Randomized Crossover Comparison of Personalized MPC and PID … · 2016-06-13 · To date, no...
8
Randomized Crossover Comparison of Personalized MPC and PID Control Algorithms for the Artificial Pancreas Diabetes Care 2016;39:1135–1142 | DOI: 10.2337/dc15-2344 OBJECTIVE To evaluate two widely used control algorithms for an artificial pancreas (AP) under nonideal but comparable clinical conditions. RESEARCH DESIGN AND METHODS After a pilot safety and feasibility study (n= 10), closed-loop control (CLC) was evaluated in a randomized, crossover trial of 20 additional adults with type 1 diabetes. Personalized model predictive control (MPC) and proportional integral derivative (PID) algorithms were compared in supervised 27.5-h CLC sessions. Challenges included overnight control after a 65-g dinner, response to a 50-g breakfast, and response to an unannounced 65-g lunch. Boluses of announced dinner and breakfast meals were given at mealtime. The primary outcome was time in glucose range 70–180 mg/dL. RESULTS Mean time in range 70–180 mg/dL was greater for MPC than for PID (74.4 vs. 63.7%, P = 0.020). Mean glucose was also lower for MPC than PID during the entire trial duration (138 vs. 160 mg/dL, P = 0.012) and 5 h after the unannounced 65-g meal (181 vs. 220 mg/dL, P = 0.019). There was no significant difference in time with glucose <70 mg/dL throughout the trial period. CONCLUSIONS This first comprehensive study to compare MPC and PID control for the AP indi- cates that MPC performed particularly well, achieving nearly 75% time in the target range, including the unannounced meal. Although both forms of CLC pro- vided safe and effective glucose management, MPC performed as well or better than PID in all metrics. Numerous studies have evaluated the efficacy of controlled artificial pancreas (AP) devices for persons with type 1 diabetes (T1DM). These studies were performed in camps, in a clinic setting, in supervised outpatient settings, and at subjects’ homes (1–9). Comparing results across these studies to determine which AP control algo- rithm works best has been difficult due to the many variables inherent in T1DM management. For example, clinical trials can be held in different locations; involve subjects of different ages and lifestyles; use different devices, algorithms, and settings; and use single or multihormonal therapy. Other factors include different (or no) exercise periods, announced (bolused) versus unannounced meals, overnight- only or 24-h trials, and prebolus for meals versus bolus at mealtime. 1 William Sansum Diabetes Center, Santa Barbara, CA 2 Department of Chemical Engineering, Univer- sity of California, Santa Barbara, Santa Barbara, CA 3 John A. Paulson School of Engineering and Ap- plied Sciences, Harvard University, Cambridge, MA Corresponding author: Francis J. Doyle III, [email protected]. Received 29 October 2015 and accepted 18 February 2016. Clinical trial reg. nos. NCT02438670 and NCT01987206, clinicaltrials.gov. This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/ suppl/doi:10.2337/dc15-2344/-/DC1. J.E.P., J.B.L., and E.D. are co–first authors and contributed equally to this study. © 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. See accompanying articles, pp. 1123, 1127, 1143, 1151, 1161, 1168, 1175, and 1180. Jordan E. Pinsker, 1 Joon Bok Lee, 1,2 Eyal Dassau, 1,2,3 Dale E. Seborg, 1,2 Paige K. Bradley, 1 Ravi Gondhalekar, 1,2 Wendy C. Bevier, 1 Lauren Huyett, 1,2 Howard C. Zisser, 1,2 and Francis J. Doyle III 1,2,3 Diabetes Care Volume 39, July 2016 1135 ARTIFICIAL PANCREAS
Transcript of Randomized Crossover Comparison of Personalized MPC and PID … · 2016-06-13 · To date, no...

Randomized CrossoverComparison of PersonalizedMPC and PID Control Algorithmsfor the Artificial PancreasDiabetes Care 2016;39:1135–1142 | DOI: 10.2337/dc15-2344
OBJECTIVE
To evaluate two widely used control algorithms for an artificial pancreas (AP)under nonideal but comparable clinical conditions.
RESEARCH DESIGN AND METHODS
After a pilot safety and feasibility study (n = 10), closed-loop control (CLC) wasevaluated in a randomized, crossover trial of 20 additional adults with type 1diabetes. Personalized model predictive control (MPC) and proportional integralderivative (PID) algorithms were compared in supervised 27.5-h CLC sessions.Challenges included overnight control after a 65-g dinner, response to a 50-gbreakfast, and response to an unannounced 65-g lunch. Boluses of announceddinner and breakfast meals were given at mealtime. The primary outcome wastime in glucose range 70–180 mg/dL.
RESULTS
Mean time in range 70–180 mg/dL was greater for MPC than for PID (74.4 vs.63.7%, P = 0.020). Mean glucose was also lower forMPC than PID during the entiretrial duration (138 vs. 160 mg/dL, P = 0.012) and 5 h after the unannounced 65-gmeal (181 vs. 220 mg/dL, P = 0.019). There was no significant difference in timewith glucose <70 mg/dL throughout the trial period.
CONCLUSIONS
This first comprehensive study to compare MPC and PID control for the AP indi-cates that MPC performed particularly well, achieving nearly 75% time in thetarget range, including the unannounced meal. Although both forms of CLC pro-vided safe and effective glucose management, MPC performed as well or betterthan PID in all metrics.
Numerous studies have evaluated the efficacy of controlled artificial pancreas (AP)devices for persons with type 1 diabetes (T1DM). These studies were performed incamps, in a clinic setting, in supervised outpatient settings, and at subjects’ homes(1–9). Comparing results across these studies to determine which AP control algo-rithm works best has been difficult due to the many variables inherent in T1DMmanagement. For example, clinical trials can be held in different locations; involvesubjects of different ages and lifestyles; use different devices, algorithms, andsettings; and use single or multihormonal therapy. Other factors include different(or no) exercise periods, announced (bolused) versus unannounced meals, overnight-only or 24-h trials, and prebolus for meals versus bolus at mealtime.
1William SansumDiabetes Center, Santa Barbara,CA2Department of Chemical Engineering, Univer-sity of California, Santa Barbara, Santa Barbara,CA3John A. Paulson School of Engineering and Ap-plied Sciences, Harvard University, Cambridge,MA
Corresponding author: Francis J. Doyle III,[email protected].
Received 29 October 2015 and accepted 18February 2016.
Clinical trial reg. nos. NCT02438670 andNCT01987206, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-2344/-/DC1.
J.E.P., J.B.L., and E.D. are co–first authors andcontributed equally to this study.
© 2016 by the American Diabetes Association.Readersmayuse this article as longas thework isproperly cited, the use is educational and not forprofit, and the work is not altered.
See accompanying articles, pp. 1123,1127, 1143, 1151, 1161, 1168, 1175,and 1180.
Jordan E. Pinsker,1 Joon Bok Lee,1,2
Eyal Dassau,1,2,3 Dale E. Seborg,1,2
Paige K. Bradley,1 Ravi Gondhalekar,1,2
Wendy C. Bevier,1 Lauren Huyett,1,2
Howard C. Zisser,1,2 and
Francis J. Doyle III1,2,3
Diabetes Care Volume 39, July 2016 1135
ARTIFIC
IALPANCREA
S

To date, no clinical trial has directlycompared the performance of modelpredictive control (MPC) and propor-tional integral derivative (PID) controlalgorithms for AP under identical con-ditions in a randomized crossover de-sign. Similarly, most studies have notintentionally stressed the limits of APsystems to see how well they performunder nonideal conditions. For instance,some protocols have subjects prebolusas much as 30 min prior to meals (10).While this strategy improves results(11), it does not test operation of thesystem under realistic conditions, suchas when patients bolus at mealtime, orforget to bolus, as can happen in unsu-pervised home settings, where up tohalf of adults report omission of boluses(12).Anticipating that challenges may oc-
cur with practical use of AP technologiesoutside of clinical research protocols,we performed the first randomized,crossover study to expressly compareMPC and PID for AP under identical,nonideal conditions in 27.5-h sessions.Challenges in the study were designedto model the realistic use of a future AP,including no prior optimization of sub-jects’ insulin pump settings, overnightcontrol (midnight to 7:00 A.M.) after a65-g dinner, response to a 50-g break-fast (both bolused at mealtime), and anunannounced 65-g lunch to evaluatethe response to a missed meal bolusscenario.
RESEARCH DESIGN AND METHODS
The study was performed at the WilliamSansum Diabetes Center. Design of thecontrol algorithms and engineering ofthe AP device were done at the Depart-ment of Chemical Engineering at theUniversity of California, Santa Barbara.Due to the numerous challenges in thestudy and the potential for hyper- andhypoglycemia, an initial safety and fea-sibility study was performed (n = 10)(NCT01987206, clinicaltrials.gov) withhourly YSI 2300 Stat (Yellow Springs In-struments, Yellow Springs, OH) glucosemonitoring and close clinical supervisionfor the 27.5 h of closed-loop control(CLC). Based on the results of the pilotstudy (13), we improved safety of thecontrol algorithms and subsequently per-formed this study (n = 20) (NCT02438670,clinicaltrials.gov) with less stringent clini-cal monitoring (described below). The
primary end point was percent time inglucose range 70–180 mg/dL (safe glu-cose range) by continuous glucose moni-toring. Secondary end points includedtime spent in the hypoglycemic range(,70 mg/dL), time spent in the hypergly-cemic range (.180 mg/dL), and the needfor outside intervention to prevent hypo-or hyperglycemia. The study comparedresults from both CLC strategies (MPCand PID). These end points were deter-mined for the entire study: the 5-hpostprandial meal responses for both an-nouncedmeals and the unannouncedmealand for the nocturnal period (12:00 A.M.–
7:00 A.M.). The trial was approved byboth the U.S. Food and Drug Administra-tion and the Cottage Health System In-stitutional Review Board.
Subjects and Closed-Loop SystemA total of 30 subjects completed thestudies, as summarized in Fig. 1. Tensubjects completed the pilot safety andfeasibility trial. An additional 20 subjectscompleted the current study. Inclusioncriteria were age 21–65 years with diag-nosed T1DM for more than 1. year, useof continuous subcutaneous insulin in-fusionpump therapy for at least 6months,and anHbA1c between5.0% (31mmol/mol)and 10.0% (86 mmol/mol). Exclusioncriteria were diabetic ketoacidosis orsevere hypoglycemia within the pastyear, abnormal lab findings, pregnancy,current participation in another study,and comorbidities that would affect thesafety of the subject or prevent comple-tion of the study. Informed consent wasobtained prior to all study procedures.Recruitment and enrollment of subjectswere in compliance with ethics stan-dards set by the Santa Barbara CottageHealth System Institutional ReviewBoard.
The subjects wore two Dexcom G4Platinum continuous glucose monitors(CGM) (Dexcom, Inc., San Diego, CA),placed at least 48 h prior to study visits.Subjects calibrated both CGMs 30 minbefore all meals and at bedtime through-out the study session. During CLC, sub-jects wore the Animas OneTouch PingGlucose Management System (AnimasCorporation, Westchester, PA) continu-ous subcutaneous insulin infusion pump.Wireless communication among the sys-tem components occurred with our por-table artificial pancreas system (pAPS),version 1.9.8.1, running on a Windows
tablet computer (14). The pAPS used thesubjects’ open-loop basal rates, insulin-to-carbohydrate ratios (CR), and insulinsensitivity factors to initialize both CLCsessions.
Study DesignEach subject was randomly assigned tothe MPC or the PID arm of the study for27.5 h in a supervised outpatient suite.Each subject returned 5–14 days afterthe first session to cross over to the sec-ond arm of the study (Fig. 1). Prior to thestart of each session, subjects weregiven a supervised lunch while still onsensor-augmented pump (SAP) therapyand observed to ensure equitable start-ing conditions for each CLC session. Oneprimary CGM was selected for use withthe pAPS at the start of each CLC ses-sion, and the secondary CGM was keptas a backup in case of sensor failure(occurred for two subjects). Two an-nounced meals (dinner, 65 g, at;7:00 P.M.
and breakfast, 50 g, at ;7:00 A.M.) andan unannounced meal (lunch, 65 g, at;1:00 P.M.) were provided. The contentsof the dinner and next day’s lunch wereidentical for each subject in both arms ofthe study, although the contents of eachmeal varied across subjects. All mealswere separated by at least 5 h to ensurethat the effects of the previous meal bo-lus were no longer present by the nextmeal. Boluses for announced meals un-der CLCwere given atmealtime based onthe subject’s CR. Similar to our previousstudy designs (1), the CLC system modi-fied the mealtime bolus based on CGMvalue at the time of the meal as follows:for CGM ,140 mg/dL, 80% of the boluscalculated using the subject’s own CRwas delivered; for CGM $140 mg/dL,the full bolus was given with an addi-tional correction based on the subject’sown correction factor to 140 mg/dL. Nointerventions were made to optimizeglucose levels prior to bedtime. Capil-lary fingerstick glucose measurementswere performed 30 min prior to meals,2 h after meals, at bedtime, and whenprompted by the University of Califor-nia, Santa Barbara health monitoringsystem (HMS) (6). Subjects were dis-charged at ;7:00 P.M. on the secondday of the study.
SafetyThe AP incorporated the HMS, an algo-rithm that added an independent safetylayer (15). The HMS was independent
1136 Comparison of MPC and PID AP Algorithms Diabetes Care Volume 39, July 2016

from the AP control algorithms and ad-vised subjects to ingest 16 g carbohydrateafter confirmation of blood glucose (BG)by fingerstick to prevent impending hy-poglycemia that could not be preventedby controller action alone. Hypoglyce-mia treatments resulting from HMSalerts were counted as hypoglycemicevents in our analysis, as previously rec-ommended (16). The goal of the AP de-vice was to operate without outsideintervention, apart from meal bolusesand HMS alerts. The pAPS system, withthe HMS, was active for 99.6% of theentire trial duration.
Control Algorithm DesignIn comparison of multiple control algo-rithms, it is imperative to reproduce
the same test conditions. That is, thealgorithms should be designed usingthe same available information andevaluated under identical conditions.It was reported by Percival et al. (17)that MPC with a specific choice of de-sign parameters yields a control lawthat is functionally identical to a partic-ular PID design; i.e., a PID controller re-sponse can be recreated by a suitableMPC design. MPC and PID (includinginternal model control) control algo-rithms have been designed for the APand compared in silico in prior studies(18,19). However, in those studies,identical models were not used inboth algorithms, and the algorithmswere not balanced for a detailed com-parison regarding things like insulin on
board. Thus, we built upon the resultsof this prior literature and our own re-cent work to design balanced control-lers for comparison in clinical trials (20).
Both the MPC and PID controllerswere derived using model-based designmethods and the same empirical modelof BG-insulin dynamics (20), with a setpoint of 110 mg/dL. A novel model per-sonalization scheme that takes into ac-count each subject’s basal profile andresponds to individual time-dependentvariation in insulin sensitivities was usedwithin this model (21). MPC is not a spe-cific design but a general control para-digm. MPC comes in many flavors and isextremely flexible, with the capability toincorporate zone-based objectives andasymmetric costs (22,23). This flexibility
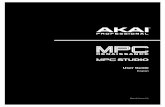
Figure 1—Study design. Ten adults completed the pilot safety and feasibility study, and 20 adults completed the full study. Each subject underwenttwo crossover randomized 27.5-h closed-loop sessions, each under PID or MPC control.
care.diabetesjournals.org Pinsker and Associates 1137

has also allowedMPC to be used for dualhormone approaches to AP (2).To facilitate an equitable comparison
of MPC and PID, we opted to use a ge-neric MPC strategy that does not incor-porate these additional features. Eachcontroller was modified to compensatefor insulin stacking using methods thathave been verified in clinical trials (in-sulin feedback method for PID controland insulin on board for MPC) (24,25).The controllers were tuned to have thesame level of aggressiveness and wereevaluated under identical simulationconditions using the U.S. Food andDrug Administration–accepted Univer-sities of Virginia/Padova metabolic sim-ulator with 100 in silico adult subjects(26).Additional details about the deriva-
tion and development of these controlalgorithms have previously been pub-lished (21,27) and are also available inSupplementary Data.
Statistical AnalysisPower analysis was performed based onthe results of the pilot safety and feasi-bility study for the proposed end points(% time in the safe glucose range). Withthe criterion for significance (a) set at0.05, analysis indicated aminimum sam-ple size of 18 subjects to achieve apower of 80%. We chose to enroll 20subjects in the current study. All glucosedata are reported as mean (SD) unlessotherwise specified. Missing CGM datawere linearly interpolated, and missingCGM data at the end of the study wereimputed to be unchanged from the finaltime point until the expected end of thestudy (28). This imputation was con-ducted primarily to account for subjectswho ended the study early for persistenthyperglycemia after the unannouncedmeal. The imputation did not alter theresults, which is similar to other studieswhere missing CGM data were imputed(29).The differences between each control-
ler group for each metric were comparedusing paired two-sample t tests. MATLAB2015B software (Mathworks, Inc., Natick,MA) was used for all analyses.
RESULTS
Subject CharacteristicsTen subjects completed the pilot study(6 female and 4 male). Twenty additionalsubjects (13 and 7 male) completed the
current study. Subject demograph-ics are summarized in SupplementaryTable 1.
Glycemic ControlResults are reported for all 20 subjectswho completed the study. Cumulativedistributions of glucose levels compar-ing MPC and PID are shown in Fig. 2A.For the overall study,MPC showed a sta-tistically significant greater percent timein the safe glucose range compared withPID (74.4 vs. 63.7%, P = 0.021) (Table 1).Similarly, percent time in the tight targetrange (80–140 mg/dL) was statisticallygreater for MPC compared with PID(49.8 vs. 36.5%, P = 0.009) (Table 1).This improvement is also exhibited inthe statistically significant improve-ments in high BG index (HBGI) (30) for
the entire study period (4.4 vs. 7.51, P =0.011) and the decreases in the percenttime .180 mg/dL (21 vs. 33.3%, P =0.020) (Table 1). The mean glucose val-ues for each subject were statisticallylower for MPC in comparison with PID(138 vs. 160 mg/dL, P = 0.012) (Table 1),which can also be seen in Fig. 3A, repre-senting the mean and % time in the safeglucose range for each individual sub-ject. Overnight control was excellentwith both controllers, showing similartimes in the safe glucose range (89.1and 83.7%) (Table 1).
Both closed-loop controllersminimizedhypoglycemia with regard to both thenumber of hypoglycemic events requiringtreatment and the duration of the events(% time ,70 mg/dL) (Table 1), with nosignificant differences between groups.
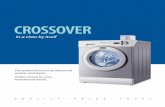
Figure 2—Glucose control performance (by CGM) characterized by median and interquartilerange cumulative % time in glucose range (A), overall glucose (B), and insulin traces (C) of 20adult subjects with glucose controlled by PID and MPC algorithms. The overall glucose tracesalso show the window of time for the administration of eachmeal in the study. The insulin tracesshow mean controller action apart from meal boluses.
1138 Comparison of MPC and PID AP Algorithms Diabetes Care Volume 39, July 2016

The majority of hypoglycemia treatmentsoccurred in a small cohort of subjects forboth arms of the study (SupplementaryFig. 2).Analysis of 5-h postprandial glucose
levels for the dinner meal showed nodifferences between the controllers(Supplementary Table 3). Although timein range 70–180 mg/dL was also similarafter the 50-g breakfast (SupplementaryTable 3), time in range 80–140mg/dL wasstatistically improved for MPC versus PID(38.1 vs. 20.9%, P = 0.008) (SupplementaryTable 3).After the unannounced 65-g lunch,
mean glucose during the 5-h postpran-dial period was 181 mg/dL for MPC and220 mg/dL for PID (P = 0.019) (Table 1and Fig. 3D), with similar results forchange in glucose from premeal base-line (146 and 142 mg/dL, respectively)andpercent time in the safe glucose range.As expected, some subjects, particularly
those who chose to consume meals witha high fat content (30–60 g), experi-enced greater degrees of hyperglyce-mia after the unannounced meal, withone subject requesting to end the ses-sion early under PID control per protocolfor persistent hyperglycemia requiring acorrection bolus.
There were no differences in theoverall insulin delivery between MPCand PID (Fig. 1C, Supplementary Table4). Both control algorithms also deliv-ered similar mean amounts of insulinin the 5-h period after the unannouncedmeal. Of note, the PID controller sus-pended insulin delivery more frequentlythan MPC (Supplementary Table 4), al-though the total insulin delivery wasstatistically similar for both MPC andPID controllers.
Individual traces for all 27.5-h CLCsessions from the study are provided inSupplementary Data.
Adverse EventsThere were no unanticipated adverseevents during the study. Anticipated ad-verse events included hyper- and hypo-glycemia. Hyperglycemia in particularwas anticipated owing to the unan-nounced high-carbohydrate meal. Onesubject had prolonged hyperglycemiaafter the unannounced meal under PIDcontrol. Although there was no signifi-cant ketone formation (,0.6 mmol/L),the subject’s glucose levels rose .250mg/dL and remained persistently ele-vated. Since the subject was not comfort-able continuing the trial, the sessionwas terminated early and a manual in-sulin bolus was administered, as perprotocol.
The HMS functioned well for predict-ing glucose levels,65mg/dL and advisedtreatment with 16 g carbohydrates, ifnecessary. No subject experienced BG,50 mg/dL by fingerstick BG during thestudy under CLC without a prior warningfrom the HMS and subsequent treatmentwith carbohydrates. These interventionsrapidly restored euglycemia. Eight sub-jects experienced four or more hypogly-cemia treatments during a closed-loopsession, as seen in Supplementary Fig. 2.Of these, 4 subjects experienced a similarnumber of alarms for both sessions. Al-though not statistically significant, MPCsessions exhibited a greater number ofhypoglycemia alarms and treatments forthe remaining four sessions than corre-sponding PID sessions.
CONCLUSIONS
In contrast to previous assertions sup-porting the superior performance ofany one type of algorithm across differ-ent trials (31,32), this first randomizedstudy expressly designed to directlycompare the performance of MPC andPID showed that both controllers per-formed very well overall, even after a65-g unannounced meal was accountedfor, and did so with low rates of hypo-glycemia. MPC showed a significantlygreater improvement in glucose controlover PID, with a statistically greater per-cent time in the safe glucose rangethroughout the entire trial period.Both controllers also performed wellin the presence of an unannouncedmeal, with MPC exhibiting a statisticallylower mean glucose value during the5-h postprandial period in comparisonwith PID.
Table 1—Summary of clinical metrics that characterize glucose control performanceof 20 adult subjects controlled by PID and MPC algorithms for 27.5-h sessions
MPC PID P
Overall studyGlucose (mg/dL) 138 (20.40) 160 (31.5) 0.012*Glucose at 7:00 A.M. (mg/dL) 119 (28.0) 135 (51.7) 0.229% time ,70 mg/dL 4.6 (4.65) 2.93 (5.92) 0.329% time 80–140 mg/dL 49.8 (13.1) 36.5 (17.1) 0.009*% time .180 mg/dL 21.0 (12.1) 33.3 (19.1) 0.020*% time 70–180 mg/dL 74.4 (11.0) 63.7 (16.4) 0.021*No. of ,70 mg/dL events .15 min 2.75 (3.02) 1.75 (4.05) 0.382No. of treatments 2.60 (2.68) 1.60 (2.68) 0.246LBGI 1.21 (0.86) 0.82 (1.09) 0.222HBGI 4.40 (2.56) 7.51 (4.52) 0.011*
Overnight onlyGlucose (mg/dL) 109 (15.1) 126 (35.9) 0.058% time ,70 mg/dL 7.29 (10.2) 3.59 (9.18) 0.235% time 80–140 mg/dL 70.2 (23.3) 57.9 (34.2) 0.189% time .180 mg/dL 3.59 (7.37) 12.7 (22.7) 0.095% time 70–180 mg/dL 89.1 (12.4) 83.7 (22.4) 0.351No. of ,70 mg/dL events .15 min 1.25 (2.00) 0.65 (1.81) 0.326No. of treatments 1.05 (1.36) 0.35 (0.81) 0.055LBGI 1.94 (1.74) 1.18 (1.73) 0.173HBGI 0.96 (1.30) 2.48 (3.58) 0.082
5-hour postprandial period afterunannounced meal (65 g CHO)
Mean glucose (mg/dL) 181 (42.0) 220 (55.9) 0.019*Max Dglucose (mg/dL) 146 (44.3) 142 (43.1) 0.774% time ,70 mg/dL 1.89 (3.58) 1.64 (5.70) 0.871% time 80–140 mg/dL 22.2 (18.7) 13.7 (18.9) 0.160% time .180 mg/dL 52.0 (30.3) 66.9 (31.6) 0.135% time 70–180 mg/dL 46.1 (28.8) 31.5 (28.8) 0.116Minutes to ,180 mg/dL 157 (92.5) 188 (102) 0.313HBGI 10.6 (6.91) 17.9 (10.2) 0.012*
Data are means (SD). Sessions include a 65-g carbohydrate dinner, a 50-g carbohydratebreakfast, and an unannounced 65-g carbohydrate lunch. CHO, carbohydrate; LBGI, low BGindex. *Significance with a = 0.05.
care.diabetesjournals.org Pinsker and Associates 1139

One common argument against claim-ing the superiority of any single controlalgorithm is that the algorithms are de-signed to achieve different objectives,such as minimizing hyperglycemia (33)or hypoglycemia (5). Other studies fo-cused on postprandial glucose control(11). All of these factors affect how anAP control algorithm performs, creatingdifficulty in formulating an objectivecomparison of algorithms.In this study, we focused on realistic
challenges an AP may face with morewidespread use. These included over-night control after a 65-g dinner, responseto a 50-g breakfast, and response to anunannounced 65-g lunch. Boluses weregiven at mealtime for the dinner andbreakfastmeal. As shown in our previousstudies, the AP system had respondedwell to unannounced meals of up to50 g carbohydrates (6,7). This study in-cluded an unannounced meal of 65 gcarbohydrates for lunch the secondday because missed meal boluses arelikely to occur for practical use of APsystems. Moreover, while some studiesincorporated a bedtime snack or ele-vated control targets to prevent noc-turnal hypoglycemia (34), both theMPC and PID controllers in this study
were challenged with no changes tothe controller settings overnight andthe subjects’ normal meal plan forbedtime.
Both controllers performedwell over-all and performed similarly to otherstudies of SAP use that did not specifi-cally include unannounced meals (35).The response to the unannounced 65-gmeal, the most difficult challenge in thisstudy, showed overall good results, withmost subjects returning to the targetrange by the end of the 5-h window(mean time to ,180 mg/dL 157 min[MPC] and 188 min [PID], P = 0.313).Some subjects showed prolonged pe-riods of hyperglycemia, most likely re-lated to their consumption of mealswith high fat content. This delayed hy-perglycemia, seen after consumptionof a high-fat meal, may improve withthe introduction of automated bolusesusing biphasic or multiphasic patterns,as previously suggested (36). The AP sys-tem used in this study did not supportthe use of extended boluses, explainingthe difficulties some subjects faced afterconsuming high–fat content meals. Inaddition, our results show that at 5 hafter the unannounced meal, bothforms of CLC delivered slightly less
insulin than would have been deliveredhad the meal of the same carbohydratecontent been delivered with announce-ment, aswas the case for dinner, althoughthis differencewasnot significant. Theper-formance of both algorithms may be im-proved if the controller could betterdifferentiate corrections for postprandialglucose elevation in comparison with el-evated glucose levels not directly relatedto meals. In addition, a subject requestedto stop a session early after the unan-nounced meal under PID control due toelevated glucose levels. This is a veryimportant finding, as it should be ex-pected that AP systems will be facedwith similar challenges to the 65-g un-announced meal when CLC use isadopted by a larger population. Whenaccounting for the 65-g unannouncedmeal and two large announced mealsunder CLC, the very high percent oftime in the target glucose range forboth controllers overall supports previ-ous assertions that single hormonetherapy is suitable for AP, reducingthe number of interventions necessaryunder SAP (37).
The study was designed to comparethe performance of the PID and MPCcontrollers under conditions that wereas equitable as possible. As we have pre-viously demonstrated, the basic MPCstrategy that was used in this studycan be extended with additional fea-tures, such as zone-based approach toreplace the fixed set point, added veloc-ity penalties, and asymmetric weightingof glucose excursions above or belowthe target (27,38). Similar versatilitycan be achieved for PID control usingzones and switching between control-ler settings depending on glucoseabove or below the target. We chosenot to use these features in order tofacilitate an equitable comparison ofthe controllers.
We acknowledge there are manyother limitations to this study. First,even with a session duration of 27.5 hclosed-loop time, it is still not possible todefinitively determine how the algo-rithms will function for prolonged timeperiods in the home setting. In addition,frequent meal boluses will constrain thecontroller from giving corrections. Asweonly had three meals in the study, wedid not test the controller under thecondition of short meal intervals. Third,although we made our best efforts to
Figure 3—Bubble plot representation of the individual mean (black lines; center of the circles)and % time in 70–180mg/dL range (radius of the circle) of the glucose values (CGM) experiencedby each subject controlled by the PID or MPC algorithms for the entire study (A), the overnightperiod (B), and the study period excluding the unannounced meal (C). Mean (black lines; centerof the circles) and % time in 70–180 mg/dL range of the glucose values experienced by eachsubject during the 5-h postprandial period after the 65-g unannounced meal are displayed in D.*Statistically significant differences in the mean values (P , 0.05).
1140 Comparison of MPC and PID AP Algorithms Diabetes Care Volume 39, July 2016

design the controllers under as equita-ble settings as possible, we acknowl-edge that there are many algorithmscurrently being used in different studies,and we could not compare all of them.There are also other varieties of every-day challenges that have not beentested in this study, such as exercise.Finally, we recognize that the controlleris only a part of the overall AP system.Many other components used in the sys-tem, or the activities of the subject (suchas performing regular exercise), mayplay an equal, or possibly more impor-tant, role in achieving glycemic goals.For example, two subjects (subjectsnos. 15-032 and 15-036) in the studyexperienced undesirable glycemic vari-ability during both CLC sessions, requir-ing 6 and 11 and 9 and 9 treatments,respectively, for MPC and PID sessions.This appeared to be a direct conse-quence of the same, or worse, variabilitythat the subjects experienced duringopen-loop care due to suboptimal basalinsulin delivery settingsdmost likelybasal rates that were set too high. Thesefew subjects experienced the highestrate of hypoglycemia treatments, in-creasing the overall mean number of hy-poglycemia treatments under CLC,although most subjects only neededzero or one treatment (SupplementaryFig. 2). While the mean number of hy-poglycemic alerts overall averaged attwo per session, four PID sessions andeight MPC sessions exhibited more thantwo treatments per day, a threshold fornumber of hypoglycemia treatmentsthat may be too high for ambulatoryclinical practice. Zero alerts per dayand no need for supplemental carbohy-drate to treat hypoglycemia are what weaim for; however, this may be an unrea-sonable expectation at this developmentstage without increase in mean glucoseand greater time spent in the hyperglyce-mic range. Instead, we suggest a thresh-old of two treatments per day as anacceptable compromise. Twenty percentof the PID clinical sessions and 40% of theMPC clinical sessions experienced moretreatments than this threshold. Detuningof the aggressiveness of the controllers,as was done in previous trials; elevationof the set point; or adjustment of otherconstraints may be necessary to limit hy-poglycemia in these subjects while stilladdressing the concern of overall glucosecontrol performance (39). This is an
important issue that can also be ad-dressed with optimization of insulin de-livery settings prior to initiating CLC,possibly by using run-to-run adaptationstrategies with algorithmic or clinician-directed adjustment (1,40).
We conclude that the MPC controllermatched or outperformed the PID con-troller on all clinical metrics of glucosecontrol in this study, although both con-trollers provided safe and effective glu-cose management and appear wellsuited for future AP applications. Futurestudies should continue to report on re-sults under nonideal conditions so thatthe readiness of CLC for widespread usecan be ascertained.
Acknowledgments. The authors acknowledgeDr. David Kerr, Dr. Kristin Castorino,Dr. AlexanderMorf, Tyler Jean, and Katie Tovar (WilliamSansum Diabetes Center), as well as all thesupport staff at the William Sansum DiabetesCenter, for assistancewith this study. The authorsfurther acknowledge Dr. Isuru Dasanayake (IntelCorporation) for his assistance. Finally, the au-thors thank and acknowledge product supportfrom Animas Corporation; Dexcom, Inc.; andLifeScan, Inc.Funding. This work was supported by the JDRF(grant 22-2011-237) and National Institute ofDiabetes and Digestive and Kidney Diseases, Na-tional Institutes of Health (grants DP3-DK-094331 and R01-DK-085628).DualityofInterest.H.C.Z. is currentlyemployedby the Insulet Corporation. No other potentialconflicts of interest relevant to this article werereported.Author Contributions. J.E.P., J.B.L., and E.D.helped design the study protocol, contributed tothe technology design, and ensured the regula-tory approval of the CLC system; providedprimary technical and clinical support on siteduring all sessions; analyzed data; and authoredthe manuscript. D.E.S. contributed to the tech-nology design of the CLC system and edited andrevised the manuscript. P.K.B. and W.C.B. con-ducted the clinical trials, researched data, andreviewedandedited themanuscript.R.G.helpedconstruct the controller infrastructure, contrib-uted to the discussion, and reviewed and editedthe manuscript. L.H. helped conduct the clinicaltrial, contributedto thediscussion,and reviewedand edited the manuscript. H.C.Z. designed thestudy protocol, contributed to the technologydesign, contributed to the discussion, and re-viewed and edited the manuscript. F.J.D. editedand reviewed the manuscript and was theprincipal investigator of the project. F.J.D. isthe guarantor of this work and, as such, hadfull access to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.Prior Presentation. Parts of this study werepresented in abstract form at the 76th ScientificSessions of the American Diabetes Association,New Orleans, LA, 10–14 June 2016.
References1. Dassau E, Brown SA, Basu A, et al. Adjust-ment of open-loop settings to improve closed-loop results in type 1 diabetes: a multicenterrandomized trial. J Clin Endocrinol Metab2015;100:3878–38862. Russell SJ, El-Khatib FH, Sinha M, et al. Out-patient glycemic control with a bionic pancreasin type 1 diabetes. N Engl J Med 2014;371:313–3253. Nimri R, Muller I, Atlas E, et al. MD-Logicovernight control for 6 weeks of home use inpatients with type 1 diabetes: randomizedcrossover trial. Diabetes Care 2014;37:3025–30324. Ly TT, Breton MD, Keith-Hynes P, et al. Over-night glucose control with an automated, uni-fied safety system in children and adolescentswith type 1 diabetes at diabetes camp. DiabetesCare 2014;37:2310–23165. Kovatchev BP, Renard E, Cobelli C, et al.Safety of outpatient closed-loop control: firstrandomized crossover trials of a wearable arti-ficial pancreas. Diabetes Care 2014;37:1789–17966. Harvey RA, Dassau E, Bevier WC, et al. Clin-ical evaluation of an automated artificial pan-creas using zone-model predictive control andhealth monitoring system. Diabetes TechnolTher 2014;16:348–3577. Dassau E, Zisser H, Harvey RA, et al. Clinicalevaluation of a personalized artificial pancreas.Diabetes Care 2013;36:801–8098. Cobelli C, Renard E, Kovatchev BP, et al. Pilotstudies of wearable outpatient artificial pan-creas in type 1 diabetes. Diabetes Care 2012;35:e65–e679. Thabit H, Tauschmann M, Allen JM, et al.;APCam Consortium; AP@home Consortium.Home use of an artificial beta cell in type 1 di-abetes. N Engl J Med 2015;373:2129–214010. Capel I, Rigla M, Garcıa-Saez G, et al. Artifi-cial pancreas using a personalized rule-basedcontroller achieves overnight normoglycemiain patients with type 1 diabetes. Diabetes Tech-nol Ther 2014;16:172–17911. Chase HP, Doyle FJ 3rd, Zisser H, et al.; Con-trol to Range Study Group. Multicenter closed-loop/hybrid meal bolus insulin delivery withtype 1 diabetes. Diabetes Technol Ther 2014;16:623–63212. Peyrot M, Rubin RR, Kruger DF, Travis LB.Correlates of insulin injection omission. Diabe-tes Care 2010;33:240–24513. Lee J, Pinsker JE, Dassau E, et al. Clinicalcomparison of MPC and PID artificial pancreascontrollers: a randomized crossover trial (Ab-stract). Diabetes 2015;64(Suppl. 1):A27514. Dassau E, Zisser H, C Palerm C, A BuckinghamB, Jovanovic L, J Doyle F 3rd. Modular artificialbeta-cell system: a prototype for clinical re-search. J Diabetes Sci Technol 2008;2:863–87215. Harvey RA, Dassau E, Zisser H, Seborg DE,Jovanovic L, Doyle FJ III. Design of the healthmonitoring system for the artificial pancreas:low glucose prediction module. J Diabetes SciTechnol 2012;6:1345–135416. Doyle FJ 3rd, Huyett LM, Lee JB, Zisser HC,Dassau E. Closed-loop artificial pancreas sys-tems: engineering the algorithms. DiabetesCare 2014;37:1191–1197
care.diabetesjournals.org Pinsker and Associates 1141

17. Percival MW, Zisser H, Jovanovic L, Doyle FJ3rd. Closed-loop control and advisory modeevaluation of an artificial pancreatic beta cell:use of proportional-integral-derivative equiva-lent model-based controllers. J Diabetes SciTechnol 2008;2:636–64418. Magni L, Raimondo DM, Bossi L, et al.Modelpredictive control of type 1 diabetes: an in silicotrial. J Diabetes Sci Technol 2007;1:804–81219. Parker RS, Doyle FJ 3rd, Peppas NA. Amodel-based algorithm for blood glucose con-trol in type I diabetic patients. IEEE Trans Bi-omed Eng 1999;46:148–15720. van Heusden K, Dassau E, Zisser HC, SeborgDE, Doyle FJ 3rd. Control-relevant models for glu-cose control using a priori patient characteristics.IEEE Trans Biomed Eng 2012;59:1839–184921. Lee JB, Dassau E, Seborg DE, Doyle FJ III.Model-based personalization scheme of an artifi-cial pancreas for type 1 diabetes applications.American Control Conference (ACC), 17–19 June2013, Washington, DC. IEEE Xplore Abstract.p. 2911–291622. Turksoy K, Bayrak ES, Quinn L, Littlejohn E,Cinar A.Multivariable adaptive closed-loop con-trol of an artificial pancreas without meal andactivity announcement. Diabetes Technol Ther2013;15:386–40023. Grosman B, Dassau E, Zisser HC, JovanovicL, Doyle FJ 3rd. Zone model predictive control: astrategy to minimize hyper- and hypoglycemicevents. J Diabetes Sci Technol 2010;4:961–97524. Steil GM, Palerm CC, Kurtz N, et al. The effectof insulin feedback on closed loop glucose con-trol. J Clin Endocrinol Metab 2011;96:1402–140825. Ellingsen C, Dassau E, Zisser H, et al. Safetyconstraints in an artificial pancreatic beta cell:an implementation of model predictive controlwith insulin on board. J Diabetes Sci Technol2009;3:536–544
26. Kovatchev BP, BretonM,Man CD, Cobelli C.In silico preclinical trials: a proof of concept inclosed-loop control of type 1 diabetes. J Diabe-tes Sci Technol 2009;3:44–5527. Gondhalekar R, Dassau E, Zisser HC, DoyleFJ 3rd. Periodic-zone model predictive controlfor diurnal closed-loop operation of an artificialpancreas. J Diabetes Sci Technol 2013;7:1446–146028. Little RJA, Rubin DB. Statistical AnalysisWith Missing Data. New York, John Wiley &Sons, 1987, p. 59–7229. Beck RW, Hirsch IB, Laffel L, et al.; JuvenileDiabetes Research Foundation ContinuousGlucose Monitoring Study Group. The effectof continuous glucose monitoring in well-con-trolled type 1 diabetes. Diabetes Care 2009;32:1378–138330. Kovatchev BP, Cox DJ, Gonder-Frederick L,Clarke WL. Methods for quantifying self-moni-toring blood glucose profiles exemplified by anexamination of blood glucose patterns in pa-tients with type 1 and type 2 diabetes. DiabetesTechnol Ther 2002;4:295–30331. Steil GM. Algorithms for a closed-loop arti-ficial pancreas: the case for proportional-integral-derivative control. J Diabetes Sci Technol 2013;7:1621–163132. Bequette BW. Algorithms for a closed-loopartificial pancreas: the case for model predictivecontrol. J Diabetes Sci Technol 2013;7:1632–164333. Finan DA, McCann TW Jr, Mackowiak L,et al. Closed-loop control performance of thehypoglycemia-hyperglycemia minimizer (HHM)system in a feasibility study. J Diabetes Sci Tech-nol 2014;8:35–4234. Tauschmann M, Allen JM, Wilinska ME,et al. Day-and-night hybrid closed-loop insulindelivery in adolescents with type 1 diabetes: a
free-living, randomized clinical trial. DiabetesCare. 6 January 2016 [Epub ahead of print]35. Kropff J, Del Favero S, Place J, et al.;AP@home consortium. 2 month evening andnight closed-loop glucose control in patientswith type 1 diabetes under free-living condi-tions: a randomised crossover trial. Lancet Di-abetes Endocrinol 2015;3:939–94736. Srinivasan A, Lee JB, Dassau E, Doyle FJ 3rd.Novel insulin delivery profiles for mixed mealsfor sensor-augmented pump and closed-loopartificial pancreas therapy for type 1 diabetesmellitus. J Diabetes Sci Technol 2014;8:957–96837. Haidar A, Legault L, Messier V, Mitre TM,Leroux C, Rabasa-Lhoret R. Comparison of dual-hormone artificial pancreas, single-hormone ar-tificial pancreas, and conventional insulin pumptherapy for glycaemic control in patients withtype 1 diabetes: an open-label randomised con-trolled crossover trial. Lancet Diabetes Endocri-nol 2015;3:17–2638. Gondhalekar R, Dassau E, Doyle FJ III. MPCdesign for rapid pump-attenuation and expe-dited hyperglycemia response to treat T1DMwith an artificial pancreas. American ControlConference (ACC), 4–6 June 2014, Portland,OR. IEEE Xplore Abstract. p. 4224–423039. Luijf YM, DeVries JH, Zwinderman K, et al.;AP@home Consortium. Day and night closed-loop control in adults with type 1 diabetes: acomparison of two closed-loop algorithms driv-ing continuous subcutaneous insulin infusionversus patient self-management. DiabetesCare 2013;36:3882–388740. Wang Y, Dassau E, Doyle FJ 3rd. Closed-loopcontrol of artificial pancreatic Beta -cell in type 1diabetes mellitus using model predictive itera-tive learning control. IEEE Trans Biomed Eng2010;57:211–219
1142 Comparison of MPC and PID AP Algorithms Diabetes Care Volume 39, July 2016