Raised intracranial pressure complicating cryptococcal meningitis: immune reconstitution...
7
Raised intracranial pressure complicating cryptococcal meningitis: immune reconstitution inflammatory syndrome or recurrent cryptococcal disease? Josephine York a , Istvan Bodi b , Iain Reeves a , Paul Riordan-Eva c , Philippa J. Easterbrook a, * a Department of HIV/GUM, The Guy’s, King’s and St Thomas’ School of Medicine, Weston Education Centre, King’s College Hospital, Denmark Hill Campus, Cutcombe Road, London SE5 9RT, UK b Department of Clinical Neuropathology, King’s College Hospital, London, UK c Department of Ophthalmology, King’s College Hospital, London, UK Accepted 29 April 2005 Available online 14 June 2005 KEYWORDS Cryptococcal meningitis; Immune reconstitu- tion inflammatory syndrome (IRIS); Highly active anti-ret- roviral therapy (HAART) Abstract We report the case of a patient with advanced HIV disease and cryptococcal meningitis, who after an initially good clinical and mycological response to systemic anti-fungal treatment developed symptomatic raised intracranial pressure 10 days after initiation of highly active anti-retroviral therapy. We describe the subsequent clinical management and the features that suggest that this persistently raised ICP was more likely due to an immune reconstitution syndrome (IRIS) following HAART rather than relapse of cryptococcal disease or failure of anti- fungal therapy. Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. Introduction A raised intracranial pressure (ICP) (defined as an opening pressure of O20 cm H 2 O) is a recognised complication of cryptococcal meningitis in both HIV-positive and HIV-negative patients, and is associated with a poorer clinical response and increased mortality. 1,2 A raised ICP has also been reported as an uncommon manifestation of immune reconstitution inflammatory syndrome (IRIS) in patients with advanced HIV disease and underlying cryptococcal infection who received highly active anti-retroviral therapy (HAART). 3–8 The clinical spectrum of this syndrome is diverse and IRIS associated mycobacterial, cytomegaloviral, herpes zoster, and pnemocystis carinii infections have also all been described with a characteristic paradoxical deterioration in clinical status following HAART. 3 The pathogenesis of IRIS remains poorly Journal of Infection (2005) 51, 165–171 www.elsevierhealth.com/journals/jinf 0163-4453/$30.00 Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jinf.2005.04.022 * Corresponding author. Tel.: C44 20 7848 5770; fax: C44 20 7848 5769. E-mail address: [email protected] (P.J. Easterbrook).
-
Upload
josephine-york -
Category
Documents
-
view
213 -
download
0
Transcript of Raised intracranial pressure complicating cryptococcal meningitis: immune reconstitution...

Raised intracranial pressure complicatingcryptococcal meningitis: immune reconstitutioninflammatory syndrome or recurrentcryptococcal disease?
Josephine Yorka, Istvan Bodib, Iain Reevesa, Paul Riordan-Evac,Philippa J. Easterbrooka,*
aDepartment of HIV/GUM, The Guy’s, King’s and St Thomas’ School of Medicine, Weston Education Centre,King’s College Hospital, Denmark Hill Campus, Cutcombe Road, London SE5 9RT, UKbDepartment of Clinical Neuropathology, King’s College Hospital, London, UKcDepartment of Ophthalmology, King’s College Hospital, London, UK
Accepted 29 April 2005Available online 14 June 2005
01do
78
(P
KEYWORDSCryptococcalmeningitis;Immune reconstitu-tion inflammatorysyndrome (IRIS);Highly active anti-ret-roviral therapy(HAART)
63-4453/$30.00 Q 2005 The Britishi:10.1016/j.jinf.2005.04.022
* Corresponding author. Tel.: C44 248 5769.E-mail address: philippa.easterbro
.J. Easterbrook).
Abstract We report the case of a patient with advanced HIV disease andcryptococcal meningitis, who after an initially good clinical andmycological responseto systemic anti-fungal treatment developed symptomatic raised intracranialpressure 10 days after initiation of highly active anti-retroviral therapy. We describethe subsequent clinical management and the features that suggest that thispersistently raised ICP was more likely due to an immune reconstitution syndrome(IRIS) following HAART rather than relapse of cryptococcal disease or failure of anti-fungal therapy.Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.
Introduction
A raised intracranial pressure (ICP) (defined as anopening pressure of O20 cm H2O) is a recognisedcomplication of cryptococcal meningitis in bothHIV-positive and HIV-negative patients, and isassociated with a poorer clinical response and
Infection Society. Published by
0 7848 5770; fax: C44 20
increased mortality.1,2 A raised ICP has also beenreported as an uncommon manifestation of immunereconstitution inflammatory syndrome (IRIS) inpatients with advanced HIV disease and underlyingcryptococcal infection who received highly activeanti-retroviral therapy (HAART).3–8 The clinicalspectrum of this syndrome is diverse and IRISassociated mycobacterial, cytomegaloviral, herpeszoster, and pnemocystis carinii infections have alsoall been described with a characteristic paradoxicaldeterioration in clinical status following HAART.3
The pathogenesis of IRIS remains poorly
Journal of Infection (2005) 51, 165–171
www.elsevierhealth.com/journals/jinf
Elsevier Ltd. All rights reserved.

J. York et al.166
understood, but is thought to be due to increasedinflammatory activity to antigens in tissues frompre-existing infections following recovery of thehost’s immune system.
We report a case of a patient with cryptococcalmeningitis who after an initially good clinical andmycological response to systemic anti-fungal treat-ment developed symptomatic raised intracranialpressure 10 days after initiation of highly activeanti-retroviral therapy (HAART). The case high-lights the difficulties in differentiating between araised ICP due to persistent or recrudescentcryptococcal infection and that due to IRIS, whichhas important implications for appropriate clinicalmanagement.
Case history
A 34-year-old Jamaican woman, who had beenresident in the U.K. for 4 years, presented with a3-day history of severe headache, photophobia,nausea and vomiting. Two weeks prior to admission,she had been diagnosed with advanced HIV infec-tion (CD4 cell count: 9!106/l; viral load (VL)O500 000 copies/ml). She was apyrexial with mildneck stiffness but no focal neurological deficit orevidence of papilloedema. CSF examination showeda normal opening pressure (OP) of 9.5 cm H2O,protein 290 mg/l, glucose 3.1 mmol/l, white cell
Figure 1 Clinical course of cryptococcal meningitis showintherapy, and HAART in relation to raised ICP and CSF results oflucytosine; Flcn, fluconazole; +, CSF drainage.
count (WCC) !5/mm3, and red cells !5/mm3.India ink stain and culture were positive forCryptococcus neoformans, and cryptococcal anti-gen titre (CRAG) was 1:640. An MRI brain scanshowed a well defined, non-enhancing 15 mm cysticlesion on the left choroid fissure, with smallperivascular spaces present bilaterally (also non-enhancing). The remaining brain and ventricleswere unremarkable. She received 2 weeks ofintravenous liposomal amphotericin B(1 mg/kg/day increasing to 3 mg/kg/day) andflucytosine (150 mg/kg/day) (first anti-fungalcourse), with good clinical response. Maintenancefluconazole 400 mg daily, and HAART (zidovudine,lamivudine and nevirapine) were then commenced.Fig. 1 shows the time course of CSF results, anti-fungal and HAART therapy over the subsequent 6months.
Thirty-one days after initiation of anti-fungaltherapy (17 days after change from systemic anti-fungal therapy to oral fluconazole), and 10 daysafter initiation of HAART she developed a severeheadache and blurred vision, in association withpapilloedema and a left visual field defect. A CT(computed tomography) brain scan showed persist-ence of the left choroid fissure lesion, but noevidence of hydrocephalus. CSF OP was 39.5 cmH2O, protein 535 mg/l, glucose 3.4 mmol/l, WCC!5/mm3, India ink stain was positive, culture wasnegative, and CSF CRAG was 1:20. Intravenous
g the timing of the three courses of systemic anti-fungalver 6 months. OP, opening pressure; A, amphotericin B; F,

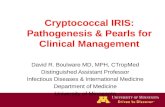
Figure 2 (A) Coronal section of the brain demonstratescystic necrotic changes in the left hippocampus and, lessprominent, tiny cystic areas in the basal ganglia. (B)Granulomatous cryptococcal meningoencephalitis withonly a few cryptococci around deep leptomeningeal bloodvessels (!200, H&E). (C) Numerous cryptococci withassociated inflammatory reaction in the left hippocampus(!300, PAS-diastase).
Raised intracranial pressure complicating cryptococcal meningitis 167
liposomal amphotericin B and flucytosine wererestarted and continued for 4 weeks (second anti-fungal course), followed by maintenance flucona-zole 400 mg daily. Daily lumbar punctures (LP) wereperformed for CSF drainage for 7 days withsymptomatic improvement and reduction of theOP to 20 cm H2O. However, 5 days after the last LP,her symptoms returned with a raised ICP of 41 cmH2O. An external lumbar drain was inserted, whichover the next 10 days continued to drain between 5and 10 ml of CSF hourly, and so was replaced by alumboperitoneal shunt. This was ligated after 1week when she developed a severe headache and aCT scan showed imminent cerebellar tonsillarconing. Despite continued clinical improvement,new choroidal lesions in both eyes were noted14 days after discontinuing systemic anti-fungaltherapy suggestive of recurrent focal cryptococcaldisease. Yeast like organisms was seen on CSFmicroscopy, protein was 316 mg/l, glucose1.8 mmol/l, culture was negative and CRAG titrewas 1:1. Analysis of her original CSF isolate showedsusceptibility to amphotericin, flucytosine andfluconazole with minimal inhibitory concentrationlevels of 0.5, 4 and 8 mg/l, respectively. Because ofcontinuing concerns about the adequacy of CSFpenetration of her anti-fungal drugs particularlywith amphotericin, fluconazole 800 mg twice dailyand flucytosine (150 mg/kg/day) were started(third anti-fungal course), with continuing resol-ution of the papilloedema and choroidal lesions. Inher HAART regimen, zidovudine was substitutedwith abacavir in view of persistent transfusion-dependent anaemia and she was discharged fromhospital 12 weeks after initial presentation.
Over the next 6 weeks she remained symptom-free, and 10 weeks after commencing HAART, herVL was !50 copies/ml and CD4 cell count: 59!106 cells/l. She was then readmitted with arecrudescence of headache, meningeal signs, andpapillodema. MRI scan showed a reduction in size ofthe left choroid fissure cyst consistent with recentrupture, and the presence of a new small right sidedposterior internal capsule lesion, both with mildcontrast enhancement. CSF OP was 40 cm H2O,protein 434 mg/l, India ink stain and culture werenegative, and CRAG titre was 1:1. She had alternateday therapeutic LPs on three occasions and theninsertion of an external lumbar drain. The followingday, she had a cardio respiratory arrest, and wasconfirmed brain-stem dead—5 months following herinitial presentation and diagnosis. A CT scan showedcerebral oedema and parieto-occiptal infarctionsecondary to transtentorial and foramen magnumherniation.
At post-mortem, macroscopic examination
revealed a prominently swollen brain with groovedcerebellar tonsils. However, no definite herniationwas present and no infarct was confirmed. Coronalsectioning showed cystic necrotic changes in theleft hippocampus and, less prominent, tiny cysticareas were also seen in the basal ganglia (Fig. 2(A)).Histological examination confirmed a widespread

Table 1 Previous reports of HAART-induced IRIS in association with central nervous system cryptococcosis
Author No. ofcases
Previouscryptococcalmeningitis
Baseline CD4(!106/l)and VL(copies/ml)
Time fromHAART toonset ofsymptoms
CD4 (!106/l)and VL(copies/ml)at onset ofsymptoms
CSF WCC(cells/mm3)
CSFpro-tein(mg/l)
CSF OP(cm H2O)
CSFCrAg
Treatment
Shelburne et al.3 1 Yes 76, 238 000 11 days 138, 11 000 71 2550 – 1:2048 Rapid resolutionof symptoms withreducing course ofdexamethasone,recurrence ofsymptoms severalweeks later:steroids restartedwith good clinicalresponse
Woods et al.4 3 No 5, 230 000 4 days –, – 14!103/l 452 – – Antifungal RxNo 30, – 39 days – 3!103/l 532 28 – Antifungal RxYes 40, 480 000 10 days –, 1300 1x105/l 1055 – 1:200 Continued on
maintenanceitraconazole, signsand symptomsresolved over 2weeks
Jenny-Avital andAbadi5
2 Yes 10, 45 496 4 months 223, !50 17 – 34 1:32 Headachesresolved after 2weeks of serial LPsand amphotericinB
Yes 47, 224 000 10 months 306, !50 149 – 39 1:1 Symptoms and CSFpleocytosis even-tually resolvedwith amphotericinB and serial LPsover a 3-weekperiod
J.York
etal.
168

Cinti,Arm
strong
andKau
ffman
61
Yes
67,65
000
03weeks
370,
537
500
1520
331:81
92Continued
maintenan
cedose
offluco
nazole.
After2weeks
his
CSF
WBCan
dCrAg
had
improve
d.
Asymptomatic
after4weeks
and
norm
alOPafter6
weeks
Kingetal.7
1Yes
41,75
000
4weeks
44,!40
010
710
–1:32
Failedto
respond
toam
photericinB
alonean
dsymp-
tomsprogressed
promptly.
Raised intracranial pressure complicating cryptococcal meningitis 169
granulomatous cryptococcal meningoencephalitis,mainly affecting the deep sulci and invadingsurrounding brain parenchyma. Only a few crypto-coccal organisms were seen within the areas withgranulomatous inflammation (Fig. 1(B)). The hippo-campi, however, revealed cystic necrosis withnumerous cryptococci and inconspicuous inflamma-tory reaction (Fig. 2(C)). Granulomatous crypto-coccal inflammation was also demonstrated in bothoptic nerves.
Discussion
This patient with advanced HIV disease andcryptococcal meningitis developed symptomaticraised intracranial pressure characterised by severeheadache, vomiting, loss of visual acuity andpapillodema 10 days after starting HAART and17 days after a good clinical and mycologicalresponse to anti-fungal therapy. This was initiallyinterpreted and managed as persistent cryptococ-cal infection on the basis of evidence of newcryptococcal choroidal lesions. However, the raisedICP persisted despite a total of 10 weeks of systemiccombination anti-fungal therapy and 5 months of allanti-fungals, in association with both negative CSFfungal cultures and a low positive CSF CRAG titre.
Several features suggest that this persistentlyraised ICP was more likely due to an immunereconstitution syndrome following HAART ratherthan relapse of cryptococcal disease or failure ofanti-fungal therapy alone: (i) there was an initialgood clinical response (declining fever, reducingmeningeal symptoms, and improving mental status)and mycological response (all CSF cultures negativeand a marked reduction in CSF CRAG titre from1:640 to 1:1) to the initial course of anti-crypto-coccal therapy; (ii) the recurrence of meningealsymptoms with new onset raised ICP occurred10 days after initiation of HAART; (iii) the patienthad advanced HIV immunodeficiency at initiation ofHAART (CD4 cell count 9!106 cells/ml) and had amarked immunological and virological response toHAART (a six-fold increase in CD4 count from 9 to59!106 cells/l and a O5 log decrease in VL fromO500 000 to !50 copies/ml after 10 weeks ofHAART); (iv) there was no mycological evidence ofpersistent cryptococcal infection (all CSF culturesremained negative and the CSF CRAG titre was at alow positive titre of 1:1 following the initial anti-fungal course); (v) there was no evidence ofresistance to anti-fungal agents on the initialpositive CSF culture, although there were nofollow-up positive CSF cultures available for further

J. York et al.170
testing; (vi) there was evidence of an inflammatoryprocess with raised ICP and CSF protein, togetherwith the presence of diffuse leptomeningealinflammation on biopsy—an uncommon finding inHIV-positive patients.11 The absence of a cellularresponse in any of our patient’s CSF samples whichis typically associated with an immune reconstitu-tion profile is likely to be explained by the patient’ssevere immunodeficiency even after a six-fold risein the CD4 cell count to 59 cells.
Features consistent with persistent or relapse ofcryptotococcal infection include the developmentof new cryptococcal choroidal lesions after 8 weeksof anti-fungal therapy; the presence of a probablecryptococcoma in the choroid fissure and develop-ment of a new lesion in the left internal capsule onfollow-up CT scan; the presumed premorbid ruptureof the internal capsule cryptococcoma; and thepost-mortem findings of severe cryptococcal inva-sion present in the left hippocampus causing almosttotal destruction and cystic cavitation. However,this evidence of persistence of cryptococcal infec-tion is still not inconsistent with IRIS as the primarypathology accounting for the raised intracranialpressure, whereby there is an enhanced immuneresponse against residual C. neoformans as a resultof HAART therapy.
There are several possible mechanisms for theraised intracranial pressure in our patient. None ofthe CT or MRI scans showed any evidence ofventricular dilatation consistent with obstructivehydrocephalus, and although small lesions noted inthe choroid fissure and internal capsule weresuggestive of cryptoccomas, there were no localisingneurological signs or evidence of mass effect. It ismore likely that the raised ICP resulted from intensemeningeal inflammation due to a combination of IRISand residual infection. It is also possible that therewas a degree of communicating hydrocephalusresulting from interference with CSF reabsorption inthe arachnoid villi due to the initially high levels offungal polysaccharide antigen.
To date, there have been 22 cases of IRIS centralnervous system (CNS) complications associatedwith cryptococcal meningitis following HAARTreported in the literature,3–8 and a further eightcases of IRIS associated with non-CNS cryptococco-sis.3,5,8 Table 1 summarises the characteristics ofeight cases of IRIS CNS cryptococcal disease fromsix case reports.3–7 Six of these eight casespresented during the treatment of confirmedcryptococcal meningitis, while two were newpresentations of a pre-existing but clinically silentinfection following the initiation of HAART. Themedian time from initiation of HAART to onset ofIRIS-related symptoms was 25 days (range 4 days to
10 months). Half of the cases presented with raisedICP, and seven had an accompanying CSF leucocy-tosis. The median CD4 cell count and viral load was40!106/l and 225 000 copies/ml, respectively, atbaseline, and 223!106/l and 470 copies/ml,respectively, at onset of symptoms.
There is limited data on factors predictive of thedevelopment of IRIS, but a low baseline CD4 cellcount12 and younger age at HAART initiation13 havebeen identified. In a recent retrospective cohortstudy by Shelburne et al.8 of 84 patients with aprevious diagnosis of cryptococcal neoformans infec-tion, 18 of the 66 patients who received HAARTsubsequently developed IRIS. Factors associatedwithan increased risk of developing IRIS included moresevere cryptococcal disease (higher CSF CRAG andlonger duration of anti-fungal treatment), and bothtiming and response to HAART (no prior HAART, ahigher initial VLandaO2 logdroppostHAART,aO50cell increase in CD4 count, and commencing HAARTwithin30days of cryptococcal diagnosis). A raised ICPwas also significantly more common among patientswith IRIS. The majority of these predictive factorswere present in our patient: she was anti-retroviraltreatment naı̈ve, HAART was started within 30 daysof initial diagnosis, initial viral load wasO500 000 copies/ml, and there was a O2 log dropin her VL, with a 50 cell increase in her CD4 count.Taken together with the timing of onset of thepersistently raised ICP in relation to HAART, theclinical features and pathological characteristics inour patient were most consistent with an IRIS typephenomenon.
There are several management options for raisedintracranial pressure, and in the absence of a spaceoccupying lesion, mechanical decompression of theCSF pressure has been found to be the mosteffective way of controlling ICP.2 The currentguidelines recommend aggressive decompressionof the CSF volume with either sequential or dailylumbar punctures if the pressure is above 25 cm, orinsertion of a lumbar drain or placement of aventriculperitoneal shunt if the elevated pressureremains persistently high, or if the initial presen-tation is with a very high opening pressure (O40 cmH2O). However, unfortunately in our patient the useof a lumbar drain was associated with labile controlof the ICP and resulted in fatal coning. Nursingguidelines in patients with lumbar drains rec-ommend hourly neurological observation andmeasurement of CSF drainage which should gener-ally be between 5 and 10 ml/h, to maintain a CSFpressure of approximately 10 cm H2O.
14 Patientactivities should be restricted to the minimum, anda body position maintained to keep the drain belowthe level of the ear lobe. In addition to potential

Raised intracranial pressure complicating cryptococcal meningitis 171
over-drainage, other complications associated withthe use of lumbar drains, lumboperitoneal andventricular shunts include drain or shunt infection,distal catheter migration, and need for shuntrevision. The use of ventricular shunts has beenassociated with a lower risk of shunt obstructionand revision than lumboperitoneal shunts.15 Medi-cal approaches to control ICP such as corticoster-oids, acetazolamide and mannitol have not beenshown to be effective in HIV-negative patients2,9
and currently they are not recommended in themanagement of elevated ICP associated with AIDSrelated cryptococcal meningitis. However, it isnoteworthy that two of the eight cases of IRISassociated cryptococcal meningitis in the caseseries summarised in Table 1 received steroids,and both experienced a prompt clinical improve-ment following the addition of dexamethasone.7,8
Steroids are now also increasingly used as atreatment strategy for certain IRIS events such asmycobacterial disease, toxoplasmosis and PCP.10
The increasing availability of HAART in areas ofthe world with endemic cryptococcal disease suchas sub-Saharan Africa, presents an opportunity tofurther define the incidence and spectrum of IRISassociated cryptococcal disease, as well as themost appropriate duration of anti-fungal therapybefore initiation of HAART, and the role of steroids.For now, the main clinical lessons from this casereport to date are: that exacerbation of meningealsymptoms in HIV-positive patients receiving treat-ment for cryptococcal meningitis does not necess-arily imply treatment failure requiring an increaseor change in anti-fungal therapy; the importance ofconsidering immune reconstitution as a cause ofraised intracranial pressure following cryptococcalmeningitis in a patient recently started on HAART;and to consider corticosteroids as a managementoption, when both optimal anti-fungal therapy hasbeen given and maintained, and response tomechanical drainage has been poor or associatedwith complications.
References
1. Graybill JR, Sobel J, Saag M, Van Der Horst C, Powderly W,
Cloud G, et al. Diagnosis and management of increasedintracranial pressure in patients with AIDS and cryptococcalmeningitis. Clin Infect Dis 2000;30:47–54.
2. Saag MS, Graybill RJ, Larsen RA, Pappas PG, Perfect JR,Powderly WG, et al. Practice guidelines for the managementof cryptococcal disease. Clin Infect Dis 2000;30:710–8.
3. Shelburne SA, Hamill RJ, Rodriguez-Barradas MC,Greenbery SB, Atmar RL, Musher DW, et al. Immunereconstitution inflammatory syndrome: emergence of aunique syndrome during highly active antiretroviral therapy.Medicine (Baltimore) 2002;81(3):213–27.
4. Woods ML, MacGinley R, Eisen DP, Allworth AM. HIVcombination therapy: partial immune restitution unmaskinglatent cryptococcal infection. AIDS 1998;12(12):1491–4.
5. Jenny-Avital ER, Abadi M. Immune reconstitution crypto-coccosis after initation of successful highly active antire-troviral therapy. Clin Infect Dis 2002;35:e128–e33.
6. Cinti S, Armstrong W, Kauffman C. Case report. Recurrenceof increased intracranial pressure with antiretroviral therapyin an AIDS patient with cryptococcal meningitis. Mycoses2001;44:497–501.
7. King M, Perlino C, Cinnamon J, Jernigan J. Paradoxialrecurrent meninigitis following therapy of cryptococcalmeninigitis: an immune reconstitution syndrome afterinitiation of highly active antiretroviral therapy. Int J STDAIDS 2002;13:724–6.
8. Shelburne SA, Visnegarwala F, Darcourt J, Graviss EA,Giordan TP, White Jr AC, et al. Incidence and risk factorsfor immune reconstitution inflammatory syndromeduring highly active antiretroviral therapy. AIDS 2005;19(4):399–406.
9. Newton PN, Thai le H, Tip NQ, Short JM, Chierakul W,Rajanuwong A, et al. A randomised, double-blind, placebo-controlled trial of acetazolamide for the treatment ofelevated intracranial pressure in cryptococcal meningitis.Clin Infect Dis 2002;35(6):769–72.
10. French MAH. Immune restoration diseases in HIV-infectedpatients on HAART. AIDS Read 1999;9(8):548–9 [see alsop. 554–5 and 559–62].
11. Lee SC, Dickson DW, Casadevall A. Pathology of cryptococcalmeningoencephalititis: analysis of 27 patients with patho-genic implications. Hum Pathol 1996;27:839–47.
12. French MA, Lenzo N, John M, Mallal SA, McKinnon EJ,James IR, et al. Immune restoration disease after thetreatment of immunodeficient HIV-infected patients withhighly active antiretroviral therapy. HIV Med 2000;1:107–15.
13. Thevarajan I, Chiu C, Murad S, Easterbrook PJ. Epidemiologyof immune reconstitution inflammatory syndrome (IRIS) in anethnically diverse HIV infected cohort. 9th European AIDSconference, Warsaw, Poland 2003 [abstract no. 21].
14. Jones CC, Caynird CH. Care of intracranial pressuremonitoring devices. A nursing responsibility. J NeurosurgNurs 1982;14(5):255–61.
15. McGirt MJ, Woodworth G, Thomas G, Miller N, Williams M,Rigamonti D, et al. Cerebrospinal fluid shunt placement forpseudotumor cerebri-associated intractable headache: pre-dictors of treatment response and an analysis of long-termoutcomes. J Neurosurg 2004;101(4):627–32.