Rangsang Nyeri
33
Rangsang Nyeri PSIK Block 1.3 Year 2009 Andreanyta Meliala, Dr.,Ph.D Dept. of Physiology (Med.F-GMU)
-
Upload
maulidaannisa -
Category
Documents
-
view
80 -
download
2
Transcript of Rangsang Nyeri
Rangsang Nyeri
PSIK Block 1.3 Year 2009
Andreanyta Meliala, Dr.,Ph.D
Dept. of Physiology (Med.F-GMU)

Nyeri….Terjadi oleh karena gangguan keseimbanganeksitasi dan inhibisi
Eksitasi Inhibisi

Low intensity stimulus
High intensitystimulus
Lowthreshold
A betafibre
High thresholdA deltaand Cnociceptor
PNSCNS
Cortex
Non-painful sensation PAINStubhaug, 2002
Modifikasi Meliala, 2003

HEAT
CHEMICAL
PRESSUREBRAINPANASPEGELPERIH
Modifikasi Meliala, 2003

Activation
External
Stimuli
Heat
Mechanical
Chemical
VR1
Ca2+
mDEG
P2X3
Generator potentials
action potentials
Voltage gated sodium channels
Pain and auto-sensitization
Woolf & Mitchel, 2001
TRANSDUCTION
ATP
Na+
Modifikasi Meliala, 2003
PAINPAIN

Pemeriksaan Neuromuskuloskeletal (5 menit)
OA, RA, Trigger OA, RA, Trigger fingerfinger
De QuervainDe Quervain
Tennis ElbowTennis Elbow
Frozen shoulderFrozen shoulderSindrom Sindrom servikalservikal
Low back Low back painpain
IschialgiaIschialgia
OA lututOA lututFasciitis Fasciitis plantarisplantaris
TendinitisTendinitis

Anger
Fear
Anxiety
Depression
Noxious Stimuli P
SY
CH
OL
OG
ICA
L
NOCICEPTIVE
A
B
MELIALA 2004

Glu
C-fiber terminal
GABA Badenosine
AMPAKAI
NMDA
K+
NK1mGluR TrkB
VGCC NSC GABA-A GLY
Inhibitory interneuron
Gly/GABAGABA B
Adenosine
NociceptiveDorsal horn neuron
Activation: AMPA/KAI receptor fast EPSPs
HIPERSENSITIFITAS : Sensitisasi Perifer (Modulasi)
Woolf & Mitchel, 2001Modifikasi Meliala, 2003
K+
K+K+
Glu
Ca2+

Glu SP
C-fiber terminal
GABA Badenosine
AMPAKAI
NMDA
K+
NK1mGluR TrkB
VGCC NSC GABA-A GLY
Inhibitory interneuron
Gly/GABAGABA B
Adenosine
Woolf & Mitchel, 2001Modifikasi Meliala, 2003
K+
K+K+
Glu
Ca2+
Ca2+
IP3
Ca2+ Na2+
Activation: Slow EPSPs, plateau potentials, summation & wind-up
HIPERSENSITIFITAS: Sensitisasi sentral
P2XNMDA
Ca2+
Ca2+
Ca2+ Na2+
Ca2+
Ca2+Ca2+
Mg2+

Beydoun, 2002
TERAPI BERDASAR MEKANISME
MedulaSpinalis
Sensitisasi perifer ion Na
PAINTPAINTBRAIN
InhibisiDescenden
NE/SHT
ReseptorOpoid
Modifikasi Meliala, 2003

Beydoun, 2002
TERAPI BERDASAR MEKANISME
MedulaSpinalis
Sensitisasi perifer ion Na
CBZOXCPHTMEXILETINLIDOCAINDLL
TX
CBZOXCPHTMEXILETINLIDOCAINDLL
PAINPAINBRAIN
InhibisiDescenden
NE/SHT
ReseptorOpoid
NO PAINNO PAIN
Modifikasi Meliala, 2003

Beydoun, 2002
TERAPI BERDASAR MEKANISME
MedulaSpinalis
Sensitisasi perifer ion Na
PAINPAINBRAIN
InhibisiDescenden
NE/SHT
ReseptorOpoid
NO PAINNO PAIN
SensitisasiSentral
(NMDA,Calcium)
TX
GBPOXCLTGKetaminDextroMetorphanDLL
GBPOXCLTGKetaminDextroMetorphanDLL
Modifikasi Meliala, 2003

Beydoun, 2002
TERAPI BERDASAR MEKANISME
MedulaSpinalis
Sensitisasi perifer ion Na
TCATramadolOpioidDLL
TX
TCATramadolOpioidDLL
PAINPAINBRAIN
InhibisiDescenden
NE/SHT
ReseptorOpoid
NO PAIN NO PAIN
Modifikasi Meliala, 2003
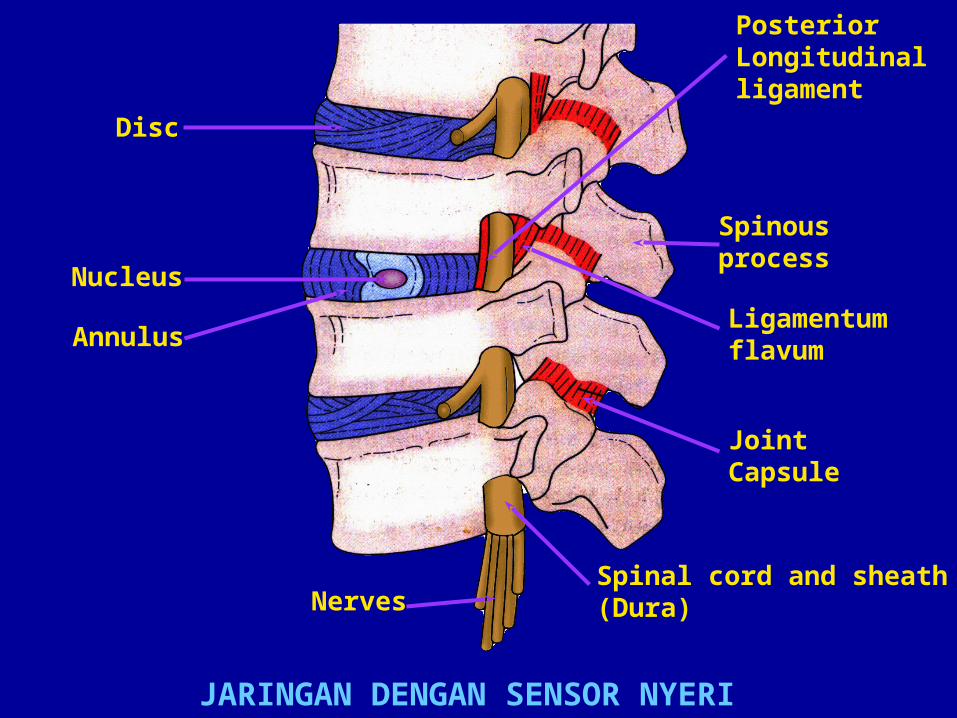
Disc
Nucleus
Annulus
PosteriorLongitudinalligament
Spinousprocess
Ligamentumflavum
JointCapsule
Spinal cord and sheath(Dura)Nerves
JARINGAN DENGAN SENSOR NYERI

Disc bulging
Osteophytes (trapping nerve)
JointCapsule
TITIK TEKAN DISEKITAR ARTIKULASIO SPINALIS

Longissimuscapitis
Spinalisthoracis
Longissimus
Keterangan : Otot pendek berfungsi sebagai stabilisator dan otot panjang untuk pergerakan
GAMBAR OTOT PUNGGUNG
Longissimuscervicis
Spinaliscervicis
Iliocostalislumborum
Iliocostalisthoracis
Multifidus
Intertransversarii
Iliocostaliscervicis

Penurunan fungsi oleh usia
Epesode akut dengan pengobatan yang baik
Pengobatan tidak adekuat menyebabkan NPB kronik
Pengobatan Nyeri yang baik memungkinkan rehabilitasi
Keku
ata
n/S
tabili
tas/
Fungsi
WaktuKeterangan :


2.3.
4.5.
Histamin
Sel Mast
DRG
Medulaspinalis
Pembuluhdarah
Lesi
1.
1.
BRAIN
Meliala, 2005

Mekanisme Proteksi Nyeri spasme otot
I
II-IV
III-IV
Ia
Joint receptor (nociceptor)
Joint dysfunctionor pain
Nociceptor
Muscle painA
B
Muscle spindle
-Motoaxon
-Motoaxon
Descending influencesCSpinothalamic
tract
I
Eperison
PAINNO PAIN

Diabetic foot ulcer in typical location
Medscape http://www.medscape.com

Semmes-Weinstein monofilament being used to
test sensation in a diabetic patient
Medscape http://www.medscape.com

Measuring temperature sensation thresholds using
the CASE IV quantitative sensory testing device.
Medscape http://www.medscape.com

Measuring vibratory sensation thresholds using the
CASE IV quantitative sensory testing device
Medscape http://www.medscape.com
Medscape http://www.medscape.com

Polyneuropathy is caused by the degeneration of axon terminals and results in symmetric distal sensory loss with shading to normal sensation. A compression neuropathy often results in demyelination with the axon left relatively intact. Sensory loss follows a radicular pattern. When the neuronal cell body dies the condition is called "neuronopathy." If the cell body is in the sensory ganglion the condition is often referred to as "ganglionopathy." The pattern is usually random
Axonal polyneuropathy Demyelinating Neuropathy Neuronopathy (Ganglionopathy)

• Pain in a patient with no pre-existing chronic painful condition
• Pain in patient with a chronic painful condition, not related to the pre-existing problem.
• Pain due to an exacerbation of a chronic painful condition.
TYPES OF ACUTE PAINTYPES OF ACUTE PAIN
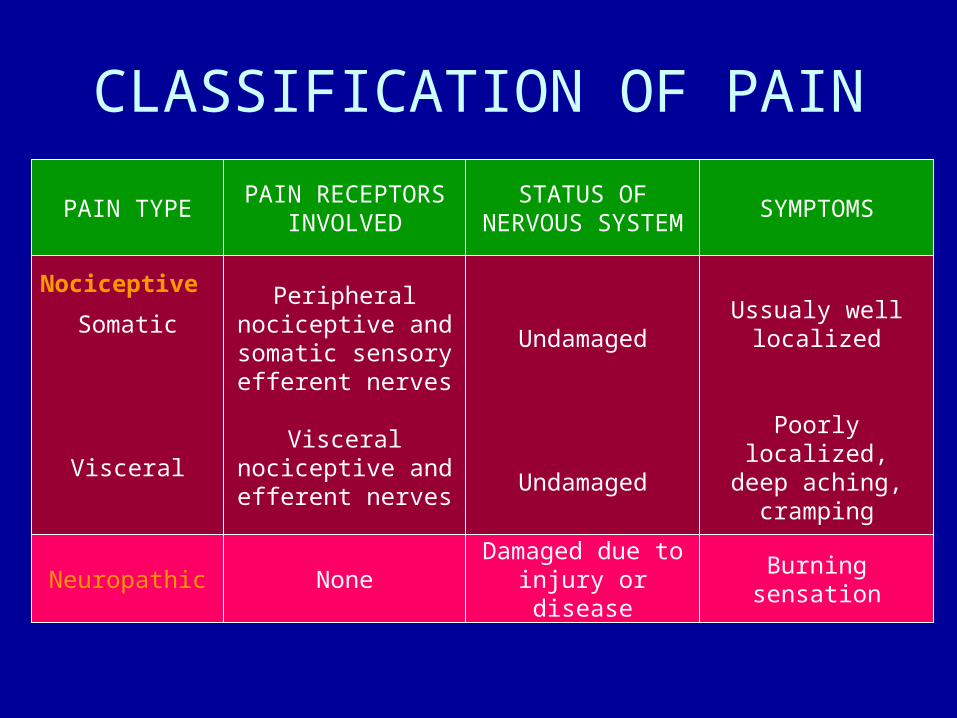
CLASSIFICATION OF PAIN
PAIN TYPEPAIN RECEPTORS
INVOLVED
STATUS OF NERVOUS SYSTEM
SYMPTOMS
Somatic
Visceral
Peripheral nociceptive and somatic sensory efferent nerves
Visceral nociceptive and efferent nerves
Undamaged
Undamaged
Ussualy well localized
Poorly localized,deep aching,
cramping
Nociceptive
Neuropathic NoneDamaged due to injury or disease
Burning sensation

PAIN MANAGMENTNoninvasive• Physical
– Physical therapy– Occupational therapy– Activity modification– Brancing
• Cognitive-behavioural– Relaxation therapy– Psychological/psychiatric management
• Pharmacological
Invasive• Blocks
– Diagnostic– Therapeutic– Implanted devices– Medication pumps– Spinal-cord stimulators
• Surgery

ANALGESIC MEDICATIONSPRIMARY ANALGESICS• Acetminophen• Prostaglandin synthesis inhibitors
– Salicylates– Traditonal NSAIDs– COX-2-selective NSAIDs (coxibs)
• Tramadol• Opioids
– Traditional– Mixed
ADJUVANT MEDICATIONS• Antidepressants• Anticonvulsants• Local anesthetics• Miscellaneous agents

PERCEPTION
MODULATION
TRANSMISSION
TRANSDUCTION
PAIN – SERIES OF EVENTS
PAIN

V. PRINCIPLES OF PAIN MANAGEMENT WITH ANALGESICS
See text

Andreanyta Meliala, Dewanto Husodo, Benaia Decitta Husodo, Jedidia Suksmatatya Husodo
Picture taken: May, 2007