
Radiotherapy with concurrent or sequential
7
RADIATION ONCOLOGY—ORIGINAL ARTICLE Radiotherapy with concurrent or sequential temozolomide in elderly patients with glioblastoma multiforme Sameh A Hashem, 1 Ahmed Salem, 1 Abdulla Al-Rashdan, 1 Najeeb Ezam, 2 Ala’a Nour, 1 Amer Alsharbaji, 4 Chandrababu Rejeeth, 5 Issa Mohamad, 1 Maher Sughayer, 2 Maher Elyan, 4 Maysa Al-Hussaini, 2 Ala’ Addasi 3 and Abdelatif Almousa 1 Departments of 1 Radiation Oncology, 2 Pathology and Laboratory Medicine, 3 Medical Oncology, 4 Surgery, King Hussein Cancer Center, Amman, Jordan and 5 Department of Zoology, School of Life Sciences, Bharathiar University, TamilNadu, India SA Hashem MD; A Salem MD; A Al-Rashdan MD; N Ezam MD; A Nour MD; A Alsharbaji MD; C Rejeeth MSc; I Mohamad MD; C Rejeeth MSc; M Sughayer MD; M Elyan MD; M Al-Hussaini MD; A Addasi MD; A Almousa MD, PhD. Correspondence Dr Abdelatief Almousa, Department of Radiation Oncology, King Hussein Cancer Center, PO Box 1269 Al-Jubeiha, Queen Rania Al Abdullah Street, Amman 11941, Jordan. Email: [email protected] Competing interests: None. Submitted 12 April 2011; accepted 17 July 2011. doi:10.1111/j.1754-9485.2011.02325.x Abstract Objective: The objective of this article was to evaluate therapeutic outcomes of elderly patients with glioblastoma multiforme (GBM) treated by surgery fol- lowed by combined modality therapy and compare achievable outcomes to those of a younger age population. Methods and Materials: Seventy-eight adult patients with histologically con- firmed grade IV astrocytoma were treated at King Hussein Cancer Center (Amman, Jordan) between September 2004 and December 2008. Records were retrospectively reviewed and included 55 males and 23 females between 19 and 78 years of age (median age 50 years). This case series included 20 patients aged 60 years or older. All patients underwent craniotomy followed radiotherapy and concurrent or sequential temozolomide. The follow-up ranged from 1 to 56 months (median 9.4 months). Results: The median survival for the whole cohort was 13.8 months. The median survival for patients less than 60 years was 14.3 months and for patients 60 years or older was 12.3 months (P = 0.19). Among elderly patients, radical surgical resection (P = 0.002), concurrent delivery of chemo- radiation (0.041) and radiotherapy dose 5400 cGy (P = 0.0001) conferred statistically significant improvements in overall survival. Conclusion: Management of GBM in elderly patients should include maximal surgical resection followed by radiotherapy and temozolomide whenever medically feasible. Outcomes comparable to those obtained in younger age groups can be expected. Our results indicate that concurrent chemoradiation is superior to sequential chemoradiation in these patients. Key words: concurrent; elderly; GBM; radiotherapy; sequential; temozolomide. Introduction Despite the widespread adoption of multimodality therapy, the diagnosis of glioblastoma multiforme (GBM) continues to carry a dismal prognosis with a grave overall survival estimate set at 9–12 months. 1–3 Historically, surgery followed by radiotherapy was considered the standard of care. 3 In 2005, Stupp et al. 4 demonstrated that temozolomide administered in addition to adjuvant radiotherapy significantly prolongs overall survival. Cur- rently, temozolomide concurrent with radiotherapy fol- lowed by adjuvant temozolomide has been adopted as the new standard of care. Prognosis of elderly patients with GBM is grim with an overall survival ranging from 4 to 8 months. 5 Furthermore, management of elderly patients with GBM is still hindered by the paucity of clear protocols due in part to the exclusion of this age group from the majority of randomised trials in this field. As a consequence, debate is unfolding as to whether these patients would benefit from aggressive surgical resection Journal of Medical Imaging and Radiation Oncology 56 (2012) 204–210 © 2012 The Authors Journal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 204
-
Upload
jordan-medics -
Category
Documents
-
view
224 -
download
1
description
Radiotherapy with concurrent or sequential temozolomide in elderly patients with glioblastoma multiforme Sameh A Hashem,1 Ahmed Salem,1 Abdulla Al-Rashdan,1 Najeeb Ezam,2 Ala’a Nour,1 Amer Alsharbaji,4 Chandrababu Rejeeth,5 Issa Mohamad,1 Maher Sughayer,2 Maher Elyan,4 Maysa Al-Hussaini,2 Ala’ Addasi3 and Abdelatif Almousa1 Departments of 1Radiation Oncology,
Transcript of Radiotherapy with concurrent or sequential

RADIATION ONCOLOGY—ORIGINAL ARTICLE jmiro_2325 204..210
Radiotherapy with concurrent or sequential temozolomide inelderly patients with glioblastoma multiformeSameh A Hashem,1 Ahmed Salem,1 Abdulla Al-Rashdan,1 Najeeb Ezam,2 Ala’a Nour,1 Amer Alsharbaji,4
Chandrababu Rejeeth,5 Issa Mohamad,1 Maher Sughayer,2 Maher Elyan,4 Maysa Al-Hussaini,2 Ala’ Addasi3
and Abdelatif Almousa1
Departments of 1Radiation Oncology, 2Pathology and Laboratory Medicine, 3Medical Oncology, 4Surgery, King Hussein Cancer Center, Amman, Jordan
and 5Department of Zoology, School of Life Sciences, Bharathiar University, TamilNadu, India
SA Hashem MD; A Salem MD; A Al-RashdanMD; N Ezam MD; A Nour MD; A AlsharbajiMD; C Rejeeth MSc; I Mohamad MD;
C Rejeeth MSc; M Sughayer MD; M ElyanMD; M Al-Hussaini MD; A Addasi MD;
A Almousa MD, PhD.
CorrespondenceDr Abdelatief Almousa, Department of
Radiation Oncology, King Hussein Cancer
Center, PO Box 1269 Al-Jubeiha, Queen Rania
Al Abdullah Street, Amman 11941, Jordan.
Email: [email protected]
Competing interests: None.
Submitted 12 April 2011; accepted 17 July
2011.
doi:10.1111/j.1754-9485.2011.02325.x
Abstract
Objective: The objective of this article was to evaluate therapeutic outcomes ofelderly patients with glioblastoma multiforme (GBM) treated by surgery fol-lowed by combined modality therapy and compare achievable outcomes tothose of a younger age population.Methods and Materials: Seventy-eight adult patients with histologically con-firmed grade IV astrocytoma were treated at King Hussein Cancer Center(Amman, Jordan) between September 2004 and December 2008. Recordswere retrospectively reviewed and included 55 males and 23 females between19 and 78 years of age (median age 50 years). This case series included 20patients aged 60 years or older. All patients underwent craniotomy followedradiotherapy and concurrent or sequential temozolomide. The follow-upranged from 1 to 56 months (median 9.4 months).Results: The median survival for the whole cohort was 13.8 months. Themedian survival for patients less than 60 years was 14.3 months and forpatients 60 years or older was 12.3 months (P = 0.19). Among elderlypatients, radical surgical resection (P = 0.002), concurrent delivery of chemo-radiation (0.041) and radiotherapy dose �5400 cGy (P = 0.0001) conferredstatistically significant improvements in overall survival.Conclusion: Management of GBM in elderly patients should include maximalsurgical resection followed by radiotherapy and temozolomide whenevermedically feasible. Outcomes comparable to those obtained in younger agegroups can be expected. Our results indicate that concurrent chemoradiationis superior to sequential chemoradiation in these patients.
Key words: concurrent; elderly; GBM; radiotherapy; sequential;temozolomide.
Introduction
Despite the widespread adoption of multimodalitytherapy, the diagnosis of glioblastoma multiforme (GBM)continues to carry a dismal prognosis with a grave overallsurvival estimate set at 9–12 months.1–3 Historically,surgery followed by radiotherapy was considered thestandard of care.3 In 2005, Stupp et al.4 demonstratedthat temozolomide administered in addition to adjuvantradiotherapy significantly prolongs overall survival. Cur-
rently, temozolomide concurrent with radiotherapy fol-lowed by adjuvant temozolomide has been adopted as thenew standard of care. Prognosis of elderly patients withGBM is grim with an overall survival ranging from4 to 8 months.5 Furthermore, management of elderlypatients with GBM is still hindered by the paucity of clearprotocols due in part to the exclusion of this age groupfrom the majority of randomised trials in this field. As aconsequence, debate is unfolding as to whether thesepatients would benefit from aggressive surgical resection
bs_bs_banner
Journal of Medical Imaging and Radiation Oncology 56 (2012) 204–210
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists204

followed by combined modality therapy. In this retrospec-tive review, we assessed the therapeutic outcomes ofelderly patients with GBM treated by surgical resec-tion followed by chemoradiotherapy and compared theachievable outcomes with those of a younger agepopulation.
Materials and methods
Charts of consecutive patients with a pathologic diagnosisof World Health Organization grade IV astrocytoma diag-nosed and treated at King Hussein Cancer Center betweenSeptember 2004 and December 2008 were retrospec-tively reviewed following acquisition of institutionalreview board approval in an attempt to extract datapertaining to pathological characteristics, clinical status,therapeutic alternatives and disease outcome. Records ofimaging studies were made available for this review.Patients �18 years of age at the time of diagnosis wereexcluded from this case series. All patients underwentcraniotomy followed by radiotherapy and concurrent orsequential temozolomide. Patients who did not receivecombined modality therapy were excluded. Patients wereclassified into two age groups: those less than 60 years ofage (group 1) and those 60 years or older (group 2).Pretreatment performance status was evaluated accord-ing to the Karnofsky performance indicator scale (KPS)with scores divided into those above and equal or belowthan 70%.6 Tumour size was evaluated whenever possiblewith lesions divided into those more or equal or those lessthan 5.5 cm. Surgical resection status was designated aspartial if only biopsy was performed or radical if anattempt at aggressive resection was undertaken includingnear total (NTR), subtotal (STR) and gross total resection(GTR). Radiation dose was classified according to dose:more/equal or less than 5400 cGy. Toxicity data were notavailable for this review.
Kaplan–Meier survival analysis was utilised to assessoverall survival. Subgroup analysis was based upon KPS,extent of surgical resection, tumour size, radiotherapydose and concurrent versus sequential delivery of temo-zolomide. A P-value �0.05 was considered statisticallysignificant. Statistical analysis was performed using SASversion 9.1 (SAS Institute Inc, Cary, NC, USA).
Results
Seventy-eight patients met the eligibility criteria of whom55 were males and 23 were females between 19 and78 years in age (median age 50 years). Fifty-eightpatients were less than 60 years of age at the time ofdiagnosis (group 1). The median age for this group was45 years (range 19–59 years). Twenty patients were60 years or older at the time of diagnosis (group 2).The median age for this group was 65 years (range60–78 years). Table 1. Supratentorial tumours werefound in 52 patients (89.7%) in group 1 and 19 patients(95%) in group 2. Assessment of tumour size was pos-sible in 46 patients (79.3%) in group 1 and 18 (90%)patients in group 2. Tumours were �5.5 cm in 30 patients(65.2%) in group 1 and in eight patients (44.4%) in group2. Thirty-five patients (60.3%) in group 1 and 13 patients(65%) in group 2 were designated with KPS score �70. Allpatients underwent craniotomy. The extent of surgicalresection depended on the location and size of thetumour, patient performance and disease extent. Radicalsurgical resection was performed in 38 patients (65.5%)in group 1 and 10 patients (50%) in group 2. Uponpathological examination and immunohistochemical con-firmation by glial fibrillary acidic protein, GBM was foundin 76 patients. Specimens from two patients who har-boured gliosarcoma revealed evidence of mesenchymaldifferentiation and increased deposition of reticulin inareas of sarcomatomous differentiation.
Table 1. Patients characteristics
Characteristics <60 years (58 patients), % �60 years (20 patients), % P-value*
Male sex 41 (70.7) 14 (70) 0.95
Supratentorial location 52 (89.7) 19 (95) 0.11
Tumour size evaluated 46 (79.3) 18 (90) 0.50
Tumour size �5.5 cm 30 (65.2) 8 (44.4) 0.37
KPS �70 at time of diagnosis 35 (60.3) 13 (65) 0.71
Radical surgery (other than biopsy) 38 (65.5) 10 (50) 0.22
Type of surgery
Biopsy 20 (34.5) 10 (50) 0.52
STR/PR 29 (50) 8 (40)
NTR/GTR 9 (15.5) 2 (10)
Radiotherapy dose �5400 Gy 51 (87.9) 17 (85) 0.71
Concurrent chemoradiation 38 (65.5) 16 (80) 0.27
*P-value was calculated based on chi-square or Fisher’s exact test. GTR, gross total resection; KPS,
Karnofsky performance indicator scale; PR, partial resection; NTR, near total resection; STR, subtotal
resection.
Glioblastoma multiforme in elderly patients
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 205

Concurrent chemoradiation entailed radiotherapy con-current with daily TMZ at a dose of 75 mg/m2 to befollowed by daily adjuvant temozolomide (TMZ) at adose of 150 mg/m2 during days 1–5 of a 28-day cycle forsix cycles initiated 3–4 weeks following completion ofconcurrent therapy. Concurrent chemoradiation wasdelivered in 38 patients (65.5%) in group 1 and 16patients (80%) in group 2. The remaining patientsexhibited poor overall performance and/or unfavourableprognostic variables and received sequential chemoradi-ation regimen consisting of radiotherapy followed byadjuvant TMZ after 3–4 weeks of rest in the form of150 mg/m2 during days 1–5 of a 28-day cycle for sixcycles. Radiation dose ranged from 5400 to 6000 cGyand was delivered via conventional 180–200 cGy frac-tionation, 5 days per week for 5–6 weeks. In 10 patients(six in group 1 and four in group 2), suboptimal radiationdoses ranging from 4400 to 5000 cGy were deliveredbecause of the dose-limiting tolerance limits of neigh-bouring normal tissues. No treatment discontinuation ormajor therapy-induced interruption was reported.
At a median follow-up of 9.4 months (range1–56 months), the median survival for the whole cohortwas 13.8 months (Figure 1). The median survival forgroups 1 and 2 was 14.3 and 12.3 months, respectively(P = 0.19). Because of the small number of patients aged70 years or older, we cannot draw firm conclusionsregarding the outcome of combined modality therapy inthese patients (Figure 2). Survival was significantlybetter in patients who underwent partial (partial resec-tion, STR) or aggressive surgical resection (NTR, GTR)as opposed to those who underwent biopsy for groups1 and 2 (P < 0.0001 and P < 0.0092, respectively;Figures 3 and 4). Using univariate analysis, survival wassignificantly better among group 1 patients with KPS�70% (P = 0.04), who underwent radical tumour resec-tion (P � 0.0001) and who received radiotherapy dose�5400 cGy (P = 0.003). Tumour size and chemoradia-tion sequencing did not confer any statistically significantdifference in survival in this age group. Among group 2patients, univariate analysis demonstrated that radicalsurgical resection (P = 0.002), concurrent delivery of
Fig. 1. Kaplan–Meier survival curve for groups 1 and 2.
SA Hashem et al.
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists206
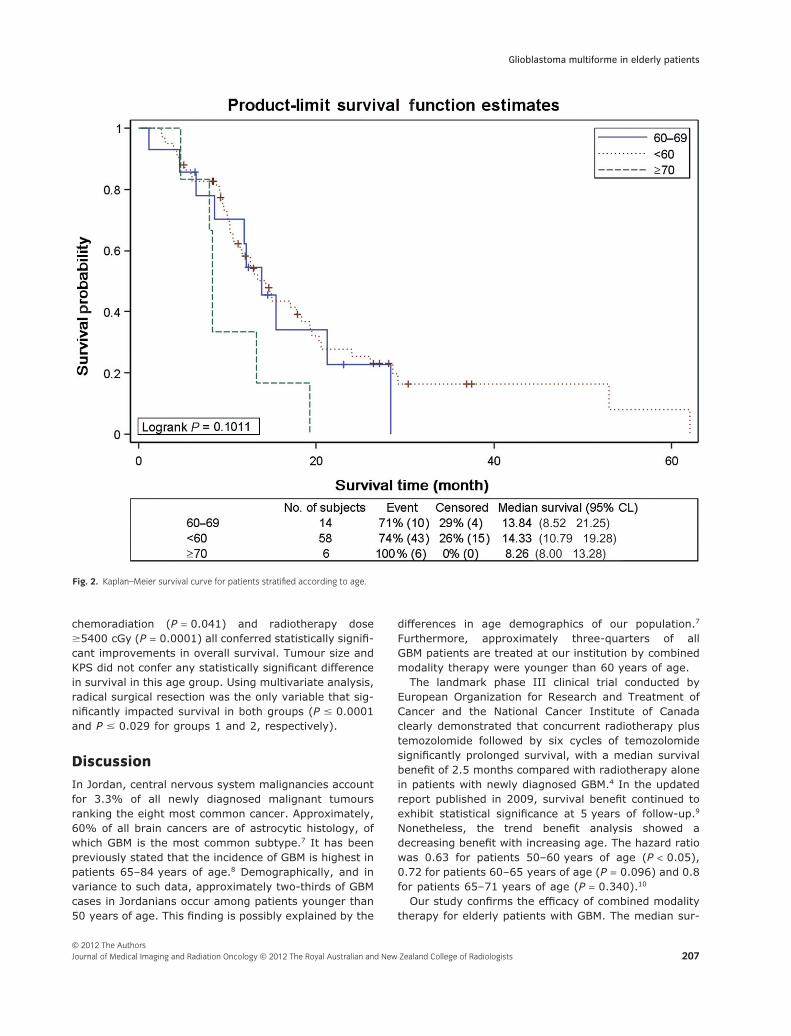
chemoradiation (P = 0.041) and radiotherapy dose�5400 cGy (P = 0.0001) all conferred statistically signifi-cant improvements in overall survival. Tumour size andKPS did not confer any statistically significant differencein survival in this age group. Using multivariate analysis,radical surgical resection was the only variable that sig-nificantly impacted survival in both groups (P � 0.0001and P � 0.029 for groups 1 and 2, respectively).
Discussion
In Jordan, central nervous system malignancies accountfor 3.3% of all newly diagnosed malignant tumoursranking the eight most common cancer. Approximately,60% of all brain cancers are of astrocytic histology, ofwhich GBM is the most common subtype.7 It has beenpreviously stated that the incidence of GBM is highest inpatients 65–84 years of age.8 Demographically, and invariance to such data, approximately two-thirds of GBMcases in Jordanians occur among patients younger than50 years of age. This finding is possibly explained by the
differences in age demographics of our population.7
Furthermore, approximately three-quarters of allGBM patients are treated at our institution by combinedmodality therapy were younger than 60 years of age.
The landmark phase III clinical trial conducted byEuropean Organization for Research and Treatment ofCancer and the National Cancer Institute of Canadaclearly demonstrated that concurrent radiotherapy plustemozolomide followed by six cycles of temozolomidesignificantly prolonged survival, with a median survivalbenefit of 2.5 months compared with radiotherapy alonein patients with newly diagnosed GBM.4 In the updatedreport published in 2009, survival benefit continued toexhibit statistical significance at 5 years of follow-up.9
Nonetheless, the trend benefit analysis showed adecreasing benefit with increasing age. The hazard ratiowas 0.63 for patients 50–60 years of age (P < 0.05),0.72 for patients 60–65 years of age (P = 0.096) and 0.8for patients 65–71 years of age (P = 0.340).10
Our study confirms the efficacy of combined modalitytherapy for elderly patients with GBM. The median sur-
Fig. 2. Kaplan–Meier survival curve for patients stratified according to age.
Glioblastoma multiforme in elderly patients
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 207

vival for patients less than 60 and patients 60 years orolder was 14.3 and 12.3 months, respectively. Althoughthere was a trend towards lower overall survival in GBMpatients aged 60 years or older, this difference was notstatistically significant. Concurrent delivery of temozolo-mide and radiotherapy dose in excess to 5400 cGy wasstatistically significant predictors of improved overallsurvival in our elderly patient population. One shouldtake the previous statement with caution because nor-mally, it would be expected that patients treated withhigher radiotherapy dose and those receiving concurrenttemozolomide have improved overall performance andlonger life expectancy. As has been previously narratedby Ewelt et al.11; the extent of surgical resectionbroached as the most significant predictor of therapeuticoutcome in both age groups.
Elderly GBM patients are generally considered to beless tolerant to combined modality treatment thanyounger patients.12 This has led some to investigate theefficacy of hypofractionated radiotherapy as a substitute
to conventional fractionation. In their prospective ran-domised trial, Roa et al.13 reported no significant differ-ence in overall survival of patients 60 years or oldertreated by standard (6000 cGy/30 fractions) over short-course radiotherapy (4000 cGy/15 fractions). During thestudy period, all our elderly patients received conven-tionally fractionated radiotherapy. Disappointingly,detailed toxicity data are not available in this report.However, treatment discontinuation or interruption wasgenerally acceptable in our patients.
Conclusions
Management of GBM in elderly patients should includemaximal surgical resection followed by radiotherapy andtemozolomide whenever medically feasible. Outcomescomparable with those obtained in younger age groupscan be expected. Our results indicate that concurrentchemoradiation is superior to sequential chemoradiationin these patients. Limitations of our study include the
Fig. 3. Kaplan–Meier survival curve for group 1 patients stratified according to resection status.
SA Hashem et al.
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists208

small number patients treated at a single institution. Webelieve that a prospective randomised trial is warrantedto confirm these findings.
Acknowledgement
We would like to thank Ms Ayat Taqash for her efforts inthe completion of the statistical analysis of this paper
References
1. Kristiansen K, Hagen S, Kollevold T et al. Combinedmodality therapy of operated astrocytomas grade IIIand IV. Confirmation of the value of postoperativeirradiation and lack of potentiation of bleomycin onsurvival time: a prospective multicenter trial of theScandinavian Glioblastoma Study Group. Cancer1981; 47: 649–52.
2. Chamberlain MC, Kormanik PA. Practical guidelinesfor the treatment of malignant gliomas. West J Med1998; 168: 114–20.
3. Walker MD, Alexander E Jr, Hunt WE et al. Evaluationof BCNU and/or radiotherapy in the treatment ofanaplastic gliomas. A cooperative clinical trial.J Neurosurg 1978; 49: 333–43. 1978/09/01 ed.
4. Stupp R, Mason WP, van den Bent MJ et al.Radiotherapy plus concomitant and adjuvanttemozolomide for glioblastoma. N Engl J Med 2005;352: 987–96.
5. Idbaih A, Taillibert S, Simon JM et al. Short course ofradiation therapy in elderly patients with glioblastomamultiforme. Cancer Radiother 2008; 12 (8): 788–92.
6. Schag CC, Heinrich RL, Ganz PA. Karnofskyperformance status revisited: reliability, validity, andguidelines. J Clin Oncol 1984; 2: 187–93.
7. Tarawneh M, Nimri O. Jordan National CancerRegistry 2007. Vol. 12, 12th edn. Ministry of Health,Amman, Jordan, 2007.
8. Scott JG, Suh JH, Elson P et al. Aggressive treatmentis appropriate for glioblastoma multiforme patients 70years old or older: a retrospective review of 206cases. Neuro Oncol 2011; 13 (4): 428–36.
Fig. 4. Kaplan–Meier survival curve for group 2 patients stratified according to resection status.
Glioblastoma multiforme in elderly patients
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 209

9. Stupp R, Hegi ME, Mason WP et al. Effects ofradiotherapy with concomitant and adjuvanttemozolomide versus radiotherapy alone on survivalin glioblastoma in a randomised phase III study:5-year analysis of the EORTC-NCIC trial. LancetOncol 2009; 10: 459–66.
10. Laperriere N, O’Callaghan C, Ding K et al. Rationaleand design for a phase III randomized controlled trialin elderly patients with glioblastoma multiforme:NCIC CTG CE. 6 13th Biannual CanadianNeuro-Oncology Meeting 2008.
11. Ewelt C, Goeppert M, Rapp M et al. Glioblastomamultiforme of the elderly: the prognostic effect of
resection on survival. J Neurooncol 2010; 103:611–8. [Epub ahead of print].
12. Brandes AA, Franceschi E, Tosoni A et al.Temozolomide concomitant and adjuvantto radiotherapy in elderly patients withglioblastoma: correlation with MGMT promotermethylation status. Cancer 2009; 115 (15):3512–18.
13. Roa W, Brasher PM, Bauman G et al. Abbreviatedcourse of radiation therapy in older patientswith glioblastoma multiforme: a prospectiverandomized clinical trial. J Clin Oncol 2004; 22 (9):1583–8.
SA Hashem et al.
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists210


















