Radiation Oncology Quality and Safety Considerations in ...
36
Western University Scholarship@Western Oncology Publications Oncology Department 11-11-2016 Radiation Oncology Quality and Safety Considerations in Low Resource Seings: A Medical Physics Perspective Jacob Van Dyk e University of Western Ontario, [email protected] Ahmed Meghzifene Follow this and additional works at: hps://ir.lib.uwo.ca/oncpub Part of the Medical Biophysics Commons , and the Oncology Commons Citation of this paper: Van Dyk, Jacob and Meghzifene, Ahmed, "Radiation Oncology Quality and Safety Considerations in Low Resource Seings: A Medical Physics Perspective" (2016). Oncology Publications. 117. hps://ir.lib.uwo.ca/oncpub/117
Transcript of Radiation Oncology Quality and Safety Considerations in ...
Western UniversityScholarship@Western
Oncology Publications Oncology Department
11-11-2016
Radiation Oncology Quality and SafetyConsiderations in Low Resource Settings: AMedical Physics PerspectiveJacob Van DykThe University of Western Ontario, [email protected]
Ahmed Meghzifene
Follow this and additional works at: https://ir.lib.uwo.ca/oncpub
Part of the Medical Biophysics Commons, and the Oncology Commons
Citation of this paper:Van Dyk, Jacob and Meghzifene, Ahmed, "Radiation Oncology Quality and Safety Considerations in Low Resource Settings: AMedical Physics Perspective" (2016). Oncology Publications. 117.https://ir.lib.uwo.ca/oncpub/117

Author’s Accepted Manuscript
Radiation Oncology Quality and SafetyConsiderations in Low Resource Settings: AMedical Physics Perspective
Jacob Van Dyk, Ahmed Meghzifene
PII: S1053-4296(16)30063-7DOI: http://dx.doi.org/10.1016/j.semradonc.2016.11.004Reference: YSRAO50575
To appear in: Seminars in Radiation Oncology
Cite this article as: Jacob Van Dyk and Ahmed Meghzifene, Radiation OncologyQuality and Safety Considerations in Low Resource Settings: A Medical PhysicsP e r s p e c t i v e , Seminars in Radiation Oncology,http://dx.doi.org/10.1016/j.semradonc.2016.11.004
This is a PDF file of an unedited manuscript that has been accepted forpublication. As a service to our customers we are providing this early version ofthe manuscript. The manuscript will undergo copyediting, typesetting, andreview of the resulting galley proof before it is published in its final citable form.Please note that during the production process errors may be discovered whichcould affect the content, and all legal disclaimers that apply to the journal pertain.
www.elsevier.com/locate/enganabound

Page 1 of 34
RADIATION ONCOLOGY QUALITY AND SAFETY CONSIDERATIONS IN LOW
RESOURCE SETTINGS: A MEDICAL PHYSICS PERSPECTIVE
Jacob Van Dyk, DSc,* Ahmed Meghzifene, PhD+
* Jacob Van Dyk BSc, MSc, FCCPM, FAAPM, FCOMP, DSc(hon), Professor Emeritus,
Departments of Oncology and Medical Biophysics, Western University, London, Ontario,
Canada
+ Ahmed Meghzifene PhD, Section Head, Dosimetry and Medical Radiation Physics Section,
Division of Human Health, Department of Nuclear Sciences and Applications, International
Atomic Energy Agency (IAEA), Vienna, Austria
Address reprint requests to Jacob Van Dyk, DSc, 146 Parks Edge Crescent, London, Ontario,
Canada N6K 3P7. E-mail: [email protected] Phone: 519-472-2951
Disclosure: Jacob Van Dyk has a license agreement with Modus Medical Devices Inc., London,
Ontario, Canada associated with radiation therapy quality assurance equipment.
Page 2 of 34
Abstract
The last few years have seen a significant growth of interest in the global radiation therapy crisis.
Various organizations have quantified the need and are providing aid in support of addressing the
shortfalls existing in many low-to-middle income countries (LMICs). With the tremendous
demand for new facilities, equipment and personnel, it is very important to recognize the quality
and safety challenges and to address them directly. An examination of publications on quality
and safety in radiation therapy indicates a consistency in a number of the recommendations;
however, these authoritative reports were generally based on input from high-resourced contexts.
Here we review these recommendations with a special emphasis on issues that are significant in
LMICs. While multidimensional, training and staffing are top priorities; any support provided to
lower resourced settings must address the numerous facets associated with quality and safety
indicators. Strong partnerships between high-income and other countries will enhance the
development of safe and resource-appropriate strategies for advancing the radiation treatment
process. The real challenge is the engagement of a strong spirit of cooperation, collaboration and
communication between the multiple organizations in support of reducing the cancer divide and
improving the provision of safe and effective radiation therapy.
Page 3 of 34
1. Introduction
There has been a recent increased recognition of the growing cancer crisis, especially in low-to-
middle income countries (LMICs). This is clearly demonstrated by Figure 1(a) which shows a
significant increase in the number of publications dealing with the global cancer problem of
which nearly 30% were published in 2014 and 2015. What is noteworthy, however, is that a
similar publications search on the global radiotherapy problem yielded about 3% of the global
cancer papers and of those about 80% were published in 2014 and 2015 (Figure 1(b)). The most
significant recent report is the Lancet Oncology Commission on global access to radiotherapy1.
This report indicates that radiation therapy (RT) is essential for effective cancer treatment, but the
availability of RT in LMICs is unacceptably low. It quantifies the shortfall in access to RT by
country and globally for 2015 to 2035 based on current and projected need, and it shows the
substantial health and economic benefits to investing in RT in spite of the high up-front costs.
The projections to 2035 indicate the need for very significant growth in RT facilities and
personnel so that 22,000 additional medical physicists will be required in LMICs to meet the
overall demand and recommends an action in human resource capacity building of at least 6,000
newly trained medical physicists by 2025. With this tremendous demand for new facilities,
equipment and personnel, it is important to recognize the quality and safety considerations in the
lower resourced settings and to address them directly as a means of maximizing treatment quality
and minimizing potential patient mis-administrations.
As pointed out in a report by the International Atomic Energy Agency (IAEA) on inequity in
cancer care2, “quality” in health care is a multidimensional concept3 with components of
‘inequality’ (or disparity) encompassing all the other elements of ‘quality’. A program to improve
quality must therefore include activities to address the inequality problem. While this paper does
Page 4 of 34
not address the problems of solving basic inequalities, it does address quality issues related to
societal contexts where RT infrastructure is just being developed.
2. The Radiation Treatment Process and Elements of Quality and Safety
The radiation treatment process is complex with multiple steps and involves various professional
personnel. Elements of quality and safety occur at both the programmatic and individual patient
level as shown in Figure 2.
3. Impact of Quality on Patient Outcome
There is growing quantitative evidence that the quality of radiation treatment has a direct impact
on clinical outcomes. A recent review4 which specifically addressed the question “Does quality
of radiotherapy predict outcomes of multicenter cooperative group trials?” found, through a
thorough literature review, that in nearly half the trials, clinical failure rates were significantly
higher after inadequate versus adequate RT and that significantly worse overall and progression-
free survival occurred after poor quality RT. Peters et al 5 demonstrated significantly inferior
outcomes for those patients with major deficiencies in their treatment plans from data submitted
for review for a large international phase III trial of head and neck cancers comprised of 687
patients. They noted that centers treating only a few patients are the major source of quality
problems. Analogous data regarding dosimetry audit pass rates have been presented by the
Radiological Physics Center / Imaging and Radiation Oncology Core and demonstrated that the
pass rates improved with the number of machines in the department, with a pass rate of about
78% for departments with 1 to 2 machines versus 86% for departments with 5 or more
machines6.

Page 5 of 34
The problem of treatment errors is a more extreme manifestation of poor treatment quality and
has the potential for much more significant negative short term clinical consequences7-10
. New
technologies provide new risks of treatment errors as indicated by the 2009 ICRP report8, the
articles from the New York Times11
and multiple other reports12-15
.
4. Overview of Quality and Safety Considerations
In 1988, the World Health Organization defined quality assurance (QA) as “all those procedures
that ensure consistency of the medical prescription and the safe fulfillment of that prescription as
regards to the target volume, together with minimal dose to normal tissue, minimal exposure of
personnel, and adequate patient monitoring aimed at determining the end result of treatment”16
.
Thus, the components of QA include:
Dose delivered to the target according to the prescription
Safe dose to normal tissues
Minimal dose to personnel
Patient monitoring
Over the years, multiple reports have been written on quality assurance programs and quality
control procedures with the aim of safely delivering the prescribed dose to the patient. However,
in spite of these reports, treatment errors have occurred, albeit in only a very small percentage (1-
2%) of all RT patients treated 17, 18
, with the rate of serious or adverse errors estimated to be
around 0.2% per patient 18, 19
. Over the last decade, various international and national
organizations have provided recommendations on how RT can be made safer. Dunscombe 20
performed a detailed review of seven authoritative reports 8-10, 21-24
published since 2008 which
provided 117 recommendations. Through a mapping exercise, the 117 recommendations were

Page 6 of 34
distilled to 61 unique recommendations with 12 topics being identified in three or more of the
seven documents. These were, in order of most to least cited: training, staffing, documentation,
incident learning, communication, checklists, quality control and preventive maintenance,
dosimetric audit, accreditation, minimizing interruptions, prospective risk assessment, and safety
culture. IAEA TRS43025
summarized common errors in treatment planning to be related to
education, documentation, verification, and communication. Clearly these overlap directly with
the 12 topics identified from the authoritative reports.
5. Issues in Low Resourced Settings
5.1 Planning and Integration of Radiotherapy in National Health Programs
The Lancet Oncology Commission1 on expanding global access to RT had five “Calls for
Action” with the first being a target that 80% of countries should have national cancer plans that
include RT by the year 2020. Clearly, if national plans are not in place, the likelihood of any RT
occurring in the country is low. The access to RT problem is most acute in sub-Saharan Africa,
where most countries almost completely lack radiation therapy facilities. The IAEA is working
together with pre-eminent cancer-related health organizations to leverage the effectiveness of
radiation medicine, particularly in LMICs, by integrating it into comprehensive national cancer
programs26
. They, along with the World Health Organization (WHO), have developed a National
Cancer Control Programme/Plan (NCCP) Core Capacity Self-Assessment Tool that has been
used to obtain a simple and quick qualitative overview of national cancer control planning and
on-going activities. The results from 50 member states highlight specific areas where WHO,
IAEA and partners could strengthen collaboration with countries to leverage on-going
interventions and improve availability of resources. Clearly, cancer plans are essential for RT to
be reasonably organized in a national context.

Page 7 of 34
5.2 Adequate Facilities
In a systematic review of the published literature, Grover et al27
found 49 articles that addressed
RT capacity in LMICs. They concluded that: (1) there is a dearth of publications on RT therapy
infrastructure in LMICs; (2) based on limited published data, availability of RT resources reflects
the countries’ economic status; (3) the challenges of delivering radiation therapy in LMICs are
multidimensional and include: (a) lack of physical resources, (b) lack of human personnel, and
(c) lack of data. Furthermore, access to existing RT and affordability of care remain large
problems.
The Lancet Oncology Commission report1 demonstrated that by the year 2035 the following
resources would be needed in LMICs to provide equal access to RT globally: (1) 6,300
departments with two-megavoltage RT machines each; (2) 12,600 megavoltage RT machines; (3)
6,300 CT scanners; and (4) 30,000 Radiation Oncologists, 22,100 Medical Physicists and 78,300
Radiation Therapists, all to be trained. The second Call for Action in this report is a target of
increasing RT capacity by 25% by 2025.
5.3 Funding for Up-to-Date Equipment
The most significant RT challenges in LMICs include the quality and quantity of physical
resources, the scarceness of skilled human resources, and the unequal distribution of available
resources1, 27, 28
. The number, age, and quality of machines contribute to suboptimal RT capacity
with many countries relying on machines that are more than 20 years old, which brings their
functionality and reliability into question27, 29
. These issues all relate to a lack of adequate
funding, often based on the lack of appropriate NCCPs.

Page 8 of 34
5.4 Trained Staff and Local Education and Training Programs for Clinically Qualified Medical
Physicists
Most reports on the availability of radiation oncology personnel and training programs indicate
that there are not enough qualified professional staff to treat the number of patients requiring RT.
The insufficient number of personnel is in part due to the insufficient number of training
programs available locally. In view of the recognized deficiencies in human resources and
financing, the Lancet Oncology Commission’s1 Actions 3 and 4 aim for training 7,500 radiation
oncologists, 6,000 Medical Physicists and 20,000 Radiation Therapists by 2025 and target a $46
billion investment by 2025 to establish RT and training infrastructure in LMICs.
5.5 Resources for Equipment Parts and Qualified Support Staff for Maintaining Complex RT
Equipment
Efficient equipment service and maintenance are key components of continuous operation of an
RT facility. Stories abound of how equipment in LMICs sits idle because of a lack of
maintenance support or a lack of funding for such support30-32
.
5.6 New Departments Often Start de novo in LMICs
When a new radiation therapy facility is developed in a high income country, basic infrastructure
for planning and architectural design is readily available and education and training programs are
in place to train radiation oncology-related professionals. Furthermore, continuing education
programs and certification procedures are available through professional organizations and
certifying bodies. In many LMICs such support is often not available nor can they get much
support from colleagues from nearby centers because often there are no nearby centers. Thus,
training and education is a very significant challenge in these settings. Furthermore, the planning
of new departments is frequently performed by non-radiation oncology specialists who often do

Page 9 of 34
not understand that radiation oncology-related professional staff should be part of the planning
discussions in developing a new RT facility and should be available before the new center opens
(see Programmatic QA in Figure 2). In addition, decisions on equipment specifications are often
taken without input from a medical physicist, leading to the purchase of inadequate equipment or
lack of connectivity to existing systems. Whatever education and training mechanisms are
developed, they should be as close to home as possible to match the training with the nearby
medical/technological environment and to minimize the “brain drain”33
.
6. Considerations for New Facilities or Upgrade of Existing Facilities
In planning for new departments or additional machines in existing departments, the IAEA has
developed some excellent resources2, 34-36
. Crucial to describing the operation of a new radiation
oncology facility are five principal components: (1) facility design and development, (2)
equipment, (3) consumable materials, (4) human resources and (5) procedures. A clear chain of
authority and communication needs to be established early. One of the general concerns in
developing a new cancer program is that decisions are made from the “top down” sometimes
without consultation with the appropriate radiation oncology-related professionals. This has
resulted in significant cost over-runs and time delays. Once the project to commission a RT
facility has been approved, a team of professionals needs to be constituted to manage the project.
If expertise is not available locally, external experts should be consulted. At a minimum, the team
should include qualified: architect, structural engineer, mechanical engineer, electrical engineer,
cost consultant, clinical medical physicist, and radiation oncologist34
. Ideally, key individuals
will be available as part of the planning process, but the full staffing complement should be
available when the center starts patient treatments.
Page 10 of 34
6.1 Donated Equipment
Resource constraints in LMICs often encourage the consideration of donated medical equipment.
Such donations allow for the surplus from high resource settings to be passed on to low resource
settings; however, if poorly executed, donations could turn into a burden for the recipient,
wasting money, human resources, and with long term implications on the healthcare systems.
Furthermore, the lack of appropriately trained staff could have significant implications for safety
and quality. These issues are of particular significance for the high technology, complex and
expensive equipment used in RT.
The WHO has developed resources on donated equipment including a guidance manual37
. The
following main barriers to effective donation of medical equipment have been identified:
Lack of genuine partnership between donor and recipient
Insufficient appreciation for the challenges of the recipient’s context
Limited standardized inventory of medical equipment in resource constrained settings to
identify needs
Insufficient support for the long term integration of new equipment
Insufficient connectivity between activities of various organizations working on donations
Lack of accountability - no tracking and monitoring of donations and no existing
quantification framework for impact of donations
Insufficient capacity and capacity building programs for recipients
The IOMP working with the AAPM has a joint equipment donation program specifically focused
on equipment associated with radiation medicine. The bottom line, however, is that equipment

Page 11 of 34
donations are often more of a hindrance than help to LMICs; thus, there needs to be well thought
out plans before embarking on the donation of expensive and complex equipment.
7. Lessons Learned from Past Experience
The seven authoritative reports referred to in the Dunscombe paper20
provide guidance on
delivering safe RT, based on lessons learned from past experience – experience which is
primarily based on high income contexts. The question is what the corresponding risks are in
lower income settings. Table 1 lists the topics of the 12 top most cited recommendations made in
these papers. Based on our national and international experience, our interactions with medical
physicists in both low and high income settings, and published reports, we have estimated a level
of risk in LMIC contexts. While not a precise science, it is a way of raising concerns which we
hope will be useful to the development of RT programs. Brief comments are made on several of
the recommendation categories.
7.1 Training
Insufficient numbers of radiation therapy professionals and inadequate training of existing staff
members are one of the main causes of radiation therapy mis-administrations and inferior quality
treatments. “Education” provides the theoretical knowledge and is usually given through
university programs. “Training” provides the skills to perform specialized tasks. For Medical
Physics activities, training is the “on-the-job” learning usually given through a clinical residency
program. In addition to learning how to perform specific tasks, the prime purposes of education
and training of Medical Physicists is to be able to solve unexpected and unique problems,
combined with providing safe, competent, independent and effective service in the clinical
environment. The specialized training for specific technologies can be quickly outdated with the
evolution of new technologies. Both the IOMP38
and the IAEA39
recommend a postgraduate

Page 12 of 34
degree in Medical Physics, generally an MSc or equivalent, and clinical training for a period not
less than two years. European and IAEA surveys indicate that the minimum academic education
and clinical training time frame for employment as a hospital medical physicist varies between
three and nine years, with an average of six years39
.
According to Datta et al28
, 55 LMICs, representing 358 million people, have no access to RT.
Clearly, these 55 countries have no Medical Physics training programs. Even in some countries
with RT, education and training are non-existent or at an embryonic stage. Thus, there is a
“bootstrapping” problem of how to provide education and training without existing experienced
university and clinical staff to lead the necessary education and training programs. There are
several considerations in this context. For development of new facilities or expansion of existing
facilities in LMICs, a multidimensional approach can be used whereby the national government,
international government or non-government agencies, not-for-profit volunteer organizations as
well as foreign hospitals and universities work in partnership to establish or expand existing
programs. Organizations like the IAEA are heavily involved in support of infrastructure
enhancement in low income settings29, 40-42
. Member states of the IAEA can apply for assistance
through their country projects since development of RT programs usually include human
resource improvement components of expert missions, scientific visits, fellowships, and national
courses or workshops40
. Regional and interregional training courses and projects are also
available. In addition, there are multiple volunteer and non-profit organizations in support of
infrastructure and educational development both at the broader and grassroots levels. Examples
include International Cancer Experts Corps (ICEC) (www.ICECcancer.org ) and Medical
Physicists Without Borders (MPWB) (www.mpwb.org ). A link in the latter website
(http://www.mpwb.org/page-18070 ) provides further hyperlinks to multiple organizations in
support of radiation therapy activities in low-to-middle income settings. Novel solutions to

Page 13 of 34
education and training issues are possible through collaboration between international
organizations, local governments, and regional organizations29
.
7.2 Staffing
Inadequate resources mean that multiple facets of healthcare are underfinanced including
equipment and staff. Staffing recommendations have been provided by various organizations.
Many of the original staffing recommendations were based primarily on patient numbers35
. A
European survey indicated that the guidelines across Europe are far from uniform and the metrics
used for capital and human resources are variable43
. Recent, more advanced staffing algorithms
are activity-based and account for patient workload, technology, techniques, procedures and
infrastructure so that they are more relevant for the reality in local circumstances44-46
and are
applicable to environments that range from 2-D RT to intensity modulation with image guidance,
motion management and 4-D considerations. The IAEA algorithm is accompanied by a
spreadsheet calculator so that it can be used as a practical tool for determining staffing levels46
.
7.3 Documentation/Standard Operating Procedures
The literature shows that 70%-80% of incidents (defined as “an unwanted or unexpected change
from a normal system behavior that causes or has the potential to cause an adverse effect to
persons or equipment”) are primarily caused by either lack of, inadequate, or failure to follow
standard procedures18, 47
. Thorough documentation is essential along with the mandate to follow
procedures as documented. Unfortunately, when staffing levels are constrained, documentation is
one of the first things to be compromised. Considerations for reducing treatment uncertainties
include the implementation of clear policies, guidelines and procedures, good documentation of
the policies and procedures as well as the results of acceptance, commissioning and QC tests6. If
the acceptance, commissioning and QC procedures are not documented, then it is effectively

Page 14 of 34
equivalent to not having performed them at all. If there is staff turnover, the new incoming staff
member will not know what procedures have occurred to commission the equipment. If there are
no protocols for patient procedures, it will be difficult to maintain consistency from one patient to
the next. Stringent QA review can have a positive impact on every day clinical practice48
. A
policies and procedures manual should be available in every department and should be reviewed
and updated annually.
7.4 Incident Learning
The Institute of Medicine’s report on “To Err is Human: Building a Safer Health System”49
was
one of the first reports to overtly emphasize that we should learn from our (or others’) mistakes.
Since the year 2000, much activity and publicity has been given on the development of incident
learning systems and various examples have shown how the error rate has been reduced as a
result of openly disclosing errors and learning from past mistakes18, 47, 50
. However, open
disclosure of errors and a well-documented incident learning process requires a working
environment of trust and agreement that patient treatment errors are not the problem of
individuals but they are a result of an inadequate quality management system. Unfortunately, in
the past and in some cultural environments, there is a tendency to want to blame individuals for
patient-related treatment errors. In some cultural contexts, the “no blame” concepts are very
difficult to accept and implement. However, without an overt acceptance of an incident learning
mentality, the error rates are not likely to decrease.
The IAEA has developed a web based user system, SAFety in Radiation ONcology (SAFRON)
for improving the safety and quality of patient care in radiation therapy by sharing knowledge
about incidents and near incidents. SAFRON allows radiotherapy centers to contribute incidents
and near misses to an international learning system, allowing the participating centers to share

Page 15 of 34
and receive information on incidents and near misses. By pooling information on the incidents,
causality and corrective actions, radiotherapy facilities can develop a safety system that can
prevent or reduce the likelihood of an incident occurring at their facility.
7.5 Communication/Questioning
A well-developed safety culture includes an atmosphere of open and non-threatening
communication. The emphasis should be on “no question is a dumb question” so that all staff will
readily ask questions of their peers, superiors and subordinates without feeling intimidated. One
study performed a cross-cultural survey of medical residents to determine perceived barriers in
questioning and challenging authority51
. The conclusion was that organizational and professional
culture may be as important, if not more so, than national culture to encourage "speaking up".
Residents (and staff) should be encouraged to overcome barriers to challenging their colleagues,
and training programs should foster improved relationships and communication between trainers
and trainees.
7.6 Checklists
The fourth most effective risk mitigation strategy proposed by the Institute for Safe Medication
Practices (ISMP) is the use of reminders, double checks and checklists52
. In WHO’s
Radiotherapy Risk Profile9 one of the suggested risk reduction interventions for all stages of the
radiation therapy process includes information transfer with redundancy. However, the challenge
of checklists is the potential for automaticity20
whereby procedures are repeated by rote without
careful thought. This results in the risk of copying errors. This automaticity is a significant
concern in busy understaffed departments as might occur in lower resourced environments. Thus,
an emphasis should be placed on developing policies and procedures that are simultaneously
effective and efficient with appropriate redundancies and checklists.

Page 16 of 34
7.7 Quality Control/Preventative Maintenance
Numerous reports have been written by national and international organizations on QC protocols
for RT-related technologies and procedures, many of which are available on-line53
. Vendors
provide detailed documentation on preventative maintenance procedures. The trend is towards
facility-unique QC programs through the use of failure modes and effects analysis (FMEA)
whereby risk assessment is made on a local basis; however, this is still an evolving process and
has not yet been practically implemented in a low resourced RT environment22
.
7.8 Dosimetric Audit
Dosimetric audits for low income settings have been in use since 1969 by the IAEA/WHO and
have proven to be an invaluable guide for identifying errors and reducing uncertainties54
. These
audits have improved the practice and accuracy of dosimetry in a wide range of RT centers and
have helped in maintaining these levels over time6. Over the years the audits have evolved from
mailed thermoluminescent dosimetry (TLD) measurements under reference conditions to non-
reference conditions55
and then to on-site end-to-end tests56
. These audits have been found so
useful that the IAEA, in its report on Accuracy Requirements and Uncertainties in Radiotherapy6
made the recommendation that “An independent dosimetry audit should be performed for every
new installation that is about to embark on radiation treatments. In addition, regular (e.g. annual)
audits should be performed using remote services or on-site visits (or equivalent).”
The IAEA audit program has been extended to include a review of the total RT care process
including observations concerning buildings, human resources, treatment and dosimetry
equipment, comprehensive patient care, adherence to standards of radiation protection and
establishment of quality assurance program, education and research57
. The quality assurance team
for radiation oncology (QUATRO) program includes an on-site team visit with a radiation
oncologist, medical physicist, radiation therapist, and a fourth member with special competencies

Page 17 of 34
such as a radiation protection officer from the visited country58
. The QUATRO audits have
proved to be a valuable tool for identifying weaknesses in infrastructure, human resources and
procedures in RT centers and have been applied primarily to LMICs.
7.10 Minimizing Interruptions
Interruptions and distractions have been shown to result in significant treatment safety concerns
in different clinical contexts59
60
. General recommendations include “no interruption zones” and
educational programs on risks associated with untimely interruptions. Other factors that were
identified as contributing to errors included cluttered therapy workstations containing multiple
computer monitors as components of various aspects of treatment, and staff traffic patterns that
do not shield the radiation therapist from extraneous conversations and interruptions21
. These
issues could be of additional concern in low income environments with non-optimum ergonomic
settings and understaffed conditions.
7.12 Safety Culture
A patient safety culture is referred to as the employees' shared beliefs, values and attitudes
regarding patient safety in an organization, all of which are reflected in the daily operational
clinical practice. A recent survey61
identified 7 subcultures of a patient safety culture: (a)
leadership, (b) teamwork, (c) evidence-based, (d) communication, (e) learning, (f) just, and (g)
patient-centered. Successful patient error reporting programs are dependent on the level of
importance given by management and it is this level of importance that determines the
organizational culture62
. An organizational culture that seeks to prevent patient harm is
characterized by effective communication, shared values about the importance of safety, and the
presence of systems that help the organization learn from errors and prevent them from occurring.
Reason63
took lessons from industry to make sense of the high number of adverse events in health

Page 18 of 34
care. He indicated that only a systems approach (as opposed to the “person” approach of blaming
an individual) will create a safer health-care culture because it is easier to change the conditions
people work in than change human actions. When a system fails, the immediate question should
be why it failed rather than who caused it to fail, e.g., which safeguards failed? Reason created
the “Swiss cheese” model64
to explain how faults in the different layers of the system can lead to
accidents/mistakes/incidents. According to the Institute of Medicine49
, “the biggest challenge to
moving toward a safer health system is changing the culture from one of blaming individuals for
errors to one in which errors are not treated as personal failures, but as opportunities to improve
the system and prevent harm.”
One manifestation of a patient safety culture is the implementation of a dedicated formal quality
assurance committee consisting of a multidisciplinary team (e.g., radiation oncologists, medical
physicists, medical dosimetrists, and radiation therapists) that meets regularly and serves as
liaison with leadership and hospital-wide safety committees45
.
In summary, a safety culture consists of an environment where patient safety is addressed as (1) a
priority from top management and down, (2) no blame is assigned to (patient) errors - errors are a
systems problem, (3) open communication at all levels is encouraged including an attitude of no
question is too dumb, (4) an error reporting system is in place so that lessons can be learned from
errors, and (5) team work is encouraged, with all team members having equal and important
roles. Unfortunately, different societal/cultural contexts may make a safety culture difficult to
implement; however, it is lessons from transformative organizations that have encouraged the
patient safety culture as being a significant approach to minimizing patient adverse events.

Page 19 of 34
8. Broad Quality and Safety Matters for Low-Resourced Settings
The specific issues for low resourced settings are not all that different from issues that existed
within high resourced settings a number of years ago, with high resourced settings having moved
forward in the meantime. Hopefully the high-resourced contexts can provide guidance and a
higher rate of implementation for lower-resourced circumstances. The broad issues of significant
concern include: (1) support from upper level management and encouragement for quality and
safety considerations along with the development of a QA culture, (2) concern about the lack of
professional recognition of medical physicists, (3) lack of educational infrastructure to educate
and train locally, (4) appropriate budgets especially for radiation technology service and
maintenance, (5) development and recording of quality metrics, and (6) support through national
and international initiatives.
8.1 Administrative Support
Quality and safety will receive much greater emphasis in an environment where they are actively
supported and promoted by senior management. The first general conclusion from a meeting
entitled “Safety in Radiation Therapy: A Call to Action” held in Miami, Florida in June 2010,
which was sponsored by the AAPM and ASTRO and hosted by 13 North American related
organizations, was that “policies and procedures to improve patient safety are successful only if
senior management emphasizes their importance. At the institutional level, safety must be
supported and encouraged by the institution's board of directors and senior management. At the
level of individual services, such as radiation oncology, the physician director, departmental
administrator, chief physicist, and chief therapist must emphasize the importance of patient
safety.”21
In some contexts this requires significant cultural shifts. However, the first step to

Page 20 of 34
transformation is recognition of the issue, the second step is open discussion and the third step is
implementation.
8.2 Professional Recognition of Medical Physicists
The profession of medical physicist is often not understood, primarily as a result its highly
specialized nature as well as its minimal presence in low-income countries65
,66
. High income
countries have about 15 to 20 medical physicists per million population while in developing
countries there may be 1 to 5 per million and in many low-income countries there are none. In
numerous countries, where the profession is not formally recognized, medical physicists are often
recruited and employed under other designations such as technician, biomedical engineer, or
research assistant. Such inappropriate recognition has a direct impact on their socio-economic
and professional status in health-care teams65
. The Bonn Call-for-Action Joint Position Statement
by the IAEA and WHO concluded that recognizing medical physics as a skilled, independent
health care profession, is a key step to strengthening radiation safety culture in health care67
.
8.3 Educational Infrastructure
The Lancet Oncology Commission report1 called for new approaches to train RT professionals
globally, with the creation of new core curricula, innovative learning methods, and international
credentialing to expand the RT workforce. Training should become part of the mandate of each
national RT center to self-propagate the required skills, enabling national expansion of cancer
therapies and providing the ability to replace staff as they leave or are recruited out of country.
Potential tools, techniques and procedures that can aid education and training in resource limited
environments include: (1) e-learning68-71
, (2) e-mentoring/e-rounds72
(e.g.,
http://chartrounds.com/), (3) collaborative course development/education/training39, 73
, and (4)
courses provided by national/international organizations74
.

Page 21 of 34
8.4 Partnerships and Peer-to-Peer Collaborations
While the growing cancer divide is becoming increasingly recognized1, 26, 28, 30, 40, 75
the solution
in support of reducing the divide is very complex since it involves multiple social, economic,
cultural and political facets. , Approaches to improving the availability of safe and effective RT
in LMICs, will require collaboration between multiple organizations including local
governments, regional, international as well as non-government organizations40, 41
. Advanced and
coordinated planning by governments, professional and other not-for-profit volunteer
organizations will be essential to the success of these initiatives. The number of organizations
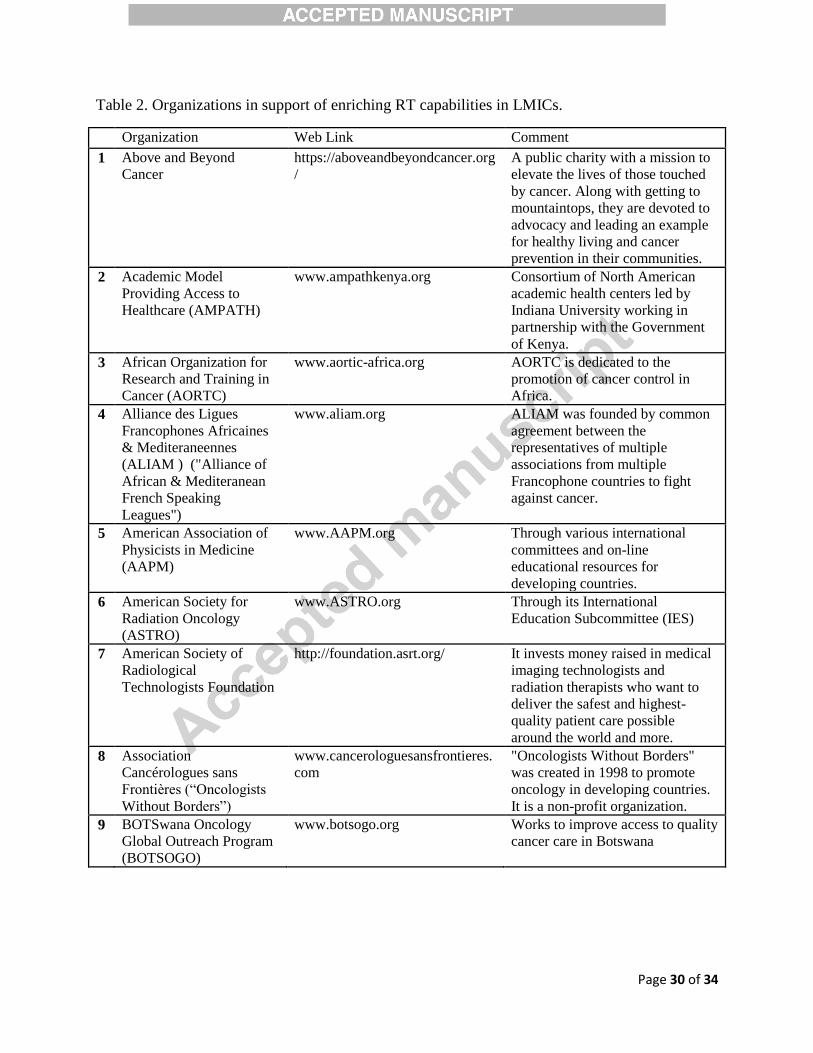
involved is significant as indicated by the 34 examples listed in Table 2. Thus, coordination will
be crucial.
Regarding the involvement of professionals in LMIC contexts, the International Cancer Experts
Corps (ICEC) proposes an altruistic service along with a philosophy that global health becomes
an integral part of the spectrum of academic and professional careers with a goal that 20% of time
be devoted to this activity. Students and residents can also consider this part of their community
service and altruistic efforts76
.
9. Summary and Conclusions
The radiation treatment process is complex involving sophisticated high technology equipment
and multiple professionals including radiation oncologists, medical physicists and radiation
therapists. The complexity, sophistication, high up-front costs and a lack of trained professional
staff have been a deterrent for implementation of RT in many LMICs. However, with appropriate
political and organizational will these barriers can be overcome and indeed are beneficial to both
the healthcare of individuals as well as to a nation’s economic status. The quality, safety and
benefits of radiation treatment are strongly dependent on the quality and safety culture. Strong

Page 22 of 34
partnerships between multiple organizations and countries will enhance the development of safe
and resource-appropriate strategies for advancing the radiation treatment process.
Page 23 of 34
References Reference List
(1) Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol 2015 Sep;16(10):1153-86.
(2) International Atomic Energy Agency (IAEA). Inequity in Cancer Care: A Global Perspective. International Atomic Energy Agency (IAEA), Vienna, Austria, 2011.
(3) Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academy Press, Washington, D.C., 2001.
(4) Fairchild A, Straube W, Laurie F, Followill D. Does quality of radiation therapy predict outcomes of multicenter cooperative group trials? A literature review. Int J Radiat Oncol Biol Phys 2013 Oct 1;87(2):246-60.
(5) Peters LJ, O'Sullivan B, Giralt J, et al. Critical impact of radiotherapy protocol compliance and quality in the treatment of advanced head and neck cancer: results from TROG 02.02. J Clin Oncol 2010 Jun 20;28(18):2996-3001.
(6) International Atomic Energy Agency (IAEA) (In press). Accuracy Requirements and Uncertainties in Radiotherapy. Human Health Series No. 31. International Atomic Energy Agency, Vienna, Austria, 2016.
(7) International Atomic Energy Agency (IAEA). Lessons learned from accidents in radiotherapy. Safety Reports Series 17. International Atomic Energy Agency, Vienna, Austria, 2000.
(8) International Commission on Radiological Protection (ICRP). Preventing Accidental Exposures from New External Beam Radiation Therapy Technologies, ICRP Publication 112. Pergamon Press, Oxford, 2009.
(9) World Health Organization (WHO). Radiotherapy Risk Profile: Technical Manual. World Health Organization, Geneva, 2008.
(10) The Royal College of Radiologists, Society and College of Radiographers, Institute of Physics and Engineering in Medicine, National Patient Safety Agency, British Institute of Radiology. Towards Safer Radiotherapy. The Royal College of Radiologists, London, 2008.
(11) Bogdanich W. Radiation offers new cures and new ways to do harm (http://www.nytimes.com/2010/01/24/health/24radiation.html?_r=0 ) (Accessed 2016-04-15). New York Times 2010.
(12) Amols HI. New technologies in radiation therapy: ensuring patient safety, radiation safety and regulatory issues in radiation oncology. Health Phys 2008 Nov;95(5):658-65.

Page 24 of 34
(13) Baeza M. Accident prevention in day-to-day clinical radiation therapy practice. Ann ICRP 2012 Oct;41(3-4):179-87.
(14) Fraass BA. Impact of complexity and computer control on errors in radiation therapy. Ann ICRP 2012 Oct;41(3-4):188-96.
(15) Fraass BA, Moran JM. Quality, technology and outcomes: evolution and evaluation of new treatments and/or new technology. Semin Radiat Oncol 2012 Jan;22(1):3-10.
(16) World Health Organization (WHO). Quality assurance in radiotherapy. WHO, Geneva, 1988.
(17) Huang G, Medlam G, Lee J, et al. Error in the delivery of radiation therapy: Results of a quality assurance review. Int J Radiat Oncol Biol Phys 2005 Apr 1;61(5):1590-5.
(18) Clark BG, Brown RJ, Ploquin J, Dunscombe P. Patient safety improvements in radiation treatment through 5 years of incident learning. Pract Radiat Oncol 2013 Jul;3(3):157-63.
(19) Kapur A, Goode G, Riehl C, et al. Incident Learning and Failure-Mode-and-Effects-Analysis Guided Safety Initiatives in Radiation Medicine. Front Oncol 2013;3:305.
(20) Dunscombe P. Recommendations for safer radiotherapy: what's the message? Front Oncol 2012;2:129.
(21) Hendee WR, Herman MG. Improving patient safety in radiation oncology. Pract Radiat Oncol 2011 Jan;1(1):16-21.
(22) Huq MS, Fraass BA, Dunscombe PB, et al. A method for evaluating quality assurance needs in radiation therapy. Int J Radiat Oncol Biol Phys 2008;71(1 Suppl):S170-S173.
(23) American Society of Radiation Oncology. Target Safely ( https://www.astro.org/Clinical-
Practice/Patient-Safety/Target-Safely/ Index.aspx ). American Society of Radiation Oncology, 2012.
(24) United States Government of Veterans Affairs. Healthcare Failure Mode and Effect Analysis ( http://www.patientsafety.va.gov/professionals/onthejob/HFMEA.asp ) . United States Government of Veterans Affairs, 2012.
(25) International Atomic Energy Agency (IAEA). Commissioning and Quality Assurance of Computerized Planning Systems for Radiation Treatment of Cancer, IAEA TRS-430. International Atomic Energy Agency, Vienna, Austria, 2004.
(26) Camacho R, Sepulveda C, Neves D, et al. Cancer control capacity in 50 low- and middle-income countries. Glob Public Health 2015 Oct;10(9):1017-31.
(27) Grover S, Xu MJ, Yeager A, et al. A systematic review of radiotherapy capacity in low- and middle-income countries. Front Oncol 2014;4:380.

Page 25 of 34
(28) Datta NR, Samiei M, Bodis S. Radiation therapy infrastructure and human resources in low- and middle-income countries: present status and projections for 2020. Int J Radiat Oncol Biol Phys 2014 Jul 1;89(3):448-57.
(29) Abdel-Wahab M, Bourque JM, Pynda Y, et al. Status of radiotherapy resources in Africa: an International Atomic Energy Agency analysis. Lancet Oncol 2013 Apr;14(4):e168-e175.
(30) Nwankwo KC, Dawotola DA, Sharma V. Radiotherapy in Nigeria: Current Status and Future Challenges. West Afr J Radiol 2013;20:84-8.
(31) Durosinmi-Etti FA. An overview of cancer management by radiotherapy in Anglophone West Africa. Int J Radiat Oncol Biol Phys 1990 Nov;19(5):1263-6.
(32) van der Giessen PH, Alert J, Badri C, et al. Multinational assessment of some operational costs of teletherapy. Radiother Oncol 2004 Jun;71(3):347-55.
(33) Dodani S, Laporte RE. Brain drain from developing countries: how can brain drain be converted into wisdom gain? J R Soc Med 2005 Nov;98(11):487-91.
(34) International Atomic Energy Agency (IAEA). Radiotherapy Facilities: Master Planning and Concept Design Considerations. International Atomic Energy Agency (IAEA), Vienna, Austria, 2014.
(35) International Atomic Energy Agency (IAEA). Setting up a Radiotherapy Programme: Clinical, Medical Physics, Radiation Protection and Safety Aspects. International Atomic Energy Agency, Vienna, Austria, 2008.
(36) International Atomic Energy Agency (IAEA). Planning National Radiotherapy Services: A Practical Tool. IAEA Human Health Series No. 14. International Atomic Energy Agency (IAEA), Vienna, Austria, 2010.
(37) World Health Organization (WHO). Medical Device Donations: Considerations for Solicitation and Provision. World Health Organization (WHO), Geneva, Switzerland, 2011.
(38) International Orgabnization of Medical Physics (IOMP). IOMP Policy Statement No. 2 Basic Requirements for Education and Training of Medical Physicists. International Organization of Medical Physics (IOMP) 2010Available from: URL: http://www.iomp.org/sites/default/files/iomp_policy_statement_no_2_0.pdf
(39) International Atomic Energy Agency (IAEA). Roles and Responsibilities, and Education and Training Requirements for Clinically Qualified Medical Physicists. International Atomic Energy Agency, Vienna, Austria, 2013.
(40) Abdel-Wahab M, Rosenblatt E, Holmberg O, Meghzifene A. Safety in radiation oncology: the role of international initiatives by the International Atomic Energy Agency. J Am Coll Radiol 2011 Nov;8(11):789-94.
(41) Salminen E, Izewska J, Andreo P. IAEA's role in the global management of cancer-focus on upgrading radiotherapy services. Acta Oncol 2005;44(8):816-24.

Page 26 of 34
(42) Salminen E, Anacak Y, Laskar S, et al. Twinning partnerships through International Atomic Energy Agency (IAEA) to improve radiotherapy in common paediatric cancers in low- and mid-income countries. Radiother Oncol 2009 Nov;93(2):368-71.
(43) Dunscombe P, Grau C, Defourny N, et al. Guidelines for equipment and staffing of radiotherapy facilities in the European countries: Final results of the ESTRO-HERO survey. Radiother Oncol 2014 Sep 19.
(44) Battista JJ, Clark BG, Patterson MS, et al. Medical physics staffing for radiation oncology: a decade of experience in Ontario, Canada. J Appl Clin Med Phys 2012;13(1):3704.
(45) American Society of Radiation Oncology (ASTRO). Safety is No Accident: A Framework for Quality Radiation Oncology and Care. American Society of Radiation Oncology (ASTRO), 2012.
(46) International Atomic Energy Agency (IAEA). Staffing in Radiotherapy: An Activity Bases Approach. International Atomic Energy Agency (IAEA), Vienna, Austria, 2015.
(47) Yeung TK, Bortolotto K, Cosby S, Hoar M, Lederer E. Quality assurance in radiotherapy: evaluation of errors and incidents recorded over a 10 year period. Radiother Oncol 2005 Mar;74(3):283-91.
(48) Haworth A, Kearvell R, Greer PB, et al. Assuring high quality treatment delivery in clinical trials - Results from the Trans-Tasman Radiation Oncology Group (TROG) study 03.04 "RADAR" set-up accuracy study. Radiother Oncol 2009 Mar;90(3):299-306.
(49) Homsted L. Institute of Medicine report: to err is human: building a safer health care system. Fla Nurse 2000 Mar;48(1):6.
(50) Williams MV. Radiotherapy near misses, incidents and errors: radiotherapy incident at Glasgow. Clin Oncol (R Coll Radiol) 2007 Feb;19(1):1-3.
(51) Kobayashi H, Pian-Smith M, Sato M, Sawa R, Takeshita T, Raemer D. A cross-cultural survey of residents' perceived barriers in questioning/challenging authority. Qual Saf Health Care 2006 Aug;15(4):277-83.
(52) Kapur A, Potters L. Six sigma tools for a patient safety-oriented, quality-checklist driven radiation medicine department. Pract Radiat Oncol 2012 Apr;2(2):86-96.
(53) Van Dyk J. Radiation Oncology Medical Physics Resources for Working, Teaching, and Learning ( www.medicalphysics.org/documents/vandykch16.pdf ) (Accessed 2016-03-14). In: Van Dyk J (ed). The Modern Technology of Radiation Oncology: A Compendium for Medical Physicists and Radiation Oncologists. Volume 3. Medical Physics Publishing, Madison, WI, 2013. p. 511-54.
(54) Izewska J, Andreo P, Vatnitsky S, Shortt KR. The IAEA/WHO TLD postal dose quality audits for radiotherapy: a perspective of dosimetry practices at hospitals in developing countries. Radiother Oncol 2003 Oct;69(1):91-7.

Page 27 of 34
(55) Izewska J, Georg D, Bera P, et al. A methodology for TLD postal dosimetry audit of high-energy radiotherapy photon beams in non-reference conditions. Radiother Oncol 2007 Jul;84(1):67-74.
(56) Gershkevitsh E, Pesznyak C, Petrovic B, et al. Dosimetric inter-institutional comparison in European radiotherapy centres: Results of IAEA supported treatment planning system audit. Acta Oncol 2014 May;53(5):628-36.
(57) International Atomic Energy Agency (IAEA). Comprehensive Audits of Radiotherapy Practices: A Tool for Quality Improvement. Quality Assurance Team for Radiation Oncology (QUATRO). International Atomic Energy Agency, Vienna, Austria, 2007.
(58) Rosenblatt E, Zubizarreta E, Izewska J, Binia S, Garcia-Yip F, Jimenez P. Quality audits of radiotherapy centres in Latin America: a pilot experience of the International Atomic Energy Agency. Radiat Oncol 2015;10:169.
(59) Anthony K, Wiencek C, Bauer C, Daly B, Anthony MK. No interruptions please: impact of a No Interruption Zone on medication safety in intensive care units. Crit Care Nurse 2010 Jun;30(3):21-9.
(60) Freeman R, McKee S, Lee-Lehner B, Pesenecker J. Reducing interruptions to improve medication safety. J Nurs Care Qual 2013 Apr;28(2):176-85.
(61) Sammer CE, Lykens K, Singh KP, Mains DA, Lackan NA. What is patient safety culture? A review of the literature. J Nurs Scholarsh 2010 Jun;42(2):156-65.
(62) Mutic S, Brame S. Error and Near-Miss Reporting: View from North America. In: Pawlicki T, Dunscombe PB, Mundt AJ, Scalliet P (eds). Quality and Safety in Radiotherapy. Taylor & Francis, Boca Raton, FL, 2011.
(63) Reason J. Human error: models and management. West J Med 2000 Jun;172(6):393-6.
(64) Reason JT. Managing the Risks of Organisational Accidents. Ashgate Publishing Ltd, Aldershot, Hamshire, England, 1997.
(65) Meghzifene A. A call for recognition of the medical physics profession. Lancet 2012 Apr 21;379(9825):1464-5.
(66) Nusslin F, Smith P. Medical physics now classified internationally as a profession. Med Phys 2011 Aug;38(8):i.
(67) International Atomic Energy Agency (IAEA), World Health Organization. Bonn Call-for-Action: 10 Actions to Improve Radiation Protection in Medicine in the Next Decade (http://www.who.int/ionizing_radiation/medical_exposure/bonncallforaction2014.pdf) (Accessed 2016-03-17). 2012.
(68) Frehywot S, Vovides Y, Talib Z, et al. E-learning in medical education in resource constrained low- and middle-income countries. Hum Resour Health 2013;11:4.
Page 28 of 34
(69) Barton MB, Thode RJ. Distance learning in the Applied Sciences of Oncology. Radiother Oncol 2010 Apr;95(1):129-32.
(70) International Atomic Energy Agency (IAEA). The Applied Sciences of Oncology (ASO) Distance Learning Course in Radiation Oncology for Cancer Treatment (Updated Version),Vienna International Atomic Energy Agency, 2010. International Atomic Energy Agency, Vienna, Austria, 2010.
(71) Woo M, Ng K. Real-time teleteaching in medical physics. Biomed Imaging Interv J 2008 Jan;4(1):e13.
(72) Ngwa W, Ngoma T, Zietman A, et al. Closing the Cancer Divide Through Ubuntu: Information and Communication Technology-Powered Models for Global Radiation Oncology. Int J Radiat Oncol Biol Phys 2016 Mar 1;94(3):440-9.
(73) International Atomic Energy Agency (IAEA). Clinical Training of Medical Physicists Specializing in Radiation Oncology. International Atomic Energy Agency, Vienna, Austria, 2010.
(74) Coleman CN, Formenti SC, Williams TR, et al. The international cancer expert corps: a unique approach for sustainable cancer care in low and lower-middle income countries. Front Oncol 2014;4:333.
(75) Grover S, Xu MJ, Yeager A, et al. A systematic review of radiotherapy capacity in low- and middle-income countries. Front Oncol 2014;4:380.
(76) Burkeen J, Coleman CN, Daphtary M, Vikram B. The medical student perspective on global health care in radiation oncology: opportunities, barriers to sustainability, and future directions. Int J Radiat Oncol Biol Phys 2014 Jul 1;89(3):492-4.

Page 29 of 34
Figure Captions
Figure 1. Number of publications from PubMed search done in January 2016: (a) with the words
“global” and “cancer” in the title; (b) with the words “global” and (“radiotherapy” or “radiation
therapy” or “radiation oncology”) in the title.
Figure 2. Elements of quality assurance (QA) activities occur at both the programmatic and
individual patient levels. (Adapted from an unpublished figure from M. Milosevic.)
Tables
Table 1. Top cited recommendations20
for patient safety and estimated level of concern in low-
to-middle income countries.
Recommendation Estimated risk level in LMICs * Very low risk
***** Very high risk
Training *****
Staffing *****
Documentation/SOP ***
Incident learning ***
Communication/questioning ***
Check lists ***
QC/PM ****
Dosimetric audit ****
Accreditation ***
Minimizing interruptions ****
Prospective risk assessment **
Safety culture ***
Page 30 of 34
Table 2. Organizations in support of enriching RT capabilities in LMICs.
Organization Web Link Comment
1 Above and Beyond
Cancer
https://aboveandbeyondcancer.org
/
A public charity with a mission to
elevate the lives of those touched
by cancer. Along with getting to
mountaintops, they are devoted to
advocacy and leading an example
for healthy living and cancer
prevention in their communities.
2 Academic Model
Providing Access to
Healthcare (AMPATH)
www.ampathkenya.org Consortium of North American
academic health centers led by
Indiana University working in
partnership with the Government
of Kenya.
3 African Organization for
Research and Training in
Cancer (AORTC)
www.aortic-africa.org AORTC is dedicated to the
promotion of cancer control in
Africa.
4 Alliance des Ligues
Francophones Africaines
& Mediteraneennes
(ALIAM ) ("Alliance of
African & Mediteranean
French Speaking
Leagues")
www.aliam.org ALIAM was founded by common
agreement between the
representatives of multiple
associations from multiple
Francophone countries to fight
against cancer.
5 American Association of
Physicists in Medicine
(AAPM)
www.AAPM.org Through various international
committees and on-line
educational resources for
developing countries.
6 American Society for
Radiation Oncology
(ASTRO)
www.ASTRO.org Through its International
Education Subcommittee (IES)
7 American Society of
Radiological
Technologists Foundation
http://foundation.asrt.org/ It invests money raised in medical
imaging technologists and
radiation therapists who want to
deliver the safest and highest-
quality patient care possible
around the world and more.
8 Association
Cancérologues sans
Frontières (“Oncologists
Without Borders”)
www.cancerologuesansfrontieres.
com
"Oncologists Without Borders"
was created in 1998 to promote
oncology in developing countries.
It is a non-profit organization.
9 BOTSwana Oncology
Global Outreach Program
(BOTSOGO)
www.botsogo.org Works to improve access to quality
cancer care in Botswana

Page 31 of 34
1
0
ChartRounds www.chartrounds.com ChartRounds brings together
academic disease site specialists
from leading cancer treatment
institutions and connects them
with the Chartrounds network of
over 1300 physicians and medical
physicists.
1
1
Cure4kids www.cure4kids.org Cure4Kids is an online resource
for healthcare professionals
dedicated to enhancing the care of
children who have cancer and
other life-threatening diseases in
countries around the globe.
1
2
European Society for
Radiotherapy and
Oncology
www.estro.org Advances all aspects of Radiation
Oncology through a range of
activities, including teaching
courses in Europe and beyond.
1
3
Foundation for Cancer
Care in Tanzania
www.tanzaniacancercare.org The Foundation for Cancer Care in
Tanzania enhances cancer care to
improve the lives of the citizens of
Tanzania through education,
programs for prevention and
screening, and services providing
treatment and palliation.
1
4
Global Oncology www.globalonc.org Global Oncology is a volunteer
community of physicians,
scientists, designers, engineers,
public health experts, policy
makers, nurses, lawyers, students,
and other professionals working in
teams to help people throughout
the world who are treating cancer
and its related pain.
1
5
Global RT http://globalrt.org GlobalRT is a movement to turn
radiotherapy into a global health
priority. It provides a virtual
platform for education, exchange,
and action around the essential
nature of radiotherapy for cancer
care.
1
6
International Agency for
Research on Cancer
(IARC)
www.iarc.fr IARC is the specialized cancer
agency of the World Health
Organization to promote
international collaboration in
cancer research.
1
7
International Atomic
Energy Agency (IAEA)
(a) Programme of Action
for Cancer Therapy
(PACT)
http://cancer.iaea.org/mission.asp
PACT strives for global
partnerships to confront the cancer
crisis in developing countries, with

Page 32 of 34
(b) Human Health
Campus
(c) Technical Cooperation
https://nucleus.iaea.org/HHW/
https://www.iaea.org/technicalcoo
peration/
WHO, and the Joint Programme
on Cancer Control established in
2009.
Online information resource for
health professionals working in
nuclear medicine, radiation
oncology, medical physics, and
nutrition.
Supports human resource capacity
building, networking, knowledge
sharing, partnership facilitation
and procurement of equipment.
1
8
International Campaign
for Establishment and
Development of Oncology
Centers (ICEDOC)
www.icedoc.org A non-governmental organization
which aims to lessen the human
suffering from cancer all over the
world.
1
9
International Cancer
Experts Corps (ICEC)
www.iceccancer.org "Partnering to transform global
cancer care"
2
0
International Cancer
Research Partnership
(ICRP)
https://www.icrpartnership.org/ ICRP is a unique alliance of cancer
organizations working together to
enhance global collaboration and
strategic coordination of research.
2
1
International Network for
Cancer Treatment and
Research (INCTR)
www.inctr.org A not-for-profit organization
dedicated to helping build capacity
for cancer research and treatment
in developing countries.
2
2
International Organization
for Medical Physics
(IOMP)
www.iomp.org Advances medical physics practice
worldwide by disseminating
scientific and technical
information, fostering educational
and professional development of
medical physics and promoting the
highest quality medical services
for patients.
2
3
Medical Physicists
Without Borders (MPWB)
www.mpwb.org MPWB is a not for profit,
membership-based volunteer
organization to support the
effective and safe use of physics
and technologies in medicine
through advising, training,
demonstrating and/or participating
in medical physics-related
activities, especially in LMICs.
2
4
Mephida www.okonmedphys.com Mephida is an independent NGO
with a novel approach to improve
cancer care in Africa through
medical physics services.
2
5
Physicien Médical Sans
Frontière
www.pmsf.asso.fr French-based non-government
organization with expertise in
Medical Physics and devoted to

Page 33 of 34
the fight against cancer.
2
6
Pink Ribbon Red Ribbon http://pinkribbonredribbon.org A global organization powered by
partnerships, Pink Ribbon Red
Ribbon saves lives from cancer in
countries where the need is
greatest.
2
7
Rad-Aid www.rad-aid.org Its mission is to improve and
optimize access to medical
imaging and radiology in poor and
developing regions of the world
for increasing radiology’s
contribution to global public health
initiatives and patient care.
2
8
Radiating Hope www.radiatinghope.org Volunteer-run, mountain climbing,
cancer-cure focused, non-profit
organization with the mission of
improving cancer care, specifically
radiation oncology care, around
the globe.
2
9
Radiation Safety Without
Borders
https://hps.org/documents/rswb_fl
yer.pdf
An initiative of the Health Physics
Society to provide peer support to
radiation safety professionals in
developing countries.
3
0
TreatSafely Foundation www.treatsafely.org A free, peer-to-peer training and
sharing site that hosts clinically
practical, very useful videos and
documents.
3
1
Union for International
Control of Cancer (UICC)
www.uicc.org The UICC is a membership-based
organization which unites the
cancer community to reduce the
global cancer burden, to promote
greater equity, and to integrate
cancer control into the world
health and development agenda.
3
2
World Cancer Research
Fund International
(WCRF)
www.wcrf.org WCRF is the world’s leading
authority on the link between diet,
weight, physical activity and
cancer. It is a not-for-profit
organization that leads and unifies
a network of cancer prevention
charities with a global reach.
3
3
World Health
Organization (WHO) -
Cancer
www.who.int/cancer/en/ This is the component of the WHO
website devoted to cancer.
3
4
Worldwide Cancer
Research (WCR)
www.worldwidecancerresearch.or
g
WCR is a charity which funds
research anywhere in the world.

Page 34 of 34