroenterol Nutr 2000;31:220e31.
14. Gogate A, De A, Nanivadekar R, Mathur M, Saraswathi K, Jog A,et al. Diagnostic role of stool culture & toxin detection in anti-biotic associated diarrhoea due to Clostridium difficile in chil-dren. Indian J Med Res 2005;122:518e24.
15. Garey KW, Jiang Z-D, Yadav Y, Mullins B, Wong K, Dupont HL.Peripartum Clostridium difficile infection: case series and re-view of the literature. Am J Obstet Gynecol 2008;199:322e7.
16. Rouphael NG, O’Donnell JA, Bhatnagar J, Lewis F, Polgreen PM,Beekmann S, et al. Clostridium difficile-associated diarrhea:an emerging threat to pregnant women. Am J Obstet Gynecol2008;198:635. doi:10.1016/j.ajog.2008.01.062. e1e635.e6.
17. Klein EJ, Boster DR, Stapp JR, Wells JG, Qin X, Clausen CR, et al.Diarrhea etiology in a children’s hospital emergency department:a prospective cohort study. Clin Infect Dis 2006;43:807e13.
18. Kyne L, Warny M, Qamar A, Kelly CP. Asymptomatic carriage ofClostridium difficile and serum levels of IgG antibody againsttoxin A. N Engl J Med 2000;342:390e7.
19. Kyne L, Warny M, Qamar A, Kelly CP. Association betweenantibody response to toxin A and protection against
recurrent Clostridium difficile diarrhoea. Lancet 2001;357:189e93.
20. Warny M, Vaerman JP, Avesani V, Delmee M. Human antibodyresponse to Clostridium difficile toxin A in relation to clinicalcourse of infection. Infect Immun 1994;62:384e9.
21. Chang JY, Antonopoulos DA, Kalra A, Tonelli A, Khalife WT,Schmidt TM, et al. Decreased diversity of the fecal Mircobiomein recurrent Clostridum difficile-associated diarrhea. J InfectDis 2008;197:435e8.
22. Pepin J, Alary M-E, Valiquette L. Increasing risk of relapse aftertreatment of Clostridium difficile colitis in Quebec, Canada.Clin Infect Dis 2005;40:1591e7.
23. McFarland LV, Surawicz CM, Rubin M, Fekety R, Elmer GW,Greenberg RN. Recurrent Clostridium difficile disease: epide-miology and clinical characteristics. Infect Control Hosp Epide-miol 1999;20:43e50.
24. Garey KW, Sethi S, Yadav Y, DuPont HL. Meta-analysis to assessrisk factors for recurrent Clostridium difficile infection. J HospInfect 2008;70:298e304. doi:10.1016/j.jhin.2008.08.012.
25. Mayfield JL, Leet T, Miller J, Mundy LM. Environmental controlto reduce transmission of Clostridium difficile. Clin Infect Dis2000;31:995e1000.
26. Muto CA, Blank MK, Marsh JW, Vergis EN, O’Leary MM, Shutt KA,et al. Control of an outbreak of infection with the hyperviru-lent Clostridium difficile BI strain in a university hospital usinga comprehensive ‘‘bundle’’ approach. Clin Infect Dis 2007;45:1266e73.
27. Scheurer D. Diagnostic and treatment delays in recurrent Clos-tridium difficile-associated disease. J Hosp Med 2008;3:156e9.
28. Pepin J, Routhier S, Gagnon S, Brazeau I. Management and out-comes of a first recurrence of Clostridium difficile-associateddisease in Quebec, Canada. Clin Infect Dis 2006;42:758e64.
29. Teasley DG, Gerding DN, Olson MM, Peterson LR, Gebhard RL,Schwartz MJ, et al. Prospective randomized trial of metronida-zole versus vancomycin for Clostridium-difficile-associateddiarrhea and colitis. Lancet 1983;2:1043e6.
30. Wenisch C, Parschalk B, Hasenhundl M, Hirschl AM,Graninger W. Comparison of vancomycin, teicoplanin, metroni-dazole, and fusidic acid for the treatment of Clostridium diffi-cile-associated diarrhea. Clin Infect Dis 1996;22:813e8.
31. Musher D, Aslam S, Logan N, Nallacheru S, Bhaila I, Borchert F,et al. Relatively poor outcome after treatment of Clostridiumdifficile colitis with metronidazole. Clin Infect Dis 2005;40:1586e90.
32. Lagrotteria D, Holmes S, Smieja M, Smaill F, Lee C. Prospec-tive, randomized inpatient study of oral metronidazole versusoral metronidazole and rifampin for treatment of primary epi-sode of Clostridium difficile-associated diarrhea. Clin InfectDis 2006;43:547e52.
33. Sanchez JL, Gerding DN, Olson MM, Johnson S. Metronidazolesusceptibility in Clostridium difficile isolates recovered fromcases of C. difficile-associated disease treatment failures andsuccesses. Anaerobe 1999;5:201e4.
34. Zar FA, Bakkanagari SR, Moorthi KM, Davis MB. A comparison ofvancomycin and metronidazole for the treatment of Clostrid-ium difficile-associated diarrhea, stratified by disease sever-ity. Clin Infect Dis 2007;45:302e7.
35. Louie T, Gerson M, Grimard D, Johnson S, Poirier S, Weiss K. Re-sults of a phase III trial comparing tolevamer, vancomycin andmetronidazole in patients with Clostridium difficile-associateddiarrhea. In: Presented at the 47th interscience conference onantimicrobial agents and chemotherapy (ICAAC), September 17to 20, 2007, Chicago, IL.
36. European Society for Clinical Microbiology and Infectious Dis-eases. Guidance document of Clostridium difficile infection(CDI) diagnosis and treatment: treatment guideline. ClinMicrobiol Infect, in press.
410 S. Johnson
37. Gerding DN. Treatment of Clostridium difficile-associateddiarrhea and colitis. Curr Top Microbiol Immunol 2000;250:127e39.
38. Kokkotou E, Moss AC, Michos A, Espinoza D, Cloud JW,Mustafa N, et al. Comparative efficacies of rifaximin and van-comycin for treatment of Clostridium difficile-associated diar-rhea and prevention of disease recurrence in hamsters.Antimicrob Agents Chemother 2008;52:1121e6.
39. Johnson S, Schriever C, Galang M, Kelly CP, Gerding DN. Inter-ruption of recurrent Clostridium difficile-associated diarrheaepisodes by serial therapy with vancomycin and rifaximin.Clin Infect Dis 2007;44:846e8.
40. Jiang ZD, Ke S, Palazzini E, Riopel L, Dupont H. In vitro activityand fecal concentration of rifaximin after oral administration.Antimicrob Agents Chemother 2000;44:2205e6.
41. O’Connor J, Galang M, Sambol SP, Hecht DW, Vedantam G,Gerding DN, et al. Rifampin and rifaximin resistance in clinicalisolates of Clostridium difficile. Antimicrob Agents Chemother2008;52:2813e7.
42. Curry SR, Marsh JW, Shutt KA, Muto CA, O’Leary MM, Saul MI,et al. High frequency of rifampin resistance identified in an ep-idemic Clostridium difficile clone from a large teaching hospi-tal. Clin Infect Dis 2009;48:425e9.
43. Musher DM, Logan N, Mehendiratta V, Melgarejo NA, Garud S,Hamill RJ. Clostridium difficile colitis that fails conventionalmetronidazole therapy: response to nitazoxanide. J Antimi-crob Chemother 2007;59:705e10.
44. Buggy BP, Fekety R, Silva Jr J. Therapy of relapsing Clostridiumdifficile-associated diarrhea and colitis with the combination ofvancomycin and rifampin. J Clin Gastroenterol 1987;9:155e9.
45. Surawicz CM, McFarland LV, Greenberg RN, Rubin M, Fekety R,Mulligan ME, et al. The search for a better treatment for recur-rent Clostridium difficile disease: use of high-dose vancomycincombined with Saccharomyces boulardii. Clin Infect Dis 2000;31:1012e7.
46. McDonald LC, Owings M, Jernigan DB. Clostridium difficileinfection in patients discharged from US short-stay hospitals,1996e2003. Emerg Infect Dis 2006;12:409e15.
47. McFarland LV, Surawicz CM, Greenberg RN, Fekety R, Elmer GW,Moyer KA, et al. A randomized placebo controlled trial of Saccha-romyces boulardii in combination with standard antibiotics forClostridium difficile disease. JAMA 1994;271:1913e8.
48. Graf C, Gavazzi G. Saccharomyces cerevisiae fungemia in animmunocompromised patient not treated with Saccharomycesboulardii preparation. J Infect 2007;54:310e1.
49. Wullt M, Hagslatt ML, Odenholt I. Lactobacillus plantarum 299vfor the treatment of recurrent Clostridium difficile-associateddiarrhoea: a double-blind, placebo-controlled trial. Scand JInfect Dis 2003;35:365e7.
50. Wilcox WH. Descriptive study of intravenous immunoglobulinfor the treatment of recurrent Clostridium difficile diarrhoea.J Antimicrobial Chemother 2004;53:882e4.
51. Beales ILP. Intravenous immunoglobulin for recurrent Clostrid-ium difficile diarrhoea. Gut 2002;51:456.
52. Sougioultzis S, Kyne L, Drudy D, Keates S, Maroo S,Pothoulakis C, et al. Clostridium difficile toxoid vaccine inrecurrent C. difficile-associated diarrhea. Gastroenterology2005;128:764e70.
53. Aas J, Gessert CE, Bakken JS. Recurrent Clostridium difficilecolitis: case series involving 18 patients treated with donorstool administered via a nasogastric tube. Clin Infect Dis2003;36:580e5.
54. Moncino MD, Falletta JM. Multiple relapses of Clostridium dif-ficile-associated diarrhea in a cancer patient: successful con-trol with long-term cholestyramine therapy. Am J PediatrHematol Oncol 1992;14:361e4.
55. Pruksananonda P, Powell KR. Multiple relapses of Clostridiumdifficile-associated diarrhea responding to an extended courseof cholestyramine. Pediatr Infect Dis J 1989;8:175e8.
56. Kurtz CB, Cannon EP, Brezzani A, Pitruzzello M, Dinardo C,Rinard E, et al. GT160-246, a toxin-binding polymer for treat-ment of Clostridium difficile colitis. Antimicrob Agents Che-mother 2001;45:2340e7.
57. Ackermann G, Loffler B, Adler D, Rodloff AC. In vitro activity ofOPT-80 against Clostridium difficile. Antimicrob Agents Che-mother 2004;48:2280e2.
58. Louie T, Miller M, Donskey C, Mullane K, Goldstein EJ. Clinicaloutcomes, safety and pharmacokinetics of OPT-80 in a phase 2trial of patients with Clostridium difficile infection. Antimi-crob Agents Chemother 2009;53:223e8.
59. Louie TJ, Emery J, Krulicki W, Byrne B, Mah M. OPT-80 elimi-nates Clostridium difficile and is sparing of Bacteroides spe-cies during treatment of C. difficile infection. AntimicrobAgents Chemother 2009;53:261e3.


















