Recommendation on 36 months isoniazid preventive therapy ...
30
Recommendation on 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings 2015 update
Transcript of Recommendation on 36 months isoniazid preventive therapy ...
Recommendation on 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
2015 update

Recommendation on 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings

Recommendation on 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
2015 update
WHO Library Cataloguing-in-Publication Data
Recommendation on 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings – 2015 update.
1.Tuberculosis - prevention and control. 2.Tuberculosis - diagnosis. 3.HIV Infections - complications. 4.Isoniazid - therapeutic use. 5.Predictive Value of Tests. 6.Developing Countries. 7.Guideline. I.World Health Organization.
ISBN 978 92 4 150887 2 (NLM classification: WF 220)
© World Health Organization 2015
All rights reserved. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications –whether for sale or for non-commercial distribution– should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Designed by North Creative, Geneva, Switzerland
WHO/HTM/TB/2015.15
WHO/HIV/2015.13
This is an update to the 2011 WHO Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings
http://whqlibdoc.who.int/publications/2011/9789241500708_eng.pdf?ua=1

1
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
Contents
Acknowledgements 2
Declaration and management of conflict of interest 4
Executive summary 6
1. Background and process 7
1.1 Background 7
1.2 Scope of the update to the recommendation 7
1.3 Target audience for the update 7
1.4 Process of development of the guidelines 7
2. Recommendation 9
2.1 Summary of the evidence 9
2.1.1 Incidence of active TB and mortality 9
2.1.2 Adverse events 9
2.1.3 Adherence 9
2.1.4 Effect of TST 10
2.1.5 Effect of concomitant use of IPT with ART 10
2.1.6 Drug resistance 10
2.1.7 Cost–effectiveness of 36 months of IPT 10
2.1.8 Conclusions on the evidence 10
2.2 Balance of benefits and harms 10
2.3 Values and preferences of clients and health-care providers 11
2.4 Resource considerations 11
2.5 Conclusion 11
References 12
Annex 1: Evidence-to-decision framework 13

2
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
Acknowledgements
Overall coordination and writing of the guidelines
Alberto Matteelli with input from Haileyesus Getahun.
WHO Steering Group
Dennis Falzon (Global TB Programme, WHO), Nathan Ford (HIV/AIDS Department, WHO), Haileyesus Getahun (Global TB Programme, WHO), Chris Gilpin (Global TB Programme, WHO), Christian Lienhardt (Global TB Programme, WHO), Knut Lönroth (Global TB Programme, WHO), Alberto Matteelli (Global TB Programme, WHO), Lisa Nelson (HIV/AIDS Department, WHO), Andreas Reis (Knowledge, Ethics and Research Department, WHO), Mukund Uplekar (Global TB Programme, WHO).
Co-chairs of the WHO Guidelines Development Group
Holger Schünemann (McMaster University Health Sciences Centre, Canada), Jay Varma (US Centers for Disease Control and Prevention, United States of America, [USA]).
GRADE methodologist for the WHO Guidelines Development Group
Holger Schünemann (McMaster University Health Sciences Centre, Canada).
Members of the WHO Guidelines Development Group
Ibrahim Abubakar (National Centre for Infectious Disease Surveillance and Control, University College London and Public Health England, United Kingdom of Great Britain and Northern Ireland), Draurio Barreira (National TB Programme, Ministry of Health, Brazil), Susana Marta Borroto Gutierrez (Pedro Kourí Institute of Tropical Medicine, Cuba), Judith Bruchfeld (Karolinska Institute and Karolinska University Hospital, Sweden), Erlina Burhan (Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, University of Indonesia, Indonesia), Solange Cavalcante (Rio de Janeiro Municipal Health Secretariat FIOCRUZ, Brazil), Rolando Cedillos (Servicio de Infectología y Programade Atención Integral en ITS/VIH/SIDA, El Salvador), Richard Chaisson (Center for TB Research, Johns Hopkins University, USA), Cynthia Bin-Eng Chee (Tan Tock Seng Hospital, Singapore), Lucy Chesire (TB Advocacy Consortium, Kenya), Elizabeth Corbett (London School of Hygiene & Tropical Medicine, United Kingdom), Justin Denholm (Royal Melbourne Hospital, Australia), Gerard de Vries (KNCV TB Foundation, the Netherlands), Margaret Gale-Rowe (Public Health Agency of Canada, Canada), Un-Yeong Go (Department of HIV/AIDS and TB Control Korea, Korea Centers for Disease Control and Prevention, Republic of Korea), Alison Grant (London School of Hygiene & Tropical Medicine, United Kingdom), Robert Horsburgh (Department of Epidemiology, Boston University School of Public Health, USA), Asker Ismayilov (Main Medical Department, Ministry of Justice, Azerbaijan), Philippe LoBue (Division of Tuberculosis Elimination, Centers for Disease Control and Prevention, USA), Guy Marks (Woolcock Institute of Medical Research, University of Sydney, Australia), Richard Menzies (Respiratory Division, McGill University, and Montreal Chest Institute, Canada), Giovanni Battista Migliori (WHO Collaborating Centre for TB and Lung Diseases Fondazione Salvatore Maugeri, Italy), Davide Mosca (Migration Health Department, International Organization of Migration, Switzerland), Ya Diul Mukadi (Infectious Disease Division, Bureau for Global Health, US Agency for International Development, USA), Alwyn Mwinga (Zambart Project, Zambia), Lisa Rotz (Centers for Disease Control and Prevention, USA), Holger Schünemann (Clinical Epidemiology & Biostatistics, McMaster University, Canada), Surender Kumar Sharma (Department of Medicine, All India Institute of Medical Sciences, India), Timothy Sterling (Vanderbilt University School of Medicine, USA), Tamara Tayeb (Ministry of Health, Saudi Arabia), Marieke van der Werf (European Centre for Disease Prevention and Control, Sweden), Wim Vandevelde (European AIDS Treatment Group, Belgium), Jay Varma (US Centers for Diseases Control and Prevention, USA), Natalia Vezhnina (HIV/TB and Penal System Projects, Russian Federation), Constantia Voniatis (Clinical Laboratories, Ministry of Health, Cyprus), Robert John Wilkinson (Institute of Infectious Disease and Molecular Medicine, University of Cape Town, South Africa), Takashi Yoshiyama (Division of Respiratory Medicine, Japan Anti-Tuberculosis Association, Japan), Jean Pierre Zellweger (Tuberculosis Competence Centre, Switzerland).

3
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
WHO consultant for systematic review
Saskia den Boon (Independent consultant,Switzerland).
Peer Review Group
Helen Ayles (Zambart Project, Zambia), Constance Benson (University of California, USA), Amy Bloom (US Agency for International Development, USA), Graham Bothamley (Tuberculosis Network, European Study Group Clinical trials, United Kingdom), Gavin Churchyard (The Aurum Institute, South Africa), Daniela Maria Cirillo (San Raffaele del Monte Tabor Foundation, San Raffaele Scientific Institute, Italy), Frank Cobelens (KNCV Tuberculosis Foundation, the Netherlands ), Robert Colebunders (Institute of Tropical Medicine, Belgium), Charles Daley (University of Colorado, USA), Riitta Dlodlo (International Union against TB and Lung Diseases, Zimbabwe ), Raquel Duarte (General Directorate of Health, Portugal), Connie Erkens (KNCV Tuberculosis Foundation, the Netherlands), Brian Farrugia (Geriatric Medicine and Chest Clinic, Malta), Michel Gasana (National TB Programme, Rwanda), Stephen Graham (Centre for International Child Health, Australia), Mark Harrington (Treatment Action Group, USA), Antony Harris (International Union against TB and Lung Diseases, France), Barbara Hauer (Robert Koch Institute, Germany), Diane Havlir (University of California, USA), Einar Heldal (International Union against TB and Lung Diseases, Norway), Rein Houben (Tuberculosis Modelling and Analysis Consortium, United Kingdom), Mohamed Akramul Islam (BRAC Health Programme, Bangladesh), Jerker Jonsson (Swedish Institute for Infectious Disease Control, Sweden), Michael Kimerling (Bill & Melinda Gates Foundation, USA), Christopher Lange (Clinical Infectious Diseases, Medical Clinic Research Center, Germany), Wang Lixia (National Centre for TB Control and Prevention, China), Gary Maartens (University of Cape Town, South Africa), Joan O’Donnell (National TB Programme, National Disease Surveillance Unit, Ireland), Anshu Prakash (Ministry of Health and Family Welfare, India), Ejaz Qadeer (National TB Control Programme, Federal Ministry of Health, Pakistan), Lidija Ristic (Committee for TB, Ministry of Health, Serbia), Laura Sanchez-Cambronero (Ministry of Health, Social Services and Equality, Spain), Andreas Sandgren (European Centre for Disease Prevention and Control, Sweden), Martina Sester (Saarland University, Germany), Joseph Kimagut Sitienei (Ministry of Public Health, Kenya), Alena Skrahina (Republic Scientific and Practical Center for Pulmonology and Tuberculosis, Belarus), Ivan Solovic (National Institute for TB, Lung Diseases and Thoracic Surgery, Slovakia), Elena Suciliene (Children’s Hospital, affiliate of Vilnius University Hospital Santariskiu Klinikos, Lithuania), Soumya Swaminathan (National Institute for Research in Tuberculosis, India), Maarten van Cleeff (KNCV Tuberculosis Foundation, the Netherlands), Francis Varaine (Médecins Sans Frontières, France), Martina Vasakova (Respiratory Diseases and Pulmonology Department at Prague Thomayer Hospital, Czech Republic), Irina Vasilyeva (Ministry of Health, Russian Federation), Mercedes Vinuesa Sebastián (Ministry of Health, Spain), Dalene von Delft (TB PROOF, South Africa), Brita Askeland Winje (Norwegian Institute of Public Health, Norway), Dominik Zenner (Public Health England, United Kingdom).
WHO headquarters and regional offices
Mohamed Abdel Aziz (WHO/EMRO), Annabel Baddeley (WHO/HQ), Masoud Dara (WHO/EURO), Malgorzata Grzemska (WHO/HQ), Ernesto Jaramillo (WHO/HQ), Nobuyuki Nishikiori (WHO/WPRO), Diana Weil (WHO/HQ), Karin Weyer (WHO/HQ).
Acknowledgement of financial support
The development of these guidelines was supported financially by the United States President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development (USAID).
Next update of these guidelines: The next update will be done in conjunction with the revision of the 2011 WHO “Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings”.

4
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
Declaration and management of conflict of interest
All the contributors completed a WHO Declaration of Interest form. All stated declarations of interest were evaluated by three members of the Steering Group (the Legal Department of WHO was consulted when necessary) for the existence of possible financial conflicts of interest which warrant exclusion from membership of the Guidelines Development or Peer Review Groups or from the discussions as part of the guidelines development process. Intellectual conflict of interest was not considered grounds for exclusion from membership of the Guidelines Development Group as broader expertise on Latent TB Infection (LTBI) was the main criteria for selection and representation on the group; the group itself was felt to be large enough to overcome any potential intellectual conflict of interest. During the guidelines development process and the Guideline Development Group meeting, any emergence of intellectual conflict of interest was monitored by the Chairs and the Coordinator of the Secretariat, and any perceived intellectual conflict of interest was discussed with members of the Guidelines Development Group.
The following interests were declared:
WHO Guidelines Development Group:
Ibrahim Abubakar declared that his employer received grants from the National Institutes of Health (£2.7 million for the PREDICT study: Prognostic Evaluation of Interferon Gamma Release Assays (IGRAs) and Skin test in a cohort of 10 000 contacts and migrants) and the UK Department of Health (£900 000 for a randomized controlled trial to assess isoniazid-rifapentine compared to isoniazid-rifampicin on LTBI treatment completion and £490 000 for the Academic, Clinical & Enterprise (ACE) study, and detection of latent TB in emergency departments). He is currently the chair of the UK National Institute for Health and Care Excellence (NICE) guideline development group developing guidelines on TB which includes active and latent TB treatment. NICE pays his employer (University College London) for his time at about £500 a day. He was a member of the European Centre for Disease Prevention and Control (ECDC) guideline development group on IGRAs published in 2011, for which he did not receive any remuneration. He has written extensively on this subject including a recent commentary in The Lancet on LTBI in the UK.
Cynthia Bin-Eng Chee declared that she has attended meetings pertaining to IGRAs sponsored by Qiagen (1st meeting of Asia TB Experts Community, Chiba, Japan 13 May 2012 and the 2nd Meeting of Asia TB Experts Community, Bangkok, Thailand, July 2013) and University of California, San Diego (3rd Global IGRA Symposium, Waikoloa, Hawaii, January 2012) with an estimated overall value of US$ 4500 for travel and accommodation.
Richard Chaisson declared that he received remuneration for consulting on TB drug development from Vertex of US$ 2000 in 2012 one time only and received research grants from the National Institutes of Health, the Centers for Disease Control and Prevention (CDC) and the Gates Foundation of more than US$ 15 million which is ongoing.
Liz Corbett declared that her employer received research grants concerning the public health impact of combined TB prevention from Wellcome Trust grants.
Guy Marks declared that his employer received research grants (related to TB, though not specifically on LTBI) from the National Health and Medical Research Council of Australia.
Richard Menzies declared that he received research support from the Canadian Institutes of Health Research with a total grant related to latent TB infection – approximately C$ 6 million over a six-year period. The main research is a randomized control trial comparing 4 month-RIF to 9-month INH for LTBI (about C$ 1 million each year).
Surender Sharma declared that his employer received a research grant for “impact of HIV infection on latent TB among patients with HIV/TB co-infection” supported by the Department of Biotechnology, Ministry of Science & Technology, Government of India (US$ 133 197.56) for which the project work is over.
Timothy Sterling declared that he received remuneration from Sanofi for a one-day consultancy meeting (and preparation) at the Food and Drug Administration (FDA) to answer questions related to the CDC-sponsored Study 26 of the TB Trials Consortium where he was the protocol chair (US$ 3800 in 2012).

5
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
Peer Review Group:
Gavin Churchyard declared that he received research support grants for the following trials at the Aurum Institute: Rifaquin approximately €500 000 expired in 2011; Remox less than €200 000 which is ongoing; Thibela TB, US$ 32 million expired in 2012; evaluation of Expert MTB/RIF US$ 13 million which is ongoing; evaluation of TB/HIV integration US$ 250 000 expired in 2011.
Raquel Duarte declared that she received payments from 2011 to 2014 for lectures on TB screening in patients with immune mediated inflammatory diseases who are candidate for biological therapy from Pfizer, Abbot and Janssen.
Diane Havlir declared that she received support grants from the National Institutes of Health for research on TB.
Christopher Lange declared that he received remuneration from Celltrion Korea for consultation on the risk of TB related to treatment with bio similar TNF antagonists for one time in 2013.
Martina Sester declared that she received non-monetary support from Qiagen (formerly Cellestis) and Oxford Immunotech to perform investigator-initiated research studies, where the kits were in part provided free-of-charge by the two companies. She received travel support from Qiagen for presentation of the data in scientific meetings. She is a co-inventor for a patent application entitled “in vitro process for the quick determination of a patient’s status relating to infection with Mycobacterium tuberculosis” (international patent number WO2011113953/A1).
Dalene von Delft declared that she received support for giving presentations or speeches at the International Union against TB and Lung Diseases Conferences in 2012 and 2013 from the Treatment Action Group (TAG) and United States Agency for International Development (USAID); support from Janssen Pharmaceuticals to attend the Leadership Summit Critical Path to TB Drug Regimens (CPTR); and, support from the American Society of Tropical Medicine and Hygiene (ASTMH)-AERAS to attend meetings.
Dominik Zenner declared that he is a co-author of one of the underpinning systematic reviews on LTBI treatment and also the head of the TB screening unit in Public Health England and has a professional interest in the subject matter.
All declarations of interest are available on electronic file at the WHO Global Tuberculosis Programme.

6
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
Executive summary
Human immunodeficiency virus (HIV) infection is the strongest risk factor for developing tuberculosis (TB) disease in those with latent or new Mycobacterium tuberculosis infection. TB is responsible for more than a quarter of deaths in people living with HIV. Isoniazid preventive therapy (IPT) is recognized as a key intervention for the prevention of TB among people living with HIV.
In 2011, the World Health Organization (WHO) issued “Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource constrained settings” and conditionally recommended the use of at least 36 months of IPT (as a proxy for lifelong or continuous treatment) for people living with HIV in high TB-prevalence and transmission settings, based on the results of unpublished studies. It was decided to update the evidence as the studies are now published, and explore whether the findings might require any change in the recommendation of lifelong IPT for people living with HIV.
The main objective of this update is to reassess the recommendation to provide IPT for 36 months to children and adults living with HIV, including pregnant women, those receiving antiretroviral therapy (ART), and those who have successfully completed TB treatment and are living in settings with high TB and HIV prevalence and transmission, based on the requirements of the WHO Guidelines Review Committee. One systematic review of the literature was conducted, restricted to randomized controlled trials, and a meta-analysis of all the different outcomes of interest was performed. The GRADE system was used for quality assessment of the body of evidence for each outcome and for going from evidence to recommendations. The recommendation was developed by a Guidelines Development Group composed of external content experts, national TB programme managers, academicians and representatives of patients groups and civil society, led by the WHO Guideline Steering Group. The External Review Group reviewed the draft of the guidelines and gave further contributions.
Based on this, the following conditional recommendation was made: “In resource-constrained settings with high TB incidence and transmission, adults and adolescents living with HIV, who have an unknown or positive tuberculin skin test (TST) status and among whom active TB disease has been safely ruled out, should receive at least 36 months of IPT. IPT should be given to such individuals regardless of whether or not they are receiving ART. IPT should also be given irrespective of the degree of immunosuppression, history of previous TB treatment, and pregnancy.” The quality of evidence was rated as low. The conditionality of the recommendation was primarily due to the fact that implementation of continuous IPT requires considerations of TB epidemiology, health infrastructure, programmatic priorities and patient adherence.

7
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
1. Background and process
1.1 BackgroundHuman immunodeficiency virus (HIV) infection is the strongest risk factor for developing TB disease in those with latent or new Mycobacterium tuberculosis infection. The risk of developing TB is approximately 30 times greater among people living with HIV than among those with no HIV infection (1). TB is responsible for more than a quarter of deaths in people living with HIV. IPT is recognized as a key intervention for the prevention of TB among people living with HIV.
In 2011, WHO issued the “Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource constrained settings” (2). This guideline strongly recommends providing at least six months of IPT for children and adults living with HIV, including pregnant women, those receiving ART, and those who have successfully completed TB treatment. It also conditionally recommends providing IPT for 36 months (as a proxy for lifelong or continuous treatment) to children and adults living with HIV in settings with high TB prevalence and transmission. The conditionality of the recommendation was based on the weakness of the evidence, which was based on unpublished data, feasibility concerns and potential adverse events. Following the 2011 WHO guidelines and the conditional recommendation on the 36 months of IPT for people living with HIV in high TB prevalence and transmission settings, new studies including randomized controlled trials were published necessitating an update of the recommendation (3–5).
1.2 Scope of the update to the recommendationThe main objective is to reassess the 2011 recommendation to provide IPT for 36 months (as a proxy for lifelong or continuous treatment) to children and adults living with HIV, including pregnant women, those receiving ART, and those who have successfully completed TB treatment and are living in settings with high TB and HIV prevalence and transmission. As the 2011 recommendation on 36 months of IPT was based on unpublished data, it was decided to update the evidence as the studies are now published and explore whether the findings might require any change in the recommendation of lifelong IPT for people living with HIV.
1.3 Target audience for the updateThis update is aimed at health-care workers providing care for people living with HIV, policy-makers and health programme managers working in the field of HIV and TB in resource-constrained settings with high TB and HIV prevalence. These guidelines are also intended for governments, nongovernmental organizations, donors and patient support groups who address HIV and TB.
1.4 Process of development of the guidelines The update to this recommendation was conducted in parallel with the WHO guidelines development process on the management of latent TB infection. The following three groups were established to develop the guidelines in agreement with the WHO Guideline Review Committee’s recommended process:
• The WHO Guideline Steering Group with the Global TB Programme, the HIV/AIDS Department, and the Department of Knowledge, Ethics and Research to lead the guideline development process;
• The Guidelines Development Group (hereafter known as the Panel) comprising external content experts, national programme managers, academics and representatives of civil society to provide inputs throughout all the stages of the guideline development process. Panel members were carefully selected to ensure relevant expertise, and geographic and gender balanced representation of both stakeholders and patient groups; and
• The External Review Group comprising individuals with expertise in HIV care, latent TB infection and TB/HIV co-infection to provide inputs and perspectives at selected stages of the guideline development process and to review the final draft of the guidelines.

8
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
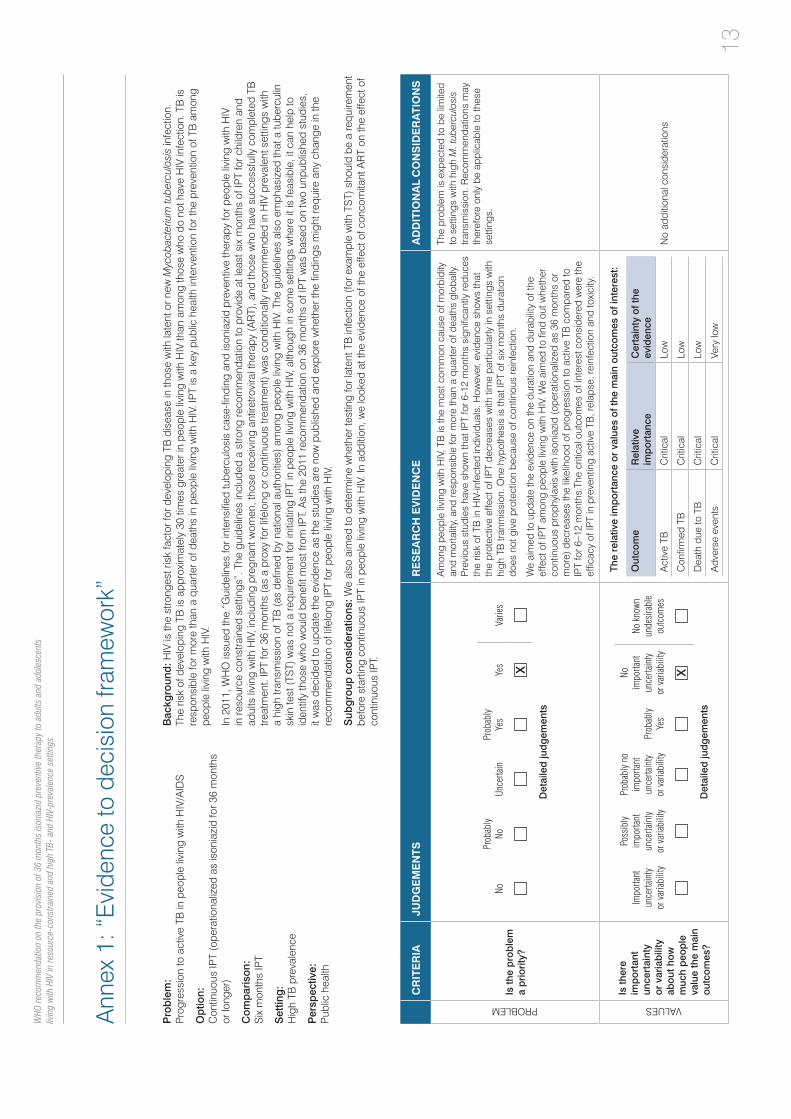
The WHO Steering Group identified the following key question and developed the scoping document: In people living with HIV/AIDS, does prophylaxis with 36 months (or longer) of IPT versus six months of IPT decrease the likelihood of progression to active TB? The Panel reviewed the document and agreed with the WHO Steering Group regarding the scope of the update.
The table below shows the list of potential outcomes of interest, which were pre-defined for the question and were circulated to all members of the Panel. Each member of the Panel scored the importance of each outcome on a scale of 1 to 9 as follows: 1 to 3 to indicate an outcome considered not important; 4 to 6 to indicate an outcome considered important; 7 to 9 to indicate an outcome considered critical.
Outcomes Relative importance (average)
Active TB incidence (presumptive, probable, confirmed) 9
Confirmed TB 9
Mortality 9
Progression of HIV disease 8
Adverse events 8
Adherence 7
TB drug resistance 7
Cost–effectiveness 7
Interval to active TB 6
Interval to death 6
The Panel met in person and also conducted meetings electronically. The meetings were co-chaired by a technical expert and a Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodologist. Recommendations were drafted taking into consideration the costs, feasibility, acceptability and values and preferences of the individuals and stakeholders, as well as the benefits/harms profile. Recommendations and their relative strengths were decided by consensus and when consensus could not be reached according to the judgment of the Chairs, open voting was used to arrive at a decision. Consensus was defined either as unanimous or majority agreement. A majority was defined by a proportion of more than 50% of those having the right to vote and expressing their vote. Additional inputs from the Peer Review Group were also obtained and incorporated. For definitions of strength of recommendations and evidence, please refer to the original WHO 2011 guidelines.
9
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
2. Recommendation
In resource-constrained settings with high TB incidence and transmission, adults and adolescents living with HIV, who have an unknown or positive tuberculin skin test (TST) status and among whom active TB disease has been safely ruled out, should receive at least 36 months of isoniazid preventive therapy (IPT). IPT should be given to such individuals regardless of whether or not they are receiving ART. IPT should also be given irrespective of the degree of immunosuppression, history of previous TB treatment, and pregnancy.
(Conditional recommendation, low quality of evidence).
Remarks: People living with HIV in high TB incidence and transmission settings, regardless of their TST status, benefit more from IPT of 36 months or longer, compared to six-month IPT, with greater protective benefit in those with a positive TST. There is a significant additional benefit from longer-term IPT for those receiving ART. TST is encouraged whenever feasible, but it is not a pre-requisite for IPT. If TST is performed, those with a negative TST should not receive 36 months of IPT. Settings with high TB incidence and transmission should be defined by national authorities, taking into consideration the local epidemiology and transmission of both TB and HIV.
2.1 Summary of the evidence A systematic review was carried out and a meta-analysis of the three identified randomized controlled trials was performed (Annex 1). The number of events of the pre-specified outcomes was compared in those receiving continuous IPT and those who received a six-month IPT regimen or an equivalent one (isoniazid plus ethambutol). Data on population with “irrespective of TST” status obtained from the meta-analysis was assumed to be equivalent to the population “with unknown TST” status to draw the recommendation.
2.1.1 Incidence of active TB and mortality
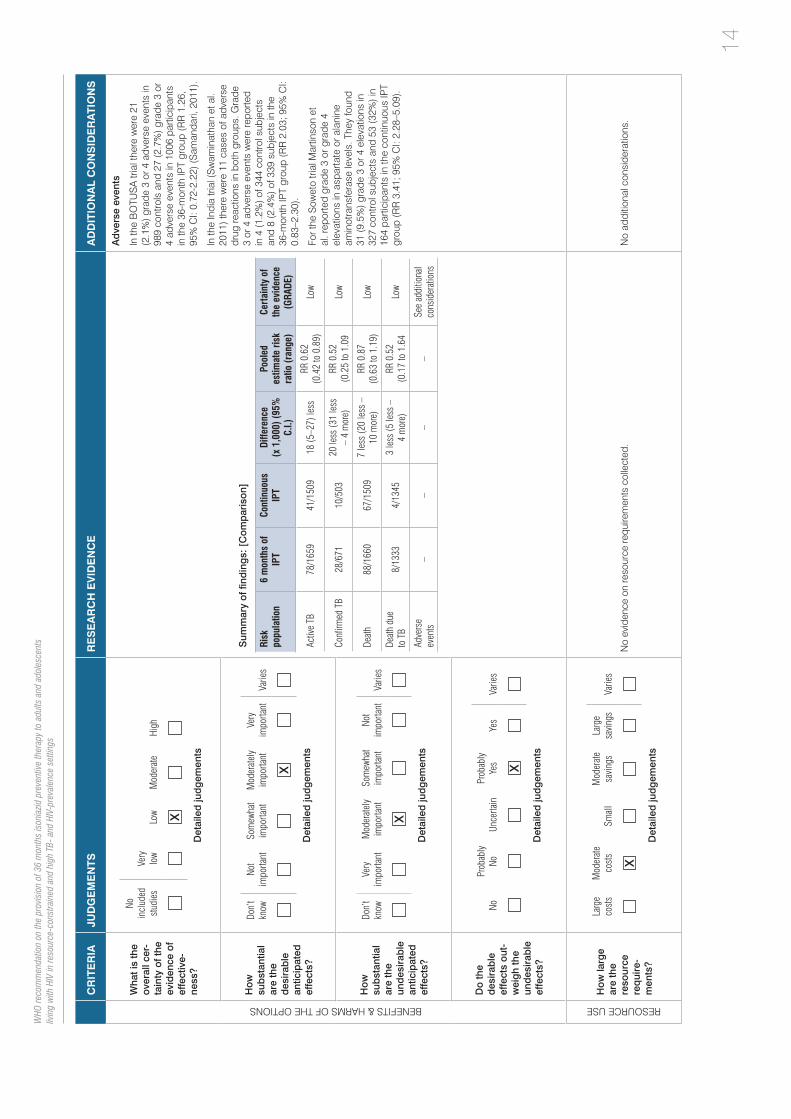
In the population with “irrespective of TST” status, the incidence of active TB was significantly lower in the continuous IPT group (41 cases among 1509 individuals, 2.7%) compared to the control group (78 cases among 1659 individuals, 4.7%), (relative risk, RR, 0.62; 95% confidence interval, CI: 0.42–0.89). There was no difference in mortality (RR 0.87; 95% CI: 0.63–1.19) between the two groups.
2.1.2 Adverse events
A meta-analysis of adverse events was not performed due to the heterogeneity in the definition of side effects and reporting among the studies. One of the studies (Annex 1) reported significantly more grade 3 or grade 4 elevations in the aspartate and/or alanine aminotransferase levels in the continuous isoniazid group (RR 3.41; 95% CI: 2.28–5.09) (5). The other two studies reported a non-significant increased risk for grade 3 or 4 adverse events in the continuous IPT group (3, 4). The systematic review we performed identified five additional observational studies describing 36 months of IPT in persons living with HIV. No information on side effects was available in these studies.
2.1.3 Adherence
Adherence was not adequately defined and reported in the studies. Swaminathan et al. did not report information on adherence (4). Samandari et al. found that high adherence to continued isoniazid treatment in participants with a positive tuberculin skin test was associated with the largest decrease in tuberculosis incidence (3). In Martinson’s et al study adherence was 83.8% in the 6-month–isoniazid group, compared to 60.4% in patients on 36 months treatment (5).

10
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
2.1.4 Effect of TST
When the analysis was restricted to individuals with a positive TST, the protective effect on active TB was stronger (RR 0.51; 95% CI: 0.30–0.86); in those with a negative TST, the difference between the two treatment regimens was not statistically significant (RR 0.73; 95% CI: 0.43–1.26).
A reduction in mortality was also seen among TST-positive individuals (RR 0.50; 95% CI: 0.27–0.91) but not among TST-negative individuals (RR 1.29; 95% CI: 0.77–2.16).
2.1.5 Effect of concomitant use of IPT with ART
Samandari et al. study carried out in Botswana reported data on TB incidence according to the IPT group and duration of ART (3). The results of this study showed additional protective benefit from IPT among people living with HIV receiving 360 days of ART and who were TST positive; in TST-negative persons, IPT had only a marginal beneficial effect in addition to ART.
2.1.6 Drug resistance
All three studies were reviewed to appraise whether 36 months of IPT leads to significant development of drug resistance compared to six months of IPT. Martinson’s et al study reported resistance rates in both the continuous IPT and six-month IPT groups. They found one case of isoniazid resistance in 164 individuals (0.6%) receiving 36 months of IPT and 0 (0%) cases in 327 individuals receiving six months of IPT (RR 5.96; 95% CI: 0.24–146) (5). The other two studies reported that the observed proportion of resistant cases among confirmed TB cases was similar to the expected rate (3,4).
2.1.7 Cost–effectiveness of 36 months of IPT
Data on the cost–effectiveness of continuous IPT is limited. In a study from India (6) the incremental cost per year of life saved for people living with HIV (27% of whom were on ART), compared to no intervention, was estimated to be US$ 1,140 for six months of IPT and US$ 3120 for 36 months of IPT. In this study 36 months of IPT only provided one additional month of life; an increase from a projected life expectancy of 136.1 months to 137.1 months. Another study from Botswana (7) found that, compared to six months of IPT, treating TST-positive persons living with HIV with a 36-month IPT would result in an incremental cost of US$ 1282 per TB case averted and of US$ 1436 per death averted.
2.1.8 Conclusions on the evidence
In summary, these data show that, for people living with HIV in settings with high TB prevalence and transmission, continuous IPT reduced the risk of developing active TB by 38% compared to six-months of IPT. The effect was stronger in those with a positive TST (49% for active TB and 50% for death). In those with a negative TST, neither effect was significant.
Continuous IPT conferred significant additional protection to people living with HIV who are on ART. In the study reported by Samandari (3), the effect appeared to be limited to TST-positive individuals. Additionally, the Panel also considered the results of a recently published study showing a significant benefit of administering 12-month IPT among TST-negative people living with HIV receiving ART in South Africa (8).
There is insufficient evidence to indicate whether or not continuous use of isoniazid increases the risk of isoniazid resistance.
2.2 Balance of benefits and harms After careful consideration of the benefits/harms balance, the Panel concluded by unanimous consensus that, for people living with HIV in settings of high TB prevalence and transmission, continuous IPT is beneficial and probably outweighs the risk of adverse events. Although not statistically significant, the Panel noted a reduction in TB incidence of 27% among TST-negative persons. The Panel concluded by majority agreement that there is benefit in providing IPT for 36 months or longer to people living with HIV regardless of their TST status in settings

11
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
of high TB prevalence and transmission. TST is encouraged whenever feasible and in this case continuous IPT should be limited to people living with HIV with a positive TST. Continuous IPT is recommended regardless of the ART status. The Panel underlined the importance of regular adverse event monitoring and measures to ensure a high level of treatment adherence and completion for people living with HIV who will receive continuous IPT depending on the national and local context.
2.3 Values and preferences of clients and health-care providersThe Panel noted that the current global implementation of six-month IPT for people living with HIV is very low (1), and the provision of continuous IPT as a public health intervention is almost non-existent, even in settings with high TB prevalence and transmission. Concern was also expressed that treatment completion rates and adherence may be lower with longer treatment (9-11). In addition, the Panel recognized that concerns about the development of resistance to isoniazid (12) as well as about the possible need for TST before starting continuous IPT (13), are potential barriers to implementation. National TB and HIV programmes should consider the local epidemiology and health infrastructure context to identify and address these potential challenges. It was also noted that individual factors among people living with HIV should be considered prior to starting treatment.
2.4 Resource considerations The Panel noted that the decision to extend the duration of IPT among people living with HIV to 36 months or longer, should include consideration of the availability and efficient use of resources. In addition the Panel stated the need for national programmes to consider the potential implications for additional human and financial resources necessary to implement continuous IPT compared to a six-month IPT regimen.
2.5 Conclusion The Panel agreed to retain the conditional strength of the recommendation based on majority agreement. The conditionality of the recommendation was primarily due to the fact that implementation of continuous IPT requires considerations of TB epidemiology, health infrastructure and programmatic priorities.

12
12
WHO recommendation on the provision of 36 months isoniazid preventive therapy to adults and adolescents living with HIV in resource-constrained and high TB- and HIV-prevalence settings
References
1. Global tuberculosis control 2014 report. Geneva: World Health Organization; 2014.
2. Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings. Geneva: World Health Organization; 2011.
3. Samandari T, Agizew TB, Nyirenda S, Tedla Z, Sibanda T, Shang N, et al. 6-month versus 36-month isoniazid preventive treatment for tuberculosis in adults with HIV infection in Botswana: a randomised, double-blind, placebo-controlled trial. Lancet. 2011;377(9777):1588–98.
4. Swaminathan S, Menon PA, Gopalan N, Perumal V, Santhanakrishnan RK, Ramachandran R, et al. Efficacy of a six-month versus a 36-month regimen for prevention of tuberculosis in HIV-infected persons in India: a randomized clinical trial. PloS One. 2012;7(12):e47400.
5. Martinson NA, Barnes GL, Moulton LH, Msandiwa R, Hausler H, Ram M, et al. New regimens to prevent tuberculosis in adults with HIV infection. N Eng J Med. 2011;365(1):11–20.
6. Pho MT, Swaminathan S, Kumaraswamy N, Losina E, Ponnuraja C, Uhler L, et al. The cost-effectiveness of tuberculosis preventive therapy for HIV-infected individuals in southern India: a trial-based analysis. PLoS One. 2012;7(4):e36001.
7. Gupta S, Abimbola T, Date A, Suthar AB, Bennett R, Sangrujee N, et al. Cost-effectiveness of the Three I’s for HIV/TB and ART to prevent TB among people living with HIV. Int J Tuberc Lung Dis. 2014 Oct;18(10):1159-65.
8. Rangaka MX, Wilkinson RJ, Boulle A, Glynn JR, Fielding K, van Cutsem G, et al. Isoniazid plus antiretroviral therapy to prevent tuberculosis: a randomised double-blind, placebo-controlled trial. Lancet. 2014;384:682–90.
9. Tortajada C, Martinez-Lacasa J, Sánchez F, Jiménez-Fuentes A, De Souza ML, García JF, et al.Is the combination of pyrazinamide plus rifampicin safe for treating latent tuberculosis infection in persons not infected by the human immunodeficiency virus? Int J Tuberc Lung Dis. 2005 Mar,9(3):276–81.
10. Sterling TR, Villarino ME, Borisov AS, Shang N, Gordin F, Bliven-Sizemore E,et al. Three months of rifapentine and isoniazid for latent tuberculosis infection. N Engl J Med. 2011 Dec 8;365(23):2155–66.
11. Villarino ME, Scott NA, Weis SE, Weiner M, Conde MB, Jones B, et al; for the International Maternal Pediatric and Adolescents AIDS Clinical Trials Group (IMPAACT) and the Tuberculosis Trials Consortium (TBTC). Treatment for preventing tuberculosis in children and adolescents: a randomized clinical trial of a 3-Month, 12-dose regimen of a combination of rifapentine and isoniazid. JAMA Pediatr. 2015 Mar 1;169(3):247–255.
12. Balcells ME, Thomas SL, Godfrey-Faussett P, Grant AD. Isoniazid preventive therapy and risk for resistant tuberculosis. Emerg Infect Dis. 2006;12:744–51.
13. Aisu T, Raviglione MC, van Praag E, Eriki P, Narain JP, Barugahare L, et al. Preventive chemotherapy for HIV-associated tuberculosis in Uganda: an operational assessment at a voluntary counselling and testing centre. AIDS. 1995 Mar;9(3):267–73.
1312
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Ann
ex 1
: “E
vide
nce
to d
ecis
ion
fram
ewor
k”
Pro
ble
m:
Pro
gres
sion
to a
ctiv
e TB
in p
eopl
e liv
ing
with
HIV
/AID
S
Op
tion:
C
ontin
uous
IPT
(ope
ratio
naliz
ed a
s is
onia
zid
for 3
6 m
onth
s or
long
er)
Com
par
ison
: S
ix m
onth
s IP
T
Set
ting
: H
igh
TB p
reva
lenc
e
Per
spec
tive:
P
ublic
hea
lth
Bac
kgro
und
: HIV
is th
e st
rong
est r
isk
fact
or fo
r dev
elop
ing
TB d
isea
se in
thos
e w
ith la
tent
or n
ew M
ycob
acte
rium
tube
rcul
osis
infe
ctio
n.
The
risk
of d
evel
opin
g TB
is a
ppro
xim
atel
y 30
tim
es g
reat
er in
peo
ple
livin
g w
ith H
IV th
an a
mon
g th
ose
who
do
not h
ave
HIV
infe
ctio
n. T
B is
re
spon
sibl
e fo
r mor
e th
an a
qua
rter o
f dea
ths
in p
eopl
e liv
ing
with
HIV
. IP
T is
a k
ey p
ublic
hea
lth in
terv
entio
n fo
r the
pre
vent
ion
of T
B a
mon
g pe
ople
livi
ng w
ith H
IV.
In 2
011,
WH
O is
sued
the
“Gui
delin
es fo
r int
ensi
fied
tube
rcul
osis
cas
e-fin
ding
and
ison
iazi
d pr
even
tive
ther
apy
for p
eopl
e liv
ing
with
HIV
in
reso
urce
con
stra
ined
set
tings
”. T
he g
uide
lines
incl
uded
a s
trong
reco
mm
enda
tion
to p
rovi
de a
t lea
st s
ix m
onth
s of
IPT
for c
hild
ren
and
adul
ts li
ving
with
HIV
, inc
ludi
ng p
regn
ant w
omen
, tho
se re
ceiv
ing
antir
etro
vira
l the
rapy
(AR
T), a
nd th
ose
who
hav
e su
cces
sful
ly c
ompl
eted
TB
tre
atm
ent.
IPT
for 3
6 m
onth
s (a
s a
prox
y fo
r life
long
or c
ontin
uous
trea
tmen
t) w
as c
ondi
tiona
lly re
com
men
ded
in H
IV p
reva
lent
set
tings
with
a
high
tran
smis
sion
of T
B (a
s de
fined
by
natio
nal a
utho
ritie
s) a
mon
g pe
ople
livi
ng w
ith H
IV. T
he g
uide
lines
als
o em
phas
ized
that
a tu
berc
ulin
sk
in te
st (T
ST)
was
not
a re
quire
men
t for
initi
atin
g IP
T in
peo
ple
livin
g w
ith H
IV, a
lthou
gh in
som
e se
tting
s w
here
it is
feas
ible
, it c
an h
elp
to
iden
tify
thos
e w
ho w
ould
ben
efit m
ost f
rom
IPT.
As
the
2011
reco
mm
enda
tion
on 3
6 m
onth
s of
IPT
was
bas
ed o
n tw
o un
publ
ishe
d st
udie
s,
it w
as d
ecid
ed to
upd
ate
the
evid
ence
as
the
stud
ies
are
now
pub
lishe
d an
d ex
plor
e w
heth
er th
e fin
ding
s m
ight
requ
ire a
ny c
hang
e in
the
reco
mm
enda
tion
of li
felo
ng IP
T fo
r peo
ple
livin
g w
ith H
IV.
Sub
gro
up c
onsi
der
atio
ns: W
e al
so a
imed
to d
eter
min
e w
heth
er te
stin
g fo
r lat
ent T
B in
fect
ion
(for e
xam
ple
with
TS
T) s
houl
d be
a re
quire
men
t be
fore
sta
rting
con
tinuo
us IP
T in
peo
ple
livin
g w
ith H
IV. I
n ad
ditio
n, w
e lo
oked
at t
he e
vide
nce
of th
e ef
fect
of c
onco
mita
nt A
RT
on th
e ef
fect
of
cont
inuo
us IP
T.
CR
ITE
RIA
JUD
GE
ME
NTS
RE
SE
AR
CH
EV
IDE
NC
EA
DD
ITIO
NA
L C
ON
SID
ER
ATI
ON
S
PROBLEM
Is th
e p
rob
lem
a
prio
rity?
NoPr
obab
ly
NoUn
certa
inPr
obab
lyYe
sYe
sVa
ries
Det
aile
d ju
dg
emen
ts
Am
ong
peop
le li
ving
with
HIV
, TB
is th
e m
ost c
omm
on c
ause
of m
orbi
dity
an
d m
orta
lity,
and
resp
onsi
ble
for m
ore
than
a q
uarte
r of d
eath
s gl
obal
ly.
Pre
viou
s st
udie
s ha
ve s
how
n th
at IP
T fo
r 6-1
2 m
onth
s si
gnifi
cant
ly re
duce
s th
e ris
k of
TB
in H
IV-in
fect
ed in
divi
dual
s. H
owev
er, e
vide
nce
show
s th
at
the
prot
ectiv
e ef
fect
of I
PT
decr
ease
s w
ith ti
me
parti
cula
rly in
set
tings
with
hi
gh T
B tr
anm
issi
on. O
ne h
ypot
hesi
s is
that
IPT
of s
ix m
onth
s du
ratio
n do
es n
ot g
ive
prot
ectio
n be
caus
e of
con
tinou
s re
infe
ctio
n.
We
aim
ed to
upd
ate
the
evid
ence
on
the
dura
tion
and
dura
bilit
y of
the
effe
ct o
f IP
T am
ong
peop
le li
ving
with
HIV
. We
aim
ed to
find
out
whe
ther
co
ntin
uous
pro
phyl
axis
with
ison
iazi
d (o
pera
tiona
lized
as
36 m
onth
s or
m
ore)
dec
reas
es th
e lik
elih
ood
of p
rogr
essi
on to
act
ive
TB c
ompa
red
to
IPT
for 6
–12
mon
ths.
The
criti
cal o
utco
mes
of i
nter
est c
onsi
dere
d w
ere
the
effic
acy
of IP
T in
pre
vent
ing
activ
e TB
, rel
apse
, rei
nfec
tion
and
toxi
city
.
The
prob
lem
is e
xpec
ted
to b
e lim
ited
to s
ettin
gs w
ith h
igh
M. t
uber
culo
sis
trans
mis
sion
. Rec
omm
enda
tions
may
th
eref
ore
only
be
appl
icab
le to
thes
e se
tting
s.
VALUES
Is th
ere
imp
orta
nt
unce
rtai
nty
or v
aria
bili
ty
abou
t how
m
uch
peo
ple
va
lue
the
mai
n ou
tcom
es?
Impo
rtant
un
certa
inty
or
var
iabi
lity
Poss
ibly
im
porta
nt
unce
rtain
ty
or v
aria
bilit
y
Prob
ably
no
impo
rtant
un
certa
inty
or
var
iabi
lity
Prob
ably
Yes
No
impo
rtant
un
certa
inty
or
var
iabi
lity
No k
nown
un
desi
rabl
e ou
tcom
es
Det
aile
d ju
dg
emen
ts
The
rela
tive
imp
orta
nce
or v
alue
s of
the
mai
n ou
tcom
es o
f int
eres
t:
Out
com
eR
elat
ive
im
por
tanc
eC
erta
inty
of t
he
evid
ence
Act
ive
TBC
ritic
alLo
w
Con
firm
ed T
BC
ritic
alLo
w
Dea
th d
ue to
TB
Crit
ical
Lo
w
Adv
erse
eve
nts
Crit
ical
Ve
ry lo
w
No
addi
tiona
l con
side
ratio
ns
14
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
CR
ITE
RIA
JUD
GE
ME
NTS
RE
SE
AR
CH
EV
IDE
NC
EA
DD
ITIO
NA
L C
ON
SID
ER
ATI
ON
SBENEFITS & HARMS OF THE OPTIONS
Wha
t is
the
over
all c
er-
tain
ty o
f the
ev
iden
ce o
f ef
fect
ive-
ness
?
Noin
clud
edst
udie
sVe
ry
low
Low
Mod
erat
eHi
gh
Det
aile
d ju
dg
emen
ts
Sum
mar
y of
find
ing
s: [
Com
par
ison
]
Risk
po
pula
tion
6 m
onth
s of
IP
TCo
ntin
uous
IP
TDi
ffere
nce
(x
1,0
00) (
95%
C.
I.)
Pool
ed
estim
ate
risk
ratio
(ran
ge)
Cert
aint
y of
th
e ev
iden
ce(G
RADE
)
Activ
e TB
78/1
659
41/1
509
18 (5
–27)
less
RR 0
.62
(0.4
2 to
0.8
9)Lo
w
Confi
rmed
TB
28/6
7110
/503
20 le
ss (3
1 le
ss
– 4
mor
e)RR
0.5
2(0
.25
to 1
.09
Low
Deat
h88
/166
067
/150
97
less
(20
less
–
10 m
ore)
RR 0
.87
(0.6
3 to
1.1
9)Lo
w
Deat
h du
e to
TB
8/13
334/
1345
3 le
ss (5
less
–
4 m
ore)
RR 0
.52
(0.1
7 to
1.6
4Lo
w
Adve
rse
even
ts–
––
–Se
e ad
ditio
nal
cons
ider
atio
ns
Ad
vers
e ev
ents
In th
e B
OTU
SA
tria
l the
re w
ere
21
(2.1
%) g
rade
3 o
r 4 a
dver
se e
vent
s in
98
9 co
ntro
ls a
nd 2
7 (2
.7%
) gra
de 3
or
4 ad
vers
e ev
ents
in 1
006
parti
cipa
nts
in th
e 36
-mon
th IP
T gr
oup
(RR
1.2
6,
95%
CI:
0.72
-2.2
2) (S
aman
dari,
201
1).
In th
e In
dia
trial
(Sw
amin
atha
n et
al.
2011
) the
re w
ere
11 c
ases
of a
dver
se
drug
reac
tions
in b
oth
grou
ps. G
rade
3
or 4
adv
erse
eve
nts
wer
e re
porte
d in
4 (1
.2%
) of 3
44 c
ontro
l sub
ject
s an
d 8
(2.4
%) o
f 339
sub
ject
s in
the
36-m
onth
IPT
grou
p (R
R 2
.03;
95%
CI:
0.83
–2.3
0).
For t
he S
owet
o tri
al M
artin
son
et
al. r
epor
ted
grad
e 3
or g
rade
4
elev
atio
ns in
asp
arta
te o
r ala
nine
am
inot
rans
fera
se le
vels
. The
y fo
und
31 (9
.5%
) gra
de 3
or 4
ele
vatio
ns in
32
7 co
ntro
l sub
ject
s an
d 53
(32%
) in
164
parti
cipa
nts
in th
e co
ntin
uous
IPT
grou
p (R
R 3
.41;
95%
CI:
2.28
–5.0
9).
How
su
bst
antia
l ar
e th
e d
esira
ble
an
ticip
ated
ef
fect
s?
Don’
t kn
owNo
t im
porta
ntSo
mew
hat
impo
rtant
Mod
erat
ely
impo
rtant
Very
im
porta
ntVa
ries
Det
aile
d ju
dg
emen
ts
How
su
bst
antia
l ar
e th
e un
des
irab
le
antic
ipat
ed
effe
cts?
Don’
t kn
owVe
ry
impo
rtant
Mod
erat
ely
impo
rtant
Som
ewha
t im
porta
ntNo
t im
porta
ntVa
ries
Det
aile
d ju
dg
emen
ts
Do
the
des
irab
le
effe
cts
out-
wei
gh
the
und
esira
ble
ef
fect
s?
NoPr
obab
ly
NoUn
certa
inPr
obab
lyYe
sYe
sVa
ries
Det
aile
d ju
dg
emen
ts
RESOURCE USE
How
larg
e ar
e th
e re
sour
ce
req
uire
-m
ents
?
Larg
e co
sts
Mod
erat
e co
sts
Smal
lM
oder
ate
savi
ngs
Larg
e sa
ving
sVa
ries
Det
aile
d ju
dg
emen
ts
No
evid
ence
on
reso
urce
requ
irem
ents
col
lect
ed.
No
addi
tiona
l con
side
ratio
ns.

1514
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
CR
ITE
RIA
JUD
GE
ME
NTS
RE
SE
AR
CH
EV
IDE
NC
EA
DD
ITIO
NA
L C
ON
SID
ER
ATI
ON
SRESOURCE USE
How
larg
e is
the
incr
emen
tal
cost
rel
ativ
e to
the
net
ben
efit?
Very
larg
e IC
ERLa
rge
ICER
Mod
erat
eIC
ERSm
all
ICER
Savi
ngs
Varie
s
Det
aile
d ju
dg
emen
ts
In a
stu
dy fr
om In
dia
(Pho
et a
l. 20
12) t
he in
crem
enta
l cos
t per
yea
r of
life
sav
ed fo
r per
sons
livi
ng w
ith H
IV (2
7% o
n A
RT)
, com
pare
d to
no
inte
rven
tion,
was
est
imat
ed to
be
US
$ 11
40 a
nd U
S$
3120
for
six
mon
ths
and
36 m
onth
s of
IPT,
resp
ectiv
ely.
How
ever
, it s
houl
d be
not
ed th
at th
e 36
-mon
th IP
T m
odel
onl
y pr
ovid
ed o
ne a
dditi
onal
m
onth
of l
ife, a
n in
crea
se fr
om a
pro
ject
ed li
fe e
xpec
tanc
y of
136
.1
mon
ths
to 1
37.1
mon
ths.
Ano
ther
stu
dy (G
upta
et a
l. 20
13) f
ound
that
, com
pare
d to
si
x m
onth
s IP
T, tr
eatin
g TS
T-po
sitiv
e pe
rson
s liv
ing
with
HIV
in
Bot
swan
a w
ith 3
6 m
onth
s of
IPT
wou
ld re
sult
in a
n in
crem
enta
l cos
t of
US
$ 12
82 p
er T
B c
ase
aver
ted
and
US
$ 14
36 p
er d
eath
ave
rted.
A m
odel
ling
stud
y (S
mith
et a
l. 20
11) e
valu
atin
g th
e di
ffere
nt
stra
tegi
es to
pre
vent
HIV
-ass
ocia
ted
TB fo
und
that
the
stra
tegy
w
ith 9
0% A
RT
cove
rage
, TB
infe
ctio
n co
ntro
l (IC
), in
tens
ified
TB
ca
se fi
ndin
g (IC
F)/IP
T fo
r 36
mon
ths,
and
Gen
e-Xp
ert l
abor
ator
y di
agno
sis
for T
B c
ase
findi
ng a
verte
d th
e m
ost T
B c
ases
at t
he
low
est c
ost w
ith a
n in
crem
enta
l cos
t–ef
fect
iven
ess
ratio
of U
S$
5547
per
TB
cas
e av
erte
d co
mpa
red
with
the
base
cas
e (5
5% A
RT
cove
rage
and
TB
scr
eeni
ng u
sing
cou
gh).
No
addi
tiona
l con
side
ratio
ns.
EQUITY
Wha
t wou
ld
be
the
imp
act
on h
ealth
in
equi
ties?
Incr
ease
dPr
obab
lyin
crea
sed
Unce
rtain
Prob
ably
redu
ced
Redu
ced
Varie
s
Det
aile
d ju
dg
emen
ts
No
evid
ence
col
lect
ed.
The
Gui
delin
e D
evel
opm
ent G
roup
/Pan
el re
com
men
ds
cons
ider
ing
poss
ible
impa
cts
on h
ealth
ineq
uitie
s of
IPT
for a
ll pe
ople
livi
ng w
ith H
IV v
ersu
s th
ose
peop
le li
ving
w
ith H
IV w
ho a
re T
ST
posi
tive.
ACCEPTABILITY
Is th
e op
tion
acce
pta
ble
to
key
st
akeh
old
ers?
NoPr
obab
ly
NoUn
certa
inPr
obab
lyYe
sYe
sVa
ries
Det
aile
d ju
dg
emen
ts
No
evid
ence
col
lect
ed.
The
num
ber o
f pro
gram
mes
pro
vidi
ng T
B p
reve
ntiv
e th
erap
y in
peo
ple
livin
g w
ith H
IV h
as b
een
low
. The
fo
llow
ing
reas
ons
are
ofte
n gi
ven
for n
ot p
rovi
ding
(c
ontin
uous
) IP
T: lo
w c
ompl
etio
n ra
tes
(adh
eren
ce m
ay
parti
cula
rly b
e a
prob
lem
in p
rolo
nged
trea
tmen
t), a
nd
the
crea
tion
of re
sist
ance
aga
inst
the
drug
s us
ed fo
r pr
ophy
laxi
s (k
ey is
to e
xclu
de a
ctiv
e TB
bef
ore
star
ting
IPT)
. A p
oten
tial t
hird
bar
rier m
ay b
e th
e ne
ed to
test
for
late
nt T
B in
fect
ion
if th
is is
a re
quire
men
t bef
ore
star
ting
IPT.
FEASIBILITY
Is th
e op
tion
feas
ible
to
imp
lem
ent?
NoPr
obab
ly
NoUn
certa
inPr
obab
lyYe
sYe
sVa
ries
Det
aile
d ju
dg
emen
ts
No
evid
ence
col
lect
ed.
TB a
nd H
IV p
rogr
amm
es a
re in
crea
sing
ly b
eing
in
tegr
ated
. Sin
ce h
ealth
-car
e w
orke
rs fr
eque
ntly
mon
itor
HIV
-pos
itive
indi
vidu
als
on A
RT,
it m
ay b
e re
lativ
ely
easy
to a
dd th
e m
anag
emen
t of I
PT.
Thi
s w
ould
invo
lve
scre
enin
g fo
r act
ive
TB, m
onito
ring
adve
rse
even
ts, a
nd
mon
itorin
g ad
here
nce.
HIV
-pos
itive
indi
vidu
als
not (
yet)
on A
RT
are
also
mon
itore
d, p
rovi
ding
opp
ortu
nitie
s to
of
fer c
ontin
uous
IPT.

16
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
SU
MM
AR
Y O
F JU
DG
ME
NTS
Cri
teri
aFa
vour
s 36
mon
ths
of IP
TP
rob
ably
favo
urs
36 m
onth
s of
IPT
Cho
ose
eith
er 3
6 m
onth
s of
IPT
or s
ix m
onth
s of
IPT
Pro
bab
ly fa
vour
s si
x m
onth
s of
IPT
Favo
urs
six
mon
ths
of IP
T
Bal
ance
of e
ffect
s
Pro
blem
Valu
es
Cer
tain
ty o
f the
evi
denc
e of
effe
cts
Res
ourc
e us
e
Equ
ity
Acc
epta
bilit
y
Feas
ibili
ty
Typ
e o
f re
com
men
dat
ion
We
reco
mm
end
36
mon
ths
of
IPT
We
sug
ges
t 36
mon
ths
of IP
TW
e su
gg
est u
sing
eith
er 3
6 m
onth
s of
IPT
or s
ix m
onth
s of
IPT
We
sug
ges
t six
mon
ths
of IP
TW
e re
com
men
dsi
x m
onth
s of
IPT
Rec
om
men
dat
ion
In r
eso
urce
-co
nstr
aine
d s
ettin
gs
with
hig
h T
B in
cid
ence
and
tra
nsm
issi
on
adul
ts a
nd a
do
lesc
ents
livi
ng w
ith H
IV, w
ho
hav
e an
unk
now
n o
r p
osi
tive
tub
ercu
lin s
kin
test
(TS
T) s
tatu
s, a
nd a
mo
ng w
ho
m a
ctiv
e TB
dis
ease
has
bee
n ru
led
out
, sh
oul
d r
ecei
ve a
t le
ast
36 m
ont
hs
of
iso
niaz
id p
reve
ntiv
e th
erap
y (I
PT)
. IP
T sh
oul
d b
e g
iven
to
suc
h in
div
idua
ls r
egar
dle
ss o
f w
het
her
or
not
they
are
rec
eivi
ng A
RT.
IPT
sho
uld
als
o b
e g
iven
irre
spec
tive
of
the
deg
ree
of
imm
uno
sup
pre
ssio
n, h
isto
ry
of
pre
vio
us T
B t
reat
men
t an
d p
reg
nanc
y.
Sub
gro
up c
ons
ider
atio
nsTS
TP
roph
ylax
is w
ith is
onia
zid
for 3
6 m
onth
s or
long
er re
duce
d TB
inci
denc
e in
peo
ple
livin
g w
ith H
IV b
y 38
% c
ompa
red
to IP
T fo
r six
mon
ths.
Tho
ugh
not s
igni
fican
t, pr
olon
ged
IPT
also
see
med
to re
duce
the
inci
denc
e of
con
firm
ed T
B a
nd d
eath
due
to T
B. I
n th
ose
with
con
firm
ed la
tent
TB
infe
ctio
n (a
s m
easu
red
by a
TS
T >
5 m
m),
cont
inuo
us IP
T si
gnifi
cant
ly
redu
ced
the
risk
of a
ctiv
e TB
(by
49%
) and
dea
th (b
y 50
%).
In th
ose
with
a n
egat
ive
TST,
non
e of
the
findi
ngs
wer
e si
gnifi
cant
. The
se fi
ndin
gs a
re c
onsi
sten
t with
thos
e fro
m a
re
cent
sys
tem
atic
revi
ew th
at a
sses
sed
vario
us tr
eatm
ent o
ptio
ns fo
r lat
ent T
B in
fect
ion
in H
IV-in
fect
ed in
divi
dual
s (A
kolo
et a
l. 20
10).
They
foun
d th
at in
TS
T-po
sitiv
e in
divi
dual
s an
y pr
even
tive
treat
men
t red
uced
the
risk
by 6
2% (R
R 0
.38;
95%
CI:
0.25
–0.5
7). T
here
was
no
evid
ence
of e
ffect
on
indi
vidu
als
with
a n
egat
ive
TST
(RR
0.8
9; 9
5% C
I: 0.
64–1
.24)
. C
ontra
dict
ing
thes
e re
sults
, a re
cent
stu
dy th
at c
ompa
red
12 m
onth
s IP
T w
ith p
lace
bo in
HIV
-pos
itive
indi
vidu
als
on A
RT
foun
d a
sign
ifica
nt e
ffect
of I
PT
on th
e ra
te o
f all
TB in
thos
e w
ho w
ere
TST
nega
tive
(adj
uste
d H
azar
d R
atio
(HR
) 0.4
3; 9
5% C
I: 0.
21–0
.86)
, but
not
in th
ose
who
wer
e TS
T po
sitiv
e (a
djus
ted
HR
0.8
6; 9
5% C
I: 0.
37–2
.0) (
Ran
gaka
et a
l. 20
14).
The
mos
t lik
ely
expl
anat
ion
for T
ST
nega
tives
not
ben
efitti
ng a
s m
uch
from
IPT
is th
at th
ey a
re n
ot in
fect
ed w
ith M
. tub
ercu
losi
s. H
owev
er, R
anga
ka a
nd c
o-w
orke
rs m
entio
ned
that
man
y ne
gativ
e TS
T re
sults
in H
IV-in
fect
ed in
divi
dual
s in
are
as w
ith a
hig
h TB
pre
vale
nce
are
likel
y to
be
fals
e ne
gativ
es, e
spec
ially
in th
ose
with
low
er C
D4-
coun
ts. A
stu
dy in
U
gand
a re
porte
d a
high
neg
ativ
e to
pos
itive
TS
T co
nver
sion
rate
of 3
0.2/
100
pers
on-y
ears
in th
e fir
st s
ix m
onth
s af
ter s
tarti
ng A
RT
(Kire
nga
et a
l. 20
13).
AR
TO
nly
the
BO
TUS
A tr
ial (
Sam
anda
ri, 2
011)
repo
rted
data
on
TB in
cide
nce
acco
rdin
g to
the
IPT
grou
p an
d A
RT
dura
tion.
The
resu
lts o
f thi
s st
udy
show
ed th
at in
TS
T po
sitiv
es 3
6 m
onth
s of
IPT
prov
ided
a 4
6% fu
rther
redu
ctio
n in
TB
inci
denc
e co
mpa
red
to s
ix m
onth
s of
IPT,
in th
ose
rece
ivin
g 36
0 da
ys A
RT
(red
uctio
n in
TB
inci
denc
e is
50%
with
six
mon
ths
IPT
and
96%
with
36
mon
ths
IPT,
bot
h co
mpa
red
to a
gro
up re
ceiv
ing
no A
RT
and
six
mon
ths
IPT)
. On
the
cont
rary
, in
TST-
nega
tive
pers
ons,
36
mon
ths
of IP
T pr
ovid
ed o
nly
a 4%
fu
rther
redu
ctio
n in
TB
inci
denc
e on
top
of th
e 50
% re
duct
ion
achi
eved
by
AR
T (a
nd s
ix m
onth
s IP
T), (
redu
ctio
n in
TB
inci
denc
e is
50%
in th
ose
on s
ix m
onth
s IP
T an
d 54
% in
thos
e on
36
mon
ths
IPT,
bot
h co
mpa
red
to a
gro
up re
ceiv
ing
no A
RT
and
six
mon
ths
IPT)
.
Evi
denc
e fro
m a
rece
ntly
pub
lishe
d st
udy
show
ed th
at H
IV-in
fect
ed in
divi
dual
s co
ncur
rent
ly re
ceiv
ing
AR
T si
gnifi
cant
ly b
enefi
tted
from
12
mon
ths
IPT
com
pare
d to
pla
cebo
, re
gard
less
of T
ST
or in
terfe
ron-
gam
ma
rele
ase
assa
y (IG
RA
) sta
tus
(HR
0.6
3; 9
5% C
I: 0.
41–0
.94)
(Ran
gaka
et a
l. 20
14).
Toge
ther
this
see
ms
to in
dica
te th
at th
ere
is a
sig
nific
ant
addi
tiona
l ben
efit f
rom
long
er-te
rm IP
T fo
r peo
ple
livin
g w
ith H
IV a
nd re
ceiv
ing
AR
T in
hig
h TB
-inci
denc
e ar
eas.

1716
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Imp
lem
enta
tion
cons
ider
atio
nsTh
e m
ain
impl
emen
tatio
n co
nsid
erat
ion
is k
now
ing
in w
hich
set
tings
long
-term
IPT
wou
ld b
e of
ben
efit.
Impl
emen
tatio
n of
long
-term
IPT
shou
ld p
ossi
bly
be re
stric
ted
to h
igh
burd
en
TB s
ettin
gs s
uch
as th
ose
incl
uded
in th
e sy
stem
atic
revi
ew (2
012
prev
alen
ce o
f TB
per
100
,000
in In
dia:
230
(155
–319
), B
otsw
ana:
343
(157
–600
), S
outh
Afri
ca: 8
57 (3
05–1
685)
. Six
m
onth
s IP
T in
HIV
-pos
itive
indi
vidu
als
with
a p
ositi
ve T
ST
was
sho
wn
to b
e ef
fect
ive
in p
reve
ntin
g TB
up
to s
even
yea
rs a
fter c
essa
tion
of IP
T in
the
med
ium
- bur
den
TB s
ettin
g of
Rio
de
Jan
eiro
in B
razi
l (20
12 p
reva
lenc
e of
TB
per
100
000
in B
razi
l: 59
(25–
107)
. Alth
ough
this
stu
dy re
porte
d an
initi
al in
crea
se in
TB
risk
imm
edia
tely
afte
r ces
satio
n of
IPT,
ther
e w
as
no in
crea
se o
ver t
he s
even
-yea
r fol
low
-up
perio
d (G
olub
et a
l. 20
14).
In m
oder
ate
TB in
cide
nce
setti
ngs,
six
mon
ths
of IP
T m
ay b
e ro
bust
and
suf
ficie
nt to
pre
vent
TB
in H
IV-in
fect
ed
indi
vidu
als.
Mo
nito
ring
and
eva
luat
ion
cons
ider
atio
nsTo
eva
luat
e w
heth
er th
e re
vise
d m
onito
ring
and
eval
uatio
n re
com
men
datio
n fo
r IP
T in
peo
ple
livin
g w
ith H
IV is
app
licab
le to
the
36 m
onth
s of
IPT.
Res
earc
h p
rio
ritie
sE
ligib
ility
crit
eria
• A
new
poi
nt-o
f-car
e te
st to
iden
tify
thos
e w
ith a
ctiv
e TB
, lat
ent T
B in
fect
ion
and
thos
e no
t inf
ecte
d w
ith M
. tub
ercu
losi
s, w
ith a
par
ticul
ar e
mph
asis
on
new
dia
gnos
tics
for c
hild
ren.
• Th
e ro
le o
f IG
RA
in p
eopl
e liv
ing
with
HIV
who
are
infe
cted
with
M. t
uber
culo
sis
with
or w
ithou
t act
ive
TB, w
ith in
form
atio
n ab
out t
he a
ssoc
iatio
n be
twee
n pe
rform
ance
of I
GR
A a
nd
imm
une
stat
us.
• Th
e us
e of
TS
T in
peo
ple
livin
g w
ith H
IV a
nd re
ceiv
ing
AR
T, w
ith a
par
ticul
ar e
mph
asis
on
the
frequ
ency
of p
erfo
rmin
g TS
T to
det
erm
ine
imm
une
reco
nstit
utio
n an
d/or
boo
stin
g in
th
ose
who
wer
e in
itial
ly T
ST
nega
tive.
Pre
vent
ive
trea
tmen
t for
TB
• E
valu
ate
bene
fits
and
harm
s of
rifa
myc
in-c
onta
inin
g re
gim
ens
for T
B p
reve
ntiv
e th
erap
y in
peo
ple
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
set
tings
with
hig
h H
IV a
nd T
B
prev
alen
ce.
• C
o-fo
rmul
ate
a fix
ed-d
ose
com
bina
tion
of is
onia
zid
and
vita
min
B6
with
co-
trim
oxaz
ole
alon
g w
ith a
ntire
trovi
rals
, and
eva
luat
e th
e ef
ficac
y an
d ef
fect
iven
ess
of s
uch
fixed
-dos
e co
mbi
natio
ns.
• E
valu
ate
the
effic
acy
and
feas
ibili
ty o
f lon
g-te
rm IP
T in
HIV
-pos
itive
chi
ldre
n.•
Stu
dy th
e ef
ficac
y an
d ad
vers
e ev
ents
of l
ong-
term
IPT
in p
eopl
e w
ith H
IV a
nd h
epat
itis
C v
irus
(HC
V) c
o-in
fect
ion.
• D
eter
min
e op
timal
tim
ing
for i
nitia
tion
of lo
ng-te
rm IP
T in
rela
tion
to in
itiat
ion
of A
RT.
• D
eter
min
e if
ther
e is
val
ue in
dis
cont
inui
ng li
felo
ng IP
T af
ter i
mm
une
reco
nstit
utio
n.•
Und
erta
ke m
odel
ling
stud
ies
to e
stim
ate
the
risks
and
ben
efits
of l
ong-
term
IPT
– ke
y co
nsid
erat
ions
sho
uld
incl
ude
the
inci
denc
e an
d pr
eval
ence
of H
IV a
nd T
B, r
isk
for T
B
by im
mun
e st
atus
, im
pact
of A
RT
on p
reve
ntio
n of
bot
h H
IV a
nd T
B, a
dded
ben
efit o
f lon
g-te
rm IP
T, o
ptim
um d
urat
ion
of IP
T, p
reva
lenc
e of
ison
iazi
d an
d rif
ampi
cin
resi
stan
ce,
imm
une
stat
us a
nd T
ST
stat
us.
Op
erat
iona
l res
earc
h
• S
tudy
pot
entia
l lim
itatio
ns o
f lon
g-te
rm IP
T in
pop
ulat
ions
with
a h
igh
prev
alen
ce o
f iso
niaz
id-r
esis
tant
TB
.•
Det
erm
ine
the
risks
and
ben
efits
of a
dmin
iste
ring
ison
iazi
d (in
err
or) t
o un
diag
nose
d pe
ople
with
act
ive
TB.
• A
scer
tain
the
effe
ctiv
enes
s of
long
-term
IPT
prog
ram
mes
in re
sour
ce-li
mite
d se
tting
s; c
ost–
effe
ctiv
enes
s an
d co
st–b
enefi
t fro
m th
e pe
rspe
ctiv
e of
hea
lth s
yste
ms
and
patie
nts.
• D
eter
min
e th
e us
e of
long
-term
IPT
for s
peci
al p
opul
atio
ns: b
enefi
ts/d
urat
ion
for h
ealth
-car
e w
orke
rs li
ving
with
HIV
; fre
quen
cy o
f scr
eeni
ng; b
enefi
ts fo
r TS
T-ne
gativ
e he
alth
-car
e w
orke
rs; H
IV-e
xpos
ed c
hild
ren.
• D
eter
min
e op
erat
iona
lizat
ion
of s
hort-
term
and
life
long
IPT
with
a p
artic
ular
focu
s on
mon
itorin
g pr
ogra
mm
es a
nd in
divi
dual
s (i.
e. c
linic
al s
tatu
s an
d ad
here
nce)
.•
Und
erta
ke p
opul
atio
n-ba
sed
drug
-res
ista
nce
surv
eilla
nce
to d
eter
min
e th
e im
pact
of l
ong-
term
IPT
prog
ram
mes
on
drug
-res
ista
nt T
B in
the
com
mun
ity, i
nclu
ding
incr
ease
s or
de
crea
ses
in m
ono-
ison
iazi
d an
d m
ono-
rifam
pici
n re
sist
ance
, and
mul
tidru
g-re
sist
ant T
B.
• E
valu
ate
the
best
nat
iona
l pro
gram
mes
or s
ervi
ces
to le
ad th
e im
plem
enta
tion
of lo
ng-te
rm IP
T (e
.g. H
IV, m
ater
nal a
nd c
hild
hea
lth (M
CH
), TB
, all
prog
ram
mes
).•
Ens
ure
optim
al d
eliv
ery
of lo
ng-te
rm IP
T an
d ot
her H
IV c
are
for s
peci
al g
roup
s in
clud
ing
wom
en a
nd c
hild
ren.

18
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Evi
den
ce p
rofil
e
Am
ong
thos
e w
ith c
onfir
med
, pro
babl
e or
pos
sibl
e TB
dis
ease
, pre
vent
ive
chem
othe
rapy
redu
ces
the
over
all r
isk
of d
evel
opin
g TB
by
38%
(RR
0.6
2; C
I: 0.
42–0
.89)
. For
thos
e w
ho w
ere
TST
posi
tive,
the
redu
ctio
n in
con
firm
ed, p
roba
ble
or p
ossi
ble
TB in
crea
sed
to 4
9% (R
R 0
.51;
95%
CI:
0.3–
0.86
). A
lthou
gh n
ot s
tatis
tical
ly s
igni
fican
t, th
e re
duct
ion
amon
g TS
T-ne
gativ
e pe
rson
s w
as 2
7% (R
R 0
.73;
95%
C
I: 0.
43–1
.26)
.
Aut
hor(
s): S
aski
a de
n B
oon
Dat
e: 2
014-
04-2
8Q
uest
ion:
Sho
uld
cont
inuo
us IP
T ve
rsus
six
-mon
th IP
T be
use
d fo
r TB
pre
vent
ion
in p
eopl
e liv
ing
with
HIV
, irr
espe
ctiv
e of
TS
T?S
ettin
gs:
Sou
th A
frica
, Bot
swan
a, In
dia
Bib
liog
rap
hy: M
artin
son
et a
l. 20
11, S
aman
dari
et a
l. 20
11, S
wam
inat
han
et a
l. 20
12
Qua
lity
asse
ssm
ent
No
of p
atie
nts
Effe
ct
Qua
lity
Imp
orta
nce
No
of
stud
ies
Des
ign
Ris
k of
bia
sIn
cons
iste
ncy
Ind
irect
ness
Imp
reci
sion
Oth
er
cons
ider
atio
nsC
ontin
uous
IP
TS
ix-m
onth
IP
TR
elat
ive
(95%
CI)
Ab
solu
te
Act
ive
TB (
confi
rmed
, pro
bab
le, p
ossi
ble
), (
follo
w-u
p 3
0–47
mon
ths;
1 as
sess
ed w
ith c
ultu
re, s
mea
r, si
gns
and
sym
pto
ms
of T
B +
res
pon
se to
trea
tmen
t)
3R
ando
miz
ed
trial
sse
rious
2no
ser
ious
in
cons
iste
ncy
serio
us3,
4,5
no s
erio
us
impr
ecis
ion
none
41/1
509
(2.7
%)
78/1
659
(4.7
%)
RR
0.6
2 (0
.42
to
0.89
)
18 fe
wer
per
100
0 (fr
om
5 fe
wer
to 2
7 fe
wer
)LO
W
CR
ITIC
AL
2%8
few
er p
er 1
000
(from
2
few
er to
12
few
er)
50%
190
few
er p
er 1
000
(from
55
few
er to
290
few
er)
Con
firm
ed T
B (
follo
w-u
p 3
0–47
mon
ths;
ass
esse
d w
ith c
ultu
re p
ositi
ve fo
r M
.tub
ercu
losi
s
2R
ando
miz
ed
trial
sse
rious
6no
ser
ious
in
cons
iste
ncy
serio
us3,
5no
ser
ious
im
prec
isio
nno
ne10
/503
(2
%)
28/6
71
(4.2
%)
OR
0.5
2 (0
.25
to
1.09
)
20 fe
wer
per
100
0 (fr
om
31 fe
wer
to 4
mor
e)LO
W
CR
ITIC
AL
2%9
few
er p
er 1
000
(from
15
few
er to
2 m
ore)
50%
158
few
er p
er 1
000
(from
30
0 fe
wer
to 2
2 m
ore)
Dea
th (
follo
w-u
p 3
0–47
mon
ths;
ass
esse
d w
ith c
linic
al o
r ve
rbal
aut
opsy
, hos
pita
l rec
ord
s, o
r d
eath
cer
tifica
tes)
3R
ando
miz
ed
trial
sse
rious
6no
ser
ious
in
cons
iste
ncy
serio
us3,
4,5
no s
erio
us
impr
ecis
ion
none
67/1
509
(4.4
%)
88/1
660
(5.3
%)
RR
0.8
7(0
.63
to
1.19
)
7 fe
wer
per
100
0 (fr
om
20 fe
wer
to 1
0 m
ore)
LOW
CR
ITIC
AL
2%3
few
er p
er 1
000
(from
7
few
er to
4 m
ore)
50%
65 fe
wer
per
100
0 (fr
om
185
few
er to
95
mor
e)
Dea
th d
ue to
TB
(fo
llow
-up
med
ian
30–3
6 m
onth
s; a
sses
sed
with
clin
ical
or
verb
al a
utop
sy o
r ho
spita
l rec
ord
s)
2R
ando
miz
ed
trial
sse
rious
7no
ser
ious
in
cons
iste
ncy
serio
us3
no s
erio
us
impr
ecis
ion
none
4/13
45
(0.3
%)
8/13
33
(0.6
%)
OR
0.5
2 (0
.17
to
1.64
)
3 fe
wer
per
100
0 (fr
om 5
fe
wer
to 4
mor
e)LO
W
CR
ITIC
AL
0.1%
0 fe
wer
per
100
0 (fr
om 1
fe
wer
to 1
mor
e)
15%
66 fe
wer
per
100
0 (fr
om
121
few
er to
74
mor
e)

1918
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Qua
lity
asse
ssm
ent
No
of p
atie
nts
Effe
ct
Qua
lity
Imp
orta
nce
No
of
stud
ies
Des
ign
Ris
k of
bia
sIn
cons
iste
ncy
Ind
irect
ness
Imp
reci
sion
Oth
er
cons
ider
atio
nsC
ontin
uous
IP
TS
ix-m
onth
IP
TR
elat
ive
(95%
CI)
Ab
solu
te
Tub
ercu
losi
s or
dea
th (
follo
w-u
p 3
0–47
mon
ths;
ass
esse
d w
ith a
ll TB
(co
nfirm
ed, p
rob
able
, pos
sib
le)
3R
ando
miz
ed
trial
sse
rious
2no
ser
ious
in
cons
iste
ncy
serio
us3,4
,5no
ser
ious
im
prec
isio
nno
ne10
7/15
09
(7.1
%)
160/
1660
(9
.6%
)R
R 0
.76
(0.6
to
0.96
)
23 fe
wer
per
100
0 (fr
om
4 fe
wer
to 3
9 fe
wer
)LO
W
CR
ITIC
AL
2%5
few
er p
er 1
000
(from
1
few
er to
8 fe
wer
)
50%
120
few
er p
er 1
000
(from
20
few
er to
200
few
er)
Ad
vers
e ev
ents
– n
ot r
epor
ted
0–
––
––
none
––
––
CR
ITIC
AL
Ad
here
nce
– no
t rep
orte
d
0–
––
––
none
––
––
IMP
OR
TAN
T
1 Med
ian
follo
w-u
p pe
riod
varie
d fro
m 2
.5 y
ears
(30
mon
ths)
in th
e 36
mon
ths
ison
iazi
d ar
m a
nd 2
.6 y
ears
in th
e 6
mon
ths
ison
iazi
d pl
us e
tham
buto
l arm
in th
e S
wam
inat
han
et a
l. 20
12 s
tudy
, and
3.9
yea
rs (4
7 m
onth
s) fo
r bot
h th
e co
ntin
uous
and
six
-mon
th is
onia
zid
grou
ps in
the
Mar
tinso
n et
al.
2011
stu
dy. M
edia
n fo
llow
-up
was
not
repo
rted
for t
he S
aman
dari
et a
l. 20
11 s
tudy
but
is p
roba
bly
clos
e to
36
mon
ths.
2 S
wam
inat
han
et a
l. 20
12 a
nd M
artin
son
et a
l. 20
11 s
tudi
es w
ere
not b
linde
d, a
nd th
e al
loca
tion
conc
ealm
ent i
n th
e S
aman
dari
et a
l. 20
11 s
tudy
was
not
cle
arly
des
crib
ed a
nd m
ight
hav
e le
d to
sel
ectio
n bi
as.
3 The
con
trol g
roup
in th
e S
wam
inat
han
et a
l. 20
12 s
tudy
rece
ived
300
g is
onia
zid
+ 8
00 g
eth
ambu
tol.
4 Diff
eren
ces
in in
clud
ed p
atie
nt p
opul
atio
n: M
artin
son
et a
l. 20
11 e
xclu
ded
patie
nts
elig
ible
for A
RT;
med
ian
CD
4 co
unt a
t bas
elin
e w
as 4
84 c
ells
/mm
3. In
Sam
anda
ri et
al.
2011
stu
dy 2
% w
ere
on A
RT
befo
re
enro
lmen
t and
47%
wer
e on
AR
T by
mon
th 3
6. M
edia
n C
D4
coun
t at b
asel
ine
was
297
cel
ls/m
m3.
Sw
amin
atha
n et
al.
2012
stu
dy in
clud
ed A
RT-
naïv
e pa
tient
s w
ith a
med
ian
CD
4 co
unt o
f 325
cel
ls/m
m3.
5 Mar
tinso
n et
al.
2011
stu
dy in
clud
ed o
nly
patie
nts
with
pos
itive
TS
T (>
5 m
m).
6 Mar
tinso
n et
al.
2011
and
Sw
amin
atha
n et
al.
2012
stu
dies
wer
e no
t blin
ded.
7 Sw
amin
atha
n et
al.
2012
stu
dy w
as n
ot b
linde
d, a
nd th
e al
loca
tion
conc
ealm
ent i
n th
e S
aman
dari
et a
l. 20
11 s
tudy
was
not
cle
arly
des
crib
ed a
nd m
ight
hav
e le
d to
sel
ectio
n bi
as.
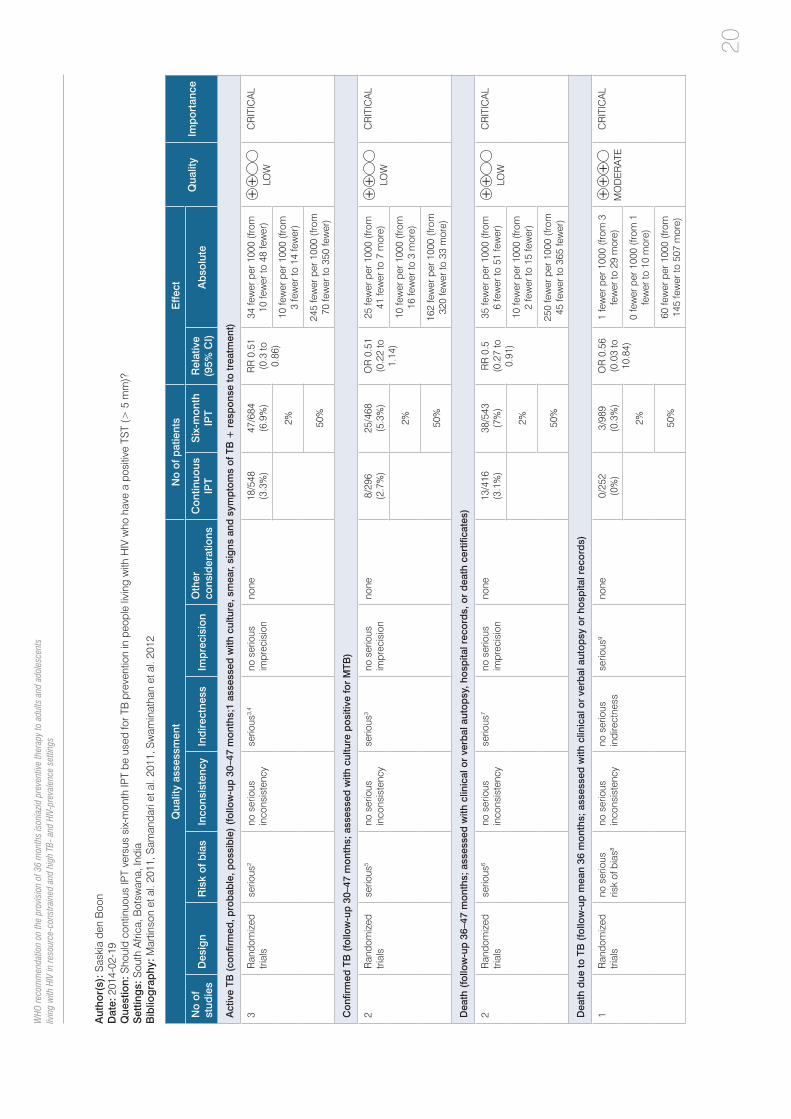
20
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Aut
hor(
s): S
aski
a de
n B
oon
Dat
e: 2
014-
02-1
9Q
uest
ion:
Sho
uld
cont
inuo
us IP
T ve
rsus
six
-mon
th IP
T be
use
d fo
r TB
pre
vent
ion
in p
eopl
e liv
ing
with
HIV
who
hav
e a
posi
tive
TST
(> 5
mm
)?S
ettin
gs:
Sou
th A
frica
, Bot
swan
a, In
dia
Bib
liog
rap
hy: M
artin
son
et a
l. 20
11, S
aman
dari
et a
l. 20
11, S
wam
inat
han
et a
l. 20
12
Qua
lity
asse
ssm
ent
No
of p
atie
nts
Effe
ct
Qua
lity
Imp
orta
nce
No
of
stud
ies
Des
ign
Ris
k of
bia
sIn
cons
iste
ncy
Ind
irect
ness
Imp
reci
sion
Oth
er
cons
ider
atio
nsC
ontin
uous
IP
TS
ix-m
onth
IP
TR
elat
ive
(95%
CI)
Ab
solu
te
Act
ive
TB (
confi
rmed
, pro
bab
le, p
ossi
ble
) (f
ollo
w-u
p 3
0–47
mon
ths;
1 as
sess
ed w
ith c
ultu
re, s
mea
r, si
gns
and
sym
pto
ms
of T
B +
res
pon
se to
trea
tmen
t)
3R
ando
miz
ed
trial
sse
rious
2no
ser
ious
in
cons
iste
ncy
serio
us3,
4no
ser
ious
im
prec
isio
nno
ne18
/548
(3
.3%
)47
/684
(6
.9%
)R
R 0
.51
(0.3
to
0.86
)
34 fe
wer
per
100
0 (fr
om
10 fe
wer
to 4
8 fe
wer
)LO
W
CR
ITIC
AL
2%10
few
er p
er 1
000
(from
3
few
er to
14
few
er)
50%
245
few
er p
er 1
000
(from
70
few
er to
350
few
er)
Con
firm
ed T
B (
follo
w-u
p 3
0–47
mon
ths;
ass
esse
d w
ith c
ultu
re p
ositi
ve fo
r M
TB)
2R
ando
miz
ed
trial
sse
rious
5no
ser
ious
in
cons
iste
ncy
serio
us3
no s
erio
us
impr
ecis
ion
none
8/29
6 (2
.7%
)25
/468
(5
.3%
)O
R 0
.51
(0.2
2 to
1.
14)
25 fe
wer
per
100
0 (fr
om
41 fe
wer
to 7
mor
e)LO
W
CR
ITIC
AL
2%10
few
er p
er 1
000
(from
16
few
er to
3 m
ore)
50%
162
few
er p
er 1
000
(from
32
0 fe
wer
to 3
3 m
ore)
Dea
th (
follo
w-u
p 3
6–47
mon
ths;
ass
esse
d w
ith c
linic
al o
r ve
rbal
aut
opsy
, hos
pita
l rec
ord
s, o
r d
eath
cer
tifica
tes)
2R
ando
miz
ed
trial
sse
rious
6no
ser
ious
in
cons
iste
ncy
serio
us7
no s
erio
us
impr
ecis
ion
none
13/4
16
(3.1
%)
38/5
43
(7%
)R
R 0
.5
(0.2
7 to
0.
91)
35 fe
wer
per
100
0 (fr
om
6 fe
wer
to 5
1 fe
wer
)LO
W
CR
ITIC
AL
2%10
few
er p
er 1
000
(from
2
few
er to
15
few
er)
50%
250
few
er p
er 1
000
(from
45
few
er to
365
few
er)
Dea
th d
ue to
TB
(fo
llow
-up
mea
n 36
mon
ths;
ass
esse
d w
ith c
linic
al o
r ve
rbal
aut
opsy
or
hosp
ital r
ecor
ds)
1R
ando
miz
ed
trial
sno
ser
ious
ris
k of
bia
s8no
ser
ious
in
cons
iste
ncy
no s
erio
us
indi
rect
ness
serio
us9
none
0/25
2 (0
%)
3/98
9 (0
.3%
)O
R 0
.56
(0.0
3 to
10
.84)
1 fe
wer
per
100
0 (fr
om 3
fe
wer
to 2
9 m
ore)
MO
DE
RAT
E
CR
ITIC
AL
2%0
few
er p
er 1
000
(from
1
few
er to
10
mor
e)
50%
60 fe
wer
per
100
0 (fr
om
145
few
er to
507
mor
e)
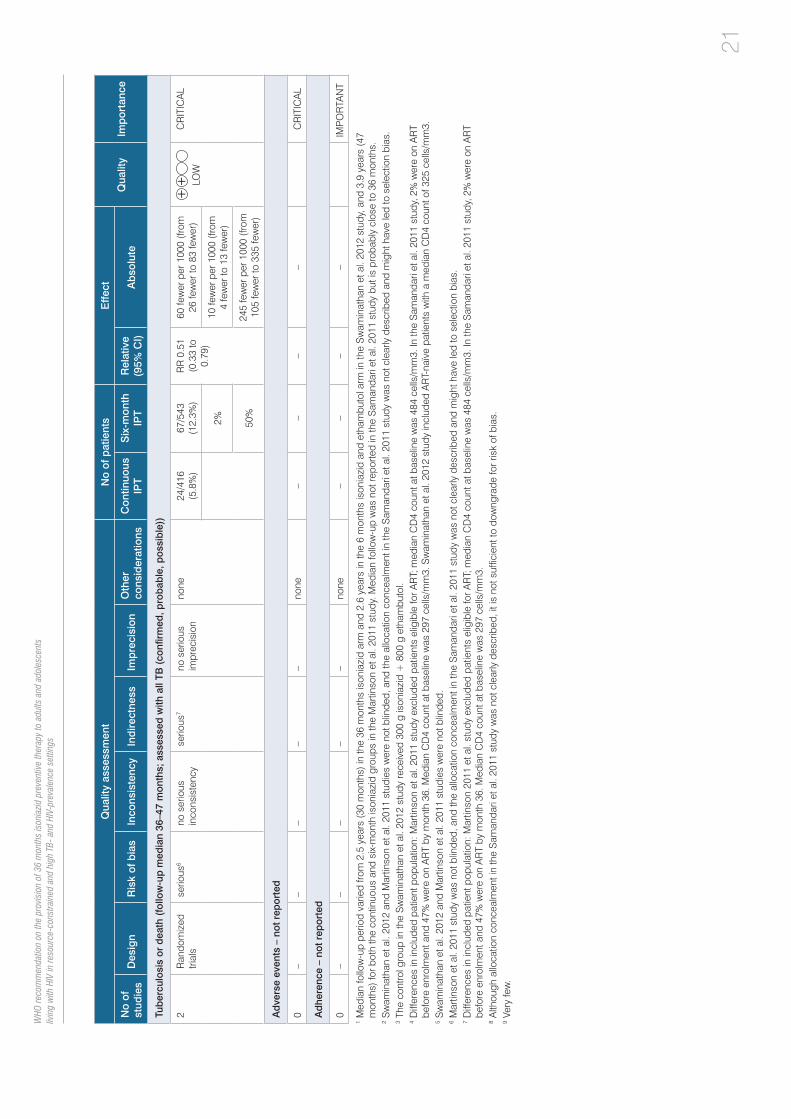
2120
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Qua
lity
asse
ssm
ent
No
of p
atie
nts
Effe
ct
Qua
lity
Imp
orta
nce
No
of
stud
ies
Des
ign
Ris
k of
bia
sIn
cons
iste
ncy
Ind
irect
ness
Imp
reci
sion
Oth
er
cons
ider
atio
nsC
ontin
uous
IP
TS
ix-m
onth
IP
TR
elat
ive
(95%
CI)
Ab
solu
te
Tub
ercu
losi
s or
dea
th (
follo
w-u
p m
edia
n 36
–47
mon
ths;
ass
esse
d w
ith a
ll TB
(co
nfirm
ed, p
rob
able
, pos
sib
le))
2R
ando
miz
ed
trial
sse
rious
6no
ser
ious
in
cons
iste
ncy
serio
us7
no s
erio
us
impr
ecis
ion
none
24/4
16
(5.8
%)
67/5
43
(12.
3%)
RR
0.5
1 (0
.33
to
0.79
)
60 fe
wer
per
100
0 (fr
om
26 fe
wer
to 8
3 fe
wer
)LO
W
CR
ITIC
AL
2%10
few
er p
er 1
000
(from
4
few
er to
13
few
er)
50%
245
few
er p
er 1
000
(from
10
5 fe
wer
to 3
35 fe
wer
)
Ad
vers
e ev
ents
– n
ot r
epor
ted
0–
––
––
none
––
––
CR
ITIC
AL
Ad
here
nce
– no
t rep
orte
d
0–
––
––
none
––
––
IMP
OR
TAN
T
1 Med
ian
follo
w-u
p pe
riod
varie
d fro
m 2
.5 y
ears
(30
mon
ths)
in th
e 36
mon
ths
ison
iazi
d ar
m a
nd 2
.6 y
ears
in th
e 6
mon
ths
ison
iazi
d an
d et
ham
buto
l arm
in th
e S
wam
inat
han
et a
l. 20
12 s
tudy
, and
3.9
yea
rs (4
7 m
onth
s) fo
r bot
h th
e co
ntin
uous
and
six
-mon
th is
onia
zid
grou
ps in
the
Mar
tinso
n et
al.
2011
stu
dy. M
edia
n fo
llow
-up
was
not
repo
rted
in th
e S
aman
dari
et a
l. 20
11 s
tudy
but
is p
roba
bly
clos
e to
36
mon
ths.
2 S
wam
inat
han
et a
l. 20
12 a
nd M
artin
son
et a
l. 20
11 s
tudi
es w
ere
not b
linde
d, a
nd th
e al
loca
tion
conc
ealm
ent i
n th
e S
aman
dari
et a
l. 20
11 s
tudy
was
not
cle
arly
des
crib
ed a
nd m
ight
hav
e le
d to
sel
ectio
n bi
as.
3 The
con
trol g
roup
in th
e S
wam
inat
han
et a
l. 20
12 s
tudy
rece
ived
300
g is
onia
zid
+ 8
00 g
eth
ambu
tol.
4 Diff
eren
ces
in in
clud
ed p
atie
nt p
opul
atio
n: M
artin
son
et a
l. 20
11 s
tudy
exc
lude
d pa
tient
s el
igib
le fo
r AR
T; m
edia
n C
D4
coun
t at b
asel
ine
was
484
cel
ls/m
m3.
In th
e S
aman
dari
et a
l. 20
11 s
tudy
, 2%
wer
e on
AR
T be
fore
enr
olm
ent a
nd 4
7% w
ere
on A
RT
by m
onth
36.
Med
ian
CD
4 co
unt a
t bas
elin
e w
as 2
97 c
ells
/mm
3. S
wam
inat
han
et a
l. 20
12 s
tudy
incl
uded
AR
T-na
ïve
patie
nts
with
a m
edia
n C
D4
coun
t of 3
25 c
ells
/mm
3.5 S
wam
inat
han
et a
l. 20
12 a
nd M
artin
son
et a
l. 20
11 s
tudi
es w
ere
not b
linde
d.6 M
artin
son
et a
l. 20
11 s
tudy
was
not
blin
ded,
and
the
allo
catio
n co
ncea
lmen
t in
the
Sam
anda
ri et
al.
2011
stu
dy w
as n
ot c
lear
ly d
escr
ibed
and
mig
ht h
ave
led
to s
elec
tion
bias
.7 D
iffer
ence
s in
incl
uded
pat
ient
pop
ulat
ion:
Mar
tinso
n 20
11 e
t al.
stud
y ex
clud
ed p
atie
nts
elig
ible
for A
RT;
med
ian
CD
4 co
unt a
t bas
elin
e w
as 4
84 c
ells
/mm
3. In
the
Sam
anda
ri et
al.
2011
stu
dy, 2
% w
ere
on A
RT
befo
re e
nrol
men
t and
47%
wer
e on
AR
T by
mon
th 3
6. M
edia
n C
D4
coun
t at b
asel
ine
was
297
cel
ls/m
m3.
8 A
lthou
gh a
lloca
tion
conc
ealm
ent i
n th
e S
aman
dari
et a
l. 20
11 s
tudy
was
not
cle
arly
des
crib
ed, i
t is
not s
uffic
ient
to d
owng
rade
for r
isk
of b
ias.
9 V
ery
few
.

22
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Aut
hor(
s): S
aski
a de
n B
oon
Dat
e: 2
014-
03-2
7Q
uest
ion:
Sho
uld
cont
inuo
us is
onia
zid
vers
us s
ix-m
onth
ison
iazi
d be
use
d fo
r tub
ercu
losi
s pr
even
tion
in p
eopl
e liv
ing
with
HIV
and
with
a n
egat
ive
TST
(< 5
mm
)?S
ettin
gs:
Sou
th A
frica
, Bot
swan
a, In
dia
Bib
liog
rap
hy: M
artin
son
et a
l. 20
11, S
aman
dari
et a
l. 20
11, S
wam
inat
han
et a
l. 20
12
Qua
lity
asse
ssm
ent
No
of p
atie
nts
Effe
ct
Qua
lity
Imp
orta
nce
No
of
stud
ies
Des
ign
Ris
k of
bia
sIn
cons
iste
ncy
Ind
irect
ness
Imp
reci
sion
Oth
er
cons
ider
atio
nsC
ontin
uous
IP
TS
ix-m
onth
IP
TR
elat
ive
(95%
CI)
Ab
solu
te
Act
ive
TB (
confi
rmed
, pro
bab
le, p
ossi
ble
) (f
ollo
w-u
p 3
0–36
mon
ths;
ass
esse
d w
ith c
ultu
re, s
mea
r, si
gns
and
sym
pto
ms
of T
B +
res
pon
se to
trea
tmen
t)
2R
ando
miz
ed
trial
sse
rious
1no
ser
ious
in
cons
iste
ncy
serio
us2
no s
erio
us
impr
ecis
ion
none
22/9
29
(2.4
%)
30/9
32
(3.2
%)
RR
0.7
3 (0
.43
to
1.26
)
9 fe
wer
per
100
0 (fr
om
18 fe
wer
to 8
mor
e)LO
W
CR
ITIC
AL
2%5
few
er p
er 1
000
(from
11
few
er to
5 m
ore)
50%
135
few
er p
er 1
000
(from
28
5 fe
wer
to 1
30 m
ore)
Con
firm
ed T
B (
follo
w-u
p m
edia
n 30
mon
ths;
ass
esse
d w
ith c
ultu
re p
ositi
ve fo
r M
TB)
1R
ando
miz
ed
trial
sse
rious
3no
ser
ious
in
cons
iste
ncy
serio
us2
no s
erio
us
impr
ecis
ion
none
2/20
7 (0
.97%
)3/
203
(1.5
%)
OR
0.6
5 (0
.11
to
3.93
)
5 fe
wer
per
100
0 (fr
om
13 fe
wer
to 4
1 m
ore)
LOW
CR
ITIC
AL
2%7
few
er p
er 1
000
(from
18
few
er to
54
mor
e)
50%
106
few
er p
er 1
000
(from
40
1 fe
wer
to 2
97 m
ore)
Dea
th (
follo
w-u
p m
ean
36 m
onth
s; a
sses
sed
with
clin
ical
or
verb
al a
utop
sy, h
osp
ital r
ecor
ds,
or
dea
th c
ertifi
cate
s)
1R
ando
miz
ed
trial
sno
ser
ious
ris
k of
bia
s4no
ser
ious
in
cons
iste
ncy
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
32/7
22
(4.4
%)
25/7
29
(3.4
%)
RR
1.2
9 (0
.77
to
2.16
)
10 m
ore
per 1
000
(from
8
few
er to
40
mor
e)H
IGH
CR
ITIC
AL
2%6
mor
e pe
r 100
0 (fr
om 5
fe
wer
to 2
3 m
ore)
50%
145
mor
e pe
r 100
0 (fr
om
115
few
er to
580
mor
e)
Dea
th d
ue to
TB
(fo
llow
-up
mea
n 36
mon
ths;
ass
esse
d w
ith c
linic
al o
r ve
rbal
aut
opsy
or
hosp
ital r
ecor
ds)
1R
ando
miz
ed
trial
sno
ser
ious
ris
k of
bia
s4no
ser
ious
in
cons
iste
ncy
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
4/72
2 (0
.55%
)3/
729
(0.4
1%)
OR
1.3
5 (0
.3 to
6.
05)
1 m
ore
per 1
000
(from
3
few
er to
20
mor
e)H
IGH
CR
ITIC
AL
2%0
mor
e pe
r 100
0 (fr
om 1
fe
wer
to 5
mor
e)
50%
42 m
ore
per 1
000
(from
10
0 fe
wer
to 3
66 m
ore)
Tub
ercu
losi
s or
dea
th (
follo
w-u
p m
edia
n 36
mon
ths;
ass
esse
d w
ith a
ll TB
(co
nfirm
ed, p
rob
able
, pos
sib
le)

2322
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Qua
lity
asse
ssm
ent
No
of p
atie
nts
Effe
ct
Qua
lity
Imp
orta
nce
No
of
stud
ies
Des
ign
Ris
k of
bia
sIn
cons
iste
ncy
Ind
irect
ness
Imp
reci
sion
Oth
er
cons
ider
atio
nsC
ontin
uous
IP
TS
ix-m
onth
IP
TR
elat
ive
(95%
CI)
Ab
solu
te
1R
ando
miz
ed
trial
sno
ser
ious
ris
k of
bia
s4no
ser
ious
in
cons
iste
ncy
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
47/7
22
(6.5
%)
45/7
29
(6.2
%)
RR
1.0
5 (0
.71
to
1.57
)
3 m
ore
per 1
000
(from
18
few
er to
35
mor
e)H
IGH
CR
ITIC
AL
2%1
mor
e pe
r 100
0 (fr
om 6
fe
wer
to 1
1 m
ore)
50%
25 m
ore
per 1
000
(from
14
5 fe
wer
to 2
85 m
ore)
Ad
vers
e ev
ents
– n
ot r
epor
ted
0–
––
––
none
––
––
CR
ITIC
AL
Ad
here
nce
0N
o ev
iden
ce
avai
labl
e–
––
–no
ne–
––
–IM
PO
RTA
NT
1 Sw
amin
atha
n et
al.
2012
stu
dy w
as n
ot b
linde
d, th
e al
loca
tion
conc
ealm
ent i
n th
e S
aman
dari
et a
l. 20
11 s
tudy
was
not
cle
arly
des
crib
ed a
nd m
ight
hav
e le
d to
sel
ectio
n bi
as.
2 The
con
trol g
roup
in th
e S
wam
inat
han
et a
l. 20
12 s
tudy
rece
ived
300
g is
onia
zid
+ 8
00 g
eth
ambu
tol.
3 Sw
amin
atha
n et
al.
2011
stu
dy w
as n
ot b
linde
d.4 A
lthou
gh a
lloca
tion
conc
ealm
ent i
n th
e S
aman
dari
et a
l. 20
11 s
tudy
was
not
cle
arly
des
crib
ed, i
t is
not s
uffic
ient
to d
owng
rade
for r
isk
of b
ias.
Ref
eren
ces
• A
kolo
C,
Ade
tifa
I, S
hepp
erd
S,
Volm
ink
J. T
reat
men
t of
late
nt t
uber
culo
sis
infe
ctio
n in
HIV
infe
cted
per
sons
. C
ochr
ane
Dat
abas
e S
yst
Rev
. 20
10 J
an
20;(
1):C
D00
0171
.
• G
olub
JE
, Coh
n S
, Sar
acen
i V, C
aval
cant
e S
C, P
ache
co A
G, M
oulto
n LH
, et a
l. Lo
ng-te
rm p
rote
ctio
n fro
m is
onia
zid
prev
entiv
e th
erap
y fo
r tub
ercu
losi
s in
H
IV-in
fect
ed p
atie
nts
in a
med
ium
-bur
den
tube
rcul
osis
set
ting:
the
TB/H
IV in
Rio
(TH
Rio
) tud
y. C
lin In
fect
Dis
. 201
5 Fe
b 15
;60(
4):6
39–4
5.
• G
upta
S, A
bim
bola
T, D
ate
A, S
utha
r AB
, Ben
nett
R, S
angr
ujee
N, e
t al.
Cos
t-effe
ctiv
enes
s of
the
Thre
e I’s
for H
IV/T
B a
nd A
RT
to p
reve
nt T
B a
mon
g pe
ople
liv
ing
with
HIV
. Int
. J T
uber
c Lu
ng D
is. 2
014
Oct
;18(
10):
1159
–65.
• K
ireng
a B
J, W
orod
ria W
, Mas
sing
a-Lo
embe
M, N
alw
oga
T, M
anab
e YC
, Kes
tens
L, e
t al.
Tube
rcul
in s
kin
test
con
vers
ion
amon
g H
IV p
atie
nts
on a
ntire
trovi
ral
ther
apy
in U
gand
a. In
t J T
uber
c Lu
ng D
is. 2
013;
17(3
):33
6-41
.
• M
artin
son
NA
, Bar
nes
GL,
Mou
lton
LH, M
sand
iwa
R, H
ausl
er H
, Ram
M, e
t al.
New
regi
men
s to
pre
vent
tube
rcul
osis
in a
dults
with
HIV
infe
ctio
n. N
ew E
ng
J M
ed. 2
011
Jul 7
;365
(1):
11-2
0.
• P
ho M
T, S
wam
inat
han
S, K
umar
asw
amy
N, L
osin
a E
, Pon
nura
ja C
, Uhl
er L
, et a
l. Th
e co
st-e
ffect
iven
ess
of tu
berc
ulos
is p
reve
ntiv
e th
erap
y fo
r HIV
-infe
cted
in
divi
dual
s in
sou
ther
n In
dia:
a tr
ial-b
ased
ana
lysi
s. P
LoS
One
. 201
2;7(
4):e
3600
1.
• R
anga
ka M
X, W
ilkin
son
RJ,
Bou
lle A
, Gly
nn J
R, F
ield
ing
K, v
an C
utse
m G
, et a
l. Is
onia
zid
plus
ant
iretro
vira
l the
rapy
to p
reve
nt tu
berc
ulos
is: a
rand
omis
ed
doub
le-b
lind,
pla
cebo
-con
trolle
d tri
al. L
ance
t. 20
14;3
84:6
82–9
0.
• S
aman
dari
T, A
gize
w T
B, N
yire
nda
S, T
edla
Z, S
iban
da T
, Sha
ng N
, et a
l. 6-
mon
th v
ersu
s 36
-mon
th is
onia
zid
prev
entiv
e tre
atm
ent f
or tu
berc
ulos
is in
adu
lts
with
HIV
infe
ctio
n in
Bot
swan
a: a
rand
omis
ed, d
oubl
e-bl
ind,
pla
cebo
-con
trolle
d tri
al. L
ance
t. 20
11;3
77(9
777)
:158
8–98
.
• S
mith
T,
Sam
anda
ri T,
Abi
mbo
la T
, M
arst
on B
, S
angr
ujee
N.
Cos
t-effe
ctiv
enes
s of
alte
rnat
ive
polic
ies
to r
educ
e TB
dis
ease
and
dea
th in
HIV
-infe
cted
pe
rson
s in
Bot
swan
a. A
m J
Res
pir C
rit C
are
Med
. 201
1;18
3:A
5310
(abs
tract
).
• S
wam
inat
han
S, M
enon
PA
, Gop
alan
N, P
erum
al V
, San
than
akris
hnan
RK
, Ram
acha
ndra
n R
, et a
l. E
ffica
cy o
f a s
ix-m
onth
ver
sus
a 36
-mon
th re
gim
en fo
r pr
even
tion
of tu
berc
ulos
is in
HIV
-infe
cted
per
sons
in In
dia:
a ra
ndom
ized
clin
ical
tria
l. P
loS
One
. 201
2;7(
12):
e474
00.

24
WHO
reco
mm
enda
tion
on th
e pr
ovis
ion
of 3
6 m
onth
s is
onia
zid p
reve
ntiv
e th
erap
y to
adu
lts a
nd a
dole
scen
ts
livin
g w
ith H
IV in
reso
urce
-con
stra
ined
and
hig
h TB
- and
HIV
-pre
vale
nce
setti
ngs
Defi
nitio
ns fo
r ra
ting
s of
the
cert
aint
y of
the
evid
ence
(G
RA
DE
)**
Rat
ing
sD
efini
tions
Hig
hTh
is re
sear
ch p
rovi
des
a ve
ry g
ood
indi
catio
n of
the
likel
y ef
fect
. The
like
lihoo
d th
at th
e ef
fect
will
be
subs
tant
ially
diff
eren
t* is
low
.
Mod
erat
eTh
is re
sear
ch p
rovi
des
a go
od in
dica
tion
of th
e lik
ely
effe
ct. T
he li
kelih
ood
that
the
effe
ct w
ill b
e su
bsta
ntia
lly d
iffer
ent4
is m
oder
ate.
Low
This
rese
arch
pro
vide
s so
me
indi
catio
n of
the
likel
y ef
fect
. How
ever
, the
like
lihoo
d th
at it
will
be
subs
tant
ially
diff
eren
t4 is
hig
h.
Ver
y lo
wTh
is re
sear
ch d
oes
not p
rovi
de a
relia
ble
indi
catio
n of
the
likel
y ef
fect
. The
like
lihoo
d th
at th
e ef
fect
will
be
subs
tant
ially
diff
eren
t4 is
ver
y hi
gh.
*Sub
stan
tially
diff
eren
t: la
rge
enou
gh d
iffer
ence
that
it m
ight
hav
e an
effe
ct o
n a
deci
sion
**Th
e G
radi
ng o
f Rec
omm
enda
tions
Ass
essm
ent,
Dev
elop
men
t and
Eva
luat
ion
(GR
AD
E) W
orki
ng G
roup
beg
an in
the
year
200
0 as
an
info
rmal
col
labo
ratio
n of
peo
ple
with
an
inte
rest
in a
ddre
ssin
g th
e sh
ortc
omin
gs o
f pre
sent
gra
ding
sys
tem
s in
hea
lth c
are.
The
wor
king
gro
up h
as d
evel
oped
a c
omm
on, s
ensi
ble
and
trans
pare
nt a
ppro
ach
to g
radi
ng q
ualit
y of
evi
denc
e an
d st
reng
th o
f rec
omm
enda
tions
. Man
y in
tern
atio
nal o
rgan
izat
ions
hav
e pr
ovid
ed in
put i
nto
the
deve
lopm
ent o
f the
app
roac
h an
d ha
ve s
tarte
d us
ing
it.


9789241508872
For further information, please contact:
World Health Organization20, Avenue Appia CH-1211 Geneva 27 SwitzerlandGlobal TB ProgrammeE-mail: [email protected] site: www.who.int/tb
HIV/AIDS DepartmentEmail: [email protected] site: www.who.int/hiv