Rajeev Venugopal - Caribbean Poison Information Networkcarpin.org/p_Chemicals/chemical_burns.pdf ·...
40
Rajeev Venugopal
Transcript of Rajeev Venugopal - Caribbean Poison Information Networkcarpin.org/p_Chemicals/chemical_burns.pdf ·...

Rajeev Venugopal

Aims
• Definition• Classification• Pathophysiology• Special Chemicals• General Management• Local Experience
Definition
• Transfer of potential energy from chemicalreactions, leading to tissue damage.
• The extent of injury is dependent on:– Nature of the agent– Duration of exposure– Concentration

Types of Burn
50%
30%
13%7%
FlameScaldChemicalElectrical

Causes of Burn
79%
4%
17%
AccidentalSelf InflictedAssault

Classification
• Acids: hydrochloric acid, sulfuric acids, chromicacid
• Alkalis: bleach, cement and hydroxidecompounds
• Poison Control Centers have the ability to list thecontents of household and industrial agents.

Pathophysiology
Acids
• Protein injury by hydrolysis
• Thermal injury is made with skin contact

Pathophysiology
Alkali
• Saponification of fat• Hygroscopic effect- dehydrates cells• Dissolves proteins by creation of alkaline
proteinates (hydroxide ions)

Pathophysiology
• Alkalis causes more damage than Acids
• Hydroxide ions causes much deeperpenetration
• Hydrolysis creates a hard eschar whichacts as a barrier
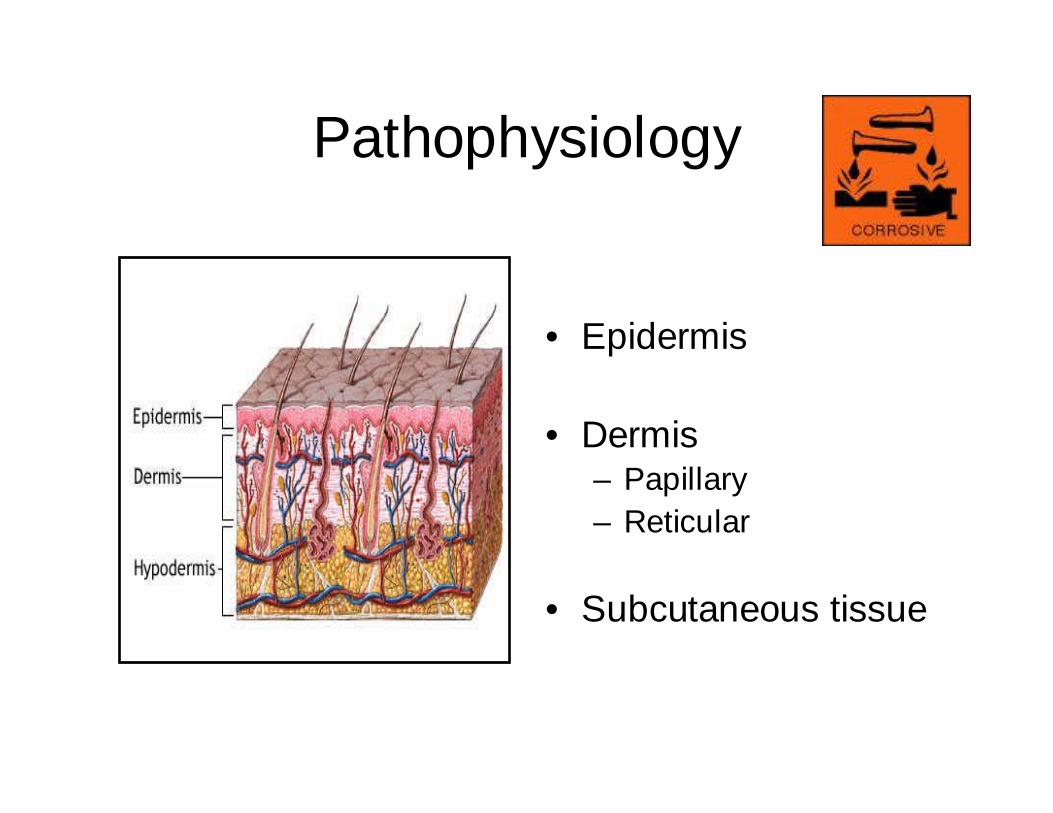
Pathophysiology
• Epidermis
• Dermis– Papillary– Reticular
• Subcutaneous tissue

Management
Prehospital Care
• Remove all clothing• WASH / IRRIGATE/ LAVAGE
– 15 to 20 L– Drain away the effluent– Monitoring pH
• Exception – Powders

Management
• Call The Poison Center to assess theneed for further intervention
• HAZMAT (Hazardous Material)– Contain the materials– Treat the patient

Management
• Neutralization is not recommended– Heat is generated which can potential cause
additional damage.

Management
• All burn patients should be managed astrauma victims.
• ATLS protocol - ABC

Management
Airway and Breathing
• Hydrochloric acid fumes can causepneumonitis

Management
Circulation
• Parklands formula– Percentage of Surface Area Burnt (BSA)– Weight in Kilograms (Wt)
– 4 X BSA X Wt.

Management
80% of assault chemical burns affect thehead and neck
Permanent ocular injury is a real riskIrrigation with normal saline aided with alocal anaestheticAssess corneal injuryOpthalmological consultOphthalmic antibiotic ointments
Management
• Hydrofluoric Acid– Calcium and Magnesium chelation
• Arrhythmias• Pain
– Treatment• 2.5% Calcium gluconate gel• 10% Calcium Gluconate intravenously• Intradermal and intrarterial Calcium gluconate

Management
• Formic Acid– Metabolic acid– Electrolyte disturbance– Haemolysis– Renal Failure– ARDS
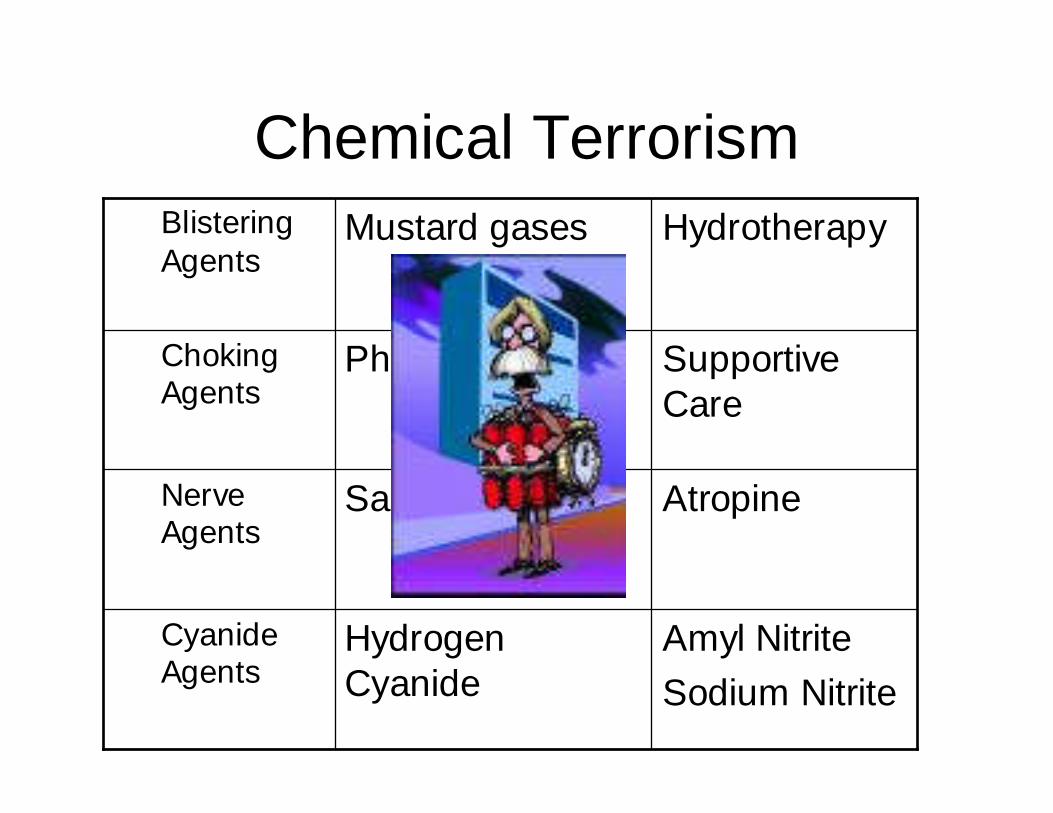
Chemical Terrorism
Amyl NitriteSodium Nitrite
HydrogenCyanide
CyanideAgents
AtropineSarinNerveAgents
SupportiveCare
PhosgeneChokingAgents
HydrotherapyMustard gasesBlisteringAgents
Management
Surgical Options
Escharectomy
CoverageSkin graftsFlaps

Local Experience
• Jamaica held the highest incidence ofchemical assault.– Branday et al 1990 reported a 14% incidence.
• A review of admissions between 1999-2004 had a 10% incidence.
• Stricter penalties for assailants waspassed by the courts

Local Experience
• The aim is to disfigure the victim due to afailed relationship
– The burns involved head and neck in mostinstances followed by extremities
– Third of the patients also had ophthalmologicinvolvement

Local Experience

Local Experience

International Experience
• The current highest incidence of chemicalassault is in Uganda (17%).– Used as a weapon in robberies
• Sri Lanka has also a high incidence and issolely against females.
• Most other centers is secondary todomestic accidents

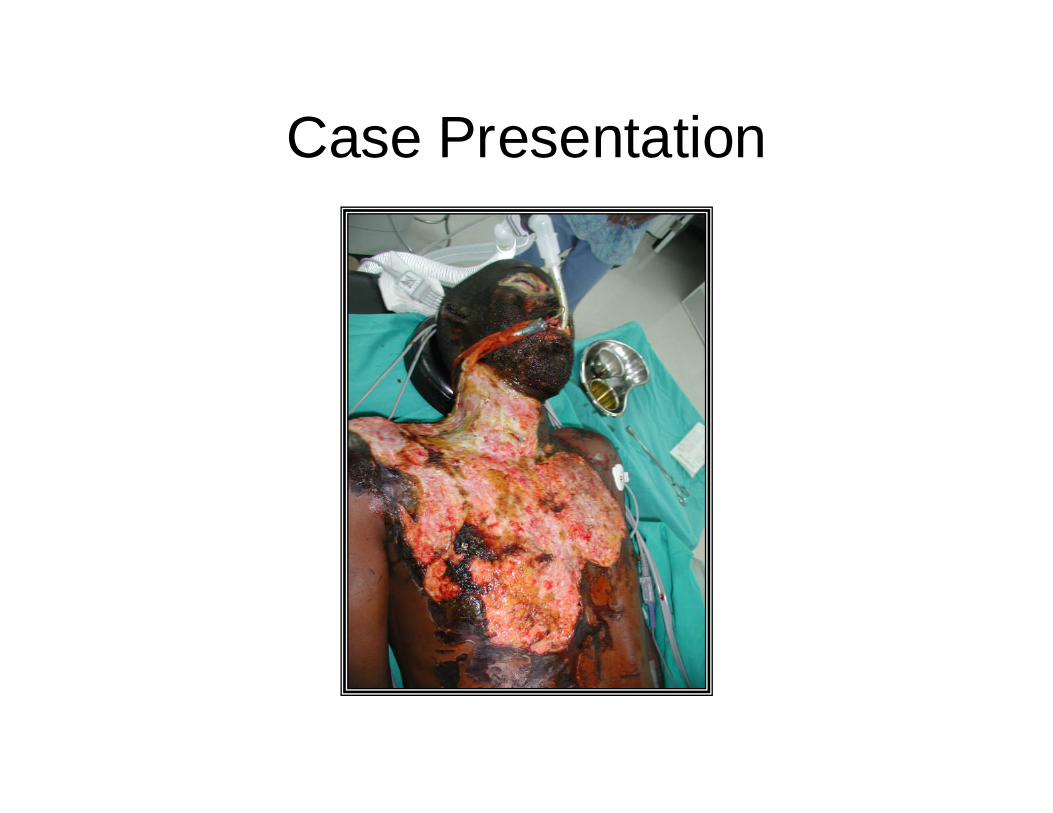
Case Presentation
• 38 year old male who had a dispute withcommon law wife.
• Poured a cleaning agent onto head whileasleep.
• No other significant medical history
• Showered at the scene

Case Presentation
• Transferred to Hospital where he had showeringand irrigation of eyes.
• The injuries affected 18% of Body Surface Area– The entire face including entire cornea bilaterally– The scalp except for the occipital region– The Anterior torso

Case Presentation

Case Presentation
• Noted to have significant renal dysfunction andsevere metabolic acidosis.
• Had escharotomy of the anterior torso and neckwith placement of temporary dialysis catheter.
• Opthamological care– Topical antibiotic– Artificial tears– Corneal chamber
Case Presentation

Case Presentation
• Had staged resurfacing of face and neckwith thick meshed skin grafts.
• Attempt at salvage of cornea with amnioticmembrane.

Case Presentation

Case Presentation

Case Presentation
• Developed ectropions in all four lids whichwas treated with release and full thicknessgrafting.
• The nasal region and scalp where allowedto demarcate.

Case Presentation

Case Presentation

Case Presentation
• Financial Cost
– In Patient Care : > $500000.00
– Productivity Costs
– Disability Costs

Conclusions
• Chemical burns continues to pose aserious problem to our society.
• Penalties must be reinforced
• Public Education