
Recurrence of Leiomyomata (cont’d)
44
Recurrence of Leiomyomata (cont’d) Indeed, between 10% and 25% of women undergoing myomectomies require another surgical procedure within the next decade.
-
Upload
aubrey-allen -
Category
Documents
-
view
43 -
download
1
description
Recurrence of Leiomyomata (cont’d). Indeed, between 10% and 25% of women undergoing myomectomies require another surgical procedure within the next decade. Recurrence of Leiomyomata (cont’d). - PowerPoint PPT Presentation
Transcript of Recurrence of Leiomyomata (cont’d)
Recurrence of Leiomyomata (cont’d)
Indeed, between 10% and 25% of women undergoing myomectomies require another surgical procedure within the next decade.
Recurrence of Leiomyomata (cont’d)
Isolated large fibroids have lower recurrence rates than when multiple small tumors are present, despite an overall smaller volume of leiomyomata .

Postoperative Pelvic AdhesionsThe frequency of postoperative adhesions following
myomectomy exceeds 50% and can result in reduced fertility, pain, or bowel obstruction.
Careful surgical technique to minimize the degree of surgical trauma,
confining the incisions to the anterior uterine surface so as to prevent contact with the bowel and adnexal structures, and
covering the posterior uterine incisions with surgical barriers ,
have been advocated to minimize the rate of postoperative adhesions.

Non-extirpative Options
Myolysis UAE MRI-guided HIFUMedically induced hypogonadism GnRH agonist GnRH agonist with “add-back” therapy
Medical Suppression
Many medicinal agents have been considered for the treatment of symptomatic leiomyomata, including:
1.estrogen antagonists, 2.progesterone antagonists (mifepristone),
3.androgens (danazol), 4.pituitary down-regulation with GnRH
agonists.
Medical Suppression (cont’d)
Hypogonadism cannot be sustained for a prolonged interval because of the significant side effects such as:
vasomotor hot flashes, accelerated bone loss, genital tract atrophy, and loss of the cardiovascular protection.

Medical Suppression (cont’d)
The important question to ask is, “What is the goal of medical suppression?”
Currently, the most relevant clinical use of GnRH agonists is to stop excessive vaginal bleeding and improve the hemogram prior to surgery or in order to delay surgery to correct other medical problems that are posing an increased surgical risk.
Myolysis
There have been many attempts at inducing therapeutic necrosis of cells within the center of a fibroid (e.g., myolysis), thereby shrinking the tumor size, relieving symptoms, and preventing progressive growth of the tumors.

Myolysis (cont’d)
• The aseptic necrosis may cause significant pain in the immediate post-treatment interval, comparable to that observed with degeneration of leiomyomata seen in pregnancy.

Myolysis (cont’d)
Myolysis should be confined to those women who are not interested in subsequent pregnancy until well-designed, long-term comparative trials demonstrate safety.
Uterine Artery Embolization
When menorrhagia is the primary clinical symptom and either the surgical risk is judged unacceptable or the patient declines extirpative surgery, therapeutic embolization of the uterine arteries can be utilized to reduce symptoms. This strategy is to simultaneously deprive the uterus and the fibroids of their blood supply, induce necrosis, and reduce the symptoms .

UAE (cont’d)
Since UAE has only been widely utilized for only slightly over a decade, the long-term safety and efficacy remain to be demonstrated.


14
Adenomyosis

15
Definition
A benign uterine condition in which endometrial glands and stroma are present within the uterine musculature

16
Etiology
• The cause of adenomyosis is unknown• uterine trauma – caesarean section– tubal ligation– pregnancy
• Basal endometrial hyperplasia invading a hyperplastic myometrial stroma.

Four primary theories
HeredityTraumaHyperestrogenemiaViral transmission
17

18

19

20

21
The thickened and spongy appearing myometrial
wall of this sectioned uterus is typical of adenomyosis. There is also a small white leiomyoma at the lower left.

Adenomyosis, Hysterectomy Specimen
22

23

• Adenomyosis correlates with abnormal amounts of multiple substances, possibly indicating a causative link in its pathogenesis:
– Endometrial IL-18 receptor mRNA and the ratio of IL-18 binding protein to IL-18 are significantly increased in adenomyosis patients in comparison to normal people
24

25
Clinical features1• Asymptomatic
• Classic symptoms: secondary dysmenorrhea abnormal uterine bleeding• Chronic pelvic pain may occur

26
Clinical features2:• Most common physical sign a diffusely enlarged uterus • particularly tender during menstruation

27
Diagnosis:• History• Pelvic examinations• Ultrasonography• MRI• Serum markersCA-125 • definitive diagnosis can only be made from
histological examination of a hysterectomy specimen

28
Treatment
• Hormone therapy• NSAIDs• Hysterectomy the only uniformly
successful treatment for adenomyosis is necessary.
Endometrial polyps
29
Definition
• Benign localised overgrowth of endometrial glands and stroma, covered by epithelium, projecting above the adjacent epithelium
30

epidemiology• 12-80 Years old• Most occur in women in their 40s and 50s• Endometrial polyps occur in up to 10% of
women• It is estimated that they are present in 25% of
women with abnormal vaginal bleeding• Large endometrial polyps can also be
associated with tamoxifen use(associated with a higher risk of neoplasia and different molecular alterations)
31

Risk factors
• Risk factors include
• obesity• high blood pressure• history of cervical polyps• tamoxifen• hormone replacement therapy
32

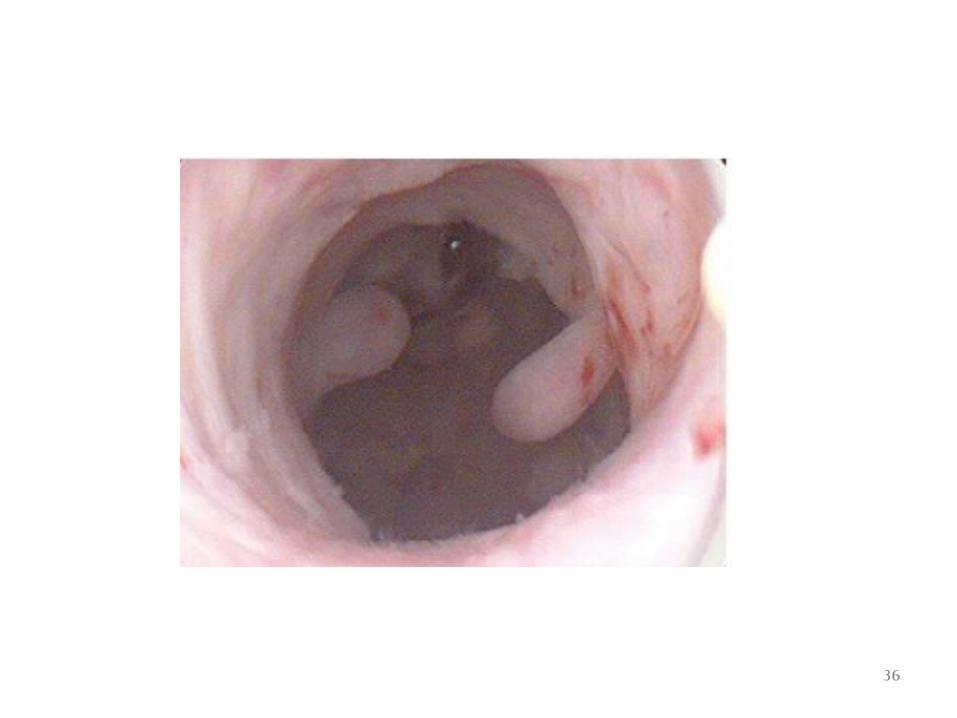
Pathological findings• Sessile or pedunculated• Size: 1mm and beyond – may fill the endometrial
cavity and project through the cervical os• red/brown color ,large ones can appear to be a
darker red• May be multiple• May originate anywhere, but most commonly
fundus
33
etiology
• No definitive cause of endometrial polyps is known
• affected by hormone levels and grow in response to circulating estrogen
34

35
36
37

38

symptoms
• They often cause no symptoms• Where they occur, symptoms include – "spotting" between menstrual periods, or after
menopause– irregular menstrual bleeding– bleeding between menstrual periods– excessively heavy menstrual bleeding – vaginal bleeding after menopause– If the polyp protrudes through the cervix into the
vagina, pain (dysmenorrhea) may result 39

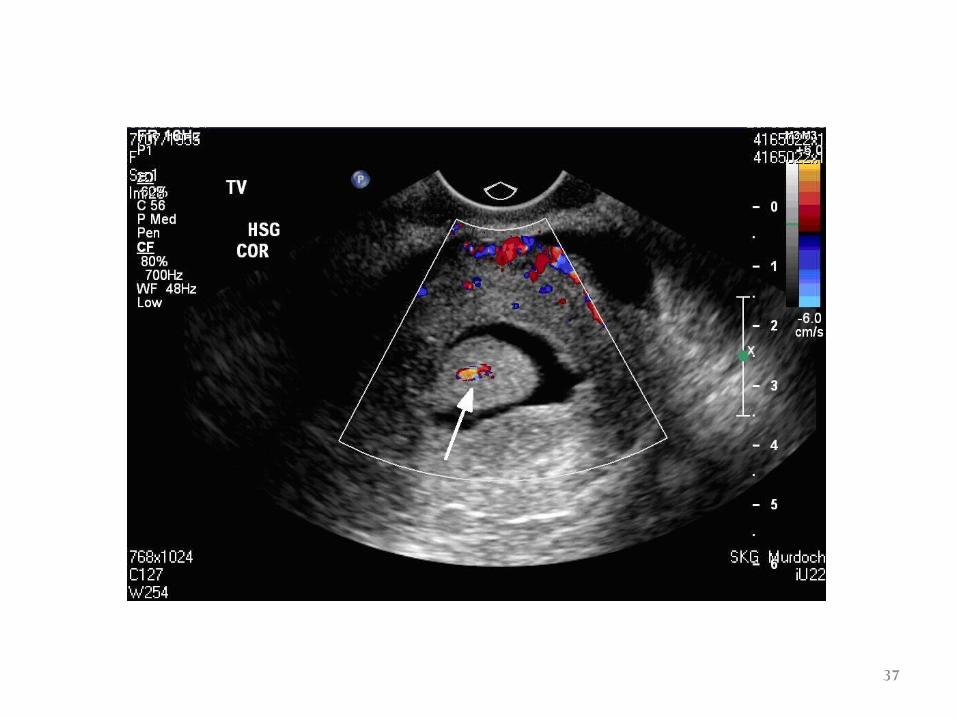
Diagnosis
• vaginal ultrasound (sonohysterography)
• hysteroscopy
• dilation and curettage
40
Treatment
• IntraUterine System containing levonorgestrel in women taking Tamoxifen may reduce the incidence of polyps
• Polyps can be surgically removed using curettage or hysterescopy
• If it is a large polyp, it can be cut into sections before each section is removed
• If cancerous cells are discovered, a hysterectomy may be performed
41

42

Prognosis and complications
• Endometrial polyps are usually benign although some may be precancerous or cancerous
• About 0.5% of endometrial polyps contain adenocarcinoma cells
• Polyps can increase the risk of miscarriage in women undergoing IVF treatment
• Although treatments such as hysterescopy usually cure the polyp concerned, recurrence of endometrial polyps is frequent
• Untreated, small polyps may regress on their own
43

44


















