Rapid Sequence Intubation Joshua Rocker, MD Pediatric Emergency Medicine Schneider Children’s...
36
Rapid Sequence Rapid Sequence Intubation Intubation Joshua Rocker, MD Joshua Rocker, MD Pediatric Emergency Pediatric Emergency Medicine Medicine Schneider Children’s Schneider Children’s
-
Upload
matilda-ball -
Category
Documents
-
view
233 -
download
0
Transcript of Rapid Sequence Intubation Joshua Rocker, MD Pediatric Emergency Medicine Schneider Children’s...
Rapid Sequence Rapid Sequence IntubationIntubation
Joshua Rocker, MDJoshua Rocker, MD
Pediatric Emergency MedicinePediatric Emergency Medicine
Schneider Children’s HospitalSchneider Children’s Hospital
What is it?What is it?
What is it?What is it?
NPO status is unknownNPO status is unknown Meds same but precautions Meds same but precautions
increasedincreased
Cricoid pressureCricoid pressure Try not to Bag Try not to Bag

Why intubate?Why intubate?
Airway ProtectionAirway Protection– GCS <8, lack of gagGCS <8, lack of gag
Control CO2Control CO2– Head InjuryHead Injury
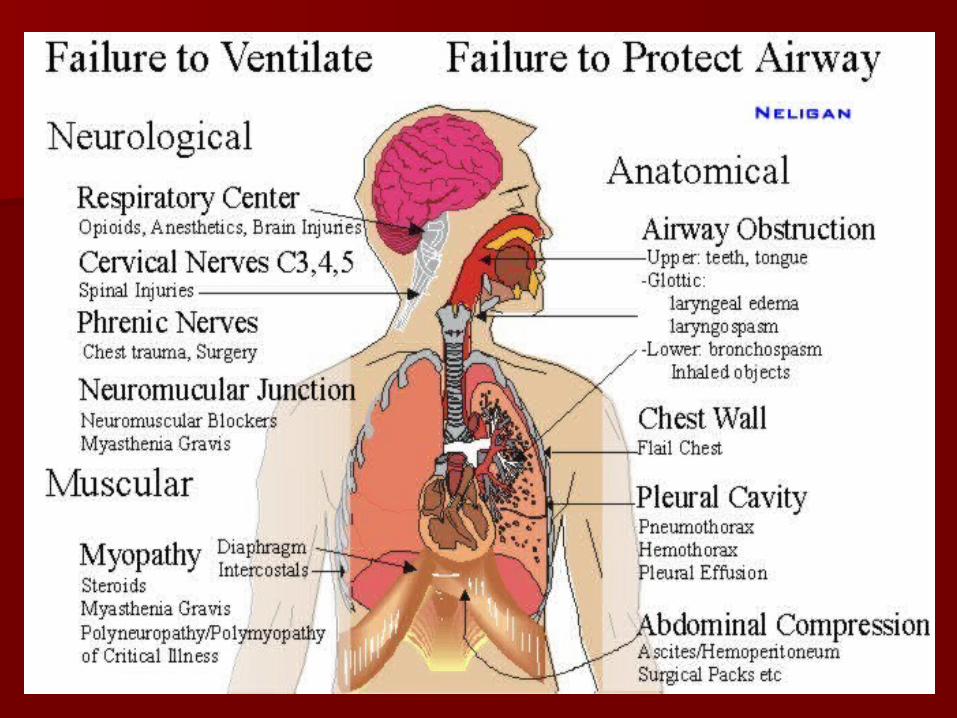
Decrease work of breathingDecrease work of breathing Bronchopulmonary ToiletBronchopulmonary Toilet Failure to OxygenateFailure to Oxygenate Failure to VentilateFailure to Ventilate
But before we intubate…But before we intubate…
Have we exhausted our options…Have we exhausted our options…
AdjuvantsAdjuvants– CPAPCPAP– BiPAPBiPAP– Oral-pharyngeal AirwayOral-pharyngeal Airway– Nasal-pharyngeal AirwayNasal-pharyngeal Airway– LMALMA
RSI Check ListRSI Check List
Patient Airway EvaluationPatient Airway Evaluation PreparationPreparation PersonnelPersonnel Pre-oxygenationPre-oxygenation Pre-medicationPre-medication Suction / SedativeSuction / Sedative ParalyticParalytic
6Ps and 2Ss

Patient Airway EvaluationPatient Airway Evaluation
Facial, cervical or neck traumaFacial, cervical or neck trauma Short neck, micrognathia, dysmorphic Short neck, micrognathia, dysmorphic
facial features, low set earsfacial features, low set ears Limited mouth opening, small mouth, Limited mouth opening, small mouth,
large tongue or loose teethlarge tongue or loose teeth Stridor, history of obstructive sleep Stridor, history of obstructive sleep
apnea or loud snoringapnea or loud snoring Previous traumatic attempts at Previous traumatic attempts at
intubationintubation Mallampati classification class III-IVMallampati classification class III-IV

Patient Airway EvaluationPatient Airway Evaluation
Mallampati classificationMallampati classification
PreparationPreparation
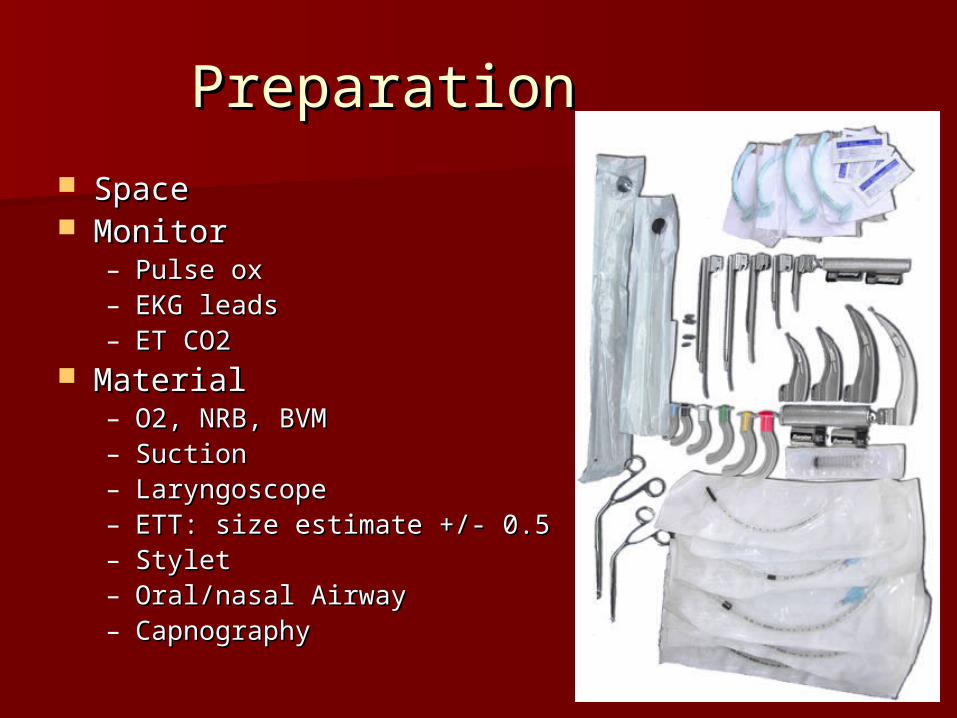
SpaceSpace MonitorMonitor
– Pulse oxPulse ox– EKG leadsEKG leads– ET CO2ET CO2
MaterialMaterial– O2, NRB, BVMO2, NRB, BVM– SuctionSuction– LaryngoscopeLaryngoscope– ETT: size estimate +/- 0.5ETT: size estimate +/- 0.5– StyletStylet– Oral/nasal AirwayOral/nasal Airway– CapnographyCapnography
PersonnelPersonnel
Medication AdministrationMedication Administration Cricoid PressureCricoid Pressure Watching monitor/patientWatching monitor/patient
Paralyzing? Paralyzing? – Make sure someone who can handle Make sure someone who can handle
difficult intubations or who can get an difficult intubations or who can get an emergency airway is around!!!!!!emergency airway is around!!!!!!
Pre-OxygenatePre-Oxygenate
100% NRB100% NRB– Make sure connectedMake sure connected– Make sure reservoir inflatedMake sure reservoir inflated
Avoid BVMAvoid BVM
Pre-medicatePre-medicate
AtropineAtropine– Prevent Vagal responsePrevent Vagal response– Reduce secretionsReduce secretions
LidocaineLidocaine– Blunt Increase in ICPBlunt Increase in ICP
SuctionSuction
SecretionsSecretions Vomitus/FoodVomitus/Food
SedateSedate
Opiates (Fentanyl)Opiates (Fentanyl)– Chest wall rigidityChest wall rigidity
EtomidateEtomidate– Myoclonus, adrenal suppressionMyoclonus, adrenal suppression
KetamineKetamine– laryngospasm., secretions, sympathomimeticlaryngospasm., secretions, sympathomimetic
BenzodiazepinesBenzodiazepines BarbituatesBarbituates PropofolPropofol

ParalyticParalytic
DepolarizingDepolarizing– SuccinylcholineSuccinylcholine
Fasciculations, hyperkalemia, malign Fasciculations, hyperkalemia, malign hyperthermia, MGhyperthermia, MG
Non-depolarizingNon-depolarizing– RocuroniumRocuronium– VecuroniumVecuronium– PancuroniumPancuronium– AtracuriumAtracurium

ScenariosScenarios
ScenariosScenarios
Head traumaHead trauma– Concern of Increased Intracranial Concern of Increased Intracranial
pressure (ICP)pressure (ICP) Pre-medicatePre-medicate
– Lidocaine Lidocaine SedationSedation
– Avoid: Ketamine (Incr ICP)Avoid: Ketamine (Incr ICP)– Avoid: Benzo, Barbit (possible hypotension)Avoid: Benzo, Barbit (possible hypotension)
Thiopental- Cerebral protectiveThiopental- Cerebral protective ParalysisParalysis
– Avoid: Succinylcholine (fasciculations)Avoid: Succinylcholine (fasciculations)
Head TraumaHead Trauma
LidocaineLidocaine– Theoretically blunts ICP responseTheoretically blunts ICP response
Cough suppressionCough suppression Brain stem depressionBrain stem depression Decreased cerebral metabolismDecreased cerebral metabolism Cell membrane stabilizationCell membrane stabilization
– Not well demonstrated in human studies Not well demonstrated in human studies and still controversial and still controversial
ScenariosScenarios
Asthmatic Asthmatic – SedationSedation
KetamineKetamine– BronchodilatorBronchodilator– SE: laryngospasm SE: laryngospasm
Chances increased if history of asthma or mild Chances increased if history of asthma or mild symptomssymptoms
BUT if paralyzing no issues, just be awareBUT if paralyzing no issues, just be aware
ScenariosScenarios
Shock/HypotensionShock/Hypotension– SedationSedation
BenzodizapinesBenzodizapines– May cause hypotensionMay cause hypotension
BarbituatesBarbituates– May cause hypotensionMay cause hypotension
KetamineKetamine– CV stimulantCV stimulant
EtomidateEtomidate– CV neutralCV neutral

CasesCases
Case 1Case 1
14 y/o in MVA comes in with GCS of 6 14 y/o in MVA comes in with GCS of 6 with gross deformity of R femur and with gross deformity of R femur and a taught belly. HR-125 BP-94/55 a taught belly. HR-125 BP-94/55 Pulse ox- 94%.Pulse ox- 94%.
What to do?What to do?
Case 1Case 1
14 y/o in MVA comes in with GCS of 6 14 y/o in MVA comes in with GCS of 6 with gross deformity of R femur and with gross deformity of R femur and a taught belly. HR-125 BP-100/75 a taught belly. HR-125 BP-100/75 Pulse ox- 94%.Pulse ox- 94%.
What to do?What to do?
NEURO-INTUBATIONNEURO-INTUBATION
What meds should I use?What meds should I use?
A. Ketamine, RocA. Ketamine, Roc B. Ketamine, Lidocaine, RocB. Ketamine, Lidocaine, Roc C. Etomidate, Lidocaine, RocC. Etomidate, Lidocaine, Roc D. Etomidate, Atropine, Lidocaine, D. Etomidate, Atropine, Lidocaine,
RocRoc E. Propofol, Lidocaine, RocE. Propofol, Lidocaine, Roc
Case 2Case 2
3 y/o asthmatic with hx of 3 previous 3 y/o asthmatic with hx of 3 previous intubations presents in respiratory intubations presents in respiratory distress. Sat 75%. Tachypneic to 65 distress. Sat 75%. Tachypneic to 65 with grunting. Obtunded.with grunting. Obtunded.
What meds should I use to What meds should I use to intubate?intubate?
A. Roc and SuccA. Roc and Succ B. Versed and EtomidateB. Versed and Etomidate C. Etomidate and RocC. Etomidate and Roc D. Ketamine and AtropineD. Ketamine and Atropine E. Ketamine and Atropine and RocE. Ketamine and Atropine and Roc

Case 3Case 3
6 mo old male with fever for 3 days 6 mo old male with fever for 3 days and purpuric rash has a pulse of 60 and purpuric rash has a pulse of 60 and a BP of 50/palp. and a BP of 50/palp.
SO…SO…

What meds now?What meds now?
A. Etomidate and AtropineA. Etomidate and Atropine B. Atropine, Ketamine and RocB. Atropine, Ketamine and Roc C. Atropine, Etomidate and VersedC. Atropine, Etomidate and Versed D. Versed, Fentanyl and SuccD. Versed, Fentanyl and Succ E. Motrin, Tylenol and MiralaxE. Motrin, Tylenol and Miralax
Case 4Case 4
17 y/o involved in MVA, his body was 17 y/o involved in MVA, his body was ejected through the windshield head ejected through the windshield head first. He has a weak pulse with a first. He has a weak pulse with a 70/palp BP. His face anatomy is 70/palp BP. His face anatomy is distorted and his L globe is clearly distorted and his L globe is clearly ruptured. ruptured.
Ouch…Ouch…
Next?Next?
Next?Next?
Lung exam and Tracheal positionLung exam and Tracheal position– Pneumothorax?Pneumothorax?– Hemothorax?Hemothorax?– Pneumohemothorax?Pneumohemothorax?– Tension pneumothorax?Tension pneumothorax?
His exam is normal…His exam is normal…
What to do next?What to do next?
A. Oral intubationA. Oral intubation B. Nasal intubationB. Nasal intubation C. Wait for back-upC. Wait for back-up D. Surgical AirwayD. Surgical Airway E. Soil yourself and then do surgical E. Soil yourself and then do surgical
airwayairway F. Do surgical airway, then soil selfF. Do surgical airway, then soil self

Case 5Case 5
3 mo old presents DOA. 3 mo old presents DOA. Temperature is 34 degrees Celsius. Temperature is 34 degrees Celsius. Rigor Mortis has set in.Rigor Mortis has set in.
What do I intubate with?What do I intubate with?
A. No meds neededA. No meds needed B. Atropine, SuccB. Atropine, Succ C. Epi onlyC. Epi only D. Propofol and RocD. Propofol and Roc

ThanksThanks
Any questions...Any questions...