
READY SET - Home | St. Mary's Medical Centerre_Just_Getting_Started-Neuro_Reha… · HealthSouth...
17
HealthSouth Rehabilitation Hospital Huntington Dr. Timothy Saxe, Medical Director READY ………… SET …………. OUR BRAINS!!!!! Stroke Facts 795,000 strokes each year-600,000 new strokes 5.5 million stroke survivors Leading cause of disability in adults Many strokes are preventable Stroke rehab works stroke
Transcript of READY SET - Home | St. Mary's Medical Centerre_Just_Getting_Started-Neuro_Reha… · HealthSouth...
HealthSouth Rehabilitation Hospital Huntington
Dr. Timothy Saxe, Medical Director
READY …………
SET ………….
OUR BRAINS!!!!!
Stroke Facts
� 795,000 strokes each year- 600,000 new strokes
� 5.5 million stroke survivors
�Leading cause of disability in adults
�Many strokes are preventable
�Stroke rehab works stroke

Stroke Prevalence per 1,000
Three Groups of Stroke Survivors
� 10-20 % recover full
independence in two weeks
� 10-20 % have severe residual
deficits
� 60-80 % are in the middle group
stroke survivors
TBI� Most common of serious, disabling neurologic
disorders
� Large proportion of males younger than 30
� Commonly affects people with pre-existing mental health issues
� Persistent effects of TBI on cognition, emotion and behavior

Realms Impacted� Physical
� Cognitive
� Psychological
� Emotional
� Visual
� Perceptual
� Communicative
� Social
� Educational
� Recreational
� Vocational
� Family Structure
Collateral Sprouting
�Collateral sprouting to reinnervate cells and circuits
8
BACK TOGETHER

Neural Plasticity
�Unmasking of other neural pathways and synapses (neural plasticity)
Neural Plasticity
� Improvement requires the performance of functional tasks
� Neural plasticity can take place for years after a stroke
yearsafter
stroke
Neural plasticity
Neural Plasticity
The ability of the Central Nervous
System (CNS) to adapt to
injuries or environmental
requirements.

Neurons Repair Slowly� Maximize brain repair & restoration with rest.
� Comprehend & accept strengths & limitations.
� Relearn old concepts, habits, & skills.
� Master compensatory strategies and/or assistive technology.
� Make new friends.
� Create a new life of meaning, joy & value.
COULD YOU DO THIS WITHOUT HELP?
Rescue vs. Collapse
� Intermediate loss of
connections
� Critical state
� Either lose connectivity permanently or recover
� Need REHAB!
rehabilitation
restore function
Rehabilitation Drives Recovery
Rehabilitation (learning) can drive recovery by
enhancing interconnections to reconfigure the
neural circuits and restore function.
RehabilitationAggressive rehabilitation can make a difference in
how quickly one is able to return home and get back to the quality of life they deserve following an illness or injury. Rehabilitation hospitals utilize a team approach to offer a more intense regimen and higher level of care such as greater physician involvement and therapy time
Principles of Rehabilitation� Rehab needs to start immediately
� Patient-centered (family/caregiver included)
� Goal Oriented emphasizing abilities
� Team approach
� Education starts immediately
� Wellness promotion
� Education, Adjustment, and Change
Goals of RehabilitationTo improve and Individual’s Quality of Life & help
him or her reach the fullest possible physical, psychological, educational, vocational and social potential.
Focuses on…..
“ADAPTATION
”

Who are Rehab Candidates??ANYONE with deficits & potential to “recover”
� functional, cognitive, communication, psychological, educational, or vocational
RECOVERY/TREATMENTS (patient specific)
� Full or Partial
� Restorative or Compensatory
� Training & Education to “Caregivers”
Rehabilitation Rehabilitation should immediately begin when the
patient is ……….
STABILIZED!!!!!!
The Rehabilitation TeamThe Rehabilitation Treatment Team takes on a
Interdisciplinary team approach to successful rehabilitation. The team members are dedicated to meeting patient’s physical, psychological and social needs in an environment that promotes wellness, confidence and Independence. A team of professionals have the ability to pinpoint specific needs and set goals in order to maximize recovery.

The “Special Teams”
� Physiatrist� Attending Physician*� Physical Therapist� Occupational Therapist� Speech/ Language Pathologist� Rehabilitation Nurse� Case Manager� Respiratory Therapist-as needed� Clinical psychologist- as needed� Nutritionist-as needed
* Varies from facility to facility
Physiatrists: or rehabilitation
physicians, are nerve, muscle, and
bone experts who treat injuries or
illnesses that affect how you move.
Rehabilitation physicians are medical
doctors who have completed training
in the medical specialty of physical
medicine and rehabilitation (PM&R). .
The focus is on the development of a
comprehensive program for putting the
pieces of a person’s life back together
after injury or disease-without surgery.
They provide ongoing medical
management and supervision of the
rehabilitation team.
RolesAttending Physician: Primarily oversees the medical
management of the patient. Some of their responsibilities may include the monitoring of medications, lab values, the need for further diagnostic testing. They work closely with the physiatrist and treatment team to measure the patient’s progress. He or she also oversees the continuity of care from the surgical team to the PCP

RolesPhysical Therapist: - assists in increasing overall
physical mobility. The primary focus for physical therapists is on evaluating and designing a treatment program to address limitations in physical function, mobility and safety. Areas that are emphasized include: flexibility, strength, endurance, and pain management.
AutoAmbulator
RolesOccupational Therapist: -assists in achieving
independence in activities of daily living. They design and deliver activity based therapy to promote independence in the areas of self care, home management, and community re-entry. The individualized program is tailored toward safely relearning or compensating tasks for the disabled following injury or illness.

RolesSpeech /Language Pathologist: Assesses and treats
individuals with communication and comprehension disorders, cognitive difficulties, and swallowing disorders

RolesRehabilitation Nurse: Integrates rehabilitation and
medical care as directed by physician. The nurses monitor the patient’s physical status as well as provide emotional support, encouragement, and education on wellness and medical management. This will include bowel and bladder training, skin care, medications, wound management, and coping in a healthy productive manner.
RolesCase management: Focuses on involving the
family and other caregivers in the patient’s rehabilitation. This includes helping the family adjust to changes brought about by the disability or illness. They are primarily responsible for discharge planning by providing appropriate equipment and or services that may be needed upon discharge.
ROAD TO RECOVERY
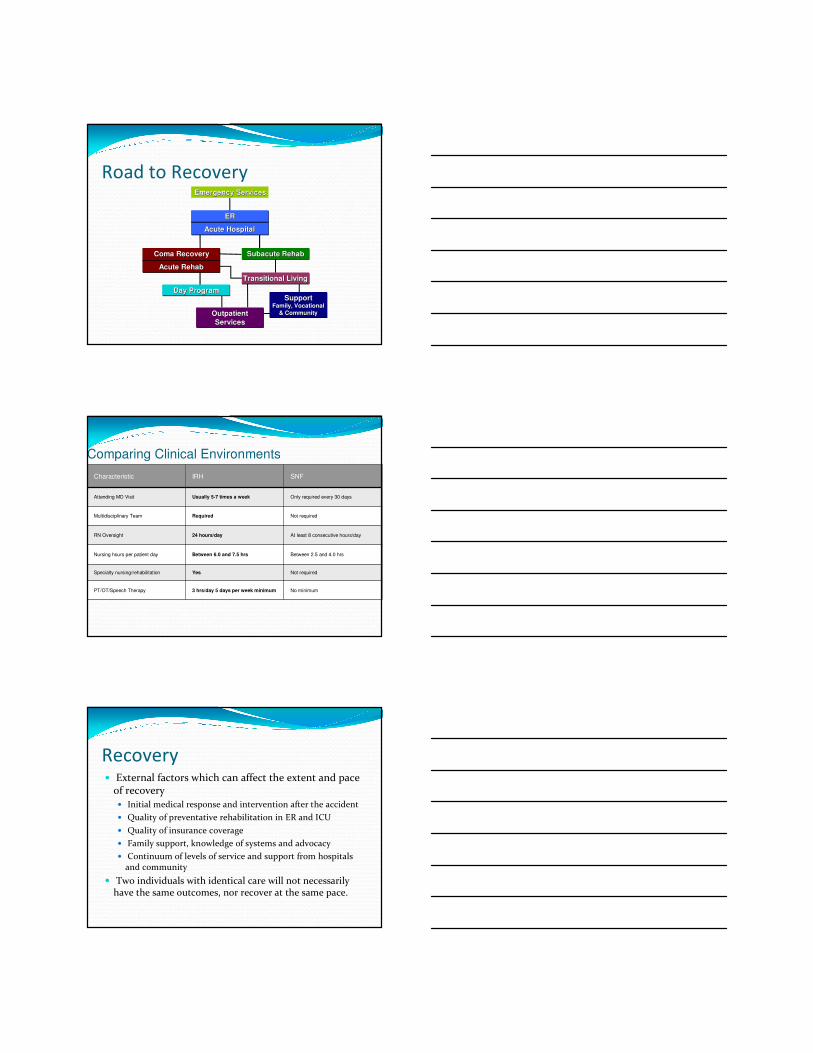
Road to RecoveryEmergency ServicesEmergency Services
ER
Acute Hospital
ERER
Acute HospitalAcute Hospital
Coma Recovery
Acute Rehab
Coma RecoveryComa Recovery
Acute RehabAcute Rehab
Subacute RehabSubacute Subacute RehabRehab
Transitional LivingTransitional LivingTransitional Living
Day ProgramDay ProgramDay Program
Outpatient
Services
OutpatientOutpatient
ServicesServices
SupportFamily, Vocational
& Community
SupportSupportFamily, VocationalFamily, Vocational
& Community& Community
Comparing Clinical Environments
Characteristic IRH SNF
Attending MD Visit Usually 5-7 times a week Only required every 30 days
Multidisciplinary Team Required Not required
RN Oversight 24 hours/day At least 8 consecutive hours/day
Nursing hours per patient day Between 6.0 and 7.5 hrs Between 2.5 and 4.0 hrs
Specialty nursing/rehabilitation Yes Not required
PT/OT/Speech Therapy 3 hrs/day 5 days per week minimum No minimum
Recovery� External factors which can affect the extent and pace
of recovery� Initial medical response and intervention after the accident
� Quality of preventative rehabilitation in ER and ICU
� Quality of insurance coverage
� Family support, knowledge of systems and advocacy
� Continuum of levels of service and support from hospitals and community
� Two individuals with identical care will not necessarily have the same outcomes, nor recover at the same pace.
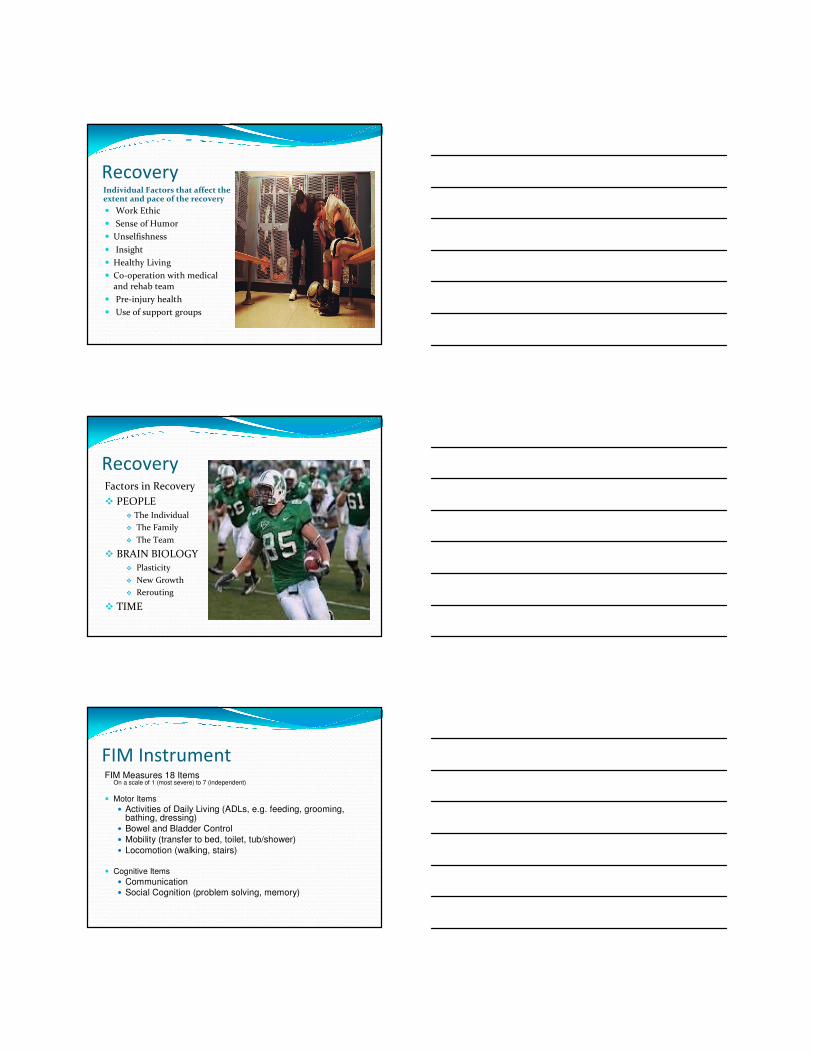
RecoveryIndividual Factors that affect the extent and pace of the recovery
� Work Ethic
� Sense of Humor
� Unselfishness
� Insight
� Healthy Living
� Co-operation with medical and rehab team
� Pre-injury health
� Use of support groups
RecoveryFactors in Recovery
� PEOPLE� The Individual
� The Family
� The Team
� BRAIN BIOLOGY� Plasticity
� New Growth
� Rerouting
� TIME
FIM InstrumentFIM Measures 18 Items
On a scale of 1 (most severe) to 7 (independent)
� Motor Items
� Activities of Daily Living (ADLs, e.g. feeding, grooming, bathing, dressing)
� Bowel and Bladder Control
� Mobility (transfer to bed, toilet, tub/shower)
� Locomotion (walking, stairs)
� Cognitive Items
� Communication� Social Cognition (problem solving, memory)

F.I.M. InstrumentLevels of (In) Dependence (0-7)
No Helper7= complete independence (safe, timely)6= modified independence (device, slow)
Helper5= supervision ( subject 100%; helper nearby)4= minimal assistance (subject 75%; helper 25%)3= moderate assistance ( 50%/ 50%)2= maximal assistance (subject 25%; helper 75%)1= total assistance (subject <25%; helper > 75%0= not assessed or N/A
Rancho Los Amigos Scale� I…No response
� II…Generalized response
� III…Localized response
� IV…confused and agitated
� V…confused, inappropriate, non-agitated
� VI…confused & appropriate
� VII…automatic & appropriate
� VIII…purposeful & appropriate
Case Study� 57 year old male presented to ER with left sided
weakness, facial dropping, slurred speech and difficulty walking. Patient also complained of a pressure like headache in his right temporal area for 2 days.
� Medical history included; HTN, MI, CAD
� BMI was only 22
� 2 ppd Smoker
� Independent at home, very active

Case Study� Home Medications included; Aspirin and Plavix
� Original CT scan of head – No acute findings
� MRI of brain impression – left MCA infarct
� Admitted to HealthSouth on 7.26.12
� Discharged on 8.17.12
� FIM Gain of 63

We ALL have a HAND in making
sure the patient has a Successful
Outcome…
George Eliot (1819-80)
“It is never too late to be what you might have been”
-Mary Ann Evans

Questions?


















