Randomized Controlled Trial of Osmotic-Release Methylphenidate With Cognitive-Behavioral Therapy in...
12
NEW RESEARCH Randomized Controlled Trial of Osmotic- Release Methylphenidate With Cognitive- Behavioral Therapy in Adolescents With Attention-Deficit/Hyperactivity Disorder and Substance Use Disorders Paula D. Riggs, M.D., Theresa Winhusen, Ph.D., Robert D. Davies, M.D., Jeffrey D. Leimberger, Ph.D., Susan Mikulich-Gilbertson, Ph.D., Constance Klein, L.C.S.W., Marilyn Macdonald, B.A., Michelle Lohman, R.N., Genie L. Bailey, M.D., Louise Haynes, M.S.W., William B. Jaffee, Ph.D., Nancy Haminton, MPA, Candace Hodgkins, Ph.D., Elizabeth Whitmore, Ph.D., Kathlene Trello-Rishel, M.D., Leanne Tamm, Ph.D., Michelle C. Acosta, Ph.D., Charlotte Royer-Malvestuto, M.Ed., Geetha Subramaniam, M.D., Marc Fishman, M.D., Beverly W. Holmes, M.S.W., Mary Elyse Kaye, B.S.N., Mark A. Vargo, Ph.D., George E. Woody, M.D., Edward V. Nunes, M.D., David Liu, M.D. Objective: To evaluate the efficacy and safety of osmotic-release methylphenidate (OROS- MPH) compared with placebo for attention-deficit/hyperactivity disorder (ADHD), and the impact on substance treatment outcomes in adolescents concurrently receiving cognitive- behavioral therapy (CBT) for substance use disorders (SUD). Method: This was a 16-week, randomized, controlled, multi-site trial of OROS-MPH CBT versus placebo CBT in 303 adolescents (aged 13 through 18 years) meeting DSM-IV diagnostic criteria for ADHD and SUD. Primary outcome measures included the following: for ADHD, clinician-administered ADHD Rating Scale (ADHD-RS), adolescent informant; for substance use, adolescent-reported days of use in the past 28 days. Secondary outcome measures included parent ADHD-RS and weekly urine drug screens (UDS). Results: There were no group differences on reduction in ADHD-RS scores (OROS-MPH: 19.2, 95% confidence interval [CI], 17.1 to 21.2; placebo, 21.2, 95% CI, 19.1 to 23.2) or reduction in days of substance use (OROS-MPH: 5.7 days, 95% CI, 4.0 –7.4; placebo: 5.2 days, 95% CI, 3.5–7.0). Some secondary outcomes favored OROS-MPH, including lower parent ADHD-RS scores at 8 (mean difference 4.4, 95% CI, 0.8 –7.9) and 16 weeks (mean difference 6.9; 95% CI, 2.9-10.9) and more negative UDS in OROS-MPH (mean 3.8) compared with placebo (mean 2.8; p .04). Conclusions: OROS-MPH did not show greater efficacy than placebo for ADHD or on reduction in substance use in adolescents concurrently receiving individual CBT for co-occurring SUD. However, OROS-MPH was relatively well tolerated and was associated with modestly greater clinical improvement on some secondary ADHD and substance outcome measures. Clinical Trial Registration Infor- mation—Attention Deficit Hyperactivity Disorder (ADHD) in Adolescents with Substance Use Disorders (SUD); http://www.clinicaltrials.gov; NCT00264797. J. Am. Acad. Child Adolesc. Psychiatry, 2011;50(9):903–914. Key Words: osmotic-release methylphenidate, randomized controlled trial, ADHD, substance use disorders I ndividuals with attention-deficit/hyperactiv- ity disorder (ADHD) have at least twice the lifetime risk for substance use disorders (SUD) compared with non-ADHD controls. 1-3 As many as 30% to 50% of adolescents referred to sub- stance treatment have co-occurring ADHD. 4,5 Despite high rates of co-occurrence, ADHD often goes untreated in community-based substance JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY VOLUME 50 NUMBER 9 SEPTEMBER 2011 903 www.jaacap.org
Transcript of Randomized Controlled Trial of Osmotic-Release Methylphenidate With Cognitive-Behavioral Therapy in...

NEW RESEARCH
Randomized Controlled Trial of Osmotic-Release Methylphenidate With Cognitive-Behavioral Therapy in Adolescents WithAttention-Deficit/Hyperactivity Disorder
and Substance Use DisordersPaula D. Riggs, M.D., Theresa Winhusen, Ph.D., Robert D. Davies, M.D.,
Jeffrey D. Leimberger, Ph.D., Susan Mikulich-Gilbertson, Ph.D.,Constance Klein, L.C.S.W., Marilyn Macdonald, B.A., Michelle Lohman, R.N.,
Genie L. Bailey, M.D., Louise Haynes, M.S.W., William B. Jaffee, Ph.D.,Nancy Haminton, MPA, Candace Hodgkins, Ph.D., Elizabeth Whitmore, Ph.D.,Kathlene Trello-Rishel, M.D., Leanne Tamm, Ph.D., Michelle C. Acosta, Ph.D.,
Charlotte Royer-Malvestuto, M.Ed., Geetha Subramaniam, M.D.,Marc Fishman, M.D., Beverly W. Holmes, M.S.W., Mary Elyse Kaye, B.S.N.,Mark A. Vargo, Ph.D., George E. Woody, M.D., Edward V. Nunes, M.D.,
David Liu, M.D.
Objective: To evaluate the efficacy and safety of osmotic-release methylphenidate (OROS-MPH) compared with placebo for attention-deficit/hyperactivity disorder (ADHD), and theimpact on substance treatment outcomes in adolescents concurrently receiving cognitive-behavioral therapy (CBT) for substance use disorders (SUD). Method: This was a 16-week,randomized, controlled, multi-site trial of OROS-MPH � CBT versus placebo � CBT in 303adolescents (aged 13 through 18 years) meeting DSM-IV diagnostic criteria for ADHD and SUD.Primary outcome measures included the following: for ADHD, clinician-administered ADHDRating Scale (ADHD-RS), adolescent informant; for substance use, adolescent-reported days of usein the past 28 days. Secondary outcome measures included parent ADHD-RS and weekly urinedrug screens (UDS). Results: There were no group differences on reduction in ADHD-RSscores (OROS-MPH: �19.2, 95% confidence interval [CI], �17.1 to �21.2; placebo, �21.2, 95%CI, �19.1 to �23.2) or reduction in days of substance use (OROS-MPH: �5.7 days, 95% CI,4.0–7.4; placebo: �5.2 days, 95% CI, 3.5–7.0). Some secondary outcomes favored OROS-MPH,including lower parent ADHD-RS scores at 8 (mean difference � 4.4, 95% CI, 0.8–7.9) and 16weeks (mean difference �6.9; 95% CI, 2.9-10.9) and more negative UDS in OROS-MPH (mean �3.8) compared with placebo (mean � 2.8; p � .04). Conclusions: OROS-MPH did not showgreater efficacy than placebo for ADHD or on reduction in substance use in adolescentsconcurrently receiving individual CBT for co-occurring SUD. However, OROS-MPH wasrelatively well tolerated and was associated with modestly greater clinical improvement onsome secondary ADHD and substance outcome measures. Clinical Trial Registration Infor-mation—Attention Deficit Hyperactivity Disorder (ADHD) in Adolescents with Substance UseDisorders (SUD); http://www.clinicaltrials.gov; NCT00264797. J. Am. Acad. Child Adolesc.Psychiatry, 2011;50(9):903–914. Key Words: osmotic-release methylphenidate, randomizedcontrolled trial, ADHD, substance use disorders
as
I ndividuals with attention-deficit/hyperactiv-ity disorder (ADHD) have at least twice thelifetime risk for substance use disorders (SUD)
compared with non-ADHD controls.1-3 As many
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011
s 30% to 50% of adolescents referred to sub-tance treatment have co-occurring ADHD.4,5
Despite high rates of co-occurrence, ADHD often
goes untreated in community-based substance903www.jaacap.org

cScddpth
mdm1
lshtswa1
A
RIGGS et al.
treatment programs and is associated withpoorer substance treatment outcomes.5-7 Clini-cians may be reluctant to prescribe psychostimu-lants for ADHD in adolescents with SUD becauseof the lack of research on the efficacy and safetyof these agents in substance-abusing youth, orbecause of concerns about medication abuse anddiversion.1,3,8
Only one previous controlled psychostimulantmedication (pemoline) trial has been conductedon adolescents with co-occurring ADHD andSUD, showing pemoline to have greater efficacythan placebo for ADHD but no impact on sub-stance use in the absence of behavioral treatmentfor SUD.9 Additional research is needed to eval-uate whether psychostimulant medications aresafe and effective for ADHD in adolescents withSUD and improve substance treatment out-comes. The current study addresses the need foradditional research addressing whether psycho-stimulant medication is safe and effective forADHD in adolescents with SUD and improvessubstance treatment outcomes. We hypothesizedthat participants treated with OROS-MPH � CBTwould have greater reduction in ADHD symp-toms (ADHD-RS scores, adolescent informant)and in days of past-28-day non-tobacco sub-stance use compared with those treated withplacebo � CBT.
OROS-MPH was selected as the study medi-cation because once-daily dosing would enhancemedication compliance and it is considered tohave lower abuse and diversion liability comparedwith shorter-acting psychostimulant medications.10
Substance treatment, consisting of weekly individ-ual CBT, was provided to all participants to complywith ethical and human subjects’ protection re-quirements to provide standard of care treatmentfor SUD, and was manual-standardized across 11participating sites to reduce variability and poten-tial site effects.
METHODParticipantsParticipants were 303 adolescents (aged 13–18 years)recruited from existing referral sources (e.g., juvenilejustice, social services agencies), primary care andmental health clinics, schools, and media advertisingat 11 community-based substance treatment programsin the National Institute on Drug Abuse (NIDA) Clin-ical Trials Network (CTN). Institutional review boardsapproved the protocol before participant enrollment,
which occurred between March 2006 and September wJOURN
904 www.jaacap.org
2008. Written informed consent was obtained from allparticipants (and parent/guardian for minors) beforebaseline assessment. Criteria for study participationincluded meeting Diagnostic and Statistical Manual ofMental Disorders (Fourth Edition)11 (DSM-IV) diagnosticriteria for current ADHD and at least one non-tobaccoUD. Exclusion criteria were current or past psy-hotic disorder, bipolar disorder, suicide risk, opiateependence, methamphetamine abuse or depen-ence, cardiac illness or serious medical illness,regnancy, past-month use of psychotropic medica-
ions, or participation in other substance or mentalealth treatment.
Randomization and BlindingThe Alza Corporation prepared OROS-MPH andmatching placebo, which was supplied to the CTNcontract pharmacy (EMINENT Services Corporation)by McNeil Consumer and Specialty Pharmaceuticals(distributor for Concerta). Randomization blocks werestratified by site. Sites were provided blinded medica-tion bottles for each randomized participant.
InterventionsMedication. Participants were started on a 18-mgdose of OROS-MPH/matching placebo and titratedto a single, fixed, morning dose of 72 mg (or highestdose tolerated) during the first 2 study weeks,post-randomization.Cognitive-Behavioral Therapy. Participants in both
edication groups received manual-standardized, in-ividual cognitive-behavioral therapy (CBT) usingotivational enhancement approaches throughout the
6-week medication trial.12 The efficacy and feasibilityof training and implementation of the manual-drivenCBT used in this study has been demonstrated inprevious studies, and CBT principles have been widelyadopted and are used in most existing community-basedsubstance treatment programs.13,14 Master’s degree–evel CBT therapists were trained and certified by thetudy’s national trainer (Constance Klein), who waserself trained and certified as both therapist and
rainer by the developer of the manual.13,14 All CBTessions were audio-taped, and approximately 5%ere selected and independently rated for fidelity and
dherence by Constance Klein. Of 147 sessions rated,38 (94%) were rated as adherent.
Diagnostic and Outcome MeasuresK-SADS-E. The Schedule for Affective Disorders andSchizophrenia for School-Age Children- Epidemio-logic Version (K-SADS-E)15 was administered bystudy physicians or masters’ degree–level cliniciansand used to determine current DSM-IV diagnosis of
DHD. Study physicians and masters’ level clinicians
ere trained to administer the K-SADS-E by the PIAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011

ond
smaf
papAgpgA
OROS-MPH FOR ADHD IN ADOLESCENT SUD
(Riggs) and Co-Investigator (Davies) at a 3-day na-tional protocol training (face-to-face) meeting beforeprotocol implementation. Ongoing clinical supervisionrelated to the administration of the K-SADS-E wereaddressed by the PI/lead team on weekly nationalprotocol teleconference calls.Comprehensive International Diagnostic Interview.The Comprehensive International Diagnostic Inter-view (CIDI) is a computer-assisted structured diagnos-tic assessment, administered by research staff, to es-tablish DSM-IV diagnoses of abuse or dependence in11 drug categories: tobacco, alcohol, cannabis, cocaine,hallucinogens, inhalants, opiates, sedatives, phencycli-dine, amphetamines, and club drugs.16 The reliabilityand psychometric validity of DSM-IV substance diag-noses generated by the CIDI in adolescents is wellestablished.16
ADHD Outcome Measures. Because there is no clear“gold standard” outcome measure for ADHD inadolescents, three senior ADHD clinical researchers(Timothy Wilens, M.D., James Swanson, Ph.D., andLen Adler, M.D.) consulted to the NIDA CTN andPI/protocol development team on selection of ADHDoutcome measures. The clinician-administered DSM-IV ADHD Rating Scale17 (ADHD-RS; adolescent infor-mant) was selected by consensus as the most valid,reliable, and feasible primary ADHD outcome mea-sure for this study.17-21 Medical clinicians were trainedto administer the ADHD-RS by completing CD-ROMtraining (developed by Timothy Wilens, M.D.) andrequired to pass a post-training proficiency test and tocomplete booster training and proficiency testing ap-proximately every 6 months throughout the trial. Theseverity of ADHD symptoms was rated by clinicianswho administered the ADHD-RS weekly to adolescentinformants using specific behavioral examples to illus-trate the range of symptom severity for each of 18ADHD symptoms, anchored to ADHD-RS rating scale(0 � never/rarely; 1 � sometimes; 2 � often; 3 � veryoften).Secondary ADHD Outcome Measures. Four mea-sures were used to assess ADHD outcomes. (1)ADHD-RS (parent informant) was administered bymedical clinicians to parents at study weeks 8 and 16.(2) Clinical Global Impression—Improvement (CGI-I)was assessed monthly by medical clinicians who wereblinded to participants’ medication status but whomay have administered ADHD, substance, and ad-verse effects assessment measures. Medical clinicianswere trained in the administration of the CGI-I by thePI/lead investigative team. ADHD treatment responsewas defined a priori as a final CGI-I score of 1 (verymuch improved) or 2 (much improved) with respect tothe participant’s baseline ADHD severity (with scores�2 considered CGI-I nonresponders). (3) The Adoles-cent Relapse Coping Questionnaire (ARCQ)22 con-tained two items which asked participants about
change in their “problem-solving ability” and acquisi- (JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011
tion of “focused coping skills” for managing tempta-tions to use drugs/alcohol at treatment completion.These questions were selected to assess differencesbetween OROS-MPH and placebo treatment groups inparticipants’ acquisition of skills specifically targetedin CBT/substance treatment. (4) The MassachusettsGeneral Hospital (MGH) Liking Scale was used. Onequestion (“Do you think the medication has beeneffective in treating your ADD/ADHD symptoms?”)was taken from the scale and administered at week 16week as a secondary ADHD outcome measure.Substance Outcome Measures. The primary substance
utcome measure is the number of days of past–28-dayon-tobacco drug/alcohol use, assessed using stan-ardized timeline follow-back (TLFB) procedures.23
The validity of adolescent self-reported drug use hasbeen established in a number of previous studies,when confidentiality is assured as it was in the currenttrial.24 The mean number of negative urine drugcreens (UDS) was a secondary substance outcomeeasure. Using negative, as opposed to positive, UDS
voids the problem of imputing a positive UDS resultor any missed weekly sample collections.25
Safety and Treatment Compliance Measures. Safetymeasures included a baseline physical examination, elec-trocardiogram, and a detailed medical and cardiovascu-lar history. Laboratory assessments ascertained at base-line and 16 weeks included liver function tests, completeblood count with differential, and urinalysis. Pregnancytests were performed at baseline and monthly in femalesubjects. Adverse events (AEs) and serious adverseevents (SAEs) were systematically assessed by medicalclinicians during weekly research visits. Medication com-pliance was assessed by pill counts in conjunction withweekly review of subjects’ medication diaries and self-reported medication compliance. Discrepancies betweenpill counts (expected number of returned pills) andadolescents’ self-reported medication compliance diarieswere resolved using the most conservative estimate ofmedication compliance (e.g., assuming lost or unre-turned pills/bottles not taken). The MGH DiversionQuestionnaire, developed by Wilens et al., is a self-administered assessment of the medication misuse/diversion (e.g., selling the medication, taking more thanprescribed, etc.) was completed monthly.
Statistical MethodsStatistical Power and Sample Size. The number of
articipants targeted for randomization nationally,cross all participating sites, was 300 participants (150er treatment arm). The effect size of OROS-MPH forDHD has consistently been shown to be 0.8 orreater in non–substance abusing youth. Thus, a sam-le size of 300 participants was assumed to havereater than 0.8 power to detect a difference inDHD-RS scores between OROS-MPH and placebo
primary aim). Because the impact of psychostimulant
905www.jaacap.org

fpmepaw
chttf
RIGGS et al.
treatment for ADHD (compared with placebo) onsubstance treatment outcomes is not known, the studywas powered to detect an effect size of 0.4 (low-to-medium effect size) or greater on days of past-28-daynon-tobacco substance use at treatment termination.Power was calculated using a procedure and computerprogram described in Hedecker et al.26 and assumingas much as 10% attrition per month.
Primary analyses were intent-to-treat (ITT), includingall randomized study participants, and were conductedusing SAS statistical software. The primary outcomevariables for ADHD and SUD used likelihood basedmethods (i.e., mixed [random coefficient] models withinSAS Proc Mixed version 8.2).27 Because past-28-day druguse differed moderately from normality, results wereconfirmed with more general methods not assumingnormality within SAS Proc GLIMMIX.28
Each outcome was assessed with the same mixedmodel design, including a fixed treatment group effect,a fixed time effect, and a treatment by time interaction,estimating the average group specific intercepts, ratesof change over time, and group specific differences inthose rates, respectively. Linear, quadratic, and cubicrelationships with time in the fixed and random effectswere evaluated, and nonsignificant higher-order termswere dropped to determine the best modeling of time.Fixed site effects were also examined (as a main effectand interaction with time and treatment) and droppedif not significant to simplify model interpretation.Specified random effects that allowed the interceptand curve (e.g., slope) of the lines to vary by subjectand serially correlated residual errors (i.e., spatialpower approach) were considered in determiningmodel fit with likelihood-based procedures.29 ForADHD, “time” consisted of baseline and weekly as-sessments measured as days from randomization. ForSUD, time and corresponding past-28-day use wascalculated “backward” for each subject from that indi-vidual’s final observation in increments of 28 daysbecause of varied study end times resulting from thetrial design and visit windows. This method wasadvantageous in standardizing final 28-day assess-ment periods. Results from these analyses were similarto results computing past-28-day substance use “for-ward” from baseline.
Treatment responses (defined as a CGI-I score of 1 or2) over time (weeks 4, 8, 12, and 16) between groups werecompared using a general linear mixed model approachexpedited by SAS Proc GLIMMIX,28 specifying a binaryoutcome and logit link. Logistic models evaluating dif-ferent relationships with time in the fixed and randomeffects were fit, and fixed site effects were evaluated forinclusion as a main effect and interaction with time andtreatment. Minimum values for the Akaike informationcriterion determined the best model.29 Responder rates atthe end of treatment (i.e., 16 weeks) were comparedbetween groups, with and without using multiple im-
puted values from the general linear mixed model ap-JOURN
906 www.jaacap.org
proach for the missing data.30 These methods all allowor estimates of changes in repeated measures in theresence of missing data, assuming that those data wereissing at random.30,31 The pattern of missing data was
valuated with �2 tests comparing groups at each timeoint. Secondarily, treatment response using the lastvailable assessment was compared between groupsith a �2 test.
All comparisons used a two-tailed, .05 significancelevel. The approach of Hochberg32 was used to ac-ount for multiple endpoints for the two primaryypotheses. Pearson �2 tests were used to compare
reatment differences for categorical variables, and a-test or nonparametric Kruskal–Wallis test was usedor continuous outcomes.
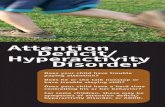
RESULTSPatient DispositionAs shown in Figure 1, a total of 1,334 adolescentswere prescreened, of whom 450 consented andwere screened, and 303 of whom were random-ized to OROS-MPH or placebo and included inITT analyses. There were no statistically signifi-cant differences between groups in study com-pletion, compliance with weekly research visitsor CBT session attendance, or medication com-pliance. The most conservative measure of med-ication compliance, determined by weekly pillcounts of the number returned divided by num-ber of pills prescribed and assuming that nonre-turned pills/bottles were not taken, was 79%.Medication compliance, based on adolescent self-reports, was 82.3% overall.
Demographic and Baseline CharacteristicsThere were no statistically significant differencesbetween groups at baseline on demographics,primary outcomes or other relevant clinical char-acteristics (Table 1). The mean (standard devia-tion [SD]) age was 16.5 (1.3) years, and 78.9% ofthe subjects were male. Race and ethnicity wereself-classified (race: white, 61.7%; African Amer-ican, 23.2%; other, 15.1%; ethnicity: Hispanic,15.2%). At baseline, participants had moderatelysevere ADHD (mean ADHD-RS � 38.7 [8.9]) andreported using non-tobacco substances abouthalf of the days in the past month (mean �14.6/28 days).
Efficacy OutcomesBefore conducting longitudinal analyses, we con-
firmed that there were no statistically significantAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011

OROS-MPH FOR ADHD IN ADOLESCENT SUD
differences between groups with regard to thepattern the percentage of primary outcome datathat were missing (ADHD-RS: OROS-MPH �21.2%; placebo � 24.5%, p � .05; days of substanceuse assessed: OROS-MPH � 11.9%; placebo �16.5%, p � .05). In addition, completers (n � 227)
FIGURE 1 Study flow diagram. Note: CBT � cognitivemethylphenidate.
were not different from noncompleters (n � 76) on
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011
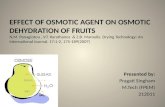
baseline demographic or clinical characteristics(ADHD-RS scores; days of past-28-day substanceuse; number of substance use disorders, all p � .05),and the proportion of completers did not differ bytreatment assignment (p � .05).ADHD. Primary ADHD outcome. Figure 2 illus-
avioral therapy; OROS � osmotic-release
-behtrates the longitudinal course of DSM-IV
907www.jaacap.org

opiate
RIGGS et al.
ADHD-RS scores over time by treatment group.There was a clinically and statistically significantdecrease in ADHD score in both treatmentgroups, but no between-group difference. Theestimated decrease from baseline to study endfor the OROS-MPH � CBT group was �19.2(95% CI, �17.1 to �21.2; p � .001) and for theplacebo � CBT group was �21.2 (95% CI, �19.1to �23.2, p � .001). Likelihood-based criteria
TABLE 1 Baseline Clinical Characteristics by Treatment G
Variable
ADHD SeverityADHD Rating Scale score, mean (SD)
ADHD Diagnostic Subtype, n (%)a
CombinedInattentiveHyperactive-impulsiveNot otherwise specified
Substance SeverityDays/28-day non-tobacco substance use, n (SD)Non-tobacco abuse/dependence diagnoses, n (SD)
Dependence Diagnoses, n (%)b
Cannabis dependenceAlcohol dependenceCocaine dependenceHallucinogen dependenceSedative dependenceAmphetamine dependencePCP dependenceInhalant dependenceOpiate dependenced
Other dependenceAbuse Diagnosis, n (%)b
Alcohol abuseCannabis abuseOpiate abuseHallucinogen abuseSedative abuseAmphetamine abusec
Cocaine abuseInhalant abuseOther abusePCP abuse
Major Depressive Disorder, n (%)Conduct Disorder, n (%)
Note: CBT � cognitive-behavioral therapy; OROS-MPH � osmotic-releasaOne subject did not meet diagnostic criteria for attention-deficit/hype
Hyperactivity Disorder Rating Scale (ADHD-RS) score of �22, but bothbTwo subjects did not meet diagnostic criteria for a non-tobacco substanccExcluding methamphetamine.dCurrent opiate dependence was an exclusion criterion; one subject with
determined that the longitudinal course of ado-
JOURN
908 www.jaacap.org
lescent DSM-IV ADHD-RS score in the ITT sam-ple followed a cubic curve with random subjectand linear time effects and serially correlatedresidual errors.Secondary ADHD outcomes. ADHD-RS parent in-formant. Parent ADHD-RS scores were signifi-cantly lower in participants treated with OROS-MPH � CBT compared with placebo � CBT at 8weeks (OROS-MPH, n � 85, mean score � 26.0
p
OS-MPH � CBT(n � 151)
Placebo � CBT(n � 152)
All(N � 303)
38.1 (9.0) 39.3 (8.8) 38.7 (8.9)
104 (68.9) 104 (68.4) 208 (68.6)43 (28.5) 42 (27.6) 85 (28.1)4 (2.6) 4 (2.6) 8 (2.6)0 (0) 2 (1.3) 2 (0.7)
14 (9.6) 15.1 (9.4) 14.6 (9.5)2.1 (1.2) 1.9 (1.3) 2.0 (1.2)
95 (62.9) 107 (70.4) 202 (66.7)48 (31.8) 42 (27.6) 90 (29.7)11 (7.3) 11 (7.2) 22 (7.3)11 (7.3) 4 (2.6) 15 (5.0)5 (3.3) 3 (2.0) 8 (2.6)3 (2.0) 1 (0.7) 4 (1.3)0 (0) 1 (0.7) 1 (0.3)1 (0.7) 0 (0) 1 (0.3)0 (0) 1 (0.7) 1 (0.3)1 (0 .7) 0 (0) 1 (0.3)
40 (26.5) 40 (26.3) 80(26.4)43 (28.5) 34 (22.4) 77 (25.4)20 (13.2) 17 (11.2 37 (12.2)10 (6.6) 13 (8.6) 23 (7.6)14 (9.3) 8 (5.3) 22 (7.3)6 (4.0) 3 (2.0) 9 (3.0)3 (2.0) 5 (3.3) 8 (2.6)1 (0.7) 4 (2.6) 5 (1.7)1 (0.7) 1 (0.7) 2 (0.7)1 (0.7) 0 (0) 1 (0.3)
19 (12.6) 19 (12.5) 38 (12.5)48 (32) 50 (33) 98 (32.3)
hylphenidate; PCP � phencyclidine.y disorder (ADHD) and one subject did not have an Attention-Deficit/included in analyses.disorder but were included in analyses.
dependence �1 year before study entry was enrolled/randomized.
rou
OR
e metractivit
weree use
[10.5]; placebo, n � 79, mean score � 30.4 [12.5];
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011

9Cp3mr2cf
OROS-MPH FOR ADHD IN ADOLESCENT SUD
mean difference between groups � 4.4; 95% CI,0.8–7.9; p � .0163, t-test) and at 16 weeks (OROS-MPH, n � 84, mean score � 24.0 [11.8]; placebo, n�6 8, mean score � 30.9 [13.0]; mean differencebetween groups � 6.7; 95% CI, 2.9–10.9; p � .001,t-test).CGI-I. When the logit model with a linear timeeffect and random intercept that adjusted for asignificant site effect was implemented via thegeneral linear mixed model, the proportion ofADHD treatment responders (CGI-I score of 1 or2) was surprisingly low in OROS-MPH � CBTgroup (25.5%) and not significantly different (p �.715) from that in the placebo � CBT group(23.2%). Rates of treatment response were evenlower with multiple imputation for missing dataand not significantly different (p � .418) betweenOROS-MPH � CBT (23.4%) and placebo � CBT(19.1%). Similarly, there was not a statisticallysignificant difference (p � .64) in treatment re-sponders based on participants’ last CGI-I rating(OROS-MPH � CBT � 23.6%, n � 144; placebo �CBT�21.3%, n � 141). Of the completers, 26.1%were treatment responders in the OROS-MPH �CBT group (n � 119), and 22.2% were treatmentresponders in the placebo � CBT group (n �108), which was also not statistically differentbetween groups (p � .50). As a validity check ofthe CGI-I measure, CGI-I responders were com-pared with nonresponders with regard to changein ADHD-RS scores in completers. Responders(CGI-I � 1, 2) had significantly greater decline inADHD-RS scores (mean � �26.4 [11.6]) com-pared with nonresponders (CGI-I � 2; mean ��18.8 [11.7], p � .001; mean difference � �7.6,
FIGURE 2 Change in DSM-IV Attention-Deficit/Hyperagroup. Note: Estimates are derived from the cubic longituserially correlated residual errors. OROS � osmotic-relea
95% CI, �11.2 to �4.0; Cohen’s d � 0.66). A
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011
ARCQ change in “problem-solving ability” and“focused coping skills.” Compared with pla-cebo, adolescents treated with OROS-MPH �CBT reported significantly greater improvementin their “problem solving ability” (median differ-ence between groups � 7, favoring OROS-MPH;95% CI, 3–8; P � .002, Cohen’s d � 0.35) andacquisition of “focused coping skills” (mediandifference between groups � 4, favoring OROS-MPH; 95% CI, 1–7; p � .02, Cohen’s d � 0.25).MGH liking scale. In response to the MGH Lik-ing Scale question “Do you feel that your medi-cation has been effective in treating your ADD/ADHD symptoms?”, the median affirmativeresponse was significantly greater in participantstreated with OROS-MPH (median � 6, [5,8] 25th,5th percentile, n � 144) than in those givenplacebo (median � 5 [2,6], n � 141; p � .001,Cohen’s d � 0.56).
Substance Use. Primary substance use outcome. Fig-ure 3 shows the longitudinal course of days ofpast-28-day non-tobacco drug use (TLFB) overtime by treatment group, indicating that therewas a clinically and statistically significant de-crease in both the OROS-MPH � CBT (�5.7 days,5% CI, �7.4 to �4.0; p � .001) and placebo �BT groups (�5.2 days; 95% CI, �7.0 to �3.5;� .001) but no between-group difference (�2 �
.5, 3df, p � .321). Likelihood-based criteria deter-ined that the longitudinal course of adolescent-
eported days of non-tobacco drug use in the past8 days in the ITT sample followed a quadraticurve, with random subject and linear time ef-ects. Table 2 shows the response of the primary
y Disorder Rating Scale (ADHD-RS) scores by treatmentl model with random subject and linear time effects andethylphenidate.
ctivitdinase m
DHD and substance outcome variables based
909www.jaacap.org

RIGGS et al.
on estimates from the longitudinal models (alsosee Figures 2 and 3).
Secondary Substance OutcomesAdolescents treated with OROS-MPH � CBThad significantly more negative UDS (3.8, 95%CI, 3.0–4.6) compared with participants treatedwith placebo � CBT (2.8, 95% CI, 2.1-3.5; p �0.05, Cohen’s d � 0.22), and there was no differ-
FIGURE 3 Change in past 28-day non-tobacco drug utrajectories were modeled based on the assumption of nosample; here, N � 302, one subject did not have valid dselected quadratic longitudinal model with random subjecmethylphenidate.
TABLE 2 Estimated Measures of Attention-Deficit/Hyperaby Treatment Group in the Intent-To-Treat Sample (N � 3
ADHD-RS
OROS-MPH � CBT(n � 151)
Study Week, Meana (95%confidence interval)
Week 0 36.2 (34.6–37.7) 3Week 4 20.6 (19.1–22.1) 2Week 8 18.2 (16.6–19.9) 1Week 12 20.0 (18.1–21.9) 1Week 16 17.0 (14.7–19.3) 1
Note: ADHD-RS � Attention-Deficit/Hyperactivity Disorder Rating Scale; Cdate.
aEstimated ADHD score and number of days of substance use in past 28
random effects derived from the polynomial random coefficient model selecteJOURN
910 www.jaacap.org
ence between groups in the number of UDScollected (11.7 and 11.3, respectively).
Medication Tolerability, Safety,and Adverse EventsOf the participants treated with OROS-MPH,96% achieved the maximum daily dose of 72 mg,and 86.6% sustained this dose throughout thetrial. Participants treated with OROS-MPH had
treatment group. Note: Past 28-day drug usedistribution for the response variable (intent-to-treator this variable). Estimates were derived from thed linear time effects. OROS � osmotic-release
ty Disorder (ADHD) and Substance Use Disorder (SUD)
Treatment Group
SUD (Days of Past 28-Day Non-TobaccoDrug Use)
bo � CBT� 152)
OROS-MPH � CBT(n � 151)
Placebo � CBT(n � 152)
36.1–39.1) 14.0 (12.5–15.4) 15.2 (13.8–16.7)19.9–22.9) 11.0 (9.7–12.4) 11.7 (10.3–13.0)16.5–19.8) 9.1 (7.7–10.5) 9.6 (8.2–11.1)17.5–21.3) 8.2 (6.8–9.6) 9.1 (7.6–10.5)14.1–18.8) 8.3 (6.7–9.9) 10.0 (8.3–11.7)
cognitive-behavioral therapy; OROS-MPH � osmotic-release methylpheni-
. Means are used for predicted individual scores, adjusted for fixed and
se byrmalata ft an
ctivi03)
Place(n
7.6 (1.4 (8.2 (9.4 (6.4 (
BT �
days
d for each variable from likelihood-based criteria.AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011

OROS-MPH FOR ADHD IN ADOLESCENT SUD
more treatment-emergent study-related AEs persubject (mean � 2.4, 95% CI, 1.9–2.9) comparedwith participants given placebo (mean � 1.6, 95%CI, 1.3–1.9; p � .02). More participants treated withOROS-MPH had permanent reductions in theirmedication dose compared with placebo (10.7% vs.6.8%, respectively). Specific AEs treated with pla-cebo (panic/anxiety [one subject]; auditory halluci-nations/vomiting [one subject]; nausea/upper ab-dominal pain [two subjects]; influenza [onesubject]; rash [one subject]; nervousness [one sub-ject]; depressed mood [one subject]; and mass [onesubject]). Eleven SAEs occurred throughout thetrial. Four SAEs occurred in participants treatedwith OROS-MPH, only one of which was judgedas study related, in which a participant wasbriefly hospitalized for evaluation of psychosisafter attending a “rave” at which he ingestedunknown substances. Seven SAEs occurred inparticipants treated with placebo, four of whichwere judged as possibly study related, and whichresulted in brief hospitalizations for syncope,drug toxicity, asthma, and increased aggression,respectively.
In all, 70% of the participants (OROS-MPH,68%; placebo, 72%) reported using drugs or alco-hol on days that they took study medication, butonly 4 (2.8%) taking OROS-MPH and 3 (2.1%)taking placebo reported possible adverse interac-tions between medication and drugs/alcoholtaken on the same day.
Medication Abuse and DiversionThere were no statistically significant differencesbetween OROS-MPH and placebo, respectively, onself-reported medication abuse (“taking more med-ication than prescribed,” 4.8% vs. 2.8%, p � .05) ordiversion (“selling medication to others,” 2.1% vs.1.4%, respectively, p � .05; “letting others take yourmedication,” 3.5% vs. 1.4%, respectively, p � .05),as assessed by the MGH Abuse and DiversionQuestionnaire.
Assessment of Study BlindAt study exit, adolescents and clinicians wereasked to guess whether the adolescent had beenon active medication or placebo during the trial.Of the participants taking OROS-MPH, 59.8%guessed correctly, and of the clinicians 59.7%guessed correctly. Of participants taking placebo,66.7% guessed correctly, and of the clinicians
67.3% guessed correctly. The percentage of correctJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011
guesses was significantly greater than chance basedon �2 tests of association (p � .001) for both theadolescents and clinicians. However, given thatthere were no significant group differences onmeasures relying on adolescent or clinician ratings,it is unlikely that the correct guesses biased the trialtoward finding a medication effect.
DISCUSSIONThe main study finding from this multi-site trialis that OROS-MPH failed to show greater efficacythan placebo for ADHD in adolescents concur-rently receiving CBT as outpatient substancetreatment, based on the primary outcome mea-sure (ADHD-RS, adolescent informant) and medi-cal clinician ratings (CGI-I) of ADHD treatmentresponders (secondary outcome measure). More-over, compared with placebo, participants treatedwith OROS-MPH did not have greater reductionin days of past-month drug use beyond thatachieved in substance treatment with CBT. De-spite nonabstinence in most participants, OROS-MPH demonstrated a fairly good overall safetyprofile and was relatively well tolerated. How-ever, it is important to point out that the studywas not powered to address safety and therewere some safety concerns, including more treat-ment emergent adverse events with OROS-MPHcompared with placebo.
The primary study outcome suggests that clini-cians should refer adolescents with co-occurringADHD and SUD to substance treatment withoutinitiating OROS-MPH, or perhaps any medica-tion, for ADHD before or during substance treat-ment. However, our confidence in this clinicalimplication is somewhat diminished in consider-ation of secondary outcomes favoring OROS-MPH including the following: ADHD-RS scoreswere lower, based on parent informants at 8 and16 weeks; more adolescents treated with OROS-MPH reported that medication was helpful intreating their ADHD; there was greater improve-ment in problem-solving ability and coping skillsfor managing temptations to use drugs/alcohol(targeted in CBT); and there were more negativeurine drug screens.
Although these secondary outcomes suggestedsome “added benefit” of OROS-MPH comparedwith placebo treatment, further consideration ofpotential reasons for failed efficacy on the primaryoutcome measure is warranted in the context of
study limitations, as discussed below.911www.jaacap.org

mAcfipqtt
mticsnwC
cagaftAt(r
sMrsbsssiia(otd
RIGGS et al.
First, was the ADHD-RS, Adolescent Infor-mant, reliable? The validity of the clinician-administered ADHD-RS based on patients asself-informants is well established in adults withADHD.18-21 Because of the paucity of studies inadolescents, there is no current consensus re-garding the most valid outcome measures forADHD in adolescents with or without SUD.However, several studies support the reliabilityof clinician-assessed ADHD symptom severitybased on adolescent informants.4,9,13,14,22-24 In thecurrent study, several steps were taken to en-hance the reliability of the ADHD-RS, includingclinicians’ careful attention to educating adoles-cent participants about ADHD symptoms, whichincluded specific examples to illustrate the rangeof ADHD-RS symptom severity ratings. Giventhe limitations of study design and methodology,we cannot further evaluate the validity of theADHD-RS based on adolescent informants orrule out the possibility of a Hawthorne effect,whereby symptoms may improve in response toexperimental study.
Second, was medication compliance sufficientto support trial validity? Medication compliancewas at least 80% (even by the most conservativemeasure). In addition, participants treated withOROS-MPH reported more psychostimulant-related adverse events. Taken together, this sug-gests that medication compliance was at leastadequate to support trial validity.
Third, was OROS-MPH efficacy compromisedby nonabstinence, given that most participantsreported using drugs/alcohol on days that theytook medication? The results of two previouscontrolled medication trials suggest that the fail-ure of OROS-MPH to separate from placebo inthe current trial is not likely to be explained byparticipants’ nonabstinence. The first was a ran-domized controlled trial of pemoline (a scheduleIII psychostimulant) for ADHD in 69 nonabsti-nent adolescents with co-occurring SUD, inwhich pemoline showed superior efficacy overplacebo for ADHD (effect size � 0.5) but in whichthere was no reduction in substance use in eithergroup in the absence of concurrent substancetreatment.9 Similarly, a controlled trial of atom-oxetine in 147 adults with ADHD and alcohol usedisorders reported greater efficacy for atomox-etine compared with placebo despite nonabsti-nence (effect size � 0.48; 43% vs. 21% symptomreduction, respectively), but no group differences
in alcohol use in the absence of substance treat- oJOURN
912 www.jaacap.org
ent.33 The efficacy of active medication forDHD in nonabstinent participants not receiving
oncurrent substance treatment suggests that theailure of OROS-MPH to separate from placebon the current trial is not likely to be explained byarticipants’ substance use, but it does raise theuestion of whether CBT may have contributedo the more than 50% reduction in ADHD symp-oms in both groups.
Fourth, did CBT contribute to ADHD treat-ent response and failed efficacy? Three con-
rolled psychostimulant (methylphenidate) med-cation trials in nonabstinent adults witho-occurring ADHD and SUD have reportedignificant reductions in ADHD symptoms, buto difference between medication and placebo,hen participants concurrently received weeklyBT for SUD.34-36 The potential contribution of
CBT to failed efficacy was not highlighted orseriously considered in these adult studies pub-lished between 2002 and 2007. However, whenwe obtained similar results in a 12-week con-trolled trial of atomoxetine � CBT (for SUD) in 70adolescents with ADHD and SUD conductedconcurrently with this study and published in2010,37 we did raise the question of whether CBTontributed to the failure of atomoxetine to sep-rate from placebo, given emerging research sug-esting the efficacy of CBT for ADHD indults.38,39 Limitations of study design preventurther determination of the potential contribu-ion of CBT to OROS-MPH’s failed efficacy forDHD in the current trial. However, results of
his study add to a growing suspicion that CBTfor SUD) may contribute to ADHD treatmentesponse and warrants further investigation.
In summary, the primary outcome of thistudy does not support the efficacy of OROS-
PH for ADHD in adolescents who are concur-ently receiving individual CBT as outpatientubstance treatment. However this result shoulde interpreted with caution, and should be con-idered in the context of study limitations andecondary outcomes favoring OROS-MPH, con-istent with the consideration given to multiplenformants and measures in many pediatric med-cation trials. Additional studies are needed thatre specifically designed to address whether CBTfor SUD) contributes to ADHD and perhapsther co-occurring psychiatric symptom reduc-ion. Finally, additional research is needed toetermine the most reliable and valid ADHD
utcome measures and optimal frequency of as-AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011

OROS-MPH FOR ADHD IN ADOLESCENT SUD
sessment in adolescents with co-occurring disor-ders to move the field forward in ways that willincrease scientific knowledge and that may im-prove treatment outcomes for the large subgroupof our nation’s youth. &
Accepted June 14, 2011.
Drs. Riggs, Davies, Mikulich-Gilbertson, and Whitmore, and Ms.Klein, Ms. Macdonald, and Ms. Lohman are with the University ofColorado–Denver. Dr. Winhusen is with the University of Cincinnati.Dr. Leimberger is with the Duke Clinical Research Institute. Dr. Bailey iswith Brown University, and Stanley Street Treatment and Resources,Inc. Ms. Haynes is with the Medical University of South Carolina. Dr.Jaffee is with Harvard University. Dr. Hodgkins is with GatewayCommunity Services. Drs. Trello-Rishel and Tamm are with the Univer-sity of Texas. Dr. Acosta is with the Center for Technology and Healthand National Development and Research Institutes, Inc. Dr. Woodyand Ms. Royer-Malvestuto are with the University of Pennsylvania. Drs.Subramaniam and Fishman are with Johns Hopkins University. Dr.Subramaniam is also with the Division of Clinical Neuroscience andBehavioral Research, National Institute on Drug Abuse (NIDA), Na-tional Institutes of Health (NIH). Dr. Fishman is also with the MountainManor Treatment Center. Ms. Holmes is with the Lexington/RichlandAlcohol and Drug Abuse Council. Ms. Kaye is with the Univer-sity of Pittsburgh. Dr. Vargo and Ms. Hamilton are with Operation PAR,Inc. Dr. Nunes is with Columbia University and the New York StatePsychiatric Institute. Dr. Liu is with the Center for Clinical TrialsNetwork, NIDA, NIH.
The project described was supported by the following grants from theNational Institute on Drug Abuse (NIDA): U10 DA13716 (P.D.R.,R.D.D., S.M.G., C.K., M.M., M.L., E.W.); U10 DA13732 (P.D.R.,T.W., R.D.D., S.M.G., C.K., M.M., M.L., E.W.); U10 DA15831(G.L.B., W.B.J.); U10 DA13727 (L.H., B.W.H.); U10 DA13720(N.H., C.H., M.A.V.); U10 DA20024 (K.T.R., L.T.); U10 DA13035(E.V.N., M.C.A.); K24 DA022412 (E.V.N.); U10 DA13043(C.R.M., G.E.W.); U10 DA13034 (G.S., M.F.); K12 DA000357(G.S.); and U10 DA20036 (M.E.K.). Drug and matching placebowere provided by Ortho McNeil Janssen Scientific Affairs, LLC.
Timothy Wilens, M.D. (Harvard University) provided technical assis-tance for K-SADS-E training, and with Len Adler, M.D. (New YorkUniversity) and James Swanson, Ph.D. (University of California–LosAngeles) served as external consultants to the National Intitute of DrugAbuse (NIDA) and the primary investigator (PI)/lead team on theselection of study outcome measures. Jeffery Leimberger, Ph.D. (DukeClinical Research Institute) and Susan Mikulich-Gilbertson, Ph.D. (Uni-
versity of Colorado–Denver) provided biostatistical expertise. Ashleypsychiatric comorbidity on treatment of adolescent drug abusers.J Subst Abuse Treat. 2004;26:129-140.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011
Kayser, M.A.S. (University of Colorado–Denver) provided experteditorial assistance in preparing the manuscript. Suzell Klein, M.A.(University of Colorado–Denver) and Frankie Kropp, M.S. (Universityof Cincinnati) provided administrative and training support for imple-mentation. The following persons provided site medical support:Georgia Welnick, R.N, (Lexington/Richland Alcohol and Drug AbuseCouncil); Himanshu Upadhyaya, M.D. (Medical University of SouthCarolina); Jill Ridley, R.N. (Synergy Outpatient Services, University ofColorado–Denver); Eileen Duggan, M.D. (Crittenton Children’s Cen-ter); Steven Cuffe, M.D. (Lexington/Richland Alcohol and Drug AbuseCouncil); Charles Maddix, R.N. (Gateway Community Services);Roberto Dominguez, M.D. (University of Miami); Betsy Macaraig,R.N. (Stanley Street Treatment and Resources, Inc.); John Thomas,M.D. (Rehab After Work); Michael Sheehan, M.D. (OperationPAR, Inc.). The following individuals collected data at participatingsites: Ashley Myracle, M.A. (Synergy Outpatient Services, Univer-sity of Colorado–Denver); Michelle Rapoza (Stanley Street Treat-ment and Resources, Inc.); Kim Pressley, M.A. (Lexington/RichlandAlcohol and Drug Abuse Council); John Bensinger, M.A. (AddictionMedicine Services, Western Psychiatric Institute and Clinic, Univer-sity of Pittsburgh Medical Center); Christine Neuenfeldt, Ph.D.(Gateway Community Services); Randi Adelman, N.P. (St. Luke’s-Roosevelt Hospital Center); and Julia Hemphill, B.A. (OperationPAR, Inc.).
The contents of this manuscript are solely the responsibility of theauthors and do not necessarily represent the official views of theNational Institute on Drug Abuse.
Disclosure: Dr. Bailey has received research support from theNational Institute of Drug Abuse (NIDA), Titan Pharmaceuticals,Inc., and Alkermes, Inc. Dr. Trello-Rishel has served on the speakers’bureau for Shire. Dr. Woody is a member of the RADARS Systempost-marketing study external advisory group, which is administeredby Denver Health, and supported by pharmaceutical companies.He has served as a consultant for Alkermes. Drs. Riggs, Winhusen,Davies, Leimberger, Mikulich-Gilbertson, Jaffee, Hodgkins, Whit-more, Tamm, Acosta, Royer-Malvestuto, Subramaniam, Fishman,Vargo, Nunes, and Liu, and Ms. Klein, Ms. Macdonald, Ms.Lohnman, Ms. Haynes, Ms. Hamilton, Ms. Holmes, and Ms. Kayereport no biomedical financial interests or potential conflicts ofinterest.
Correspondence to Dr. Paula D. Riggs, University of Colorado–Denver, Mail Stop F478, 12469 E. 17th Place, Room 235,Aurora, CO 80045; e-mail: [email protected]
0890-8567/$36.00/©2011 American Academy of Child andAdolescent Psychiatry
DOI: 10.1016/j.jaac.2011.06.010
REFERENCES1. Wilens TE, Gignac M, Swezey A, Monuteaux MC, Biederman J.
Characteristics of adolescents and young adults with ADHD whodivert or misuse their prescribed medications. J Am Acad ChildAdolesc Psychiatry. 2006;45:408-414.
2. Kessler RC, Adler L, Ames M, et al. The prevalence and effects ofadult attention deficit/hyperactivity disorder on work perfor-mance in a nationally representative sample of workers. J OccupEnviron Med. 2005;47:565-572.
3. Katusic SK, Barbaresi WJ, Colligan RC, Weaver AL, Leibson CL,Jacobsen SJ. Psychostimulant treatment and risk for substanceabuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. JChild Adolesc Psychopharmacol. 2005;15:764-776.
4. Whitmore EA, Riggs PD. Developmentally informed diagnosticand treatment considerations in comorbid conditions. In: LiddleHA, Rowe CL, eds. Adolescent Substance Abuse: Research andClinical Advances. Cambridge, UK: Cambridge University Press;2006:264-283.
5. Rowe CL, Liddle HA, Greenbaum PE, Henderson CE. Impact of
6. Wise BK, Cuffe SP, Fischer T. Dual diagnosis and successfulparticipation of adolescents in substance abuse treatment. J SubstAbuse Treat. 2001;21:161-165.
7. Grella CE, Hser YI, Joshi V, Rounds-Bryant J. Drug treatmentoutcomes for adolescents with comorbid mental and substanceuse disorders. J Nerv Ment Dis. 2001;189:384-392.
8. Sussman S, Pentz MA, Spruijt-Metz D, Miller T. Misuse of “studydrugs:” prevalence, consequences, and implications for policy.Subst Abuse Treat Prev Policy. 2006;1:15.
9. Riggs PD, Hall SK, Mikulich-Gilbertson SK, Lohman M, KayserA. A randomized controlled trial of pemoline for attention deficithyperactivity disorder in substance abusing adolescents. J AmAcad Child Adolesc Psychiatry. 2004;43:420-429.
10. McBurnett K, Starr HL. OROS methylphenidate hydrochloridefor adult patients with attention deficit/hyperactivity disorder.Expert Opin Pharmacother. 2011;12:315-324.
11. American Psychiatric Association. Diagnostic and Statistical Man-ual of Mental Disorders. 4th ed. Washington, DC: AmericanPsychiatric Association; 1994.
12. Nunes EV, Ball S, Booth R, et al. Multisite effectiveness trials oftreatments for substance abuse and co-occurring problems: have
913www.jaacap.org

RIGGS et al.
we chosen the best designs? J Subst Abuse Treat. Jun 2010;38(Suppl 1):S97-S112.
13. Waldron HB, Kaminer Y. On the learning curve: the emergingevidence supporting cognitive-behavioral therapies for adoles-cent substance abuse. Addiction. 2004;99(Suppl 2):93-105.
14. Waldron HB, Turner CW. Evidence-based psychosocial treat-ments for adolescent substance abuse. J Clin Child AdolescPsychol. 2008;37:238-261.
15. Orvaschel H. Schedule for Affective Disorder and Schizophreniafor School-Age Children Epidemiologic Version. Ft. Lauderdale,FL: Nova Southeastern University, Center for Psychological Stud-ies; 1994.
16. Cottler LB, Robins LN, Helzer JE. The reliability of the CIDI-SAM:a comprehensive substance abuse interview. Br J Addict. 1989;84:801-814.
17. DuPaul GJ, Power TJ, Anastopoulos AD, Reid R. ADHD RatingScale-IV: Checklists, Norms, and Clinical Interpretation. NewYork, NY: Guilford Press; 1998.
18. Adler LA, Faraone SV, Spencer TJ, et al. The reliability andvalidity of self- and investigator ratings of ADHD in adults. JAtten Disord. 2008;11:711-719.
19. Adler LA, Shaw D, Stein MA, et al. Updates in attention-deficit/hyperactivity disorder: current concepts and future develop-ments. J ADHD Relat Disord. 2009;1:63-83.
20. Zhang S, Faries DE, Vowles M, Michelson D. ADHD Rating ScaleIV: psychometric properties from a multinational study as aclinician-administered instrument. Int J Methods Psychiatr Res.2005;14:186-201.
21. Szomlaiski N, Dyrborg J, Rasmussen H, Schumann T, Koch SV,Bilenberg N. Validity and clinical feasibility of the ADHD ratingscale (ADHD-RS): a Danish nationwide multicenter study. ActaPaediatr. 2009;98:397-402.
22. Myers MG, Brown SA. The Adolescent Relapse Coping Question-naire: psychometric validation. J Stud Alcohol. 1996;57:40-46.
23. Sobell LC, Sobell MB. Timeline Follow-back: a technique forassessing self-reported alcohol consumption. In: Litten RZ, AllenJP, eds. Measuring Alcohol Consumption: Psychosocial and Bio-chemical Methods. Totowa, NJ: Humana Press; 1992:41-72.
24. Winters KC. Clinical perspectives on the assessment of adolescentdrug abuse. In: Liddle HA, Rowe CL, eds. Adolescent SubstanceAbuse: Research and Clinical Advances Cambridge, UK: Cam-bridge University Press; 2006:223-240.
25. Ling W, Shoptaw S, Wesson D, Rawson RA, Compton M, Klett CJ.Treatment effectiveness score as an outcome measure in clinical
JOURN
914 www.jaacap.org
trials. Rockville, MD: National Intitute of Drug Abuse (NIDA)Research Monograph 98-4125. 1997;175:208-220.
26. Hedeker D, Gibbons RD, Waternaux C. Sample size estimationfor longitudinal designs with attrition: comparing time-relatedcontrasts between two groups. J Educ Behav Stat. 1999;24:70-93.
27. SAS Institute. The MIXED Procedure. SAS/STAT User’s Guide,Version 8. Cary, NC: SAS Institute; 1999:2083–2226.
28. Schabenberger O. Introducing the GLIMMIX Procedure for Gen-eralized Linear Models. SUGI 30. Cary, NC: SAS Institute; 2007.
29. Jones RH. Longitudinal Data with Serial Correlation: a State-Space Approach. New York, NY: Chapman and Hall; 1993.
30. McCulloch CE, Searle SR. Generalized linear mixed models(GLMMs). In: Generalized, Linear, and Mixed Models. New York,NY: Wiley; 2001:220–246.
31. Brown H, Prescott R. Applied Mixed Models in Medicine. NewYork, NY: Wiley; 1999.
32. Hochberg Y. A sharper Bonferroni procedure for multiple tests ofsignificance. Biometrika. 1988;75:800-802.
33. Wilens TE, Adler LA, Weiss MD, et al. Atomoxetine treatment ofadults with ADHD and comorbid alcohol use disorders. DrugAlcohol Depend. 2008;96:145-154.
34. Levin FR, Evans SM, Brooks DJ, Garawi F. Treatment of cocainedependent treatment seekers with adult ADHD: double-blindcomparison of methylphenidate and placebo. Drug Alcohol De-pend. 2007;87:20-29.
35. Levin FR, Evans SM, Brooks DJ, Kalbag AS, Garawi F, Nunes EV.Treatment of methadone-maintained patients with adult ADHD:double-blind comparison of methylphenidate, bupropion, andplacebo. Drug Alcohol Depend. 2006;81:137-148.
36. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adultADHD patients with comorbid cocaine dependence. Exp ClinPsychopharmacol. 2002;10:286-294.
37. Thurstone C, Riggs PD, Salomonsen-Sautel S, Mikulich-GilbertsonSK. Randomized, controlled trial of atomoxetine for attention-deficit/hyperactivity disorder in adolescents with substanceuse disorder. J Am Acad Child Adolesc Psychiatry. 2010;49:573-582.
38. Safren SA, Sprich S, Mimiaga MJ, et al. Cognitive behavioraltherapy vs relaxation with educational support for medication-treated adults with ADHD and persistent symptoms: a random-ized controlled trial. JAMA. 2010;304:875-880.
39. Solanto MV, Marks DJ, Wasserstein J, et al. Efficacy of meta-
cognitive therapy for adult ADHD. Am J Psychiatry. 2010;167:958-968.AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 9 SEPTEMBER 2011