Rad T 110
38
Rad T 110 Radiation Monitoring and Protection
-
Upload
dennis-donovan -
Category
Documents
-
view
29 -
download
0
description
Rad T 110. Radiation Monitoring and Protection. Personnel Monitoring. Required when a worker may receive 10% or more of the annual MPD Typically monitoring is done when 1% is expected Placement Collar level Outside the apron if used Second may be used for pregnancy Extremity monitors also. - PowerPoint PPT Presentation
Transcript of Rad T 110

Rad T 110
Radiation Monitoring and Protection

Personnel Monitoring
• Required when a worker may receive 10% or more of the annual MPD– Typically monitoring is done when 1% is
expected
• Placement– Collar level– Outside the apron if used
• Second may be used for pregnancy• Extremity monitors also

Types
• Film badges– 10 mrem to 500 rem– Cheap
• OSL; MC device today– Aluminum oxide which is read by a laser
• Typically worn for 2 months
– 1 mrem and sensitive to 5 keV to 40 MeV of energy

Types cont.
• TLD– Lithium floride– Reasonably sensitive
• Cannot be re-read
• Pocket ionization chambers– Good for immediate feedback
• Not very reliable– Sensitive to mechanical energy

Dosimetry Reports
• Deep
• Eye
• Shallow doses

Patient Protection
• Effective Communication– Verbal messages– Concise instructions– Appropriate communication

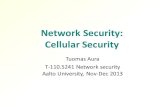
Immobilization
• Voluntary motion– Lack of control– Immobilization devices work with this group
• Involuntary motion– Fast exposure times with high mA helps– Possibly increasing kVp will help
• 15% rule shorter exposure
– Fast film/screen combinations

Beam Limiting Devices
• Diaphragms
• Cones
• Collimators
• Limit the amount of tissue the beam exposes– Also, limit the amount of scatter produced
• Our exposure

Variable Collimator
• 2 sets of lead shutters limit the divergence of the beam
• Collimator and light field – +/- 2% of the SID
• Positive beam limitation (PBL)– Automatic collimator, collimates to the field
size put in the bucky tray

Filtration
• Total filtration– Inherent plus added
filtration
• Inherent– Glass envelope– Oil– Window of the tube
housing– 0.5 mm Al
• Added– Aluminum added to
meet requirements

Total Filtration
• 2.5 mm Al > 70 kVp• 1.5 mm Al 50 – 70 kVp• 0.5 mm Al < 50 kVp• Mobiles/portables and
Fluoro units are required to have at least 2.5 mm Al

Long wavelength photons
Short wavelength photons
Filter

Half Value Layer (HVL)
• This is the amount of aluminum required to reduce the beam intensity to half its original value.
• This is variable based on the selected kVp– As kVp is increased the penetrability of the
beam increases– Therefore, the amount of Al necessary to
halve the beam intensity will have to increase as well.

Protective Shielding
• Gonadal shields– Gonads need to be shielded when they are
within 5cm of the beam– Unless shielding will obscure anatomy– Required to have at least 0.5 mm Pb

Types of Gonadal Shields
• Flat contact
• Shadow
• Shaped contact
• Clear lead

Specific area shielding
• Breast during scoliosis screening– Clear lead filter– PA instead of AP

Compensating filters
• Trough or bilateral wedge– For chest images
• Wedge filter
• Specialized metal filters– Copper


Technical Factors
• Technique charts
• High kVp low mAs techniques– This is within a specific body part or region

Film Processing and QC
• The processor has to work correctly. If not, films will be poor and repeats necessary.
• QC insures that the processor is maintained to a standard level of acceptance

Film/Screen
• Rare earth screens are generally faster– This occurs due to their higher atomic number
which results in a higher absorption of photons. Consequently, more light is produced per photon meaning less photons have to be used for a good film.

Grids
• Prevent scattered radiation from reaching the film.
• They actually increase pt dose.
• However, film quality is dramatically improved.


Repeat Analysis
• Systematic review of repeated films to determine trends that can be eliminated thru education, procedural changes, or equipment maintenance.

Unnecessary Procedures
• Make sure films are completed and recorded.
• Listen to pts about possible previous exams.
• When in doubt ask.

SID
• Must be a minimum of 12 inches
• The longer the SID the lower the pt dose


Digital Imaging
• CR and DR are the two methods currently used for digital diagnostic imaging
• Images are displayed on a computer for viewing– Analogous to digital pictures at home
• Image quality can be manipulated post acquisition– Possible reduction in repeats
Fluoroscopy Procedures
• High pt dose– Potentially high tech exposure
• Exams provide dynamic info
• ‘real time’ feedback for positioning of devices

Dose recording to patients
• ESE– Entrance skin dose
• GSD– Genetically significant dose
• Bone marrow dose

Pregnant pts
• Should not be radiographed– If necessary, informed consent should be
obtained
• Pts needed to be asked about potential pregnancy before the exam begins
Pediatrics
• More radio-sensitive than adults
• More likely to move
• Need to get instructions they understand not fear
• Gonadal shielding collimation

Protection of Personnel
• MPD
• ALARA

Dose Reduction Methods
• No repeats
• Patient is the source of scatter
• Filtration
• Protective apparel
• Technical factors

Pregnant personnel
• Lower MPD
• Protective apparel
• Additional monitoring
• Work schedule alteration

Basic Principles of Protection
• Time
• Distance
• Shielding

Structural Shielding
• Primary– 7 feet high– 1/16 in Pb
• Secondary– 1/32 in Pb
• Operator booth– Photons should scatter at least twice before
entering the booth area– Secondary barrier