
R Balance:Hyponatremia and Hypernatremiavetfolio-vetstreet.s3.amazonaws.com/mmah/82/9534a5... ·...
17
*A companion article on polyuria and polydipsia begins on page 612. a Dr. Lunn discloses that she has received financial support from ContinuEd Continuing Education Company and Fort Dodge Animal Health. everal important terms relating to water balance are defined in the box on page 590. TERMS AND CONCEPTS Body Fluid Balance Balance refers to the ratio of the amount of a substance assimilated into the body to the amount that is lost from the body. When this ratio approximates 1:1 (unity), the body is in bal- ance for that substance. Under normal steady- state conditions, on a day-to-day basis, the volume of total body fluid stays the same; this body fluid balance is achieved when fluid intake and losses are equivalent. Total body water comprises two main compartments: intracel- lular water and extracellular water. The extracellular fluid (ECF) compart- ment is further divided into interstitial water and plasma water. The relative distribution of body water for a typical dog is shown in Figure 1; how- ever, the percentage of total body water in an individual animal is affected by body fat content. 1 Body fluid balance depends on the interrelation- ship between two key components that must be simultaneously kept in balance: salt and water. Salt balance refers to the maintenance of optimal body fluid volume, as shown in Figure 2. It depends primarily on the sodium ion (Na + ) content of the ECF because Na + is the principal extracellular cation. Although the total solute concentrations in the extracellular and intracel- lular compartments are equivalent, their com- positions differ; within cells, potassium and magnesium ions are the principal cations, October 2007 589 COMPENDIUM Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia * Katherine M. James, DVM, PhD, DACVIM Veterinary Information Network Katharine F. Lunn, BVMS, MS, PhD, MRCVS, DACVIM a Colorado State University S ABSTRACT: This article discusses normal and abnormal water balance in small animals.The terms and concepts central to understanding the maintenance of normal salt and water balance and the manifestations of dysregulation are presented, the physiology of body fluid balance is reviewed, and the concepts of sodium content and sodium concentration are explored.The emphasis of this review is that abnormalities of serum sodium concentration are, in fact, abnormalities of water balance.Thus, hyponatremia reflects too much water relative to sodium in the extracellular fluid, whereas hypernatremia reflects a relative deficit of water. Article # 1 CE Illustration by Tamara Rees • Take CE tests • See full-text articles CompendiumVet.com An In-Depth Look: NORMAL AND ABNORMAL WATER BALANCE
Transcript of R Balance:Hyponatremia and Hypernatremiavetfolio-vetstreet.s3.amazonaws.com/mmah/82/9534a5... ·...

*A companion article on polyuria and polydipsia begins on page 612.aDr. Lunn discloses that she has received financial support from ContinuEd ContinuingEducation Company and Fort Dodge Animal Health.
everal important terms relating to waterbalance are defined in the box on page 590.
TERMS AND CONCEPTSBody Fluid Balance
Balance refers to the ratio of the amount of asubstance assimilated into the body to theamount that is lost from the body. When thisratio approximates 1:1 (unity), the body is in bal-ance for that substance. Under normal steady-state conditions, on a day-to-day basis, thevolume of total body fluid stays the same; thisbody fluid balance is achieved when fluid intake
and losses are equivalent. Totalbody water comprises twomain compartments: intracel-lular water and extracellular
water. The extracellular fluid (ECF) compart-ment is further divided into interstitial water andplasma water. The relative distribution of bodywater for a typical dog is shown in Figure 1; how-ever, the percentage of total body water in anindividual animal is affected by body fat content.1
Body fluid balance depends on the interrelation-ship between two key components that must besimultaneously kept in balance: salt and water.
Salt balance refers to the maintenance ofoptimal body fluid volume, as shown in Figure2. It depends primarily on the sodium ion (Na+)content of the ECF because Na+ is the principalextracellular cation. Although the total soluteconcentrations in the extracellular and intracel-lular compartments are equivalent, their com-positions differ; within cells, potassium andmagnesium ions are the principal cations,
October 2007 589 COMPENDIUM
Normal and Abnormal WaterBalance: Hyponatremia andHypernatremia*
Katherine M. James, DVM, PhD, DACVIM
Veterinary Information Network
Katharine F. Lunn, BVMS, MS, PhD, MRCVS, DACVIMa
Colorado State University
S
ABSTRACT: This article discusses normal and abnormal water balance in small animals.The terms
and concepts central to understanding the maintenance of normal salt and water balance and the
manifestations of dysregulation are presented, the physiology of body fluid balance is reviewed, and
the concepts of sodium content and sodium concentration are explored.The emphasis of this
review is that abnormalities of serum sodium concentration are, in fact, abnormalities of water
balance.Thus, hyponatremia reflects too much water relative to sodium in the extracellular fluid,
whereas hypernatremia reflects a relative deficit of water.
Article #1CEIll
ustr
atio
n by
Tam
ara
Rees
•Take CE tests• See full-text articles
CompendiumVet.com
An In-Depth Look:NORMAL AND ABNORMAL WATER BALANCE

replacing Na+. These differences in solute compositionbetween intracellular and extracellular space are main-tained by active ion transport.2
Because Na+ is the principal extracellular cation, andbecause the osmolality of body fluids is regulated withina very narrow range,2 the Na+ content of the body deter-mines the volume of ECF and total body fluid volume.If sodium ions (always with accompanying anions) areadded to the ECF space, the same proportion of watermolecules must be added to the ECF space or theosmolality will increase beyond the limits compatible
COMPENDIUM October 2007
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia590 CE
Content—The total amount of a substance in a givenspace. The content of a substance such as Na+ onlychanges when molecules of that substance are gainedor lost from a body space, such as the extracellularfluid space. This term is used in contrast toconcentration, which reflects the content of asubstance contained within a certain volume of water,typically plasma or urine. Concentrations ofelectrolytes (e.g., Na+) are measured by laboratoryinvestigations. The content of a substance iscalculated by multiplying the concentration of thesubstance by the volume of the fluid space.
Osmolality—The concentration of an osmotic solution,especially when measured in osmoles or milliosmolesper 1,000 g of solvent (usually water). Osmolarity is asimilar term and is often used interchangeably withosmolality when the solvent is water. However,osmolarity refers to the measurement in osmoles or milliosmoles of solute per liter of water—ameasurement of osmoles per volume rather than perweight of solvent.
Osmosis—The movement of water through asemipermeable membrane (such as a cell membrane)into a solution of higher solute concentration thattends to equalize the concentrations of solute on thetwo sides of the membrane. Solutions that causewater to move by osmosis are termed osmoticsolutions.
Tonicity—The osmotic pressure of a solution.The tonicity of a solution (e.g., an intravenous fluidsolution, plasma, urine) is only relevant in referenceto another physiologic system. For example,intravenous fluids are hypertonic, isotonic, orhypotonic relative to plasma. A patient’s plasma is hypertonic, isotonic, or hypotonic relative tonormal plasma. A patient’s urine is hypertonic(hypersthenuria), isotonic (isosthenuria), or hypotonic(hyposthenuria) relative to the patient’s plasma.
Glossary of Important TermsTotal Body Water (TBW)
Intracellular water Extracellular water
Interstitialwater
67%TBW
25%TBW
8%TBW
60%TBW
TBW
Water movesdue to
osmotic forces
75% ofECF volume
25% ofECF
volume
Water movesdue to
Starling’s forces
Plasmawater
Figure 1. The distribution of body fluids bycompartment. Starling’s forces are hydrostatic and oncoticforces that determine fluid movement across capillarymembranes as a result of filtration.
Illus
trat
ion
by T
amar
a R
ees
Figure 2. Normal salt balance exists when the intake ofNa+ in food is equivalent to losses, principally in feces andurine. A dog in normal salt balance has an appropriate number ofNa+ in its total body fluid, including the interstitial space (tan) andthe intravascular space (blue and red vessel representing acomposite of arterial, venous, and capillary blood volumes).Anions (not shown) are present in equal numbers to maintainelectroneutrality.Water molecules are present in appropriateproportion (depicted as equal numbers) to maintain a normalECF osmolality.The cells (depicted by a single representativebrown cell) contain sufficient intracellular osmoles to maintain anequal concentration of water in intracellular fluid and ECF,resulting in an optimal cell volume. (O = osmole)
Illus
trat
ion
by T
amar
a R
ees

with a healthy state. Thus, increasing the number ofsodium ions in the ECF (the Na+ content) increases theECF volume. Similarly, if sodium ions are removedfrom the ECF space, water molecules must leave in pro-portion, thereby reducing the ECF volume; otherwise,the osmolality of the ECF would decrease below thelevel allowed in a healthy individual.
The dog shown in Figure 3 has increased total bodyfluid and ECF volumes due to increased Na+ content.Increased Na+ content can be the result of increaseddietary salt intake or increased renal Na+ retention. Con-versely, the dog shown in Figure 4 has decreased totalbody fluid and ECF volumes due to decreased Na+ con-tent. This solute deficit can result from gastrointestinalor urinary losses.
Water balance (Figure 5) defines the maintenance ofoptimal body fluid tonicity. Tonicity refers to the osmoticpressure of a solution—its ability to cause water to moveacross a membrane. Body fluid tonicity is tightly regu-lated because it determines the volume of the body’scells, which in turn affects cell function.2 Although ECFand intracellular fluid have very different compositions,they must maintain the same solute concentrations (thesame tonicity) so that water can move freely across mostcell membranes. Looking at this concept “in reverse,” thewater concentrations of the ECF and the intracellular
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 591CE
Salt
1 Na+ ingestion
2 Renal Na+ retention
Figure 3. A dog in positive salt balance has too manysodium ions in its total body fluid. Both the interstitial spaceand vascular volume are expanded.The dog can drink water, andthe number of water molecules has increased proportionally tomaintain a normal ECF osmolality.Thus the equilibrium betweenthe intracellular and extracellular fluid spaces is unchanged (redarrows of equal size). Positive salt balance can result from (1) anincrease in salt intake through ingestion or intravenous fluidadministration or (2) renal Na+ retention (blue arrows), such as inpatients with heart failure or cirrhosis.
Illus
trat
ion
by T
amar
a R
ees
3 Diarrhea
1 Renal loss
2 Vomiting
Figure 4. A dog in negative salt balance has too fewsodium ions in its total body fluid. Both the interstitial spaceand vascular volume are reduced.The number of water moleculeshas decreased proportionally through isotonic fluid loss, andnormal ECF osmolality is maintained.With mild negative saltbalance, the equilibrium between the intracellular andextracellular fluid spaces is unchanged (red arrows of equal size).Negative salt balance commonly results from (1) renal or (2 and3) gastrointestinal or urinary fluid loss.Very little Na+ is present invomit; however, without oral replacement of Na+, there will beongoing obligate renal Na+ loss in a vomiting patient.
Illus
trat
ion
by T
amar
a R
ees
Figure 5. Normal water balance exists when waterintake is equal to insensible (nonmeasurable; primarilythrough the respiratory tract) and sensible (measurablein urine and feces) losses. Intracellular fluid and ECF areisotonic (have an equal water concentration); therefore, watermovement is in equilibrium (red arrows of equal size).The volumeof body cells and the plasma osmolality are appropriate.
Illus
trat
ion
by T
amar
a R
ees
fluid must remain the same. Inequalities of water con-centration between body fluid compartments exist onlytransiently because water immediately and rapidly moves

osmolality of body fluids. Glucose and urea make minorcontributions, as reflected in the following equationa:
Plasma osmolality = 2(Na+ concentration [mEq/L]) +(glucose concentration [mg/dl] ÷ 18) +
(BUN concentration [mg/dl] ÷ 2.8)
Osmolality is usually measured by freezing pointdepression, and the measured value is often higher thanthe calculated value because equations such as the onepresented above do not include all osmotically activeparticles present in the plasma.3 The difference betweenthe measured and the calculated values is termed theosmolal gap. In the clinical setting, the term osmolar gapis often used (see the box on page 590 for an explana-tion of the difference between osmolarity and osmolal-ity). This value should be no higher than 10 mOsm/kgin normal dogs.4 Two situations are associated with asignificantly elevated osmolal gap: (1) the presence ofexogenous solutes (e.g., metabolites of ethylene glycol)in the plasma and (2) a reduced fraction of plasma waterresulting from high plasma triglycerides or proteins(e.g., myeloma proteins).
Plasma Na+ concentration accurately reflects plasmatonicity in normal patients. As stated previously, tonicityis the ability of a solution to move water across a mem-brane. This movement affects cellular volume. Hyper-tonicity results when impermeant solutes are added tothe ECF; this promotes cellular dehydration. Hypo-tonicity results from a decrease in the concentration ofimpermeant solutes in the ECF and promotes watermovement into cells and cell swelling. Hypertonic solu-tions are always hyperosmolar. The reverse is not alwaystrue: hyperosmolar solutions are not necessarily hyper-tonic because ineffective osmoles contribute to osmolal-ity but not tonicity. As a clinical example, the additionof glucose to a saline solution with the same Na+ con-centration as plasma results in a hyperosmolar solution.However, the solution is not hypertonic when infusedinto a nondiabetic patient because glucose moves freelyinto cells in the presence of insulin. In a diabetic patient,due to the lack of insulin, glucose is not rapidly taken upby the cells. In this case, the glucose molecules are effec-tive osmoles, rendering the solution hypertonic: water
COMPENDIUM October 2007
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia592 CE
aThis equation is a simplification because it does not accountfor the fact that plasma is only 93% water; that sodium saltsare incompletely dissociated in solution; that some anions arepolyvalent; or that calcium, magnesium, and potassium saltsalso contribute. However, these factors cancel out numerically,allowing 2 × Na+ concentration to be used as an estimate ofthe osmotic effect of the plasma ions.1,2
Figure 6. The hypertonic hyponatremia that occursin unregulated diabetes mellitus is an example oftranslocation hyponatremia. The baseline influence ofintracellular and extracellular osmoles on water movementremains (thick red arrows), but the presence of an additionalimpermeant solute (▲) in the ECF drives water translocationfrom the intracellular to extracellular space (thin red arrows) to maintain an equal concentration of water across the cellmembrane.Thus the proportion of water molecules relative toNa+ in the ECF is increased, resulting in hyponatremia (illustratedby a 2:1 ratio of water to Na+).The dog has a decreasedintracellular fluid volume (shrunken cell and brain) and acorrespondingly increased ECF volume. Because fluid has movedbetween compartments, the dog’s body weight is unchanged.
Illus
trat
ion
by T
amar
a R
ees
to correct these inequalities when the two compartmentshave different tonicities.
Osmolality Versus TonicityThe concentration of solutes in a solvent defines a
solution’s osmolality. Because cell membranes are per-meable to water, and because water will move across amembrane until the solutions on either side of themembrane are isosmolar, the osmolality of plasmareflects the osmolality of total body fluid. When consid-ering how osmolality affects tonicity, it is important todistinguish between permeant and impermeant solutes.Permeant solutes (e.g., urea) move freely across cellmembranes and thus do not induce net water movementwhen they are introduced into a solution; they aretermed ineffective osmoles. Impermeant solutes (e.g., Na+)do not freely move across cell membranes. Thus, they doinduce water movement when introduced into a solu-tion and are termed effective osmoles.
Plasma Na+ concentration is the key determinant of the

moves out of the cells into the ECF, the ECF Na+ con-centration declines, and so-called hypertonic hypona-tremia is observed (Figure 6). When hyperglycemiadevelops slowly, idiogenic osmoles are generated withinthe cells; this helps to increase intracellular water con-tent and mitigate the decrease in cell volume.5
OsmoregulationThe term osmoregulation refers to the control of body
fluid tonicity. Because cell membranes are permeable towater, cells are in osmotic equilibrium with the fluidthat surrounds them. Therefore, by stabilizing bodyfluid tonicity, osmoregulation controls cell volume.Hypothalamic cells called osmoreceptors sense changes intheir own volume in response to an osmotic gradientbetween themselves and plasma.2
Content Versus ConcentrationSeparate mechanisms regulate Na+ content and Na+
concentration (Table 1). The Na+ content of the body isregulated by mechanisms that control the renal excre-tion of Na+,6 which can vary more than 500-fold,depending on Na+ intake and physiologic need. Thesemechanisms operate in response to body fluid volume,not plasma Na+ concentration. The kidneys have evolvedmechanisms to conserve salt; however, the homeostaticmechanisms that control Na+ content are poorly under-stood. Although species differences may exist, many
animals have evolved a salt appetite to increase Na+
intake in salt-deficient states.Regulation of Na+ content is generally a slow process
compared with regulation of Na+ concentration. Whileexcess water intake stimulates the osmoregulatory mecha-nisms and is dealt with very rapidly, many hours passbefore excessive sodium intake (e.g., infusion of isotonicsaline) is corrected by increased renal Na+ excretion.When dietary Na+ intake is increased, it takes several daysto reach a new steady state of neutral Na+ balance.2 Na+
excretion is influenced by several regulatory factors, andmechanisms for Na+ retention are generally better devel-oped than are those for Na+ excretion. It can be extremelydifficult to sort out the roles of the many sensors andmediators involved (Table 1) and understand the relativeimportance of the various regulatory systems.7
In contrast, plasma Na+ concentration is regulated byosmoregulatory control mechanisms.2 Changes inplasma osmolality (pOsm) sensed by the hypothalamicosmoregulatory cells alter the secretion of vasopressin(antidiuretic hormone [ADH]). ADH is the primaryregulator of renal water excretion. Its primary functionis to increase the water permeability of the luminalmembrane of the renal collecting duct through theinsertion of water channels called aquaporins. Water isreabsorbed through these channels in the collectingducts along the concentration gradient established inthe renal medullary interstitium.8 Changes in pOsm also
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 593CE
Table 1. Mechanisms That Sense and Regulate Na+ Content and Na+ Concentrationa
Type of Mechanism RegulationRegulation Signal Sensors Effectors Effected Characteristics
aAdapted from Rose BD: Clinical Physiology of Acid-Base and Electrolyte Disorders, ed 3. New York, Raven, 1992, pp 2837–2872.bEffective plasma volume is a phrase used to describe salt-retaining states. It is not a measurable quantity, and the concept lacks a precisedefinition. It refers to the fullness of the vascular volume and is the portion of the vascular volume that is being sensed by the mechanismsthat regulate body fluid volume. An inadequate effective circulating volume is inferred when salt-retaining mechanisms are activated.
Na+ concentration;osmoregulation(water balance)
Plasmaosmolality
Hypothalamicosmoreceptor
• Vasopressin• Thirst
• Urine osmolality (urineconcentration)
• Water intake
• Rapid• Precise
Na+ content;volume regulation(salt balance)
Effectiveplasmavolumeb
• Carotid sinus• Juxtaglomerular
cell• Atrial pressure
receptors• Hepatic volume
receptors• Cerebrospinal fluid
volume receptors
• Renin–angiotensin–aldosterone system
• Sympatheticnervous system
• Peritubular capillaryhemodynamics
• Atrial natriureticpeptide
Urine Na+
excretion• Slow• Dominant
in deficiency

strongly affect the thirst mechanism. This is whypatients that are deficient in ADH (those with centraldiabetes insipidus) cannot conserve water through renalmechanisms but can maintain a normal pOsm if theyhave access to water.2 In contrast to salt balance andcontrol of body fluid volume, when pOsm changes, thechanges in thirst and ADH secretion and the resultantrenal response are brisk, occurring within minutes.9,10
Hypotension and hypovolemia also stimulate ADHrelease. ADH release is not as sensitive to hemodynamicstimuli as it is to changes in pOsm; however, when thehemodynamic stimulus is sufficiently strong, the ADHresponse will be of greater magnitude, and volume willbe preserved at the expense of decreased osmolality.4
The kidneys have a primary role in water balancethrough their concentrating and diluting functions. Thedetails of these complex hormonally regulated processesare beyond the scope of this article but are summarizedhere and in Figure 7. The osmolality of the glomerular fil-trate as it enters the proximal tubule is identical to that of
plasma. In this segment of the tubule, the bulk of the uri-nary solutes (e.g., Na+ and other electrolytes, amino acids,glucose) and water is reabsorbed isosmotically. As the fil-trate traverses the descending limb of the loop of Henle,water diffuses from the tubule lumen to the hypertonicmedullary interstitium. The tubular fluid then becomesprogressively more dilute as it travels through the ascend-ing limb of the loop of Henle. This diluting process occursbecause active Na+ reabsorption is unaccompanied bywater in this segment. The fluid is hypoosmotic to plasmaon its arrival in the distal tubule. ADH stimulates reab-sorption of sodium chloride in the ascending limb andthus facilitates generation of the renal medullary solutegradient necessary for urinary concentration.11
Hormonal action on the collecting ducts determinesthe final concentration of urine produced. In a state ofantidiuresis, ADH increases water permeability and aug-ments aldosterone-stimulated Na+ reabsorption, therebypromoting water movement from the tubule lumen tothe interstitium for reclamation. In a state of waterdiuresis, when ADH is not present, the collecting ductremains impermeable to water, and dilute urine is pro-duced. Also, in the distal collecting duct, urea permeabil-ity is relatively high and is increased in the presence ofADH; thus, urea moves back into the renal medullaryinterstitium for maintenance of the medullary gradient.2
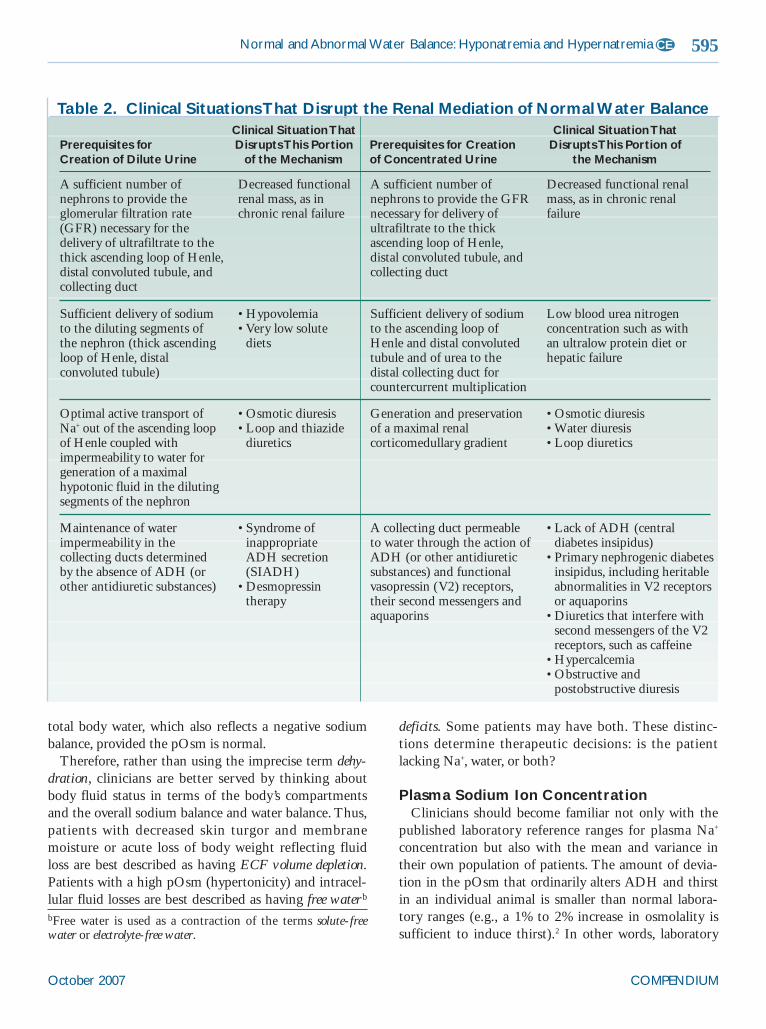
The ability of the kidneys to maintain a normal waterbalance through creation of hypertonic or hypotonicurine can be disrupted in many ways (Table 2). Disor-ders that affect renal concentrating ability are discussedin more detail in the companion article on p. 612.
CONCEPTS OF WATER BALANCE IN CLINICAL SITUATIONSDehydration
Dehydration can have several different meanings,which may lead to confusion and therapeutic error. Onedefinition is based on clinical findings when hydrationtests such as skin turgor, mucous membrane moisture,pulse rate, and capillary refill time are conducted. Typi-cally, when a clinician considers the issue of whether apatient is clinically dehydrated, he or she is referring tophysical examination findings that assess interstitial andplasma fluid volume status.12 These findings reflect thepatient’s low ECF volume and negative sodium balance.However, another definition of dehydration is a decreasein intracellular water (i.e., dehydrated cells). Thisreflects a high plasma tonicity and a problem of negativewater balance. Yet another definition is a decrease in
COMPENDIUM October 2007
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia594 CE
Proximal tubule Loop of Henle Distal tubule Collecting duct
H2O
H2O
H2O
H2O
H2O
H2O
NaCl
NaCl
NaCl
NaCl
NaCl
Urea
V2 ADH
ADH
V2
Figure 7. Differences in solute transport and waterpermeability in specific nephron segments are essentialto renal concentrating and diluting ability. In the presenceof ADH, water channels (V2) allow water to move from thecollecting duct to the hypertonic renal medullary interstitium.
Illus
trat
ion
by T
amar
a R
ees
total body water, which also reflects a negative sodiumbalance, provided the pOsm is normal.
Therefore, rather than using the imprecise term dehy-dration, clinicians are better served by thinking aboutbody fluid status in terms of the body’s compartmentsand the overall sodium balance and water balance. Thus,patients with decreased skin turgor and membranemoisture or acute loss of body weight reflecting fluidloss are best described as having ECF volume depletion.Patients with a high pOsm (hypertonicity) and intracel-lular fluid losses are best described as having free waterb
deficits. Some patients may have both. These distinc-tions determine therapeutic decisions: is the patientlacking Na+, water, or both?
Plasma Sodium Ion Concentration Clinicians should become familiar not only with the
published laboratory reference ranges for plasma Na+
concentration but also with the mean and variance intheir own population of patients. The amount of devia-tion in the pOsm that ordinarily alters ADH and thirstin an individual animal is smaller than normal labora-tory ranges (e.g., a 1% to 2% increase in osmolality issufficient to induce thirst).2 In other words, laboratory
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 595CE
Table 2. Clinical Situations That Disrupt the Renal Mediation of Normal Water Balance
Prerequisites for Creation of Dilute Urine
Clinical Situation ThatDisrupts This Portion
of the MechanismPrerequisites for Creationof Concentrated Urine
Clinical Situation ThatDisrupts This Portion of
the Mechanism
A sufficient number ofnephrons to provide theglomerular filtration rate(GFR) necessary for thedelivery of ultrafiltrate to thethick ascending loop of Henle,distal convoluted tubule, andcollecting duct
Decreased functionalrenal mass, as inchronic renal failure
A sufficient number ofnephrons to provide the GFRnecessary for delivery ofultrafiltrate to the thickascending loop of Henle,distal convoluted tubule, andcollecting duct
Decreased functional renalmass, as in chronic renalfailure
Sufficient delivery of sodiumto the diluting segments ofthe nephron (thick ascendingloop of Henle, distalconvoluted tubule)
• Hypovolemia• Very low solute
diets
Sufficient delivery of sodiumto the ascending loop ofHenle and distal convolutedtubule and of urea to thedistal collecting duct forcountercurrent multiplication
Low blood urea nitrogenconcentration such as with an ultralow protein diet orhepatic failure
Optimal active transport ofNa+ out of the ascending loopof Henle coupled withimpermeability to water forgeneration of a maximalhypotonic fluid in the dilutingsegments of the nephron
• Osmotic diuresis• Loop and thiazide
diuretics
Generation and preservationof a maximal renalcorticomedullary gradient
• Osmotic diuresis• Water diuresis• Loop diuretics
Maintenance of waterimpermeability in thecollecting ducts determinedby the absence of ADH (orother antidiuretic substances)
• Syndrome ofinappropriate ADH secretion(SIADH)
• Desmopressintherapy
A collecting duct permeableto water through the action ofADH (or other antidiureticsubstances) and functionalvasopressin (V2) receptors,their second messengers andaquaporins
• Lack of ADH (centraldiabetes insipidus)
• Primary nephrogenic diabetesinsipidus, including heritableabnormalities in V2 receptorsor aquaporins
• Diuretics that interfere withsecond messengers of the V2receptors, such as caffeine
• Hypercalcemia• Obstructive and
postobstructive diuresis
bFree water is used as a contraction of the terms solute-freewater or electrolyte-free water.

reference ranges are often wider than differences thatare important for clinical decision making. For example,a patient may normally have a plasma Na+ concentrationof 145 mEq/L. If water losses are ongoing and theplasma Na+ concentration begins to increase, ADH andthirst will be fully stimulated before the plasma Na+
concentration reaches 150 mEq/L, which may still bewell within the laboratory’s reported reference range.Such a change in plasma Na+ concentration for a patientthat is receiving intravenous fluid therapy and unable todrink would warrant a change in the free water prescrip-tion. By the time the plasma Na+ concentrationincreases beyond the reference range, even by 1 mEq/L,it may be clinically significant and abnormal for thatanimal. Similarly, trends in plasma Na+ concentrationcan be very significant in patients being monitored over
COMPENDIUM October 2007
Question: My patient’s plasma Na+ concentration isonly mildly outside the laboratory’s reference range. Idon’t include such minor abnormalities in serumenzymes on the problem list. Why is this analytedifferent?
Answer: Any abnormalities in plasma Na+ concentrationwarrant clinical attention, even if the Na+ concentrationis only 1 or 2 mEq/L outside the normal referencerange. The body tightly regulates plasma Na+
concentration (as well as the plasma concentration of theother electrolytes), so any deviations in plasma Na+
concentration suggest a water balance disorder.
Question: Can I begin therapy for hyponatremiapending diagnostics?
Answer: Empirical treatment for hyponatremia dependsprimarily on the mechanism. Thus the patient’s volumestatus must be assessed to determine appropriate fluidtherapy.
Question: Why don’t animals with central diabetesinsipidus have hypernatremia?
Answer: ADH is not necessary to maintain a normalpOsm. Even patients with complete central diabetesinsipidus can have a normal pOsm, provided they areable to drink.17 However, it is important to realize thattheir obligate urinary water losses are exceptionally high.Life-threatening hypernatremia can ensue in a matter ofa few hours in these patients, which can lead to theclinical description of “water hunger” (extreme water-seeking behavior, even after short periods of deprivation)in these patients.
Clinical Questions and Answers
598 CE

a prolonged period, such as cats receiving subcutaneousfluids for chronic renal failure. If such a cat were to havea plasma Na+ concentration of 150 to 152 mEq/L con-sistently for several months, followed by an upwardtrend of 153, 155, and 156 mEq/L over the next fewmonths, the increase may be very significant for that cat,despite the value consistently remaining within the lab-oratory’s reported reference range for cats.c
When clinicians are dealing with laboratory values inwhich minor changes can be clinically meaningful, the“noise” of day-to-day measuring variance can cloudinterpretation. This makes it even more important foreach clinician to become familiar with the assay fromhis or her specific laboratory. Generally speaking, anydeviation of plasma Na+ concentration should be noted.When it is unexpected, the first course of action may beverification of repeatability. However, small deviations
in plasma Na+ concentration should not be dismissedand omitted from the problem list because the osmoreg-ulatory system controls the pOsm within such a narrowrange in healthy animals.2
HYPONATREMIADiagnostic Approach
The plasma Na+ concentration does not measure thetotal Na+ content in the ECF and, therefore, does notreflect the volume of ECF or total body fluid. The plasmaNa+ concentration merely reflects the amount of waterrelative to the Na+ content, which is determined by theosmoregulatory system. Thus hyponatremia is a disorderof water balance because the amount of water is increasedrelative to the amount of Na+ in the ECF. The Na+ con-tent of the ECF (and, therefore, the body), and thus thetotal body fluid volume, can be normal, increased, ordecreased in hyponatremia. Further localization ofhyponatremia by mechanism is shown in Figure 8.
Hyponatremia is usually associated with hypoosmo-lality. Exceptions are so-called pseudohyponatremia andtranslocational hyponatremia secondary to exogenous
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 599CE
cAlthough uncommon, cats with chronic renal failure that receivesubcutaneous fluids can receive a sufficient chronic Na+ load suchthat the kidneys cannot excrete it and hypernatremia ensues. Thefact that this often occurs before clinical volume overload mayreflect an inadequate thirst response in this species.
• Volume depletion• Advanced renal failure• Diuretics• SIADH• Decreased solute intake
Hypoosmolar hyponatremia Pseudohyponatremia
1 Defect in renal water excretion
2 Water intake exceeding a normal renal excretory capacity
• Mannitol• Glycine
Translocational hyponatremia
2 Exogenous solutes
1 Hyperglycemia (normal osmolar gap)
1 Hyperlipidemia
2 Hyperproteinemia
Hyponatremia
Figure 8. Low Na+ concentration can be hypoosmolar or hyperosmolar (translocational) or can reflectpseudohyponatremia.

osmoles, in which a large concentration of alternativeosmoles is present (Figure 6).
Pseudohyponatremia results from an in vitro artifactobserved when measuring serum Na+ concentration byflame photometry in the presence of elevated plasmalipids or proteins. In these situations, the measured Na+
concentration is lower than the true Na+ concentration.4
Although newer ion-selective electrodes have largelyeliminated this problem in undiluted samples, the termpersists as a way to distinguish this in vitro phenomenon
from clinically significant hyponatremia.Translocational hyponatremia may be divided into
two categories: (1) conditions in which the measuredand calculated serum osmolalities are the same (hyper-glycemia); and (2) conditions in which there is an osmo-lar gap: some osmoles are clearly present and aremeasured but have not been identified. Unidentifiedosmoles may include mannitol, glycine, and alcoholssuch as ethanol and ethylene glycol.2 Only impermeantsolutes (e.g., glucose in the absence of insulin, mannitol,
glycine) will lead to water translocation from inside tooutside cells and cause hyponatremia (Figure 6).
In diagnosing true hypoosmolar hyponatremia, twoprincipal pathophysiologic mechanisms must be consid-ered.13 The first is impaired renal excretion of free water, orimpaired diluting ability. In this situation, the animal can-not excrete maximally dilute urine (urine osmolality[uOsm] <100 mOsm/L). Several disease states and condi-tions can be associated with impaired renal diluting capac-ity and free water excretion. Most common ishypovolemia, which can reflect either absolute volumedepletion caused by gastrointestinal, transepidermal, orrenal losses or high-volume edematous states associatedwith reduced effective plasma volume. When absolute oreffective plasma volume is decreased, the ensuing reducedrenal perfusion limits the quantity of glomerular filtratereaching the diluting segment of the kidneys. In volumedepletion, Na+ conservation in the proximal nephron isenhanced and less Na+ reaches the thick ascending limb ofthe loop of Henle. ADH may also be released in responseto volume depletion, overriding the effect of the hypo-tonicity and compounding the defect in water excretion.
Impaired diluting ability is also a feature of advancedrenal failure13 in which the ability to excrete water isapproximately 20% of that of a normal, healthy kidney.14
It is a common misconception that renal azotemia isruled out by the finding of hyposthenuria. In early andmoderate renal failure, the kidneys retain some tubularfunction and, therefore, meaningful diluting capacity.2,14
Urinary water excretion is also impaired when ADHremains elevated in the presence of plasma hypoosmo-lality, as in hypovolemia. Figure 9 shows hypovolemic
hyponatremia in a patient with Addison’s disease. Simi-larly, gastrointestinal Na+ losses in a patient that is stilldrinking water will result in hypovolemic hyponatremia.
In contrast to hypovolemia, in which ADH elevationis appropriate (i.e., in response to hypovolemic shock),the syndrome of inappropriate ADH secretion (SIADH)refers to conditions in which the ADH elevation lead-ing to hyponatremia is not a consequence of volumedepletion. The urine Na+ concentration in these patientsis greater than 20 mEq/L, indicating no volume deple-
COMPENDIUM October 2007
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia600 CE
Figure 9. A patient with Addison’s disease typifieshypovolemic hyponatremia. Renal Na+ wasting results in asufficient decrease in ECF to stimulate ADH.Thirst is stimulateddespite a decreasing plasma Na+ concentration, which falls furtheras the ECF volume declines.The hyponatremia is illustrated bythe 2:1 ratio of water molecules to Na+. Water movesintracellularly to maintain an equivalent water concentrationinside and outside cells (red arrows of unequal size).
Illus
trat
ion
by T
amar
a R
ees
The serum sodium concentration does not reflect the total amount of sodium in the extracellular fluid.

tion. SIADH, although well described in humans, israrely reported in dogs or cats.4 In humans, SIADHmay be associated with the following conditions:(1) ectopic production of ADH by certain neoplasms;(2) administration of exogenous ADH or oxytocin;(3) enhanced hypothalamic ADH secretion due to neu-ropsychiatric disorders, drugs, or pulmonary disease; or(4) drug-related potentiation of ADH effects.2
Certain diuretics, such as loop diuretics and thiazides,impair renal water excretion because they decrease Na+
transport in the diluting segment of the nephron.2
Decreased renal diluting ability is also reported withhighly reduced dietary solute intake.15 This is unlikeother causes of decreased free water excretory capacitybecause the uOsm is less than 100 mOsm/L. In humans,this occurs with the practice of beer potomania—a syn-drome in which individuals consume large quantities ofbeer (which is hypoosmolar) but an inadequate amount
of food, leading to insufficient dietary solute andimpaired ability to excrete free water.13,16 This would be ahighly unexpected mechanism in dogs or cats.
The second principal mechanism for the developmentof hypoosmolar hyponatremia is when water intakeexceeds maximal renal excretory capacity. This is a farless common cause of hyponatremia than is impairedrenal water excretion. Normally, renal diluting capacityis adequate to keep pace even with ardent drinkers.Thus most primary polydipsias do not result in overthyponatremia. In humans, hyponatremia may occurwith polydipsia accompanying psychosis.13 Perhaps anal-ogous in dogs is so-called psychogenic polydipsia, in whichnervous or hyperactive dogs respond to the stress ofconfinement or boredom by drinking obsessively.17 Suchdogs usually have hyposthenuria and mild hypona-tremia, although they may remain within a laboratory’spublished range. Often, removing these patients fromtheir routine, such as through overnight hospitalizationwith free access to water, will disrupt the unwantedbehavior and demonstrate the polydipsia as primary byrevealing a concentrated urine specific gravity when theabnormal drinking routine is interrupted.
Because the kidneys are ordinarily highly efficient inexcreting water, patients with primary polydipsia aremore likely to have overt hyponatremia when impairedrenal water excretion is concurrently present.9 Thus it isclinically important to assess patients with primarypolydipsia and hyponatremia for concurrent renal dilut-ing defects such as SIADH or abnormally regulatedADH secretion.18
Clinical ApproachFor the clinician, distinguishing between the physical
causes of hyponatremia relies heavily on a complete his-tory and an analysis of the patient’s other problems. Thefirst question that should come to mind when assessingany patient with hyponatremia is, “Why is there toomuch water?” Evaluation of a blood sample for lipemiaand assessment of the plasma protein concentration canrapidly rule out pseudohyponatremia. Translocational
hyponatremia is easily ruled out by assessment of theserum glucose concentration and the absence of a his-tory of administration of an exogenous solute, such asmannitol. The clinician is then left to distinguish pri-mary polydipsia exceeding renal excretory capacity fromimpaired diluting capacity (impaired water excretion),although the two may exist simultaneously. The historyis often illuminating in cases of true psychogenic poly-dipsia, such as a “high-strung,” bored dog. Other pri-mary polydipsias rarely cause overt hyponatremia in thepresence of normal renal diluting capacity.
The patient should be carefully assessed for ECF vol-ume depletion. Some animals can sustain a loss of 5%body weight from ECF volume depletion withoutdetectable clinical signs.19 Because clinical estimates ofbody fluid deficits can be inaccurate,20 the patient his-tory should be carefully scrutinized for clues to suggestgastrointestinal or urinary fluid loss.
For more difficult cases, key laboratory evaluationsinclude pOsm, uOsm, and urine Na+ concentration. uOsmcan be used to help distinguish impaired water excretionfrom polydipsia. Hyponatremic animals with a uOsmgreater than 100 mOsm/L have impaired water excretion.
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 601CE
Any abnormality in serum sodium concentration warrants clinical attention; this includes minorchanges beyond laboratory reference ranges and changes within the reference range that
deviate from typical values for an individual patient.

A decreased pOsm with a uOsm less than 100 mOsm/Lsuggests primary polydipsia (when polyuria is present) orlow solute intake (in which case, a recognizable increase inurine volume may be notably absent). Decreased soluteintake is rare in the veterinary setting; therefore, a lowuOsm typically suggests primary polydipsia.
A low urinary Na+ concentration (<20 mEq/L inhuman patients) suggests hypovolemia as the cause ofhyponatremia. Veterinary patients with SIADH,diuretic-induced hyponatremia, mineralocorticoid defi-ciency, or renal failure should have a urine Na+ concen-tration greater than 20 mEq/L.11
The clinical signs of hyponatremia arise from theeffects on the central nervous system. Reduction of theplasma Na+ concentration drives water from the ECFinto cells. Clinical signs—lethargy, confusion, nausea,vomiting, seizures, and coma—result from cerebraledema. The development of signs depends on the mag-nitude of hyponatremia and the rate at which it devel-oped; the signs of chronic hyponatremia are generallymore subtle and nonspecific than those of acutehyponatremia.13
Although severe hyponatremia can lead to neurologicsigns, too rapid a rate of correction of this disorder canalso lead to brain disease, termed myelinolysis. Clinicalsigns may include weakness, obtundation, ataxia, paresis,and coma, and death may result. Myelinolysis has beenwell documented in humans, dogs, rats, and rabbits as aresult of rapid correction of chronic (>48 hr duration)hyponatremia.21–23 Some canine patients have survivedthe development of myelinolysis with supportivecare.22–24 The pathogenesis of myelinolysis is complexand incompletely understood, but it appears that thelower the rate of correction of chronic hyponatremia,the lower the risk of myelinolysis. It has, therefore, beenrecommended that chronic hyponatremia should be cor-rected as slowly as possible, with an upper rate limit ofno more than 10 mEq/L during any 24-hour period.21
TreatmentRegardless of the cause of hyponatremia, moderation
in therapy is key. The serum Na+ concentration shouldbe measured frequently and therapy adjusted to ensurethat chronic hyponatremia is not corrected by more than10 mEq/L/day.4 Although there are no rules for howfrequently to monitor (and frequency may decrease asseverely affected patients improve), we recommendusing a central venous catheter to allow monitoring asoften as every 3 to 4 hours initially.
COMPENDIUM October 2007
604 CE

Patients with hypovolemia (negative sodium balance)require restoration of the ECF Na+ content; this willreturn control of ADH secretion and thirst to osmoticfactors, and the kidneys will excrete the excess free wateronce the diluting defect resulting from the hypovolemia iscorrected. Thus patients with hypovolemia can initially betreated safely with isotonic (or very mildly hypertonic forthat patient) fluid replacement. In a hyponatremic patient,a fluid that is truly isotonic would, in fact, be of lowerosmolality than a fluid that is isotonic for a normalpatient. Thus typical balanced electrolyte solutions used inhyponatremic patients are actually mildly hypertonic forthose individuals. Fluids that are hypotonic to the patientshould always be avoided, as should hypertonic saline,unless death from hypovolemic shock is imminent. How-ever, even if isotonic fluids are used, as indicated above,solute-free water will be excreted once hypovolemia is cor-rected, and this alone could lead to rapid correction ofhyponatremia; thus, serial monitoring of serum Na+ con-centration is essential in these patients. It is also importantto remember that hypovolemia is a result of fluid lossesexceeding intake, so a provision must be made in the fluid
therapy prescription to meet these ongoing losses, in addi-tion to restoring deficits, until the underlying disease (e.g.,Addison’s disease, primary gastrointestinal disease) can beresolved with appropriate specific therapy.
Patients with translocational hyponatremia mayhave different fluid needs, depending on the osmoleinvolved. The most common clinical scenario is unregu-lated diabetes mellitus, in which hypovolemia is oftenpresent and needs to be corrected. Subsequent initiationof insulin therapy lowers plasma glucose levels andreturns the excess ECF water to its intracellular location.
Patients with edema or ascites have excess ECF Na+
and an even greater excess of ECF water. Therapy ismore challenging because these patients have adecreased effective plasma volume and renal mecha-nisms for retention of Na+ are stimulated. Correction ofhyponatremia generally requires restriction of waterintake to below the level of urine output. This can bevery difficult because thirst is stimulated. Therapy forthe primary underlying disorder is required; therefore,therapy before diagnostics is generally not indicated.
Patients with hyponatremia secondary to water
intoxication are rare in veterinary medicine; however,these patients may have clinical signs related to hypo-tonicity. Treatment generally consists of water restrictionand careful monitoring.
HYPERNATREMIAHypernatremia is also a disorder of water balance. It
reflects a state of too little water relative to Na+ content inthe ECF. The Na+ content of the body can be normal,increased, or decreased. Similar to hyponatremia, inpatients with hypernatremia, the plasma Na+ concentrationdoes not provide a measurement of an animal’s volume sta-tus. The first question a clinician should ask after detectinghypernatremia is, “Why is there too little water?”
Many cases of hypernatremia develop while patients arehospitalized, and the diagnosis involves analysis of thepatient’s fluid intake and losses. The presence or absenceof hypovolemia helps to distinguish pure water losses fromhypotonic fluid losses. uOsm can help to distinguish thecause of hypernatremia. In patients with extrarenal hypo-tonic losses, such as those with severe diarrhea, the renalsalt-conserving mechanisms should be maximally stimu-
lated to preserve ECF volume. The urine of these patientshas a low Na+ concentration and a low water content dueto high ADH, but the uOsm is high because other solutesare present. Patients with a very low uOsm (<150mmol/L)25 in a setting of hypertonicity and polyuria havediabetes insipidus, which may be central or nephrogenic.2
Diagnostic ApproachImpaired water intake leading to a water deficit, as
shown in Figure 10, is one cause of hypernatremia. Indogs, pOsm increases of as little as 1% stimulate thirst.26
These deviations are normally rapidly corrected bywater ingestion; thus, sustained hypertonicity implies adefect in thirst sensation, restricted access to water, or aphysical inability to drink.
Primary hypodipsia is a condition of diminished orabsent thirst that results in hypernatremia. Thirst is theultimate defense against hypernatremia. If an animaldoes not drink, hypernatremia will develop due to nor-mal insensible water losses. Hypodipsia is usually associ-ated with identifiable hypothalamic disease.2,4,17 If ADHproduction is intact, renal water conservation will miti-
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 605CE
Chronic hyponatremia must be corrected slowly to avoid the development of myelinolysis.

gate the hypernatremia, provided the defect in the thirstmechanism is not severe.
Essential hypernatremia2 is a similar condition inwhich the osmostat in the hypothalamus is reset and agreater degree of hypertonicity is required to trigger thethirst and ADH responses. A number of case reportshave proposed this syndrome in a cat27 and severaldogs28–32; miniature schnauzers appear to be overrepre-sented in some case series.4
Salt toxicity resulting from ingestion of salt or admin-istration of hypertonic fluids is rare in veterinary medi-cine. Nonetheless, it is an issue of too little waterrelative to salt, as opposed to a problem of too muchsalt. These patients typically do not have significantclinical signs related to extracellular volume overloadunless cardiac disease is present, leading to intoleranceof an acutely expanded ECF volume. Hypernatremiaassociated with salt ingestion should be mild and tran-sient, provided water intake is not impaired. In cases ofsalt poisoning, or when hypertonic saline is given with-out free water, neurologic signs consequent to rapiddecreases in brain cell volume include lethargy, irritabil-
ity, weakness, behavior changes, hyperreflexia, disorien-tation, ataxia, seizures, and coma. These signs resultfrom water translocation to the hypertonic ECF and theassociated rupture of cerebral vessels4 and may be suffi-ciently severe and rapid in onset to impair the thirstresponse that would ordinarily protect the animal.
Inadequate free water intake in the presence of excesswater loss (Figures 11 and 12) accounts for most cases ofhypernatremia. In humans, geriatric patients are particu-larly at risk due to decreased thirst.9 The same risk mayapply to geriatric animals and would be increased in thepresence of declining renal concentrating ability. Waterintake is often impaired in very sick, hospitalized patientsdue to debility, sedation, or other problems that impairthe ability to drink. Long-term use of intravenous or sub-cutaneous fluids that are isotonic and do not provide suf-ficient free water will also lead to hypernatremia inpatients that do not drink. This is particularly true if renalwater-conserving mechanisms are impaired.
TherapyFor all patients, ECF volume deficits must be replaced.
COMPENDIUM October 2007
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia606 CE
Figure 10. When water is available, thirst is the primarydefense against hypernatremia. When water is not available,obligate respiratory and urinary losses are not offset.The ECFNa+ concentration increases (hypernatremia), illustrated by the2:1 ratio of Na+ to water molecules. ADH is stimulated, and thekidneys retain water (blue arrow), producing a small volume ofconcentrated urine. Net water movement is from intracellular toextracellular space until the water concentration is againequivalent (red arrows of unequal size). In this situation, the patienthas a decreased intracellular fluid volume (shown as shrunken cell and brain), and ECF Na+ content is unchanged.
Illus
trat
ion
by T
amar
a R
ees
1 ADH deficiency or lack of efficacy
2 Panting
Figure 11. Excess water loss, such as from (1) urinary or(2) respiratory losses, predisposes a patient withinadequate water intake to hypernatremia. Excessiveurinary water loss may result from central or nephrogenicdiabetes insipidus and can lead to hypernatremia if the patient isunable to drink enough water to compensate for this loss. In thissituation, the ECF Na+ concentration increases (illustrated by the2:1 ratio of Na+ to water molecules) and net water movement isfrom the intracellular to extracellular space (red arrows of unequalsize).The patient has a decreased intracellular fluid volume (shownas shrunken cell and brain), and ECF Na+ content is unchanged.
Illus
trat
ion
by T
amar
a R
ees

The fluid therapy plan for hypernatremic patients mustinclude a provision for maintenance and replacement ofongoing losses in addition to restoration of the free waterdeficit. Patients with mild hypernatremia that have beenrestricted from water and are normal neurologically willcorrect their own deficits when water is provided, andthey do not require fluid therapy support. Therapeuticcorrection of more severe hypernatremia when the patientis sick requires replacement of the calculated water deficitwith fluid therapy. Data from the patient history aboutthe time course over which the hypernatremia likelydeveloped are particularly important.
The volume of the deficit can be estimated using thefollowing equation33,d:
Free water deficit = 0.6 × body weight (kg) ×[(plasma Na+ ÷ 148) – 1]
Water can be replaced either enterally (orally or bygastric tube) or intravenously with hypotonic saline or
5% dextrose in water.Hypernatremia that is known to have developed
acutely (over no more than 24 to 36 hr34) can be correctedrelatively rapidly. This may be observed in patients withacute water deprivation, especially in hot environmentswhere respiratory water losses for thermoregulation arevery high. Therapy requires rapid correction of both thefree water and the ECF Na+ content deficits. This acutetime course is also likely in rare cases when hyperna-tremia results from solute administration (e.g., hypertonicfluid administration). These patients require both wateradministration and solute removal (with loop diuretics).
In contrast, patients with more chronic hypernatremiaadapt by increasing intracellular solutes in the brain toprotect against the adverse effects of intracellular dehy-dration. The initial response of the brain to hyperna-tremia is to accumulate intracellular electrolytes, but thiscan impair brain function. So, with time, the brain accu-mulates organic solutes (idiogenic osmoles) such asamino acids, trimethylamines, and myoinositol.4,5,35
Although these adaptations diminish the effects of theECF hypertonicity, they put the patient at risk for cere-
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 607CE
• Fever• Hyperventilation• Panting• Central or nephrogenic diabetes insipidus
Pure Water Losses
• Gastrointestinal fluid loss• Diuretic therapy• Osmotic diuresis• Movement of fluid to the third space• Burns
Hypotonic Fluid Losses
Free Water Losses
Fluid is lost from both the intracellular and extracellular compartments. Signs of ECF volume depletion are rarely present.
ECF loss exceeds intracellular fluid loss. Signs of ECF volume depletion are often present.
Figure 12. Increased free water losses may result from pure water loss or hypotonic fluid loss.
dThe value of 148 in this formula is modified from the stan-dard 140 mEq/L used in humans to better estimate a desiredtarget plasma Na+ concentration for dogs and cats.

bral edema if the hypernatremia is corrected too quickly.When these brain adaptations have taken place, hyper-natremia must be corrected more slowly. No ideal, uni-versally safe rate of correction has been established fordogs and cats in which neurologic signs of hyperna-tremia are present; however, based on recommendationsin human medicine, a rate of no more than 0.5 to 1mEq/L/hr can serve as a guideline until the signsresolve. In human medicine, a rate of correction of nomore than 0.5 mEq/L/hr has been recommended.9
Once neurologic signs have resolved, the rate can beadjusted to provide the remainder of the correction overthe next 48 hours. Deterioration of the neurologic statuswith correction of hypernatremia suggests cerebraledema and too rapid a rate of correction. When thetime course over which hypernatremia developed isunknown, clinicians should err on the side of slow,steady correction.
REFERENCES1. Oh GS, Carroll HJ: Regulation of intracellular and extracellular volume, in
Arieff AI, DeFronzo RA (eds): Fluid, Electrolyte, and Acid-Base Disorders.New York, Churchill Livingstone, 1995, pp 1–22.
2. Rose BD, Post TW: Clinical Physiology of Acid-Base and Electrolyte Disorders.New York, McGraw-Hill, 2001.
3. Wellman ML, DiBartola SP, Kohn CW: Applied physiology of body fluidsin dogs and cats, in DiBartola SP (ed): Fluid, Electrolyte, and Acid-Base Disor-ders in Small Animal Practice. St. Louis, Saunders, 2006, pp 3–26.
4. DiBartola SP: Disorders of sodium and water: Hypernatremia and hypona-tremia, in DiBartola SP (ed): Fluid, Electrolyte, and Acid-Base Disorders inSmall Animal Practice. St. Louis, Saunders, 2006, pp 47–79.
5. Morrison G, Singer I: Hyperosmolar states, in Narins RG (ed): Maxwell andKleeman’s Clinical Disorders of Fluid and Electrolyte Metabolism. New York,McGraw-Hill, 1994, pp 617–658.
6. Kirchner KA, Stein JH: Sodium metabolism, in Narins RG (ed): Maxwelland Kleeman’s Clinical Disorders of Fluid and Electrolyte Metabolism. New York,McGraw-Hill, 1994, pp 45–80.
7. Briggs JP, Singh I, Sawaya BE, Schnermann J: Disorders of salt balance, inKokko JP, Tannen RL (eds): Fluids and Electrolytes. Philadelphia, WB Saun-ders, 1996, pp 3–62.
8. Cohen M, Post GS: Water transport in the kidney and nephrogenic diabetesinsipidus. J Vet Intern Med 16(5):510–517, 2002.
9. Sterns RH, Spital A, Clark AC: Disorders of water balance, in Kokko JP,Tannen RL (eds): Fluids and Electrolytes. Philadelphia, WB Saunders, 1996,pp 63–109.
10. Zerbe RL, Robertson GL: Osmotic and nonosmotic regulation of thirst andvasopressin secretion, in Narins RG (ed): Maxwell and Kleeman’s Clinical Dis-orders of Fluid and Electrolyte Metabolism. New York, McGraw-Hill, 1994, pp81–100.
11. Blumenfeld JD, Vaughan ED: Renal physiology and pathophysiology, inWalsh PC, Retik AB, Vaughan ED, Wein AJ (eds): Campbell ’s Urology.Philadelphia, WB Saunders, 2002, pp 169–227.
12. DiBartola SP, Bateman S: Introduction to fluid therapy, in DiBartola S (ed):Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice. St. Louis,Saunders, 2006, pp 325–344.
13. Sterns RH, Ocdol H, Schrier RW, Narins RG: Hyponatremia: Pathophysiol-ogy, diagnosis, and therapy, in Narins RG (ed): Maxwell and Kleeman’s Clini-cal Disorders of Fluid and Electrolyte Metabolism. New York, McGraw-Hill,1994, pp 583–615.
14. Black RM: Diagnosis and management of hyponatremia. J Intensive CareMed 4:205–220, 1989.
15. Thaler SM, Teitelbaum I, Berl T: “Beer potomania” in non-beer drinkers:Effect of low dietary solute intake. Am J Kidney Dis 31(6):1028–1031, 1998.
16. Fenves AZ, Thomas S, Knochel JP: Beer potomania: Two cases and review ofthe literature. Clin Nephrol 45(1):61–64, 1996.
17. Feldman EC, Nelson RW: Canine and Feline Endocrinology and Reproduction.St. Louis, Saunders, 2004.
18. van Vonderen IK, Kooistra HS, Elpetra PM, Rijnberk A: Disturbed vaso-pressin release in 4 dogs with so-called primary polydipsia. J Vet Intern Med13(5):419–425, 1999.
19. Hardy RM, Osborne CA: Water deprivation test in the dog: Maximal nor-mal values. JAVMA 174(5):479–483, 1979.
20. Hansen B, DeFrancesco T: Relationship between hydration estimate andbody weight change after fluid therapy in critically ill dogs and cats. J VetEmerg Crit Care 12(4):235–243, 2002.
21. Laureno R, Karp BI: Myelinolysis after correction of hyponatremia. Ann IntMed 126(1):57–62, 1997.
22. Churcher RK, Watson ADJ, Eaton A: Suspected myelinolysis followingrapid correction of hyponatremia in a dog. JAAHA 35:493–497, 1999.
23. O’Brien DP, Kroll RA, Johnson GC, et al: Myelinolysis after correction ofhyponatremia in two dogs. J Vet Intern Med 8(1):40–48, 1994.
24. O’Brien DP: CNS effects of sodium imbalances. Proc 24th ACVIMForum:323–324, 2006.
25. Halperin ML, Goldstein MB: Fluid, Electrolyte, and Acid-Base Physiology: AProblem-Based Approach. Philadelphia, WB Saunders, 1999.
26. O’Connor WJ, Potts DJ: Kidneys and drinking in dogs, in Michell AR (ed):Renal Disease in Dogs and Cats: Comparative and Clinical Aspects. Oxford,Blackwell Scientific Publications, 1988, pp 30–47.
27. Dow SW, Fettman MJ, LeCouteur RA, Allen TA: Hypodipsic hyperna-tremia and associated myopathy in a hydrocephalic cat with transient hypopi-tuitarism. JAVMA 191(2):217–221, 1987.
28. Crawford MA, Kittleson MD, Fingk GD: Hypernatremia and adipsia in adog. JAVMA 184(7):818–821, 1984.
29. Hawks D, Giger U, Miselis R, Bovee KC: Essential hypernatremia in a youngdog. J Small Anim Pract 32:420–424, 1991.
30. Bagley RS, de Lahunta A, Randolph JF, Center SA: Hypernatremia, adipsia,and diabetes insipidus in a dog with hypothalamic dysplasia. JAAHA29:267–271, 1993.
31. DiBartola SP, Johnson SE, Johnson GC, Robertson GL: Hypodipsic hyper-natremia in a dog with defective osmoregulation of antidiuretic hormone.JAVMA 204(6):922–925, 1994.
32. Sullivan SA, Harmon BG, Purinton PT, et al: Lobar holoprosencephaly in aminiature schnauzer with hypodipsic hyponatremia. JAVMA 223(12):1783–1787, 2003.
33. Fried LF, Palevsky PM: Hyponatremia and hypernatremia. Med Clin NorthAm 81(3):585–609, 1997.
34. Sterns RH, Heilig CW, Narins RG: Water and sodium metabolism:Hyponatremia and hypernatremia, in Massry SG, Glassock RJ (eds): Massryand Glassock’s Textbook of Nephrology. Baltimore, Williams & Wilkins, 1995,pp 276–292.
35. Lien Y-HH, Shapiro JI, Chan L: Effects of hypernatremia on organic brainosmoles. J Clin Invest 85:1427–1435, 1990.
COMPENDIUM October 2007
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia608 CE

1. Effective osmoles a. move freely across cellular membranes and thus do
not induce net water movement across cell mem-branes.
b. affect a solution’s tonicity.c. include urea and ethanol.d. are subtracted from ineffective osmoles to determine
the osmolar gap.
2. A patient with increased plasma Na+ content has a. hypervolemic hypernatremia.b. hypovolemic hypernatremia.c. hypovolemia.d. hypervolemia.
3. A patient with hypernatremia hasa. a salt balance disorder.b. a water balance disorder.c. too high a plasma Na+ content.d. expanded intracellular volume.
4. Patients with congestive heart failure, edema,and hyponatremia have a. impaired renal diluting capacity due to hypovolemia.b. impaired renal diluting capacity due to decreased
effective plasma volume.c. renal salt wasting.d. primary polydipsia.
5. Which of the following values indicates only pri-mary polydipsia?a. uOsm = 50 mOsm/L c. pOsm = 330 mOsm/Lb. uOsm = 310 mOsm/L d. pOsm = 360 mOsm/L
6. A 5% dextrose solution given intravenously to anondiabetic patient with a normal plasma Na+
concentration is a. hypoosmolar but hypertonic.b. hypertonic and hyperosmolar.
c. used for provision of free water.
d. used to expand the ECF volume.
7. A patient presenting with hypernatremia within2 hours of ingesting a rock salt driveway deicershould have its hypernatremia correcteda. as rapidly as possible by provision of intravenous
and/or enteral free water.
b. over 24 to 48 hours by provision of enteral freewater.
c. over 24 to 48 hours by provision of intravenous freewater.
d. as rapidly as possible for the first 35% of the calcu-lated free water deficit and then over 24 to 48 hours.
8. The osmolality of the ultrafiltrate as it enters therenal proximal tubule is a. the same as that of plasma.
b. much higher than that of plasma.
c. much lower than that of plasma.
d. unpredictable.
9. Which of the following does not impair renaldiluting ability?a. thiazide diuretics
b. central diabetes insipidus
c. markedly reduced dietary solute intake
d. Addison’s disease
10. Myelinolysis a. is caused by translocational hyponatremia.
b. is the delayed effect of incomplete correction ofchronic hypernatremia.
c. can result from rapid correction of chronic hypona-tremia.
d. is rare, provided glucocorticoids are given before anycorrection of the plasma Na+ concentration.
October 2007 COMPENDIUM
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia 609CE
ARTICLE #1 CE TESTThis article qualifies for 2 contact hours of continuing education credit from the Auburn University College of Veterinary Medicine. Subscribers may purchase individual CE tests or sign up for our annual CE program. Those who wish to apply this credit to fulfill state relicensure requirements should consult their respective state authorities regarding theapplicability of this program. CE subscribers can take CE tests online and get real-time scores at CompendiumVet.com.
CE


















