
Rc repair philosophy and technique microhand 2014
57
www.shoulder.gr www.shoulder.gr Manos Antonogiannakis Head B’ Orthopaedics Dept Center for shoulder arthroscopy IASO GENERAL Hospital Arthroscopic Treatment of Rotator Cuff Tears – Philosophy and Technique
-
Upload
shoulder-library -
Category
Health & Medicine
-
view
24 -
download
0
Transcript of Rc repair philosophy and technique microhand 2014

www.shoulder.grwww.shoulder.gr
Manos AntonogiannakisHead B’ Orthopaedics Dept
Center for shoulder arthroscopy IASO GENERAL Hospital
Arthroscopic Treatment of Rotator Cuff Tears – Philosophy and Technique

Philosophy of treatment:
restore the equilibrium between the functional demands of the patient and the capacity of the rotator cuff
Lower the functional demands of the patient. Increase the functional capacity of the remaining
intact cuff repair the cuff.
www.shoulder.gr

www.shoulder.grwww.shoulder.gr
Back to Basics


www.shoulder.grwww.shoulder.gr
Partial Thickness Tear Bursal side tears Articular side tears Intratendinus tears
Partial tear classification by Ellman Grade I <3mm deep Grade II 3-6mm deep Grade III >6mm deep (i.e. >50% thickness)

www.shoulder.grwww.shoulder.gr
Partial Tears Treatment By far the most common partial tears are Articular-
side, vascular or age related
Traditionally partial tears classifications
are based to 50%
BUT
“How healthy is the remaining,
intact tissue?”

www.shoulder.grwww.shoulder.gr
Partial Tears Treatment Options
1. Debride partial tear only2. In-situ Repair3. Convert to full thickness, Debride, Repair
Etiology drives the decision!!!
Because most tears are degenerative, option 3 should be the best for most cases
Trauma or young athletes are candidates for in-situ repair If partial tear causes significant pain then debridement alone
[Yamaguch K, 2006 Nice Shoulder Course]
r

www.shoulder.grwww.shoulder.gr
Partial Tears In situ repair

www.shoulder.grwww.shoulder.gr
COMPLETE TEARS
Small 1cm Medium 2-3cm Large 3-5 cm Massive >5cm Cofield et all

www.shoulder.grwww.shoulder.gr
Type Description Preoperative MRI Findings Treatment Prognosis
1 Crescent Short and wide tear End-to-
bone repair Good to excellent
2 Longitudinal
(L or U) Long and narrow tear
Margin
convergence
Good to excellent
3 Massive
contracted Long and wide
> (2 x 2 cm)
Interval slides or partial repair
Fair to good
4 Cuff tear
arthropathy Cuff tear arthropathy
Arthroplast
y Fair to good.
www.shoulder.grwww.shoulder.gr
ANY TYPE OF RECONSTRUCTION MUST AVOID TENSION OVER-LOAD
OF THE REPAIR

www.shoulder.grwww.shoulder.gr
Surgical Technique
Steps
1. GH Joint and Subacromial Joint Inspection
2. Bursal debridement
3. Acromioplasty (+/-)
4. Cuff mobilization
5. Strong mechanical repair without tension(side to side, tendon to bone)
6. Biologic enhancement of the repair

www.shoulder.grwww.shoulder.gr
Patient Position
Lateral decubitus my preferred position

www.shoulder.grwww.shoulder.gr
Bleeding control

www.shoulder.grwww.shoulder.gr
Keys to control bleeding

www.shoulder.grwww.shoulder.gr
30º Scope Entrance from posterior portal but change portal and viewing angle of scope ( 30 to 70) as needed

www.shoulder.grwww.shoulder.gr
Joint Side Inspection

www.shoulder.grwww.shoulder.gr
Bursal Side Inspection-Bursectomy
www.shoulder.grwww.shoulder.gr
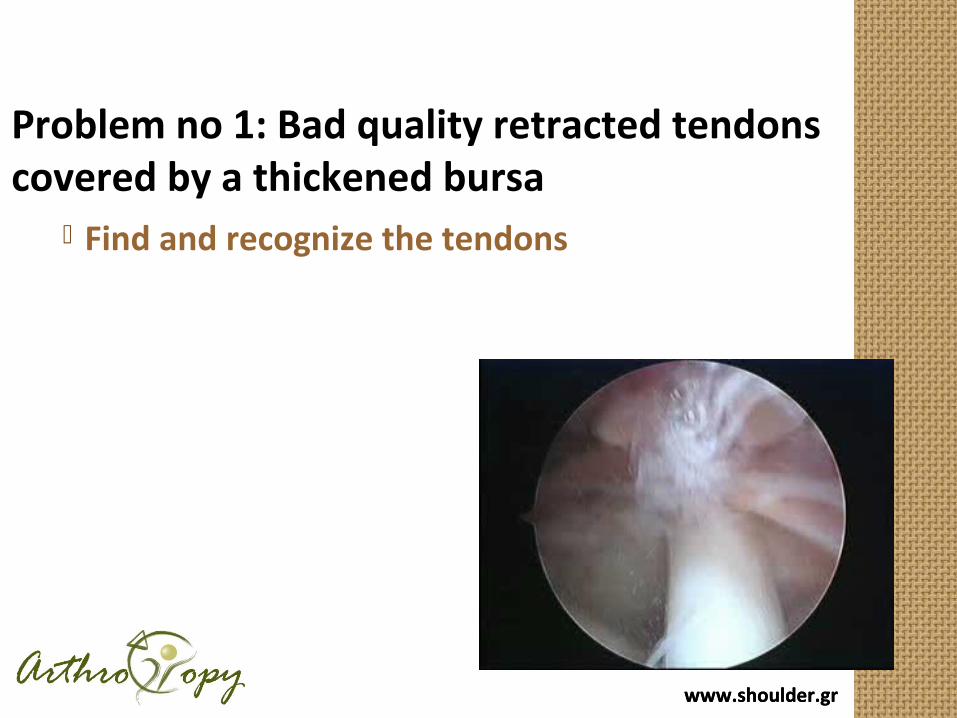
Problem no 1: Bad quality retracted tendons covered by a thickened bursa
Find and recognize the tendons

www.shoulder.grwww.shoulder.gr
Remove the thickened bursa till to see the posterior edge of the cuff ending to the greater tuberosity.Everything that goes around the tuberosity to the deltoid is bursa
Don’t suture the bursa instead of the cuff. It doesn’t work

www.shoulder.grwww.shoulder.gr
The posterior extent of the tear
Differentiate thickened bursa from the infraspinatus by finding the posterior insertion of the cuff to the tuberosity
www.shoulder.grwww.shoulder.gr
Solution Idendify recognizable landmarks
1. the undersurface of the acromion and the underolateral corner 2.the acromioclavicular joint 3.the spine of the scapula 4.the lateral border of the tuberosity
And remove the bursa

www.shoulder.grwww.shoulder.gr
Identify: 1. the Anterolateral Corner of the Acromion

www.shoulder.grwww.shoulder.gr
Identify: 2. the acromioclavicular joint

www.shoulder.grwww.shoulder.gr
Identify: 3. Lateral edge of the greater tuberosity

www.shoulder.grwww.shoulder.gr
Identify
4. the keel of the acromion

www.shoulder.grwww.shoulder.gr
Recognize the Tear PatternTears must be repaired in the direction of greatest mobility -> minimal strain
The muscle-tendon junction must be 2-3 mm medial of the edge of the cartilage at the tuberosity after the repair

www.shoulder.grwww.shoulder.gr
Tear Patterns Crescent shaped U-Shaped L-shaped (or reverse L) Massive Contracted Immobile
tears S.S. Burkhart

www.shoulder.grwww.shoulder.gr
Crescent Shaped Tear
mobilized easily for tendon to
bone fixation
S.S Burkhart

www.shoulder.grwww.shoulder.gr
Crescent-Shaped TearsRepair to bone with increased points of fixation
Double row repair ? Single row triple loadead anchors Mc Stitch configuration

www.shoulder.grwww.shoulder.gr

www.shoulder.gr

www.shoulder.grwww.shoulder.gr
Double Row FixationRestoration of the footprint

Medial Row - Matress Sutures - 2 anchors
www.shoulder.gr

Lateral Row - Simple Sutures - 2 anchors
www.shoulder.gr

www.shoulder.grwww.shoulder.gr
Suture Bridge double row

www.shoulder.gr

www.shoulder.grwww.shoulder.gr
L-Shaped & U-Shaped Tears Side to side sutures from medial to
lateral Progressively converge the margin of the
tear lateral to the bone bed Closing 50% of a U-Shaped tear ->
reduces strain at converge margin by a factor of 6
[S. S .Burkhart]

www.shoulder.grwww.shoulder.gr
Large U-shaped cuff tear extending to glenoid
Margin convergence
The free margin of the cuff is repaired to bone with suture anchors

www.shoulder.grwww.shoulder.gr
U-Shaped tear: Margin covergence with side to side sutures

www.shoulder.grwww.shoulder.gr
Massive Contracted Immobile Tears No mobility from medial to lateral
or from anterior to posterior Represent 9.6% of massive tears
[S.Burkhart]

www.shoulder.grwww.shoulder.gr
Massive Contracted Tears
Anterior Interval Slide
and/or
Posterior Interval Slide
Single and double interval slide

www.shoulder.grwww.shoulder.gr
Anterior slide-supraspinatus from coracoid –coracohumeral ligament

www.shoulder.grwww.shoulder.gr
Posterior slideInfraspinatus - supraspinatus

www.shoulder.grwww.shoulder.gr
Before
After

www.shoulder.grwww.shoulder.gr
Biologic enhancement of healing
•Acromioplasty•Tuberoplasty•PRGF injection in the subacromial space

www.shoulder.grwww.shoulder.gr
Acromioplasty

www.shoulder.grwww.shoulder.gr
Tuberoplasty

www.shoulder.grwww.shoulder.gr
Arthroscopic repair yields 90-95% excellent in small and medium size tears at 4 to
10 years F.Up.• Burkhart SS, Danaceau SM, Pearce CM Jr. Arthroscopic rotator cuff repair: Analysis of results by tear size and by repair
technique—Margin convergence versus direct tendon to bone repair. Arthroscopy 2001;17:905-912.• Wolf EM, Pennington WT, Agrawal V. Arthroscopic rotator cuff repair: 4- to 10-year results. Arthroscopy 2004;20:5-12.• Luis G. Marrero, M.D., Kyle R. Nelman, M.D., and Wesley M. Nottage, M.D., Long-Term Follow-Up of Arthroscopic Rotator
Cuff Repair. Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol xx, No x (Month), 2011: pp xxx
Good to excellent results in massive tears with less than 75% fatty infiltration of the infraspinatus, even at 10 years F.Up
• Burkhart SS, Barth JR, Richards DP, Zlatkin MB, Larsen M., Arthroscopic repair of massive rotator cuff rears with stage 3 and 4 fatty degeneration. Arthroscopy 2007;23:347-354.
• Jones CK, Savoie FH III. Arthroscopic repair of large and massive rotator cuff tears. Arthroscopy 2003;19:564-571.
• Dodson CC, Kitay A, Verma NN, et al. The long-term outcome of recurrent defects after rotator cuff repair. Am J Sports Med 2010;38:35-39.
• Luis G. Marrero, M.D., Kyle R. Nelman, M.D., and Wesley M. Nottage, M.D., Long-Term Follow-Up of Arthroscopic Rotator Cuff Repair. Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol xx, No x (Month), 2011: pp xxx

www.shoulder.grwww.shoulder.gr
Using the above techniques Burkhart reported less than
3% irreparable cuff tears

www.shoulder.grwww.shoulder.gr
Complete loss of active external rotation (external rotation lag ) is a bad prognostic factor
Superior migration of the humeral head in contact with the acromion – repair attempt is going to be a failure
Rotator Cuff Arthropathy
What are the limits?

www.shoulder.grwww.shoulder.gr
Conclusions Acute Crescent Tear Standard Techniques for tendon to bone fixation U- or L- shaped Tears
Side to side margin convergence
Partially mobile tears Anterior / Posterior Slide Medialized Repair Incomplete repair
Irreparable Tears debridement Tendon transfers Reverse – Extended head arthroplasty

www.shoulder.grwww.shoulder.gr
Thank you for your attention

www.shoulder.grwww.shoulder.gr
Single and double interval slide
Anterior slide through release in the rotator interval (supraspinatus–coracobrachialis)
Posterior slide through release of the interval supraspinatus-infraspinatus

www.shoulder.grwww.shoulder.gr
Stay sutures to the cuff

www.shoulder.grwww.shoulder.gr
Release of MMP and GF after acromioplasty Platelet-derived growth factor-AB (PDGF-AB), basic
fibroblast growth factor basic (bFGF) and transforming growth factor beta 1 (TGF-b1) are released after acromioplasty in the subacromial space.
Knee Surg Sports Traumatol Arthrosc (2009) 17:98–101 Release of growth factors after arthroscopic acromioplasty . Pietro Randelli Ζ Fabrizio Margheritini Ζ Paolo Cabitza Ζ Giada Dogliotti Ζ Massimiliano M. Corsi
MMP-2 does not increase but MMP-9 increases after acromioplasty and their mesurment can be a useful tool to be monitored in parallel with growth factors level and other bone turnover markers in order to evaluate the bone remodelling and tissue healing.
E. Galliera , P. Randelli, G. Dogliotti, E. Dozio, A. Colombini, G. Lombardi, P. Cabitza, M. Corsi. Matrix metalloproteases MMP-2 and MMP-9: Are they early biomarkers of bone remodelling and healing after arthroscopic acromioplasty? Injury, Int. J. Care Injured 41 (2010) 1204–1207

www.shoulder.grwww.shoulder.gr
Conclusions Rot Cuff is extremely significant for the normal function of the
shoulder
Rot Cuff tears can be asymptomatic
Symptoms Produced by a tear depend on: Size Location Functional demands of the patient


















