Real Cases from the Clinic with Lung Cancer …...reported safety profile of the individual agents;...
73
REAL PATIENTS FROM THE CLINIC WITH LUNG CANCER UPDATE. A MESSAGE OF HOPE MOHAMED K. MOHAMED, MD,PHD DIVISION DIRECTOR MEDICAL ONCOLOGY DIRECTOR OF THORACIC ONCOLOGY CONE HEALTH CANCER CENTER GREENSBORO, NC
Transcript of Real Cases from the Clinic with Lung Cancer …...reported safety profile of the individual agents;...

REAL PATIENTS FROM THE CLINIC WITH LUNG CANCER
UPDATE.A MESSAGE OF HOPE
MOHAMED K. MOHAMED, MD,PHD
DIVISION DIRECTOR MEDICAL ONCOLOGY
DIRECTOR OF THORACIC ONCOLOGY
CONE HEALTH CANCER CENTER
GREENSBORO, NC

SMALL CELL LUNG CANCER(SCLC)

68 YO FEMALE WITH SMALL CELL LUNG CANCER
• She has a long history of smoking presented with abdominal pain for several weeks
• CT abdomen showed liver lesions
• CT Chest followed by PET scan showed large mass in the right upper lobe of the lung, liver and T12 bone metastases.
• MRI brain was negative
• Bronchoscopy as well as T12 Bone biopsy confirms Small Cell Lung Cancer.

68 YO FEMALE WITH SMALL CELL LUNG CANCER

68 YO FEMALE WITH SMALL CELL LUNG CANCER
• She was treated with Vertebroplasty as palliative Radiation to the T12 lesion.
• She started systemic chemotherapy with Carboplatin, Etoposide and Atezolizumab for 6 cycles.
• She has significant improvement in her disease and quality of life.
• She is currently on Maintenance treatment with Atezolizumab every 3 weeks.

68 YO FEMALE WITH SMALL CELL LUNG CANCER
Before Treatment After Treatment

68 YO FEMALE WITH SMALL CELL LUNG CANCER
Before After

CHEMOTHERAPY AND SCLC
• Historic standard for ES-SCLC is chemotherapy
• Cisplatin + etoposide introduced in the 1970s
• SCLC initially highly responsive to therapy
• EP RR 61% (10% CR)
• Responses transient
• PFS 4.0 months
• OS 8.6 months
Roth, JCO 1992

N Engl J Med 2018;[Epub ahead of print]

IMPOWER133: A PHASE III TRIAL EVALUATING ATEZOLIZUMAB WITH CARBOPLATIN AND ETOPOSIDE IN EXTENSIVE-STAGE SCLC
Carboplatin + etoposide
+ atezolizumab for four
21-day cycles
Carboplatin + etoposide
+ placebo for four 21-day
cycles
R
Eligibility (N = 201)
• Extensive-stage small cell lung cancer
• No prior systemic treatment
• ECOG performance status of 0 or 1
• No active or untreated CNS metastases
• No history of autoimmune disease
Primary endpoints: Duration of progression-free survival by the investigator using
RECIST v1.1 and overall survival
1:1Maintenance
placebo
Maintenance
atezolizumab
Horn L et al. N Engl J Med 2018;[Epub ahead of print].

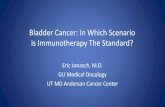
IMPOWER133: SURVIVAL OUTCOMES WITH FIRST-LINE ATEZOLIZUMAB AND CHEMOTHERAPY FOR EXTENSIVE-STAGE SMALL CELL LUNG CANCER
• The safety profile of atezolizumab + carboplatin and etoposide was consistent with the previously reported safety profile of the individual agents; no new findings were observed.
Median OS 12-mo OS HR p-value
Atezolizumab 12.3 mo 51.7%0.70 0.007
Placebo 10.3 mo 38.2%
Horn L et al. N Engl J Med 2018;[Epub ahead of print].
Pat
ien
ts w
ho
su
rviv
ed
(%
)
Months
Overall Survival
Median PFS 12-mo PFS HR p-value
Atezolizumab 5.2 mo 12.6%0.77 0.02
Placebo 4.3 mo 5.4%
Months
Pat
ien
ts w
ho
su
rviv
ed
wit
ho
ut
dis
ease
pro
gre
ssio
n (
%)
PFS

CHECKMATE 032: 3RD LINE NIVOLUMAB
Ready, JTO 2018
109 patients included, median follow up 28.3 months
• Response rate 11.9%
• Median duration of response 17.9 months
• Median survival 5.6 months
• FDA accelerated approval August 16, 2018

IMMUNOTHERAPY AND SCLC
• Addition of atezolizumab to first-line chemotherapy improves overall survival.
• Immunotherapy has modest activity in the pretreated setting but most patients do not achieve durable survival benefit.
• Randomized studies in second line have failed in an unselected population.
• Desperate need for a predictive biomarker.

NON-SMALL CELL LUNG CANCER (NSCLC)
NO ACTIONABLE MUTATIONS

52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS
• October 2007, this 52 YO former smoker female presented to the ED with persistent right shoulder and across the shoulder blades pain for several weeks.
• CXR and CT chest showed Right apical chest mass measures 6.7 x 5.1 x 6.8 cm grows into the chest wall. This extends into the neural foramina. The T3 vertebral body is collapsed. There is pathologic fracture with extensive tumor infiltration. Tumor extends posterior to the T2 vertebral body as well. Additional right hilar adenopathy measures 2.0 x 1.5 cm.
• PET Scan confirms the above findings.
• MRI Brain was negative.
• CT Core biopsy was performed and was consistent with NSCLC, NOS and no actionable mutations.

52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS

Before Treatment After Chemo and Radiation
52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS

• She did well for few months after concurrent Chemo and Radiation , then had disease progression in March of 2008 with multiple new pulmonary nodules.
• She was then started on systemic Chemotherapy with Carboplatin and Pemetexed (Alimta) for 6 cycles with partial response followed by Maintenance Pemetrexed every 3 weeks.
52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS

• October 2008, She had small solitary Brain metastasis, treated with SRS.
• Maintenance Pemetrexed (Alimta) was continued.
52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS

• January 2009, She developed left abdominal wall solitary mass. This was treated with Radiation and Maintenance Pemetrexed (Alimta) was continued.
• She developed 1-2 small new brain lesions during her course of treatment, treated with SRS and resolved.
52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS

• This patient is now 65 and she is still on Maintenance Pemetrexed (Alimta) 173 cycles and No evidence of active disease.
• Is She Cured? Probably.
• How long would I continue her on Maintenance Alimta? I do not know but she is tolerating it well and no concerning side effects.
52 YO FEMALE WITH NSCLC WITH NO ACTIONALBLEMUTATIONS

ECOG=Eastern Cooperative Oncology Group.
Cisplatin/Paclitaxel
Cisplatin/Gemcitabine
Cisplatin/Docetaxel
Carboplatin/Paclitaxel
1.0
0.8
0.6
0.4
0.2
0.0
0 5 10 15 20 25 30
Time (mos)
Pati
en
t S
urv
ival
(%)
THERAPEUTIC PLATEAU IN METASTATIC
NSCLC?
ECOG 1594
Schiller JH, et al. N Engl J Med. 2002;346:92-98.

OS OF PEMETREXED IN NON-SQUAMOUS HISTOLOGY

PARAMOUNT: Pemetrexed Final OS from Randomization
PemetrexedPlacebo
Log-rank P = 0.0195Unadjusted HR: 0.78
(95% CI: 0.64–0.96)
Patients at Risk
Pem + BSC 359 333 272 235 200 166 138 105 79 43 15 2 0Placebo + BSC 180 169 131 103 78 65 49 35 23 12 8 3 0
Surv
ival
Pro
bab
ility
Time from Randomization (Months)
0 3 6 9 12 15 18 21 24 27 30 33 36
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0

Reck, NEJM 2016
~30%PD-L1 50%EGFR/ALK WT
Primary endpoint PFS
Pembrolizumab is better than chemo in PD-L1 50%KEYNOTE-024

N Engl J Med 2018;378(22):2078-92.

KEYNOTE-189: OS AND PFS RESULTS (PRIMARY ENDPOINT ANALYSES)
Gandhi L et al. N Engl J Med 2018;378(22):2078-92.
Median OS HR p-valuePembro/pem/plat Not reached
0.49 <0.001Placebo/pem/plat 11.3 mo
Overall Survival, ITT
Median PFS HR p-value
Pembro/pem/plat 8.8 mo0.52 <0.001
Placebo/pem/plat 4.9 mo
Progression-Free Survival, ITT
Pat
ien
ts w
ith
ou
t d
ise
ase
p
rogr
ess
ion
or
de
ath
(%
)
OS,
%
Months Months
Pembrolizumabcombination (n = 410)
Placebo combination (n = 206)
Pembrolizumabcombination (n = 410)
Placebo combination (n = 206)
• Response rate (pembro combination vs placebo combination): 47.6% vs 18.9% (p < 0.001)

PEMBROLIZUMAB (PEMBRO) VERSUS PLATINUM-BASED CHEMOTHERAPY (CHEMO) AS FIRST-LINE THERAPY FOR ADVANCED/METASTATIC NSCLC WITH A PD-L1 TUMOR PROPORTION SCORE (TPS) ≥1%: OPEN-LABEL, PHASE 3 KEYNOTE-042 STUDY
Lopes G et al.
Proc ASCO 2018;Abstract LBA4.

Pembrolizumab superiority is driven by >50% PD-L1KEYNOTE-042
PD-L1 positive
PD-L1 1-49%
PD-L1 > 50% Mok, Lancet 2019;393:1819

KEYNOTE-042: PHASE III RESULTS OF FIRST-LINE PEMBROLIZUMAB IN ADVANCED/METASTATIC NSCLC (TPS ≥1%)
Lopes G et al. Proc ASCO 2018;Abstract LBA4.
* Carboplatin/paclitaxel or carboplatin/pemetrexed up to 6 cycles; a Exploratory analysis
Primary analysis: Median OS in PD-L1 TPS ≥50%, ≥20% and ≥1%
Patient subgroup Pembrolizumab Chemotherapy* HR (p-value)
TPS ≥50% (n = 299; 300) 20.0 mo 12.2 mo 0.69 (0.0003)
TPS ≥20% (n = 413; 405) 17.7 mo 13.0 mo 0.77 (0.0020)
TPS ≥1% (n = 637; 637) 16.7 mo 12.1 mo 0.81 (0.0018)
TPS ≥1%-49% (n = 338; 337)a 13.4 mo 12.1 mo 0.92 (—)
• Duration of response was longer in patients who received pembrolizumab than in those who received chemotherapy, at all PD-L1 levels examined.
• At the time of this analysis, no significant PFS benefit was observed with pembrolizumab compared to chemotherapy.

N Engl J Med 2018;378(24):2288-301.

IMPOWER150: PFS RESULTS OF FIRST-LINE ATEZOLIZUMAB WITH BEVACIZUMAB AND CHEMOTHERAPY IN METASTATIC NONSQUAMOUS NSCLC
Socinski MA et al. N Engl J Med 2018;378(24):2288-301.
PFS in WT ITT Population
WT = wild type; ABCP = atezolizumab + BCP; BCP = bevacizumab/carboplatin/paclitaxel
• Median PFS was significantly longer in the ABCP vs BCP group in the effector T-cell (Teff)-high WT population: – 11.3 mo vs 6.8 mo (HR 0.51, p < 0.001)
• PFS was also higher in the ABCP arm for the entire ITT population, patients with low or negative PD-L1 expression and patients with low Teff gene signatures
Stratified hazard ratio, 0.62 P < 0.001
Median in the ABCP group,8.3 mo
Median in the BCP group,6.8 moP
rogr
ess
ion
-fre
e s
urv
ival
(%
)
Months
At 6 mo At 12 mo
ABCP 66.9% 36.5%
BCP 56.1% 18.0%
Rate of Progression-Free Survival

IMPOWER150: INTERIM ANALYSIS OF OVERALL SURVIVAL
Socinski MA et al. N Engl J Med 2018;378(24):2288-301.
WT = wild type; ABCP = atezolizumab + BCP; BCP = bevacizumab/carboplatin/paclitaxel
Stratified hazard ratio, 0.78 p = 0.02
Rate of Overall Survival
At 12 mo At 24 mo
ABCP 67.3% 43.4%
BCP 60.6% 33.7%
OS in WT ITT Population
Months
Ove
rall
surv
ival
(%
)
Median in the BCP group,14.7 mo (95% CI, 13.3-16.9)
Median in the ABCP group,19.2 mo (95% CI, 17.0-23.8)
ABCP
BCP

KEYNOTE-407: PHASE 3 STUDY OF CARBOPLATIN-PACLITAXEL/NAB-PACLITAXEL WITH OR WITHOUT PEMBROLIZUMAB FOR METASTATIC SQUAMOUS NSCLC
Presented By Luis Paz-Ares at 2018 ASCO Annual Meeting

KEYNOTE#407 OS AND PFSPEMBRO + CHEMOTHERAPY VS. CHEMOTHERAPY ALONE

Hellmann, NEJM 2018
Primary endpoint PFS in high TMB (10Mut/Mb)HR 1.07 in <10Mut/Mb
Ipilimumab/nivolumab is better than platinum chemotherapy in TMB 10Mb irrespective of PD-L1
CheckMate 227

NON-SMALL CELL LUNG CANCER (NSCLC)
ACTIONABLE MUTATIONS


EGFR MUTATIONS

40 YO SMOKER WITH NSCLC, ADENOCARCINOMA WITH EGFR MUTATION
• This a 40 YO Heavy Smoker Male presented with worsening cough, shortness of breath and Chest and back pain.
• Cardiac work up was negative.
• CXR showed Diffuse Miliary pattern throughout both lungs. Question infectious as process such as tuberculosis/histoplasmosis. He was treated for Tuberculosis with no improvement.
• CT of the chest was performed and showed similar findings to the CXR and sclerotic bone lesions.
• Condition deteriorated and required hospitalization and was on 6 L/min O2 with O2 saturation <90%.
• Bronchoscopy was performed and the pathology was c/w NSCLC, Adenocarcinoma with positive EGFR (L858R) mutation.
• The patient was started on Erlotinib (Tarceva), Standard of Care at that time (2010).
• Within Few days of starting the treatment, he left the hospital with no O2 requirement.

40 YO SMOKER WITH NSCLC, ADENOCARCINOMA WITH EGFR MUTATION
Before After



50 YO FEMALE NEVER SMOKER WITH NSCLC, ADENOCARCINOMA WITH EGFR MUTATION
• She has been complaining of dry cough and wheezing for several months. She was treated for Allergy and cough medications with no improvements.
• CXR showed Widespread opacity, favor Miliary pattern. Miliary tuberculosis should specifically be considered.
• CT chest: Numerous bilateral subcentimeter pulmonary nodules with focal consolidation of more prominent nodules over the superior segment of the left lower lobe.
• PET scan confirms the findings with no extrathoracic disease and MRI brain was negative.
• Bronchoscopy was performed and confirms NSCLC, Adenocarcinoma but tissue was insufficient for Molecular studies. She had significant SOB with high O2 requirement.
• Guardant 360 blood test reveals positive EGFR mutation with Exon 19 deletion.
• She was started on Afatinib and not Osimertinib because of EKG abnormalities.

50 YO FEMALE NEVER SMOKER WITH NSCLC, ADENOCARCINOMA WITH EGFR MUTATION
Before Afatinib After Afatinib

AFATINIB PROGRESSION FREE SURVIVAL

N Engl J Med 2018;378(2):113-25.

SPECTRUM OF ACTIVITY OF EGFR TKIS
Drug
EGFR
L858R
EGFR
Exon
19 del
EGFR
T790M
EGFR
(WT) HER2
1st gen
gefitinib + + - + -
erlotinib + + - + -
2nd genafatinib
dacomitinib
+
+
+
+
-
-
+
+
+
+
3rd gen osimertinib + + + - -

HOW WE TREAT PATIENTS WITH EGFR MUTANT LUNG CANCER?
Diagnosis9-11 month
Median PFS
1st Gen
~10 months Median PFS with osimertinib
(T790M +)
DiagnosisStart with osimertinib?
~4 months Median PFS with Chemotherapy
?

FLAURA: OSIMERTINIB FOR PATIENTS WITH EGFR MUTATION-POSITIVE NSCLC
Soria JC et al. N Engl J Med 2018;378(2):113-25.
Osimertinib (n = 279)
Standard EGFR-TKI (n = 277)
Median PFS = 18.9 mo
Median PFS = 10.2 mo
HR = 0.46p < 0.001
Primary endpoint: PFS for patients with EGFR exon 19 del or L858R mutation
Overall survival data were immature at interim analysis; 18-mo survival rate 83% vs 71% (HR 0.63, p = NS)

OSIMERTINIB VS GEFITINIB/ERLOTINIB AS FIRST TREATMENT FOR NSCLC
OVERALL SURVIVAL
Soria et al, NEJM 2017
Hazard ratio – 0.63 (95% CI, 0.45-0.88)
p=0.007

RESISTANCE TO OSIMERTINIB…IT’S NOT SO EASY
Adapted from Ramalingam FLAURA Update and Rudin ESMO 2018 presentation.
Piotrowska et al. Cancer Discov 2018, Le et al. Clin Cancer Research 2018
FLAURA AURA3 Le et al. Piotrowska et al.
N 91 83 42 41First line 91 N/A 6 1
Paired tissue (1st line)
N/A N/A 6 (0) N/A
Acquired changesSCLC/SqCC N/A N/A 2%/0% 5%/2%MET amp 15% 19% 15% 19%HER2 amp 2% 5% 2% 5%
PIK3CA mut 7% 1% 5% 12%BRAF mut 3% 3% 0% 0%KRAS mut 3% 0% 2% 0%
Fusions 1% 3% 5% 10%EGFR mut 9% 17% 26% 24%
Other 60% 52% 40% 23%

ALK INHIBITORS

ALEX PHASE III TRIAL DESIGN
In comparison to crizotinib, alectinib improved both PFS (HR = 0.47, p < 0.001) and OS (HR = 0.76, p = 0.24)
Peters S et al. N Engl J Med 2017;377:829-38.
R
Alectinib 600 mg BID
(n = 143)
Crizotinib 250 mg
BID (n = 143)
Until PD* or
premature
withdrawal
(eg, due to
toxicity)
Subsequent
therapy and
survival follow-up
1:1
* Determined by investigators,
based on RECIST v1.1
Eligibility
• ALK+• Stage IIIB/IV or
recurrent NSCLC• Chemotherapy naïve• ECOG PS 0-2

ALEX: UPDATED PFS AND OS OUTCOMES IN THE ITT POPULATION
Camidge DR et al. Proc ASCO 2018;Abstract 9043.
Stratified HR = 0.43 Hazard ratio for death, 0.76
Time (months) Time (months)
PFS
est
imat
e (
%)
Ove
rall
surv
ival
est
imat
e (%
)
Alectinib (N = 152)Crizotinib (N = 151)Censored+
Alectinib (N = 152)Crizotinib (N = 151)Censored+
34.8 months
10.9 months

ALTA-1L: PROGRESSION-FREE SURVIVAL WITH BRIGATINIBVERSUS CRIZOTINIB FOR ALK-POSITIVE NSCLC
• The confirmed objective response rate was 71% with brigatinib and 60% with crizotinib.
• The confirmed rate of intracranial response among patients with measurable lesions was 78% with brigatinib and 29% with crizotinib.
• No new safety concerns were noted.
Brigatinib
(N = 137)
Crizotinib
(N = 138)
Median PFS, months NR 9.8
12-month PFS 67% 43%
Camidge DR et al. N Engl J Med 2018;[Epub ahead of print].
Pro
gre
ssio
n-f
ree
su
rviv
al(%
of
pat
ien
ts)
Months
Hazard ratio for disease progression or death, 0.49
p < 0.001 by log-rank test

PROGRESSION FREE SURVIVAL WITH LORLATINIB IN PATIENTS WITH PRIOR 2ND-GEN ALK TKI(S) – TUMOR TISSUEA
EXP3B,4–5 (n=135)
No Mutation
(n=81)
≥1 Mutation
(n=29)
Number with event, n (%) 57 (70.4) 17 (58.6)
Median PFS, months
(95% CI)
5.4
(3.9, 6.9)
11.0
(6.9, 22.9)
aDetected in archival or de novo tumor tissue.
40
Time (months)
60
80
100
20
010 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
7681 56 44 37 34 30 25 23 22 20 20 14 12 8 6 3 3 2 2 2 0 0 0
2929 26 24 24 23 20 18 17 15 14 14 10 8 7 4 3 3 3 3 3 2 2 0
Pro
gre
ssio
n-f
ree s
urv
iva
l (%
)
EXP3B,4–5: Prior 2nd-gen TKI
(N=139)a
No Mutationb
(n=87)
≥1 Mutationb
(n=49)
BOR, n (%)
CR
PR
SD
PD
IND
2 (2.3)
21 (24.1)
36 (41.4)
21 (24.1)
7 (8.0)
1 (2.0)
29 (59.2)
10 (20.4)
5 (10.2)
4 (8.2)
ORR, n
(%)
95% CI
23 (26.4)
17.6, 37.0
30 (61.2)
46.2, 74.8

FDA APPROVES LORLATINIB FOR SECOND- OR THIRD-LINE TREATMENT OF METASTATIC NSCLC WITH ALK REARRANGEMENT
PRESS RELEASE – NOVEMBER 2, 2018
“On November 2, 2018, the Food and Drug Administration granted accelerated approval to lorlatinib for patients with anaplastic lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) whose disease has progressed on crizotinib and at least one other ALK inhibitor for metastatic disease or whose disease has progressed on alectinib or ceritinib as the first ALK inhibitor therapy for metastatic disease.
Approval was based on a subgroup of 215 patients with ALK-positive metastatic NSCLC, previously treated with one or more ALK kinase inhibitors, enrolled in a non-randomized, dose-ranging and activity-estimating, multi-cohort, multicenter study (Study B7461001; NCT01970865). The major efficacy measures were overall response rate (ORR) and intracranial ORR, according to RECIST 1.1, as assessed by an independent central review committee.”
https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm625027.htm

OTHER TARGET MUTATIONS

CLINICAL ACTIVITY OF LOXO-292, A HIGHLY SELECTIVE RET INHIBITOR, IN PATIENTS WITH RET FUSION+ NON-SMALL CELL LUNG CANCER
Oxnard GR et al.
Proc WCLC 2018;Abstract OA12.07.

LIBRETTO-001: PHASE I RESULTS WITH LOXO-292 IN RET FUSION- POSITIVE NSCLC
• Dose exploration ongoing at 200 mg BID; most treatment-emergent AEs were Grade 1
• 4 patients experienced treatment-related AEs Grade ≥3: Diarrhea, increased ALT/AST, tumor lysis syndrome (DLT @ 240 mg BID), thrombocytopenia (DLT @ 240 mg BID)
Oxnard GR et al. Proc WCLC 2018;Abstract OA12.07.
ORR in all patients (N = 38) = 68%
4/4 confirmed intracranial responses (1 CR, 3 PR)
RET-Fusion Positive NSCLC
Be
st t
um
or
resp
on
se (
%)
KIF5B-RET
CCDC6-RET
CLIP1-RET
RET rearrangement NOS
Prior chemotherapyPrior immunotherapyPrior multikinase inhibitorPrior other therapy

ARROW: PHASE I TRIAL OF BLU-667 ANTITUMOR ACTIVITY IN RET FUSION–POSITIVE NSCLC COHORT
• Responses rapid, durable
• Most responses observed by first scan (Wk 8)
• Median DoR: NR
• 82% of responders remain on tx at data cutoff
• Patients on treatment up to 24 mos (includes dose-escalation patients, any dose)
• Responses observed regardless of prior PD-1/PD-L1 inhibitor therapy, RET fusion genotype, CNS involvement
• Active in CNS; shrinkage of measurable brain mets observed in 7 out of 9 (78%) patients
• No patient on RP2D showed progression due to new CNS involvement
Gainor. ASCO 2019. Abstr 9008. Slide credit: clinicaloptions.com
Best Response All Patients (n = 48) Previously Treated With Platinum (n = 35)
ORR, % (95% CI) CR,* n PR,*† n SD, n PD, n
58 (43-72)1
27182
60 (42-76)1
2014--
DCR (95% CI) 96 (86-99) 100 (90-100)
Data cutoff: April 28, 2019. *Responses confirmed on 2 consecutive assessments. †Confirmed PR in 5 out of 7 (71%) treatment-naive patients.

ROS1
• Crizotinib is licensed but has CNS liability, presence/absence of CNS disease may explain variable median PFS of crizotinib across PFS trials
• Entrectinib (seeking a license) has similar spectrum of activity as crizotinib but CNS penetration. ASCO 2019 Abstract 3017. CNS ORR 55%
• Repotrectinib (AKA ropotrectinib and TPX-0005) has CNS penetration and activity against G2032R reported in 2/4 cases previously (Drilon et al, ASCO 2018). ASCO 2019 abstract 9011. 18 TKI-pretreated ROS1 pts, ORR 28%, DOR of 10.2 mos. cORR 44% in 9 such pts at dose levels of ≥160 mg QD. Intracranial ORR was 3/3 (100%). LOOK for G2032R response rate!
• Lorlatinib (being used off label) has excellent CNS penetration and possibly additional activity in some ROS1 resistance mutations (but not G2032R)

CRIZOTINIB IN ROS1 REARRANGEMENT–POSITIVE NSCLC
• Median follow-up for OS: 62.6 mos
• 14 patients (26%) remain in follow-up
ROS1-Rearranged NSCLC (N = 53)
Deaths, n (%) 26 (49.1)
Median OS, mos (95% CI)
51.4 (29.3-NR)
40
OS
(%)
Mos
60
80
100
20
00 4020 60 80
53Pts at Risk, n 48 42 37 31 27 23 20 18 17 9 5 4 02033 13 3
1-yr OS rate: 79%
4-yr OS rate: 51%
Censored
Slide credit: clinicaloptions.comShaw. Ann Oncol. 2019. [Epub]

n (%)Total
N = 53
CNS disease at baselineN = 23
No CNS disease at baselineN = 30
ORR 41.7 (77.4) 17 (73.9) 24 (80.0)
CR 3 (5.7) 0 3 (10.0)
PR 38 (71.7) 17 (73.9) 21 (70.0)
SD 1 (1.9) 0 1 (3.3)
Clinical benefit rate
41 (77.4) — —
ENTRECTINIB FOR LOCALLY ADVANCED OR METASTATIC ROS1 FUSION-POSITIVE NSCLC
Doebele RC et al. Proc WCLC 2018;Abstract OA02.01.
• In patients with CNS disease at baseline, intracranial ORR and DoR were 55% and 12.9 mo, respectively.
• Most adverse events were Grade 1-2 and reversible.
• Grade 3 adverse events included anemia (4.5%), fatigue (2.8%) and increased weight (5.1%).
Change in tumor size: ROS1+ NSCLC population (n = 53) (BICR assessment)

NTRKNEUROTROPHINS AND TROPOMYOSIN RECEPTOR KINASES
• Rare gene rearrangements – should tip anyone over into doing panel based testing as now 5 FDA approved treatments for molecular subtypes of NSCLC (EGFR, ALK, ROS1, BRAF and NTRK)
• Larotrectinib licensed
• Entrectinib seeking a license

RESULTS OF A “BASKET” STUDY ON LAROTRECTINIB
Drilon A, et al. N Engl J Med. 2018;378(8):731-739.
Efficacy regardless of tumor type
ORR Inv 80%IRC 75%8.3 months median follow upMedian DoR NRMedian PFS NR3 of 4 lung tumors

Cut-off date: 31 May 2018
Note: Patients (n=6) without matched pre/post therapy scans were excluded from the plot
CI: confidence interval; CRC: colorectal cancer; MASC: mammary analogue secretory carcinoma; NSCLC: non-small cell lung cancer
Entrectinib activity in NTRK fusion-positive solid tumours: individual patient responses by tumour type
0
-30
-50
-90
Bes
t %
ch
ang
e fr
om
bas
elin
e
15
-80
-70
-60
-40
-20
-10
20
30
40
-100
50
CRCNSCLCSarcoma
Neuroendocrine tumours
PancreaticThyroidMASC Breast
CholangiocarcinomaGynaecological
NTRK+ patients (n=54)
ORR (95% CI) 57.4% (43.2–70.8)
SD 9 (16.7)
PD 4 (7.4)
Non-CR/PD, missing or unevaluable
10 (18.5)
Results per Blinded Independent Central Review (BICR)
7/9 NSCLC responses?

IMMUNOTHERAPY IN
UNRESECTABLE STAGE III NSCLC


PACIFIC: PFS BY BLINDED INDEPENDENT CENTRAL REVIEW IN THE INTENT-TO-TREAT POPULATION (PRIMARY ENDPOINT)
• No new safety signals were observed, and the most common Grade 3 or 4 adverse event associated with durvalumab compared to placebo was pneumonia (4.4% and 3.8%, respectively).
• OS data were immature at the time of this analysis.
Antonia SJ et al. N Engl J Med 2017;377(20):1919-29.
PF
Sp
rob
ab
ilit
y
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 3 6 21 24 27
Time from randomization (months)
Placebo
Durvalumab
Durvalumab
(N = 476)
Placebo
(N = 237)
Median PFS, months 16.8 5.6
12-month PFS rate 55.9% 35.3%
18-month PFS rate 44.2% 27.0%
Stratified hazard ratio, 0.52Two-sided p < 0.001
9 12 15 18

PACIFIC: OVERALL SURVIVAL IN THE INTENTION-TO-TREAT POPULATION
Durvalumab
(N = 476)
Placebo
(N = 237)
Median OS, months NR 28.7
12-month OS rate 83.1% 75.3%
24-month OS rate 66.3% 55.6%
Stratified hazard ratio, 0.68Two-sided p = 0.0025
Antonia SJ et al. N Engl J Med 2018;[Epub ahead of print].
• A total of 30.5% of the patients in the durvalumab group and 26.1% of those in the placebo group had Grade 3 or 4 adverse events of any cause.
• 15.4% and 9.8% of the patients, respectively, discontinued the trial regimen due to adverse events.
Durvalumab
Placebo
Pro
ba
bilit
yo
f o
ve
rall
su
rviv
al
Months since randomization

CONCLUSION
• Lung Cancer does not discriminate between Smokers and Non-Smokers, Males or Females, Young or Old.
• The landscape of Lung Cancer treatment has significantly changed over the last 10 years with Target Therapy and most recently Immunotherapy.
• Further improvements in early detection , Biomarkers and new therapies are still needed for better care of Lung Cancer Patients.