
Rapid Diagnostics: A Foundation for the Appropriate Use...
39
Geraldine S. Hall, PhD., D(ABMM), F(AAM) Forestville, New York June 16, 2015 Rapid Diagnostics in Clinical Microbiology as an Aid to Antibiotic Stewardship
Transcript of Rapid Diagnostics: A Foundation for the Appropriate Use...

Geraldine S. Hall, PhD., D(ABMM), F(AAM)Forestville, New YorkJune 16, 2015
Rapid Diagnostics in Clinical Microbiology as an Aid to
Antibiotic Stewardship

Objectives
Describe the impact of existing and novel methods available for the rapid detection of bacteria.
Provide possibilities for the integration of rapid methods in the laboratory as opportunities to improve antimicrobial use and clinical and economic outcomes
Explore the impact of existing and novel methods possible for the rapid determination of antibiotic susceptibility

Conventional Methods for Microbiologic Testing: ID
Identification
Manual Biochemical Testing Continuous monitoring BC machines Screening of Urine Specimens Automated (semi-automated) identification systems
o Vitek (bioMerieux, Inc)o MicroScan ( Beckman Coulter)o BD Phoenix (Becton Dickinson)o VersaTrek (Thermofisher Scientific)o Biolog (Hayward, CA)o Other
Often requires at least 24 hrs before results are available

Manual methods for Susceptibility testing Disk Diffusion E-Test MIC Trays
Automated (semi-automated) Methods for Susceptibility Testing Vitek MicroScan BD Phoenix VersaTrek Other
Conventional Methods for Microbiologic Testing: Antimicrobial Susceptibility Testing
(AST)
Requires isolated colonies; usually performed after the identification is completed; typically requires at least 48 hrs

Better outcomes for the Patient
• Lowered Mortality Rates• Use of appropriate, targeted antibiotics earlier• Less chance for more infections
MRSA C. difficile
Lowered Costs for the Patient
• Less time in the hospital• Fewer additional tests• ? Fewer antibiotics, therefore fewer adverse reactions as a possibility
Reduced Length of Stay (LOS) in the hospital
Less development of antibiotic resistance
Why are Rapid Microbiologic Results Needed?

Identification and Susceptibility Testing for:
• Blood Cultures
• CSF and other sterile sites
• Pneumonia
• Wounds
• Urine Cultures
• Sexually Transmitted Diseases
• Other
When are Rapid Microbiologic Results Needed?

Doern, GV et al. 1994. JCM 32: 1757-62 Semi-automated ID/AST systems vs. overnight
o ID in 9.6 hr vs. 19.6 hro AST in 11.3 Hr vs. 25.9 hr
LOS was the same, but mortality was lower with rapid results, 8.8 vs 15.3%
Fewer lab studies ordered Less time for appropriate antibiotics
Supporting Evidence that Rapid Makes a Difference: Older Data
Barenfanger, JE et al. 1999. JCM 34: 208-9 Evening shift verified VITEK results for ID and AST LOS was 10% with rapid vs 12% with conv. Mortality was 7.9% with rapid vs 9.6% with conv. $4,927 per patient with rapid vs. $6,677 with conv. Estimated saving $4 million per year

Beekman, SE et al. 2003. JCM 41: 3119-25. 917 blood cultures; most were SA, E. coli and CNS
• Collection of blood culture to Gram stain was 27.6 hr Continuous monitoring systems
• Time to notification significantly improved –LOS for patient with BSI–LOS after diagnosis of BSI
Barenfanger, J et al. 2008. Am J Clin Path 130: 870-6. Staining and reporting of positive Blood Cultures
• <1 hr TAT: reported in 0.1 hr; 10% mortality• > 1 hr TAT: reported in 3.3 hr; 19% mortality
Supporting Evidence that Rapid Makes a Difference: Older Data

What are the newer methods for identification?
1. MALDI-TOF
2. Sequencing
3. Direct Specimen Testing
• Probes
• NAAT
4. Other

What are the newer methods for AST?
Detection of Resistance markersVerogeneCepheid XpertMRSA using GenOhmOther
Some questions as to whether genotypic (molecular) detection will = phenotypic results

How Can One Employ Rapid Diagnostics for BSI?
1. Direct testing from a positive BC:
FISH probes MALDI-TOF Rapid MRSA testing Verigene Film Arrays
2. Direct testing from whole blood:
Out of U.S. presently:• Light Cycler Septic FAST (Roche;
broad range PCR; IVD)– Guido M et al. 2012. J Prev Med
Hyg 53: 104-8. • SestiTest (Germany; homebrew) Leitner E and Kessler HH. 2015. Meth Mol
Biol . 1287: 129-38
– Research in US• T2 Candida Neyda ND et al. 2013; DMID 77: 324-6.

Antibiotic Stewardship
Multi-faceted approach to optimize the use of antibiotics while minimizing the development of resistance and other adverse effects
Good stewardship practices (GSP) is an active and dynamic process of continuous improvement on antibiotic use — an ethic with many steps of different sizes by all involved in antibiotic use.
Prior term used: prudent antibiotic use
Stewardship = acceptance for responsibility for long-term management of something of enormous value.

Do Resistant Organism Infections Cost More Than Susceptible Organism Infections?
MRSA, VRE, K. pneumoniae (CRE), P. aeruginosa (FQ-R),
A. baumannii (Amp/sulbactam-R)
Resistant organisms: 7 d increase in LOS; even after confounding variables were removed = 1 d less
Resistant organisms: $70,000 increased charges; even after confounding variables removed = $8000.
Death rate was higher for HAI caused by VRE or KP (CRE) as compared to CA-acquired; pneumonia and UTI were also cause of higher death rates
CA-VRE resulted in $69,000 higher charges than VSE Nerdell et al. 2002. CID 55: 807-15
Healthcare Infection Control Practices Advisor Committee, in partnership with US DHHS, listed Antimicrobial Stewardship as one of top 5 messages for healthcare workers in 2009.
MRSA infections were listed as 1 of the 6 categories of healthcare associated infections for its 5 year “National Prevention Target.”Cost of SA bacteremia: $20,000 - $70,000/episode
Antibiotic Stewardship

Good Stewardship Practices in Clinical Microbiology
Antimicrobial use guidelines/categorization Voluntary restriction policies Formularies Stop orders (test utilization) Education Regulation of access to antibiotics Dealing with COI issues Implementation of good Infection Control Practices
Prescott JF et al, 2014; Vet Microbiol 171: 273-8.

Who should be involved in AS
Infectious Disease clinicians Clinical Microbiologists ID Pharmacists Infection Control Practitioners Patients Industrial colleagues
o Medical Device/Instrumentso Pharmaceutical Industry
How Do We Provide Rapid Results?
Communicate best methods for specimen collection
Use methods that will provide quickest and most accurate results for: Gram Stain ID Susceptibility Serology/antigen testing Direct specimen testing
Communicate results as quickly as they are completed: By phone By email Electronically on lab information systems All of above

Rapid Diagnostics, Bloodstream Infections and AS
Mean decrease in survival of 7.6% for each hour after onset of hypertension until effective antibiotics are on board
Use of inappropriate antibiotics within first 6 hrs after recognition of septic shock is associated with a 5-fold increase in mortality rate
SO ------ answer will be “broad spectrum antibiotics” which will further increase antibiotic resistance
Kothari A et al. 2014. CID 59:72-8.
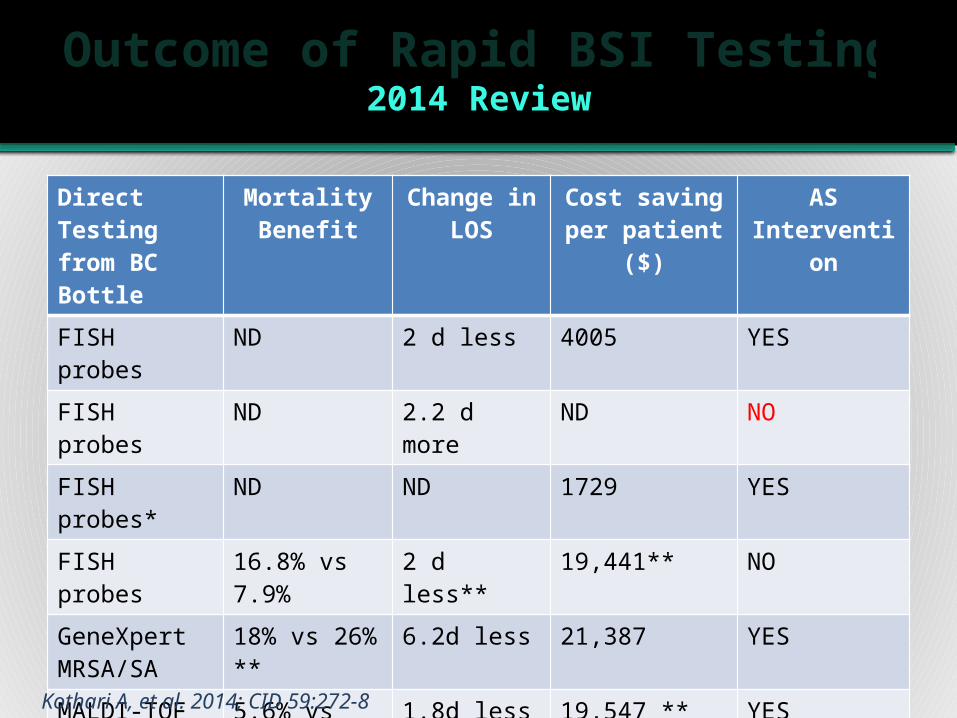
Outcome of Rapid BSI Testing2014 Review
Direct Testing from BC Bottle
Mortality Benefit
Change in LOS
Cost saving per patient ($)
AS Intervention
FISH probes ND 2 d less 4005 YES
FISH probes ND 2.2 d more ND NO
FISH probes* ND ND 1729 YES
FISH probes 16.8% vs 7.9% 2 d less** 19,441** NO
GeneXpert MRSA/SA
18% vs 26% ** 6.2d less 21,387 YES
MALDI-TOF 5.6% vs 10.7%**
1.8d less 19,547 ** YES
MALDI-TOF 12.7% vs 20.3% 2.8 d less ** ND YES
Verigene # NO 21.7d less 60,729 YES* = Yeast only; ** = difference was not statistically significant; # = enterococci
Kothari A, et al. 2014; CID 59:272-8

MRSA Bacteremia and Rapid Testing
Xpert MRSA/SA compared to conventional methods at OSU, employing partnership of Microbiology, Epidemiology, Pharmacy, Infection Control and Infectious Diseases:
o LOS: 6.2 d less with rapid methodso $21,387 less in patient costso 100% sensitivity and specificity as compared to the conventional method
ID Pharmacist was essentialo Bauer KA, et al. 2014. CID 51: 1074-80.

GNB Antibiotic Resistance and VAP: Predictors of Mortality?
76 patients, mainly infected with P. aeruginosa— 19 died within 30 days; underlying conditions:
o Coronary heart diseaseo Vasopressors o ICU diagnosis of sepsis/pneumoniao Received appropriate dose of antibiotics > 24 hr after BAL performed
(Kollef, KE et al. 2008; CHEST 134: 281-7)
E-test used directly on clinical specimens vs conventional AST testingo 1.4 d vs. 4.2 d for resultso Fewer days of fevero Fewer days of antibiotics before resolution of VAPo Lower antibiotic costso Less C. difficile
(Bouza E et al. 2007; CID 44: 382-7.

Newer Technologies and Rapid Antibiotic Susceptibility Testing
Imaging Techniques• BACcel (Accelr8 or Accelerate ID/AST; RUO; Tucson, AZ)) : use in
positive Blood Culture Bottles
Fluorescence Activated Cell Sorting (FACS)• Alone or in combination with microfluidics to distinguish cellular size
and shapes.• Fluorescent stains can distinguish “dead” from “living “ cells
Microbial Cell Weighing by Vibrating Cantilevers
Micro-calorimetry

Newer Technologies and Rapid AST (cont)
Rotating Magnets
RNA Sequencing
Testing in Microdroplets
Bacteriophage Susceptibility• Adaptations for TB testing in past
OTHER
Van Belkum et al. Ann Lab Med 2013; 33:14-27

Will Rapid Diagnostics Alone Reduce Antibiotic Resistance?
NO----also need: Better understanding of emergence and speed of
resistance Significant development of new antibiotics Sharing of global surveillance data Increase development of technical needs for our
technologists• Large scale data management• Bioinformatics• Communications
What About Other Body Sites and Rapid Testing: Urine?
Available urine screening methods with limited success/acceptance:
• Gram stain• Dip sticks for nitrates and wbc’s• Instruments that can enumerate microbes in broth rapidly
Reason for urine screen?• Provide rapid indication that microbe count exceeds threshold (104-105 cfu/ml)
• Reduce number of urines that need to be plated and read Save personnel time and money Use of appropriate antibiotics sooner Reduce use of antibiotics if screen not positive
UTI in a hospitalized patient is most often source of subsequent BSI


Operation Principle
27
Forward Laser Scattering combined with Optical Density = sensitivity below 104 to above 1010 cfu/mL
Bacteria growth imaging:

UTI Screening Clinical Study Design
Rambam Healthcare Campus, a 1000-bed tertiary Israeli hospital
BacterioScanTM 216R, two CHROMagarTM plate cultures, dipstick analysis and microscopy had been performed
2400 samples from a diverse population, hospital wards and collection methods were analyzed
Objective: quantitatively com-pare performance of various rapid screening techniques with plate culture
0 50 100 15010
3
104
105
106
107
108
109
Incubation time [min]
Con
cent
ratio
n ch
ange
[cfu
/ml]
Chromagar plate 1 Chromagar plate 2
Dipstick
Microscopy
BacterioscanTM 216R
Vitek 2
Clinitek Status

(a) Exemplary growth curves for various Gram positive, Gram negative bacteria and negative samples
(b) Additional output from BacterioScan 216R showing Optical Density and mean size of the bacteria for two coagulase negative Staphylococcus species.
Urine Screening with BacterioScan
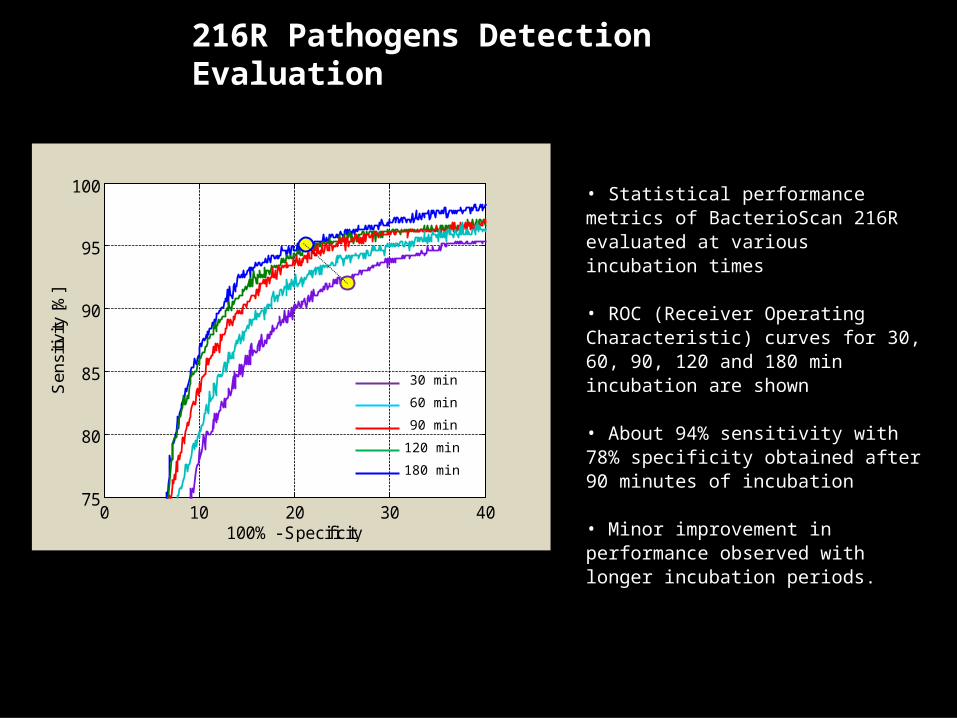
216R Pathogens Detection Evaluation
• Statistical performance metrics of BacterioScan 216R evaluated at various incubation times
• ROC (Receiver Operating Characteristic) curves for 30, 60, 90, 120 and 180 min incubation are shown
• About 94% sensitivity with 78% specificity obtained after 90 minutes of incubation
• Minor improvement in performance observed with longer incubation periods.
0 10 20 30 4075
80
85
90
95
100
100% - Specificity
Sen
sitiv
ity [%
]
30 min 60 min 90 min120 min180 min

Summary:All Evaluated Rapid Techniques
Sensitivity 86% 86% 37% 95%Specificity 94% 78% 97% 80%
NPV 94% 96% 83% 98%PPV 86% 46% 80% 62%
Accuracy 92% 79% 83% 84%
Agar Plate Culture
Microscopy
Rapid Screening Test
Dipstick BacterioScan 216R
Optical Density Changes for the Rapid Detection and AST of Microbes
Use of a laser scatter instrument to measure changes in E. coli (concentrations simulating a UTI) when exposed to varying concentrations of ciprofloxacin
Model 224R BacterioScan, St. Louis, MO) 37 °C; measurements made over 5 hr. Starting concentration of E. coli of ~ 3 X 104 CFU/ml broth
Successful at measuring the growth rate with repeatability of +/- 10% and 3-min time resolution
Ability to approximate a nominal MIC within 90 min
MIC in instrument: between 0.004 and 0.008 μg/ml compared to CLSI QC results for the E. coli of 0.004 to 0.015 μg/ml.
Marshall D et al. Poster at ASM Biodefense and Emerging Diseases Research Conference, Jan 2014.

Use of BacterioScan for Sepsis Detection and AST
1. Donor blood was seeded with E. coli (1.5 X 105 cfu/ml) and 10 ml placed into BACTEC BC bottles; incubated until machine detected a pos (+)
2. 4 aliquots removed from each of aerobic and anaerobic bottles:• 1 tube not further processed• 1 tube filtered• 1 tube centrifuged• 1 tube lysed
3. 2 μl of each sample was diluted (1000:1) and added to MHB with ciprofloxacin and measurements made over 5 hr
Anbazhagan R et al. Poster submitted to ICAAC 2015.
Results: Growth was detected and an accurate phenotypic MIC was obtained within 3 hr after BC bottle was deemed positive.


Clinical Microbiology is Changing (Beavers T and JG Wheeler. 2010. MLO 42: 20-22)
No longer passive• Perhaps it is or should be interventional
Specimen• Reflex testing• POC• 24/7 testing
Communications• Active communication between clinicians and microbiologists• Many different modes available• DATA management and data systems must change
Clinical and Public Health Impact Costs vs benefits
• May cost more in lab but if LOS is decreased and cost to patient is decreased and most importantly outcomes are better-----
The authors call this Collaborative Medicine

SUMMARY
The use of methods that reduce time to results have proven to be better for the patient and for the medical community in general
• Outcomes• LOS• Costs• Reduced antibiotic resistance development
Rapid methods are now and will become more available• One “shoe” will not fit all, but we all need to keep abreast of the potential
for these newer methods and find ones that fit our circumstances
Communication is key to using these rapid methods for obtaining effective outcomes and achieving best antibiotic stewardship goals



Thanks!
• To Barbara Lapinskas and APUA for inviting me and doing a wonderful job of planning & organizing
• You, the audience for listening and not sleeping (?)• My family for their support
Questions?
![Interventions to improve hand hygiene compliance …emerald.tufts.edu/med/apua/consumers/resources_7_962926375.pdf[Intervention Review] Interventions to improve hand hygiene compliance](https://static.fdocuments.in/doc/165x107/5aa9cabe7f8b9a90188d4cd9/interventions-to-improve-hand-hygiene-compliance-intervention-review-interventions.jpg)

















