Radiation Therapy 1 & 2
19
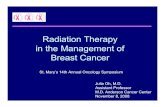
Radiation Therapy After surgery, RT is the most often used modality for head and neck cancer. Sources of Radiation Spectrum of Electromagnetic Radiation Radiation Therapy uses radiation that: creates ionization in the medium by removing electrons from the atomic shells of the target, and/or causing/breaking of chemical bonds, other damage, cell death. Two types Radiation: Directly Ionizing Indirectly Ionizing Directly Ionizing Radiation: charged particles produce ionization Alpha - helium nuclei, (2P, 2N) large charge/high energy Beta - from nucleus, e - /antineutrino, positron (anti-e - )/neutrino light, weakly charged, less easily stopped Indirectly Ionizing Radiation: neutral particles (photons, neutrons) Interact with e - and nuclei of target to produce ionizing particles e - , positrons, protons X-rays - electromagnetic, extranuclear e - , rearrang. nuclear shells Gamma - electromagnetic, nuclear photons, no mass/charge Amino Acids 10 -10 10 -9 10 -8 10 -7 10 -6 10 -5 10 -4 10 -3 10 -2 10 -1 1 10 10 2 10 3 10 4 10 5 Centimeters Gamma Rays X- Rays Ultra Violet Visible Light Infra Red Micro Radio Short Waves Waves Waves Radar TV Radio Bacteria Viruses Red Cells Epithelial Cells Protei ns Atoms
Transcript of Radiation Therapy 1 & 2

Radiation TherapyAfter surgery, RT is the most often used modality for head and neck cancer.Sources of Radiation
Spectrum of Electromagnetic Radiation
Radiation Therapy uses radiation that:creates ionization in the medium by
removing electrons from the atomic shells of the target, and/orcausing/breaking of chemical bonds, other damage, cell death.
Two types Radiation: Directly IonizingIndirectly Ionizing
Directly Ionizing Radiation: charged particles produce ionization Alpha - helium nuclei, (2P, 2N) large charge/high energyBeta - from nucleus, e-/antineutrino, positron (anti-e-)/neutrino
light, weakly charged, less easily stoppedIndirectly Ionizing Radiation: neutral particles (photons, neutrons)
Interact with e- and nuclei of target to produce ionizing particlese-, positrons, protons
X-rays - electromagnetic, extranuclear e-, rearrang. nuclear shellsGamma - electromagnetic, nuclear photons, no mass/charge
Amino Acids
10-10 10-9 10-8 10-7 10-6 10-5 10-4 10-3 10-2 10-1 1 10 102 103 104 105 Centimeters
Gamma Rays
X- Rays
UltraViolet
Visible Light
InfraRed
Micro Radio ShortWaves Waves Waves
Radar TVRadio
BacteriaViruses
Red CellsEpithelial Cells
Proteins
Atoms

Bergonie, Tribondeau "Law"- 1906 Ionizing radiation is more effective against cells that 1. are actively mitotic 2. are undifferentiated (stem and precursor) 3. have a long mitotic future.
Cell Cycle
Mitosis Growth & protein production stop. All energy is focused on cell division. Chromosomes condense. Mitosis lasts one to two hours. Gap 1 Cells produce RNA, synthesize protein making ready for DNA synthesis. Synthesis DNA replication occurs.Gap 2 Gap between S and M, the cell continues to grow and produce proteins.
Cellular Response to Radiation Division Delay cells in interphase are delayed in G2 (making ready for mitosis)Interphase Death irradiation and death of cells in G1, S, G2 phasesReproductive Failure chromosome damage during mitosisApoptosis radiation affects specific genes activating programmed cell death
Cell populations and their kinetic properties No mitosis Low mitotic index Frequent mitoses No cell renewal Little or no cell renewal Cell renewal
CNS Liver Epidermis Sense organs Thyroid Intestinal epithelium Adrenal medulla Vascular endothelium Bone marrow Connective Tissue Gonads
G1
G2
S
Mitosis

Cell Kinetic Parameters Histological Type Doubling DNA Synth. Growth Cell Loss Active Fraction Factor
Embryonal 27 days 30 % 90 % 93 %Malig. Lymphoma 29 29 90 93Sarcoma 41 4 11 68Squamous Cell 58 8 25 89
Adenocarcinoma 83 2 6 71
Doubling Time = time for 100% increase in number of cells DNA Synth. Active = % of total cells showing DNA synthesis active Growth Fraction = fraction of cells "growing" at any one time Cell Loss Factor = cells lost as a % of total cell replacement
Radiation Therapy Modalities Delivery Modalities and Examples of CA Treated
Oral IsotopeThyroid I131
Brachytherapy - "seeds"Prostate
External BeamHead and Neck
IntraOperative Radiation TherapyPancreas during surgery
Brachytherapy - Brachy - "short” Placing radioactive material directly into or adjacent to tumors Inverse square rule Isotopes - Radium, Cesium, Iridium, Cobalt, Gold, Iodine Interstitial, Intracavitary, External Uterus, cervix, prostate, lung, breast, oral nasal, orbital cavities
External Beam Electrons
Linear accelerators, Betatron; x-rays, high energy electronsProtons
Cyclotrons; limited range and dose drop off related to massGamma
Cobalt-60

External Beam (cont) Single or Fractionated Given at time of surgery – single therapy, pancreasConformal therapy – IMRT, IGRTStereotactic – single or fractionated, xyz coordinates,
External 3D frame of reference, brain, bodyStereotactic Radiation Therapy, Gamma Knife, Cyberknife
Examples of SRT/SRS Sterotactic RadioTherapy, Stereotactic Radiosurgery
Cranial and Body Stereotactic (Shaped) Beam Radiosurgery/Radiotherapy is either applied in surgery as a single session with a high dose of radiation or in a series of treatments over a period of time as radiotherapy. Both deliver similiar doses of radiation.
In fractionated treatment for head and neck cancer, a face mask is worn instead of the metal head frame. For tumors elsewhere in the body, other immobilizations devices are used to assure that the patient is positioned identically for each treatment.
In treatment planning, sophisticated software calculates the ideal access points to the tumor or lesion from previously made imaging studies and defines the individual treatment plan for radiosurgery or radiotherapy.
During treatment, precise doses of high-energy radiation are shaped to match the exact contour of the tumor or lesion, so that even irregularly shaped tumors or lesions can receive an even dose of prescribed radiation to the entire tumor or lesion. The machine continuously shapes and positions the treatment beam to match the size and shape of the tumor from all angles while the patient is held in an exact and known position. The patient may have a headframe attached to their skull for 3 to 8 hours for imaging, treatment planning and radiosurgery (one session). For fractionated stereotactic radiotherapy is given over many appointments a facemask individually formed to perfectly fit the patient's head and unique facial shape or other body immobilization device is used. This reduces potential damage to delicate structures such as the brainstem or spinal cord.
IMRT - Intensity Modulated Radiation TherapySophisticated data from images (CT, MRI, PET) is sent to treatment planning computers where normal and tumor tissues are defined. The IMRT targeting computer adjusts the intensity of energy beam and collimator(s) move in beam portal under precise computer guidance. Effect is that the beam is shaped, collimated, and tumor receives more precise doses of energy and normal tissues receive less. Collimators used for beam shaping can be referred to as dynamic wedge and multileaf collimators.

IGRT - Image Guided Radiation TherapyIGRT is used to image a patient (CT, ultrasound, x-ray)just before treatment and compare external marks and internal anatomy to the treatment plan. Additional imaging is done on the fly and shifts in patient position are made for each fraction delivered. IGRT compensates for factors such as respiratory motion, movement of body or internal organs, weight loss, and tumor shrinkage from the previous radiation treatment.
Examples of Fractionated Stereotactic Radiation Therapy
Four R's of radiobiology that affect fractionation: Recovery of cells from radiation damage Repopulation of tumor and normal cells between fractions Re-oxygenation of tumor during course of treatment Redistribution of normal and tumor cells in the cell cycle
Doses required to produce the same skin reaction Fractionation Total Dose Dose increment cGy cGy One fraction 2000 - Five fractions in 4 days 3600 1600 Five fractions in 28 days 4200 600 illustrates: recovery influences dose in fractionation, and fractionation increases dose with less damage
Free Radical Formation and Tumoricidal Effect Amifostine (Ethyol), Glutathione - antioxidants
# of Cells
Time
Treatment TreatmentTreatment
Effect of Fractionated Radiotherapy on Number of Cells and Repopulation
Normal Cells
Tumor Cells

Radiation Therapy Equipment Equipment
Linear Accelerator (-), e- and x-raysCyclotron (o), protonsBetatron (s), high energy electrons, x-raysCobalt Unit, 60 Co, gamma, less used
Elementsenergy source, tungsten target, bending magnet, beam flattening filter, scattering foil, collimators (1o, 2o)
Stereotactic RadioSurgery
Treatment Head contains: energy beam from linear accelerator, for ex.target - provides electronsbending magnet - bends electron beam as needed to direct to targetprimary collimator - to limit the maximum field sizebeam flattening filter - conical, metal, evens out beam (absorbs more photons from central area, less from periphery)scattering foil - with electron beam (not x-rays) broaden/flatten beam ion chamber - monitors beam for symmetrysecondary collimator - to shape beamfield light - to guide aiming of beam to patient
Klystron Tube generates microwaves to accelerate electrons
High Energy Electron Radiation Therapy Machine
Electron BeamBending Magnet andTreatment HeadLinear Accelerator
Treatment couch
Gantry

Radiation Therapy - Head and Neck CATreatment
Surgery, Radiation (before and/or after surgery, chemotherapy)Usually fractionated- IMRT, high energy electron beamUsually 200 cGy/day, Usually 5 days/week, Usually 5 to 7 weeks
Hyperfractionated - several tx per dayDosage
Usual total dose 5000 - 7000 cGy, compare to whole body radiation of 1000cGyFractionated Areas irradiated - diagram

Treatment Planning, Simulation Patients not usually marked with permanent markers that delineate fieldscomputers do this now and the patient is oriented to the machine by immobilization device, facemask
Oncologist, Surgeon will not know the fields to be irradiated nor the final dose.Radiation Oncologist will know this but often not until RT is completed.Radiation Oncologist will be able to give an estimate of the total dose to parotids
and to the ant and post mandible (bone). If the dose to the parotid < 24-26 Gy, some salivary flow may remain. Other tissues are still affected (mucosa, bone)
The actual dose plan is of help in making post-radiation management decisions.
Side Effects Mucositis Early cell death in the epithelial basement membrane. Begins in the second week of
RT, resolves slowly several weeks after radiation therapy is complete. Mucosa is atrophic and prone to ulceration with risk of infections.
National Cancer Institute (NCI) Scale of Mucositis Grade Symptoms, Signs
0 None1 Painless ulcers, erythema, or mild soreness with no ulcers2 Painful erythema, edema, ulcers, eating and swallowing possible3 Painful erythema, edema, ulcers, requiring IV hydration4 Severe ulceration - parenteral/enteral nutrition or intubation5 Death related to toxicity
World Health Organization (WHO) Scale of Mucositis 0 None1 Soreness with or without erythema or ulceration2 Erythema, ulcers, patients can swallow solid food3 Extensive erythema, ulcers, patients can swallow solid food4 Oral mucositis - alimentation by mouth may not be possible
Hypogeusia/DysgeusiaPermanent taste loss may occur at a dose of 6000 cGy if the tongue is in the high dose
areas. Below this, recovery takes several months. Both mucositis and decreased saliva flow may contribute/complicate. Discrete taste ability can also be affected by longer term ulceration (months/years).
XerostomiaSerous glands are affected more than mucous so parotids more affected than others so
the remaining saliva is acidic and thick. This results in decreased remineralization of enamel, antimicrobial capacity and mouth cleansing, and in changes in taste, and difficulties chewing, swallowing and speech. Atrophy of secretory cells occures resulting in xerostomia. It is hoped that IMRT will result in decreased

xerostomia but most patients exhibit some degree. If the normal functions of saliva are compromised, a host of abnormalities can occur, including.
Dental CariesDecrease in quality and quantity of saliva, decrease in normal antimicrobial and
remineralizing capacity, create risk for infection. Periodontal DiseaseIncreased periodontal attachment loss over time can occur in high-dose fields. Osteoradionecrosis Osteoradionecrosis results from small vessel changes that result in impaired healing
of bone. ORN most often occurs one year after treatment and the incidence of ORN increases over time. ORN is usually confined to the posterior mandible. ORN is most common with radiation doses of >60 Gy. Elimination of active oral disease and hopeless teeth is important to reduce the need for extractions after RT. 14-21 days of healing is preferred between extractions and start of RT.
TrismusRT results in contraction of the masticatory muscles and TMJ capsule, usually
occurring 3-6 months after radiation therapy. This may be accentuated by surgical injury and higher radiation dosing to the pterygoid regions.
Nutritional DeficiencyAs a result of mucositis, xerostomia, decreasd and altered taste and loss of appetite
can make eating difficult. Patients commonly manifest rapid weight loss, dehydration, stomatitis, or secondary oral infections such as candidiasis.
Pre-radiation Dental Management Complete Examination - establish baseline dental condition
Soft Tissue examination - PT can have as many diseases as they pleases (J. Cornyn)Periodontal ChartingRadiographs, Panoramic and FMX, must see all apices of teeth
Assess - PT's ability/desire to maintain excellent oral hygiene for the rest of their life Assessment will influence the decision to extract sound teeth within the RT field. The physical and emotional cost of CA treatment and RT is huge. Despite initial good intentions and initial positive attitude, if patients have nor previously observed good oral hygiene is almost guaranteed that they will continue this lack of care.
Treatment - eliminate sources of intra-oral trauma and infectionPerform - necessary hygiene; scaling, SCRP, Prophy remove all calculusSmooth - sharp teeth, restorationsAdjust - ill-fitting prostheses/appliances, or pts may not wear because of mucositis. Impress, Make, Deliver - custom fluoride trays for fluoride delivery. Extract - hopeless teeth, with moderate/ severe perio dz, extract partially erupted mand 3rd molars and those that can be probed at the distal of the 2nd molar if within the RT field. 2 weeks of healing is preferred between extractions and start of RT.
*Tumor size and growth may require that RT be started immediately and not allow 14-21 days of healing after dental surgery. So, dental surgery should be deferred. Extractions should be performed as soon as RT is completed and the

patient has recovered, usually within 4 to 6 weeks. This should not be delayed, since bone changes associated with radiation therapy may worsen over time with increased risk of ORN the longer dental Sx is removed from completion of RT.
Fluoride Pts should be started on fluoride therapy prior to RT. This may take the form of fluoride
gel carriers, brush-on gel, or fluoride rinses. Denture Care Removable appliances should not be worn during treatment, if possible, and dentures
should be removed at night. Follow usual prosthesis cleaning instructions. Observe pt carefully for signs of Candida infection.
Endodontics RCT is acceptable for carious teeth with pulpal involvement confined to the tooth. Teeth
with periapical lesions in the filed should be removed. Teeth outside the radiation field with necrotic or infected periapical tissue may have RCT. Cost wil loften be an important factor for Pts undergoing CA treatment. All teeth with previous RCT with PA lucencies should be assessed for signs and symptoms of current infection.
Oral and Maxillofacial Surgery Extraction should be considered for partially erupted 3rd molars, teeth with pericoronitis,
or non-restorable, teeth with unresolved periapical lesions, teeth within the radiation field in Pts where long-term oral hygiene compliance is questionable and teeth with advanced perio dz. Mandibular tori in the RT field should be removed for the future construction of a prosthesis. While 14-21 days healing is optimal before RT is begun.
Orthodontics Orthodontic bands and appliances that may cause trauma to mucosa should be removed.
Or, soft wax/plastic mouthguards may be used to cover them during RT.Periodontics Pretreatment prophylaxis and/or scaling are recommended for all patients. Teeth with 5
mm or greater periodontal pocketing should be evaluated for extraction if they are in the field of radiation, and teeth that display advanced bone loss, excessive mobility, purulence or excessive bleeding on probing should be extracted.
Xerostomia Prevention Some institutions use amifostine (Ethyol), during RT to reduce the incidence of acute
xerostomia, from 78% to 51%. As well, the dose of RT required to cause xerostomia in 50% of Pts was markedly higher in those patients receiving amifostine compared with those who did not (60 Gy v 42 Gy). One year after the completion of treatment, xerostomia was significantly less frequent in patients who received amifostine (34% vs 57%,). Despite these results, many radiation oncologists do not routinely use this agent, likely due to the problems associated with administration (hypotension, allergic reactions and nausea).
During RT - Dental Management/Treatment Dental TX Should be avoided while RT is being delivered. Care should be palliative.Patients are quite uncomfortable after he second week of RT and usually will not want to

wear oral prosthesis or fluoride trays or use mouthwashes, if irritating. Pts must practice excellent oral hygiene as well and for as long as they can during RT.
Most pts cease brushing and use of fluoride and mouthrinses because of oral irritation/ulceration/mucositis. Pts may be able to continue Triple Mix and bicarbonate rinses, meds for infection, all as tolerated.
Post RT - Dental Management/TreatmentCare should be directed toward side effects listed in the above section on RT Treatment. Dental treatment may proceed. If extractions are to be performed and the mandible has received greater than 6000 cGy, hyperbaric oxygen therapy may be indicated before and following dental extractions to lessen the chance of developing osteoradionecrosis. Typical HBO management calls for 1 compression/decompression cycle per day five days per week.
Patients who meet the definition of ORN begin with staged treatment as follows:Stage I- If the wound shows clinical improvement after 30 compression/decompression
cycles, the Pt is given a full course of 60 comp/decomp cycles. If no improvement after 30 comp/decomp cycles, the patient is advanced to stage II.
Stage II- A transoral alveolar sequestrectomy with primary closure is done and the comp/decomp cycles are resumed. If healing progresses without complication, a total of 60 comp/decomp cycles are completed. If there is incomplete healing, the patient is advanced to stage III.
Stage III- The patient undergoes a resection of the necrotic bone, the margins of which are determined by the presence of bleeding bone or by Tetracycline fluorescence. Comp/decomp cycles are continued until healthy mucosal closure is obtained or a total of 60 compression/decompression cycles are given. The patient is then advanced to stage III-R. A patient can enter this stage directly if he/she presents with a pathologic fracture, orocutaneous fistula, or radiographic evidence of resorption to the inferior border. An initial course of 30 comp/decomp cycles are given in these cases.
Stage III-R - Ten weeks after resection, 20 additional compression/decompression cycles are given and bone graft reconstruction is accomplished from a transcutaneous approach.
Oral Health in Cancer TherapyA Guide for Health Care ProfessionalsEditors - K. Vendrell Rankin, Daniel L. Jones, Spencer W. Redding
www.doep.org/images/OHCT_III_FINAL.pdf

Mouth rinses
Mouth rinses Composition/ Instructions for
use:
Uses/Functions Disadvantages
Neutral rinse 1/4 tsp. salt1/4 tsp. baking soda1 qt. H2OUse every 2 hours until soreness, nausea or ropy saliva contraindicate.Switch to1/2 tsp. soda and 1 qt. water or water only, if necessary.Should not be swallowed
May be used during mucositis (omit salt)Neutralizes acids after emesisDissolves thick, mucinous salivary secretionsSoothing to irritated tissuesDislodges debris
None
Saline rinse 1/2 tsp. salt8 oz. water
Not damaging to oral mucosa Helps reduce mucosal irritationIncreases moisture in mouthRemoves thickened secretions and debrisRecommended for treatment of leukemic gingivitis and head and neck radiation
None
Hydrogen peroxide Not recommended for use as a daily rinseShould be diluted 1:4 if usedDo not use in the presence of blood clots, as this may promote bleedingUse to cleanse wounds prior to secondary medication/rinseUse for 1-2 days maximumShould be followed by therapeutic rinses
Helpful in periodontal infections when anaerobic microorganisms are involved
May delay wound healingCause demineralizationMay promote emesisCauses dry mouth, thirst and discomfortUnpleasant taste
Anti-fungalsFluconazole (Diflucan®) 100 mg tablets Disp: 8 to 15 tablets Sig: Take 2 tabs on day one and then one tab for 6 to 13 days (Oral suspension is also available in 10 mg/ml)
Clotrimazole (Mycelex®) 10 mg troches Disp: 70 troches Sig: Dissolve one troche in the mouth five time per day for 14 days
Itraconazole (Sporonox®) suspension 100 mg/10 ml Disp: 140-280 ml Sig: Swish and swallow 200 mg for 7 to 14 days
Nystatin (Mycostatin®) 200 mg oral pastilles Disp: 56 pastilles Sig: Dissolve pastilles in mouth four times per day for 14 days
CYP3A4 metabolism and drug interactions

Gums and MintsProducts with Xylitol Manufacturer TelephoneB-Fresh® Xylitol Mints B-Fresh
Johnston, RI www.bfreshgum.com
800-555-1276
Biotene® Dry Mouth Gum Laclede, Inc. Rancho Dominquez, CA www.laclede.com
800-922-5856
Smint® Gum Perfete van Melle Lainati, Italy www.smint.com
34 93 495 2727
Smint® Mints Perfete van Melle Lainati, Italy www.smint.com
34 93 495 2727
Spry™ Gum Xlear Inc. Orem, UT www.xlear.com
877-599-5327
Spry™ Mints Xlear Inc. Orem, UT www.xlear.com
877-599-5327
TheraGum® Omni Preventive Care 3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
TheraMints® Omni Preventive Care 3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
Trident® Gum (but not Trident White or Splash)
Cadbury Adams USA LLC Parsippany, NJ www.tridentgum.com
800-874-0013
Trident Xtra Care™ Gum Also contains Recaldent® (casein phosphopetide-amorphous calcium phosphate for remineralization)
Cadbury Adams USA LLC Parsippany, NJ www.tridentgum.com
800-874-0013
Xponent® Xylitol Gum Global Sweet Polyols LLC Rehoboth, MA www.globalsweet.com
800-601-0688
Xponent® Xylitol

Mouth-wetting agentsProduct Manufacturer TelephoneBiotene® Moisturizing Mouth Spray pH 7.0, Bio-active enzymes, amino acids, milk proteins
Laclede Inc.Rancho Dominquez, CAwww.laclede.com
800-922-5856
BioXtra® Moisturizing Gel Milk proteins, salivary enzymes
Bio-X Healthcare Gembloux, Belgiumwww.bioxhealthcare.com
32 (0)81 72 34 65
BioXtra® Gel Mouthspray Milk proteins, salivary enzymes
Bio-X Healthcare Gembloux, Belgiumwww.bioxhealthcare.com
32 (0)81 72 34 65
Caphosol® (Rx) High conc calcium and phosphate ions
Cytogen CorpPrinceton, NJwww.cytogen.com
800-833-3353
Moi-Stir® Oral Spray pH 7.0 (carboxymethylcellulose), sorbitol, glycerin
Kingswood Laboratories Indianapolis, IN
800-968-7772
Numoisyn® Liquid Rx only – contains linseed extract, methylparaben and proplyparaben
Align PharmaceuticalsCary, NCwww.alignpharma.com
919-398-6225
Oasis® Mouthwash & Spray 35% glycerin oral demulcent
GlaxoSmithKlineBrentford, United Kingdomwww.gsk.com
888-825-5249
Oral Balance® Moisturizing Gel pH 6.0, Xylitol sweetener, Bio-active enzymes in a hydroxymethylcellulose base
Laclede Inc.Rancho Dominquez, CAwww.laclede.com
800-922-5856
Oral Balance® Liquid pH 7.0, Xylitol, Bio-active enzymes, 8 amino acids, milk proteins
Laclede Inc.Rancho Dominquez, CAwww.laclede.com
800-922-5856
Saliva Substitute® pH 6.5 (carboxymethylcellulose), sorbitol, mild mint flavor
Roxane Laboratories Inc. Columbus, OH www.roxane.com
800-962-8364
Salivart® Synthetic Saliva pH 6.0-7.0 (carboxymethylcellulose
Gebauer Company Cleveland, OHwww.gebauerco.com
800-321-9348
Thayers® Dry Mouth Spray (Citrus)] pH 6.0, Glycerin, trisamino, lemon flavor
Thayers Natural PharmaceuticalsWestport, CTwww.thayers.com
888-842-9371
TheraSpray® pH 7.0, 1.2% poloxamer 407/dimeticone, xylitol
Omni Preventive Care 3M ESPE Dental ProductsSt. Paul, MNhttp://solutions.3m.com/
800-634-2249
VA OraLube pH 7.0xylitol, 2 ppm F (carboxymethylcellulose)
Only available from VA Hospitals NDC 052859-005
Note: Oral moisturizers/artificial saliva having a pH < 5.5 are not recommended. Examples include MouthKote®, Stoppers 4 Dry Mouth Spray®.

SialogoguesProduct Manufacturer TelephoneBethanechol, 25 mg tablets (generic)
Global PharmaceuticalsChalfont, PAwww.globalphar.com
215-933-0323
Evoxac® (Cevimeline HCl) 30 mg capsules
Daiichi Sankyo Parsippany, NJwww.daiichius.com
877-437-7763
Pilocarpine Hydrochloride Tablets, 5 mg Equivalent to Salagen®
Roxane LaboratoriesColumbus, OHwww.roxane.com
800-962-8364
Pilocarpine Ophthalmic solution 15 ml (4% solution – 40mg/ml) dilute to 600 ml to create 1 mg/ml.
Available from local pharmacies
Salagen® Tablets (Pilocarpine HCl) 5 mg tablets
MGI Pharma, Inc.Bloomington, MNwww.mgipharma.com
800-562-5580
Chlorhexidine Mouthrinses - 0.12% Chlorhexidine Gluconate, 11.6% AlcoholProduct Manufacturer TelephoneDenti-Care® Oral Rinse Medicom USA
Tonawanda, NY www.medicom.ca
800-308-6589
Peridex® Omni Preventive Care 3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
PerioGard® Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
PerioRx® Discus Dental Culver City, CAwww.discusdental.com
800-422-9448
Pro-DenRx® 0.12% Chlorhexidine Rinse
Pro-Dentec Batesville, AK www.prodentec.com
800-228-5595

Fluoride Varnishes - 5% Sodium Fluoride - 22.6 mg/ml F, 22,600 ppm FPRODUCT MANUFACTURER TELEPHONECariFree® - Single dose syringes volume not specified
Oral BioTech Albany, OR www.carifree.com/dentists
866-928-4445
CavityShield® - Unit dose0.25ml and 0.4 ml
Omni Preventive Care 3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
Duraflor® - 10ml Tube Medicom USA Tonawanda, NY www.medicom.ca
800-308-6589
Duraflor® - Unit dose 0.25ml and 0.4ml
Medicom USA Tonawanda, NY www.medicom.ca
800-308-6589
Duraflor® Halo White Varnish Unit dose – 0.5ml
Medicom USA Tonawanda, NY www.medicom.ca
800-308-6589
Duraphat® - 10ml TubePrevident® Varnish - Unit dose - 0.4ml transparent on teeth
Colgate Oral Pharmaceuticals, Inc. Canton, MA www.colgateprofessional.com/
800-372-4346
DuraShield® - Unit dose – 0.4ml Sultan Healthcare Englewood, NJ www.sultanintl.com
800-637-8582
Enamel Pro® Varnish - Unit dose 0.25ml and 0.4ml - Dries white Contains Amorphous Ca Phosphate
Premier Dental Plymouth Meeting, PA www.premusa.com/dental
888-670-6100
Flor-Opal® - Unit dose 0.5ml Syringes Contains Xylitol
Ultradent South Jordan, UT www.ultradent.com
888-230-1420
FluoroDose® - Unit dose - 0.3ml Translucent A-2 shade
Centrix Shelton, CT www.centrixdental.com
800-235-5862
Fluorilaq – 10ml Tube Pascal Company, Inc. Bellevue, WA www.pascaldental.com
800-426-8051
Nupro® 5% Sodium Fluoride Varnish Unit dose - volume not specified
Dentsply International York, PA www.dentsply.com
800-877-0020
Varnishamerica™ - Unit dose 0.25ml and 0.4ml Contains Xylitol Dries to a natural tooth color
Medical Products Laboratories Philadelphia, PA www.medicalproductslaboratories.com/ public-health/varnishamerica.html
800-523-0191
*Unit dose packaging preferred; content per dose may vary with tube packaging.

Fluoride Gels - 1.1% Sodium Fluoride, 5000 ppm, pH 7.0Product Manufacturer TelephoneControlRx™ Omni Preventive Care
3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
Denti-Care® Sodium fluoride Gel Medicom USA Tonawanda, NY www.medicom.ca
800-308-6589
FluorideX® Discus Dental Culver City, CA www.discusdental.com
800-422-9448
FluoriSHIELD® Medical Products Laboratories Philadelphia, PA www.medicalproductslaboratories.com
800-523-0191
NeutraCare® P & G Cincinnati, OH www.oralbprofessional.com
800-543-2577
NeutraGard® Home Care Gel Pascal Company, Inc. Bellevue, WA www.pascaldental.com
800-426-8051
Prevident® Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Pro-DenRx® Neutral Sodium Brush-On Gel
Pro-Dentec Batesville, AK www.prodentec.com
800-228-5595
Topex® Take Home Care® Sultan Dental Products Englewood, NJ www.sultandental.com
800-637-8582
*The 0.4 SnF2 gels such Gel-Kam® and Omni-Gel® are not recommended

Fluoride Toothpastes - 1.1% Sodium Fluoride, 5000 ppm, pH 7.0Product Manufacturer TelephoneControlRx™ Omni Preventive Care
3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
ContolRX™ Sodium fluoride Dentifrice Omni Preventive Care 3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
FluorideX Daily Defense® Discus Dental Culver City, CA www.discusdental.com
800-422-9448
NeutraGard® Advanced Home Care Gel with Dentifrice
Pascal Company, Inc. Bellevue, WA www.pascaldental.com
800-426-8051
Prevident 5000 Plus® Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Prevident 5000 Booster® Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Prevident® 5000 Dry Mouth SLS free formulation
Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Prevident® 5000 Sensitive 5% potassium nitrate
Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Pro-DenRx® Plus Neutral Brush-On Dentifrice Pro-Dentec Batesville, AK www.prodentec.com
800-228-5595

Fluoride Mouthrinses Rx ProductNeutral pH, 0.2% NaF, 900 ppm
Manufacturer Telephone
CaviRinse® Omni Preventive Care 3M ESPE Dental Products St. Paul, MN http://solutions.3m.com/
800-634-2249
Dental Resources Neutral Gel Dental Resources, Inc. Delano, MN www.dentalresourcesinc.com
800-328-1276
Oral-B® Fluorinse® P & G Cincinnatti, OH www.oralbprofessional.com
800-543-2577
Prevident® Dental Rinse Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Pro-DenRx® Neutral Rinse Pro-Dentec Batesville, AK www.prodentec.com
800-228-5595
The 0.2% NaF rinses (900 ppm F) are an acceptable alternative for patients who will not use the 1.0-1.1% NaF gels, although more expensive and not as effective.OTC PRODUCTS - 0.05% NaF, 225 ppm MANUFACTURER TELEPHONEAct® Fluoride Rinse pH 5.8 – 6.6, 0.05%, Alcohol Free
Chattem, Inc Chattanooga, TN www.actfluoride.com
866-228-7467
Fluorigard® Colgate Oral Pharmaceuticals New York, NY www.colgateprofessional.com
800-372-4346
Oral-B® Anti-Cavity RinseAlcohol Free
P & G Cincinnati, OH www.theessentials.com
800-924-4950
Antifungal ProductsGeneric Proprietary Name DirectionsClotrimazole cream Lotrimin®, Mycelex® (1%) Apply to affected area q.i.d.Clotrimazole oral troches Mycelex® Troches 10 mg Let one troche dissolve in mouth 5x dayFluconazole tablets* Diflucan® 100 mg tabs 200 mg stat p.o., then 100 mg q.d. p.o.. Ketoconazole cream Nizoral® 2% Apply to affected area q.i.d.Miconazole cream, powder Monistat® 2% Apply to affected area q.i.d.Nystatin cream, ointment, powder Mycostatin® cream, powder
100,000 units/gramApply to affected area q.i.d.
Nystatin solution** Mycostatin® 100,000 units/ml 4-6 ml swish x 2 min & swallow q.i.d.Nystatin oral pastilles Mycostatin® 200 mg pastilles Let 1 pastille dissolve in mouth 4xdayItraconazole solution* Sporanox® Oral Solution
100 mg/10ml10 ml swish and swallow bid
* Caution with drug interactions when using the azoles systemically. Check drug reference.** Not recommended because of the high sucrose content and need to use at least 4X day