Ramathibodi IT Lessons Learned
65
1 ถอดบทเรียนการพัฒนาระบบเทคโนโลยี สารสนเทศโรงพยาบาล: โรงพยาบาลรามาธิบดี June 18, 2015 SlideShare.net/Nawanan
-
Upload
nawanan-theera-ampornpunt -
Category
Health & Medicine
-
view
158 -
download
3
Transcript of Ramathibodi IT Lessons Learned

1
ถอดบทเรียนการพัฒนาระบบเทคโนโลยีสารสนเทศโรงพยาบาล: โรงพยาบาลรามาธิบดี
June 18, 2015SlideShare.net/Nawanan

2
• All views & opinions expressed are
those of the presenter alone and do not
represent views or positions of the
Faculty of Medicine Ramathibodi
Hospital or any other affiliated
organizations
Disclaimers

3
Ramathibodi’s
Context

4
• A medical school in Mahidol University
• Established 1965, Operational 1969
• Vision: To be an internationally-recognized
leading medical institution
• Mission: Integrating education, research,
and healthcare services for the society’s
health
• Determination: To be the country’s guiding
light on health
About Ramathibodi

5

6
Ramathibodi’s Organization Chart

7
Item Ramathibodi
Hospital
QSMC SDMC
Strategic
Segmentation
Super-tertiary care
for wide variety of
patients (public &
private)
Excellence center
in advanced,
complex cases
(e.g.
transplantation)
with integrated
wards, ICU, OR,
and private care
Customer-focused
premium services
targeting patients
with private
insurance,
corporate security,
out-of-pocket &
some government
officials
Inpatient Beds 896 Beds 177 Beds
Ramathibodi’s Healthcare Services

8
• 1,087 Total Beds (Rama1=768; QSMC=79; SDMC=240)*
• 70 Wards (Rama1=44; QSMC=8; SDMC=18)*
• 32 OPDs (Regular=17; Premium=15)*
• 118 Inpatient admissions/day (+10 newborns)**
• 6,697 Outpatients/day**
– Regular (Office Hours) 4,259 patients/day
– Special (Non-Office Hours) 1,214 patients/day
– Premium (SDMC) 1,224 patients/day
• 1,155,639 Active Patients*
• 9,000 Full-time Employees*
Ramathibodi At A Glance
*Oct 2014
**Averaged over Oct 2013 - Aug 2014

9
History of
Ramathibodi’s IT
Development

10
• CIO: Dr. Suchart Soranasataporn
• Developed HIS from scratch
• Started from MPI, OPD, IPD,
Pharmacy, Billing, etc.
• Platform: Visual FoxPro (UI, Logic,
Database)
1st Generation (~1987-2001)

11
Visual FoxPro
http://en.wikipedia.org/wiki/Visual_FoxPro

12
• File-based DB, not real DBMS
– Performance Issues
• Not well designed indexing, concurrency controls
& access controls
• Indexes sensitive to network disruptions
• Single point of failures (no redundancy)
– Scalability Issues
• Database file size < 2GB
• Not service-oriented architecture
Some Limitations of Visual FoxPro

13
• Trials & errors
• Individuals or small teams
– Teams based on system modules (OPD, IPD,
Billing, etc.)
• Non-systematic, no documents
1st-Generation Development Process

14
• CIO: Dr. Piyamitr Sritara
• Developed CPOE for inpatients
medication orders
• Lab orders and lab results viewing
• Discharge summaries, etc.
• Enhanced existing HIS modules and add more
modules and departmental systems (e.g. LR, OR)
• Platform: Visual FoxPro (UI, Logic, Database)
2nd Generation (2001-2005)

15
• Java or .NET?
• Open/cost-effective
vs. timely
development
• Technology survival?
• Decision: Defer &
continue using
Visual FoxPro
2nd Generation (2001-2005)
http://thinkunlimited.org/blog/wp-content/uploads/2012/10/Fork_in_the_road_sign.jpg

16
• Small teams
– Teams based on system modules (OPD, IPD,
Billing, Pharmacy, Lab, etc.)
• Realized needs for systematic software
development process
• Started formal systems analysis & design
with some documents
2nd-Generation Development Process

17
• CIO: Dr. Artit Ungkanont
• Continued ongoing projects from
2nd Generation & implemented
– ERP, PACS
• Implemented commercial LIS
• Implemented self-developed web-
based “Doctor’s Portal”
3rd Generation (2005-2011)

18
• Architectural changes: Used middleware (web services,
JBOSS, JCAPS)
• Implemented data exchange of lab & ADT data using
HL7 v.2 & v.3 messaging
• Enhanced existing HIS & add more functions
• SDMC becomes operational (2011)
• Platform:
– Web [Mainly Java] (UI)
– Web services (Logic)
– Oracle & Microsoft SQL Server (Database)
• Legacy platform: Visual FoxPro (UI, Logic, Database)
3rd Generation (2005-2011)

19
• Small teams
– Teams based on system modules (OPD, IPD,
Billing, Pharmacy, Lab, etc.)
• Attempted systematic software
development process, with limited success
• Balancing quality development with timely
software delivery difficult
3rd-Generation Development Process

20
• CIO: Dr. Chusak Okaschareon
• Implemented CPOE for
outpatients (with gradual roll-out)
• Scanned Medical Records for
outpatients
• RamaEMR (portal & EMR
viewer for physicians and nurses
in OPD)
4th Generation (2011-Present)

21
• Ongoing projects
– CMMI & high-quality software testing
– High-Performance Data Center & IT Services (ISO)
– Business intelligence
– Security
• Platform:
– Web [Mainly Java] (UI)
– Web services (Logic)
– Oracle & Microsoft SQL Server (Database)
• Legacy platform: Visual FoxPro (UI, Logic, DB)
4th Generation (2011-Present)

22
• Project-based development
• Roles of “Business Analysts”
• From “silo” teams to “pooled” resources
– Business Analysis Team
– Systems Analysis Team
– Development Team
– Testing Teams
4th-Generation Development Process

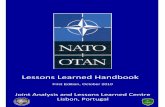
23
Project Deliverables
Good Fast
Cheap
Project Management Dilemma

24 Marchewka (2006)
The Triple Constraint

25
CMMI
Image Source: http://en.wikipedia.org/wiki/Capability_Maturity_Model_Integration

26
Next Step: Chakri Naruebodindra
Medical Institute (Bang Phli)

27
Overview of
Ramathibodi’s
Systems

28
Patient & Bed Management - Inpatient
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

29
CPOE - Inpatient
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

30
Admission Notes
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

31
Discharge Summary
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

32
Discharge Summary (Diagnoses & Operations)
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

33
Lab Orders - Inpatient
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

34
Lab Results - Inpatient
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

35
RamaEMR - Doctor’s Portal
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

36
RamaEMR - Doctor’s Portal
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

37
RamaEMR - Scanned MR Viewer
Screenshots © Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

38
Kiosk for Insurance Eligibility Verification
Photos courtesy of Faculty of Medicine Ramathibodi Hospital, Mahidol University. All rights reserved.

39
Lessons
Learned

40
Lesson #1
“Preemptive
Advantage” of Using
Health IT

41
Resources/capabilities
Valuable ?
Non-Substitutable?
Rare ?
Inimitable ?
NoCompetitive
Disadvantage
Yes
NoCompetitive
necessity
NoCompetitive
parity
Yes
Yes
No
Preemptive
advantage
Yes
Sustainable
competitive
advantage
From a teaching slide by Nelson F. Granados, 2006 at University of Minnesota Carlson School of Management
IT as a Strategic Advantage

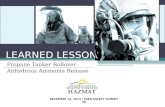
42
Strategic
Operational
ClinicalAdministrative
4 Quadrants of Hospital IT
CPOE
ADT
LIS
EHRs
CDSS
HIE
ERP
Business
Intelligence
VMI
PHRs
MPIWord
Processor
Social
Media
PACS
CRM
Nawanan Theera-Ampornpunt

43
Lesson #2
Customization vs.
Standardization: Always
a Balancing Act

44
Customization: A Tailor-Made Shirt
http://www.soloprosuccess.com/tailor-made-business-blueprint/

45
Customization & Standardization
Customization Standardization

46
Lesson #3
Build or Buy?: A
Context-Dependent,
but Serious Decision

47
Build or Buy
Build/Homegrown
• Full control of software &
data
• Requires local expertise
• Expertise
retention/knowledge
management is vital
• Maybe cost-effective if
high degree of local
customizations or long-
term projection
Buy/Outsource
• Less control of software &
data
• Requires vendor
competence
• Vendor relationship
management is vital
• Maybe cost-effective
if economies of scale or
few customizations

48
Does service offer
competitive advantage?
Is external delivery
reliable and lower cost?
Keep Internal
Keep Internal
OUTSOURCE!
Yes
No
Yes
No
From a University of Minnesota teaching slide by Nelson F. Granados, 2006
IT Outsourcing Decision Tree

49
Does service offer
competitive advantage?
Is external delivery
reliable and lower cost?
Keep Internal
Keep Internal
OUTSOURCE!
Yes
No
Yes
No
From a teaching slide by Nelson F. Granados, 2006
IT Outsourcing Decision
Tree: Ramathibodi’s Case
Core HIS, CPOE
Strategic advantages
• Agility due to local workflow accommodations
• Secondary data utilization (research, QI)
• Roadmap to national leader in informatics (internal “lab”)
External delivery unreliable
• Non-Core HIS,
External delivery higher cost
• ERP maintenance/ongoing
customization
ERP initial
implementation,
PACS, RIS,
Departmental
systems

50
IT Decision as “Marriage”
Image Source: http://charminarpearls.com/pearls/

51
Divorces
Image Source: http://3plusinternational.com/2013/04/divorce-marital-home/
http://www.violetblues.com/breaking-up/financial-cost-of-getting-divorce-3-816.html/attachment/divorce-
money-fight-2

52
Key: Successful recruitment,
sustainable retention,
effective IT management &
patience
“Build”

53
Key: Strong &
trustworthy partnership
with competent partners
“Buy”

54
Lesson #4Be careful of “Legacy
Systems Trap” or
“Vendor Lock-in”

55
Lesson #5
Invest in People

56
• About 100 IT professionals (1:80)– Health informaticians
– Business analysts
– Systems analysts
– Software developers
– Software testers
– Project managers
– Systems & network administrators
– Engineers & technicians
– Data analysts
– Help desk / user support agents
– Supporting staff
• Ratios of IT vs Health from Western countries: 1:50 - 1:60
Ramathibodi IT Workforce

57
Lesson #6
Pay attention to
“Process” (e.g. software
development process,
project management)

58 Image Source: Paragon Innovations, Inc. (2005)

59
People
TechnologyProcess

60
Lesson #7Even large hospitals still
face enormous IT
challenges.

61
Lesson #8Real-world hospital IT
management is messy,
difficult, tiring &
discouraging. Live with it...

62
Lesson #9We can’t live without IT in
today’s health care.
What an exciting time to
be in the field!

63
Ramathibodi hospital’s IT builds
upon its long history of
development and has offered
values to the organization, but it still
has a long way to go, and there is
no “perfect” implementation.
Large rooms for improvement.
Summary

64
ถอดบทเรียนการพัฒนาระบบเทคโนโลยีสารสนเทศโรงพยาบาล: โรงพยาบาลรามาธิบดี
June 18, 2015SlideShare.net/Nawanan

65
Questions?