Recurrent abdominal pain—the forgotten cause · Recurrent abdominal pain—the forgotten cause...
18
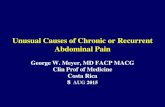
SELF ASSESSMENT QUESTIONS Recurrent abdominal pain—the forgotten cause P M S Evans, A Williams, A H El-Shaboury A 23 year old man presented to the casualty department with right periorbital oedema. A diagnosis of urticaria was made, antihistamines were prescribed, and he was discharged home. Within 24 hours he returned complaining of increased facial swelling and dysphagia, and a medical opinion was sought. He denied recent facial trauma, or insect stings. Further inquiry revealed that he had suVered a similar episode nine months earlier which had involved swell- ing of his hands and feet. These areas were not itchy or red. His past history included recur- rent bouts of abdominal pain associated with distension and vomiting requiring numerous hospital admissions under the care of diVerent consultants over the previous 14 years. A diag- nosis of abdominal migraine was frequently recorded. There were no obvious precipitating factors and the bouts resolved spontaneously over a period of a few days. Detailed family history uncovered several members with simi- lar symptoms and an inheritance pattern along the maternal line. Examination revealed a slim built, normotensive 23 year old man with bilat- eral periorbital, perioral, and pharyngeal oedema. He was comfortable at rest with no drooling, dyspnoea, or wheeze (fig 1). Routine investigations showed a normal full blood count, urea and electrolytes, liver function tests, and chest x ray film. The suspected diag- nosis of C1 esterase inhibitor (C1 INH) deficiency was confirmed with low C1 INH and C4 concentrations at 0.08 g/l (normal 0.15–0.35) and <0.06 g/l (normal 0.20–0.60) respectively. In view of the frequency and severity of his symptoms he was started on prophylactic treatment with danazol. He was advised that he would require intravenous infusions of C1 INH concentrate as prophylaxis before any future surgical intervention and review would be needed before future dental work. He was dis- charged with a Medic Alert bracelet and arrangements were made to screen other family members. To date, three years later, there have been no further relapses. Questions: true or false C1 INH deficiency: (1) Is always associated with peripheral angio-oedema and urticaria. (2) Symptoms can be precipitated by the oral contraceptive pill. (3) Is the most commonly described genetic defect of the complement system and is characterised by a reduction in comple- ment proteins C3 and C4. (4) Is inherited in an autosomal recessive manner and usually presents in the first decade of life. (5) Is primarily treated with fresh frozen plasma which has replaced steroids and antihistamines as the treatment of choice during acute episodes. (6) May be treated by antifibrinolytic drugs, particularly in the acquired variety or in those not responding to androgens. Answers on p 128. Figure 1 Periorbital and perioral angioedema in the aVected case (photograph reproduced with patient’s permission). Postgrad Med J 2001;77:121–127 121 Department of Medicine, Royal Gwent Hospital, CardiV Road, Newport NP20 2UB, UK P M S Evans Department of Immunology, Churchill Hospital, Oxford A Williams Department of Medicine, Prince Charles Hospital, Merthyr Tydfil A H El-Shaboury Correspondence to: Dr Evans Submitted 25 August 1999 Accepted 22 November 1999 www.postgradmedj.com on July 6, 2021 by guest. Protected by copyright. http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pmj.77.904.124a on 1 February 2001. Downloaded from
Transcript of Recurrent abdominal pain—the forgotten cause · Recurrent abdominal pain—the forgotten cause...
-
SELF ASSESSMENT QUESTIONS
Recurrent abdominal pain—the forgotten cause
P M S Evans, A Williams, A H El-Shaboury
A 23 year old man presented to the casualtydepartment with right periorbital oedema. Adiagnosis of urticaria was made, antihistamineswere prescribed, and he was discharged home.Within 24 hours he returned complaining ofincreased facial swelling and dysphagia, and amedical opinion was sought. He denied recentfacial trauma, or insect stings. Further inquiryrevealed that he had suVered a similar episodenine months earlier which had involved swell-ing of his hands and feet. These areas were notitchy or red. His past history included recur-rent bouts of abdominal pain associated withdistension and vomiting requiring numeroushospital admissions under the care of diVerentconsultants over the previous 14 years. A diag-nosis of abdominal migraine was frequentlyrecorded. There were no obvious precipitatingfactors and the bouts resolved spontaneouslyover a period of a few days. Detailed familyhistory uncovered several members with simi-lar symptoms and an inheritance pattern alongthe maternal line. Examination revealed a slimbuilt, normotensive 23 year old man with bilat-eral periorbital, perioral, and pharyngealoedema. He was comfortable at rest with nodrooling, dyspnoea, or wheeze (fig 1). Routineinvestigations showed a normal full bloodcount, urea and electrolytes, liver functiontests, and chest x ray film. The suspected diag-nosis of C1 esterase inhibitor (C1 INH)deficiency was confirmed with low C1 INHand C4 concentrations at 0.08 g/l (normal0.15–0.35) and
-
A rare coincidence and recurrent urinary tractinfections
D Debnath, D G Richards
A 68 year old woman was referred for recurrentepisodes of urinary tract infection and weightloss of four months’ duration. She gave ahistory of intermittent brownish dischargefrom her urethra for the same duration but wasotherwise asymptomatic. There was no signifi-cant past medical history. Laboratory evalua-tion revealed a haemoglobin level of 100 g/l,leucocyte count of 11.0 × 109/l, and a positiveurine culture (Escherichia coli). A rigid cystos-copy was performed which readily confirmedthe diagnosis. A biopsy specimen, which wastaken during cystoscopy, showed transitionalcell carcinoma.
Computed tomography of abdomen andpelvis (fig 1) was arranged. There was no nodalspread or liver metastasis. She subsequentlyunderwent laparotomy that revealed the fistu-lous communication between sigmoid colonand roof of the bladder. A defunctioning colos-tomy was performed. She was recalled after sixweeks for a second operation that entailed atotal cystectomy (along with ileal conduitformation) and low anterior resection with clo-sure of the rectal stump and left iliac fossacolostomy. Her postoperative recovery wasuneventful.
The whole specimen was sent to the patholo-gist for further evaluation (fig 2 is the micro-photograph of relevant section of the histology).
Questions(1) What is the initial diagnosis?(2) What and how common are the histologi-
cal findings?(3) What is the prognosis?
Answers on p 129.
Figure 1 Computed tomography of abdomen and pelvis.
Figure 2 Histology (haematoxylin and eosin; original magnification × 100).
122 Self assessment questions
West CumberlandHospital, Whitehaven,CumbriaD DebnathD G Richards
Correspondence to:Mr D Debnath, c/o NortonHouse, Grantham andDistrict Hospital, 101Manthorpe Road, Grantham,Lincolnshire NG31 8DG,[email protected]
Submitted 8 December 1999Accepted 22 December 1999
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
Obtunded sensorium in a trauma patient
A Mazumdar, S Kumar, S P Balasubramanian, A K Sharma
A 36 year old man, a victim of road traYc acci-dent, with head injury and epistaxis, was takento a district hospital. He was intubated with anorotracheal tube and his scalp injury wasdressed, and he was referred to this tertiary careinstitute accompanied by his relatives. Threehours after the injury, when he was brought tothe emergency room, he was noted to have inter-costal recession while breathing, a systolic bloodpressure of 95 mm Hg, and Glasgow coma score(GCS) was 2/10. Air entry on both sides of thechest was minimal and equally diminished onboth sides, the percussion note on either sidewas not dull, and the neck veins were empty.Flow from the endotracheal tube was hardlyaudible. An endotracheal suction catheter wasinserted but it could not be pushed beyond 20cm. Arterial blood gases were sampled whiletrying hard to ventilate with an Ambu bag andwere: oxygen tension 10.4 kPa, carbon dioxidetension 6.9 kPa, and pH 7.26. As per referralnote, his systolic blood pressure at the time ofreferral was 110 mm Hg and GCS 5/10. Therewas no apparent external loss of blood. (Moni-toring by pulse oximetry was not possiblebecause no pulse oximeter was available.)
Questions(1) What is the most likely cause of deteriora-
tion of GCS in this case?(2) What should be the next step?(3) What is the most probable cause of hypo-
tension in this case?(4) What is the finding shown in fig 1?(5) What is the most likely explanation for the
development of blockage of this endotra-cheal tube?
Acute appendicitis: an unusual cause
S K Clark, T Qureshi, M Sen
A 52 year old woman presented with a two dayhistory of worsening central abdominal pain,with nausea, and vomiting. Over the previousmonth she had been treated for a flare up ofrheumatoid arthritis. Her only medication wasmethotrexate 10 mg/week and buprenorphine200 µg three times a day. On examination shelooked unwell and had a pyrexia of 37.4°C.Her pulse was 110 beats/min and her bloodpressure was 110/54 mm Hg. Her abdomenwas distended and she had generalised periton-ism; bowel sounds were absent. She had a mildleucocytosis of 11.2 × 109/l but her full bloodcount and serum electrolytes were otherwisenormal. Plain abdominal radiography revealedmultiple central loops of small bowel whichwere not dilated.
At laparotomy there was free pus in the pel-vis, and a pelvic appendix was inflamed andperforated distally; the only other abnormali-ties were a 10 cm nodular cyst of the right ovaryand inflammation of the omentum. Appendi-cectomy, right salpingo-oophorectomy, andomentectomy were performed. These organswere non-adherent and were therefore re-moved separately.
Questions(1) Describe the histological features
(see p 131).(2) What further treatment is indicated?
Answers on p 130.
Figure 1 Blocked endotracheal tube extubated frompatient with deterioration in sensorium.
Department ofSurgery,Crawley Hospital,Crawley,West Sussex, UKS K ClarkT QureshiM Sen
Correspondence to:Miss S K Clark,25 Kelso Place,London W8 5QG, UK
Submitted 8 July 1999Accepted 22 December 1999
Answers on p 130.
Self assessment questions 123
Department ofSurgery, PostGraduate Institute ofMedical Education &Research, Chandigarh,IndiaA MazumdarS KumarS P BalasubramanianA K Sharma
Correspondence to:Mr Ajay Sharma, RenalTransplant Unit, Link 9C,Royal Liverpool UniversityHospitals, Prescot Street,Liverpool L7 8XP, UK
Submitted 14 June 1999Accepted 22 December 1999
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
Is spiral computed tomography the imagingmodality of choice for renal colic?
N Sarath Krishna, L Morrison, C Campbell
A 59 year old women was admitted with left loinpain of three days’ duration. There was noradiation of pain to her groin. She had no dysu-ria, urinary frequency, or vaginal discharge andwas apyrexial. On examination she had no lointenderness. She was treated with analgesics,which relieved her pain. Her urine analysis waspositive for blood. A midstream specimen ofurine showed no growth of organisms. Fullblood count, electrolytes, urea, and creatininewere all within normal limits. Intravenous urog-raphy was performed which revealed no obviouscalculus in the line of the urinary tract and anormal right kidney. A delayed dense nephro-gram was seen on the left side. There was nocontrast excretion into the left ureter. Subse-quently spiral computed tomography of theabdomen was performed to exclude a calculusas the cause of the obstruction (see fig 1).
Questions(1) What is the diagnosis, and what is spiral
computed tomography?
(2) What are the findings on the spiral com-puted tomogram?
(3) What are the advantages of spiral com-puted tomography in evaluating a case ofrenal colic?
A young woman with intractable diarrhoea
A S Kashyap, R Varadarajulu, S Kashyap
A 28 year old saleswoman reported loosemotions of three years’ duration. She wassymptomatic with recurrent copious wateryloose motions five to six times a day, which hadprogressively worsened. Symptomatic treat-ment with antimotility agents had providedpoor relief.
Moderate hypertension had been diagnosedseven years before, which was controlled withenalapril 5 mg/day. Over a period of four yearsher blood pressure settled to normal levels.Enalapril was discontinued three years ago andher blood pressure remained normal. Herfather had died suddenly of hypertension and“abdominal tumour”.
On clinical examination her blood pressurewas 130/76 mm Hg with no postural fall. Therest of the general and systemic examinationwas normal. Her packed cell volume, completeblood counts, peripheral blood smear, serumpotassium, sodium, calcium, phosphate, albu-min, glucose, serum creatinine, thyroid profile,stool microscopy and culture, fecal fat excre-tion, D-xylose absorption test, upper gastro-intestinal endoscopy, colonoscopy, small intes-tinal biopsy, small bowel barium followthrough, abdominal and chest radiographswere normal. HIV antibodies were negative byenzyme linked immunosorbent assay. The
serum and urine drug, toxicology, and laxativescreen were negative. The serum concen-trations of serotonin, gastrin, somatostatin,vasoactive intestinal peptide, and calcitoninwere normal. Concentrations of urinary5-hydroxyindole acetic acid and plasma nore-pinephrine and epinephrine were normal. Theplasma dopamine concentration was 0.94ng/ml (normal
-
acid was 13 mg/day (normal
-
A small axillary nodule—a therapeutic dilemma?
A Mazumdar, R K Vasishta, S M Bose
A 75 year, postmenopausal women presentedwith a lump in the left axilla associated withoccasional pain for six months. There was nohistory suggestive of an increase in size, anawareness of a lump in either breast or theopposite axilla, or discharge from the nipple.Past medical history was not contributory asthere was no family history of breast cancer.Examination showed a firm, mobile lump inthe centre of left axilla (1× 1 cm), subcutaneousin location. No other lump could be detected inthe axilla or either of the breasts.
The patient had been seen earlier by ageneral practitioner who considered the lumpof benign pathology. Fine needle aspirationcytology (FNAC) carried out in our hospitalrevealed features suggestive of metastatic carci-noma. Excision biopsy showed it to be an infil-trating duct carcinoma. Chest radiography,ultrasonography of the abdomen, and bilateralmammography were normal.
The patient underwent total mastectomyand axillary clearance with excision of the axil-lary scar. Histopathology revealed no primaryfocus in the entire breast or lymph nodes in theaxilla. Sections from the excised scar tissueshowed a very small focus of malignancy (fig1). The postoperative period was uneventful.An oestrogen receptor study was positive. The
patient is followed up regularly and takingtamoxifen 20 mg once a day.
Questions(1) What is the significance of an axillary
nodule in an elderly patient?(2) What should be the diagnostic modality
in a case of axillary nodule?(3) What is the treatment modality in a case
of axillary nodule with occult metastasis?(4) What are the various histopathological
considerations in such a case?
A farmer with artificial valve endocarditis
H Alsoub, S S El-Shafie
A 29 year old Yemeni man, a farmer, with StVincent aortic and mitral prosthesis replaced inApril 1996, was admitted to hospital in Febru-ary 1997 with a nine month history ofintermittent fever, general weakness, and lossof appetite. Three months before admission hedeveloped right sided hemiparesis for which hewas admitted to another hospital. No details ofthat admission could be obtained, however hehad significant improvement in his weakness.Physical examination on admission revealed:temperature 39oC, blood pressure 120/60 mmHg, pulse 104 beats/min, an early diastolicmurmur at the left sternal border, and mildright facial, right upper, and lower limbweakness. Laboratory investigations revealedthe following: haemoglobin 99 g/l, white cellcount 4.3 × 109/l, platelet count 288 × 109/l,erythrocyte sedimentation rate (ESR) 33 mmin the first hour, and brucella agglutination testand mercaptoethanol test were positive to titres
of 1: 5120 and 1:2560 respectively. Liver andrenal function tests were normal. A trans-oesophageal echocardiogram revealed small
Answers on p 135.
Figure 1 Microphotograph showing nest of tumour cellsbeneath the skin in the subcutaneous plane.
Hamad MedicalCorporation, PO Box3050, Doha, QatarH AlsoubS S El-Shafie
Correspondence to:Dr Alsoub
Submitted 18 February 1998Accepted 7 December 1999
Answers on p 136.
Figure 1 Two dimensional echocardiogram, parasternallong axis view showing prosthetic aortic and mitral valves.Note the separation between the aortic wall and theprosthesis ring (arrow); LV = left ventricle; RV = rightventricle; LA = left atrium.
126 Self assessment questions
Post GraduateInstitute of MedicalEducation andResearch, Chandigarh,India: Department ofSurgeryA Mazumdar
Department ofPathologyR K Vasishta
Surgery Unit II andEmergency ServicesS M Bose
Correspondence to:Professor S M Bose, H No75, Sector 24, Chandigarh,160023 Indiasmbose>[email protected] [email protected]
Submitted 21 September1999Accepted 20 December 1999
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
vegetation at the aortic prosthesis with moder-ate paravalvular leak, the mitral prosthesis wasnormal (fig 1). Six blood cultures grew Brucellamelitensis. He was treated with oral doxycycline100 mg twice daily, rifampin 450 mg twicedaily, and intravenous co-trimoxazole 960 mgthree times daily. Four days later he was takenfor operation, two ring abscesses were found,they were drained, and the infected valve wasreplaced by a new one. Culture of speci-menstaken during surgery yielded B melitensis.He had an uneventful postoperative course and
was discharged two weeks later on oral doxycy-cline, rifampin, and co-trimoxazole, which hetook for a total of 20 weeks.
Questions(1) What are the most common organisms
causing artificial valve endocarditis? Whatare other less common organisms shouldbe considered?
(2) How should the diagnosis be established?(3) What would be the best therapeutic
approach?
Loss of weight in a female heavy smoker withdiVuse interstitial pulmonary fibrosis
A Al-Adsani, M H Dahniya, N Al-Adsani
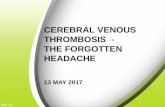
A 75 year old hypertensive woman was admit-ted with a two month history of fever andcough with scanty sputum, loss of appetite andweight, and progressive exertional dyspnoea.She had habitually smoked 20–40 cigarettes aday since the age of 19 years. Her activities hadbecome limited recently by dyspnoea and backpain. There was no history of exposure totuberculosis. Chest radiography, done twoyears before, showed extensive diVuse reticu-lonodular shadowing with honeycombing andperipheral and basal accentuation (fig 1).
Physical examination revealed an afebrileemaciated women with respiratory rate of 20breaths/min, and a blood pressure of 150/90mm Hg (after medication). Heart sounds werenormal and there were bilateral fine basalcrackles over the lungs. There was no palpableperipheral lymphadenopathy or pedal oedemabut there was clubbing of both fingers and toes.A new posteroanterior chest radiograph was
done (fig 2). Investigations revealed mildhypochromic anaemia and a normal white cellcount with eosinophilia of 16.4%. Her erythro-cyte sedimentation rate was raised at 121mm/hour. Arterial blood analysis revealed anoxygen tension of 8.96 kPa, carbon dioxidetension 3.99 kPa, and pH 7.39. Microscopicexamination of the sputum was negative foracid-fast bacilli.
Questions(1) What does the chest radiograph in fig 2
show?(2) Suggest two causes that would explain the
new radiological finding in fig 2.(3) What three further investigations would
you request?(4) What is the final diagnosis and what is the
relative risk of its development in patientswith diVuse interstitial pulmonary fibro-sis?
(5) In your opinion, what is the major riskfactor for the final diagnosis in this case?
Al-Sabah Hospital,Kuwait: Department ofMedicineA Al-Adsani
Department ofDiagnostic Radiologyand ImagingM H Dahniya
Mansouria HealthClinic, KuwaitN Al-Adsani
Correspondence to:Dr A Al-Adsani, PO Box31098, 90801 Sulaibikhat,[email protected]
Submitted 9 June 1999Accepted 22 November 1999
Answers on p 137.
Figure 1 Chest radiograph two years before presentation.
Figure 2 Posteroanterior chest radiograph.
Self assessment questions 127
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
SELF ASSESSMENT ANSWERS
Recurrent abdominal pain—the forgottencause
C1 INH deficiency:
Q1: Is always associated with peripheralangio-oedema and urticariaFalseC1 INH deficiency is not associated with urti-caria but the angio-oedema may be precededby a serpiginous erythematous rash which isnon-pruritic. Peripheral angio-oedema is a wellrecognised presentation but mucosal angio-oedema can be life threatening and may involvethe bowel.
Q2: Symptoms can be precipitated by theoral contraceptive pillTrueThe oral contraceptive pill and menstrual cyclehave been linked to exacerbations of the condi-tion but the most commonly reported precipi-tating factors are trauma, dental extraction,and emotional stress.1
Q3: Is the most commonly describedgenetic defect of the complement systemand is characterised by a reduction incomplement proteins C3 and C4FalseIt is the most commonly described geneticdefect of the complement system2 in which C4and C2 are reduced due to the uncheckedactivity of C1, but C3 is invariably normal.This is because C3 convertase is not generateddue to C4b and C2b being rapidly inactivatedin the plasma.
Q4: Is inherited in an autosomal recessivemanner and usually presents in the firstdecade of lifeFalseC1 INH deficiency may be inherited in anautosomal dominant (chromosome 11, p11.2–q13 ), manner where it usually appears early inlife, or acquired presenting in the fourthdecade or later.3 Quantitative (85%) andqualitative (15%) deficiencies of C1 INH areresponsible for the inherited variety2 while anincreased catabolic rate and autoantibodies toC1 INH are responsible for the two acquiredforms.4
Q5: Is primarily treated with fresh frozenplasma which has replaced steroids andantihistamines as the treatment of choiceduring acute episodesFalseC1 INH concentrate is preferred for the acuteepisode, because fresh frozen plasma containsC1 and C2 which may aggravate symptoms.
Q6: May be treated by antifibrinolyticdrugs, particularly in the acquiredvariety or in those not responding toandrogensTrueProphylactic treatment is by substituted andro-gens (stanozolol) and antifibrinolytic drugs(tranexamic acid). Antifibrinolytics are thetreatment of choice before puberty and inwomen trying to conceive.
DiscussionAngio-oedema was originally documented byMilton in 1876,4 while Osler described heredi-tary angioneurotic oedema in 1888.5 Donald-son et al first recognised that a deficiency of C1INH was the cause of hereditary angio-oedemain 1963.6 C1 INH is a 104 kDa protein and itsdeficiency is the most commonly describedgenetic defect of the complement system.2 Itacts as a serine protease inhibitor upon theC1qrs enzyme complex of the classical comple-ment pathway as well as those of the kallikreinand plasminogen pathways. It is believed thatangio-oedema is a result of reduced C1 INHfunction through a reduced inhibition ofkallikrein, complement system activation, andkinin generation.7
A common presentation of C1 INH defi-ciency is that of recurrent episodes of acute,colicky abdominal pain associated with vomit-ing. Reports exist of patients undergoingoperative exploration in the mistaken beliefthat a surgical emergency underlies the ab-dominal pain.8 Findings at operation include alarge amount of serous fluid and intestinal walloedema, which can lead to intussusception andhypovolaemic shock. Our case was saved fromlaparotomies because the diagnosis of “ab-dominal migraine” had been made repeatedly.Non-mucosal angio-oedema is usually welldemarcated, localised, and most commonlyfound aVecting skin on the extremities. Themucous membranes of the mouth, pharynx,and larynx may be involved.
Trauma, dental extractions, and emotionalstress are among the most common precipitat-ing factors, while the menstrual cycle and oralcontraceptive pill have also been linked toexacerbations of the condition.1
Initial investigations of suspected C1 INHdeficiency should include measurement of thecomplement components C2, C3, C4, and C1INH. Further immunological investigations mayinclude assays for functional C1 INH, C1, andC1 autoantibodies. If acquired C1 INH issuspected serum electrophoresis may identifythe monoclonal paraprotein of a B cell lympho-proliferative condition. Barium studies duringabdominal pain may show a classical “stackedcoin appearance”, but confirmation is achievedby quantitative and qualitative measurement ofC1 INH.
Treatment of the acute episode is preferen-tially with C1 INH concentrate which shouldalso be used prophylactically before surgery.
Postgrad Med J 2001;77:128–138128
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
The use of fresh frozen plasma is controversialbecause it contains C1 and C2, which mayaggravate symptoms.
Prophylactic treatment is by substitutedandrogens (stanozolol) and antifibrinolyticdrugs (tranexamic acid). Antifibrinolytics maybe eVective in the acquired variety, those notresponding to androgens, and are indicatedbefore puberty and in women trying toconceive. Treatment of associated conditionsmay lead to symptomatic improvement inacquired C1 INH deficiency.
AVected individuals should wear MedicAlert bracelets. Genetic counselling andscreening should be oVered to their families,even those apparently not aVected, because theclinical course of the disease can be sovaried.
The diagnosis of C1 INH deficiency isfrequently missed, as happened in our patientover a period of 14 years. It should be consid-ered in any case of recurrent abdominal painfor which no obvious cause can be found.
1 Yip J, CunliVe WJ. Hormonally exacerbated hereditaryangioedema. Aust J Dermatol 1992;33:35–8.
2 Carreer FMJ. The C1 inhibitor deficiency. Eur J Clin ChemBiochem 1992;30:793–807.
3 Alsenz J, Bork K, Loos M. Autoantibody mediated acquireddeficiency of C1 inhibitor. N Engl J Med 1987;316:1360–6.
4 Milton JL. On giant urticaria. Edinburgh Medical Journal1876;22:513–26.
5 Osler W. Hereditary angioneurotic oedema. Am J Med Sci1888;95:362–7.
6 Donaldson VH, Evans RR. A biochemical abnormality inhereditary angioedema: absence of serum inhibitor of C1esterase. Am J Med 1963;35:37–44.
7 Cicardi M, Agostini A. Hereditary angioedema. N Engl JMed 1996;334:1666–7.
8 Cohen N, Sharon A, Golik A, et al. Hereditary angioneu-rotic edema with severe hypovolaemic shock. J Clin Gastro-enterol 1993;16:237–39.
A rare coincidence and recurrent urinarytract infections
Q1: What is the initial diagnosis?Enterovesical fistula secondary to bladder car-cinoma complicated by urinary tract infection.
Common causes of enterovesical fistula are1:x Diverticular disease of colonx Colonic malignancyx Granulomatous bowel diseasex Iatrogenic (for example, radiation therapy)Clinical symptoms and signs are varied, mainlyurinary tract infection (100%), pneumaturia(66%), and faecaluria (50%).2 Awareness of thepossibility of an enteric origin of recurrenturinary tract symptoms should help prevent thelong delays in diagnosis.3
Cystoscopy is regarded as the most usefuldiagnostic procedures in detecting fistula.4
Other modes of investigation are barium enema,cystography, colonoscopy, and computed tom-ography.1 2 In this case computed tomographydistinctly (see p 122) showed (A) gas in thebladder (B) mass involving the bladder.
Treatment depends on the aetiology, localisa-tion, and the patient’s general condition. Com-monly used technique is resection of thefistulous tract and the compromised intestinalsegment, followed by repair of the bladder.4 Theprocedure can be performed as a single stagewhen the aetiology is diverticular or granuloma-tous bowel disease. Staged repairs are morejudicious in patients with a large interveningpelvic abscess or those in whom advancedmalignancy or radiation changes are present.1
Insertion of colonic stent, laparoscopic repair,5
and use of human fibrin glue for a recurrent fis-tula have also been described in the literature.
Q2: What and how common are thehistological findings?Unexpectedly, pathological assessment showedthat the fistula was formed by two distinct pri-maries: adenocarcinoma from the colon andtransitional cell carcinoma from the bladder.Note fig 2 (see page 122): (A) colonicadenocarcinoma and (B) poorly diVerentiatedtransitional cell carcinoma.
Malignancy is a known cause (35%–66%)2 4
of enterovesical fistula. The latter is mostcommonly vesicosigmoidal by location(50%).4 In this case the site of fistula wasbetween dome of the bladder and sigmoidcolon in deed. However, occurrence of twounrelated primaries of adjacent organs at thesame site, which collided to form a fistula, wasan extremely rare coincidence. We have notfound any published reports of a similarnature, which makes this case unique.
Q3: What is the prognosis?When the fistula is of malignant origin, the longterm prognosis remains poor, as it is for anycolonic (or bladder) carcinoma extendingbeyond the serosa and involving a contiguousorgan. Fistulas secondary to radiation necrosisand recurrent tumour have an extremely pooroutlook. Patients with fistulas due to diverticu-lar disease (and to a lesser extent, Crohn’s dis-ease) can look forward to complete correctionwith low morbidity and mortality.3
This patient sadly died eight months afterthe operation from distant metastases.
Final diagnosisMalignant vesicosigmoidal fistula due to colli-sion between two distinct primary tumoursarising from the colon and bladder respectively.
1 McBeath RB, SchiV M Jr, Allen V, et al. A 12 year experiencewith enterovesical fistulas. Urology 1994;44:661–5.
2 Hernandez Millan I, Salinas Sanchez AS, Pastor GuzmanJM, et al. Vesico-intestinal fistulae. Actas Urol Esp 1993;17:252–8.
3 Karamchandani MC, West CF Jr. Vesicoenteric fistulas. AmJ Surg 1984;147:681–3.
4 Alapont-Perez FM, Gil-Salom M, Esclapez-Valero JP, et al.Acquired enterovesical fistulas. Arch Esp Urol 1994;47:973–7.
5 Puente I, Sosa JL, Desai U, et al. Laparoscopic treatment ofcolovesical fistulas: technique and report of two cases. SurgLaparosc Endosc 1994;4:157–60.
Learning pointsC1 esterase inhibitor deficiency:x Commonest complement deficiencyx Significant morbidity and mortalityx Easy and cheap to diagnosex Eminently treatablex Should be considered in any case of
recurrent abdominal pain for which noobvious cause can be found
Self assessment answers 129
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
Obtunded sensorium in a trauma patient
Q1: What is the most likely cause ofdeterioration of GCS in this case?Hypoxia is the most important preventablecause of obtunded sensorium in a traumapatient. It may manifest in the form ofnon-purposeful motor responses, and, there-fore, is a strong indication for the need fordefinitive airway.1 Hypoxia and hypotensionare to be ruled out before incriminating intrac-ranial events or drugs (alcohol) as a cause ofdeterioration in GCS score.
Q2: What should be the next step?Extubate the patient because the tube isblocked. Oxygenate him with mask, and estab-lish a definitive airway once again.
The cuV of the endotracheal tube wasimmediately deflated and the patient was extu-bated. The oral cavity and pharynx werecleaned and he was put on an oxygen mask. Hewas reintubated with another endotrachealtube and ventilated. Immediately thereafter, abottle of saline (500 ml) was infused over 15minutes. After 30 minutes of reintubation hisblood pressure improved to 105 mm Hg systo-lic. Two hours after reintubation and ventila-tion, his arterial blood gases were: oxygen ten-sion 13.6 kPa, carbon dioxide tension 5.6 kPa,and pH 7.32. About five hours after admissionhis blood pressure was 110 mm Hg and GCSscore improved to 4/10. By this time the fluidinfusion was limited to 800 ml (since admis-sion) in view of the head injury and lack of anyapparent blood loss (internal/external).
Q3: What is the most probable cause ofhypotension in this case?In a trauma setting, hypoxia is the most impor-tant preventable cause of death. Myocardialcontractility is reduced in the presence ofhypoxia or acidosis.2 Correction of hypoxia andacidosis (respiratory) after reintubation andventilation resulted in improvement in bloodpressure. Only an 800 ml fluid infusion overfive hours was needed to raise his bloodpressure; this indicates that it was not hypovol-aemia that was the main cause of the lowerblood pressure.
Q4: What is the finding shown in fig 1 (seep 123)?The tube is blocked with a blood clot.
Q5: What is the most likely explanationfor the development of blockage of thisendotracheal tube?Aspirated blood would block the endotrachealtube. It is an important possibility in this caseas the patient had epistaxis at the time of pres-entation to the district hospital. Endotrachealsuctioning, during transfer, could have savedhim from such a catastrophe.
Blocked or displaced endotracheal tubes arean important cause of hypoxia in traumaduring transfer. Whenever a patient is shiftedfrom one ward/hospital to other, one mustensure patency and correct positioning3 of the
endotracheal tube. This can be easily accom-plished by a trained paramedic.
DiscussionIt is not surprising that there is deterioration inthe sensorium because of a blocked ordisplaced tube. What is surprising is the lack ofawareness, and desire to take appropriatemeasures (pre-hospital trauma care), amongthe public, administrators, and medical profes-sionals that hypoxia can kill very quickly. Ali etal reported much improved care after introduc-tion of the pre-hospital trauma life supportprogram (PHTLS), on the principles ofAdvanced Trauma Life Support.4 PHTLS hasbeen shown to be eVective when compared tocare before introduction of PHTLS in, forexample, the frequency of airway control(99.7% v 10%). Failure to monitor theendotracheal tube resulted in the lumen beingcompromised by blood clots, a preventablecomplication. The major clinical problem inthis case is that it took three hours for thepatient to arrive at a tertiary centre and thepatient was not accompanied by medical orparamedical staV. Besides the medical lessonslearnt from this case, an even more importantmessage is for planners of medical care. Theyshould be aware that tertiary care hospitalscannot treat patients eVectively until andunless primary and secondary care is madeeVective. Good communication and a safeparamedical escort to a further referral centreis the key as trauma patients with a compro-mised airway cannot wait.
Final diagnosisHypoxia causing obtunded sensorium.
1 Subcommittee on Advanced Trauma Life Support of theAmerican College of Surgeons Committee on Trauma1993–1997. Initial assessment and management. Advancedtrauma life support program for doctors. Chicago: AmericanCollege of Surgeons, 1997: 21–46.
2 Kaplan JA. Cardiovascular physiology. In Miller RD, ed.Anaesthesia. 2nd Ed. Edinburgh: Churchill-Livingstone,1986: 1165–97.
3 Subcommittee on Advanced Trauma Life Suport of theAmerican College of Surgeons Committee on Trauma1993–1997. Airway and ventilatory management. Advancedtrauma life support program for doctors. American College ofSurgeons, 1997: 75–85.
4 Ali J, Adam RU, Gana TJ. EVect of the prehospital traumalife support program (PHTLS) on prehospital trauma care.J Trauma 1997;42:786–90.
Acute appendicitis: an unusual cause
Q1: Describe the histological featuresHistopathological examination of the appendix(fig 1) shows deposits of adenocarcinoma asso-ciated with acute inflammation. Examinationof the ovary (fig 2) and omentum (fig 3)confirm the presence of papillary adenocarci-noma of the ovary with spread to the omentumas well as the appendix.
Q2: What further treatment is indicated?Total abdominal hysterectomy and leftsalpingo-oophorectomy (right salpingo-oophorectomy and omentectomy having al-ready been performed) to “debulk” the tumourmass, followed by cytotoxic chemotherapy
130 Self assessment answers
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
(with cisplatin and either paclitaxel or cyclo-phosphamide)1 is indicated.
DiscussionEpithelial cancer of the ovary is characterised byexfoliation of malignant cells and early dissemi-nation throughout the peritoneal cavity. Theappendix is a common site of such metastasis,both macroscopically apparent and occult, andappendicectomy is performed by some gynae-cologists as part of surgical staging and to reducetumour burden before chemotherapy. In onestudy of women with epithelial ovarian tumours,39% overall and 49% with FIGO stage III (dis-ease outside the pelvis) or IV (distant metas-tases) had appendiceal secondaries; about onethird of these were occult (that is, microscopiconly).2 In three cases appendices involved withtumour were found to be acutely inflamedmicroscopically, but none of these was sympto-matic. In another series, appendiceal metastaseswere found in 63% overall and in 80% with stageIII or IV ovarian disease.3
The aetiology of appendicitis is not entirelyclear, but obstruction of the lumen is thoughtto play an important part in some cases. Thismay be due to lymphoid tissue, foreign body,or, in an older age group, caecal carcinoma.We have found only one previous report of acase of ovarian carcinoma presenting withacute appendicitis.4 While metastatic ovariancancer is a very rare cause of appendicitis,these cases emphasise the importance of thor-ough examination of the abdomen and pelvisat appendicectomy, even in the presence ofunequivocal appendicitis.
Final diagnosisAcute appendicitis due to metastases frompapillary carcinoma of the ovary.
1 Ozols RF. Paclitaxel plus carboplatin in the treatment ofovarian cancer. Semin Oncol 1999;26:84–9.
2 Ayhan A, Tuncer ZS, Tuncer R, et al. Is routineappendectomy beneficial in the management of ovariancancer? Eur J Obstet Gynecol Reprod Biol 1994;57:29–31.
3 Sonnendecker EW, Margolius KA, Sonnendecker HE.Involvement of the appendix in ovarian epithelialcancer—an update. S Afr Med J 1989;76:667–8.
4 Costello C, Saxton J. Appendicitis and cancer. Postgrad Med1951;9:482–4.
Figure 1 Histological section of appendix (haematoxylin and eosin stain, originalmagnification × 100).
Figure 2 Histological section of right ovary (haematoxylin and eosin stain, originalmagnification × 100).
Learning pointsx Ovarian cancer frequently spreads to
the appendix, resulting inmicrometastases.
x Metastatic ovarian cancer is a very rarecause of acute appendicitis.
x It is important to perform a thoroughlaparotomy in adult cases of acuteappendicitis.
Figure 3 Histological section of omentum (haematoxylinand eosin stain, original magnification × 200).
Self assessment answers 131
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
Is spiral computed tomography theimaging modality of choice for renalcolic?
Q1: What is the diagnosis, and what isspiral computed tomography?The patient was diagnosed as having left sidedrenal colic due to a calculus in her left proximalureter. A spiral computed tomogram allowsimaging of the entire abdomen and pelvis dur-ing one breath hold, eliminating respiratoryartefacts. The entire technique of performingspiral computed tomography takes approxi-mately 30 seconds to complete.
Q2: What are the findings on the spiralcomputed tomogram?A spiral computed tomogram of the abdomenwas performed. No intravenous contrast me-dium was used during the procedure. It showeda normal right renal tract. There was a 6 mmcalculus in the proximal left ureter and an 8mm calculus in the inferior pole calyx of the leftkidney (fig 1; see p 124). These calculi were notvisualised in the intravenous urogram.
Q3: What are the advantages of spiralcomputed tomography in evaluating acase of renal colic?There are several advantages in performing aspiral computed tomogram to evaluate acuteflank pain. As the imaging with spiral computedtomography is performed without contrastmedium, the stones are not masked by the pres-ence of radio-opaque contrast. With conven-tional computed tomography stepwise slices aretaken and therefore it is possible to miss a stone.Spiral computed tomography provides a con-tinuum profile of the urinary tract and thereforeis unlikely to miss a stone. Like an intravenousurogram but unlike an ultrasound scan, a spiralcomputed tomogram gives good imaging of theureter and has the same advantage as an intra-venous urogram to be able to delineate the levelof obstruction. Unenhanced spiral computedtomography is reported to have more than 95%sensitivity and specificity in the diagnosis ofobstructing ureteral calculi. Within the next fewyears spiral computed tomography may replaceintravenous urography in the evaluation of renalcolic.
DiscussionIntravenous urography has been the procedureof choice for evaluation of renal colic since itwas first performed in 1923.1 It provides struc-tural as well as functional information of theurinary tract. In addition it gives us infor-mation regarding the site, degree, and thenature of obstruction. There are a fewdisadvantages with intravenous urography. Theincidence of contrast induced allergic reactionsis 5%–10%.2 3 There is 25% risk of contrastinduced nephrotoxicity in people with pre-existing renal failure and diabetes mellitus.4
Intravenous urography is more time consum-ing. On the other hand spiral computedtomography has several advantages. As theimaging with spiral computed tomography isperformed without contrast medium, thestones are not masked by the presence of
radio-opaque contrast. Total time taken to per-form a spiral computed tomography is less thana minute. Like an intravenous urogram, butunlike an ultrasound scan, a spiral computedtomogram gives good imaging of the ureter andhas the same advantage as an intravenous uro-gram to be able to delineate the level ofobstruction. The sensitivity and specificity ofunenhanced spiral computed tomography inthe diagnosis of renal colic is reported to bemore than 95%.5–7 Evaluation of spiral com-puted tomography and intravenous urographyrevealed comparable radiation dosages andwith a lower gonadal dose provided by the spi-ral computed tomography.8 The main disad-vantage of unenhanced spiral computed tom-ography compared with intravenous urographyis the absence of evaluation of renal functionand the lining epithelium of the urinary tract.Rarely phleboliths in the pelvis could beconfused with ureteral stones on spiral com-puted tomography.1 Osborn ED, Sutherland CG, Scholl AJ, et al. Roentgenogra-
phy of urinary tract during excretion of sodium iodide.JAMA 1923;80:368.
2 Shehadi WM, Toniolo G. Adverse reactions to contrastmedia: a report from the committee on safety of contrastmedia of the International Society of Radiology. Radiology1980;137:299–302.
3 Katayama H, Yamaguchi K, Kozuka T, et al. Adversereactions to ionic and non-ionic contrast media. Radiology1990;175:621–8.
4 Barrett BJ, Carlisle EJ. Metaanalysis of the relative nephro-toxicity of high and low osmolality iodinated contrast media.Radiology 1993;188:171–8.
5 Smith RC, Rosenfield AT, Choe KA, et al. Acute flank pain:comparison of noncontrast-enhanced CT and intravenousurography. Radiology 1995;194:789–94.
6 Sommer FG, JeVrey RB, Rubin GD, et al. Detection of ure-teral calculi in patients with suspected renal colic: value ofreformatted noncontrast helical CT. AJR 1995;165:509.
7 Smith RC, Verga M, McCarthy S, et al. Diagnosis of acuteflank pain: value of unenhanced helical CT. AJR 1996;166:97.
8 Fielding JR, Steele G, Fox LA, et al. Spiral computerisedtomography in the evaluation of acute flank pain: a replace-ment for excretory urography. J Urol 1997;157:2071–3.
Learning points: advantages of spiralcomputed tomographyx No bowel preparation or contrast
medium is requiredx It requires less time than intravenous
urography. Entire technique of spiralcomputed tomography takes approxi-mately 30 seconds
x It scans the entire abdomen and pelvisduring one breath hold, eliminating res-piratory artefacts
x It is highly accurate in identifying thesize and location of ureteral and renalcalculi
x Uric acid calculi could be accuratelydiagnosed
x The degree of obstruction to the kidneycan be assessed by the severity ofhydronephrosis, perinephric, and peri-ureteral stranding and perinephric fluidcollection indicating forniceal rupture
x In addition other abdominal organs canbe evaluated
x Radiation dosage is comparable to that ofintravenous urography (4.6 v 4.4 rad,respectively), with a lower gonadal doseprovided by the spiral computed tomog-raphy
132 Self assessment answers
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
A young woman with intractablediarrhoea
Q1: What is the diagnosis?The diagnosis is a dopamine secreting phaeo-chromocytoma. The abdominal computedtomogram (p 124) shows a left adrenal mass(8 × 6 cm) with haemorrhagic and necroticareas. A 131I-metaiodobenzylguanidine scinti-gram showed uptake in the left adrenal gland.
A histopathologically proved benign phaeo-chromocytoma was resected. Immunohisto-chemical study revealed enhanced expression oftyrosine hydroxylase and low expression ofdopamine â-hydroxylase in the tumour. Thesefindings are consistent with the secretion ofdopamine, as dopamine â-hydroxylase is theenzyme that synthesises norepinephrine fromdopamine. An increased production ofdopamine and homovanillic acid is uncommonwith benign lesions but may occur with malig-nant phaeochromocytoma.1 Over a one weekperiod her diarrhoea subsided. The plasma andurinary dopamine and urinary homovanillic acidconcentrations returned to normal. Her bloodpressure one week later was 140/80 mm Hg.
Q2: What is the cause of diarrhoea?The cessation of diarrhoea after tumour resec-tion suggests that dopamine may cause diar-rhoea, perhaps via D1-like receptors in thegastrointestinal tract.2 Diarrhoea is an uncom-mon sole manifestation of phaeochromocy-toma.3 A literature search revealed only oneother report of dopamine secreting phaeochro-mocytoma presenting solely with diarrhoea.4
Q3: What is the cause for remission of herhypertension?The dopamine receptors in peripheral tissuesare of two functional classes: D1 and D 2-likereceptor. Stimulation of postsynaptic,7 D1-likereceptors or presynaptic D2-like receptorsmay cause vasodilatation.8 Stimulation ofD1-A receptors promotes natriuresis and low-ers blood pressure in humans.9 A deficientrenal dopamine formation or action may con-tribute to hypertension,10 and a deficientdopaminergic response to salt loading mayplay an aetiological part in patients with a saltsensitive form of hypertension.11 D1-A recep-
tor deficient mice have been shown to havehypertension, suggesting a hypotensive actionfrom dopamine.12 This is consistent with thespontaneous lowering of blood pressure ini-tially and the increase in blood pressure afterresection of dopamine secreting phaeochro-mocytoma seen in our patient.13
Follow upTwo months after surgery she continues to beasymptomatic. Her blood pressure is 140/80mm Hg. The urinary 24 hour catecholamines,dopamine, and homovanillic acid of thepatient, her three siblings, and two sons werenormal. The patient and her family are onregular follow up at the endocrinology outpa-tient clinic.
Final diagnosisDopamine secreting benign phaeochromocy-toma.
1 Landsberg L, Young JB. Pheochromocytoma. In: Fauci AS,Braunwald E, Isselbacher KJ, et al, eds. Harrison’s principlesof internal medicine. 14th Ed. New York: McGraw-Hill,1998: 2057–60.
2 Marmon LM, Albrecht FE, Canessa LM, et al. Identifica-tion of dopamine D 1A receptors in the rat small intestine. JSurg Res 1993;54:616–20.
3 Werbel SS, Ober KP. Pheochromocytoma: update ondiagnosis, localization, and management. Med Clin NorthAm 1995;79:131–53.
4 Yasunari K, Kohno M, Yoshikawa J, et al. A dopamine-secreting pheochromocytoma. Am J Med 1999;106:599–600.
5 Takizawa H, Narisawa R, Asakura H. Jejunal invasion ofpheochromocytoma pathologically confirmed by endo-scopic biopsy. Am J Med Sci 1999;371:67–74.
6 Ross EJ, GriYth DNW. The clinical presentation of phaeo-chromocytoma. Q J Med 1989;71:485–96.
7 Yasunari K, Kohno M, Yokokawa K, et al. Dopamine DA1receptors on vascular smooth muscle cells are regulated byglucocorticoid and sodium chloride. Am J Physiol 1994;267:R628–34.
8 Goldberg LI. Cardiovascular and renal actions of dopamine:potential clinical applications. Pharmacol Rev 1972;24:1–29.
9 Carey RM, Stote RM, Dubb JW, et al. Selective peripheraldopamine-1 receptor stimulation with fenoldopam in humanessential hypertension. J Clin Invest 1984;74:2198–207.
10 Aperia A. Dopamine action and metabolism in the kidney.Curr Opin Nephrol Hypertens 1994;3:39–45.
11 Gordon MS, Steunkel CA, Conlin PR, et al. The role ofdopamine in nonmodulating hypertension. J Clin EndocrinolMetab 1989;69:426–32.
12 Albrecht FE, Drago J, Felder RA, et al. Role of the D 1Adopamine receptor in the pathogenesis of genetic hyper-tension. J Clin Invest 1996;97:2283–8.
13 Prey C, Fossti P, Fontaine P, et al. Dopamine secretingpheochromocytoma: an unrecognized entity? Classificationof pheochromocytomas according to their type of secretion.Surgery 1986;100:1154–62.
Box 1: Common mechanisms for loosemotions in phaeochromocytomax Ectopic production by
phaeochromocytoma of: vasoactiveintestinal peptide (watery diarrhoea,hypokalaemia, achlorhydria syndrome);serotonin; somatostatin; calcitonin.
x In phaeochromocytoma as part of multi-ple endocrine neoplasia 2A and 2B syn-dromes; calcitonin, serotonin, andprostaglandin production from medul-lary thyroid carcinoma may lead to diar-rhoea.
x Phaeochromocytoma may be associatedwith gastrinoma of Zollinger-Ellisonsyndrome, leading to presentation withdiarrhoea.
Box 2: Gastrointestinal manifestationsof phaeochromocytoma5 6
x Nausea (with or without vomiting)x Constipationx Abdominal painx Ileusx Pseudo-obstructionx Diarrhoeax Ischaemic enterocolitisx Gastrointestinal bleedingx Cholelithiasisx Acute abdomen with hyperamylasaemiax Hunger
Learning pointIntractable diarrhoea may be the onlymanifestation of a dopamine secretingphaeochromocytoma
Self assessment answers 133
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
A young man with tachycardia
Q1: What is the diVerential diagnosis?The important diVerential diagnosis for airregular broad complex QRS tachycardia is:x Atrial fibrillation with aberrant conductionx Atrial fibrillation with pre-excitationx Atrial fibrillation with pre-existing bundle
branch blockx Polymorphic ventricular tachycardia
Q2: What is the most likely diagnosis?The rapid ventricular rates and the absence ofcardiovascular risk factors should make onesuspect atrial fibrillation with pre-excitation(conduction via the accessory pathway). WolV-Parkinson-White syndrome was confirmed inthis patient in the electrocardiogram takenduring sinus rhythm after treatment.
Q3: How will you manage this patientacutely?In view of the hypotension DC cardioversion isthe best choice.
Q4: What is the long term management?Patients with WolV-Parkinson-White syn-drome with symptomatic arrhythmias, particu-larly life threatening ones like atrial fibrillation,should be referred for radiofrequency ablationfor elimination of the accessory pathway.Flecainide, propafenone, and sotalol are pro-phylactic antiarrhythmic drugs of choice whilethe patient is awaiting the procedure.
DiscussionAtrial fibrillation is the second commonest(10%–30%) arrhythmia in patients with WolV-Parkinson-White syndrome after orthodromicatrioventricular (AV) re-entrant tachycardia(AVRT) which is a narrow QRS regular tachy-cardia almost identical to AV nodal re-entranttachycardia. The cardinal features of atrialfibrillation in WolV-Parkinson-White syn-drome are the irregularity and the rapidventricular rates as well as the varying QRSconfiguration. Ventricular rate is an aggregateof conduction over the normal AV node andaccessory pathways and it can approach 300 to350 beats/min. QRS configuration is deter-mined by the route of atrial impulses which isdependent mainly upon the refractory periodof the accessory pathway.
If the refractory period of the accessorypathway is short, the antegrade conductionoccurs via the accessory pathway to produce anirregular wide QRS tachycardia as in this case,while it is no diVerent from usual atrial fibrilla-tion if conduction takes place via the AV node.Varying degrees of fusion beats can also befound. Short eVective refractory period ofaccessory pathway1 and short R-R intervalbetween consecutive pre-excited complexes2
are associated with rapid ventricular rates thatcan degenerate into ventricular fibrillation3 andsudden death.
The pathogenesis of atrial fibrillation inWolV-Parkinson-White syndrome is poorlyunderstood.4 5 It is more common in patientswith multiple accessory pathways. Though the
accessory pathway is important in the patho-genesis of atrial fibrillation, it is probably notrequired for the initiation of atrial fibrillation6
and the accessory pathway is usually a passivebystander. However some reports suggest thataccessory pathways are branched and can sup-port microre-entry.
Atrial fibrillation is almost always associatedwith concomitant inducible AVRT, and sponta-neous degeneration of AVRT into atrialfibrillation has been reported to represent themost frequent mode of initiation. It is unclearwhy all patients with AVRT do not developatrial fibrillation.7 Intrinsic atrial electrophysi-ological abnormalities5 8 and exaggerated sym-pathoadrenal discharge have all been blamed inthe pathogenesis of atrial fibrillation. Associ-ated abnormalities like mitral valve prolapseand Ebstein’s anomaly9 can be found.
Electrical cardioversion is the treatment ofchoice in pre-excited atrial fibrillation as it candegenerate into ventricular fibrillation. How-ever if haemodynamically well tolerated,chemical cardioversion can be tried. Thoughintravenous flecainide, propafenone, procaina-mide, sotalol, and amiodarone have all beenshown to be eVective in cardioverting pre-excited atrial fibrillation or reducing theventricular rate, class Ic drugs (flecainide andpropafenone) are popular choices. Verapamiland digoxin are contraindicated as they blockconduction via the AV node enhancing con-duction via the accessory pathway therebyactually increasing the ventricular rate. Intra-venous amiodarone should be used withcaution in pre-excited atrial fibrillation asincrease in the ventricular rates and ventricularfibrillation have been reported. Radiofre-quency ablation is the treatment of choice inpatients with symptomatic arrhythmias. It isusually but not always successful in preventingatrial fibrillation. However it will eliminate thelife threatening rapid ventricular rates whichcan be associated with it.
Final diagnosisWolV-Parkinson-White syndrome.
1 Wellens HJJ, Durrer D. WolV-Parkinson-White syndromeand atrial fibrillation. Relation between refractory period ofthe accessory pathway and the ventricular rate during atrialfibrillation. Am J Cardiol 1974;34:777–82.
2 Pieterson AH, et al. Atrial fibrillation in WolV-Parkinson-White syndrome. Am J Cardiol 1992;70:38A–43A.
3 Monteya PT, et al. Ventricular fibrillation in WolV-Parkinson-White syndrome. Eur Heart J 1991;12:144–50.
4 Shakespheare CF, Anderson M, Camm AJ. Pathophysiologyof supraventricular tachycardia. Eur Heart J 1993;14(suppl):2–8.
5 Muraoka Y, Karakawa S, Yamagata T, et al. Dependency onatrial electrophysiological properties of appearance ofparoxysmal atrial fibrillation in patients with WolV-Parkinson-White syndrome: evidence from atrial vulnerab-lity before and after radiofrequency catheter ablation andsurgical cryoablation. Pacing Clin Electrophysiol 1998;21:438–46.
6 Wathen M, Natale A, Wolfe K, et al. Initiation of atrial fibril-lation in the WolV Parkinson syndrome: the importance ofaccessory pathway. Am Heart J 1993;125:753–9.
7 Bauernfeind RA, Wyndham CR, Swiryn SP, et al. Paroxys-mal atrial fibrillation in the WolV-Parkinson-White syn-drome. Am J Cardiol 1981;47:562–9.
8 Michelucci A, Padeletti L, Monizzi D, et al. Atrialelectrophysiological properties of patients with asympto-matic WolV-Parkinson-White syndrome. Eur Heart J1988;9:479–83.
9 Pressley JC, Wharton JM, Tang AS, et al. EVect of Ebstein’sanomaly on short and long term outcome of surgicallytreated patients with WolV-Parkinson-White syndrome. Cir-culation 1992;86:1147–55.
134 Self assessment answers
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
A small axillary nodule—a therapeuticdilemma?
Q1: What is the significance of an axillarynodule in an elderly patient?In an elderly patient, an axillary nodule may bea metastatic deposit from a known or unknownprimary tumour. Axillary lymph node metasta-sis other than breast cancer, especially in males,includes lung, thyroid, gastric, colorectal, andpancreatic malignancy; however, in females thecommonest is ipsilateral breast cancer.1
Q2: What should be the diagnosticmodality in a case of axillary nodule?A suspicious nodule (particularly in an elderlyperson) should always have a histopathologicaldiagnosis by FNAC and/or histopathology.
Q3: What is the treatment modality in acase of axillary nodule with occultmetastasis?Once diagnosed, routine haematological andbiochemical investigations, chest radiography,ultrasonography of the abdomen, and bilateralmammography are undertaken. Additionalinvestigation to locate the exact site of primarytumour is unrewarding.2 In most of the serieson this subject, the sensitivity of mammogra-phy in the identification of the occult lesion isas low as 33%.3 Magnetic resonance imaging(MRI) may be helpful; however, the absence ofabnormality on mammography and MRI doesnot exclude the diagnosis of primary breastcancer. A bone scan may be done as a part ofmetastatic work up.
Total mastectomy and axillary clearance arepractised by the majority of surgeons.4 Recentlysome surgeons have suggested conservative sur-gery with or without radiation therapy.5 Eller-broek et al treated such patients with irradiationalone and showed a 17% five year actuarial riskfor locoregional recurrence.6 Advantagesclaimed are that the breast is preserved and sur-vival is comparable to total mastectomy. Thepresence of extensive tumour burden and multi-focality, even when the disease is clinicallyoccult, may limit breast conservation therapy asit may not be feasible to excise the primary ordeliver a boost dose of radiotherapy to theprimary site. Moreover, in the absence of detailsof the primary tumour and lymph nodal status,it is not possible to evaluate tumour characteris-tics and prescribe adjuvant treatment.
Q4: What are the various histopathologicalconsiderations in such a case?The pathologist should be alerted to the occultprimary in the breast as more sections may berequired to locate the tumour. A primarytumour is identified only in 64%–93% asreported in various series.6 Infiltrating duct car-cinoma is the commonest tumour, while carci-noma in situ is seen in 8%–20% of cases.3 Rosenand Kimmel reported median tumour size of 1.5cm (0.1–6.6 cm).7 Baron et al had noted 45% oftheir cases to be multifocal.3 A study of hormonereceptors may be helpful in confirming the diag-nosis as it is positive in 50%–60% of the casesand a negative result does not exclude breast
carcinoma.3 A positive result can also be seen inother malignancies like renal cell carcinoma,melanoma, and colorectal carcinoma.
DiscussionIn 1907, William Steward Halsted first de-scribed two patients with extensive carcinoma-tous involvement of the axilla caused by occultbreast cancer.8 The incidence of occult carci-noma with axillary nodal metastasis varies from0.35% (35 out of 10 014 patients) at theMemorial Sloan-Kettering Cancer Center to0.5% (60/12 000) at the National CancerInstitute in Milan.3
The commonest cause in females is ipsilateralbreast cancer. No investigations can identify anoccult primary lesion with accuracy. Totalmastectomy and axillary clearance, conservativesurgery with or without radiation, and primaryradiation therapy are the various options avail-able in elderly patients. Total mastectomy andaxillary clearance are undertaken especially inpatients where frequent follow up is not possibleand the patient does not opt for breast conserva-tion treatment. Since studies have shown signifi-cant survival advantage in patients with stage IIbreast cancer after adjuvant therapy, patientswith occult carcinoma metastatic to the axillashould be treated as stage II disease and henceadjuvant systemic therapy instituted.
In an elderly postmenopausal patient onlytamoxifen should be given as a treatmentoption especially in the case of an occult orsmall oestrogen receptor positive primary.
In our patient, no primary focus could bedetected in the large number of sections thatwere studied, although it is not possible for usto completely rule out the presence of a smallfocus in the unexamined parts of the breast.The axillary metastasis was in the centre of theaxilla in the subcutaneous tissue with no meta-static deposit found in the lymph nodes. It isdiYcult to predict whether the tumour waspresent in ectopic breast tissue or part of theaxillary tail or it was an occult primary in thebreast with metastasis to subcutaneous axillarytissue. Carcinoma has also been reported toarise primarily in the ectopic breast tissueinclusions present in an axillary lymph node.9
Our case demonstrated metastasis in thesubcutaneous tissue, a rare event. This casegives an important message; however small a
Learning pointsx A small axillary nodule in an elderly
woman can be metastatic tumour.x A primary tumour is usually found in
the breast; however, at times the pri-mary tumour may be occult.
x Total mastectomy and axillary clearanceare undertaken in the case of an occultprimary in the breast with lymph nodemetastasis where frequent follow up isnot possible and the patient does notopt for breast conservation therapy.
x At times, the primary site is not detectedeven on histopathological examination andsuch cases remain a therapeutic dilemma.
Self assessment answers 135
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
small nodule may be, especially in an elderlypatient, it should not be ignored.
Final diagnosisMetastatic axillary nodule with occult breastcancer.
1 Patel J, NemotoT, Rosner D, et al. Axillary lymph nodemetastasis from an occult breast cancer. Cancer1981;47:2923–7.
2 Osteen RT, Kopf G, Wilson RE. In pursuit of the unknownprimary. Am J Surg 1978;135:494–8.
3 Baron PL, Moore MP, Kinne DW, et al. Occult breast can-cer presenting with axillary metastasis. Arch Surg 1990;25:210–14.
4 Iglehart JD, Ferguson BJ, Shingleton WW. An ultrastruc-tural analysis of breast carcinoma presenting as an isolatedaxillary adenopathy. Ann Surg 1982;196:8–13.
5 Vilcoq JR , Calle R, Ferme F, et al. Conservative treatmentof axillary adenopathy due to probable subclinical breastcancer. Arch Surg 1982;117:1136–8.
6 Ellerbroek N, Holmes F, Singletary E. Treatment of patientswith isolated axillary nodal metastases from an occultprimary consistent with breast origin. Cancer 1990;66:1461–7.
7 Rosen PP, Kimmel M. Occult breast carcinoma presentingwith axillary lymph node metastases: a follow up study of 48patients. Hum Pathol 1990;21:518–23.
8 Halsted WS. The results of radical operations for the cure ofcarcinoma of the breast. Ann Surg 1907;46:1–19.
9 Walker AN, Fechner RE. Papillary carcinoma arising fromectopic breast tissue in an axillary lymph node. Diagn Gyne-col Obstet 1982;4:141–5.
A farmer with artificial valveendocarditis
Q1: What are the most commonorganisms causing artificial valveendocarditis? What are other lesscommon organisms should beconsidered?The most common aetiological organism isStaphylococcus epidermidis which accounts for29% of both early and late onset endocarditis,followed by viridans streptococci (17%), Sta-phylococcus aureus (14%), and enterococci(7%).1 Aerobic Gram negative bacilli, diph-theroids including corynebacterium Jeikeium,and fungi especially candida and asperigillusspecies uncommon in native valve endocarditisare important causes of early prosthetic valveendocarditis.1
Less common organisms include Coxiellaburnetii, Brucella spp, and the HACEK group.1
Q2: How should the diagnosis beestablished?Relapsing brucella bacteraemia after appropri-ate treatment for acute brucellosis is an impor-tant clue for the diagnosis of brucella endocar-ditis in patients who have prosthetic valves.2 Anepidemiological and exposure history is essen-tial and usually helpful in the diagnosis. Ourpatient was a farmer who kept animals likegoats in his farm. Diagnosis depends on isola-tion of brucella from blood culture and/or car-diac tissues. Serology is also helpful. Thestandard tube agglutination test is sensitive andspecific. A titre of 1:160 or more is presumptiveevidence of brucella infection. Echocardio-graphy especially transoesophageal echo-cardiography may be useful in detectingvegetations, prosthesis detachment, and
perivalvular abscess. Other indications includeanaemia, haematuria, and a high ESR.
Q3: What would be the best therapeuticapproach?Treatment for brucella endocarditis has notbeen well established, due basically to the lownumber of reported cases. Brucella organismsare susceptible to a variety of antibioticsincluding aminoglycosides, tetracyclines, chlo-ramphenicol, quinolones, macrolides, ri-fampin, and trimethoprim-sulfamethoxazole(TMP-SMZ).3 Most patients with brucellaendocarditis are treated with combinationantibiotics including tetracycline, streptomy-cin, rifampin, and/or TMP-SMZ. The bestcombination of antibiotics is not known. Someauthors suggested a combination of doxycy-cline, rifampin, and streptomycin,3 however theinterference of rifampin with the anticoagulantactivity of warfarin and related drugs, and theinconvenience of intramuscular streptomycininjection makes this combination less attrac-tive. Prosthetic valve endocarditis caused bybrucella is a primary indication for surgery4; ithas never been cured with antibiotics alone. Allreported patients had combined medical andsurgical treatment. Our patient underwentvalve replacement four days after the start ofantibiotic treatment. The optimal duration ofantimicrobial therapy for brucella endocarditisis unknown. However it seems advisable toextend antibiotic treatment for a minimum of12 weeks postoperatively. A progressive drop inantibody titre, and a negative mercaptoethanoltitre, points toward a bacteriological cure;patients who have a relapse or fail treatmentpersist with high concentrations of IgG resist-ant to mercaptoethanol.4
DiscussionBrucellosis is a zoonosis with a worldwide dis-tribution, especially in the Mediterraneanbasin, the Arabian Peninsula, the Indiansubcontinent, Mexico, Central and SouthAmerica.2 It is a systemic disease, and almostevery organ can be aVected. The infectionusually manifests itself as a febrile syndromewith no apparent focus, chills, sweating,arthralgia, and myalgia. About 30% of patientssuVer from some localisation, most commonlybone and joint involvement.1 Brucella endo-carditis is rare occurring in fewer than 2% ofpatients with brucellosis.1 Prosthetic valveendocarditis caused by brucella species is veryrare. Brucella abortus, B suis, and B melitensishave been reported to cause endocarditis.Brucella endocarditis produces highly de-structive lesions of the valve structure.5 It usu-ally involves a previously healthy native valve.The aortic valve is involved in more than 75%of cases. Mitral involvement occurs morerarely and usually aVects a previously dam-aged valve.5 The valvular lesions have beendescribed as bulky and ulcerative with grossabscesses of the myocardium, microabscesseswithin the cusps, destruction of commissures,and calcifications.6 These observations might
136 Self assessment answers
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
explain the high fatality rate for brucella endo-carditis. Although the mortality rate forbrucellosis is less than 1%, endocarditisaccounts for 80% of these deaths.6 Thecomplication, which is responsible for themajority of deaths, is heart failure.6 Major sys-temic emboli in contrast to other causes ofprosthetic valve endocarditis were rare; thishas been attributed to the tendency ofinfection to cause fibrosis, hyalinisation, andcalcification, rather than large vegetations.2 6
Diagnosis depend on isolation of brucellafrom blood culture or cardiac tissue, which arepositive in 80% of cases. Combined antibioticand surgical treatment is the best approach fortreating brucella prosthetic valve endocarditisas the mortality rate is less than for medicaltreatment alone, and infection of the newprosthesis that has been placed is low.1
Final diagnosisBrucella prosthetic valve endocarditis.
1 Threlkeld MG, Cobbs CG. Infectious disorders of prostheticvalves and intravascular devices. In: Mandel GL, Douglas RG,Bennet JE, eds. Principles and practice of infectious diseases.Edinburgh: Churchill Livingstone, 1990: 706–15.
2 Fernandez-Guerrero ML. Zoonotic endocarditis. Infect DisClin North Am 1993;7:135–41.
3 Mortensen JE, Moore DG, Clarridge JE, et al. Antimicrobialsusceptibility of clinical isolates of brucella. Diagn MicrobiolInfect Dis 1986;5:163–9.
4 Fernandez-Guerrero ML, Martinell J, Aguado JM, et al.Prosthetic valve endocarditis caused by Brucella melitensis:a report of four successfully treated with tetracycline, strep-tomycin, and sulfamethoxazole and trimethoprim plus valvereplacement. Arch Intern Med 1987;147:1141–3.
5 Colmenero JD, Reguera JM, Martos F, et al. Complicationsassociated with Brucella melitensis infection: a study of 530cases. Medicine (Baltimore) 1996;75:195–211.
6 Peery TM, Belter LF. Brucellosis and heart disease: II. Fatalbrucellosis. Am J Pathol 1960;36:673–97.
Loss of weight in a female heavy smokerwith diVuse interstitial pulmonaryfibrosis
Q1: What does the chest radiograph in fig2 (see p 127) show?In addition to the diVuse interstitial pulmonaryfibrosis (DIPF), there is an irregular left upperlobe opacity and apical pleural fibrosis.
Q2: Suggest two causes that wouldexplain the new radiological finding in fig2 (see p 127)Pulmonary tuberculosis and lung cancer arethe two most likely causes of an opacity in theupper lobe of the lung.
Q3: What three further investigationswould you request?Sputum culture for acid-fast bacilli, sputumcytology for malignant cells, and high resolu-tion computed tomography of the chest.
Sputum culture showed mycobacteriumtuberculosis that was sensitive to rifampicin,ethambutol and streptomycin, but resistant toisoniazid. Sputum cytological examination ofthree specimens revealed squamous cell carci-noma. High resolution computed tomographyconfirmed DIPF with honeycomb reticulationand ground glass opacity. A large irregular
cavitating mass was apparent in the anteriorsegment of the left upper lobe (fig 3 below).
Q4: What is the final diagnosis and whatis the relative risk of its development inpatients with diVuse interstitialpulmonary fibrosis?Lung cancer with DIPF. It is well establishedthat the occurrence of lung cancer is greatlyincreased in patients with DIPF.1 2 There is anexcess relative risk of 14.1 of lung cancer inpatients with DIPF compared with the generalpopulation of comparable age and sex.3 Thedevelopment of lung cancer in DIPF seems tobe related to DIPF itself, apart from smokingand no predicting factors for its developmentin the presence of DIPF have been identified.3
Lung cancer in this setting occurs predomi-nantly in males, in smokers, in the lower lobes,and in the peripheral regions of the lung.2
Q5: In your opinion, what is the majorrisk factor for the final diagnosis in thiscase?Cigarette smoking is the most important singleaetiological factor in the development of lungcancer. The patient was an elderly women whosmoked heavily for more than 50 years, andhad a longstanding history of DIPF. Thesquamous cell carcinoma she developed was inthe left upper lobe and was most probably theresult of her heavy smoking. Her DIPF mayhave been a contributory factor.
Clinical courseThe patient was considered unfit for surgicalexcision or therapeutic irradiation of herneoplasm, because of her pre-existing pulmo-nary fibrosis. She failed to respond to aquadruple regimen of antituberculous therapy(including rifampicin, pyrazinamide, ethambu-tol, and ciprofloxacin; streptomycin was notprescribed because she had renal impairmentduring her illness). She died 3.5 months afteradmission. There was no necropsy.
Figure 3 Computed tomography showing a large irregularcavitating mass in the anterior segment of the left upperlobe.
Self assessment answers 137
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/
-
DiscussionAlthough the association of lung cancer andDIPF is well established,3–5 little attention hasbeen given to it. In comparison with the generalpopulation of lung cancer patients, lung cancerassociated with DIPF occurs more commonlyin males, and in smokers, and is predominantlylocated in the lower lobes and peripheralregions of the lungs.2 The precise role of DIPFas a predisposing factor for lung cancer isspeculative. The fact that lung cancer occursmore frequently in the lower lobes where fibro-sis is predominant supports the view that fibro-sis and carcinoma are closely related. Bronchialsquamous metaplasia as a precancerous state inDIPF is well recognised.2 Transition fromatypical squamous metaplasia to carcinomaand anatomical correlation between sites offibrosis and the carcinoma has been demon-strated in some instances.1
The simultaneous occurrence of lung cancerand pulmonary tuberculosis has been reported
by several authors.6–10 In a review of associatedlesions in patients with lung cancer,11 pulmo-nary tuberculosis was the most frequent lesion,followed by scars, emphysema, and thickenedpleura. A firm aetiological relationship betweenlung cancer and pulmonary tuberculosis hasnot, however, been established and recentanalyses suggest that the association may becoincidental. When lung cancer does coexistwith pulmonary tuberculosis, the diagnosis istypically delayed.7–10
Final diagnosisLung cancer with diVuse interstitial pulmonaryfibrosis and pulmonary tuberculosis.
1 Fraire AE, Greenberg SD. Carcinoma and diVuse interstitialfibrosis of lung. Cancer 1973;31:1078–86.
2 Mizushima Y, Kobayashi M. Clinical characteristics of syn-chronous multiple lung cancer associated with idiopathicpulmonary fibrosis. A review of Japanese cases. Chest 1995;108:1272–7.
3 Turner-Warwick M, Lebowitz M, Burrows B, et al.Cryptogenic fibrosing alveolitis and lung cancer. Thorax1980;35:496–9.
4 Callahan WP, Sutherland JC, Fulton JK, et al. Acute diVuseinterstitial fibrosis of lungs. Arch Intern Med 1952;90:468–82.
5 GriYn JP. Interstitial pulmonary fibrosis and cancer. Chest1995;108:1193.
6 Sakai T, Ikeda T, Nishimura Y, et al. A case of coexistentbronchogenic carcinoma with pulmonary tuberculosis.Kekkaku 1992;67:409–12 [abstract].
7 Fujisawa N, Nagao R, Kimoto K, et al. Study of two cases ofactive pulmonary tuberculosis complicated by lung cancer.Kekkaku 1994;69:323–8 [abstract].
8 Martinez ME, Aparicio UJ, Cordero RP, et al. Coexistenceof bronchogenic carcinoma and active pulmonary tubercu-losis. Arch Bronchoneumol 1995;31:32–4 [abstract].
9 Nonaka M, Kadokura M, Tanio N, et al. Surgical problem oflung cancer with coexisting acute pulmonary tuberculosis.Kyobu Geka 1995;48:1019–24 [abstract].
10 Svane S. Simultaneous pulmonary tuberculosis and bron-chial cancer. A diagnostic pitfall. Tidsskr Nor Laegeforen1996;116:1318–19 [abstract].
11 Dacosta NA, Kinare SG. Association of lung carcinoma andtuberculosis. J Postgrad Med 1991;37:185–9.
Learning pointsx The association of diVuse interstitial
pulmonary fibrosis and lung cancer iswell established
x Lung cancer associated with DIPFoccurs more in males, in smokers, in thelower lobes, and in the peripheralregions of the lung
x Cigarette smoking acts as an additiverisk factor for the development of lungcancer in patients with DIPF
x Clinical and radiological screening isimportant in patients with DIPF
138 Self assessment answers
www.postgradmedj.com
on July 6, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pmj.77.904.124a on 1 F
ebruary 2001. Dow
nloaded from
http://pmj.bmj.com/