Rath Barbara
17
1 Barbara Rath 2007 Differential Diagnosis of Fever Barbara Rath, M.D. University Children‘s Hospital Basel (UKBB) Barbara Rath 2007 DIFFERENTIAL DIAGNOSIS OF FEVER Where and how should we measure body temperature? What constitutes “normal temperature”? What constitutes “fever”? What causes fever? What is “Fever of Unknown Origin” (FUO)? Barbara Rath 2007 WHERE AND HOW SHOULD WE MEASURE BODY TEMPERATURE? Barbara Rath 2007 Thermoscope (Galileo Galilei, 1592): First instrument to measure temperature Barbara Rath 2007 Thermometer (Santorio Sanctorius, 1592) Barbara Rath 2007
description
ARTICLE FEVER CHILD NEONATES
Transcript of Rath Barbara

1
Barbara Rath 2007
Differential Diagnosis of Fever
Barbara Rath, M.D.University Children‘s Hospital Basel (UKBB)
Barbara Rath 2007
DIFFERENTIAL DIAGNOSIS OF FEVER
Where and how should we measure body temperature?
What constitutes “normal temperature”?
What constitutes “fever”?
What causes fever?
What is “Fever of Unknown Origin” (FUO)?
Barbara Rath 2007
WHERE AND HOW
SHOULD WE MEASURE
BODY TEMPERATURE?
Barbara Rath 2007
Thermoscope (Galileo Galilei, 1592):First instrument to measure temperature
Barbara Rath 2007Thermometer (Santorio Sanctorius, 1592)
Barbara Rath 2007

2
Barbara Rath 2007Curved thermometers for sublingual insertion (BMJ 1912;1:1137)
Barbara Rath 2007Benjamin Rush (1745-1813): A Moral Thermometer (1812)
Barbara Rath 2007
VARIATIONS IN SUBLINGUAL TEMPERATURE BY LOCATION
Difference max vs min = 0.9°C or 1.8°F Barbara Rath 2007
THE INFRARED AURAL THERMOMETER…TM thermometers…although convenient…tend to give highly variable readings that correlate poorly with simultaneously obtained oral or rectal readings. Mackowiak P A in: Mandel G L, Bennett J E, Dolin R (Eds) Principles and
Practice of Infectious Diseases, 6th Ed, 2005, pg 704
Once outstanding issues are addressed, the tympanic site is likely to become the gold standard for measuring temperature in children. El-RadhiA S, Barry W: Arch Dis Child 2006; 91: 351-356.
…infrared ear thermometry would fail to diagnose fever in three or four out of every ten febrile children (with fever…38°C or above). Dodd S R, et al: Clin Epidemiol 2006; 59: 354-57
ITT measurements more accurately reflect core temperatures than any other measurement site during febrile and nonfebrile periods in children.Nimah M M, et al: Pediatr Crit Care Med 2006; 7: 48-55.
Our findings suggests that infrared ear thermometry does not show sufficient agreement with an established method of temperature measurement to be used in situations where body temperature needs to be measured with precision. Craig J V, et al: Lancet 2002; 360: 603-609.
Barbara Rath 2007
DIFFERENTIAL DIAGNOSIS OF FEVER
Where and how should we measure body temperature?
What constitutes What constitutes ““normal temperaturenormal temperature””??What constitutes “fever”?
What causes fever?
What is Fever of Unknown Origin (FUO)?Barbara Rath 2007
WHAT IS NORMAL “BODY” TEMPERATURE?
35.7°C (96.2°F)
36.0°C (96.8°F)
36.5°C (97.7°F)
37.0°C (98.6°F)
37.5°C (99.5°F)
37.7°C (99.9°F)

3
Barbara Rath 2007
“NORMAL” CORE TEMPERATUREBest site(s) to determine true “normal” core temperature is:
Hypothalamic artery
Pulmonary artery
Rectum (5 cm)
Sublingual artery (oral)
Tympanic membrane
Temporal artery
Axillary artery
Skin (umbilicus)Barbara Rath 2007
NORMAL BODY TEMPERATURE?
Carl Rheinhold August Wunderlich: Das Verhalten der Eigenwärme in Krankenheiten (Leipzig,1868)
Analyzed ~million observations on ~25,000 adults22 cm long, mercury-in-glass thermometerUsed axillary site, twice daily, x15-20 minutes “Temperature oscillates even in health persons according to time of day by 0.5°C = 0.9°F”“Women have slightly higher normal temperatures than men and often show greater and more sudden changes of temperature”
Barbara Rath 2007
NORMAL BODY TEMPERATURE?
“When the organism (man) is in a normal condition, the general temperature of the body maintains itself at the physiologic point: 37°C = 98.6°F”
PROBLEM:Tests with one of Wunderlich’s thermometers suggest that his instruments may have been calibrated higher than today’s instruments by as much as 1.4° to 2.2°C.
* Mackowiak P A, Worden G: Clin Inf Dis 1994; 18: 458-67. Barbara Rath 2007
“NORMAL” ADULT ORAL TEMPERATURES
* Mean, Median: 98.2°FMackowiak P A et al: JAMA 1992; 268: 1578-80
37.0°C98.6°F
*
Barbara Rath 2007
“NORMAL” RECTAL TEMPERATURE HEALTHY INFANTS & CHILDREN
36.5° (0.2)97.8° (0.5)13 YEARS36.7° (0.2)98.0° (0.5)11 YEARS36.7° (0.2)98.1° (0.5)9 YEARS36.8° (0.2)98.3° (0.5)7 YEARS37.0° (0.2)98.6° (0.5)5 YEARS37.2° (0.2)99.0° (0.5)3 YEARS37.6° (0.2)99.7° (0.5)1 YEAR37.5° (0.3)99.5° (0.6)6 MOS37.4° (0.4)99.4° (0.8)3 MOS
37.5 ° (0.4)99.5° (0.8)< 3 MOS
AGE TEMPERATURE F° & C° (±SD)
Watson E H: Growth and Development of Children (1978); Herzog L W, Coyne L J: Clin Pediatr 1993; 32:Barbara Rath 2007
“Normal” “body” temperature is a range of values, affected by:
Age: Infant > child > adolescent, adult Sex: females > males (mean: 0.2°C, 0.3°F)Race: Black > Caucasian (mean: 0.1°C, 0.1°F)Time of day: afternoon > early morning Level of Activity: post-exercise > restingMeals: hot > cold; chewing, smoking Ambient temperaturePlacement within site of measurementDuration of measurement (Hg thermometers)Nature & calibration of device used

4
Barbara Rath 2007
TYPICAL DAILY TEMPERATURE FLUCTUATION (PO, ADOLESCENT)
Richardson G S, et al: Sleep 1982; 5 (Supp 2):S82 Barbara Rath 2007
NORMAL TEMPERATURES vs SITE
36.6° – 37.9°37.0° 98.6°RECTAL
35.5° – 37.5°36.6° 97.9°SUBLINQUAL
34.7° – 37.3°36.4° 97.5°AXILLARY
SITE MEAN RANGEC° F° C°
El-Radhi A S, Barry W: Arch Dis Child 2006; 91: 351-356
Barbara Rath 2007
Sund-Levander M, Forsberg C, Wahren LK. Normal oral, rectal, tympanic and axillary body temperature in adult men and women: a systematic literature review. Scand J Caring Sci 2002;16(2):122-8.
Barbara Rath 2007
DIFFERENTIAL DIAGNOSIS OF FEVER
Where and how should we measure body temperature?
What constitutes “normal temperature”?
What constitutes “fever”?
What causes fever?
What is “Fever of Unknown Origin” (FUO)?
Barbara Rath 2007
Sumerian (2500 BC): “inflammation”or “hot thing” meaning fever
Egyptian (1700 BC): “fever”
Chinese (2nd Century): “hot disease”
HISTORY OF FEVER
Barbara Rath 2007
Sumerian (2500 BC): “inflammation”or “hot thing” meaning fever
Egyptian (1700 BC): “fever”
Chinese (2nd Century): “hot disease”
HISTORY OF FEVER

5
Barbara Rath 2007
WHAT IS “FEVER”? PHYSIOLOGIC DEFINITION
A state of elevated core temperature which is often, but not necessarily, part of the defensive responses of multicellular organisms (host) to the invasion of live (microorganisms) or inanimate matter recognized as pathogenic or alien
- IUPS Commission for Thermal Physiology (2001)
Barbara Rath 2007
WHAT IS “FEVER”?CLINICAL DEFINITION
A pyrogen-mediated rise in body temperature above the normal range
Barbara Rath 2007
WHAT IS NOT “FEVER”?HYPERTHERMIA
A failure of thermoregulatory homeostasis due to uncontrolled heat production1, inadequate heat dissipation2, or defective thermoregulation3 leading to an unregulated rise in body temperature in which pyrogenic cytokines are not directly involved and against which standard antipyretics are generally ineffective.
1. Malignant hyperthermia, exercise, endocrine, drug (e.g. thyroxine)2. Neonates, bundling, heat stroke, drug (e.g. atropine)3. Neonates, CNS damage
Barbara Rath 2007
WHAT TEMPERATURE = “FEVER”?
≥37°C (98.6°F)
≥37.7°C (100°F)
≥38°C (100.4°F)
≥38.3°C (101°F)
≥39.1°C (102.4°F)
Barbara Rath 2007
Survey: 132 Pediatric Programs, 38 Emergency Medicine ProgramsBaraff L J: Management of the febrile child: A survey of pediatric and emergency medicine residency directors. Pediatr Inf Dis J 1991; 10: 795
What do Pediatric and ER Residents Think …?
Barbara Rath 2007
WHAT TEMPERATURE = “FEVER”?PEDIATRIC LITERATURE…
Rudolph’s Pediatrics The temperature most commonly used to define fever threshold in children is 38°C (100.4°F),rectal, although lower oral temperatures in adolescents and adults (37.2° - 37.8°C) may indicate a febrile response.
Textbook of Pediatric Emergency Medicine For the appropriately dressed child who has been at rest 30 minutes, rectal temperature of 38°C (100.4°F) is fever…

6
Barbara Rath 2007
WHAT TEMPERATURE = “FEVER”?& MORE PEDIATRIC LITERATURE….
Pediatrics (Osborn, DeWitt, First)The most commonly accepted minimum temperature defining fever is 38°C (100.4°F).
Current Pediatric Therapy …fever is defined as rectal temperature above 38°C (100.4°F).
Nelson’s PediatricsNo definition given
Barbara Rath 2007
WHAT TEMPERATURE = “FEVER”?THE PEDIATRIC ID LITERATURE
Principles and Practice of Pediatric Infectious DiseasesIn general, values higher than 37.8°C (100°F) are considered to be fever
Textbook of Pediatric Infectious DiseaseGenerally, the accepted range of rectal temperature is 36.1°C to 37.8°C (97°F to 100°F)..…Clearly, a body temperature slightly above an arbitrary upper limit of 37.8°C (100°F) does not always imply a pathologic process.
Pediatric Infectious Diseases. Principles and PracticeNo definition given
Barbara Rath 2007
WHAT TEMPERATURE = “FEVER”?THE JOURNALS….
Contemporary Pediatrics (1997)
Rectal temperature >38° C (100.4° F) Tympanic temperature >38° C (100.4° F) Oral temperature >37.8° C (100° F) Axillary temperature >37.2° C (99° F)
Berlin C W Jr: Fever in children. A practical approach to management
Barbara Rath 2007
Fever as an Adverse Event Following Immunization (AEFI)
Barbara Rath 2007
Fever as an AEFI – The Brighton Collaboration Case Definition
Fever is defined as the endogenous elevation of at least one measured body temperature of >= 38 C.
The value of >38C is accepted as reflecting an abnormal elevation of temperature, irrespective of device, anatomic site, age, or environmental conditions.
While it is recognized that this value is to some extent arbitrary, it is based upon a conservative interpretation of definitions proposed and used by clinicians, investigators, and the public at large.
S. Michael Marcy et al., Vaccine 2004; 22: 551-556
Barbara Rath 2007
“FEVER” vs “NORMAL” ADULT ORAL TEMP’S
* Mean, Median: 98.2°FMackowiak P A et al: JAMA 1992; 268: 1578-80
37.0°C98.6°F
*38° C
100.4° F

7
Barbara Rath 2007
INDIVIDUAL VARIATIONS AND THE DEFINITION OF FEVER
Statement:“She always runs a low temperature and 37.5° is a fever for her…”
Response:You will never convince the caregiver to the contrary, so work with it: There are no data to confirm or refute this observation.
Barbara Rath 2007
DIFFERENTIAL DIAGNOSIS OF FEVER
Where and how should we measure body temperature?
What constitutes “normal temperature”?
What constitutes “fever”?
What causes fever?What is “Fever of Unknown Origin” (FUO)?
Barbara Rath 2007
WHAT CAUSES FEVER?Sumerian (3000 BC)
Evil spirits (Nergal & Ashakka)Egyptian (1700 BC)
Demonic possessionChinese (1000 BC)
Imbalance of good and evilIndian (800 BC – 1000 AD)
Fire demons Takman & YakshmaDisturbances of the humours: bile, air, phlegm
Greek and Roman (400 BC – 200 AD)Excess of phlegm vs blood, yellow bile, black bileExcess of yellow bile vs phlegm, blood, black bile
Medieval (500 – 1350 AD)Demonic possession
Renaissance (1300 – 1600 AD)Fermentation and putrefaction in the blood and gut
18th CenturyFriction from blood rushing through the vessels; inflammation…..
Barbara Rath 2007
Barbara Rath 2007
Non-Infectious Causes
Hyperthyroidism
Hodgkin Disease
Pulmonary Infarction
Hypernephroma
Reginoal Ileitis
Aplastic Anemia
Leukemia
Fracture
Rheumatic Fever
Rheumatic Arthritis
Cerebral Hemorrhage
Drug Fever
Dermatomyositis
Bronchogenic CA
Myocardial Infarction
Pheochromocytoma
Periatrieritis Nodosa
Thrombophlebitis
Barbara Rath 2007
Meningitis
InfectiousMononucleosis
Tracheobronchitis
Pneumonia
Subphrenic Abscess
Infectious Exanthema
Appendicitis
Osteomyelitis
Septic Arthritis
Infectious causes…Cerebral Abscess
Sinusitis
Dental Abscess
Tuberculosis
Subacute BacterialEndocarditis
Empyema
Pyelonephritis
Diverticulitis
Prostatic Abscess
Cellulitis

8
Barbara Rath 2007
ANATOMY OF THERMOREGULATION
Mackowiak P A: Arch Int Med 1998; 158:1870-1881 Barbara Rath 2007
PATHOGENESIS OF FEVER
Mackowiak P A: Arch Int Med 1998; 158:1870-1881
Barbara Rath 2007
PATHOGENESIS OF FEVER
Mackowiak P A: Arch Int Med 1998; 158:1870-1881
Acetaminophen, Ibuprofen
Barbara Rath 2007
TRUE “NORMAL” CORE TEMPERATURE
Best site(s) to determine true “normal” core temperature is:
Hypothalamic artery
Pulmonary artery
Rectum (5 cm)
Sublingual artery (oral)
Tympanic membrane
Temporal artery
Axillary artery
Skin (umbilicus)
Barbara Rath 2007
DIFFERENTIAL DIAGNOSIS OF FEVER
Where and how should we measure body temperature?
What constitutes “normal temperature”?
What constitutes “fever”?
What causes fever?
What is “Fever of Unknown Origin” (FUO)?
Barbara Rath 2007
FUO IN CHILDRENFever of unknown originis characterized by daily fever persisting for more than 3 weeks.
infectious, rheumatologic disorders, and malignancy.
Chronic episodic fever of unknown originis characterized by fever lasting for a few days to a few weeks,
followed by a fever-free interval and a sense of well-being.
Mediterranean fever, the hyper-immunoglobulin D syndrome, familial Hibernian fever, Behcet disease, the syndrome of periodic fever, aphthous stomatitis, pharyngitis and adenitis, and cyclic neutropenia.

9
Barbara Rath 2007
FUO IN CHILDREN
Majeed HA. Curr Opin Rheumatol. 2000 Sep;12(5):439-44.
Barbara Rath 2007
FUO IN CHILDREN
Barbara Rath 2007 Barbara Rath 2007
Barbara Rath 2007
Know where to look!!!
Barbara Rath 2007
ALSO RULE OUT:
Hay FeverCabin FeverIsland FeverWorld Cup FeverSaturday Night Fever
10
Barbara Rath 2007 Barbara Rath 2007
ClinicalVignettes..
Barbara Rath 2007
CASE #1: NEONATE WITH FEVER
A 3 week old boy comes to your office because he slept through his noon feeding time, seems “sleepier than usual” to the parents, and had a rectal temperature of 38.1°C (100.6°F). Examination is entirely normal, including vital signs and temperature. He has a brisk, strong cry and good muscle tonus, but the cry is not sustained and he sucks only briefly on his bottle and then becomes quiet.
What else would you like to know or do?
Barbara Rath 2007
YOUR NEXT STEP IS….?
Admit, start antimicrobial Rx (cefotaxime + ampicillin
or ceftriaxone + ampicillin or gentamicin + ampicillin)
Admit, get lab studies, and start antimicrobial Rx
Admit, observe without lab studies or antimicrobials
Get lab studies and await results to decide if pt needs admission or can be followed from home
Barbara Rath 2007
LAB STUDIES YOU COULD ORDER ARE…?CBC and differentialUA/UCBlood cultureCSF analysis and cultureChest P-A & lateral radiographSedimentation rate (ESR)C-reactive protein (CRP)ProcalcitoninIL-6 or IL-8CD11b, CD64Granulocyte colony stimulating factor
Mishra U K, et al: Arch Dis Child Fetal Neonatal Ed 2006; 91: F208-F212Barbara Rath 2007
CASE #1: NEONATE WITH FEVER(CONT’D)
Lab results:
CBC: 7,600 WBC with 44N, 47L, 7M, 2E; Hgb 11/33
Cath UA: yellow, cloudy. Sp gr 1.010, pH 7.0. Sugar, protein, ketones, bili all neg. Hgb 1+, LE 1+, nitrite neg. Micro: WBC 10-25/HPF, bacteria “few”.
CSF: clear, 1 RBC, 4 WBC (2 PMNs), sugar 52, protein 69, Gram stain neg.
Chest film: normal
Two days later lab reports >100,000 E coli in the urine
11
Barbara Rath 2007
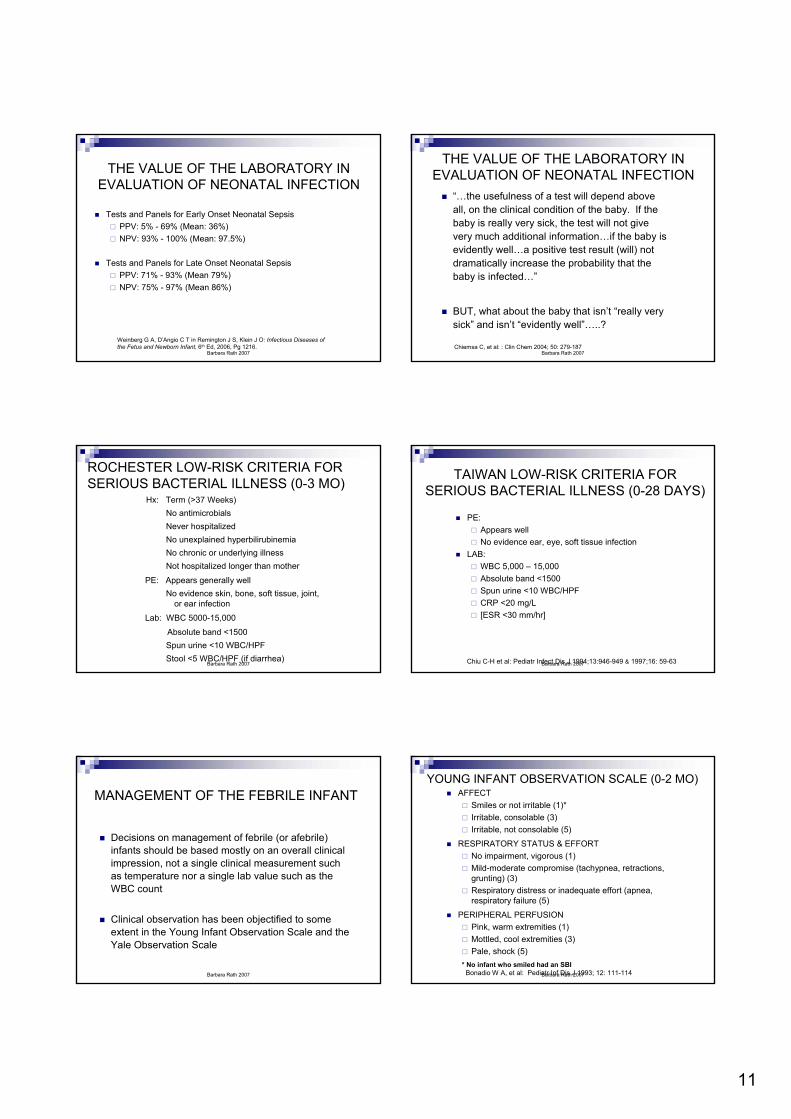
THE VALUE OF THE LABORATORY IN EVALUATION OF NEONATAL INFECTION
Tests and Panels for Early Onset Neonatal SepsisPPV: 5% - 69% (Mean: 36%)NPV: 93% - 100% (Mean: 97.5%)
Tests and Panels for Late Onset Neonatal SepsisPPV: 71% - 93% (Mean 79%)NPV: 75% - 97% (Mean 86%)
Weinberg G A, D’Angio C T in Remington J S, Klein J O: Infectious Diseases of the Fetus and Newborn Infant, 6th Ed, 2006, Pg 1216.
Barbara Rath 2007
THE VALUE OF THE LABORATORY IN EVALUATION OF NEONATAL INFECTION
“…the usefulness of a test will depend above all, on the clinical condition of the baby. If the baby is really very sick, the test will not give very much additional information…if the baby is evidently well…a positive test result (will) not dramatically increase the probability that the baby is infected…”
BUT, what about the baby that isn’t “really very sick” and isn’t “evidently well”…..?
Chiemsa C, et al: : Clin Chem 2004; 50: 279-187
Barbara Rath 2007
ROCHESTER LOW-RISK CRITERIA FOR SERIOUS BACTERIAL ILLNESS (0-3 MO)
Hx: Term (>37 Weeks)No antimicrobialsNever hospitalizedNo unexplained hyperbilirubinemiaNo chronic or underlying illnessNot hospitalized longer than mother
PE: Appears generally wellNo evidence skin, bone, soft tissue, joint,
or ear infection
Lab: WBC 5000-15,000
Absolute band <1500Spun urine <10 WBC/HPFStool <5 WBC/HPF (if diarrhea)
Barbara Rath 2007
TAIWAN LOW-RISK CRITERIA FOR SERIOUS BACTERIAL ILLNESS (0-28 DAYS)
PE:Appears wellNo evidence ear, eye, soft tissue infection
LAB:WBC 5,000 – 15,000Absolute band <1500Spun urine <10 WBC/HPFCRP <20 mg/L[ESR <30 mm/hr]
Chiu C-H et al: Pediatr Infect Dis J 1994;13:946-949 & 1997;16: 59-63
Barbara Rath 2007
MANAGEMENT OF THE FEBRILE INFANT
Decisions on management of febrile (or afebrile) infants should be based mostly on an overall clinical impression, not a single clinical measurement such as temperature nor a single lab value such as the WBC count
Clinical observation has been objectified to some extent in the Young Infant Observation Scale and the Yale Observation Scale
Barbara Rath 2007
YOUNG INFANT OBSERVATION SCALE (0-2 MO)AFFECT
Smiles or not irritable (1)*Irritable, consolable (3)Irritable, not consolable (5)
RESPIRATORY STATUS & EFFORTNo impairment, vigorous (1)Mild-moderate compromise (tachypnea, retractions, grunting) (3)Respiratory distress or inadequate effort (apnea, respiratory failure (5)
PERIPHERAL PERFUSIONPink, warm extremities (1)Mottled, cool extremities (3)Pale, shock (5)
* No infant who smiled had an SBIBonadio W A, et al: Pediatr Inf Dis J 1993; 12: 111-114

12
Barbara Rath 2007
EFFICACY OF LOW-RISK CRITERIA FOR EXCLUDING SERIOUS NEONATAL BACTERIAL INFECTIONS
Taiwan CriteriaPPV: 33.6%NPV: 99.2% (bacteremia/meningitis: 100%)
Afula CriteriaPPV: 32%NPV: 99.4%
Rochester CriteriaPPV: 27%*, 35%†, 12%‡
NPV: 94%*, 97%†, 99%‡
Young Infant Observation Scale (≥7)PPV: 37%NPV: 96%
* Ferrera P C, et al: Am J Emerg Med 1997; 15: 299-302† Gara G, et al: Acad Emerg Med 2005; 12: 921-925.‡ Jaskiewicz J A, et al: Pediatrics 1994; 94: 390-396 Barbara Rath 2007
Ooooooops……
11-month old male infant with 12 hr Hx low grade fever, irritability, intermittent crying. PE: alert, playful, smiling. Red pharynx, left TM red and bulging, flat fontanelle.
5 hrs later: T 39.9°C, increasingly lethargic, bulging fontanelle.
CSF cloudy, 8,200 WBC, sugar 45 mg%, protein 160 mg%, Gram-positive diplococci seen. Culture grew S pneumoniae penicillin-R
Baptist E C: Meningitis in the child with a smile. Arch PediatrAdolesc Med 1995; 149:1179
Barbara Rath 2007
CASE #2: FEVER IN AN 18-MONTH OLD
An 18-month old girl is brought to your office on a Thursday morning with a “fever for 4 days up to 103.8°F” by TM thermometer. Her parents tell you she first felt warm when being put to bed on Monday and since then has been more whiny, tires somewhat more easily than usual, appetite is off a bit, but she is otherwise active, alert, and generally unfazed.
ROS: Otherwise normal
PMH: Non-contributory. Immunizations up to date.
Family Hx: All well
Social Hx: No travel, friends are well.
Barbara Rath 2007
CASE #2: FEVER IN 18-MONTH OLD(CONT’D)
The enhanced urinalysis (hemocytometer count of unspun urine + Gram stain) was normal (no organisms and <10 cells/mm3). WBC: 6,400 with 74%L, 21%P, 5%M, 0E. Chest film was normal.The next day she still has a fever, but that afternoon the mother calls back concerned because a rash broke out. You tell her to bring the child in to see you.On PE you note a faint pink macular rash most prominent on the neck and trunk, slight on the face and extremities. The child is now afebrile. The mother has OCD and kept a q 4 hr record of her daughter’s temperatures…
Barbara Rath 2007 Barbara Rath 2007

13
Barbara Rath 2007
CASE #2: FEVER IN 3-36 MONTH OLD(CONT’D)
The most likely diagnosis is infection due to:HHV 6HHV 7Echovirus 16(Boston exanthem), 9, 11, 25, 27, 30Coxsackievirus A6, A9, B1, B2, B4, B5Adenovirus 1, 2, 3, 14Parainfluenza 1RotavirusParvovirus B19
Cherry J D in Feigin, Cherry, Demmler, Kaplan Eds): Textbook of Pediatric Infectious Diseases, 5th Edition, Pg 772. Barbara Rath 2007
Barbara Rath 2007 Barbara Rath 2007
Barbara Rath 2007 Barbara Rath 2007

14
Barbara Rath 2007
Krugman S, Katz SL, Gershon AA, Wilfert CM. Infectious diseases of children. 9th ed. St. Louis, Missouri: Mosby Year Book Inc. 1992.
Barbara Rath 2007
DOES TEMPERATURE MATTER?SIGNIFICANCE OF FEVER ≥41.1°C
Of no predictive value“Clinical assessment reliably identified those children with hyperpyrexia
and serious complications…and should be used to guide management decisions”Bonadio W A, et al: Pediatr Inf Dis J 1989; 8: 120-122
“Highly febrile young children … need to be evaluated as thoroughly and carefully as any other febrile child but do not merit special consideration.”Alpert G, et al: Pediatr Inf Dis J 1990; 9: 1611-63
“We advise treatment with antibiotics for all children with hyperpyrexia who do not have a confirmed viral illness and for all children with hyperpyrexia and a confirmed viral illness who are ill enough to require hospitalization”Trautner B W, et al: Pediatrics 2006; 118: 34-40
Barbara Rath 2007
DOES AGE MATTER? INCIDENCE OF SEVERE SEPSIS BY AGE
Angus DC, Linde-Zwirble WT, Lidicker J, Clermonte G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29:1303 10. Barbara Rath 2007
DOES AGE MATTER? MORTALITY DUE TO SEPSIS BY AGE
Girard TD, Opal SM, Ely EW. Insights into severe sepsis in older patients: from epidemiology to evidence-based management.
Clin Infect Dis 2005;40(5):719-27.
Barbara Rath 2007
DOES A HIGH WBC COUNT MATTER?Children 2-24 mo old (mean: 10 mo), 1992-1994, T≥38.5°C
Leukocytosis (LK): 15,000 – 24,999 (n = 94)Extreme leukocytosis (EL): ≥25,000 (n = 69)
Diagnoses
7%4.6%Other*2%1%Bacteremia6%2%Adenitis6%2%Aseptic meningitis5%7%Gastroenteritis13%12%UTI15%13%Pneumonia9%18%Viral Syndrome37%41%Otitis Media
Diagnosis LK ELProven SBI LK vs EL:17% vs 25%
Proven + ProbableSBI: 35% vs 52%
Hospitalized:
31% vs 49%
25,000-29,999:
RR SBI: 1.36
≥30,000:
RR SBI: 1.73
*Periorbital cellulitis (3), meningitis, cellulitis, mastoiditis, osteo, septic arthritis (1 each) Barbara Rath 2007
CASE #3: 16 YEAR OLD BOY WITH FEVER
A 16-year old boy comes to your office with his father who is concerned because the boy had a fever for several days, but today woke up with a fever to 40°C, flushed face, chills, vomited once, and even seemed a bit delirious about an hour before. He has been quite well otherwise except for an aching knee since he tripped and fell about a week ago.ROS: Otherwise non-contributoryPMH: Non-contributory
All immunizations, including meningococcal vaccine.Family Hx: All well, non-contributorySocial Hx: no travel, non-contributory. Friends are well

15
Barbara Rath 2007
CASE #3: 16 YEAR OLD BOY WITH FEVER(CONT’D)
PE: On examination you confirm the high fever, pulse of 132; BP 97/65; sick-looking young man. Sa02: 89%. Right knee is mildly swollen and faintly pink. Otherwise, PE normal without any rash, petechiae, or mucous membrane involvement.
Barbara Rath 2007
Barbara Rath 2007 Barbara Rath 2007
CASE #3: 16 YEAR OLD BOY WITH FEVER(CONT’D)
Labs & X-ray
WBC: 9700, 43% N, 28% B, 20% L, 9% M, toxic granulations noted; Hgb 15.3, Pl 120,000UA: 8-10 RBC / HPFESR: 85 mm/hr, CRP: 47D dimers (+), fibrin split products (+)ALT: 52, AST: 38Serum albumin: 2.43 g/dLNa: 125Creatinine 2.0; BUN 20Chest radiograph: bilateral nodular densities
Barbara Rath 2007 Barbara Rath 2007
SOME POSSIBLE ETIOLOGIES…
NEISSERIA MENINGITIDIS
GROUP A STREPTOCOCCUS
STAPHYLOCOCCUS AUREUS
SALMONELLA TYPHOSA
RICKETTSIA RICKETTSII
ERHLICHIA CHAFEENSIS
LEPTOSPIRA SPP

16
Barbara Rath 2007
CASE #3: 16 YEAR OLD BOY WITH FEVER
Pt started on ceftriaxone, vancomycin, gentamicinBlood culture grew out S aureus, methicillin-R
Severe staphylococcal sepsis in adolescents*90% with bone and/or joint infection90% with pulmonary septic emboli, pneumatocoeles, and/or parapneumonic effusions30% bacterial venous thrombophlebitis 50% Renal failureDICSkin lesions: urticaria, e multiforme, papular-pustular
* Gonzalez B E, et al: Pediatrics 2005; 115: 642-648Barbara Rath 2007
SCENARIO #4: “He’s had a fever, but he’s been teething...”
Signs and symptoms significantly associated 4 days before to 3 days after teething are:
Temp Elevation*Gum-rubbing
Ear-rubbingSucking
Appetite (solids)Rash on face
WakefulnessDrooling
IrritabilityBiting
*Day of emergence vs before: 17% vs 12% >100°F; 6% vs 3% >101°FMacknin M L, et al: Pediatrics 2000; 105:747-752
Barbara Rath 2007
Teething and Fever (Cont’d)
Mean daily temp before 1st tooth eruption
Temp >37.5°C by day before tooth eruption,46 infants, 15 with temp ≥38°C
Jaber L, et al: Arch Dis Childh1992; 67:233 Barbara Rath 2007
Scenario #5: “His temperature was around 39°…”
- Fever Detection by Palpation
~60% of parents use palpation as the usual method of fever assessment
85% - 99% believe they can detect fever by palpation
Actual accuracy of parental palpation for fever:Sensitivity: 77%1, 84%2, 90%3 , 74%4
Specificity: 82%, 76%, 78%, 86%Positive predictive value: 59%, 72%, 69%, 71%Negative predictive value: 85%, 91%, 91%, 94%
1. Katz-Sidlow R, et al: Ped Acad Soc Meeting; May 2, 2006; 2. Graneto J W, Soglin D F: Ped Emerg Care 1996; 12: 183-184; 3. Ernst T N, Philp M: Amer J Dis Child 1985; 139: 546; 4.Banco L, Veltri D: Amer J Dis Child 1984; 138; 976-978.
Barbara Rath 2007
Scenario #5: “His temperature was around39°..”*
If it is important to know the real temperature (and it may not be) ask:
Where did you take the temp?What kind of thermometer did you use?How long did you leave it in place?Around? Was it below 39° or above?
* Translation: “I’m worried and I want you to worry too.”Barbara Rath 2007
ANXIOUS PARENTS170 parents of young febrile children who presented to a pediatric emergencydepartment (ED) with fever; 90-item questionnaire (State Trait Anxiety Inventory)
Parents were asked what they had previously thought about and how they feltabout the ED process.
Mean parental anxiety was 50.1 (95% CI 48.1, 52.2), significantly elevated fromadult standards (p < 0.0001). A multivariate model comprising:
(1) feeling "not at all" well rested, (2) having no other children, (3) having thought about a blood test, and (4) feeling worried about trusting the physician
was associated with elevated anxiety.
In conclusion, parents of febrile young children in the ED are very anxious.
Parkinson GW, Gordon KE, Camfield CS, Fitzpatrick EA. Anxiety in Parents of Young Febrile Children in a Pediatric Emergency Department: Why is it Elevated? Clinical Pediatrics 1999;38(4):219.

17
Barbara Rath 2007
SUMMARY
“Normal body temperature” varies widely
“Fever” can be arbitrarily defined as a temp of ≥38°C (100.4°F) at any site using any approved instrument
Teething may be associated with minimal elevation in temperature
Palpation is not an accurate way to determine presence of fever,but it’s not bad for its absence
Barbara Rath 2007
SUMMARY
Overall clinical impression, supported by laboratory or imaging studies, rather than height of temperature or abnormal lab values alone, should be the major determinant for deciding whether or not a child has a serious bacterial illness….
Barbara Rath 2007
Acknowledgements
S MICHAEL MARCY, MDCLINICAL PROFESSOR OF PEDIATRICS
UNIVERSITY OF CALIFORNIA LOS ANGELESUNIVERSITY OF SOUTHERN CALIFORNIA
SCHOOLS OF MEDICINE
Team Lead, Brighton Collaboration Fever Working Group, Member, Brighton Collaboration Steering Committee