Ravi Vij MD Associate Professor Section of BMT and Leukemia
16
Induction Therapy For Multiple Myeloma: Two vs Three Drug Regimen and Role of Risk Stratification Ravi Vij MD Associate Professor Section of BMT and Leukemia Washington University School of Medicine
description
Induction Therapy For Multiple Myeloma: Two vs Three Drug Regimen and Role of Risk Stratification. Ravi Vij MD Associate Professor Section of BMT and Leukemia Washington University School of Medicine. 1989–1994. 1995–2000. 2001–2006. M. Trends in Overall Survival of MM. 1.0. - PowerPoint PPT Presentation
Transcript of Ravi Vij MD Associate Professor Section of BMT and Leukemia

Induction Therapy For Multiple Myeloma:
Two vs Three Drug Regimen and Role of Risk Stratification
Ravi Vij MDAssociate Professor
Section of BMT and LeukemiaWashington University School of Medicine

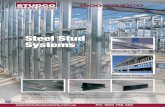
Trends in Overall Survival of MM
Overall survival 1971–2006 Diagnosis period Median OS1996–2006 45 months1971–1996 30 months
(P<0.001)
Kumar SK, et al. Blood. 2008;111:2516-2520. Time from diagnosis (Months)
Surv
ival
0
0.2
0.4
0.6
0.8
1.0
0 20 40 60 80 100 120 140
2001–2006
1995–2000
2001–2006
1989–1994
1983–1988
1977–1982
1971–1976
OS, overall survival.
2
M

CR and MM• Is CR an adequate surrogate for OS?
• Are all CRs as durable?
• Should we strive for CR pre-transplant?
• What is the role of HDCT for patients in CR pre-transplant?

CR associated with OS prolongation in post-induction and post-transplant settings1-3
1. Lahuerta et al. J Clin Oncol. 2008;26(3):5775-5782. 2. Alexanian et al. Bone Marrow Transplant. 2001;27:1037-1043. 3. Wang, et al. Bone Marrow Transplant. 2010;45(3):498-504.
Survival by response for 291 patients with MM (age <70 y) who received chemotherapy alone (left) and 375 who proceeded to ASCT (right) (CR vs PR or NR P<0.01)
Chemotherapy Alone Chemotherapy and ASCT
4

> 65 yrs
> 75 yrs
Importance of CR in Elderly MM
Gay F et al. Blood. 2011;117(11):3025-3031)

Approach to Treatment of MM
Clearly not a transplant candidate based on age, performance status
and comorbidity
Conventional Therapy
Potential transplant candidate
Non-alkylator based induction x 4 cycles
Stem cell harvest

Bortezomib-Based Induction Prior to SCT
Trial Regimen NCR+VGPR Post-Induction (%)
CR+VGPR Post-ASCT (%) PFS P Value
Cavo et al, 2010VTD
vsTD
236
238
62*
28
82*
64
68% at 3 yr
56% at 3 yr .0057
Moreau et al, 2011IFM 2007/02
VDvs
vTD
99
100
36
49‡
58
74§
Median 30 months
Median 26 mo .22
*P <.001; †P =.001; ‡P =.05; §P =.02GMMG= German Multiple Myeloma Group; SCT = stem cell transplant; CR = complete response; VGPR = very good partial response; PAD = bortezomib (V)/AD; T = thalidomide; VAD = vincristine, doxorubicin (A), dexamethasone (D); vTD = reduced-dose bortezomib.
Cavo M, et al. Lancet. 2010;376:2075-2085. Harousseau JL, et al. J Clin Oncol. 2010;28:4621-4629. Sonneveld P, et al. ASH Annual Meeting Abstracts. 2010;116(21):40. http://web.educationalconcepts.net/Newsletter/MMY015AE1/MMY015AE1.pdf. Accessed July 17, 2012. Moreau P, et al. Blood. 2011;118: 5752-5758.

Fayers PM et alBlood.2011;118(5):1239-1247
MPT vs MP in Elderly MM

Median survival:
MP 32.7 months (95% CI, 30.5-36.6 months)MPT 39.3 months (95% CI, 35.6-44.6 months).
HR 0.83 (95% CI: 0.73-0.94)P=0.004
Overall Survival

Palumbo et al. N Engl J Med 2012;366:1759-69.
MPR vs MP in Elderly MM

Study Regimen N ORR CR/nCR Outcomes
VISTASan Miguel et al.
Mateos et al.Phase III
VMPMP
344338
71%35%
33%4%
5 yr OS: 46%5 yr OS: 34.4%
UPFRONTNiesvizky et al.
Phase III
VMP/VelVTD/VelVD/Vel
30073%79%71%
31%36%34%
ORR: overall response rate; CR: complete response; nCR: near complete response; OS: overall survival; TTP: time to progression; PFS: progression free survival; VMP: Bortezomib-melphalan-dexamethasone; MP: Melphalan-Prednisone; VTP: Bortezomib-thalidomide-dexamethasone; VTD: bortezomib-thalidomide-dexamethasone; VD: bortezomib-dexamethasone; VMPT-VT: bortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance
Bortezomib in Transplant Ineligible MM

UPFRONT Study

MM-020: Len + Low-dose Dex vs MPT in Previously Untreated MM
Protocol CC-5013-MM-020/IFM 07-01. 2007; data on file, Celgene Corporation
Inclusion criteria•Previously untreated MM
•Age 65 years or not a candidate for transplantation
•No neuropathy of grade > 2
•CICr > 30 ml/min
• Lenalidomide 25 mg/day, days 1–21, every 28 days• Dexamethasone* 40 mg/day, days 1, 8, 15, 22, every
28 daysUntil PD
• Lenalidomide 25 mg/day, days 1–21, every 28 days• Dexamethasone* 40 mg/day, days 1, 8, 15, 22, every
28 days
18 four-week cycles or until PD
N = 1,590Centres in EU, Switzerland, USA and Canada
*In patients older than 75 years• Dexamethasone 20 mg/day• Thalidomide 100 mg/day• Melphalan 20 mg/kg/day
• Melphalan 0.25 mg/kg/day, days 1–4, every 42 days• Prednisone 2.0 mg/kg/day, days 1–4, every 42 days• Thalidomide* 200 mg/day, days 1–42, every 42 days
12 six-week cycles or until PD



Conclusions• Three drug induction regimen are associated with higher CR
rates compared to two drug regimen.• In the transplant eligible population prospective trials have
shown a higher CR rate and PFS for two drug regimen. Follow-up is too short for analyses of OS.
• In the transplant ineligible population three drug regimes of thalidomide and bortezomib have a OS advantage compared with MP. Whether non-melphalan containing two drug regime may be equivalent is the subject of ongoing trials.
• We have entered an era of risk stratification for deciding therapy. However no consensus has emerged on treatment paradigms.