Radiation Protection
170
Rakesh C
-
Upload
rakesh-ca -
Category
Health & Medicine
-
view
884 -
download
0
description
Radiation Protection
Transcript of Radiation Protection

Rakesh C A

Objectives of radiation protection
• The International commission of Radiation protection (ICRP) Stated that “the overall objectives of radiation protection is to provide an appropriate standard of protection for man without unduly limiting the beneficial practices giving rise to radiation exposure”.
• NCRP (1993)- “The goal of radiation protection is to prevent the occurrence of serious radiation induced conditions in exposed persons & to reduce stochastic effects in exposed persons to a degree that is acceptable in relation to the benefits to the individual & society from activities that generate such exposure”.

Protection
• Why?• From What?• Whom to protect?• How to protect?

Protection
• When to protect?

MEASUREMENTS!!!

RADIATION UNITS
• ROENTGEN– unit of radiation exposure that will liberate a charge of 2.58x10-4coulombs/kg of air.
• Independent of the area or field size

Absorbed dose • Deposition of energy in pt by radiation exposure
• Independent of composition of irradiated material and energy of beam
• RAD: unit of absorbed dose
• GRAY: SI unit of absorbed dose
• Gray defined as the quantity of radiation that results in an energy deposition of 1 joule per kilogram.
• I GRAY = 100 RAD• 1RAD = 1 cGY

Dose equivalent
• It is a measure of biological effectiveness of radiation• REM: unit of absorbed dose equivalent• SIEVERT : SI unit
• 1 sievert = 100 rems
• Dose equivalent=Absorbed dose x QF.• REM = RADS X QUALITY FACTOR

Quality factor• It is the parameter used to describe the quality of beam.• Gives the amount of energy deposited per unit length travel.
Expressed in KEV per micron.
Type of radiation Q factorX rays 1 Gamma rays 1Beta particle 1Electrons 1Thermal neutrons 5Other neutrons 20Protons 20 Alpha particle 20

EFFECTIVE DOSE EQUIVALENT
• Purpose – to relate exposure to risk• It is calculated by multiplying the dose equivalent
received by each individual organ or tissue (DT) by an appropriate tissue weighting factor (WT) and summing for all the tissues involved.

o b ta in th eE F F EC TIVE D O SE
to th e p t in m sv
sum o f a ll th e o rg an s an d tissues irrad ia ted
m ultip ly b y th eTIS S U E W E IG H IN G F AC TO R W t
fo r th e tissue o r o rg an co n cern ed
E Q U IVAL E N T D O S Eto th e o rg an in m sv
m ultip ly b y th eR AD IATIO N W E IG H IN G F AC TO R W r
O R Q U AL ITY F AC TO Rfo r th e rad ia tio n used
fo r each o rg an an d tissue es tim ate th eAB S O R B E D D O SE
in m g y

Protection
• Why?• From What?• Whom to protect?• How to protect?

Is there RADIATION in this room?


Radiation - We live with
Natural Radiation: Cosmic rays, radiation within our body, in food we eat, water we drink, house we live in, lawn, building material etc.
Human Body: K-40, Ra-226, Ra-228e.g. a man with 70 kg wt. 140 gm of K
140 x 0.012%0.0168 gm of K-40
0.1 Ci of K-40

Radiation - We live with
Gy/yrNew Delhi 700Bangalore 825Bombay 424Kerala 4000(in narrow coastal strip)

Radiation – We travel with

Radiation - We eat withFood Radioactive levels (Bq/kg)
Daily intake (g/d)
Ra-226 Th-228 Pb-210 K-40
Rice 150 0.126 0.267 0.133 62.4
Wheat 270 0.296 0.270 0.133 142.2
Pulses 60 0.233 0.093 0.115 397.0
Other Vegetables
70 0.126 0.167 -- 135.2
Leafy Vegetables
15 0.267 0.326 -- 89.1
Milk 90 -- -- -- 38.1
Composite Diet
1370 0.067 0.089 0.063 65.0
Dose equivalent=0.315 mSv/yrTotal dose from Natural sources = 1.0 to 3.0 mSv/yr


Natural and Manmade sources

SOURCES OF RADIATION
• Natural radiation: 1. External: Cosmic and gamma radiation2. Internal: radionuclides with in the body
ingested or inhaled• Medical procedures:
1. Diagnostic 2. Therapeutic
• Nuclear weapons/industry/accidents

Electromagnetic Waves
Low HighENERGY
Radio waves
Microwaves
Radar
Infrared
Visible light
Ultra-violet
X-ray
Gamma-ray
Non-ionizing radiation
Ionizing radiation

Primary Types of Ionizing Radiation
• Alpha particles• Beta particles• Gamma rays (or
photons)• X-Rays (or photons)• Neutrons
Ionizing Radiation
alpha particle
beta particle
Radioactive Atom
X-ray
gamma ray

Direct Ionization Caused By:
• Protons
• Alpha Particles
• Beta Particles
• Positron Particles

Indirect Ionization Caused By:
• Neutrons
• Gamma Rays
• X-Rays

DO WE NEED RADIATION
PROTECTION ?


Radiation health effects
CELL DEATH BOTH
TYPEOF
EFFECTS
CELL TRANSFORMATION

Radiation health effects
DETERMINISTICSomaticClinically attributable in the exposed individual
CELL DEATH
STOCHASTICsomatic & hereditaryepidemiologically attributable in large populations
ANTENATALsomatic and hereditary expressed in the foetus, in the live born or descendants
BOTH
TYPEOF
EFFECTS
CELL TRANSFORMATION

• Deterministic
(Threshold/non-stochastic)• Existence of a dose threshold
value (below this dose, the effect is not observable)
• Severity of the effect increases with dose
• A large number of cells are involved
Radiation injury from an industrial source
Deterministic effects

• Cataracts of the lens of the eye 2-10 Gy
• Permanent sterility
• males 3.5-6 Gy
• females 2.5-6 Gy
• Temporary sterility
• males 0.15 Gy
• females 0.6 Gydose
Severity ofeffect
threshold
Threshold Doses for Deterministic Effects

Stochastic Effects
• Stochastic(Non-Threshold)– No threshold – Probability of the effect increases with dose– Generally occurs with a single cell– e.g. Cancer, genetic effects




How much
DNA is
repaired ?

Repair of DNA damage
• RADIOBIOLOGISTS ASSUME THAT THE REPAIR SYSTEM IS NOT 100% EFFECTIVE.

Outcomes after cell exposure
DAMAGE REPAIRED CELL NECROSIS OR APOPTOSIS
TRANSFORMED CELL
DAMAGE TO DNA

10-6
10-12
10-9
10-15
10-3
1 second
1 hour
1 day
1 year
100 years
1 ms
100
109
106
103
Energy deposition
Excitation/ionization
Initial particle tracks
Radical formation
PHYSICAL INTERACTIONS
PHYSICO-CHEMICAL INTERACTIONS
BIOLOGICAL RESPONSE
MEDICAL EFFECTS
Diffusion, chemical reactions
Initial DNA damage
DNA breaks / base damage
Repair processesDamage fixation
Cell killing
Promotion/completion
TeratogenesisCancer
Hereditary defects
Proliferation of "damaged" cells
Mutations/transformations/aberrations
T IM
E (s
ec)
Timing of events leading to radiation effects.

C H A IN O F EVEN TS FO LLO W IN G EXPO SU R E TO IO N IZ IN GR A D IA TIO N
CELL DEATHDETERM INISTIC EFFECTS
CELLULAR TRANSFO RM ATIO NM AY BE SO M E REPAIRSTO CHASTIC EFFECTS
CELLULAR LEVEL
SUBCELLULAR DAM AG E(M EM BRANES, NUCLEI, CHRO M O SO M ES)
m olecular changes(DNA,RNA, ENZYM ES)
free radicals(chem ical changes)
ionisation
exposure

Radiosensitivity [RS]
• RS = Probability of a cell, tissue or organ of suffering an effect per unit of dose.

RS laws (Law of Bergonie & Tribondeau)
Radiosensitivity of living tissues varies with maturation & metabolism;1. Stem cells are radiosensitive. More mature
cells are more resistant2. Younger tissues are more radiosensitive3. Tissues with high metabolic activity are highly
radiosensitive4. High proliferation and growth rate, high
radiosensitivty

Radiosensitivity
Muscle
Bones
Nervous system
Skin
Mesoderm organs (liver, heart, lungs…)
Bone Marrow
Spleen
Thymus
Lymphatic nodes
Gonads
Eye lens
Lymphocytes (exception to the RS laws)
Low RSMedium RSHigh RS

RADIATION EFFECTS
DETERMINISTIC EFFECT• Mechanism is cell killing• Has a threshold dose• Deterministic in nature• Severity increases with dose• Occurs only at high doses• Can be completely avoided • Causal relationship between
radiation exposure and the effect
• Sure to occur at an adequate dose
STOCHASTIC EFFECTMechanism is cell modificationHas no thresholdProbabilistic in natureProbability increases with doseOccurs at even at low dosesCannot be completely avoidedCausal relationship cannot be established at low dosesOccurs only among a small percentage of those exposed

RADIATION EFFECTS
DETERMINISTIC EFFECT• Radiation Sickness• Radiation syndromes
– Haematopoietic syndrome– GI syndrome– CNS syndrome
• Damage to individual organs• Death• Late damage
STOCHASTIC EFFECT• Chromosomal damage• Cancer Induction (Several
years after exposure to radiation)
• Genetic Effects (Hereditary in future generations only)
• Somatic Mutations

SO WE NEED RADIATION
PROTECTION!!!

OBJECTIVES OF RADIATION PROTECTION
• PREVENTION of deterministic effect• LIMITING the probability of stochastic effect
HOW? Up to what point?

We live with1-3 mSv
Can kill4000 mSv
Radiation
Where to stop, where is the safe point?

mSv
Year
Changes in Dose Limit (ICRP)(Safe levels)
0
100
200
300
400
500
1931 1947 1977 1990

Dose Limits (ICRP 60)Occupational Public
Effective dose 20 mSv/yr averaged* 1 mSv in a yrover 5 yrs.
Annual equivalentdose to• Lens of eye 150 mSv 5 mSv• Skin 500 mSv 50 mSv• Hands & Feet 500 mSv
* with further provision that dose in any single yr > 30 mSv (AERB) and =50 mSv (ICRP)

WHAT ISBASIS FOR
DOSE LIMITS?


PRINCIPLESOF
RADIATIONPROTECTION

PRINCIPLES OF RADIATION PROTECTION
1. Justification of practices2. Optimization of protection by
keeping exposure as low as reasonably achievable
3. Dose limitation

Justification of procedure versus the net benefit
i.e. no practice involving exposures to radiation should be adopted unless it provides sufficient benefit to offset the detrimental effects of radiation.

Optimization of protection
Protection should be optimized in relation to
the magnitude of doses,
number of people exposed
for all social and economic strata of patients.

• Optimization of protection can be achieved by optimizing the procedure to administer a radiation dose which is
as low as reasonably achievable,
so as to derive maximum diagnostic information with minimum discomfort to the patient

All doses should be kept
• As
• Low
• As
• Reasonably
• AchievableThe ALARA Principle

HOW TO APPLYTHESE PRINCIPLES IN
DIAGNOSTIC RADIOLOGY?

How much time one works with radiation?
RADIOGRAPHY

Radiation ON Time
Workload=100 exposures/day
CxR = 50x50 m sec = 2500 = 2.5s
LS = 50x800 m sec = 40000=40s
Total time = 45 sec/day
Not greater than 1 min/day

Staff Doses
Dose limit ICRP = 20 mSv/yr.
Radiography work 0.1 mS/yr.
i.e. 1/200th of dose limit

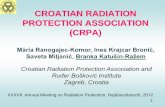
Relative Dose Received
number of chest x-rays0 50 100 150 200
Arm, head,ankle & foot (1)Head & Neck (3)
Head CT (10)Thoracic Spine (18)Mammography, Cystography (20)
Pelvis (24)Abdomen, Hip, Upper & lower femur (28)
Ba Swallow (30)Obsteric abdomen (34)
Lumbo-sacral area (43)Cholangiography (52)
Lumber Myelography (60)Lower abdomen CT male (72)Upper Abdomen CT (73)Ba Meal (76)
Angio-head, Angio-peripheral (80)Urography (87)
Angio-abdominal (120)Chest CT (136)
Lower Abd. CT fem. (142)Ba enema (154)
Lymphan. (180)
mSv.050.150.490.921.01.221.41.51.72.152.593.03.613.673.84.04.366.06.87.137.699.0
Radiation Doses in Radiological Exam. (as multiple of chest x-ray)

IS IT POSSIBLE TO GET DETERMINISTIC EFFECTS IN
RADIOGRAPHIC WORK ?
For staff, for patient..??

Radiography
Risk of Staff Patient Public
DeathSkin burnInfertilityCataractCancerGenetic effect
××××UU
××××UU
××××UU
U: unlikely

FLUOROSCOPYANDCT

Fluoroscopy
Barium study: 3-6 min/pt x 8 patients/d= 40 min/d
ANGIOGRAPHY• Diagnostic = 50 min/d• Therapeutic = 2-5 hr/d
CT = 10-45 min/d

Fluoroscopy (excl. ther angio)
Risk of Staff Patient Public
DeathSkin burnInfertilityCataractCancerGenetic effect
××××UU
××××UU
××××UU
U: unlikely


X-ray tube
Primary beam
Scattered radiation
Patient

Radiation emitted by the X Ray tube
• Primary radiation: before interacting photons• Scattered radiation: after at least one interaction;• Leakage radiation: not absorbed by the X Ray tube
housing shielding• Transmitted radiation: emerging after passage
through matter

X-ray Tube Position
• Position the X-ray tube under the patient not above the patient.
• The largest amount of scatter radiation is produced where the x-ray beam enters the patient.
• By positioning the x-ray tube below the patient, you decrease the amount of scatter radiation that reaches your upper body.
X-ray Tube
Image Intensifier

• TUBE CURRENT• TUBE POTENTIAL• HIGH OR LOW Z TARGET MATERIAL• FILTRATION• TYPE OF WAVEFORM
FACTORS AFFECTING X Ray BEAM

Tube current
• Determines the quantity of the photons which also contribute to the patient dose.
• Increased exposure time also contributes to
an increased patient dose.

X Ray spectrum: tube current
Change of QUANTITYNO change of quality
Effective kV not changed

X Ray spectrum: tube potential
Change in QUANTITY&
Change in QUALITY - spectrum shifts to higher Energy- characteristic lines appear

• use of high KV technique and low mAs (using the
shortest exposure time)• The high KV beam has higher energy photons,
which undergo a lesser degree of beam attenuation and greater penetration of the beam through the patient.
• Therefore the tissue deposition of photons is reduced, which reduces the radiation dose to the patient

A. At high KVp, majority of the photons are of high energy;therefore minimum number of photons are deposited in the patient
(dark area).B. At low KVp, a large number of photons are of low energy;
therefore larger number are deposited in the patient (dark area).

X Ray spectrum: Target Z
Higher Z
Lower Z
X Ray Energy (keV)
Number of X Rays per unit Energy

What is beam filtration?
10 15 20 25 30
15
10
5
Energy (keV)
Nu
mb
er o
f p
ho
ton
s (a
rbit
rary
no
rmal
isat
ion
)
X Ray spectrum at 30 kV for an X Ray tube with a Mo target and a 0.03 mm Mo filter
Absorber placed betweenSource and object
Will preferably absorb the lower energy photons
Or absorb parts of spectrum(K-edge filters)

Tube filtration • Inherent filtration (always present)
– reduced entrance (skin) dose to the patient (cut off the low energy X Rays which do not contribute to the image)
• Additional filtration (removable filter)– further reduction of patient skin and superficial tissue
dose without loss of image quality• Total filtration (inherent + added) • Total filtration must be > 2.5 mm Al for a > 110 kV
generator

Filtration
Change in QUANTITY&
Change in QUALITY spectrum shifts to higher energy
1- Spectrum out of anode2- After window tube housing
(INHERENT filtration)3- After ADDITIONAL filtration

Tube filtration

CollimationCollimate tightly to the
area of interest.Reduces the patient’s
total entrance skin exposure.
Improves image contrast.
Scatter radiation to the operator will also decrease.

• Antiscatter grids
Antiscatter grids reduce scattered radiation reaching the film thus improving the quality of the resulting the radiograph and reducing chances of repeat exposures.
Source of -rays
LeadScattered X Rays
Useful X RaysFilm and cassette
Patient

Patient Protection
• Correct filtration– 0.5 mm Al equivalent (inherent)– Added filtration is good– Minimum total filtration (inherent + added) must
be 2.5 mm Al equivalent – Accurate collimation
• Minimum repeats

• Good technique to avoid re-takes:– use of correct film for the view intended– use of appropriate film holder– correct film placement within film holder– correct placement (angulation) of film holder in
patient’s mouth– correct tube angulation– correct exposure time

AMOUNT & TYPE OF RADIATION EXPOSURE
– TIME
– DISTANCE
– SHIELDING

Time• The exposure time is related to radiation exposure
and exposure rate (exposure per unit time) as follows :
• Exposure time = Exposure Exposure rateOr
Exposure = Exposure rate x Time
The algebraic expressions simply imply that if the exposure time is kept short, then the resulting dose to the individual is small

TIME
- Take foot off fluoro pedal if physician is not viewing the TV monitor
- Use last image hold (freeze frame)
- Five-minute timer
- Use pulsed fluoro instead of continuous fluoro
- Low-Dose mode: 40% dose of Normal fluoro
- Pulsed Low-Dose provides further reduction with respect to Normal Dose continuous mode:
- Use record mode only when a permanent record is required
- Record beam-on time for review

• Distance
• The second radiation protection action relates to the distance between the source of radiation and the exposed individual.
• The exposure to the individual decreases inversely as the square of the distance. This is known as the inverse square law, which is stated mathematically as : 1 I ~ ——— d2

- One step back from tableside:cuts exposure by factor of 4
- Move Image Int. close to patient:less patient skin exposureless scatter (more dose interception by tower)sharper image
- Source to Skin Distance (SSD):38 cm for stationary fluoroscopes30 cm for mobile fluoroscopes

Equipment to Control Distance
• In case of X-ray equipment operating up to 125 kVp, the control panel can be located in the X-ray room.
AERB recommends that the distance between control panel and X-ray unit/chest stand should not be less than 3 m for general purpose fixed x-ray equipment.

• In mobile radiography,
where there is no fixed protective control booth, the technologist should remain at least 2 m from the patient, the x-ray tube, and the primary beam during the exposure.
• In this respect, the ICRP (1982), as well as the NCRP (1989a), recommended that the length of the exposure cord on mobile radiographic units be at least 2 m long

Shielding
• Shielding implies that certain materials (concrete, lead) will attenuate radiation (reduce its intensity) when they are placed between the source of radiation and the exposed individual.

• Lead is used as a radiation shielding material as it has a high atomic number (i.e. 82)
• Atomic number of an element is the number of protons in the nucleus (which is equal to the number of electrons around the nucleus)
• For the photoelectric process, the mass absorption coefficient increases with the cube of the atomic number (z3)

• It is known that
• 0.25 mm lead thickness attenuates 66% of the beam at 75kVp
• and 1mm attenuates 99% of the beam at same kVp.
• It is recommended that for general purpose radiography the minimum thickness of lead equivalent in the protective apparel should be 0.5mm.

- Lead aprons: cut exposure by factor of 20distant scatter: 0.25 mm Pb eqdirect involvement: 0.5 mm Pb
Alpha
Beta
Gamma and X-rays
Neutron
Paper Plastic Lead Concrete
10
n
00 g

Four aspects of shielding in diagnostic radiology
1. X-ray tube shielding
2. Room shielding (a) X-ray equipment room shielding (b) Patient waiting room shielding.
3. Personnel shielding
4. Patient shielding (of organs not under investigation)

1) X-ray tube shielding (Source Shielding)
• The x-ray tube housing is lined with thin sheets of lead because x-rays produced in the tube are scattered in all directions.
• This shielding is intended to protect both patients and personnel from leakage radiation.
• Leakage radiation is that created at the X-ray tube anode but not emitted through the x-ray tube portal.
• Rather, leakage radiation is transmitted through tube housing.

• According to AERB recommendations manufacturers of x-ray devices are required to shield
the tube housing so as to limit the leakage radiation exposure rate to
0.1 R/ hr at a distance of 1 meter from the tube anode.

2) Room shielding (Structural Shielding)
The lead lined walls of Radiology department are referred to as protective barriers because they are designed to protect individuals located outside the X-ray rooms from unwanted radiation.

• There are two types of protective barriers.
(a) Primary Barrier: is one which is directly struck by the primary or the
useful beam.
(b) Secondary Barrier: is one which is exposed to secondary radiation
either by leakage from X-ray tube or by scattered radiation from the patient.

The shielding of X-ray room is influenced by the nature of occupancy of the adjoining area. In this respect two
types of areas have been identified.
Control Area:• Is defined as the area routinely
occupied by radiation workers who are exposed to an occupational dose.
• For control area, the shielding should be such that it reduces exposure in that area to
<26mSv/kg/week
Uncontrolled areas:• Are those areas which are
not occupied by occupational workers.
• For these areas, the shielding should reduce the exposure rate to
<2.6mSv/kg/week

• AERB has laid down GUIDELINES for shielding of X-ray examination room and patient’s waiting room which are as follows.
• The room housing an X-ray unit is not less than 18m2 for general purpose radiography and conventional fluoroscopy equipment.

• In case the installation is located in a residential complex, it is ensured that
1. Wall of the x-ray rooms on which primary x-ray beam falls is not less than 35 cm thick brick or equivalent,
2. Walls of the x-ray room on which scattered x-rays fall is not less than 23 cm thick brick or equivalent
3. There is a shielding equivalent to at least 23 cm thick brick or 1.7 mm lead in front of the doors and windows of the x-ray room to protect the adjacent areas, used by general public

• Unshielded openings in an X-ray room for ventilation or natural light, are located above a height of 2 m.
• Rooms housing fluoroscopy equipment are so designed that adequate darkness can be achieved conveniently, when desired, in the room.

Rooms housing diagnostic X-ray units and related equipment are located as far away as feasible from
• areas of high occupancy and general traffic, • maternity and paediatric wards • and other departments of the hospital that are not
directly related to radiation and its use.

• Shielding of the Xray control room :
• The control room of an X-ray equipment is a secondary protective barrier which has two important aspects:
• (a) The walls and viewing window of the control booth, which should have lead equivalents of 1.5mm. (b) The location of control booth, which should not be located where the primary beam falls directly, and the radiation should be scattered twice before entering the booth

• The AERB recommends the following shielding for the Xray control room:
• The control panel of diagnostic X-ray equipment operating at 125 kVp or above is installed in a separate room located outside but contiguous to the X-ray room and provided with appropriate shielding, direct viewing and oral communication facilities between the operator and the patient

• Patient waiting area
• Patient waiting areas are provided outside the X-ray room.
• A suitable warning signal such as red light and a warning placard is provided at a conspicuous place outside the X-ray room and kept ‘ON’ when the unit is in use to warn persons not connected with the particular examination from entering the room

• 3) Personnel shielding
• Shielding of occupational workers can be achieved by following methods:
• Personnel should remain in the radiation environment only when necessary (step behind the control booth, or leave the room when practical)

• Lead aprons are shielding apparel recommended for use by radiation workers. These are classified as a secondary barrier to the effects of ionizing radiation.

• These aprons protect an individual only from secondary (scattered) radiation, not the primary beam .
• The thickness of lead in the protective apparel determines the protection it provides.

• It is recommended that women radiation workers should wear a customized lead apron that reaches below midthigh level and wraps completely around the pelvis.
• This would eliminate an accidental exposure to a conceptus

Care of the lead apparel: • It is imperative that lead aprons are not abused,
such as by– dropping them on the floor,– piling them in a heap – improperly draping them over the back of a chair.
• Because all of these actions can cause internal fracturing of the lead, they may compromise the apron’s protective ability.

• When not in use, – all protective apparel should be hung on properly
designed racks. • Protective apparel also should be radiographed for
defects such as internal cracks and tears at least once a year

• Other protective apparel include eye glasses with side shields, thyroid shields and hand gloves.
• The minimum protective lead equivalents in hand gloves and thyroid shields should be 0.5mm.

• 4)Patient shielding
• Most radiology departments shield the worker and the attendant, paying little attention to the radiation protection of the patient.
• It has been recommended that the thyroid, breast and gonads be shielded, to protect these organs especially in children and young adults

Rooms
Notification of hazard presenceSigns, Posting, Warning signs
Only authorized users may have access to x-ray devices
Energized equipment must be attended at all times
Lock lab door when equipment not attended

Posting, Warning sign
Door signWarning sign

Exposure to X-ray radiation is reduced if:
TIME exposed to source is decreased
DISTANCE from source is increased
SHIELDING from source is increased
To sum up……

Notable Changes: FDA regs.For equipment manufactured after 10 June 2006:
• Warning Label – “WARNING: This x-ray unit may be dangerous to patient and operator unless safe exposure factors, operating instructions and maintenance scheduled are observed.”
• Timer: audible signal every 5 min of irradiation time until resetAND
Irradiation time display at fluoroscopist’s working position:- means to reset display at zero for new exam/procedure
• Last Image Hold (LIH) after exposure termination- indicate if LIH = radiograph or ‘freeze-frame’ image

RADIATION IN THE CT SUITE

• It has been estimated that although CT accounts for less than 50% of all x-ray examinations it contributes upto 40% of the collective dose from diagnostic radiology .
• CT Scanners have scattered radiation levels that may prove hazardous.
• The dose unit used in CT is the computed tomography dose index “CTDI”.

• This measurement is defined in relation to the radiation field delivered at a specific point (x, y) by the CT Scanner.
• CTDI is usually expressed in terms of absorbed dose to air and is called CTDI air.
• Absorbed dose to tissue (Dtissue) is related to absorbed dose to air (Dair) by a mathematical coefficient which has a value of about 1.06 and an error not greater than ± 1%.

• Such measurements are made using a special pencil ionisation chamber or by a thermoluminescent dosimeter (TLD) .
• Langer et al evaluated scattered radiation in a CT suite and documented that the radiation on the floor of the C.T. suite could be as high as 0.3 Gy/day.

RADIATION PROTECTION IN CT SUITE

It was concluded that
• adequate shielding should be provided for the floor and roof areas of a CT suite depending on which floor the CT is located.
• It was proposed an additional thickness of 2.5mm of lead or 162mm of concrete to shield the front and rear reference points, so as to reduce the dose to 1 mGy/year

• The highly collimated X-ray beam in CT results in markedly non uniform distribution of absorbed dose perpendicular to the tomographic plane during the CT exposure.
• Therefore the size of the CT room housing the gantry of the CT unit as recommended by AERB should not be less than 25m2


• The greatest risk to the fetus of chromosomal abnormalities and subsequent mental retardation is between 8 and 15 weeks of pregnancy and examinations involving radiation to the fetus should be avoided during this period.
• For examinations which may involve rather heavy doses of radiation such as Barium enemas, pelvic or abdominal CT, the examination should be carried out during the first 10 days of the menstrual cycle to avoid irradiating any possible pregnancy

If Pelvic Area in Beam:• No possibility of pregnancy - proceed• Probably pregnant - radiologist decides
– delay X-ray until after delivery, or– use non-X-ray technique (e.g. ultrasound), or– go ahead with X-ray but keep dose low
• Possibly pregnant, low dose procedure - proceed if period is not overdue.
• High dose procedure (10s of mGy, e.g. pelvic CT)
– X-ray in first 10 days of menstrual cycle .

Pregnancy and Mammography“There is no requirement to enquire about pregnancy prior to mammography as there is no significant dose to the fetus”
NHBSP Dec 02
For pregnant staff, • a risk assessment must be performed, • dose to fetus < 1 mSv for rest of pregnancy.

Radiation detection and measurement

• The instruments used to detect radiation are referred to as
radiation detection devices.
• Instruments used to measure radiation are called radiation dosimeters

Devices monitor and record ionizing radiation doses(occupational exposure)
Must distinguish from background radiation
DOSIMETRY

• Personnel Dosimetry
Personnel dosimetry refers to the monitoring of individuals who are exposed to radiation during the course of their work.
Personnel dosimetry policies need to be in place for all occupationally exposed individuals.
The data from the dosimeter are reliable only when the dosimeters are properly worn, receive proper care, and are returned on time.

The radiation measurement is a time-integrated dose, i.e., the dose summed over a period of time, usually about 3 months.
The dose is subsequently stated as an estimate of the effective dose equivalent to the whole body in mSv for the reporting period.
Dosimeters used for personnel monitoring have dose measurement limit of 0.1 - 0.2 mSv

Proper care includes • not irradiating the dosimeter except during
occupational exposure• and ensuring proper environmental conditions
Monitoring is accomplished through the use of personnel dosimeters such as
• the pocket dosimeter, • the film badge • the thermoluminescent dosimeter

Pocket Dosimeter
• Outwardly resembles a fountain pen .
It consists of • a thimble ionization chamber
with an eyepiece and a transparent scale,
• a hollow charging rod• a fixed and a movable fiber.• electrometer----separate
-----built-in (self reading type)

The ability of radiation to produce ionization in air is
the basis for radiation detection by the ionization chamber.
It consists of an electrode positioned in the middle of a cylinder that contains gas.
When x-rays enter the chamber, they ionize the gas to form negative ions (electrons) and positive ions (positrons).

The electrons are collected by the positively charged rod, while the positive ions are attracted to the negatively charged wall of the cylinder.
The resulting small current from the chamber is
subsequently amplified and measured.
The strength of the current is proportional to the radiation intensity.

• Is sensitive for exposures upto 0.2 R
• Disadvantages------
– Easily damaged
– Unreliable in inexperienced hands
– Does not provide a permanent record

Film Badge Monitoring
• These badges use small x-ray films sandwiched between several filters to help detect radiation.
• The photographic effect, which refers to the
ability of radiation to blacken photographic films, is the basis of detectors that use film.

Film badge
detects beta, gamma, X Ray

Wearing the badge -wear the badge on the collar region, because the collar region
including head, neck, and lens of the eyes are unprotected.
Wearing period-• Each member of staff wears film badge for a period of 4
weeks.
• At the end of period the film inside is changed.• The exposed film is sent to BARC.• Useful for detecting radiation at or above 0.1 msv (10 mrem)

Advantages
– inexpensive,
– easy to use,
– permanent record of exposure,
– wide range of sensitivity ( 0.2 – 2000 msv),
– identifies type and energy of exposure,

disadvantages • they are not sensitive enough to capture very low
levels of radiation( < 0.15 msv),
• Their susceptibility to fogging caused by high temperatures , humidity and light means that they cannot and should not be worn for longer than a 4-week period at a stretch,
• Enormous task to chemically process a large number of small films and subsequently compare each to some standard test film.

Thermo luminescent dosimetry (TLD) Monitoring
• The limitations of the film badge are overcome by the thermo luminescent dosimeter (TLD).
• Thermo luminescence is the property of certain materials to emit light when they are stimulated by heat.
• Materials such as lithium fluoride (LiF), lithium borate (Li2B4O7), calcium fluoride (CaF2), and calcium sulfate (CaSO4) have been used to make TLDs

• When an LiF crystal is exposed to radiation, a few electrons become trapped in higher energy levels.
For these electrons to return to their normal energy levels, the LiF crystal must be heated.
As the electrons return to their stable state, light is emitted because of the energy difference between two orbital levels.
The amount of light emitted is measured (by a photomultiplier tube) and it is proportional to the radiation dose.

• The measurement of radiation from a TLD is a two-step procedure.
• In step 1, the TLD is exposed to the radiation.
• In step 2, the LiF crystal is placed in a TLD analyzer, where it is exposed to heat.

• As the crystal is exposed to increasing temperatures, light is emitted.
• When the intensity of light is plotted as a function of the temperature, a glow curve results.
• The glow curve can be used to find out how much radiation energy is received by the crystal because the highest peak and the area under the curve are proportional to the energy of the radiation.


Advantages
• The TLD can measure exposures to individuals as low as 5 mR can withstand a certain degree of heat, humidity, and pressure
• Their crystals are reusable• Is very compact ( suitable even for finger dosimetry)• And instantaneous readings are possible if the department has a TLD
analyzer.• Response to radiation is proportional upto 400 R
Disadvantages
• Very expensive• No permanent record ( other than glow curves)• Cannot distinguish radioactive contamination.
The greatest disadvantage of a TLD is its cost

Storing TLD Badges• Badge must not be left in an area
where it could receive a radiation exposure when not worn by the individual (e.g. On a lab coat or left near a radiation source)
• Store badges in a dark area with low radiation background (in low light away from fluorescent or uv lights, heat and sunlight)
• Lost or damaged badges should be reported immediately to the radiation safety officer and a replacement badge will be issued

The Regulatory Bodies

• There are various Regulatory Bodies at the international and National level, which lay down norms for radiation protection.
• These are • the International Commission for Radiation
Protection ( ICRP),• the National Commission for Radiation Protection
(NCRP ) in America,• and the Atomic Energy Regulatory Board (AERB) in
India.

• The International Commission of Radiation Protection (ICRP) was formed in 1928 on the recommendation of the first International Congress of Radiology in 1925.
• The commission consists of 12 members and a
chairman and a secretary who are chosen from across the world based on their expertise.
• The first International Congress also initiated the birth of the ICRU or the International Commission on Radiation Units and measurements

• The Indian regulatory board is the AERB, Atomic Energy Regulatory Board.
• The Atomic Energy Regulatory Board was constituted on November 15, 1983
• by the President of India by exercising the powers conferred by Section 27 of the Atomic Energy Act, 1962
to carry out certain regulatory and safety functions under the Act.

• Radiation safety in handling of radiation generating equipment is governed by section 17 of the Atomic Energy Act, 1962, and the Radiation Protection Rules (RPR)
• The “Radiation Surveillance Procedures of Medical Applications of Radiation,” specify general requirements for ensuring radiation protection in installation and handling of X-ray equipment. Guidance and practical aspects on implementing the requirements of this Code are provided in revised documents issued by AERB in the year 2001

Dose Limits Recommended by ICRP (1991)
Exposure Dose Limit (mSv per year)Condition
Occupational Apprentices Public(16-18 years)
Whole body: 20 mSv per year, 6 mSv in a year 1 mSv in a year,(effective dose) averaged over defined averaged over period of 5 years with 5 years,
no more than 50 mSvin a single year
Parts of the body:(equivalent dose)Lens of the eye 150 mSv per year 50 mSv in a year 15 mSv in a yearSkin* 500 mSv per year 150mSv in a year 50 mSv in a yearHands and feet** 500 mSv per year 150 mSv in a year 50 mSv in a year
*Averaged over areas of no more than any 1 cm2 regardless of the area exposed. The nominal depth is 7.0 mg cm -2
**Averaged over areas of the skin not exceeding about 100 cm2
Note 1.Dose limit for Women upon declaration of pregnancy - 2 mSv measured on the surface of the abdomen and 1/20th of ALI for exposure to internal emitters.Note 2.Dose limits do not apply to medical exposures, to natural sources of radiation and under conditions resulting from accidents.

Radiation protection survey and programme

• The responsibility for establishing a radiation protection programme rests with the hospital administration / owners of the X-ray facility
• The administration is expected to appoint a Radiation Safety Committee (RSC), and a Radiation Safety Officer (RSO).
• It is recommended by NCRP that the RSC should comprise of a radiologist, a medical physicist,, a senior nurse and an internist. It is the duty of RSC to perform a regular radiation protection survey

This survey has 5 phases which are: 1. Investigation: To obtain information regarding
layout of the department, workload, personnel monitoring and records.
2. Inspection: Each diagnostic installation in the department is examined for its protection status with respect to its operating factors, control booth and availability of protection devices.
3. Measurement: Measurements are conducted on exposure factors. In addition scattered radiation and patient dose measurements in radiography and fluoroscopy are performed.

4. Evaluation: The radiation protection status of the department is evaluated by examination of records, equipment working, status of protective clothing and the radiation doses obtained from phase-3.
5. Recommendations: A report is prepared on the protection status of the department and the problem areas if any identified, for which recommendations are made regarding corrective measures

Thin-window GM (Geiger-Mueller) survey meter may be used to- Check leaking radiation- Indicate x-ray production- Monitor routine operation
Ion chamber is used to determine dose rate at the x-ray field.
SurveyArea
Survey meters are calibrated annually.

Depicts the organizational flow chart and the administrative and functional components of radiation protection program.

CONCLUSION• Protect patient, public and staff• Remember dose is cumulative• Benefit/risk ratio• Principles of radiation protection• Dose reduction = time, distance, shielding
High speed film Lead coats toreduced exp. time steps away stop scatter radiation

Thanks!!!