
Rachel Garvin, MD Assistant Professor, Department of Neurosurgery, Neurocritical Care Assistant...
50
Rachel Garvin, MD Assistant Professor, Department of Neurosurgery, Neurocritical Care Assistant Professor, Department of Emergency Medicine UNDERSTANDING TRAUMATIC BRAIN INJURY
-
Upload
damian-sherman -
Category
Documents
-
view
219 -
download
0
Transcript of Rachel Garvin, MD Assistant Professor, Department of Neurosurgery, Neurocritical Care Assistant...

Rachel Garvin, MD
Assistant Professor, Department of Neurosurgery, Neurocritical Care
Assistant Professor, Department of Emergency Medicine
UNDERSTANDING TRAUMATIC BRAIN INJURY

OUTLINE
• Statistics• Defining TBI• Secondary injury• Management strategies

TBI STATS
• 2 million TBI’s treated each year in US, one every 15 seconds
• Up to 2% of US population living with TBI
• Leading cause of M&M in ages 1-44
• Single severe TBI victim can generate 4 million dollars in lifetime costs
• Adults ages >75 have highest rates of TBI related hospitalization and death
• 70-90% of TBI worldwide are considered “mild,” 1% of those require a surgical intervention
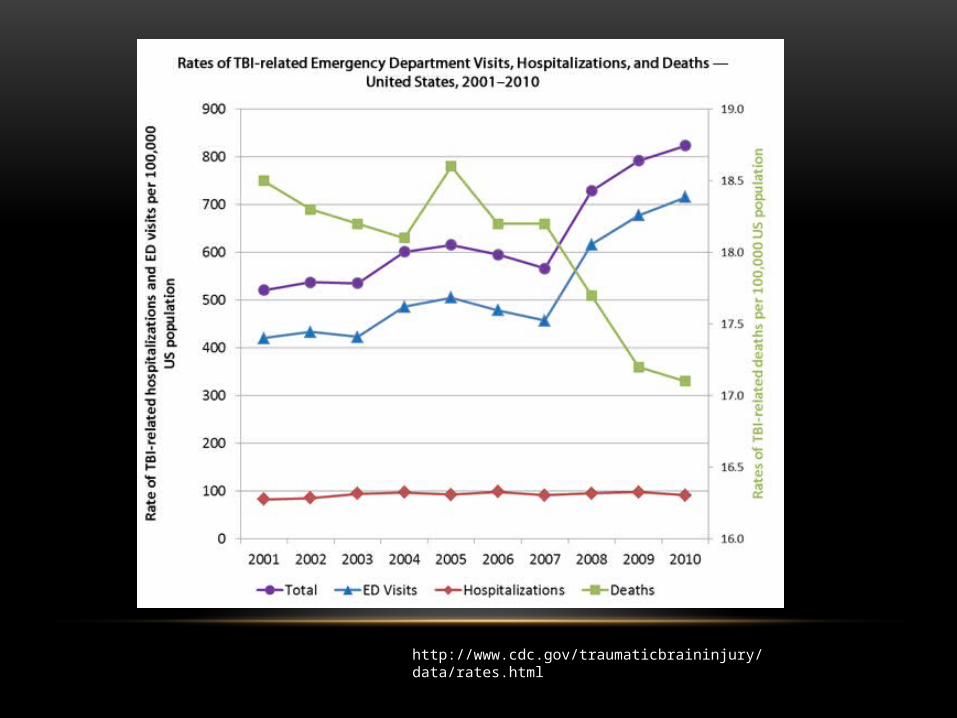
http://www.cdc.gov/traumaticbraininjury/data/rates.html

http://www.cdc.gov/traumaticbraininjury/data/dist_ed.html

CLASSIFICATION OF TBI
• Pathoanatomic
• Physical Mechanism
• Pathophysiologic
• Injury Severity

Pathoanatomic
Epidural
Subdural
Subarachnoid
Contusion
Axonal injury

KNOWING ANATOMY IS IMPORTANT
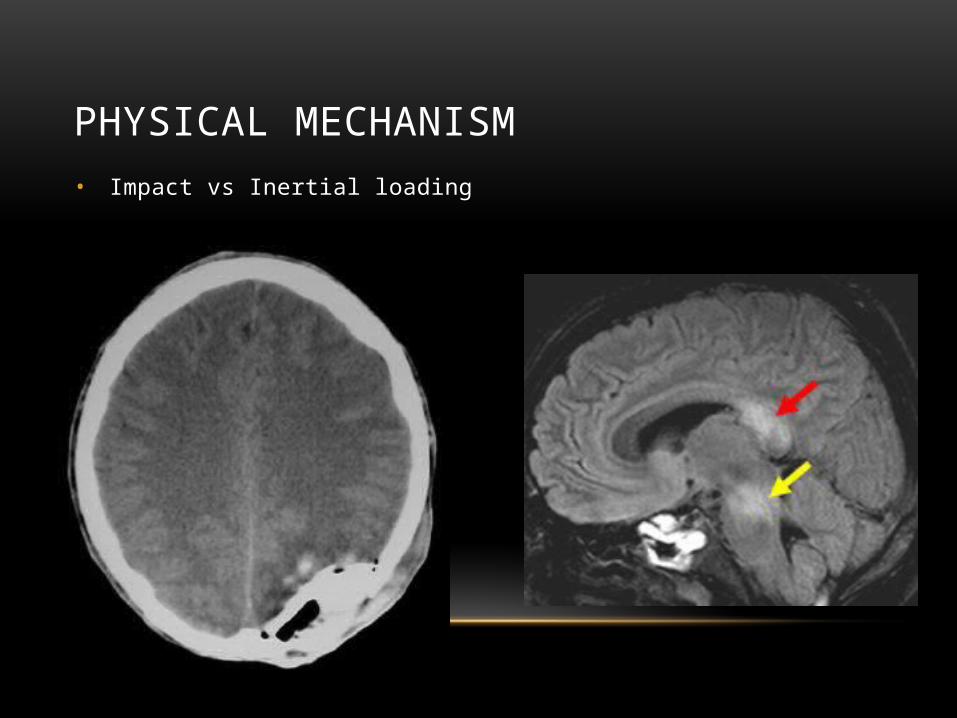
PHYSICAL MECHANISM• Impact vs Inertial loading

INJURY SEVERITY
• GCS
• 13-15 Mild TBI
• 9-12 Moderate TBI
• <8 Severe TBI

PATHOPHYSIOLOGIC
• Primary Injury
• Immediate damage done
• Secondary Injury
• Excitotoxic cascade
• Potentially avoidable factors
• Hypoxia, hypotension, hypercarbia, hyponatremia, seizures

SECONDARY INJURY

GLUTAMATE’S TOXIC EFFECTS

TIME MATTERS

GOALS OF TBI MANAGEMENT
• Preventing secondary injury
• ICP
• CPP
• Neuroprotection
• Good neurologic recovery
PREVENTING SECONDARY INJURY
• Keeping things “normal”
• Avoid processes that increase CMRO2
• Avoiding processes that increase ICP
• Maintain CPP

CEREBRAL METABOLISM
• CMRO2 rate 3.5ml/100g/min
• Accounts for 20% of O2 consumption at rest• Average blood flow of 50ml/100g/min
• CBF <20ml/100g/min = risk for permanent neurologic damage
• CBF <10ml/100g/min = neuronal death
• Uses glucose as primary substrate• >90% glucose consumption is oxidative
• <5% metabolized to lactate
• <1% ketones and others

FICK EQUATION
• CMRO2 = CBF x AVDO2
• AVDO2 = CaO2 – CjvO2
• CBF = CPP/CVR
• CMRO2 = cerebral metabolic rate of oxygen
• AVDO2 = arterio-venous difference in oxygen
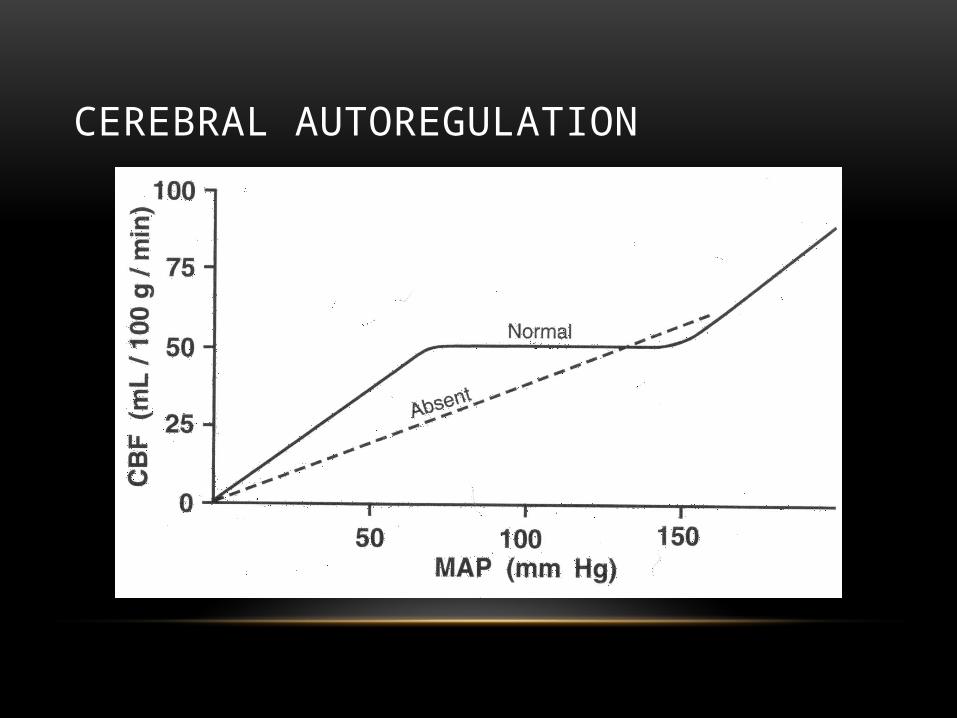
CEREBRAL AUTOREGULATION

BRAIN COMPLIANCE

• Intracranial
• Hematomas/Contusions
• Ischemia
• Hydrocephalus
• Increased CBF
• Extracranial• Hypoxia
• Hypercarbia
• Hyper/Hypotension
• Head rotation
• Fever
• Seizure
• Increased intraabdominal pressure
CAUSES OF INCREASED ICP



DO WE NEED TO MONITOR ICP

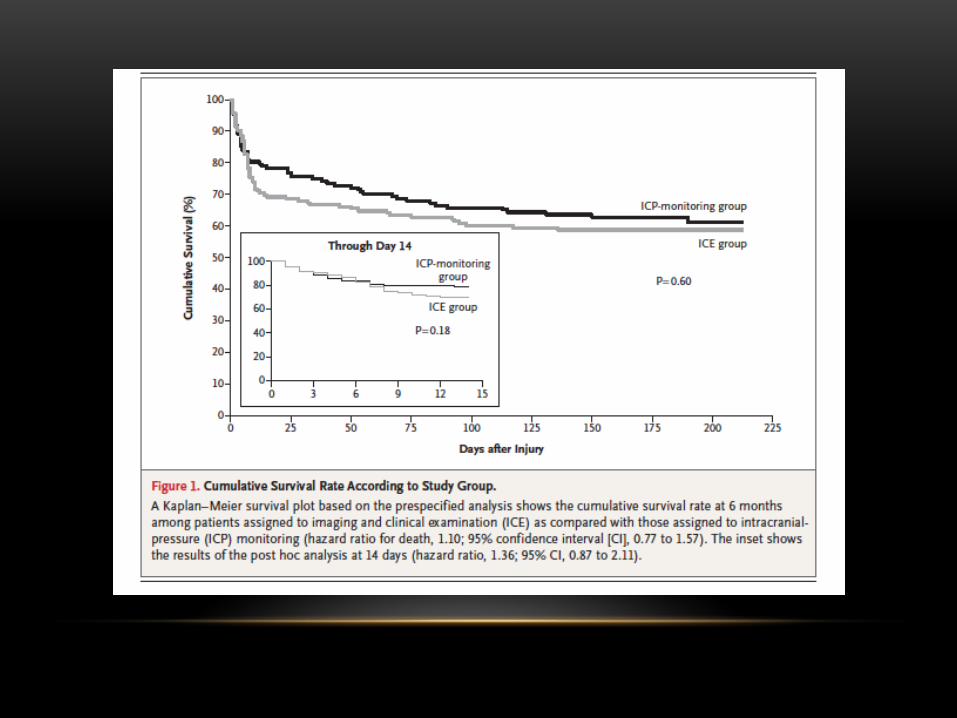
DOES MONITORING ICP IMPROVE OUTCOMES
• Multicenter, randomized, parallel-group trial
• ICP monitor vs imaging and clinical exam
• Inclusion: >13, GCS 3-8
• Groups stratified up by age and severity of injury
• Baseline CT, 48 hours and 5-7 days
• 6 month outcomes with 21 components

MANAGEMENT OF TBI
• ABC’s
• Preventing secondary injury
• ICP management
• Emergent therapies

ABC’S
• Airway
• Avoiding hypoxia
• RSI
• Post-intubation sedation
• Breathing
• Normocarbia
• Circulation
• Avoiding hypotension

TIERED APPROACH TO ICP MANAGEMENT
• Positioning
• Sedation
• Fentanyl, Propofol, Ketamine
• HTS vs Mannitol
• Pentobarbital
• Surgery

• Literature review
• Primary outcome: ICP post-ketamine
• Secondary outcome: CPP, MABP, patient outcome, AE
• Level of evidence assessment (Oxford and GRADE)
• 371 articles 7 articles
• 4 studies with continuous infusion

RESULTS
• Continuous Infusion:
• ICP: no clinically significant difference
• CPP and MABP: 2 studies no difference; 2 studies increase
• Bolus Dosing:
• ICP: no increase; trend towards decrease
• CPP and MABP: 2 no effect documented; 3rd increase CPP and decrease MABP
LEVELS OF EVIDENCE• GRADE level of evidence:
• 2 studies GRADE B
• 4 studies GRADE C
• 1 study GRADE D
• Oxford level of evidence:
• 6 studies level 2b
• 1 level 4
Recommendations: Oxford 2b, GRADE C level of evidence to support that ketamine does not increase ICP


Most often placed within ventricle or brain parenchyma
• Waveforms P1-P3
• P1: percussion wave
• Reflects arterial pressure transmitted through choroid
• P2: tidal wave
• Represents cerebral compliance
• P3: dicrotic wave
• Represents venous pressure
ICP MONITORS

• PBtO2
• Microdialysis
• Brain Temperature Monitoring
• SjvO2
• CBV
MULTI-MODAL MONITORING
EMERGENT TREATMENT
• Hyperventilation
• Decompressive Hemicraniectomy

HYPERVENTILATION
• Decreased PaCO2 alkalinizing CSF cerebral vasoconstriction
• Decreased CBV decreased ICP
• Effects last around 15 hours until CSF pH equilibrates
• Then there is re-dilation of cerebral arteries rebound ICP

• Mannitol
• Rheologic and osmotic effects
• Osmotic effects
• Crosses BBB
• Contraindicated in hypovolemic pts
• HTS
• Rheologic and Osmotic effect
• Can be used in hypovolemic pts
• Can cause hyperchloremic acidosis
MANNITOL VS HYPERTONIC SALINE

HYPEROSMOLAR THERAPY

• For expanding lesions associated with declining neuro status
• Prophylactic
• Need cranioplasty later on
DECOMPRESSIVE HEMICRANI
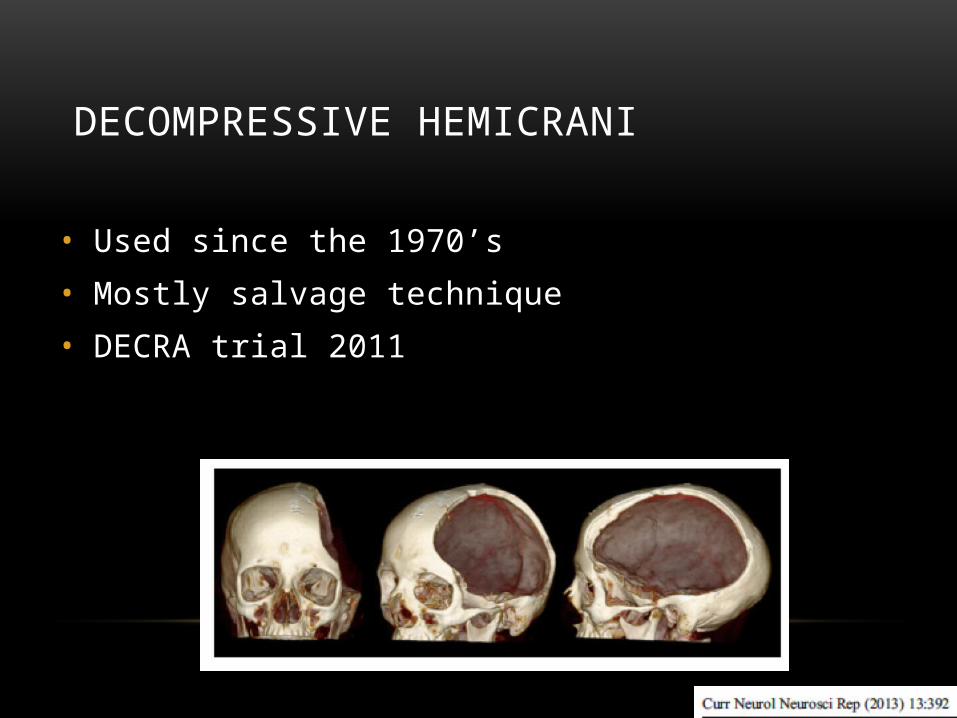
DECOMPRESSIVE HEMICRANI
• Used since the 1970’s
• Mostly salvage technique
• DECRA trial 2011

DECOMPRESSIVE HEMICRANI

OTHER THERAPIES
• Hypothermia
• Progesterone
• ProTECT III -> results now showed no improvement
• Statins
• Citicoline
• Cyclosporine A

PREDICTING OUTCOMES
• Clinical predictors:
• Age, post-resuscitation GCS, hypotension, hypoxia, pupils, multi-system injury
• Radiologic Predictors:
• Absent basal cisterns, midline shift, SAH, brainstem injury
• CRASH and IMPACT prognostic scoring



SUMMARY
• TBI is common and severe TBI can have devastating consequences
• Controlling secondary injury and the excitotoxic cascade are imperative
• ICP, CPP and multi-modality monitoring helpful but data limited
• Hypertonic saline for hyperosmolar therapy
• Surgery is an option
• Prognosis is challenging

QUESTIONS?

REFERENCES• Bazarian JJ, McClung J, Cheng YT, Flesher W, Schneider SM. Emergency department management of mild traumatic brain injury in the USA.
Emerg Med J 2005; 22:473-477
• Brain Trauma Foundation. Guidelines for the Management of Severe Traumatic Brain Injury. Journal of Neurotrauma 2007; 24
• Chestnut RM et al. A Trial of Intracranial-Pressure Monitoring in Traumatic Brain Injury. N Engl J Med 2012; 367: 2471-81.
• Le Roux et al. Consensus Summary Statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care. Neurocrit Care. Published online 11 September 2014.
• Marguiles S, Hicks R. Combination therapies for traumatic brain injury: Prospective considerations. Journal of Neurotrauma 2009; 26:925-939
• Meixensberger J, Jaeger M, Vath A, Dings J, Kunze E, Roosen K. Brain tissue oxygen guided treatment supplementing ICP/CPP therapy after traumatic brain injury. J Neurol Neuroaurg Psychiatry 2003; 74:760-764
• Rangel-Castillo L, Gopinath S, Robertson C. Management of intracranial hypertension. Neurol Clin 2008 May; 26(2): 521-541
• Roberts et al. Sedation for critically ill adults with severe traumatic brain injury: A systematic review of randomized controlled trials. Crit Care Med 2011; 39(12): 2743-2751
• Roozenbeek et al. Prediction of Outcome after Moderate and Severe Traumatic Brain Injury: External Validation of the IMPACT and CRASH Prognostic Models. Crit Care Med 2012; 40(5): 1609-1617
• Saatman KE, Duhaime AC, Bullock R, Maas A, Valadka A, Manley GT. Classification of traumatic brain injury for targeted therapies. Journal of Neurotrauma 2008; 25: 719-738.
• Sterr A, Herron K, Hayward C, Montaldi D. Are mild head injuries as mild as we think? Neurobehavioral concomittants of chronic post-concussion syndrome. BMC Neurology 2006: 1471-2377
• Spiotta AM, Stiefel MF, Gracias VH, Garuffe AM, Kofke WA, Maloney-Wilensky E, Troxel AB, Levine JM, Le Roux PD. Brain tissue oxygen-directed management and outcome in patients with severe traumatic brain injury. J Neurosurg 2010: 113: 571-580
• Thompson HJ, McCormick WC, Kagan SH. Traumatic brain injury in older adults: Epidemiology, outcomes, and future implications.
• Torre-Healy A, Marko NF, Weil RJ. Hyperosmolar Therapy for Intracranial Hypertension. Neurocrit Care 2012; 17: 117-130.


















