RECORD OF TRAINING AND EXPERIENCE OF ......RECORD OF TRAINING AND EXPERIENCE OF PROVISIONALLY...
74
COMMUNITY PHARMACY RECORD OF TRAINING AND EXPERIENCE OF PROVISIONALLY REGISTERED PHARMACIST (PRP) PHARMACY BOARD MALAYSIA 1 MINISTRY OF HEALTH MALAYSIA 2017
Transcript of RECORD OF TRAINING AND EXPERIENCE OF ......RECORD OF TRAINING AND EXPERIENCE OF PROVISIONALLY...
COMMUNITY PHARMACY
RECORD OF TRAINING AND EXPERIENCE OF
PROVISIONALLY REGISTERED PHARMACIST
(PRP)
PHARMACY BOARD MALAYSIA
1 MINISTRY OF HEALTH MALAYSIA
2017
PERSONAL PARTICULARS
(TO BE COMPLETED BY PROVISIONALLY REGISTERED PHARMACIST – PRP)
1. Name as in Identification Card (in capital letter) : 2. I/C Number : 3. Provisional Registration Number: 4. Telephone Number: 5. Mobile Phone Number: 6. Home Address : 7. Correspondence Address (if not the same as above): 8. E-mail Address : 9. Qualification (Degree awarded/University/Year) : 10. Scholarship/Sponsor Federal/MARA/PTPTN/Others) : 11. Principal Training Place : 12. Commencement Date: 13. Name & Contact Number of Person in case of emergency
I confirm that the above information is true.
Signature : Date:
Name :
2
Community Pharmacy
1. INTRODUCTION
1.1 The Registration of Pharmacists Act (Amendment) 2003 stipulates that a person who is provisionally registered shall be required to obtain experience immediately upon being provisionally registered, engage in employment as a pharmacist to the satisfaction of the Pharmacy Board for a period of not less than one year.
1.2 The engagement as a pharmacist must be in any premises accredited and approved by Pharmacy Board Malaysia (PBM).
1.3 The PBM may extend for not more than one year the period of training of a provisionally registered pharmacist (PRP) if the Board is not satisfied with the performance of that person as a pharmacist.
1.4 The provisional registration of a person shall be revoked if that person fails to engage in employment as a PRP to the satisfaction of the Pharmacy Board for a period of not less than 52 weeks in any premises accredited and approved by PBM.
1.5 All PRPs are required to pass the Qualifying Examination To Practice Pharmacy conducted by the Pharmacy Board of Malaysia.
3
Community Pharmacy
2. PRP TRAINING MODULES AND RECORD
2.1 This record book is designed primarily to guide PRP and preceptors of
various pharmacy disciplines in the training organization in coordinating
activities and programmes during the 52 weeks of training.
2.2 This record book will be the basis for the appraisal by all preceptors, which
will be submitted to the PBM for the purpose of registration as a Fully
Registered Pharmacist (FRP).
2.3 There are 6 main areas of training for the PRP; 2.3.1 Public Hospital
2.3.2 Community Pharmacy
2.3.3 Private hospital
2.3.4 Research and Development (Academia)
2.3.5 Manufacturing Pharmaceutical Industry
2.3.6 Non- Manufacturing Pharmaceutical Industry
2.4 The PRP is required to fill the following information;
2.4.1 Name, I/C Number, Name of organizations and period of training.
2.4.2 Date of task completed and evidence of proof for each section/unit of attachment. If the column is not enough, please make attachment.
2.4.3 Each evidence given is to be endorsed by the immediate preceptor/s of the section/unit
2.5 The preceptor is required to complete the record by filling the following;
2.5.1 Endorse the completion of each task with signature, name and date in the column provided.
2.5.2 Level of performance is based on the following scale;
Scale Rating Description
9 – 10 Excellent
Performance represents an extraordinary level of achievement and commitment in terms of quality and time, technical skills and knowledge, ingenuity, creativity and initiative.
7 – 8 Good Performance exceeded expectation. All goals, objectives and targets were achieved above the established standards.
5 – 6 Satisfactory Performance met expectations in terms of quality of work, efficiency and timeliness
2.5.3 The passing mark is 60 % for each respective section. The overall
average should be not less than 60%.
2.5.4 The final appraisal and Appendix A or Appendix A1 should be completed by the Master Preceptor at the end of the 12th month of the training period. The original log book with completed appraisal and Appendix A or Appendix A1 need to be sent to PBM addressed as below by the preceptor within ONE month from the end date of the PRP training:
Setiausaha Lembaga Farmasi Malaysia Bahagian Perkhidmatan Farmasi Kementerian Kesihatan Malaysia Lot 36, Jalan Universiti
Scale Rating Description
3 – 4 Unsatisfactory Performance failed to meet expectations and/or one or more of the targets were not met
1 – 2 Poor
Performance was consistently below expectations and/or reasonable progress towards achieving goals was ot made. Significant improvement is needed in one or more areas.
46350 PETALING JAYA
Community Pharmacy
3. DUTIES AND RESPONSIBILITIES OF A PRECEPTOR
3.1 CRITERIA OF A PRECEPTOR
3.1.1 Not less than three years of experience as a registered practicing pharmacist in community pharmacy and holds at least one year Type A poison license prior to training a PRP
3.1.2 Fulfill other criteria set by PBM
3.2 Responsibilities of a Preceptor;
3.2.1 To be a learning resource for the PRP who receives necessary training to develop skills and competencies as a community pharmacist.
3.2.2 To guide the PRP throughout 52 weeks of training.
3.2.3 To be a role model as a professional pharmacist to the PRP
3.2.4 To provide professional services and constructive feedbacks during the training.
3.2.5 To assess PRP performances during the training period.
3.2.6 To comply to the Preceptor to PRP ratio set by PBM.
6
Community Pharmacy
4. DUTIES AND RESPONSIBILITIES OF A PROVISIONALLY REGISTERED PHARMACIST [PRP]
Being a Provisionally Registered Pharmacist [PRP], you should;
4.1 At all-times comply with the directives and orders given to you by the preceptor.
4.2 Aim to become a competent registered pharmacist by the end of the training period.
4.3 Undertake the training modules/ program with a positive attitude and a commitment to learn from the preceptor and other staff in the training environment.
4.4 Remember that obtaining adequate working experience is your responsibility. Others will help, but it requires a conscientious effort on your own part, not just passive acceptance.
4.5 Recognize that not all of the preceptor’s time can be devoted to teaching, and you should therefore actively acquire knowledge and skills by observation, reading and questioning others.
4.6 Be aware that, in addition to the daily activities, your time should be set aside to consider activities outside working/office hours.
4.7 Always actively participate in professional development as it is essential to build on your undergraduate studies and keep abreast of current knowledge.
4.8 Be aware that the Certificate of Satisfactory Experience, required under Section 6A(2) Registration of Pharmacists Act (Amendment) 2003 will only be issued to you if the average passing mark of your training performance must be at least 60% for each section and the sum total of all the units.
4.9 Overview Of Competencies Training Schedule:
During the entire training duration, the PRP will be placed in the core Divisions/Departments in the Company under the guidance and supervision of the Department/Division Head (practicing supervisor) and supervised overall by the preceptor. The duration of training in each module is as indicated in Table 1
5.0 At least ONE (1) mini project need to be done compulsorily and the topic selection will be in the interest of the PRP and preceptor.
7
Community Pharmacy
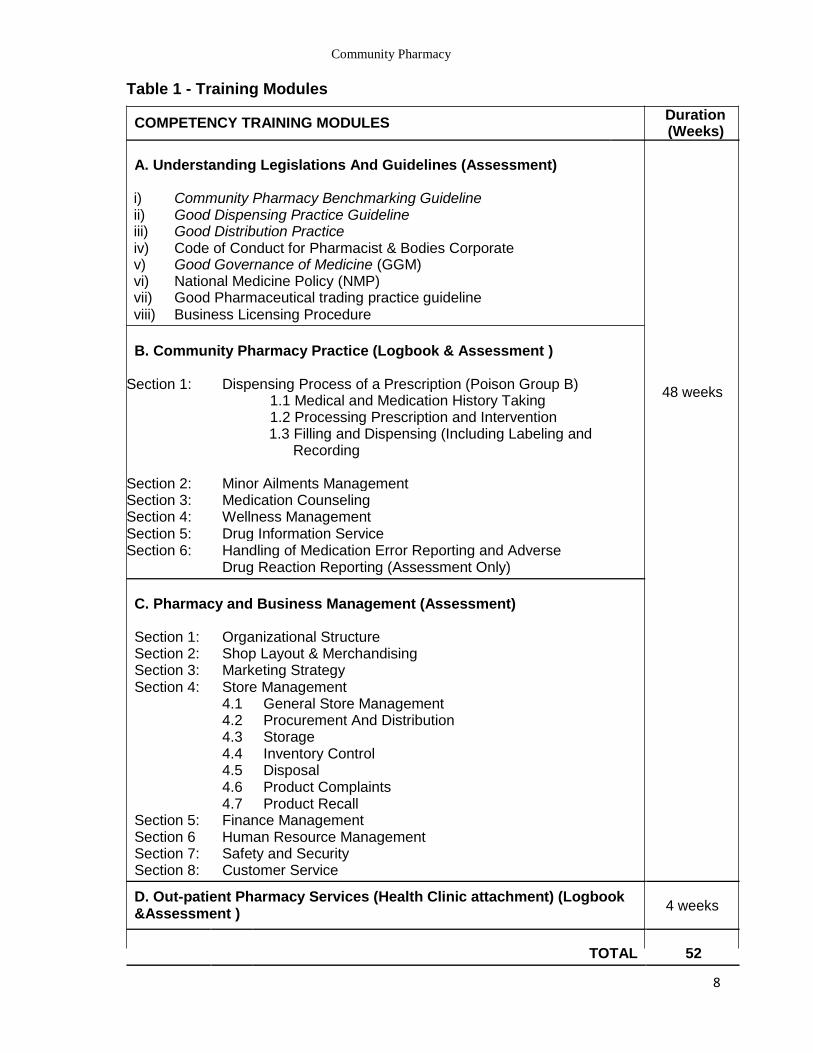
Table 1 - Training Modules
COMPETENCY TRAINING MODULES Duration (Weeks)
A. Understanding Legislations And Guidelines (Assessment)
i) Community Pharmacy Benchmarking Guideline ii) Good Dispensing Practice Guideline iii) Good Distribution Practice iv) Code of Conduct for Pharmacist & Bodies Corporate v) Good Governance of Medicine (GGM) vi) National Medicine Policy (NMP) vii) Good Pharmaceutical trading practice guideline viii) Business Licensing Procedure
B. Community Pharmacy Practice (Logbook & Assessment )
Section 1: Dispensing Process of a Prescription (Poison Group B) 48 weeks
1.1 Medical and Medication History Taking 1.2 Processing Prescription and Intervention 1.3 Filling and Dispensing (Including Labeling and
Recording
Section 2: Minor Ailments Management
Section 3: Medication Counseling
Section 4: Wellness Management
Section 5: Drug Information Service
Section 6: Handling of Medication Error Reporting and Adverse
Drug Reaction Reporting (Assessment Only)
C. Pharmacy and Business Management (Assessment)
Section 1: Organizational Structure Section 2: Shop Layout & Merchandising
Section 3: Marketing Strategy
Section 4: Store Management
4.1 General Store Management
4.2 Procurement And Distribution
4.3 Storage
4.4 Inventory Control
4.5 Disposal
4.6 Product Complaints
4.7 Product Recall
Section 5: Finance Management
Section 6 Human Resource Management
Section 7: Safety and Security
Section 8: Customer Service
D. Out-patient Pharmacy Services (Health Clinic attachment) (Logbook 4 weeks
&Assessment )
TOTAL 52
8
Community Pharmacy
LOG BOOK
9
Community Pharmacy
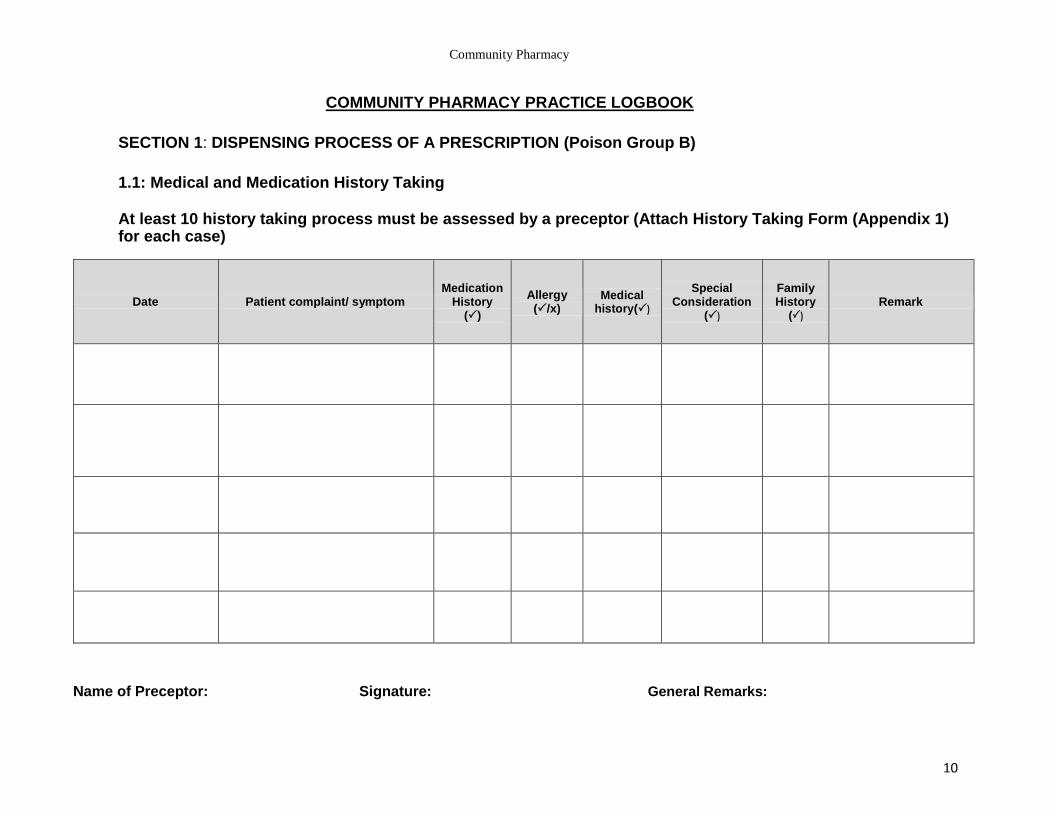
COMMUNITY PHARMACY PRACTICE LOGBOOK
SECTION 1: DISPENSING PROCESS OF A PRESCRIPTION (Poison Group B)
1.1: Medical and Medication History Taking
At least 10 history taking process must be assessed by a preceptor (Attach History Taking Form (Appendix 1) for each case)
Date Patient complaint/ symptom Medication
History ()
Allergy (/x)
Medical history()
Special Consideration
()
Family History
() Remark
Name of Preceptor: Signature: General Remarks:
10
Community Pharmacy
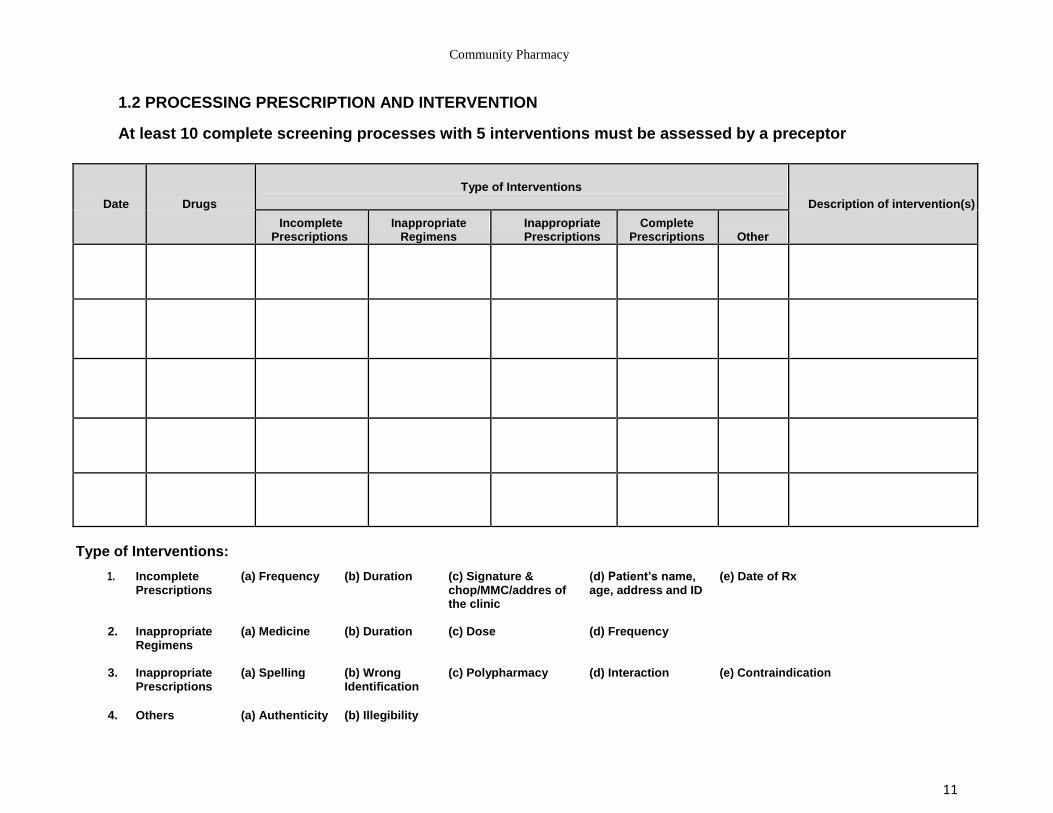
1.2 PROCESSING PRESCRIPTION AND INTERVENTION
At least 10 complete screening processes with 5 interventions must be assessed by a preceptor
Date Drugs Type of Interventions
Description of intervention(s)
Incomplete Prescriptions
Inappropriate Regimens
Inappropriate Prescriptions
Complete Prescriptions Other
Type of Interventions:
1. Incomplete (a) Frequency (b) Duration (c) Signature & (d) Patient’s name, (e) Date of Rx Prescriptions chop/MMC/addres of age, address and ID
the clinic
2. Inappropriate (a) Medicine (b) Duration (c) Dose (d) Frequency Regimens
3. Inappropriate (a) Spelling (b) Wrong (c) Polypharmacy (d) Interaction (e) Contraindication Prescriptions Identification
4. Others (a) Authenticity (b) Illegibility
11
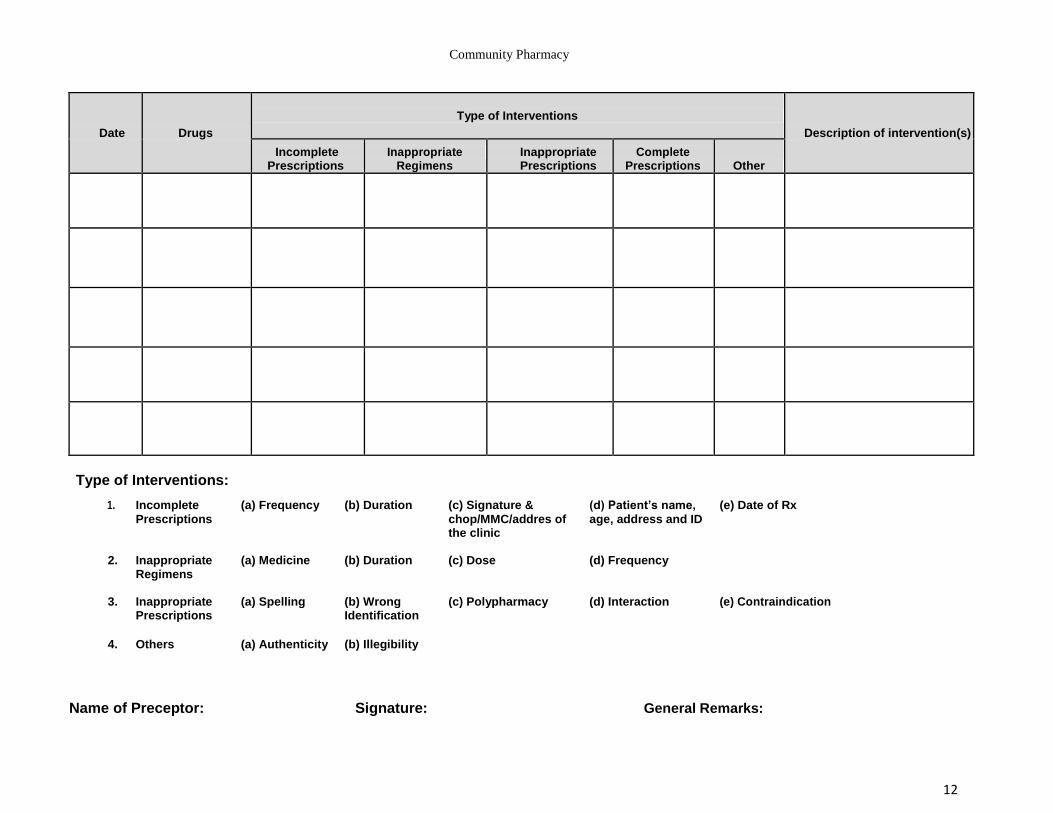
Community Pharmacy
Date Drugs Type of Interventions
Description of intervention(s)
Incomplete Prescriptions
Inappropriate Regimens
Inappropriate Prescriptions
Complete Prescriptions Other
Type of Interventions:
1. Incomplete (a) Frequency (b) Duration (c) Signature & (d) Patient’s name, (e) Date of Rx
Prescriptions chop/MMC/addres of age, address and ID
the clinic
2. Inappropriate (a) Medicine (b) Duration (c) Dose (d) Frequency Regimens
3. Inappropriate (a) Spelling (b) Wrong (c) Polypharmacy (d) Interaction (e) Contraindication Prescriptions Identification
4. Others (a) Authenticity (b) Illegibility
Name of Preceptor: Signature: General Remarks:
12
Community Pharmacy
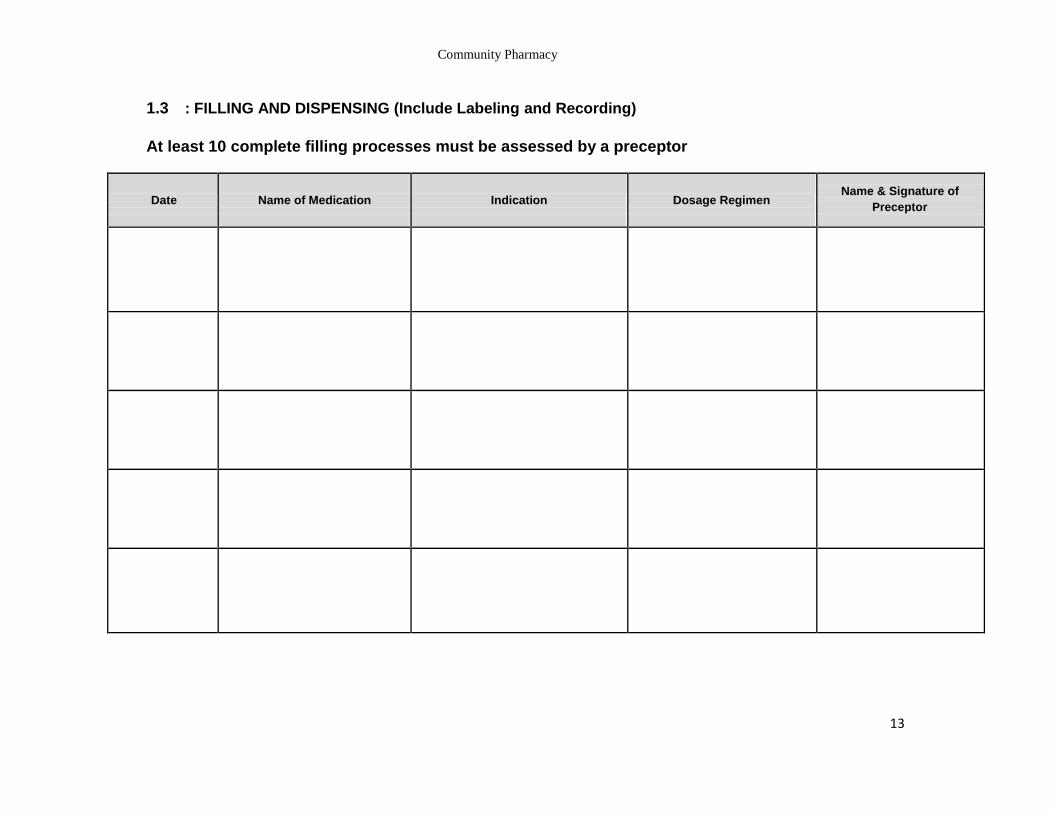
1.3 : FILLING AND DISPENSING (Include Labeling and Recording)
At least 10 complete filling processes must be assessed by a preceptor
Date Name of Medication Indication Dosage Regimen Name & Signature of
Preceptor
13
Community Pharmacy
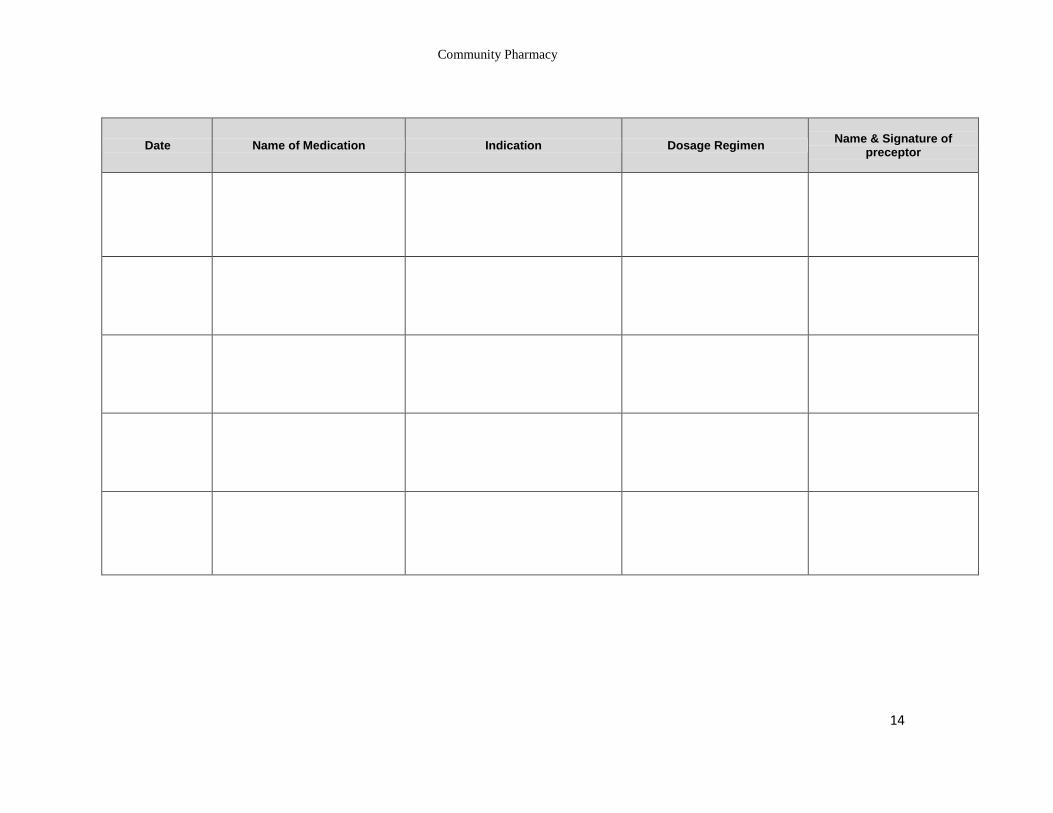
Date Name of Medication Indication Dosage Regimen Name & Signature of
preceptor
14
Community Pharmacy
SECTION 2: MINOR AILMENTS MANAGEMENT
At least 20 cases must be directly observed and assessed by a preceptor
Date Name of Patient Type of Ailments
Medication and medical history
taking ()
Action Taken (Medication/ monitoring)
Counseling()
Dispensing (Filling & Labelling
()
Name & Signature of
Preceptor
15
Community Pharmacy
Date Name of Patient Type of Ailments
Medication and medical history
taking ()
Action Taken (Medication/ monitoring)
Counseling()
Dispensing (Filling & Labelling
()
Name & Signature of
Preceptor
16
Community Pharmacy
Date Name of Patient Type of Ailments
Medication and medical history
taking ()
Action Taken (Medication/ monitoring)
Counseling()
Dispensing (Filling & Labelling
()
Name & Signature of
Preceptor
17
Community Pharmacy
Date Name of Patient Type of Ailments
Medication and medical history
taking ()
Action Taken (Medication/ monitoring)
Counseling()
Dispensing (Filling & Labelling
()
Name & Signature of
Preceptor
SECTION 3: MEDICATION COUNSELING
At least 50 counseling must be directly observed and assessed by a preceptor and documented using the Counseling Form in Appendix 2 for each case)
18
Community Pharmacy
SECTION 4: WELLNESS MANAGEMENT
At least 50 cases under the supervision of a preceptor
Date Type of device/ Supplement/ Non Information provided
Name & Signature of pharmacological intervention Preceptor
19

Community Pharmacy
Date Type of device/ Supplement/ Non Information provided
Name & Signature of pharmacological intervention Preceptor
20
Community Pharmacy
Date Type of device/ Supplement/ Non Information provided
Name & Signature of pharmacological intervention Preceptor
21
Community Pharmacy
SECTION 5: DRUG INFORMATION SERVICES
At least 50 enquiries, answered under the supervision of a preceptor
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
22
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
23
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify) (Pregnancy etc)
24
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
25
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
26
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
27
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
28
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
29
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify)
(Pregnancy etc)
30
Community Pharmacy
Type of Enquiries
Date
Source of
Poisoning
Allergy
Special Others
reference
Indication/ dose
Interaction Efficacy consideration
(Please specify) (Please specify) (Please specify) (Pregnancy etc)
31
Community Pharmacy
OUTPATIENT PHARMACY (HEALTH CLINIC ATTACHMENT) LOGBOOK
OUT PATIENT PHARMACY SERVICES (4 WEEKS)
Management of Outpatient Pharmacy
1. Knowledge of stock movement and control, patient waiting time, peak hour management (staff mobilization), staff training, handling of drug information requests and pharmacy QAP.
Dispensing of Medication / Prescriptions
2. Proficient in prescription ordering & supply system (including Integrated Medication Supply System) and verification. • Good communication skills and counter service. • Documentation of relevant data and statistics. • Proficient in reading. • Interpretation of prescriptions and completeness of prescription (e.g. drug
name, dose, frequency, duration etc).
3. Familiarity with drug range. Knowledge on generic names, proprietary names, pharmacological groupings, Hospital Formularies.
4. Proficient in the screening of prescriptions (e.g. Dosage regimen, polypharmacy, drug interactions, adequacy of instruction(s), contraindications, incompatibilities etc.). The screening of a prescription must be performed at any point of processing a prescription, e.g. during receiving, filling and dispensing.
5. Awareness of the importance of patient’s medication record (e.g. warfarin medication card)
6. Ability to contact prescriber to discuss errors or ambiguous prescriptions.
7. Proficient in filling prescriptions.
8. Proficient in dispensing.
9. Knowledge on the pre-packing process, packaging and labeling of
medication dispensed.
32
Community Pharmacy
Patient medication counseling
10. Ability to advise/ counsel on patient drug regimen/ therapy, indications, storage conditions, precautions, side effects, food / drug interactions, dosage regimen, compliance and missed doses, use of devices (e.g. inhalers, insulin pens, interferon pens).
11. Ability to perform in conducting group / individual counseling sessions.
Dangerous / Psychotropic Drugs Management
12. Knowledge of psychotropic and dangerous drugs distribution and disposal in accordance to the respective legislations:
Dangerous Drugs Act 1952 Poisons Act 1952
Poisons (Psychotropic Substances) Regulations 1989
13. The activities include in this department are:
Screening Filling
Dispensing Medication Counseling
Dangerous Drugs & Psychotropic
33
Community Pharmacy
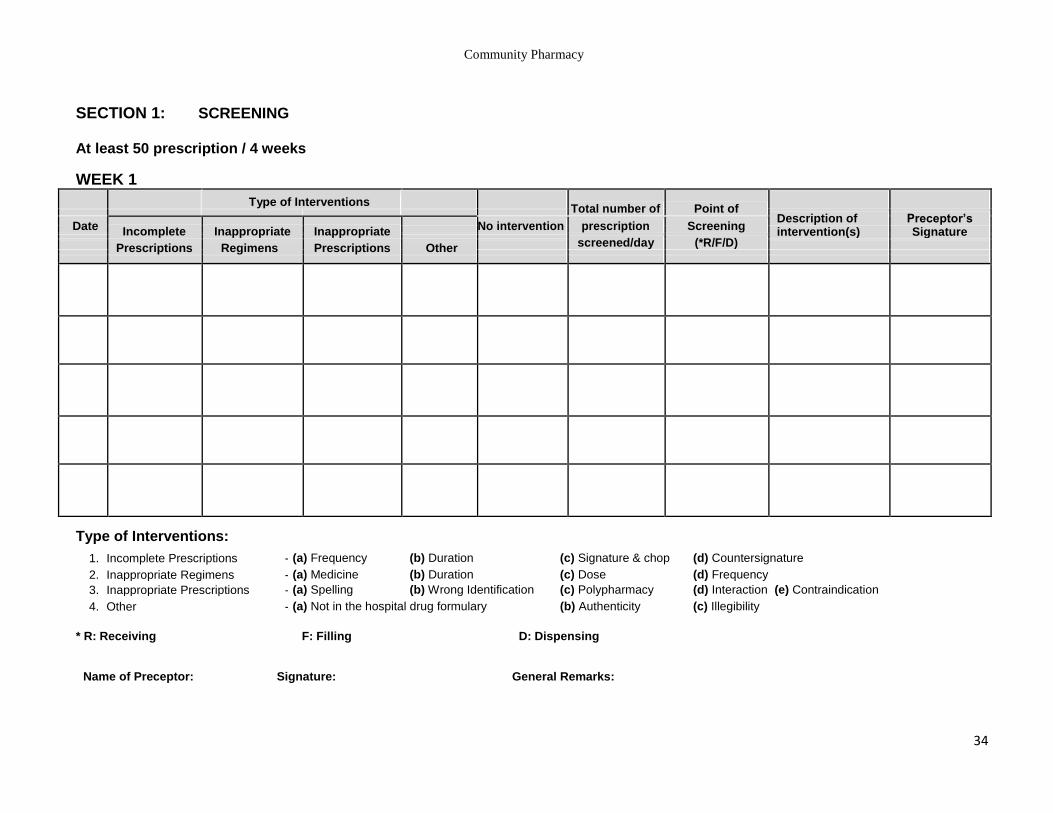
SECTION 1: SCREENING
At least 50 prescription / 4 weeks
WEEK 1
Type of Interventions Total number of Point of
Description of Preceptor’s Date Incomplete Inappropriate Inappropriate
No intervention prescription Screening intervention(s) Signature
screened/day (*R/F/D)
Prescriptions Regimens Prescriptions Other
Type of Interventions:
1. Incomplete Prescriptions - (a) Frequency (b) Duration (c) Signature & chop (d) Countersignature
2. Inappropriate Regimens - (a) Medicine (b) Duration (c) Dose (d) Frequency
3. Inappropriate Prescriptions - (a) Spelling (b) Wrong Identification (c) Polypharmacy (d) Interaction (e) Contraindication
4. Other - (a) Not in the hospital drug formulary (b) Authenticity (c) Illegibility
* R: Receiving F: Filling D: Dispensing
Name of Preceptor: Signature: General Remarks:
34
Community Pharmacy
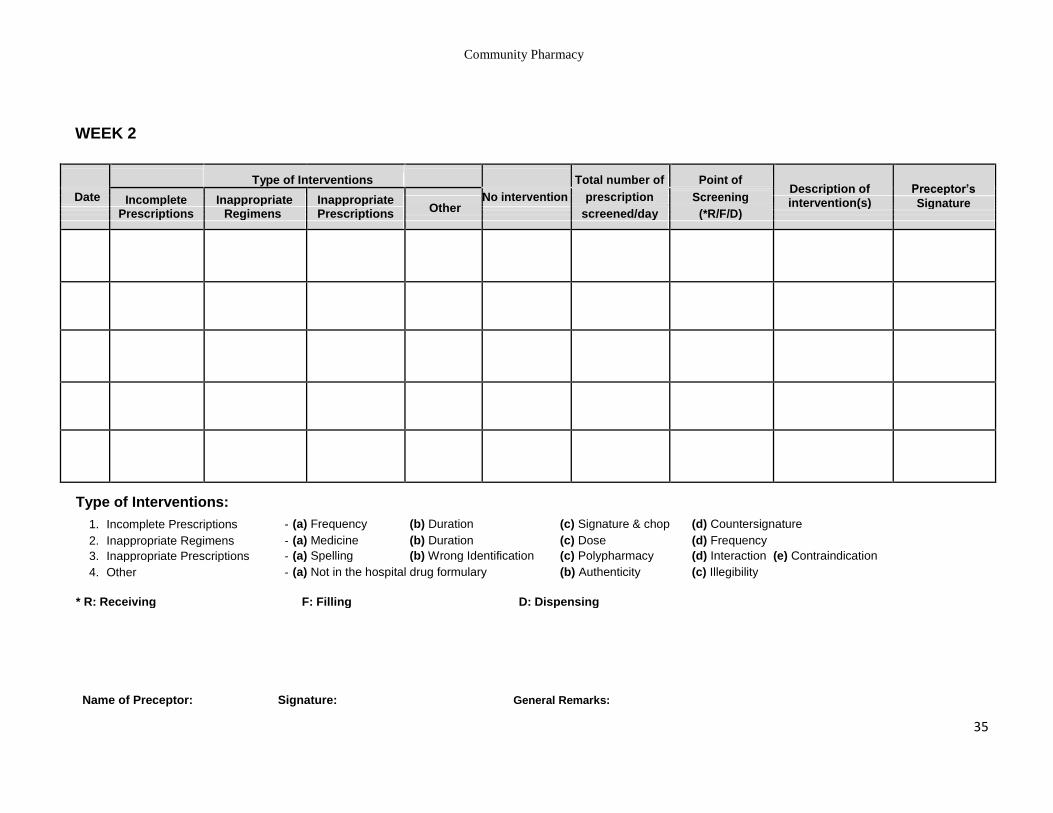
WEEK 2
Type of Interventions Total number of Point of Description of Preceptor’s
Date Incomplete Inappropriate Inappropriate
No intervention prescription Screening Other intervention(s) Signature
screened/day (*R/F/D)
Prescriptions Regimens Prescriptions
Type of Interventions:
1. Incomplete Prescriptions - (a) Frequency (b) Duration (c) Signature & chop (d) Countersignature
2. Inappropriate Regimens - (a) Medicine (b) Duration (c) Dose (d) Frequency
3. Inappropriate Prescriptions - (a) Spelling (b) Wrong Identification (c) Polypharmacy (d) Interaction (e) Contraindication
4. Other - (a) Not in the hospital drug formulary (b) Authenticity (c) Illegibility
* R: Receiving F: Filling D: Dispensing
Name of Preceptor: Signature: General Remarks:
35
Community Pharmacy
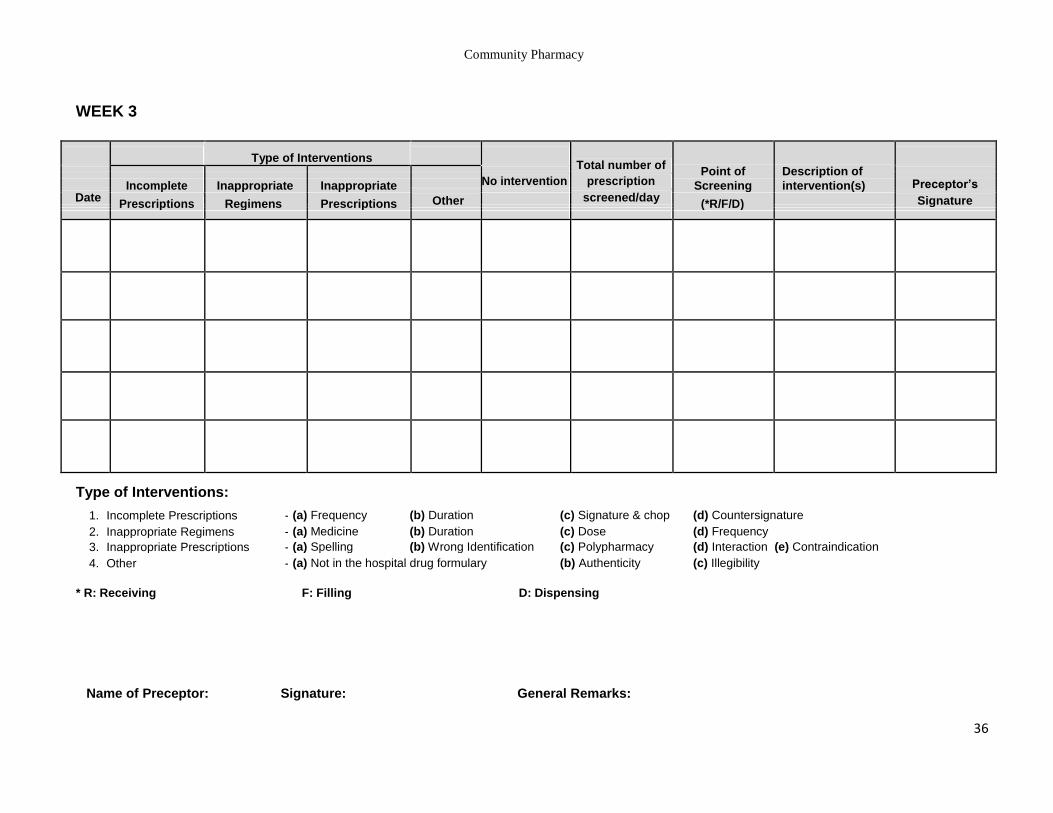
WEEK 3
Type of Interventions Total number of
Point of Description of
No intervention prescription Preceptor’s Incomplete Inappropriate Inappropriate Screening intervention(s) Date
screened/day Other
Signature Prescriptions Regimens Prescriptions
(*R/F/D)
Type of Interventions:
1. Incomplete Prescriptions - (a) Frequency (b) Duration (c) Signature & chop (d) Countersignature
2. Inappropriate Regimens - (a) Medicine (b) Duration (c) Dose (d) Frequency
3. Inappropriate Prescriptions - (a) Spelling (b) Wrong Identification (c) Polypharmacy (d) Interaction (e) Contraindication
4. Other - (a) Not in the hospital drug formulary (b) Authenticity (c) Illegibility
* R: Receiving F: Filling D: Dispensing
Name of Preceptor: Signature: General Remarks:
36
Community Pharmacy
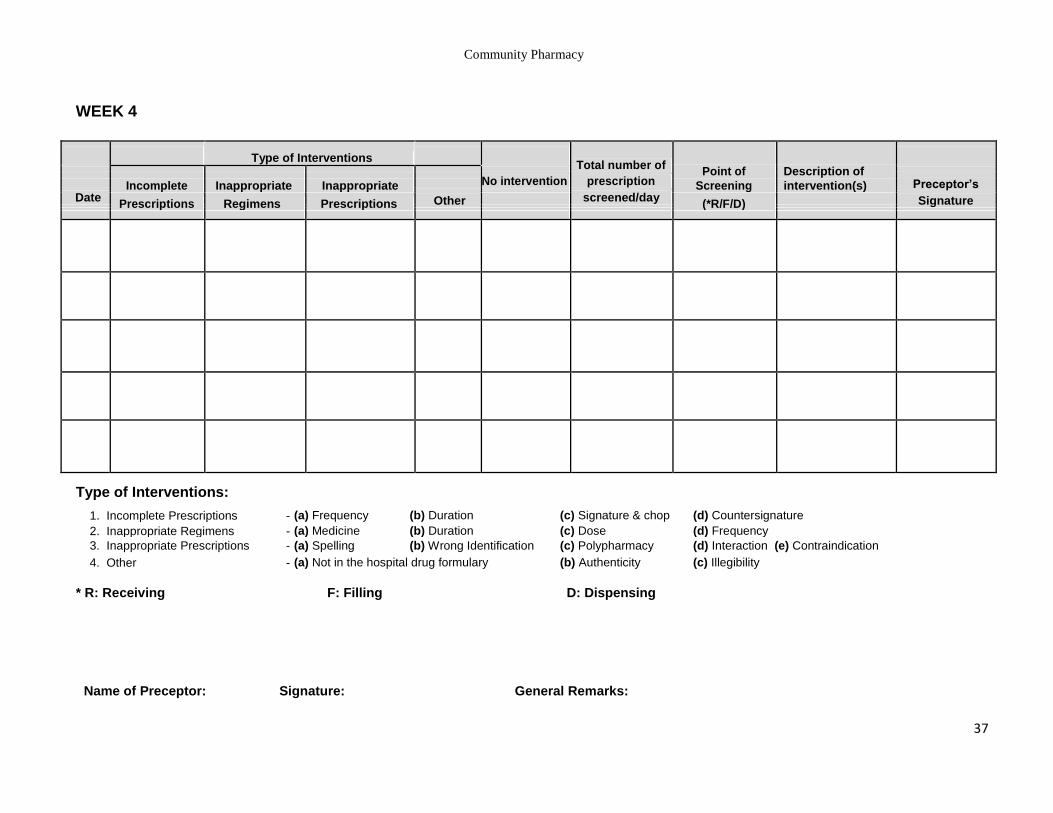
WEEK 4
Type of Interventions Total number of
Point of Description of
No intervention prescription Preceptor’s Incomplete Inappropriate Inappropriate Screening intervention(s) Date
screened/day Other
Signature Prescriptions Regimens Prescriptions
(*R/F/D)
Type of Interventions:
1. Incomplete Prescriptions - (a) Frequency (b) Duration (c) Signature & chop (d) Countersignature
2. Inappropriate Regimens - (a) Medicine (b) Duration (c) Dose (d) Frequency
3. Inappropriate Prescriptions - (a) Spelling (b) Wrong Identification (c) Polypharmacy (d) Interaction (e) Contraindication
4. Other - (a) Not in the hospital drug formulary (b) Authenticity (c) Illegibility
* R: Receiving F: Filling D: Dispensing
Name of Preceptor: Signature: General Remarks:
37
Community Pharmacy
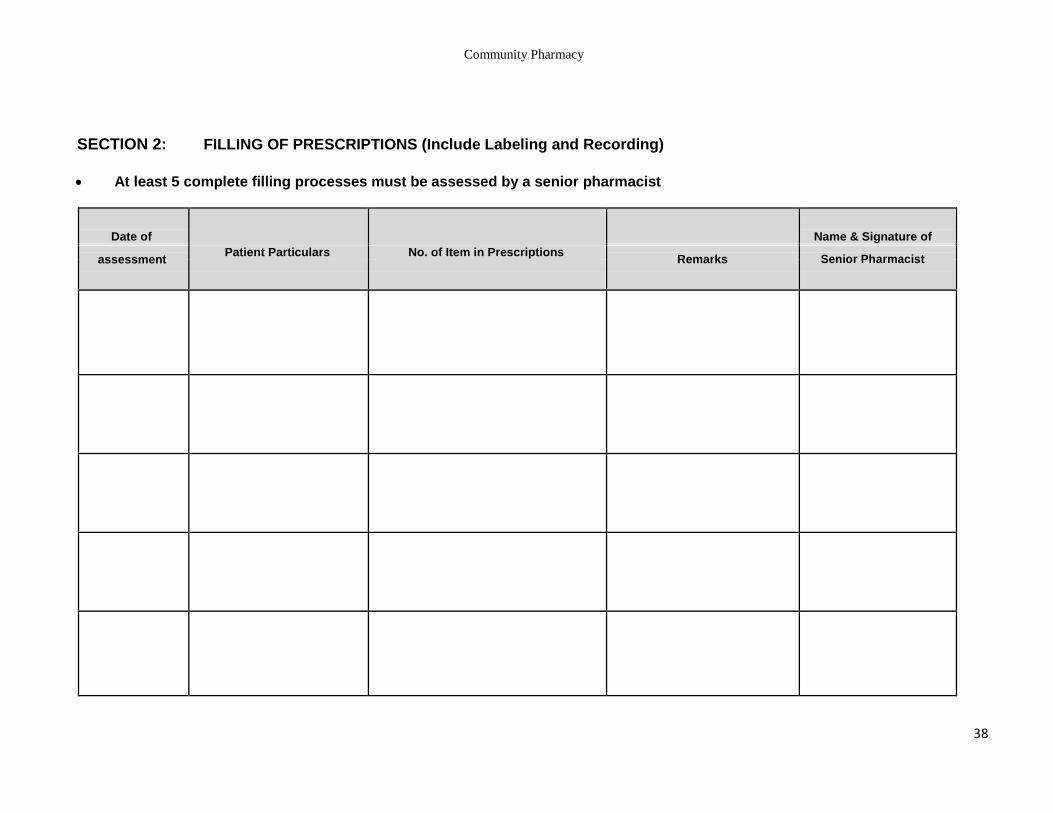
SECTION 2: FILLING OF PRESCRIPTIONS (Include Labeling and Recording)
At least 5 complete filling processes must be assessed by a senior pharmacist
Date of
Patient Particulars No. of Item in Prescriptions
Name & Signature of
assessment Remarks Senior Pharmacist
38
Community Pharmacy
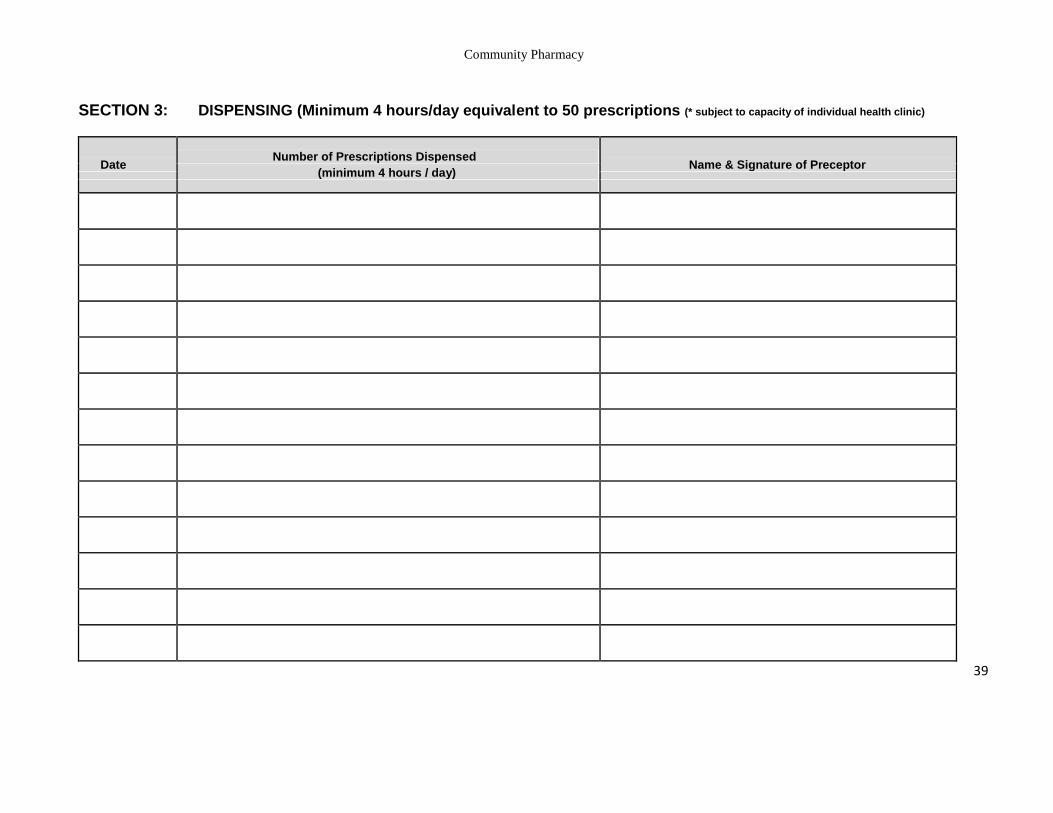
SECTION 3: DISPENSING (Minimum 4 hours/day equivalent to 50 prescriptions (* subject to capacity of individual health clinic)
Date Number of Prescriptions Dispensed
Name & Signature of Preceptor (minimum 4 hours / day)
39
Community Pharmacy
SECTION 3: DISPENSING (Minimum 4 hours/day equivalent to 50 prescriptions) (* subject to capacity of individual health clinic)
Date Number of Prescriptions Dispensed
Name & Signature of Preceptor (minimum 4 hours / day)
40
Community Pharmacy
SECTION 4: MEDICATION COUNSELING (INDIVIDUAL – Minimum 3/ week)
At least 5 counseling must be directly observed and assessed by a senior pharmacist
WEEK 1
Patients RN
Counseling Based On The Types Of Pharmacotherapy Management – minimum 5 patients/ type *where applicable
Name & Signature of
Preceptor
Date
Anti diabetics
Anti hypertensives
Anti Asthmatics
Anti Retrovirals
Anti coagulants
Others (Please Specify)
41
Community Pharmacy
WEEK 2
Patients RN
Counseling Based On The Types Of Pharmacotherapy Management – minimum 5 patients/ type *where applicable
Name & Signature of
Preceptor
Date
Anti diabetics
Anti hypertensives
Anti Asthmatics
Anti Retrovirals
Anti coagulants
Others (Please Specify)
42
Community Pharmacy
WEEK 3
Patients RN
Counseling Based On The Types Of Pharmacotherapy Management – minimum 5 patients/ type *where applicable
Name & Signature of
Preceptor
Date
Anti diabetics
Anti hypertensives
Anti Asthmatics
Anti Retrovirals
Anti coagulants
Others (Please Specify)
43
Community Pharmacy
WEEK 4
Patients RN
Counseling Based On The Types Of Pharmacotherapy Management – minimum 5 patients/ type *where applicable
Name & Signature of
Preceptor
Date
Anti diabetics
Anti hypertensives
Anti Asthmatics
Anti Retrovirals
Anti coagulants
Others (Please Specify)
44
Community Pharmacy
SECTION 5: DANGEROUS DRUG & PSYCHOTROPIC
Psychotropic & Dangerous Drug
Number Of Prescriptions Dispensed & Recorded Name & Signature of Pharmacist
Date (minimum 10 prescriptions/ week) In-charge
45
Community Pharmacy
SECTION 6: PREPARATION / OBSERVATION / COUNTER-CHECKING OF JOB SHEET OF
EXTEMPORANEOUS (MIN 5 EACH)
Ability to understand formulation and calculate the appropriate quantities required
Extemporaneous Preparations
Date MRN Name of Preparation Remarks Signature of
Preceptor
46
Community Pharmacy
ASSESSMENT
47
Community Pharmacy
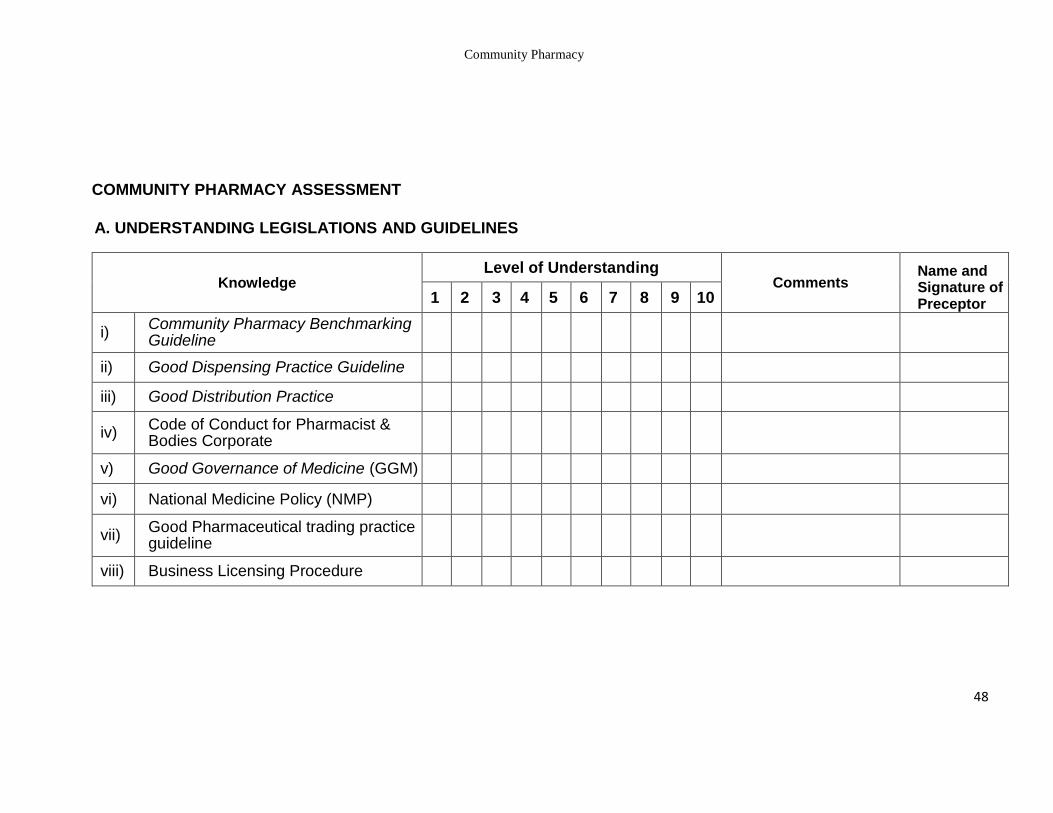
COMMUNITY PHARMACY ASSESSMENT
A. UNDERSTANDING LEGISLATIONS AND GUIDELINES
Knowledge Level of Understanding
Comments Name and Signature of Preceptor 1 2 3 4 5 6 7 8 9 10
i) Community Pharmacy Benchmarking Guideline
ii) Good Dispensing Practice Guideline
iii) Good Distribution Practice
iv) Code of Conduct for Pharmacist & Bodies Corporate
v) Good Governance of Medicine (GGM)
vi) National Medicine Policy (NMP)
vii) Good Pharmaceutical trading practice guideline
viii) Business Licensing Procedure
48
Community Pharmacy
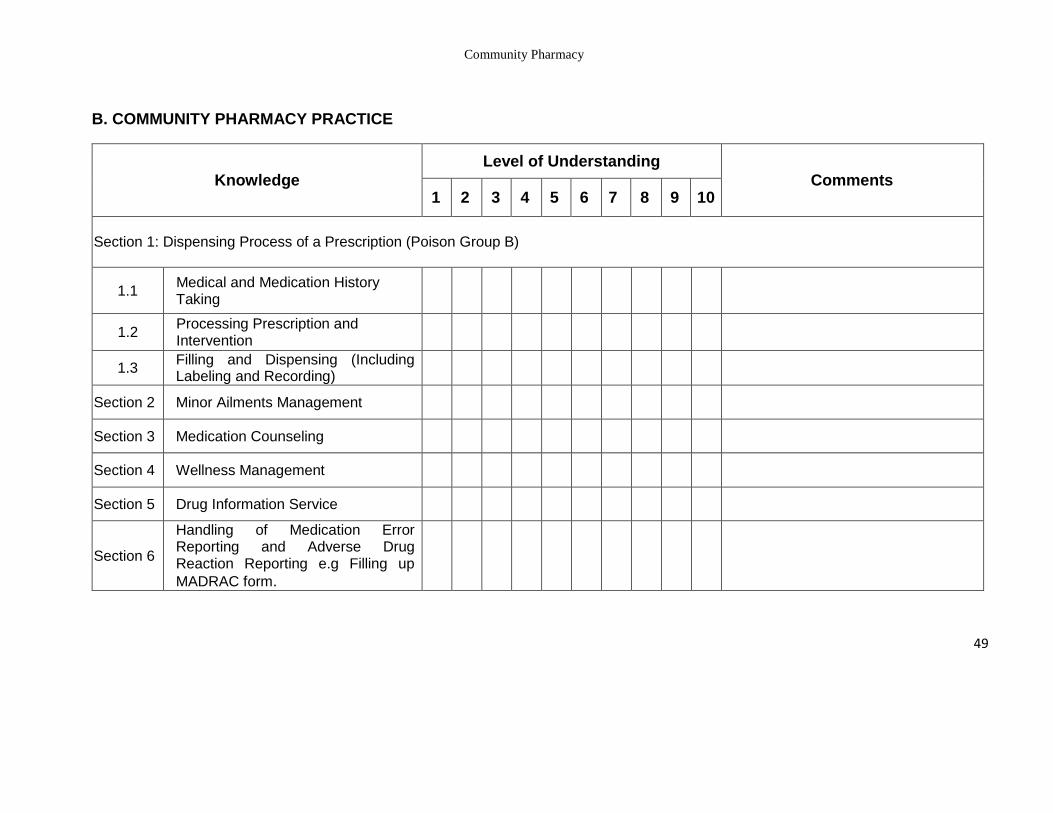
B. COMMUNITY PHARMACY PRACTICE
Knowledge
Level of Understanding
Comments 1 2 3 4 5 6 7 8 9 10
Section 1: Dispensing Process of a Prescription (Poison Group B)
1.1 Medical and Medication History Taking
1.2 Processing Prescription and Intervention
1.3 Filling and Dispensing (Including Labeling and Recording)
Section 2 Minor Ailments Management
Section 3 Medication Counseling
Section 4 Wellness Management
Section 5 Drug Information Service
Section 6
Handling of Medication Error Reporting and Adverse Drug Reaction Reporting e.g Filling up
MADRAC form.
49
Community Pharmacy
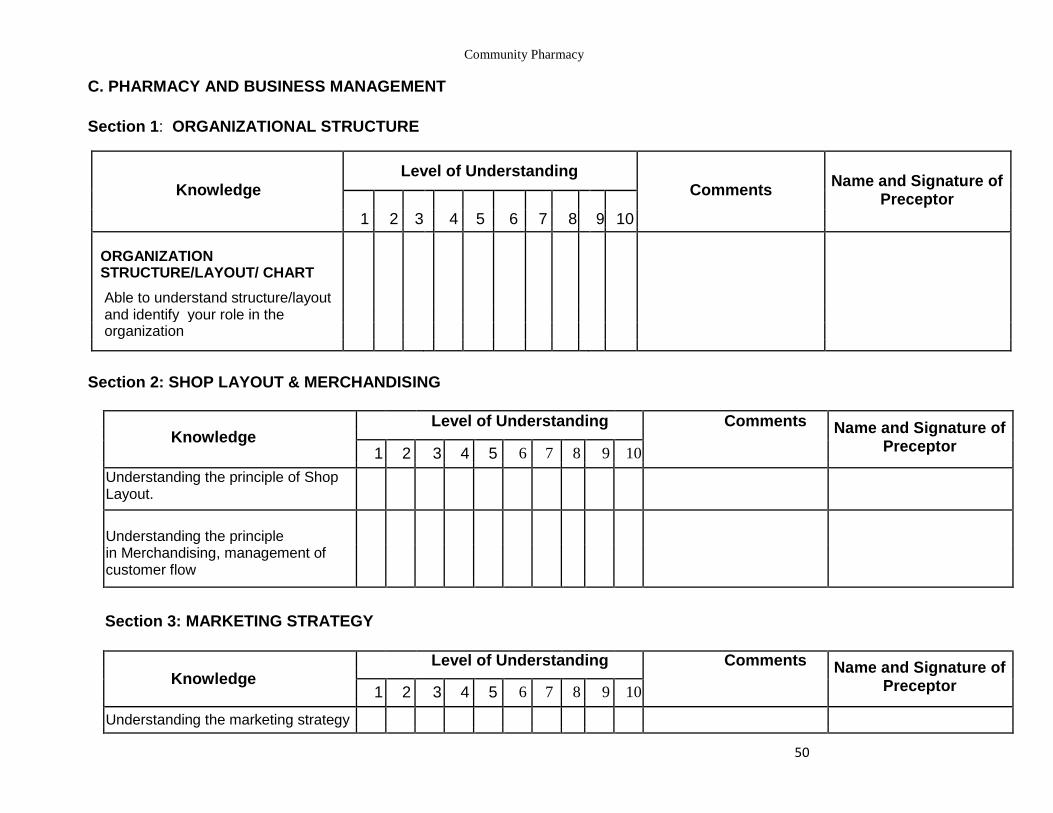
C. PHARMACY AND BUSINESS MANAGEMENT
Section 1: ORGANIZATIONAL STRUCTURE
Knowledge
Level of Understanding
Comments Name and Signature of
Preceptor
1 2 3
4 5 6 7 8
9 10
ORGANIZATION
STRUCTURE/LAYOUT/ CHART
Able to understand structure/layout and identify your role in the
organization
Section 2: SHOP LAYOUT & MERCHANDISING
Knowledge Level of Understanding Comments Name and Signature of
Preceptor
1 2 3 4 5 6 7 8 9 10
Understanding the principle of Shop Layout.
Understanding the principle
in Merchandising, management of customer flow
Section 3: MARKETING STRATEGY
Knowledge Level of Understanding Comments Name and Signature of
Preceptor
1 2 3 4 5 6 7 8 9 10
Understanding the marketing strategy
50
Community Pharmacy
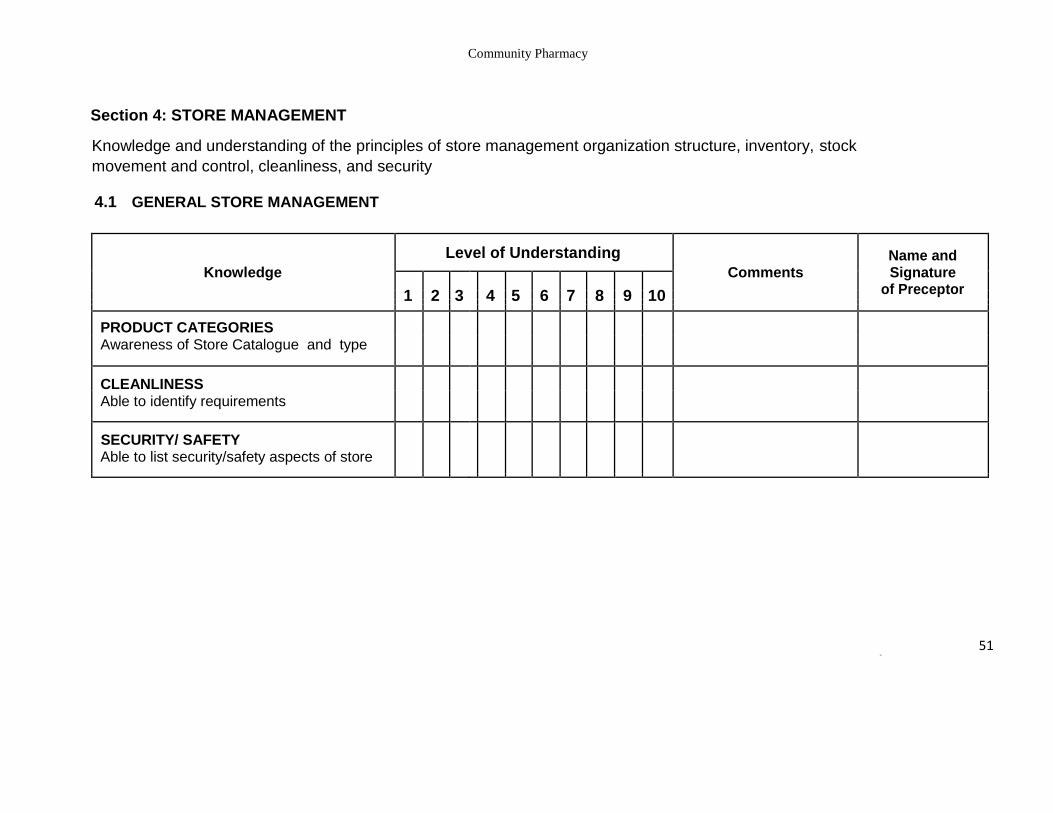
Section 4: STORE MANAGEMENT
Knowledge and understanding of the principles of store management organization structure, inventory, stock
movement and control, cleanliness, and security
4.1 GENERAL STORE MANAGEMENT
Knowledge
Level of Understanding
Comments Name and Signature
of Preceptor 1 2 3
4 5 6 7 8 9 10
PRODUCT CATEGORIES Awareness of Store Catalogue and type
CLEANLINESS Able to identify requirements
SECURITY/ SAFETY Able to list security/safety aspects of store
51 50
Community Pharmacy
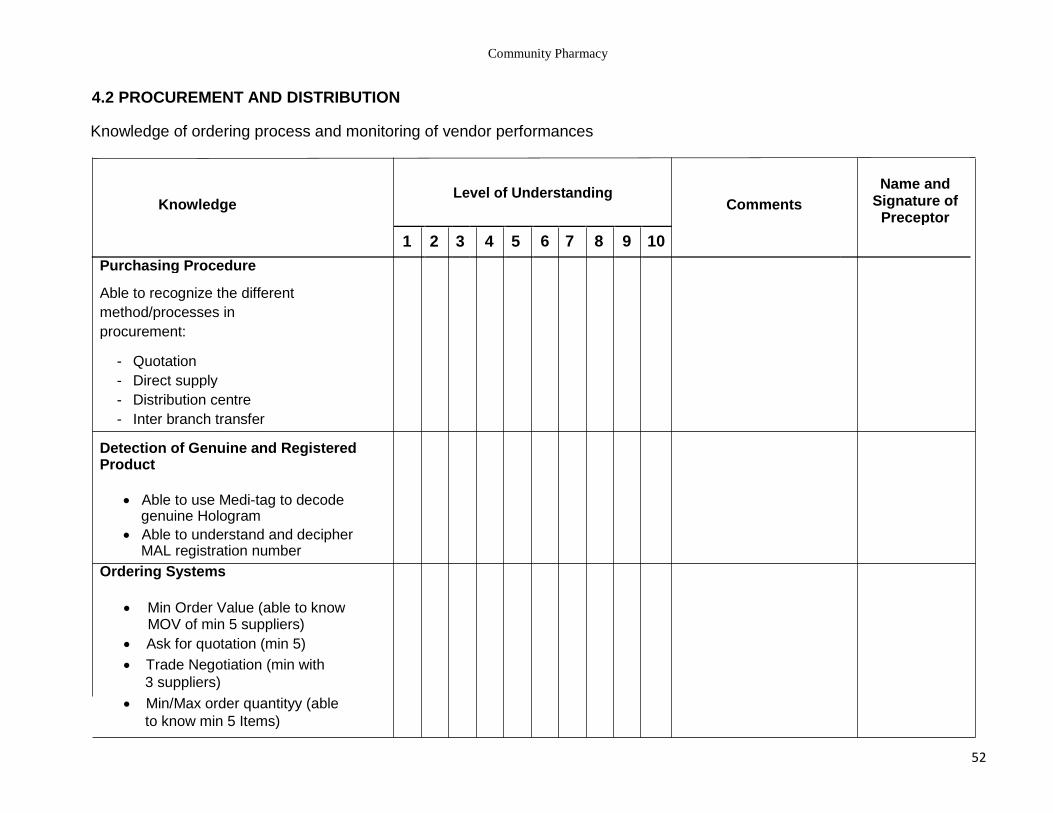
4.2 PROCUREMENT AND DISTRIBUTION
Knowledge of ordering process and monitoring of vendor performances
Level of Understanding
Name and Signature of
Preceptor
Knowledge Comments
1 2 3 4 5 6 7 8 9 10
Purchasing Procedure
Able to recognize the different
method/processes in
procurement:
- Quotation
- Direct supply
- Distribution centre
- Inter branch transfer
Detection of Genuine and Registered Product
Able to use Medi-tag to decode genuine Hologram
Able to understand and decipher MAL registration number
Ordering Systems
Min Order Value (able to know MOV of min 5 suppliers)
Ask for quotation (min 5) Trade Negotiation (min with
3 suppliers) Min/Max order quantityy (able
to know min 5 Items)
52
Community Pharmacy
Level of Understanding Name and Signature
of Preceptor Knowledge
Comments 1 2 3
4 5 6 7 8 9 10
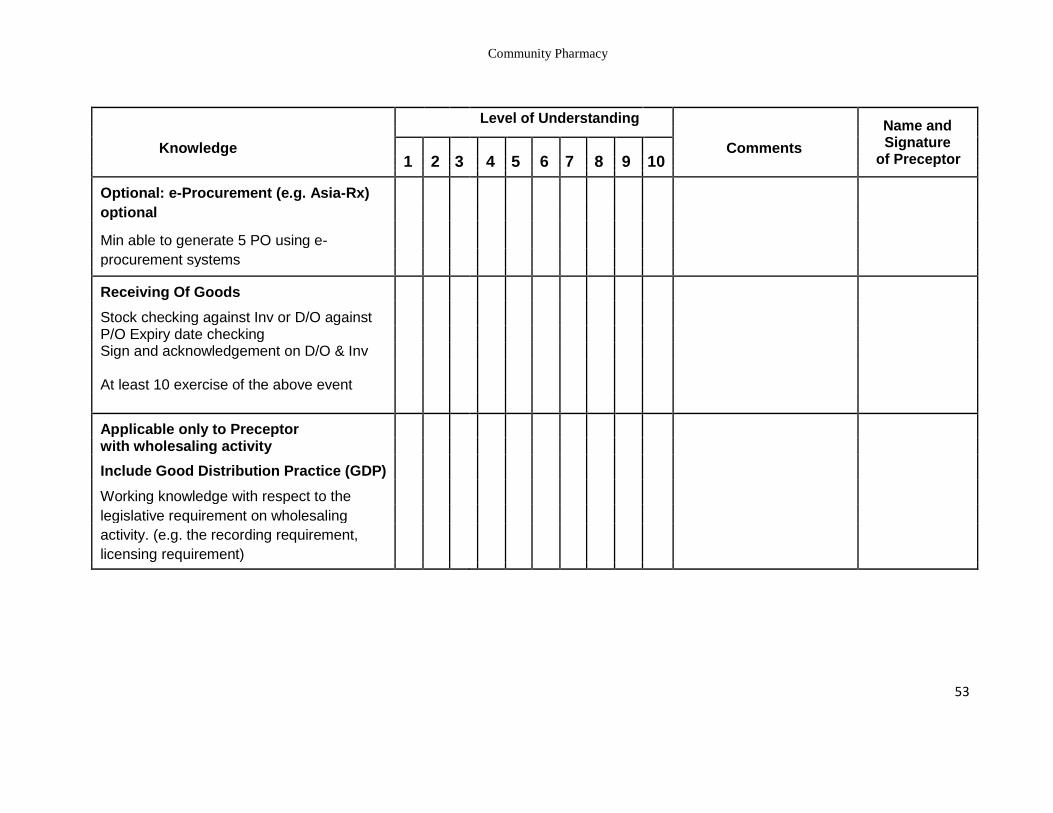
Optional: e-Procurement (e.g. Asia-Rx)
optional
Min able to generate 5 PO using e-
procurement systems
Receiving Of Goods
Stock checking against Inv or D/O against P/O Expiry date checking
Sign and acknowledgement on D/O & Inv
At least 10 exercise of the above event
Applicable only to Preceptor with wholesaling activity
Include Good Distribution Practice (GDP)
Working knowledge with respect to the
legislative requirement on wholesaling
activity. (e.g. the recording requirement,
licensing requirement)
53
Community Pharmacy
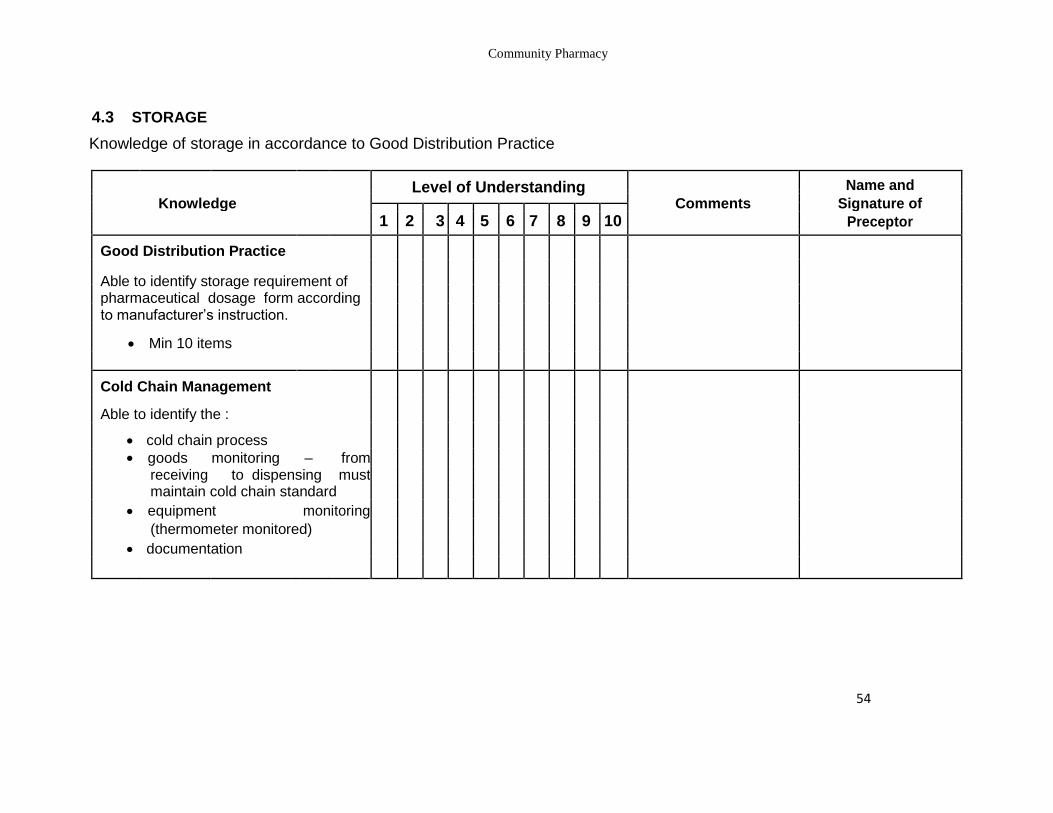
4.3 STORAGE
Knowledge of storage in accordance to Good Distribution Practice
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
Good Distribution Practice
Able to identify storage requirement of pharmaceutical dosage form according
to manufacturer’s instruction.
Min 10 items
Cold Chain Management
Able to identify the :
cold chain process
goods monitoring – from receiving to dispensing must
maintain cold chain standard
equipment monitoring
(thermometer monitored)
documentation
54
Community Pharmacy
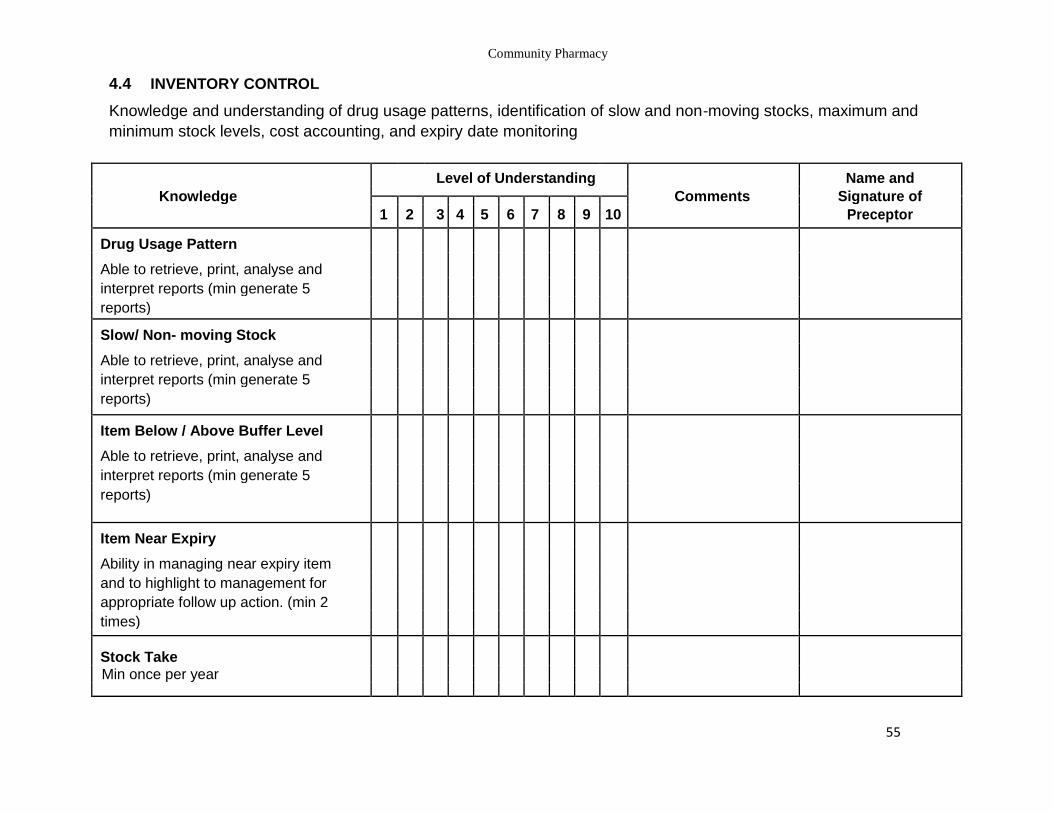
4.4 INVENTORY CONTROL
Knowledge and understanding of drug usage patterns, identification of slow and non-moving stocks, maximum and
minimum stock levels, cost accounting, and expiry date monitoring
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
Drug Usage Pattern
Able to retrieve, print, analyse and
interpret reports (min generate 5
reports)
Slow/ Non- moving Stock
Able to retrieve, print, analyse and
interpret reports (min generate 5
reports)
Item Below / Above Buffer Level
Able to retrieve, print, analyse and
interpret reports (min generate 5
reports)
Item Near Expiry
Ability in managing near expiry item
and to highlight to management for
appropriate follow up action. (min 2
times)
Stock Take Min once per year
55
Community Pharmacy
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
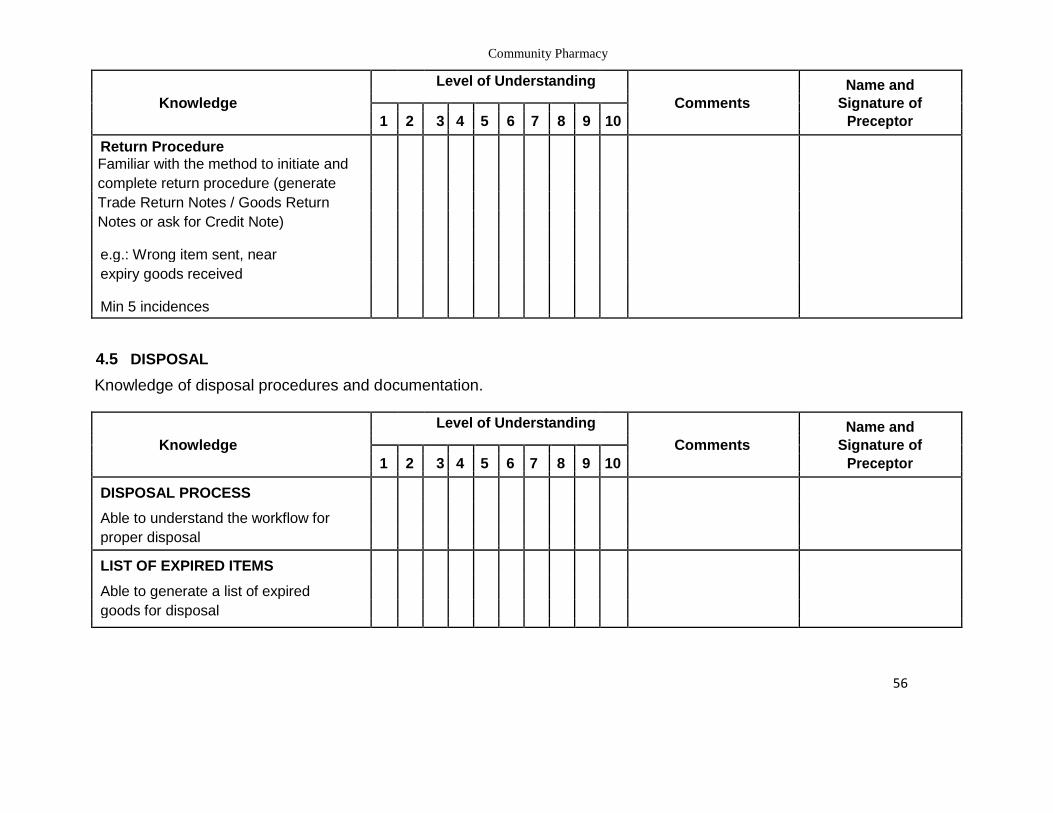
Return Procedure Familiar with the method to initiate and
complete return procedure (generate
Trade Return Notes / Goods Return
Notes or ask for Credit Note)
e.g.: Wrong item sent, near
expiry goods received
Min 5 incidences
4.5 DISPOSAL
Knowledge of disposal procedures and documentation.
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
DISPOSAL PROCESS
Able to understand the workflow for
proper disposal
LIST OF EXPIRED ITEMS
Able to generate a list of expired
goods for disposal
56
Community Pharmacy
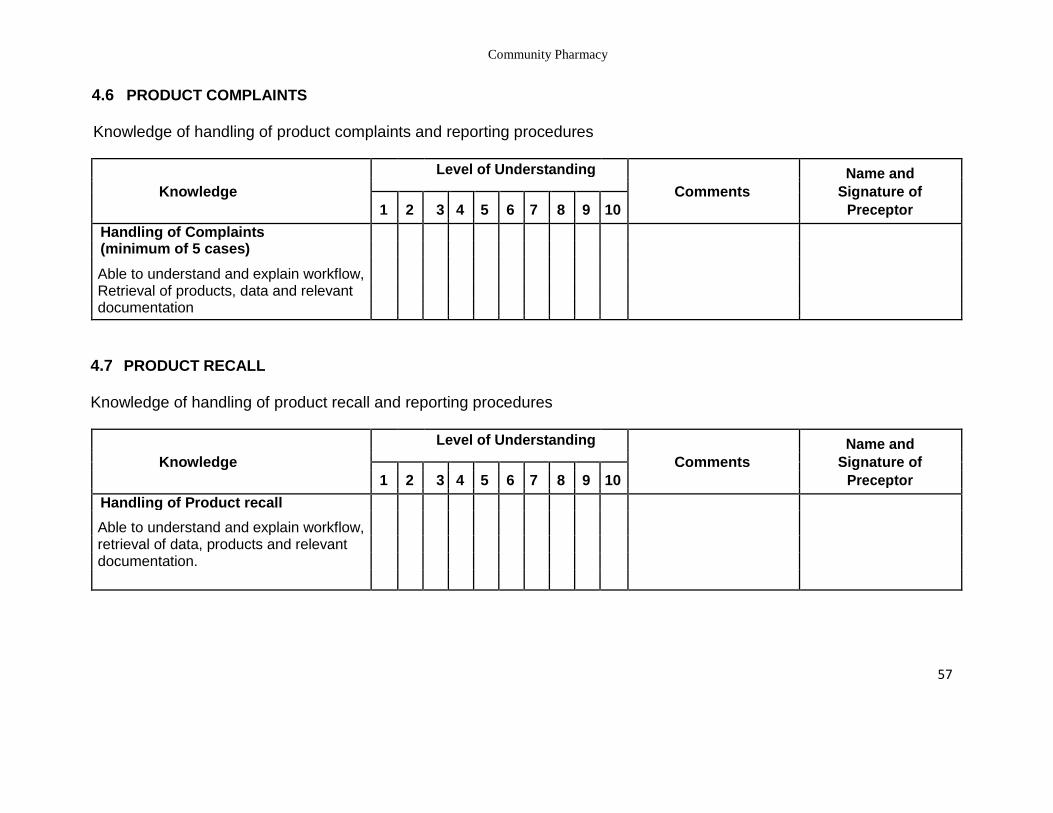
4.6 PRODUCT COMPLAINTS
Knowledge of handling of product complaints and reporting procedures
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
Handling of Complaints
(minimum of 5 cases)
Able to understand and explain workflow, Retrieval of products, data and relevant
documentation
4.7 PRODUCT RECALL
Knowledge of handling of product recall and reporting procedures
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
Handling of Product recall
Able to understand and explain workflow, retrieval of data, products and relevant
documentation.
57
Community Pharmacy
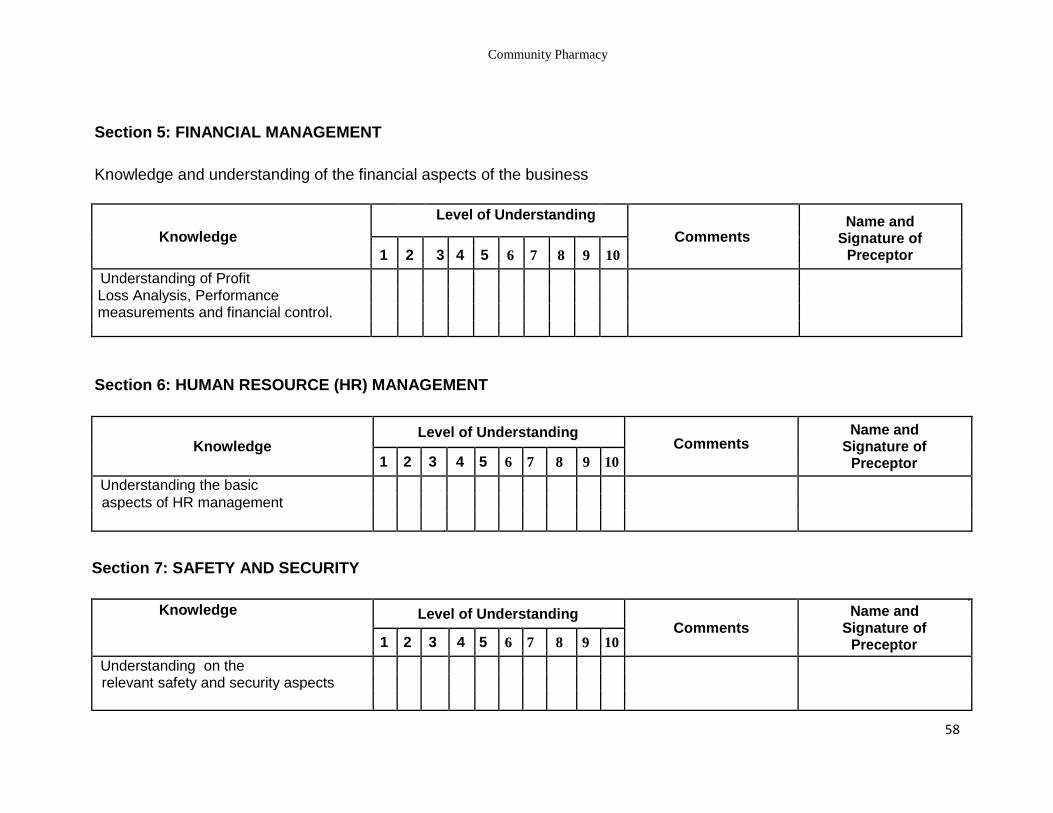
Section 5: FINANCIAL MANAGEMENT
Knowledge and understanding of the financial aspects of the business
Level of Understanding Name and
Signature of Preceptor
Knowledge
Comments
1 2 3 4 5 6 7 8 9 10
Understanding of Profit
Loss Analysis, Performance
measurements and financial control.
Section 6: HUMAN RESOURCE (HR) MANAGEMENT
Knowledge Level of Understanding
Comments Name and
Signature of Preceptor 1 2 3 4 5 6 7 8 9 10
Understanding the basic
aspects of HR management
Section 7: SAFETY AND SECURITY
Knowledge Level of Understanding Comments
Name and Signature of
Preceptor
1 2 3 4 5 6 7 8 9 10
Understanding on the
relevant safety and security aspects
58
Community Pharmacy
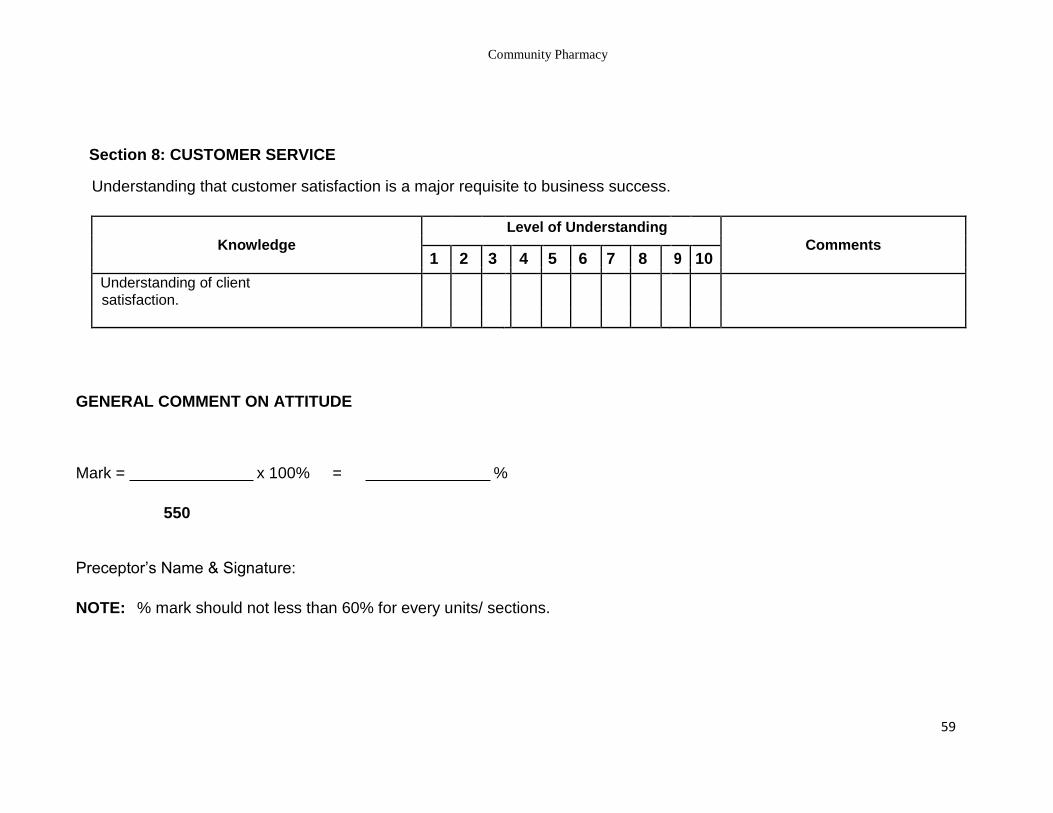
Section 8: CUSTOMER SERVICE
Understanding that customer satisfaction is a major requisite to business success.
Knowledge
Level of Understanding
Comments
1 2 3 4 5 6 7 8 9 10
Understanding of client
satisfaction.
GENERAL COMMENT ON ATTITUDE
Mark = x 100% = %
550
Preceptor’s Name & Signature:
NOTE: % mark should not less than 60% for every units/ sections.
59
Community Pharmacy
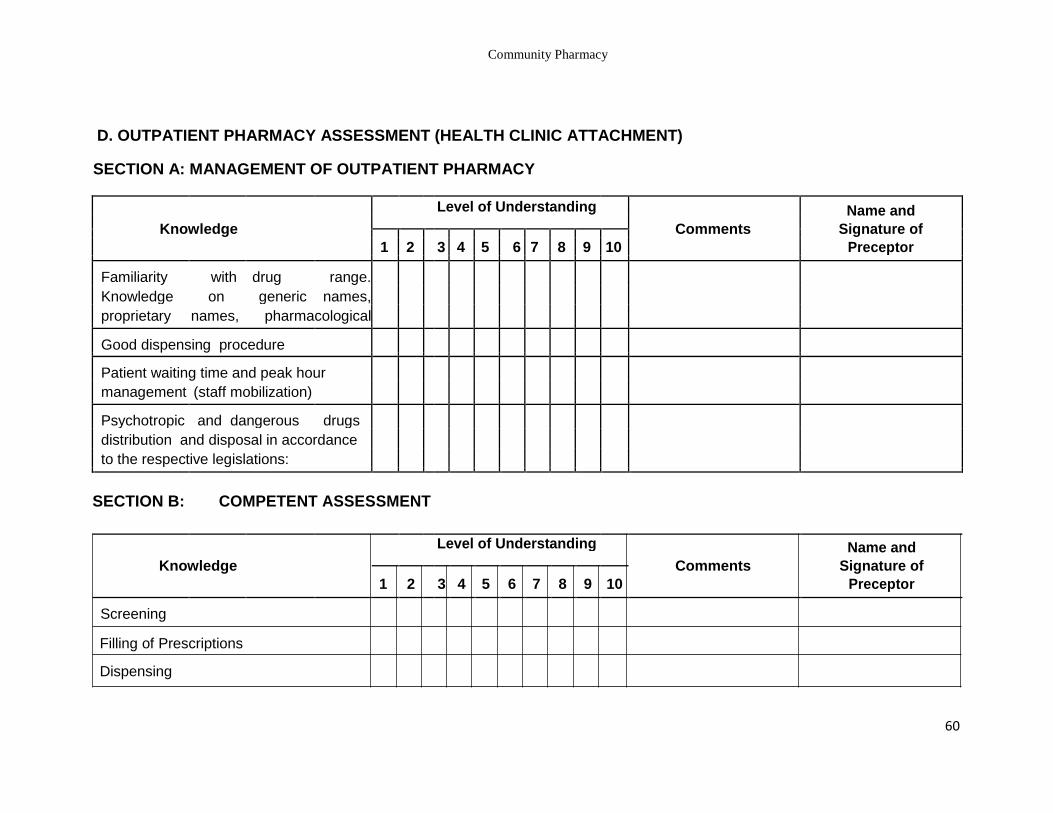
D. OUTPATIENT PHARMACY ASSESSMENT (HEALTH CLINIC ATTACHMENT)
SECTION A: MANAGEMENT OF OUTPATIENT PHARMACY
Level of Understanding Name and
Knowledge
Comments Signature of
1 2
3 4 5 6 7 8 9 10 Preceptor
Familiarity with drug range.
Knowledge on generic names,
proprietary names, pharmacological
Good dispensing procedure
Patient waiting time and peak hour
management (staff mobilization)
Psychotropic and dangerous drugs
distribution and disposal in accordance
to the respective legislations:
SECTION B: COMPETENT ASSESSMENT
Level of Understanding Name and
Knowledge
Comments Signature of
1 2
3 4 5 6 7 8 9 10 Preceptor
Screening
Filling of Prescriptions
Dispensing
60
Community Pharmacy
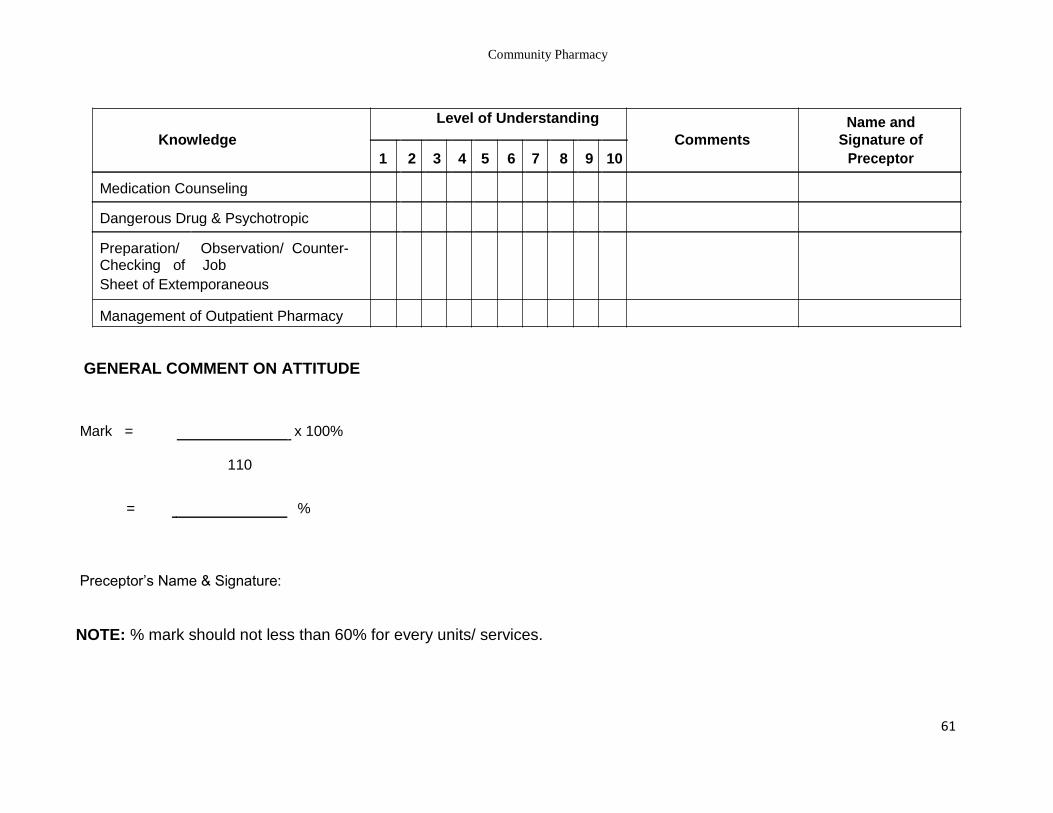
Level of Understanding Name and
Knowledge
Comments Signature of
1 2 3 4 5 6 7 8 9 10 Preceptor
Medication Counseling
Dangerous Drug & Psychotropic
Preparation/ Observation/ Counter- Checking of Job
Sheet of Extemporaneous
Management of Outpatient Pharmacy
GENERAL COMMENT ON ATTITUDE
Mark = x 100%
110
= %
Preceptor’s Name & Signature:
NOTE: % mark should not less than 60% for every units/ services.
61
Community Pharmacy
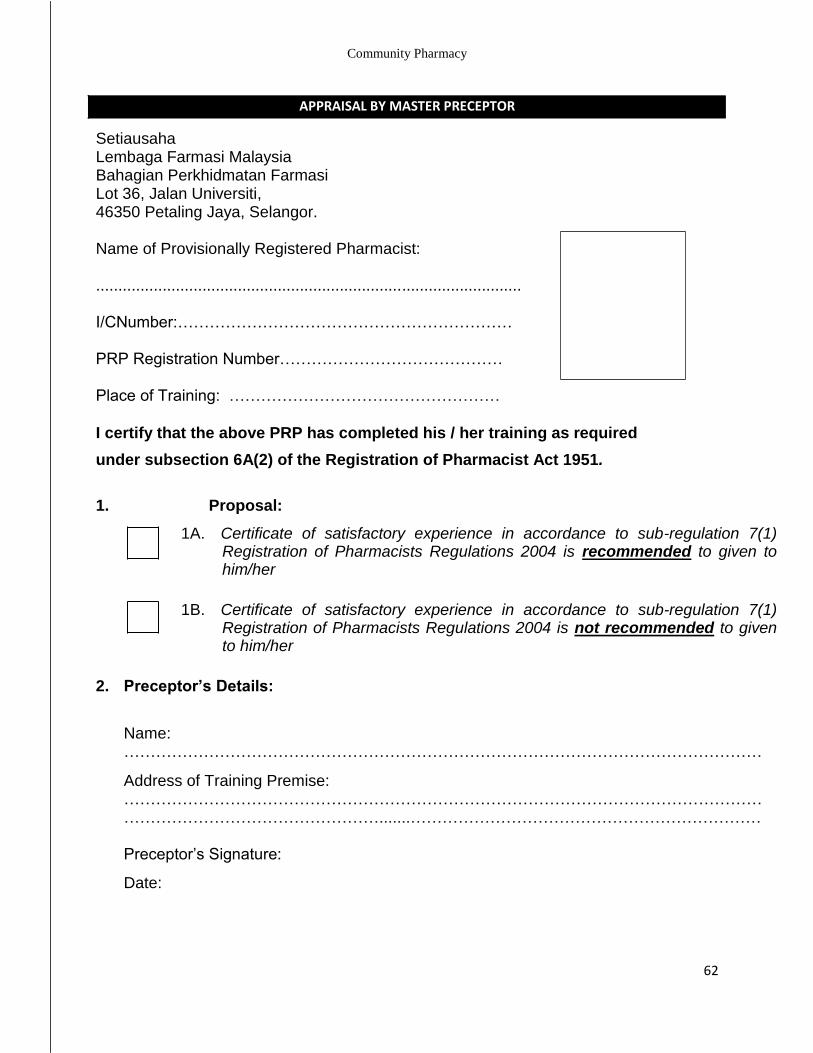
APPRAISAL BY MASTER PRECEPTOR
Setiausaha Lembaga Farmasi Malaysia Bahagian Perkhidmatan Farmasi Lot 36, Jalan Universiti, 46350 Petaling Jaya, Selangor.
Name of Provisionally Registered Pharmacist:
................................................................................................
I/CNumber:………………………………………………………
PRP Registration Number……………………………………
Place of Training: ……………………………………………
I certify that the above PRP has completed his / her training as required
under subsection 6A(2) of the Registration of Pharmacist Act 1951.
1. Proposal:
1A. Certificate of satisfactory experience in accordance to sub-regulation 7(1) Registration of Pharmacists Regulations 2004 is recommended to given to him/her
1B. Certificate of satisfactory experience in accordance to sub-regulation 7(1) Registration of Pharmacists Regulations 2004 is not recommended to given to him/her
2. Preceptor’s Details:
Name: …………………………………………………………………………………………………………
Address of Training Premise: ………………………………………………………………………………………………………… ………………………………………….......…………………………………………………………
Preceptor’s Signature:
Date:
62
Community Pharmacy
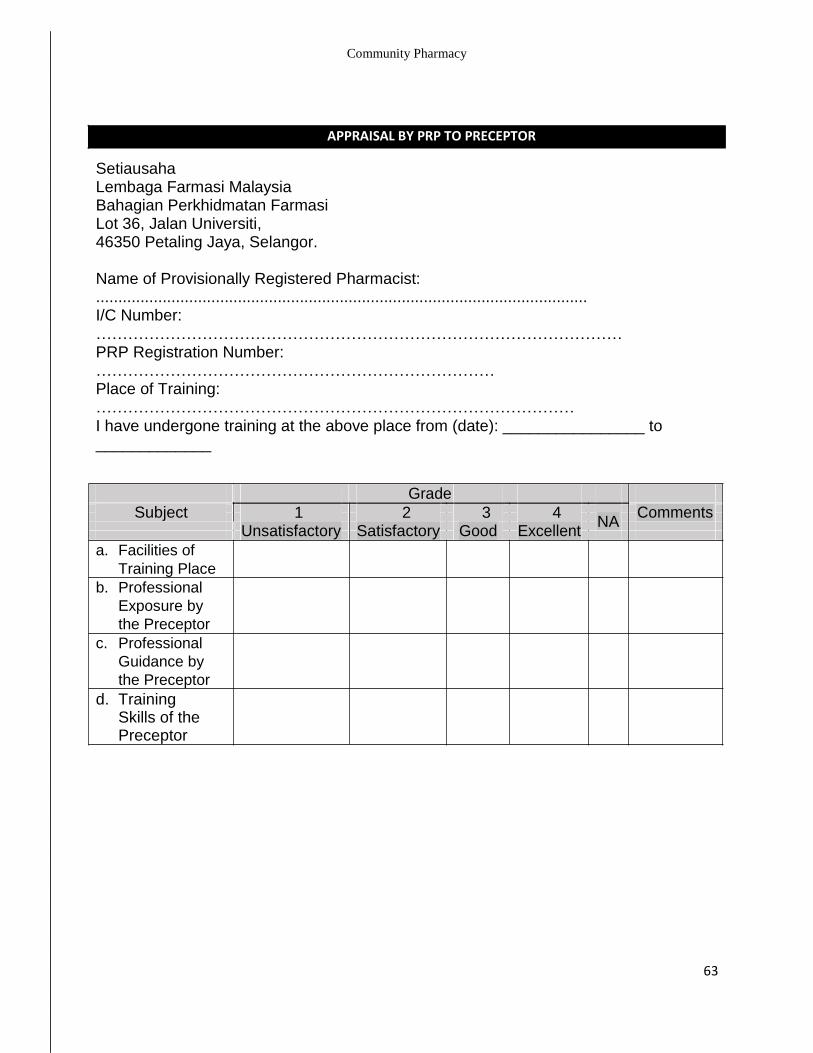
APPRAISAL BY PRP TO PRECEPTOR
Setiausaha Lembaga Farmasi Malaysia Bahagian Perkhidmatan Farmasi Lot 36, Jalan Universiti, 46350 Petaling Jaya, Selangor.
Name of Provisionally Registered Pharmacist: ............................................................................................................... I/C Number: ……………………………………………………………………………………… PRP Registration Number: ………………………………………………………………… Place of Training: ……………………………………………………………………………… I have undergone training at the above place from (date): ________________ to _____________
Grade Subject 1 2 3 4
NA Comments
Unsatisfactory
Satisfactory
Good
Excellent
a. Facilities of
Training Place b. Professional
Exposure by
the Preceptor c. Professional
Guidance by
the Preceptor d. Training
Skills of the Preceptor
63
Community Pharmacy
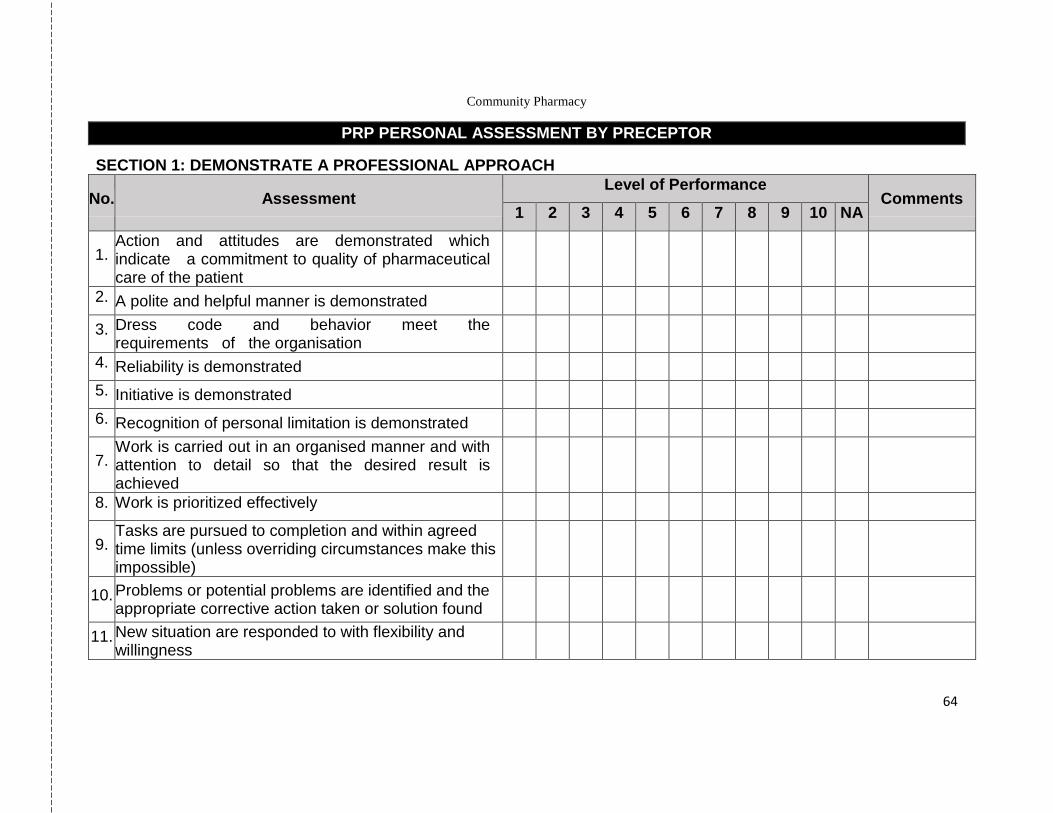
PRP PERSONAL ASSESSMENT BY PRECEPTOR
SECTION 1: DEMONSTRATE A PROFESSIONAL APPROACH
No. Assessment Level of Performance
Comments 1 2 3 4 5 6 7 8 9 10 NA
1. Action and attitudes are demonstrated which indicate a commitment to quality of pharmaceutical care of the patient
2. A polite and helpful manner is demonstrated
3. Dress code and behavior meet the requirements of the organisation
4. Reliability is demonstrated
5. Initiative is demonstrated
6. Recognition of personal limitation is demonstrated
7. Work is carried out in an organised manner and with attention to detail so that the desired result is achieved
8. Work is prioritized effectively
9. Tasks are pursued to completion and within agreed time limits (unless overriding circumstances make this impossible)
10. Problems or potential problems are identified and the appropriate corrective action taken or solution found
11. New situation are responded to with flexibility and willingness
64
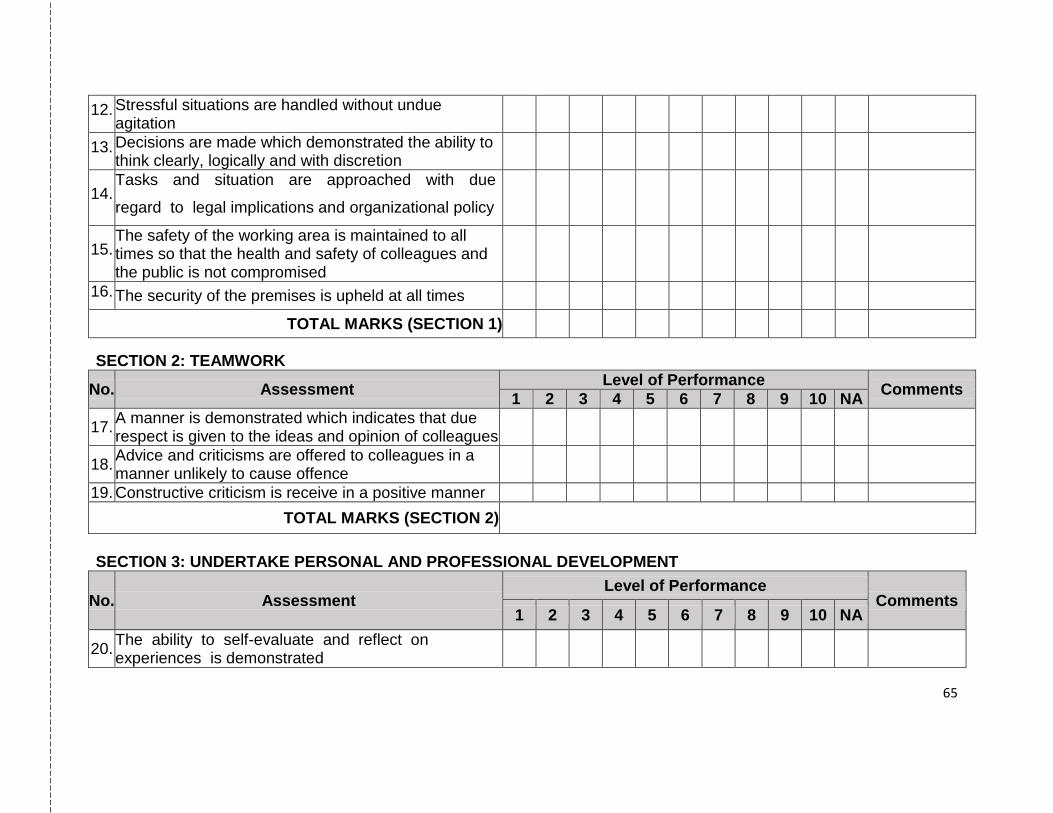
12. Stressful situations are handled without undue agitation
13. Decisions are made which demonstrated the ability to think clearly, logically and with discretion
14. Tasks and situation are approached with due
regard to legal implications and organizational policy
15. The safety of the working area is maintained to all times so that the health and safety of colleagues and the public is not compromised
16. The security of the premises is upheld at all times
TOTAL MARKS (SECTION 1)
SECTION 2: TEAMWORK
No. Assessment Level of Performance
Comments 1 2 3 4 5 6 7 8 9 10 NA
17. A manner is demonstrated which indicates that due respect is given to the ideas and opinion of colleagues
18. Advice and criticisms are offered to colleagues in a manner unlikely to cause offence
19. Constructive criticism is receive in a positive manner
TOTAL MARKS (SECTION 2)
SECTION 3: UNDERTAKE PERSONAL AND PROFESSIONAL DEVELOPMENT
No. Assessment Level of Performance
Comments 1 2 3 4 5 6 7 8 9 10 NA
20. The ability to self-evaluate and reflect on experiences is demonstrated
65
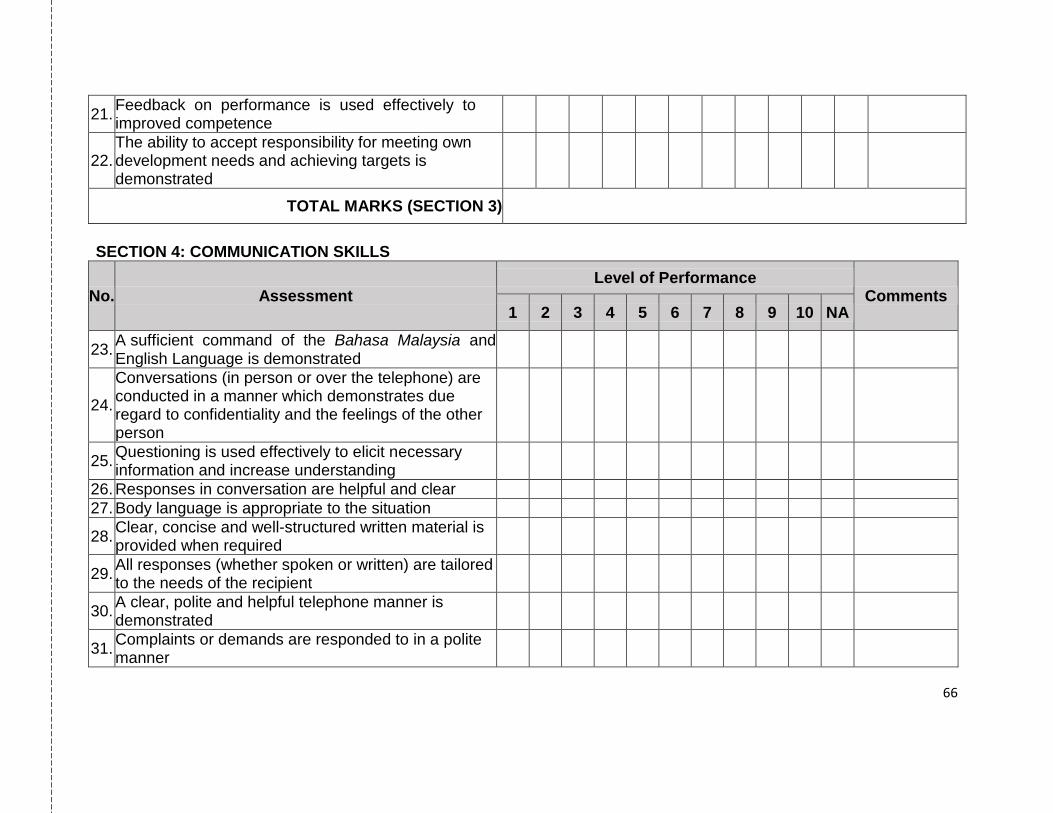
21. Feedback on performance is used effectively to improved competence
22. The ability to accept responsibility for meeting own development needs and achieving targets is demonstrated
TOTAL MARKS (SECTION 3)
SECTION 4: COMMUNICATION SKILLS
No. Assessment Level of Performance
Comments 1 2 3 4 5 6 7 8 9 10 NA
23. A sufficient command of the Bahasa Malaysia and English Language is demonstrated
24.
Conversations (in person or over the telephone) are conducted in a manner which demonstrates due regard to confidentiality and the feelings of the other person
25. Questioning is used effectively to elicit necessary information and increase understanding
26. Responses in conversation are helpful and clear
27. Body language is appropriate to the situation
28. Clear, concise and well-structured written material is provided when required
29. All responses (whether spoken or written) are tailored to the needs of the recipient
30. A clear, polite and helpful telephone manner is demonstrated
31. Complaints or demands are responded to in a polite manner
66
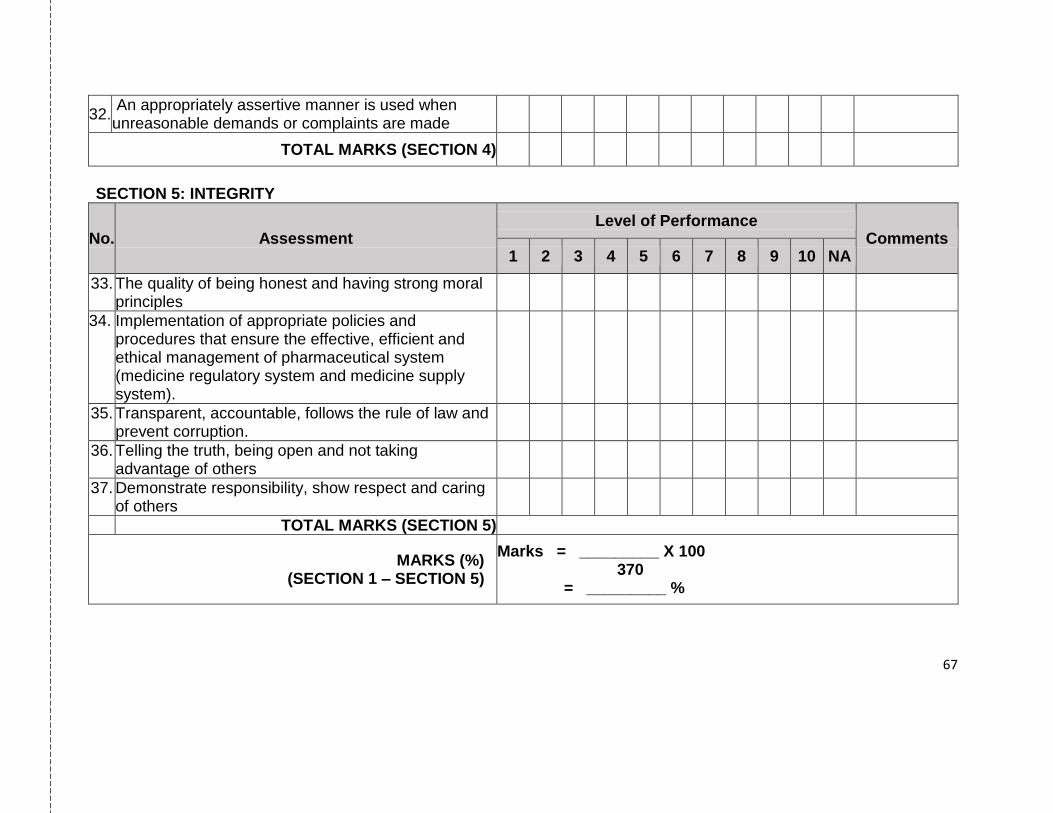
32. An appropriately assertive manner is used when unreasonable demands or complaints are made
TOTAL MARKS (SECTION 4)
SECTION 5: INTEGRITY
No. Assessment Level of Performance
Comments 1 2 3 4 5 6 7 8 9 10 NA
33. The quality of being honest and having strong moral principles
34. Implementation of appropriate policies and procedures that ensure the effective, efficient and ethical management of pharmaceutical system (medicine regulatory system and medicine supply system).
35. Transparent, accountable, follows the rule of law and prevent corruption.
36. Telling the truth, being open and not taking advantage of others
37. Demonstrate responsibility, show respect and caring of others
TOTAL MARKS (SECTION 5)
MARKS (%) (SECTION 1 – SECTION 5)
Marks = _________ X 100 370 = _________ %
67
Community Pharmacy
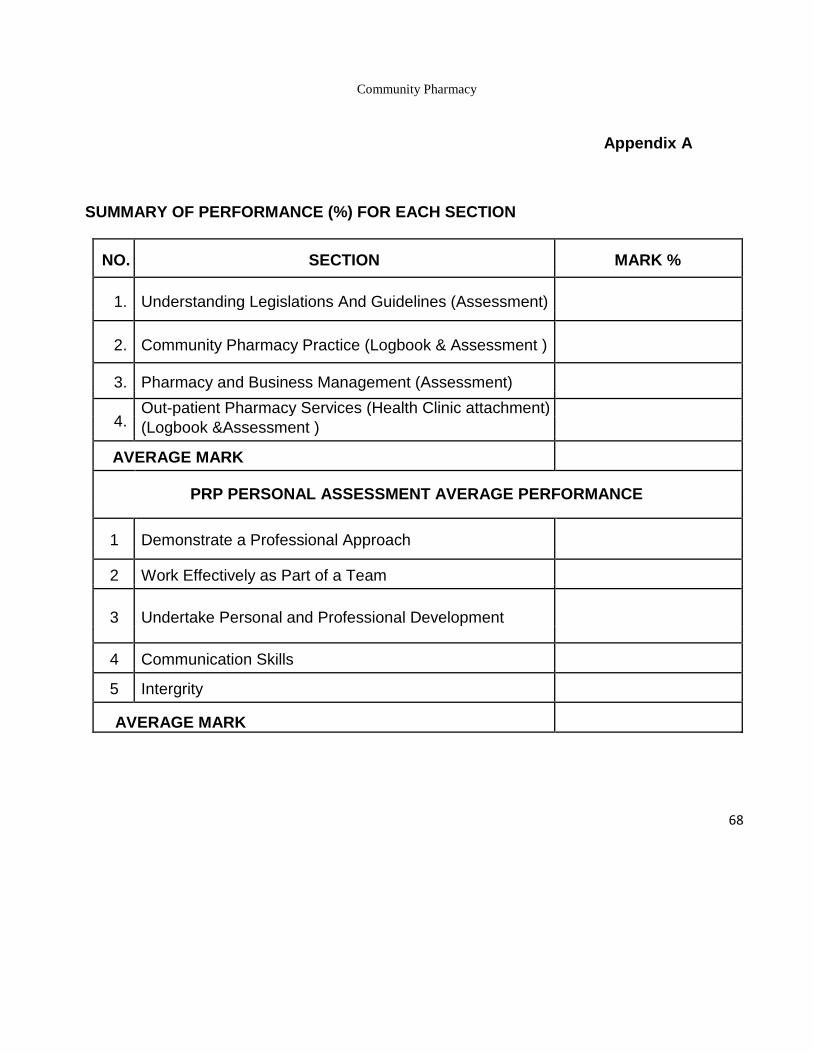
Appendix A
SUMMARY OF PERFORMANCE (%) FOR EACH SECTION
NO. SECTION MARK %
1. Understanding Legislations And Guidelines (Assessment)
2. Community Pharmacy Practice (Logbook & Assessment )
3. Pharmacy and Business Management (Assessment)
4. Out-patient Pharmacy Services (Health Clinic attachment)
(Logbook &Assessment )
AVERAGE MARK
PRP PERSONAL ASSESSMENT AVERAGE PERFORMANCE
1 Demonstrate a Professional Approach
2 Work Effectively as Part of a Team
3 Undertake Personal and Professional Development
4 Communication Skills
5 Intergrity
AVERAGE MARK
68
Community Pharmacy
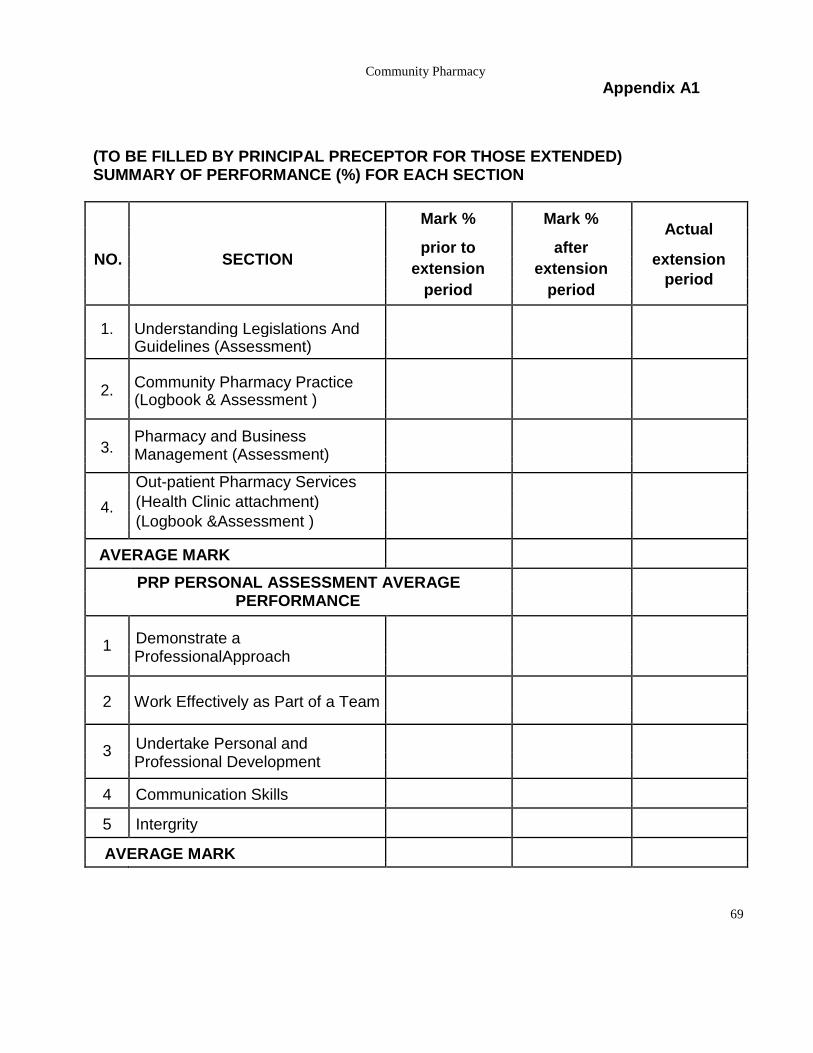
Appendix A1
(TO BE FILLED BY PRINCIPAL PRECEPTOR FOR THOSE EXTENDED) SUMMARY OF PERFORMANCE (%) FOR EACH SECTION
Mark % Mark % Actual
prior to after NO. SECTION extension
extension extension period
period period
1. Understanding Legislations And Guidelines (Assessment)
2. Community Pharmacy Practice (Logbook & Assessment )
3. Pharmacy and Business
Management (Assessment)
Out-patient Pharmacy Services
4. (Health Clinic attachment)
(Logbook &Assessment )
AVERAGE MARK
PRP PERSONAL ASSESSMENT AVERAGE
PERFORMANCE
1 Demonstrate a
ProfessionalApproach
2 Work Effectively as Part of a Team
3 Undertake Personal and
Professional Development
4 Communication Skills
5 Intergrity
AVERAGE MARK
69
Community Pharmacy
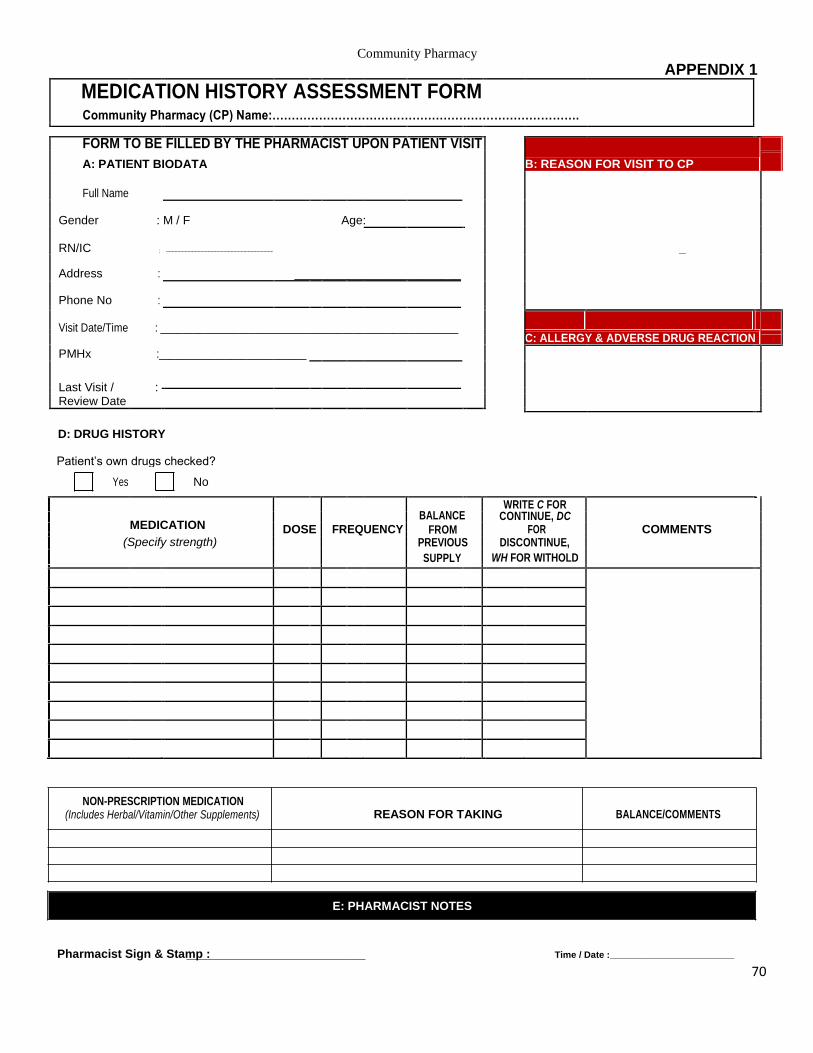
APPENDIX 1
MEDICATION HISTORY ASSESSMENT FORM
Community Pharmacy (CP) Name:…………………………………………………………………….
FORM TO BE FILLED BY THE PHARMACIST UPON PATIENT VISIT
B: REASON FOR VISIT TO CP
A: PATIENT BIODATA
Full Name
Gender : M / F Age:
RN/IC : --------------------------------------------------------------------------- _
Address : _________________________
Phone No :
Visit Date/Time : ______________________________________________________
C: ALLERGY & ADVERSE DRUG REACTION
PMHx :___________________________
Last Visit / :
Review Date
D: DRUG HISTORY
Patient’s own drugs checked?
Yes No
BALANCE
WRITE C FOR
MEDICATION CONTINUE, DC
DOSE FREQUENCY FROM FOR COMMENTS
(Specify strength)
PREVIOUS DISCONTINUE,
SUPPLY WH FOR WITHOLD
NON-PRESCRIPTION MEDICATION
REASON FOR TAKING BALANCE/COMMENTS (Includes Herbal/Vitamin/Other Supplements)
E: PHARMACIST NOTES
Pharmacist Sign & Stamp : Time / Date :________________________
70
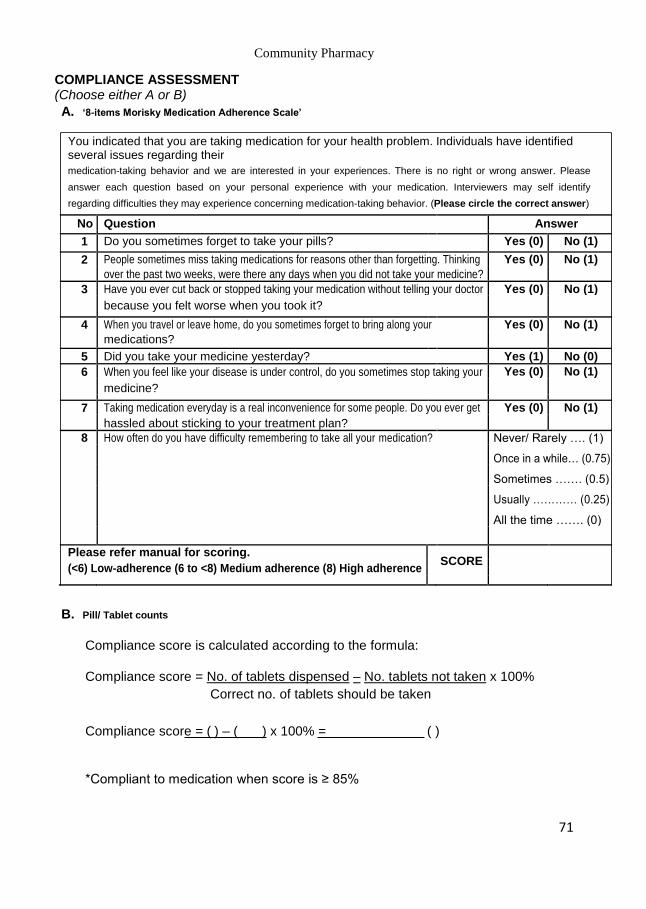
Community Pharmacy COMPLIANCE ASSESSMENT (Choose either A or B) A. ‘8-items Morisky Medication Adherence Scale’
You indicated that you are taking medication for your health problem. Individuals have identified several issues regarding their medication-taking behavior and we are interested in your experiences. There is no right or wrong answer. Please
answer each question based on your personal experience with your medication. Interviewers may self identify
regarding difficulties they may experience concerning medication-taking behavior. (Please circle the correct answer)
No Question Answer
1 Do you sometimes forget to take your pills? Yes (0) No (1)
2 People sometimes miss taking medications for reasons other than forgetting. Thinking Yes (0) No (1)
over the past two weeks, were there any days when you did not take your medicine?
3 Have you ever cut back or stopped taking your medication without telling your doctor Yes (0) No (1)
because you felt worse when you took it?
4 When you travel or leave home, do you sometimes forget to bring along your Yes (0) No (1)
medications?
5 Did you take your medicine yesterday? Yes (1) No (0)
6 When you feel like your disease is under control, do you sometimes stop taking your Yes (0) No (1)
medicine?
7 Taking medication everyday is a real inconvenience for some people. Do you ever get Yes (0) No (1)
hassled about sticking to your treatment plan?
8 How often do you have difficulty remembering to take all your medication? Never/ Rarely …. (1)
Once in a while… (0.75)
Sometimes ……. (0.5)
Usually ………… (0.25)
All the time ……. (0)
Please refer manual for scoring.
SCORE
(<6) Low-adherence (6 to <8) Medium adherence (8) High adherence
B. Pill/ Tablet counts
Compliance score is calculated according to the formula:
Compliance score = No. of tablets dispensed – No. tablets not taken x 100% Correct no. of tablets should be taken
Compliance score = ( ) – ( ) x 100% = ( )
*Compliant to medication when score is ≥ 85%
71
Community Pharmacy
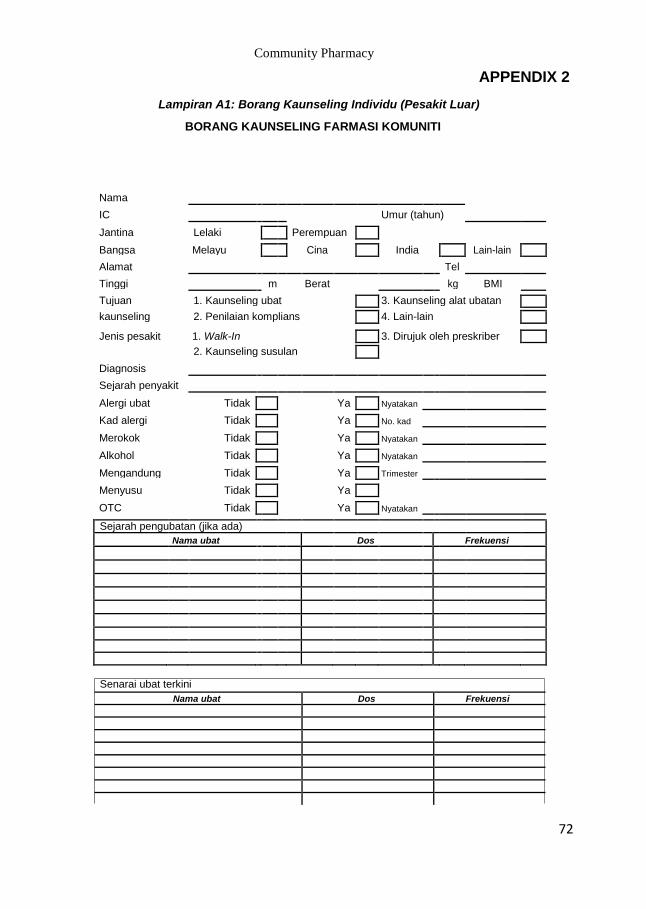
APPENDIX 2
Lampiran A1: Borang Kaunseling Individu (Pesakit Luar)
BORANG KAUNSELING FARMASI KOMUNITI
Nama
IC Umur (tahun)
Jantina Lelaki Perempuan
Bangsa Melayu Cina India Lain-lain
Alamat Tel
Tinggi m Berat kg BMI
Tujuan
1. Kaunseling ubat
3. Kaunseling alat ubatan
kaunseling
2. Penilaian komplians
4. Lain-lain
Jenis pesakit 1. Walk-In 3. Dirujuk oleh preskriber
Diagnosis
2. Kaunseling susulan
Sejarah penyakit
Alergi ubat Tidak Ya Nyatakan
Kad alergi Tidak Ya No. kad
Merokok Tidak Ya Nyatakan
Alkohol Tidak Ya Nyatakan
Mengandung Tidak Ya Trimester
Menyusu Tidak Ya
OTC Tidak Ya Nyatakan
Sejarah pengubatan (jika ada)
Nama ubat Dos Frekuensi
Senarai ubat terkini
Nama ubat Dos Frekuensi
72
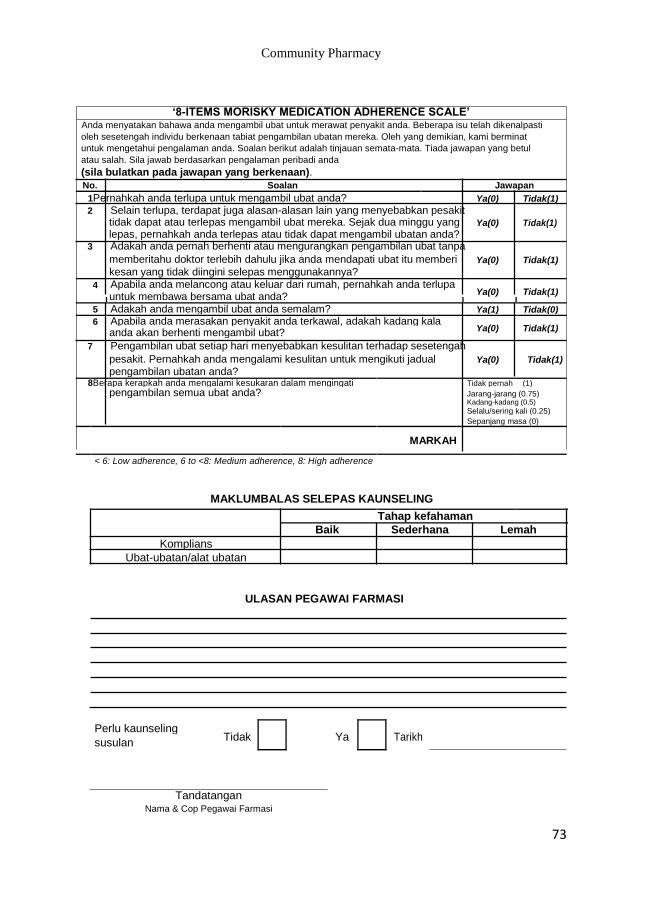
Community Pharmacy
‘8-ITEMS MORISKY MEDICATION ADHERENCE SCALE’
Anda menyatakan bahawa anda mengambil ubat untuk merawat penyakit anda. Beberapa isu telah dikenalpasti
oleh sesetengah individu berkenaan tabiat pengambilan ubatan mereka. Oleh yang demikian, kami berminat
untuk mengetahui pengalaman anda. Soalan berikut adalah tinjauan semata-mata. Tiada jawapan yang betul
atau salah. Sila jawab berdasarkan pengalaman peribadi anda (sila bulatkan pada jawapan yang berkenaan). No. Soalan Jawapan
1Pernahkah anda terlupa untuk mengambil ubat anda? Ya(0) Tidak(1) 2 Selain terlupa, terdapat juga alasan-alasan lain yang menyebabkan pesakit
tidak dapat atau terlepas mengambil ubat mereka. Sejak dua minggu yang Ya(0) Tidak(1)
lepas, pernahkah anda terlepas atau tidak dapat mengambil ubatan anda?
3 Adakah anda pernah berhenti atau mengurangkan pengambilan ubat tanpa memberitahu doktor terlebih dahulu jika anda mendapati ubat itu memberi Ya(0) Tidak(1)
kesan yang tidak diingini selepas menggunakannya?
4 Apabila anda melancong atau keluar dari rumah, pernahkah anda terlupa Ya(0) Tidak(1) untuk membawa bersama ubat anda?
5 Adakah anda mengambil ubat anda semalam? Ya(1) Tidak(0)
6 Apabila anda merasakan penyakit anda terkawal, adakah kadang kala Ya(0) Tidak(1) anda akan berhenti mengambil ubat?
7 Pengambilan ubat setiap hari menyebabkan kesulitan terhadap sesetengah pesakit. Pernahkah anda mengalami kesulitan untuk mengikuti jadual Ya(0) Tidak(1)
pengambilan ubatan anda? 8Berapa kerapkah anda mengalami kesukaran dalam mengingati Tidak pernah (1)
pengambilan semua ubat anda? Jarang-jarang (0.75) Kadang-kadang (0.5)
Selalu/sering kali (0.25)
Sepanjang masa (0)
MARKAH
< 6: Low adherence, 6 to <8: Medium adherence, 8: High adherence
MAKLUMBALAS SELEPAS KAUNSELING
Tahap kefahaman
Baik Sederhana Lemah Komplians
Ubat-ubatan/alat ubatan
ULASAN PEGAWAI FARMASI
Perlu kaunseling Tidak
Ya
Tarikh
susulan
Tandatangan
Nama & Cop Pegawai Farmasi
73
Community Pharmacy
78