Quoi de neuf dans la stratégie une syncope ? · Syncope : pronostic et conséquences ......
45
Quoi de neuf dans la stratégie diagnostique d’une syncope ? Patrick Friocourt Pôle Autonomie CH Blois Actualités en médecine gériatrique 2017
Transcript of Quoi de neuf dans la stratégie une syncope ? · Syncope : pronostic et conséquences ......
Quoi de neuf dans la stratégie diagnostique d’une syncope ?
Patrick FriocourtPôle Autonomie
CH Blois
Actualités en médecine gériatrique 2017
Que dit la littérature récente ?• Syncope dans le titre au cours des 5 dernières années (Pubmed)
– 1178 articles– Sujet âgé : 17 articles
• Recommandations syncopes– 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients
with Syncope : ACC/AHA Heart Rhythm. 2017 Mar 9. pii: S1547-5271(17)30297-7.
– Pacing as a Treatment for Reflex-Mediated (Vasovagal, Situational, or Carotid Sinus Hypersensitivity) Syncope: A Systematic Review for the 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients with Syncope : Heart Rhythm. 2017 Mar 9. pii: S1547-5271(17)30299-0.
– Guidelines for the diagnosis and management of syncope (version 2009). ESC Eur Heart J. 2009 Nov;30(21):2631-71.
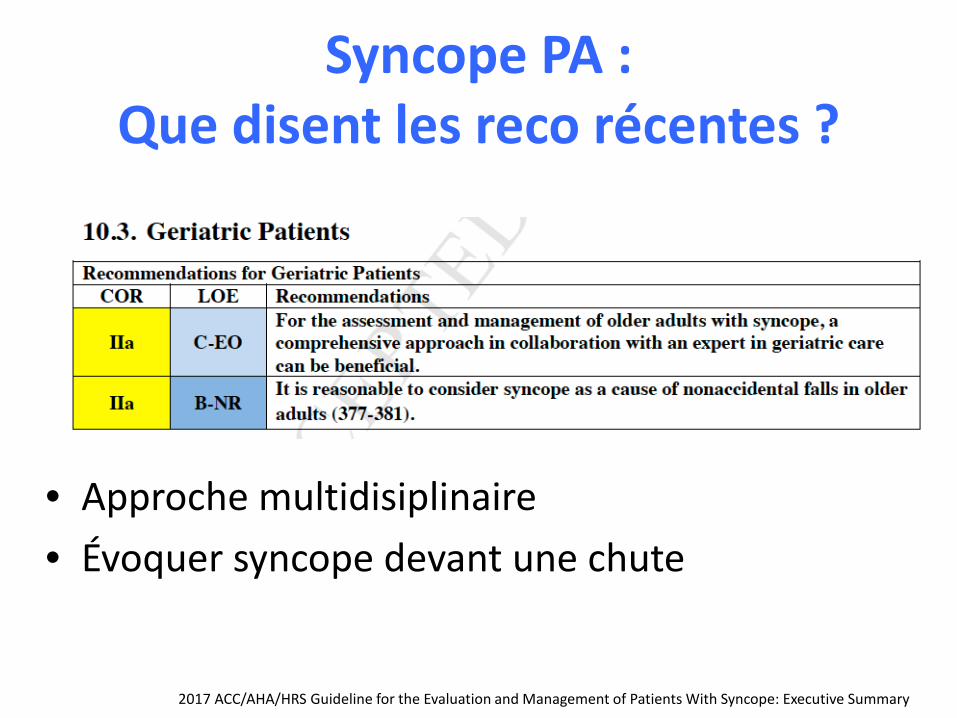
Syncope PA : Que disent les reco récentes ?
• Approche multidisiplinaire• Évoquer syncope devant une chute
2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: Executive Summary
Syncope : pronostic et conséquences
• Décès et complications mettant en jeu PC vital– En cas de cardiopathies structurales et troubles
électriques– HypoTA ortho risque de décès (fct
comorbidités)
• Récidives et risques de lésions accidentelles• Impact sur la qualité de vie• Coûts
European Heart Journal (2009) 30, 2631–2671
Syncope : définition
• La syncope est un symptôme défini par une perte de connaissance, à début rapide, de durée généralement brève, spontanément résolutive, s’accompagnant d’une perte du tonus postural, avec un retour rapide à un état de conscience normal. Elle est due à une hypoperfusion cérébrale globale et passagère.
HAS 2008
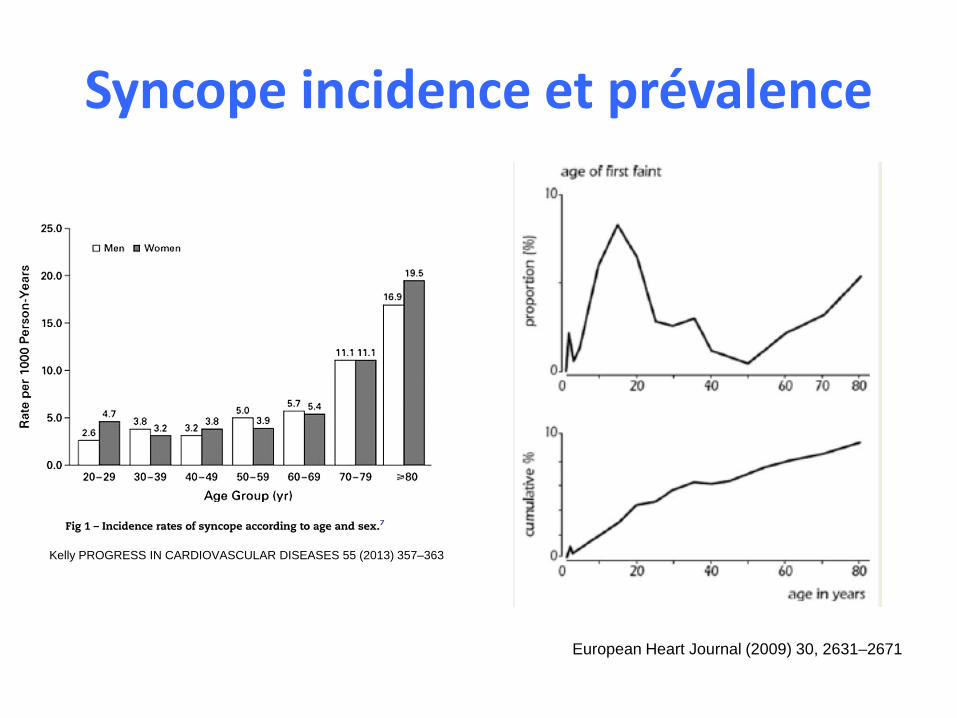
Syncope incidence et prévalence
Kelly PROGRESS IN CARDIOVASCULAR DISEASES 55 (2013) 357–363
European Heart Journal (2009) 30, 2631–2671
Une épidémiologie « floue »
• Définition• Chevauchement : syncope, malaise, chute…• Risque cumulé
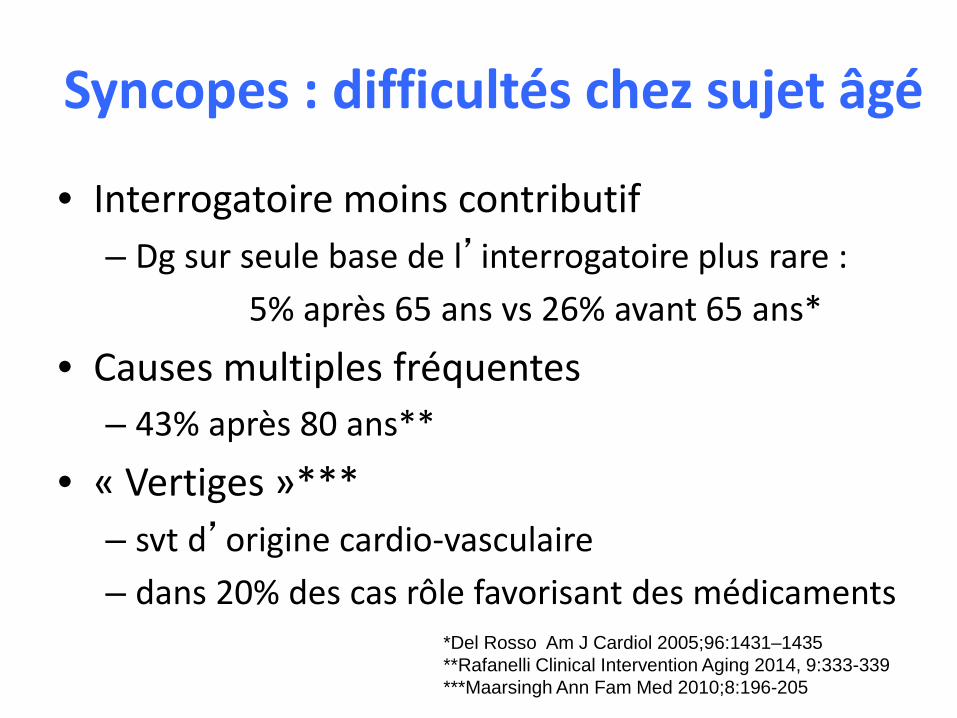
Syncopes : difficultés chez sujet âgé
• Interrogatoire moins contributif– Dg sur seule base de l’interrogatoire plus rare :
5% après 65 ans vs 26% avant 65 ans*
• Causes multiples fréquentes – 43% après 80 ans**
• « Vertiges »*** – svt d’origine cardio-vasculaire – dans 20% des cas rôle favorisant des médicaments
*Del Rosso Am J Cardiol 2005;96:1431–1435**Rafanelli Clinical Intervention Aging 2014, 9:333-339***Maarsingh Ann Fam Med 2010;8:196-205
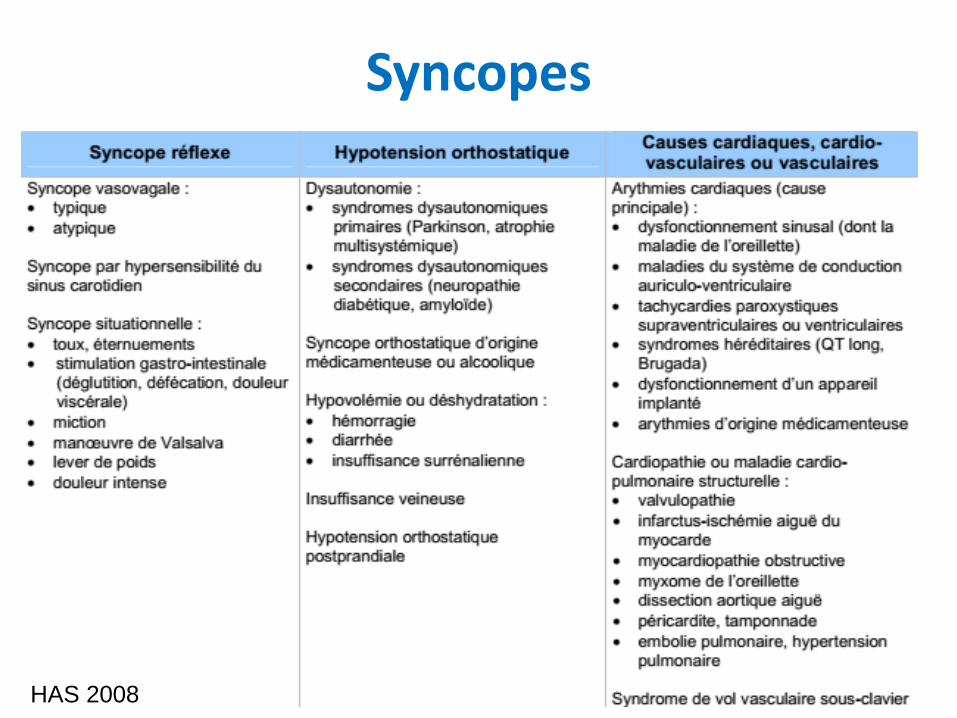
Syncopes
HAS 2008
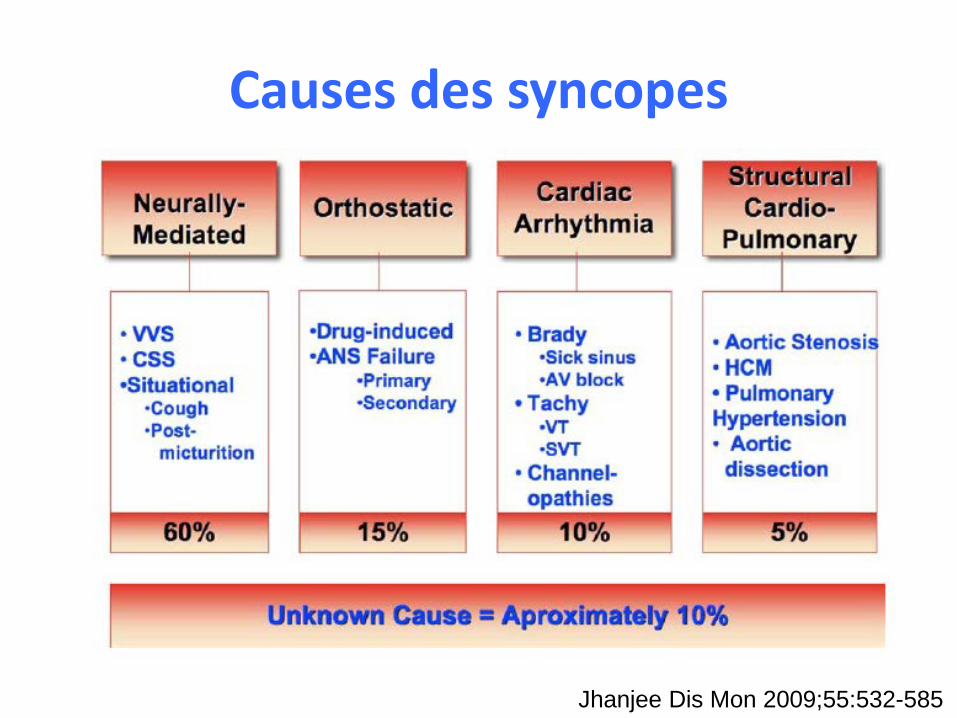
Causes des syncopes
Jhanjee Dis Mon 2009;55:532-585
Définitions : syncopes réflexes• Syncope vasovagale (VVS)
Forme la plus fréquente des syncopes réflexe. Peut se produire en position verticale (debout, ou assis) ou lors d’un stress émotionnel, d’un douleur, ou dans des situationsSe caractérise généralement par des sueurs, sensation de chaleur, nausées et pâleur. Associé à une hypotension et / ou à une bradycardie inappropriée. Souvent suivie d'une fatigue. Les caractéristiques typiques peuvent être absentes chez les patients plus âgés. Souvent précédé de déclencheurs identifiables et / ou d'un prodrome caractéristique. Le diagnostic se fait principalement sur la base d'un interrogatoire fouillé, d'un examen physique et de l’observation des témoins oculaires.
• Syndrome du sinus carotidien– Syncope réflexe associée à une hypersensibilité du sinus carotidien. – Une hypersensibilité est présente lorsque la stimulation du sinus carotidien provoque une pause ≥3 s
et / ou une baisse de la PAS ≥50 mmHg. – Observée plus fréquemment chez les sujets âgés. – L'hypersensibilité du sinus carotidien peut être associée à des degrés variables de symptômes. – Le syndrome du sinus carotidien est défini lorsque la syncope se produit en présence d’une
hypersensibilité du sinus carotidien.
• Syncope situationnelle – Syncope réflexe associée à une action spécifique, comme la toux, le rire, la déglutition, la miction ou
la défécation. AHA 2017
Définitions : HypoTA orthostatique• Hypotension orthostatique : chute de PAS ≥20 mm Hg ou le la PAD ≥10
mm Hg au passage à l’orthostatisme– Hypotension orthostatique « initiale » (immédiate)
• Baisse transitoire de la PA dans les 15 secondes suivant l’orthostatisme, avec présyncope ou syncope
– Hypotension orthostatique classique• Baisse de la PAS ≥ 20 mm Hg ou de la PA diastolique de ≥ 10 mm Hg dans les 3 min
suivant l’orthostatisme. – Hypotension orthostatique retardée
• Baisse soutenue de la PAS ≥ 20 mm Hg (ou de 30 mm Hg chez les patients ayant une HTA d’orthostatisme) ou de la PAD ≥ 10 mm Hg s’installant en > 3 min d’orthostatisme, la baisse de PA étant généralement progressive jusqu'à atteindre le seuil
– Hypotension orthostatique neurogène• sous-type d’hypotension orthostatique due à un dysfonctionnement du système
nerveux autonome et non uniquement secondaire à des facteurs environnementaux (par exemple déshydratation ou médicaments). Cette hypotension neurogène due à des lésions impliquant les nerfs autonomes centraux ou périphériques.
AHA 2017
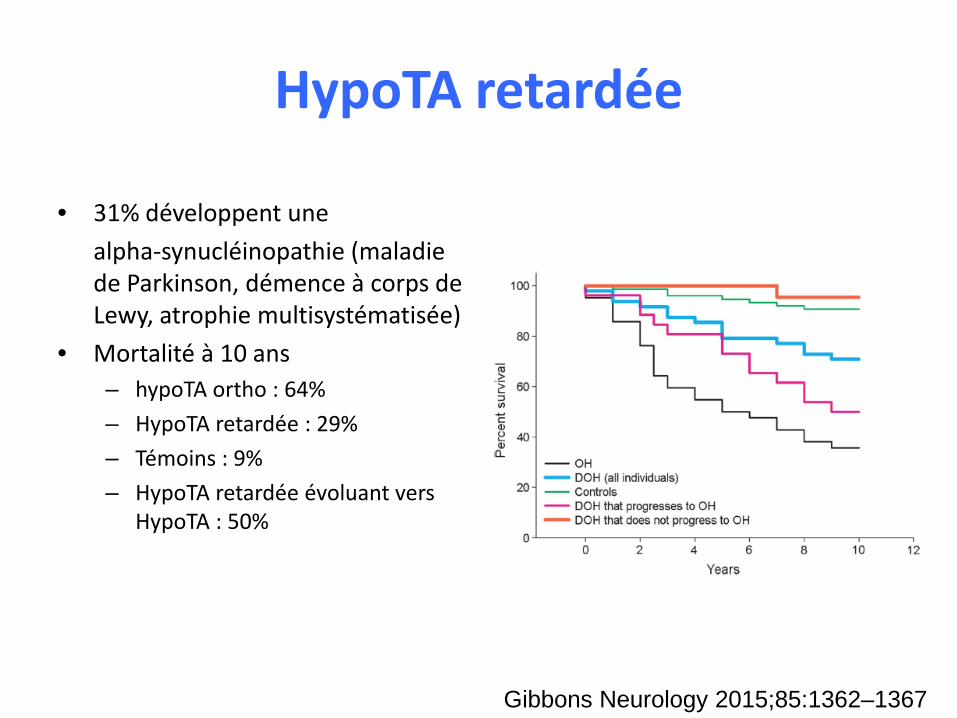
HypoTA retardée
• 31% développent une alpha-synucléinopathie (maladie de Parkinson, démence à corps de Lewy, atrophie multisystématisée)
• Mortalité à 10 ans – hypoTA ortho : 64%– HypoTA retardée : 29%– Témoins : 9%– HypoTA retardée évoluant vers
HypoTA : 50%
Gibbons Neurology 2015;85:1362–1367
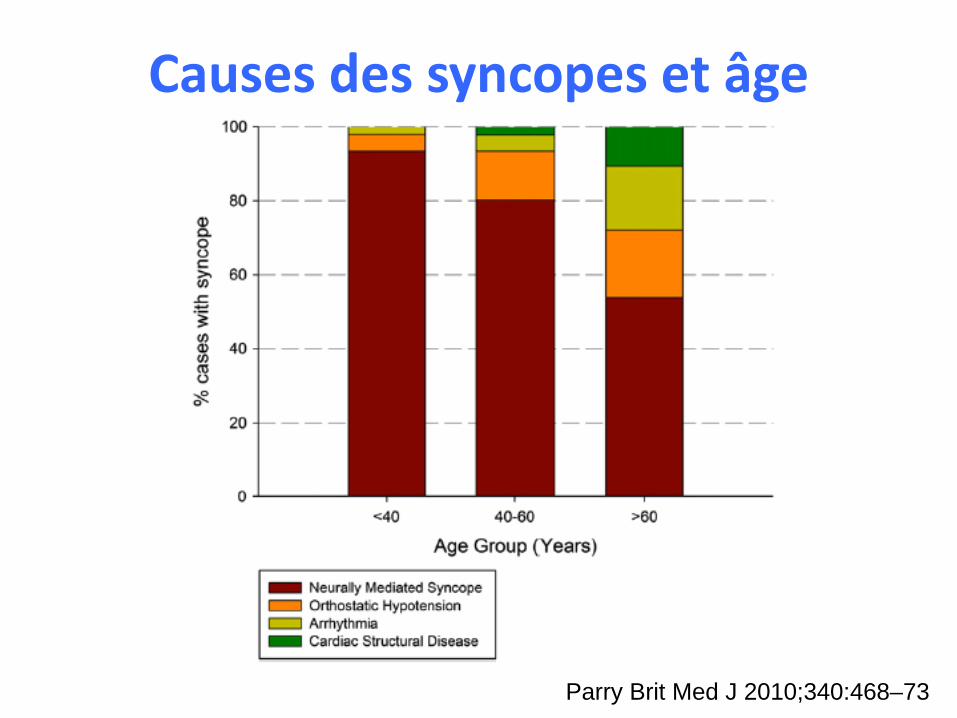
Causes des syncopes et âge
Parry Brit Med J 2010;340:468–73
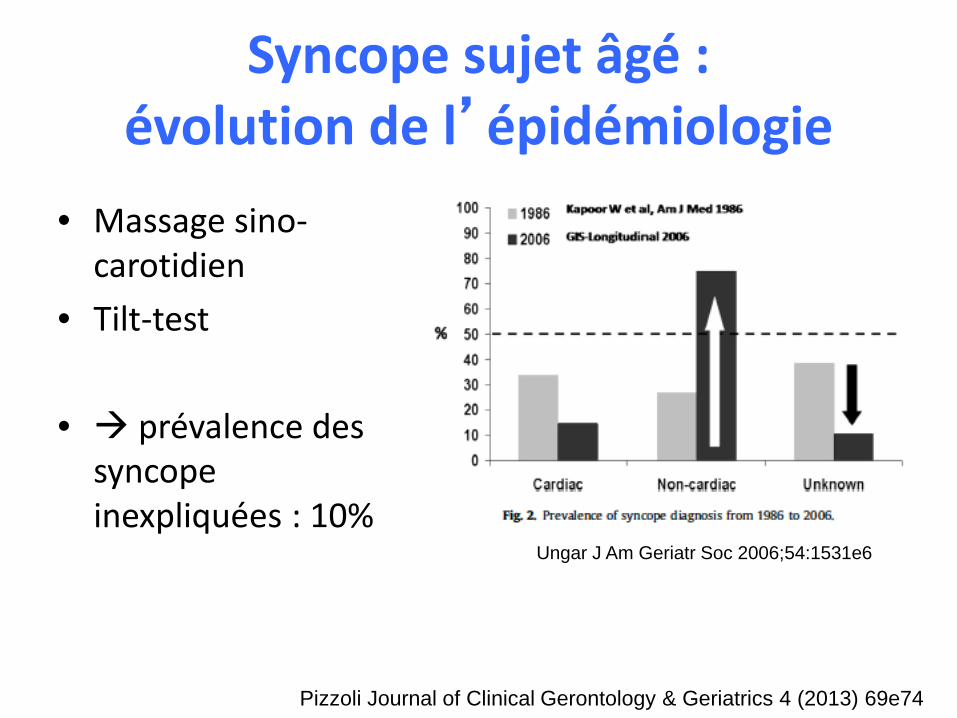
Syncope sujet âgé : évolution de l’épidémiologie
• Massage sino-carotidien
• Tilt-test
• prévalence des syncope inexpliquées : 10%
Ungar J Am Geriatr Soc 2006;54:1531e6
Pizzoli Journal of Clinical Gerontology & Geriatrics 4 (2013) 69e74
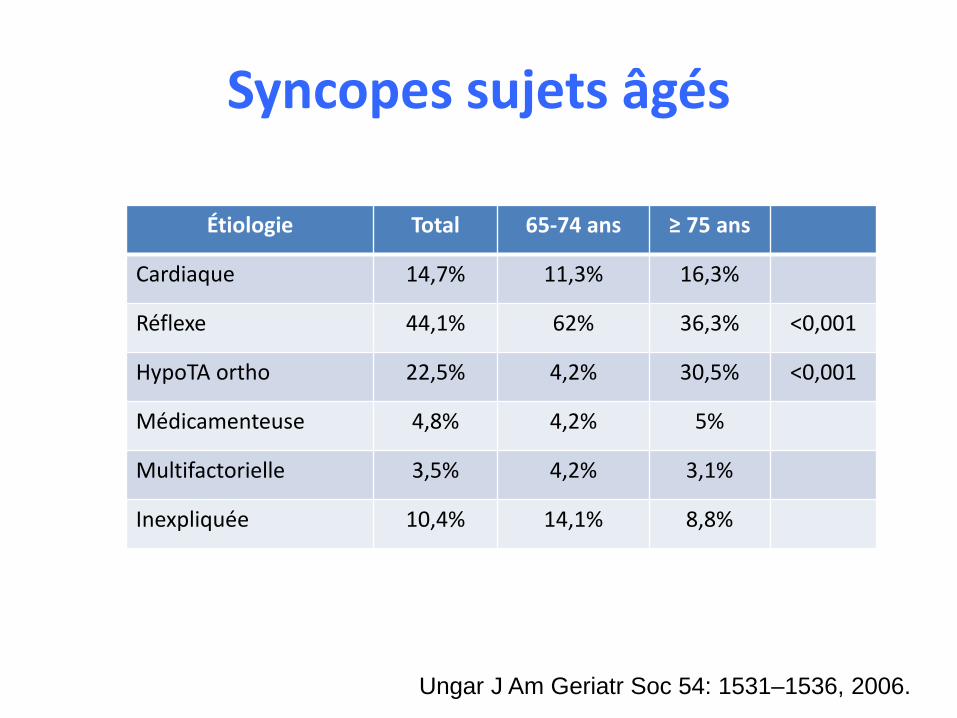
Syncopes sujets âgés
Ungar J Am Geriatr Soc 54: 1531–1536, 2006.
Étiologie Total 65-74 ans ≥ 75 ans
Cardiaque 14,7% 11,3% 16,3%
Réflexe 44,1% 62% 36,3% <0,001
HypoTA ortho 22,5% 4,2% 30,5% <0,001
Médicamenteuse 4,8% 4,2% 5%
Multifactorielle 3,5% 4,2% 3,1%
Inexpliquée 10,4% 14,1% 8,8%
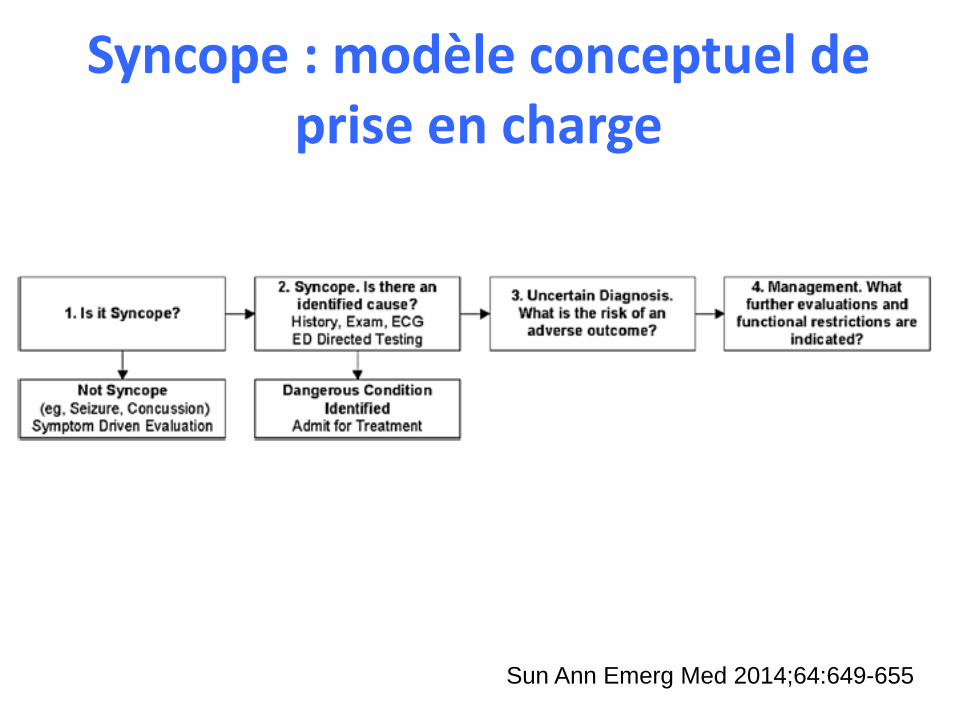
Syncope : modèle conceptuel de prise en charge
Sun Ann Emerg Med 2014;64:649-655
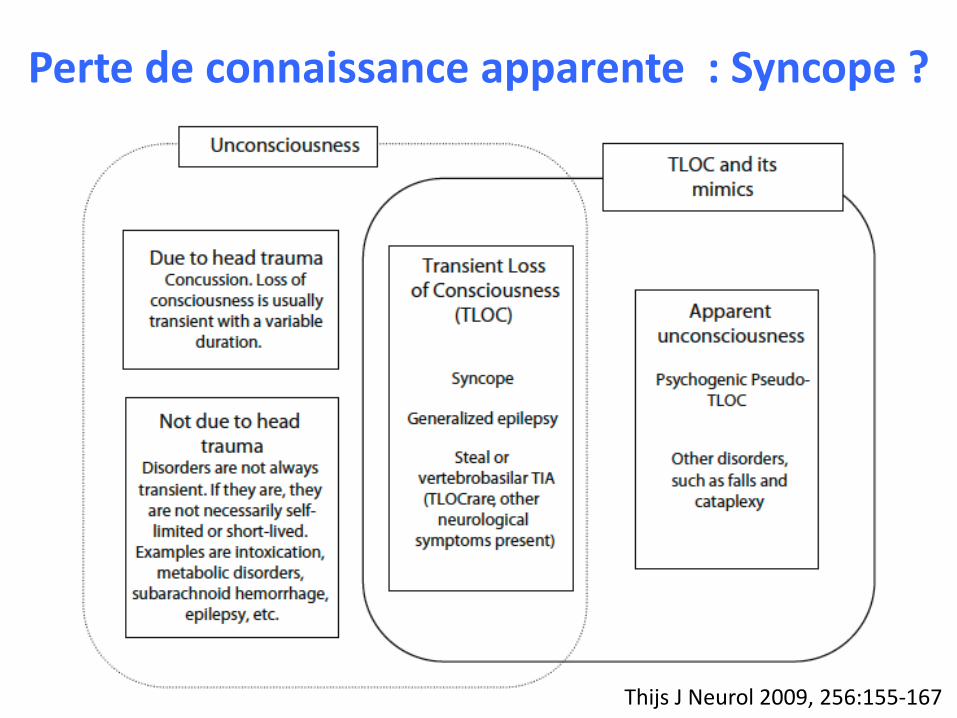
Perte de connaissance apparente : Syncope ?
Thijs J Neurol 2009, 256:155-167
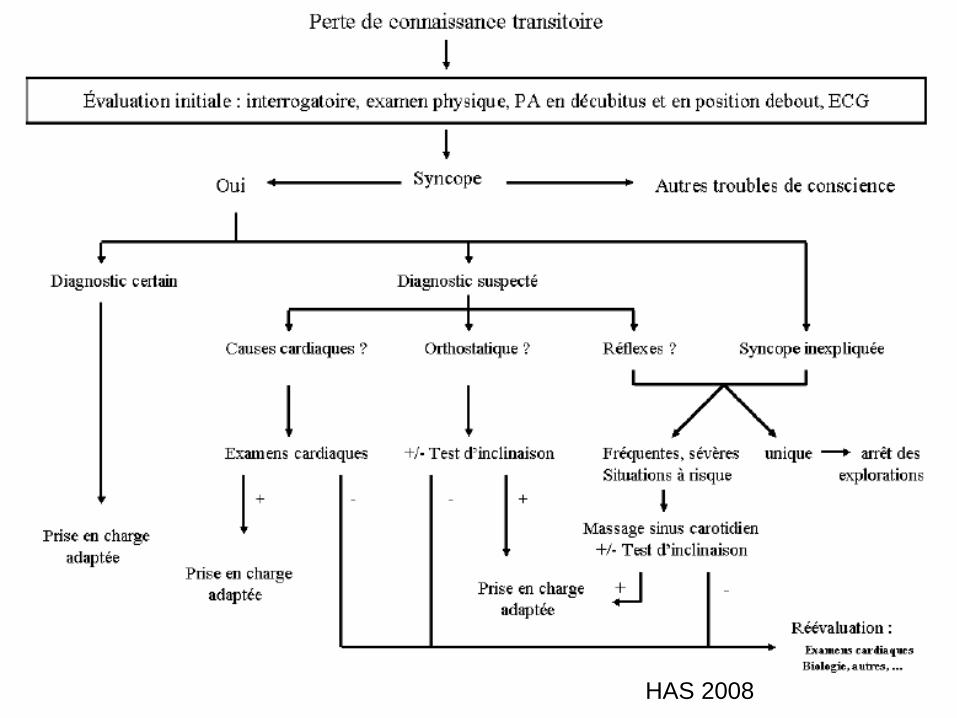
HAS 2008
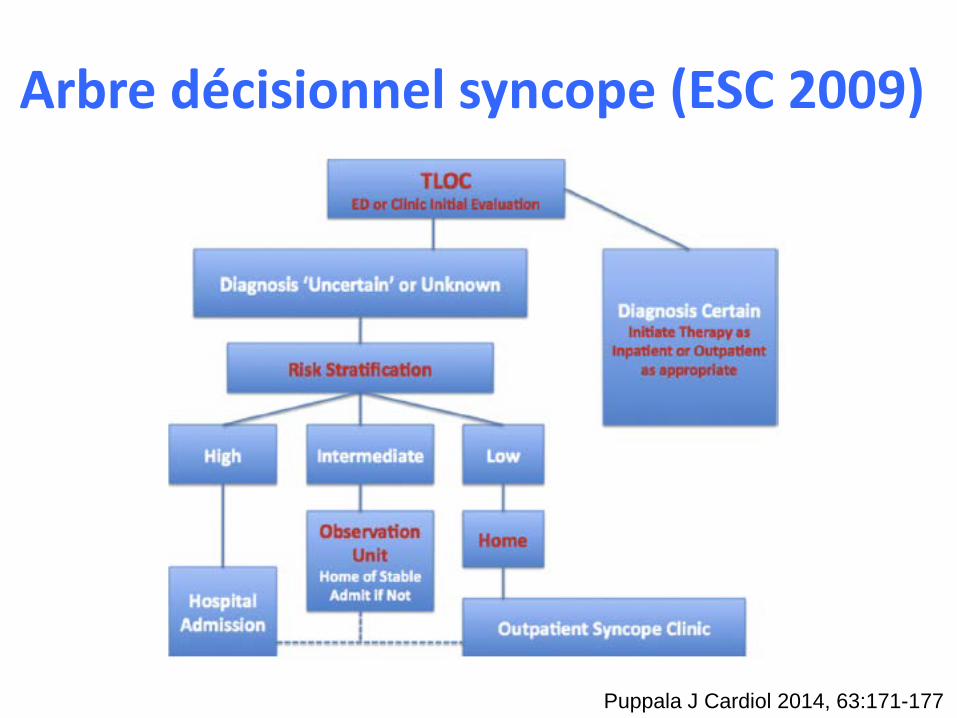
Arbre décisionnel syncope (ESC 2009)
Puppala J Cardiol 2014, 63:171-177
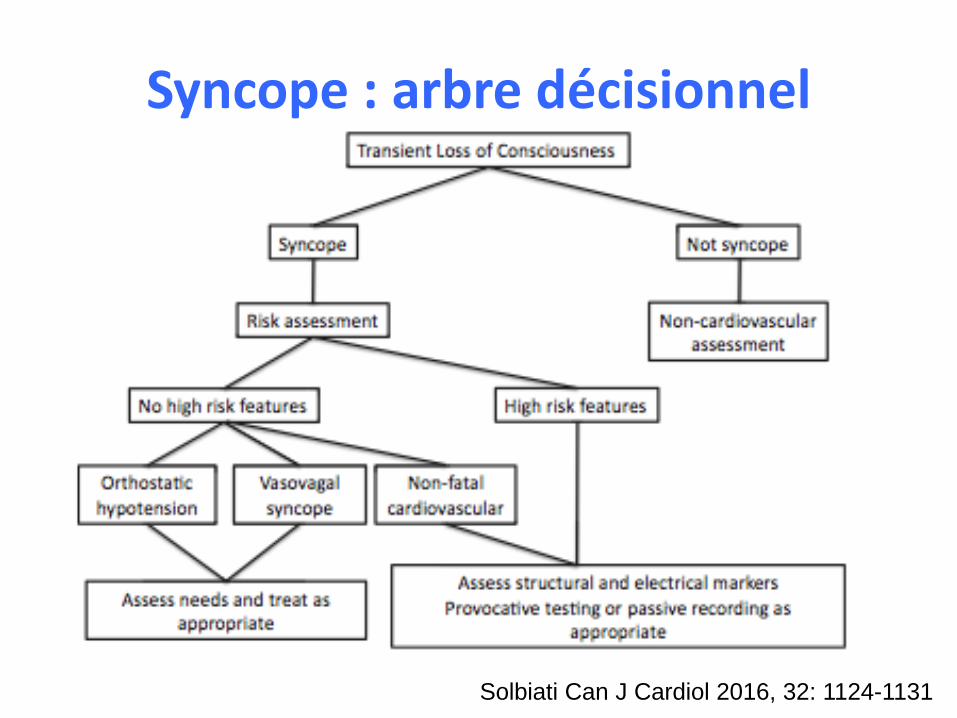
Syncope : arbre décisionnel
Solbiati Can J Cardiol 2016, 32: 1124-1131
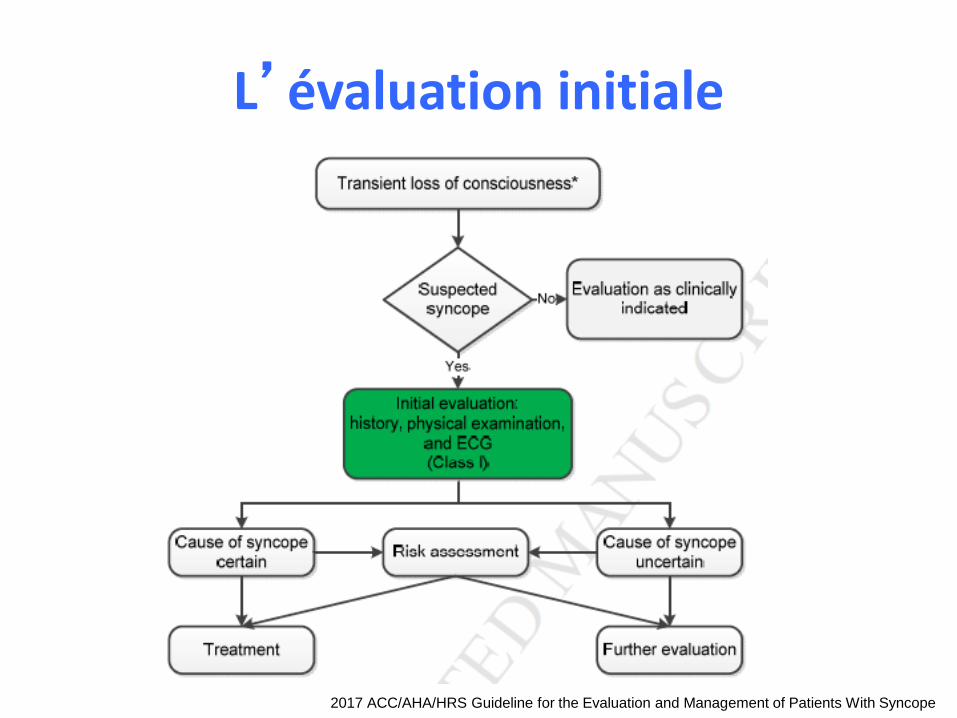
L’évaluation initiale
2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope

Les outils de l’évaluationdiagnostique/pronostique
• Clinique– Interrogatoire– Examen clinique
• Examens complémentaires• Scores
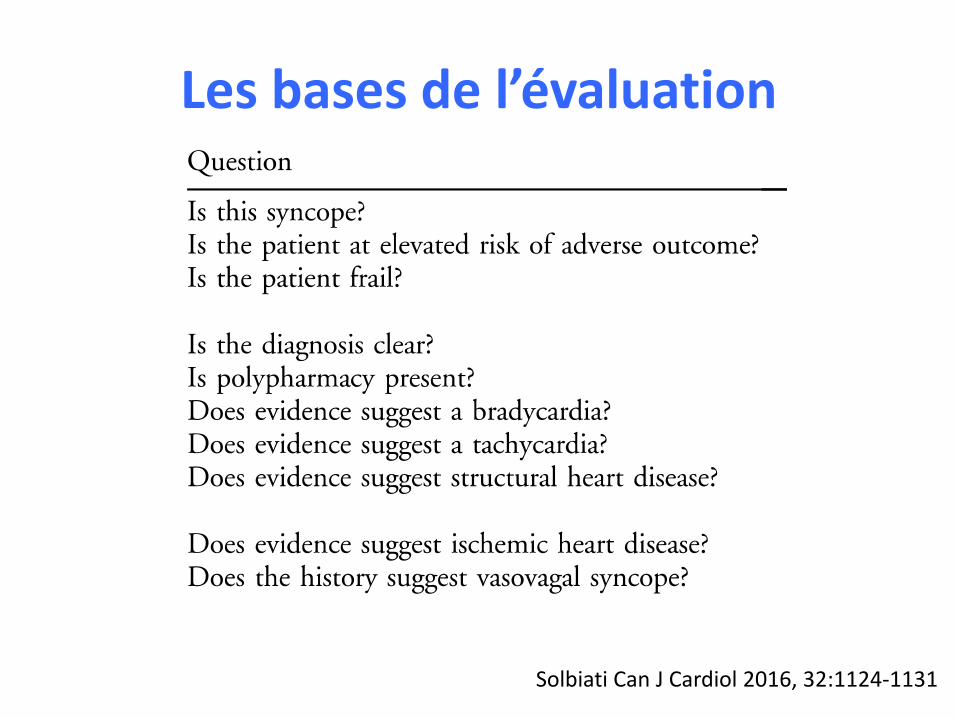
Les bases de l’évaluation
Solbiati Can J Cardiol 2016, 32:1124-1131

Données de l’interrogatoire : les 5 P
• Précipitants• Prodromes• Palpitations• Position
– Station debout prolongée– Changement positionnel brutal– Allongée
• Post-évènements
Parry BMJ 2010;340:c880
Syncopes : les explorations
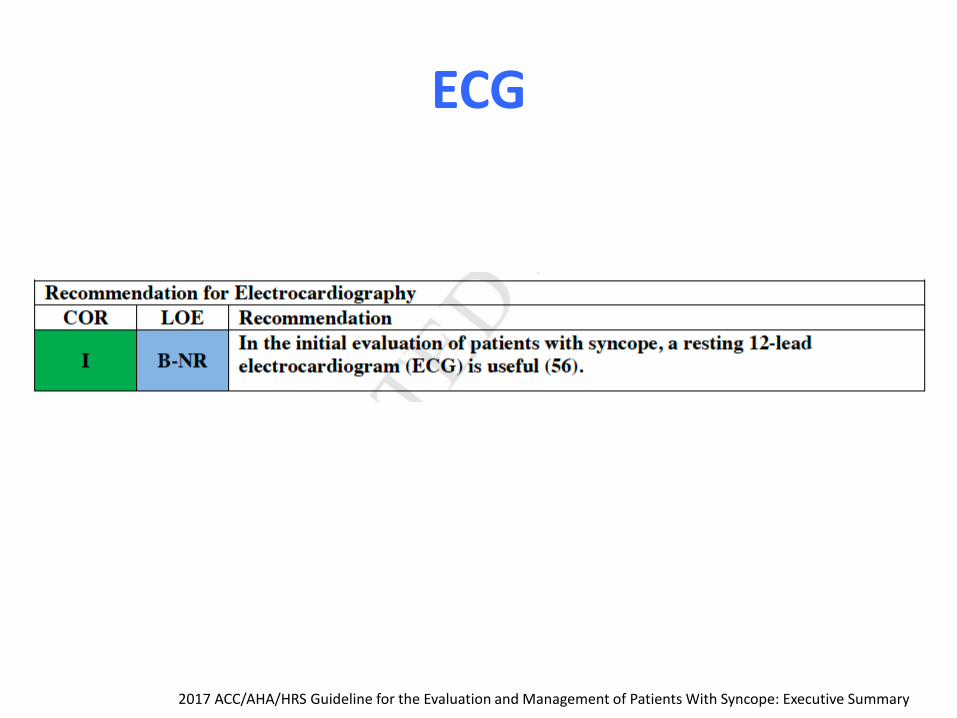
ECG
2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: Executive Summary
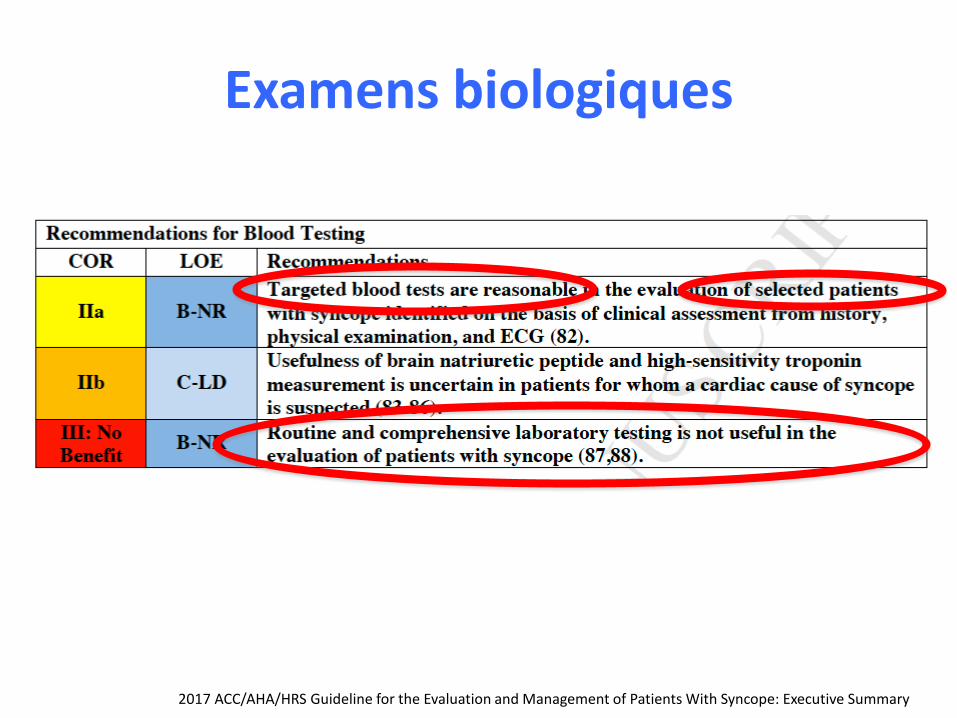
Examens biologiques
2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: Executive Summary
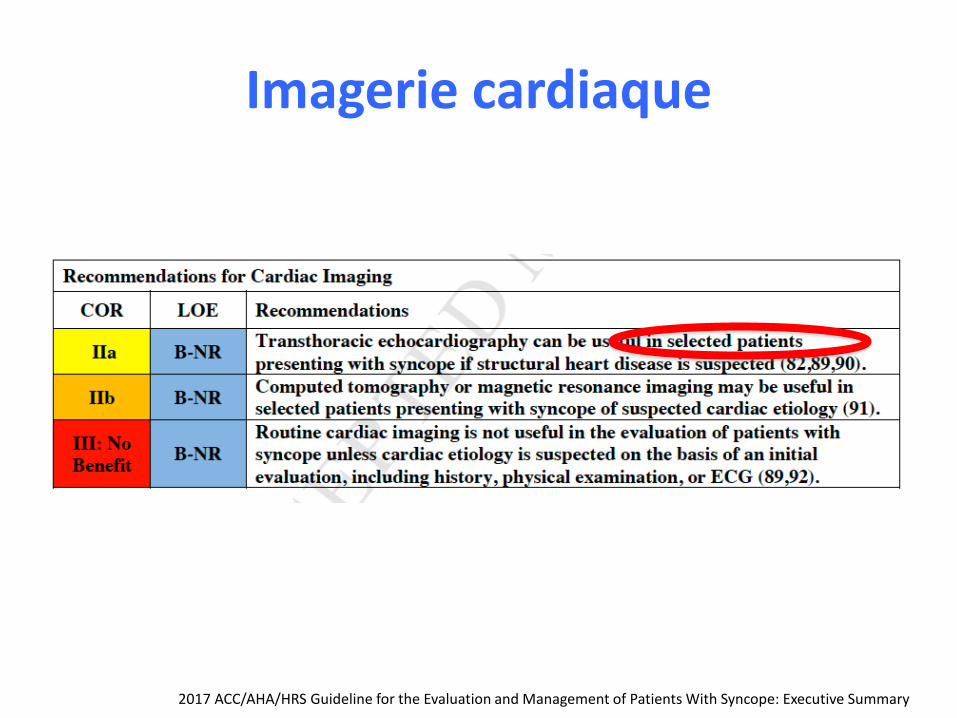
Imagerie cardiaque
2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: Executive Summary
Examens « neurologiques »
• Pas de scanner cérébral aux urgences chez un adulte asymptomatique avec syncope, traumatisme insignifiant et évaluation neurologique normale (American College of Emergency Physicians).
• Pas d’imagerie cérébrale (scanner ou IRM) dans l’évaluation d’une syncope simple avec examen neurologique normal (American College of Physicians).
• Pas d’imagerie des carotides en cas de syncope simple sans autre symptôme neurologique (American Academy of Neurology).
Runser Am Fam Physician. 2017;95(5):303-312
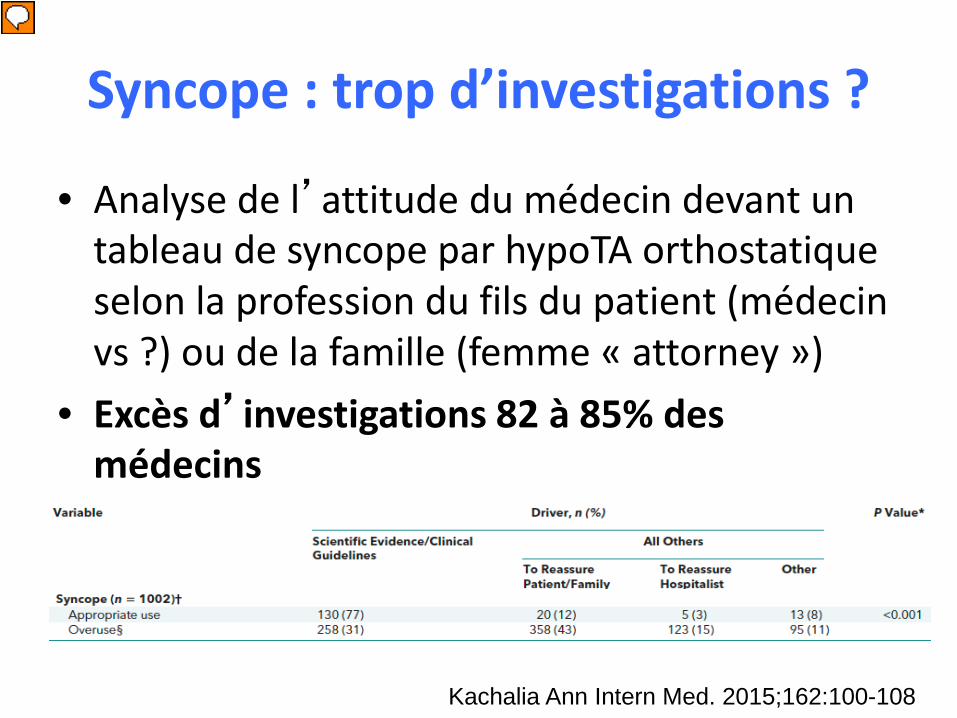
Syncope : trop d’investigations ?
• Analyse de l’attitude du médecin devant un tableau de syncope par hypoTA orthostatique selon la profession du fils du patient (médecin vs ?) ou de la famille (femme « attorney »)
• Excès d’investigations 82 à 85% des médecins
Kachalia Ann Intern Med. 2015;162:100-108
Présentateur
Commentaires de présentation
Overuse of Testing in Preoperative Evaluation and Syncope A Survey of Hospitalists Allen Kachalia, MD, JD; Aaron Berg, MD; Angela Fagerlin, PhD; Karen E. Fowler, MPH; Timothy P. Hofer, MD, MSc; Scott A. Flanders, MD; and Sanjay Saint, MD, MPH Background: Health care reform efforts and initiatives seek to improve quality and reduce costs by eliminating unnecessary care. However, little is known about overuse and its drivers, especially in hospitals. Objective: To assess the extent of and factors associated with overuse of testing in U.S. hospitals. Design: National survey of practice patterns for 2 common clinical vignettes: preoperative evaluation and syncope. Respondents were randomly selected and randomly provided 1 of 4 versions of each vignette. Each version contained identical clinical information but varied in factors that could change physician behavior. Respondents were asked to identify what they believed most hospitalists at their institution would recommend in each vignette. Setting: Mailed survey conducted from June through October 2011. Participants: Physicians practicing adult hospital medicine in the United States. Measurements: Responses indicating overuse (more testing than recommended by American College of Cardiology/American Heart Association guidelines). Results: 68% (1020 of 1500) of hospitalists responded. They reported overuse in 52% to 65% of the preoperative evaluation vignettes and 82% to 85% of the syncope vignettes. Overuse more frequently resulted from a physician's desire to reassure patients or themselves than an incorrect belief that it was clinically indicated (preoperative evaluation, 63% vs. 37%; syncope, 69% vs. 31%; P < 0.001 for each). Limitation: Survey responses may not represent actual clinical choices. Conclusion: Physicians reported substantial overuse in 2 common clinical situations in the hospital. Improving provider knowledge of guidelines may help reduce overuse, but despite awareness of the guidelines, physicians often deviate from them to reassure patients or themselves. Primary Funding Source: Blue Cross Blue Shield of Michigan Foundation, Department of Veterans Affairs Center for Clinical Management Research, University of Michigan Specialist-Hospitalist Allied Research Program, and Ann Arbor Veterans Affairs/ University of Michigan Patient Safety Enhancement Program. Ann Intern Med. 2015;162:100-108. doi:10.7326/M14-0694
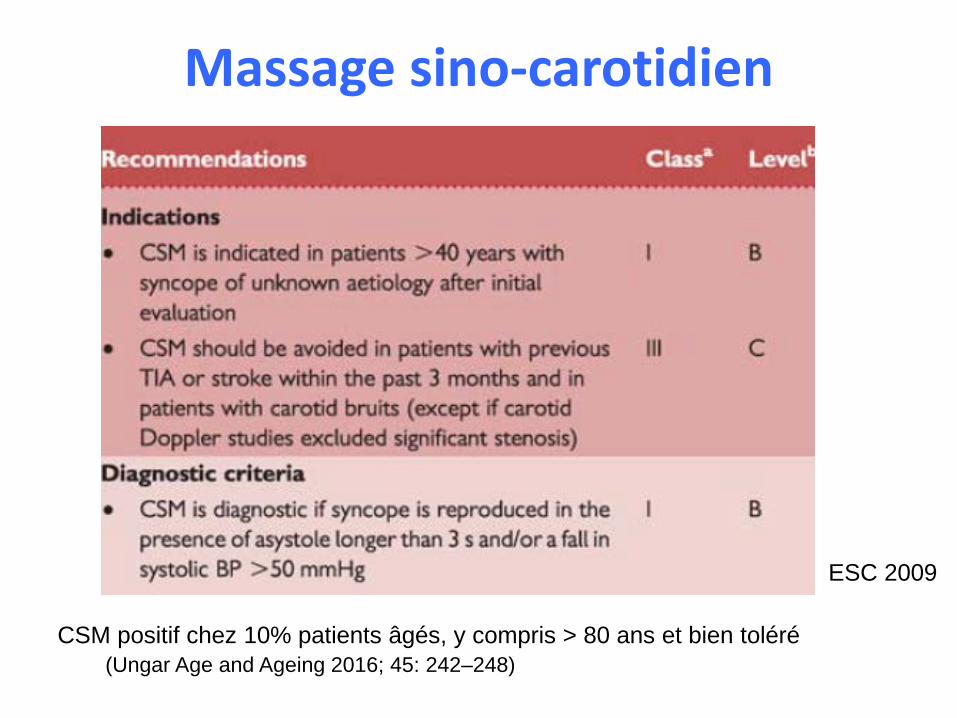
Massage sino-carotidien
ESC 2009
CSM positif chez 10% patients âgés, y compris > 80 ans et bien toléré(Ungar Age and Ageing 2016; 45: 242–248)

Facteurs de risque péjoratifs• Signes sd coronaire aigu
– Douleur thoracique suspecte– Modifications ECG ischemiques (sur
décalage ST ou sous décalage profond ST [>0.1 mV])
– Autres modif ECG (TV, FV, STV, FA rapide ou récente) anomalies ST-T
– Respiration courte
• ATCD cardiaques – ATCD coronaires, onde Q, cardiomyopathie
hypertrophique ou dilatée– ATCD Insuffisance cardiaque ou altération
fct VG– ATCD TV ou FV– Stimulateur cardiaque, défibrillateur– Utilisation préhospitalière antiarythmique
(sauf béta-bloquant ou anticalcique
• ATCD familial mort subite– Proche 1er degré mort subite, cardiopahtie
hypertrophique– Sd de Brugada ou QT long
• Valvulopathie– Souffle cardiaque
• Signes de troubles de conduction– Syncopes multiples dans les 6 mois– Tachycardie – Syncope à l’effort– QT > 500 ms– BAV 2ème ou 3ème degré, ou bloc
intraventriculaire
• Hypovolémie– Saignement digestif– Hématocrite < 30– Déshydratation non corrigée
• Persistance (>15 min) d’anomalies des signes vitaux aux urgences sans nécessité d’intervention (O2, vasopresseurs, PM)
– Fréquence respiratoire > 24 /min– saturation O2 < 90%– Rythme sinusal < 50 /min ou > 100 /min– PAS < 90 mm Hg
• Système nerveux central– événement primitif SNC (hém méningée, AVC)Grossman Arch Gerontol Geriatrics 2014, 58:110-114
Présentateur
Commentaires de présentation
Age is often a predictor for morbidity and mortality. Although we previously proposed risk factors for adverse outcome in syncope, after accounting for the presence of these risk factors, it is unclear whether age is an independent risk factor for adverse outcomes in syncope. Our objective was to determine whether age is an independent risk factor for adverse outcome following a syncopal episode. We conducted a prospective, observational study enrolling consecutive patients with syncope. Adverse outcome/critical intervention included hemorrhage, myocardial infarction/percutaneous coronary intervention, dysrhythmia, antidysrhythmic alteration, pacemaker/defibrillator placement, sepsis, stroke, death, pulmonary embolus or carotid stenosis. Outcomes were identified by chart review and 30- day follow-up. We found that of 575 patients, adverse events occurred in 24%. Overall, 35% with risk factors had adverse outcomes compared to 1.6% without risks. Age 65 were more likely to have adverse outcomes: 34.5% versus 9.3%, p < 0.001. Similarly, among patients with risk factors, elderly patients had more adverse outcomes: 43%; 36–50% versus 22%; 16–30%, p < 0.001. However, among patients with no predefined risks, there were no statistical differences: 3.6%; 0.28–13% versus 1%; 0.04– 3.8%. This was confirmed in a regression model accounting for the interaction between age > 65 and risk factors. Although the elderly with syncope are at greater risk for adverse outcomes overall and in patients with risk factors, age 65 alone was not a predictor of adverse outcome in syncopal patients without risk factors. Based on this data, it may be safe to discharge home from the ED patients with syncope, but without risk factors, regardless of age.
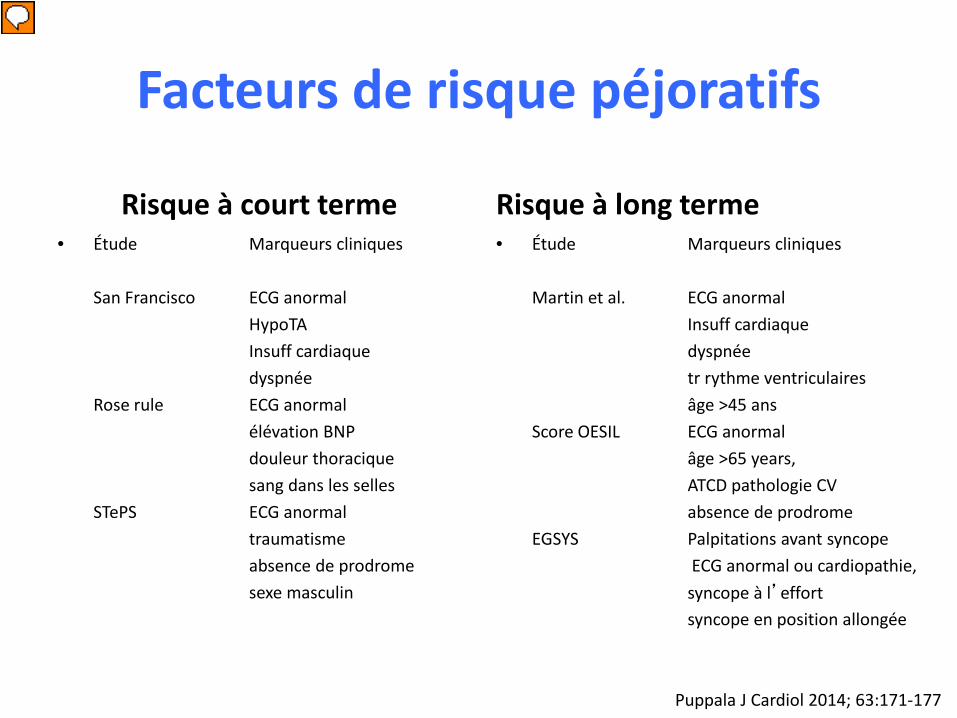
Facteurs de risque péjoratifs
Risque à court terme• Étude Marqueurs cliniques
San Francisco ECG anormalHypoTAInsuff cardiaquedyspnée
Rose rule ECG anormal élévation BNPdouleur thoraciquesang dans les selles
STePS ECG anormal traumatismeabsence de prodromesexe masculin
Risque à long terme• Étude Marqueurs cliniques
Martin et al. ECG anormalInsuff cardiaquedyspnéetr rythme ventriculairesâge >45 ans
Score OESIL ECG anormalâge >65 years, ATCD pathologie CVabsence de prodrome
EGSYS Palpitations avant syncopeECG anormal ou cardiopathie, syncope à l’effortsyncope en position allongée
Puppala J Cardiol 2014; 63:171-177
Présentateur
Commentaires de présentation
Age is often a predictor for morbidity and mortality. Although we previously proposed risk factors for adverse outcome in syncope, after accounting for the presence of these risk factors, it is unclear whether age is an independent risk factor for adverse outcomes in syncope. Our objective was to determine whether age is an independent risk factor for adverse outcome following a syncopal episode. We conducted a prospective, observational study enrolling consecutive patients with syncope. Adverse outcome/critical intervention included hemorrhage, myocardial infarction/percutaneous coronary intervention, dysrhythmia, antidysrhythmic alteration, pacemaker/defibrillator placement, sepsis, stroke, death, pulmonary embolus or carotid stenosis. Outcomes were identified by chart review and 30- day follow-up. We found that of 575 patients, adverse events occurred in 24%. Overall, 35% with risk factors had adverse outcomes compared to 1.6% without risks. Age 65 were more likely to have adverse outcomes: 34.5% versus 9.3%, p < 0.001. Similarly, among patients with risk factors, elderly patients had more adverse outcomes: 43%; 36–50% versus 22%; 16–30%, p < 0.001. However, among patients with no predefined risks, there were no statistical differences: 3.6%; 0.28–13% versus 1%; 0.04– 3.8%. This was confirmed in a regression model accounting for the interaction between age > 65 and risk factors. Although the elderly with syncope are at greater risk for adverse outcomes overall and in patients with risk factors, age 65 alone was not a predictor of adverse outcome in syncopal patients without risk factors. Based on this data, it may be safe to discharge home from the ED patients with syncope, but without risk factors, regardless of age.
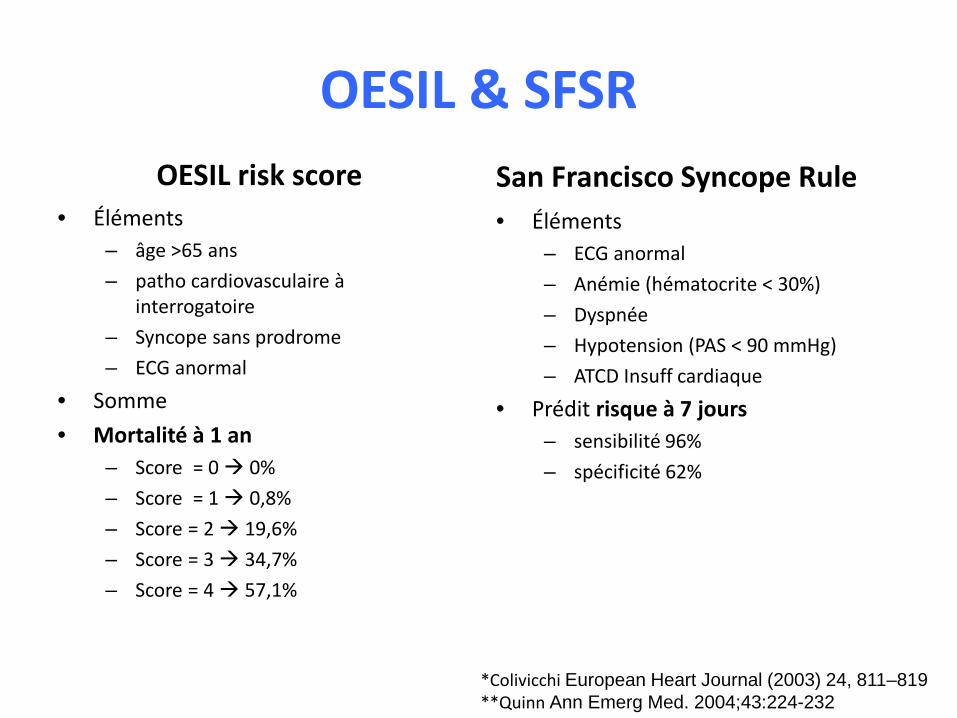
OESIL & SFSROESIL risk score
• Éléments– âge >65 ans– patho cardiovasculaire à
interrogatoire– Syncope sans prodrome– ECG anormal
• Somme • Mortalité à 1 an
– Score = 0 0%– Score = 1 0,8%– Score = 2 19,6%– Score = 3 34,7%– Score = 4 57,1%
San Francisco Syncope Rule• Éléments
– ECG anormal– Anémie (hématocrite < 30%)– Dyspnée– Hypotension (PAS < 90 mmHg)– ATCD Insuff cardiaque
• Prédit risque à 7 jours – sensibilité 96% – spécificité 62%
*Colivicchi European Heart Journal (2003) 24, 811–819**Quinn Ann Emerg Med. 2004;43:224-232
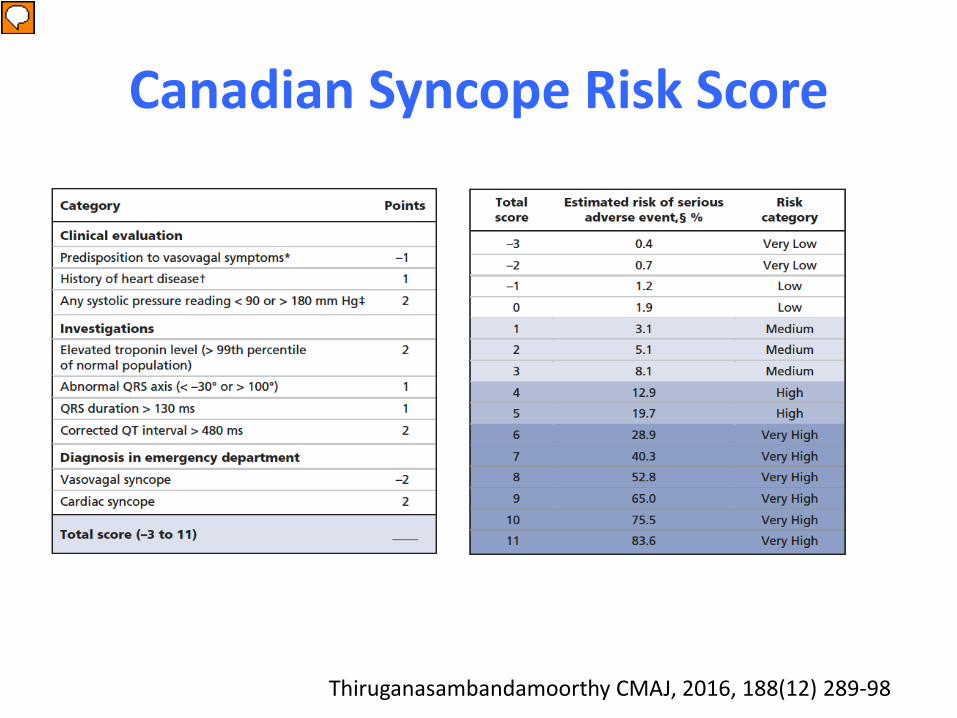
Canadian Syncope Risk Score
Thiruganasambandamoorthy CMAJ, 2016, 188(12) 289-98
Présentateur
Commentaires de présentation
Background: Syncope can be caused by serious conditions not evident during initial evaluation, which can lead to serious adverse events, including death, after disposition from the emergency department. We sought to develop a clinical decision tool to identify adult patients with syncope who are at risk of a serious adverse event within 30 days after disposition from the emergency department. Methods: We prospectively enrolled adults (age ≥ 16 yr) with syncope who presented within 24 hours after the event to 1 of 6 large emergency departments from Sept. 29, 2010, to Feb. 27, 2014. We collected standardized variables at index presentation from clinical evaluation and investigations. Adjudicated serious adverse events included death, myocardial infarction, arrhythmia, structural heart disease, pulmonary embolism, serious hemorrhage and procedural interventions within 30 days. Results: We enrolled 4030 patients with syncope; the mean age was 53.6 years, 55.5% were women, and 9.5% were admitted to hospital. Serious adverse events occurred in 147 (3.6%) of the patients within 30 days after disposition from the emergency department. Of 43 candidate predictors examined, we included 9 in the final model: predisposition to vasovagal syncope, heart disease, any systolic pressure reading in the emergency department < 90 or > 180 mm Hg, troponin level above 99th percentile for the normal population, abnormal QRS axis (< −30Æ or > 100Æ), QRS duration longer than 130 ms, QTc interval longer than 480 ms, emergency department diagnosis of cardiac syncope and emergency department diagnosis of vasovagal syncope (C statistic 0.88, 95% confidence interval [CI] 0.85–0.90; optimism 0.015; goodness-of-fit p = 0.11). The risk of a serious adverse event within 30 days ranged from 0.4% for a score of −3 to 83.6% for a score of 11. The sensitivity was 99.2% (95% CI 95.9%–100%) for a threshold score of −2 or higher and 97.7% (95% CI 93.5%–99.5%) for a threshold score of −1 or higher. Interpretation: The Canadian Syncope Risk Score showed good discrimination and calibration for 30-day risk of serious adverse events after disposition from the emergency department. Once validated, the tool will be able to accurately stratify the risk of serious adverse events among patients presenting with syncope, including those at low risk who can be discharged home quickly.
Faible intérêt pratique des outils de décision
• Nombreux outils de décision• SFSR (San Francisco Syncope Rule)* et OESIL score
(Osservatorio Epidemiologico sulla Sincope nel Lazio risk score)** validés, intérêt éventuel en pratique clinique***.
• N’augmentent pas la spécificité et la sensibilité diagnostique et ne déduisent pas les coûts****
• Les scores de stratification peuvent être raisonnables dans la prise en charge des patients ayant eu une syncope *****.
*Quinn Ann Emerg Med. 2004;43:224-232**Colivicchi European Heart Journal (2003) 24, 811–819***Serrano Ann Emerg Med. 2010;56:362-373****Sheldon (Position paper) Canadian Journal of Cardiology 27 (2011) 246–253*****2017 ACC/AHA/HRS Syncope Guideline
Présentateur
Commentaires de présentation
Serrano Study objective: We assess the methodological quality and prognostic accuracy of clinical decision rules in emergency department (ED) syncope patients. Methods: We searched 6 electronic databases, reviewed reference lists of included studies, and contacted content experts to identify articles for review. Studies that derived or validated clinical decision rules in ED syncope patients were included. Two reviewers independently screened records for relevance, selected studies for inclusion, assessed study quality, and abstracted data. Random-effects meta-analysis was used to pool diagnostic performance estimates across studies that derived or validated the same clinical decision rule. Between-study heterogeneity was assessed with the I2 statistic, and subgroup hypotheses were tested with a test of interaction. Results: We identified 18 eligible studies. Deficiencies in outcome (blinding) and interrater reliability assessment were the most common methodological weaknesses. Meta-analysis of the San Francisco Syncope Rule (sensitivity 86% [95% confidence interval {CI} 83% to 89%]; specificity 49% [95% CI 48% to 51%]) and the Osservatorio Epidemiologico sulla Sincope nel Lazio risk score (sensitivity 95% [95% CI 88% to 98%]; specificity 31% [95% CI 29% to 34%]). Subgroup analysis identified study design (prospective, diagnostic odds ratio 8.82 [95% CI 3.5 to 22] versus retrospective, diagnostic odds ratio 2.45 [95% CI 0.96 to 6.21]) and ECG determination (by evaluating physician, diagnostic odds ratio 25.5 [95% CI 4.41 to 148] versus researcher or cardiologist, diagnostic odds ratio 4 [95% CI 2.15 to 7.55]) as potential explanations for the variability in San Francisco Syncope Rule performance. Conclusion: The methodological quality and prognostic accuracy of clinical decision rules for syncope are limited. Differences in study design and ECG interpretation may account for the variable prognostic performance of the San Francisco Syncope Rule when validated in different practice settings. [Ann Emerg Med. 2010;56:362-373.] Sheldon Society Position Statement Standardized Approaches to the Investigation of Syncope: Canadian Cardiovascular Society Position Paper
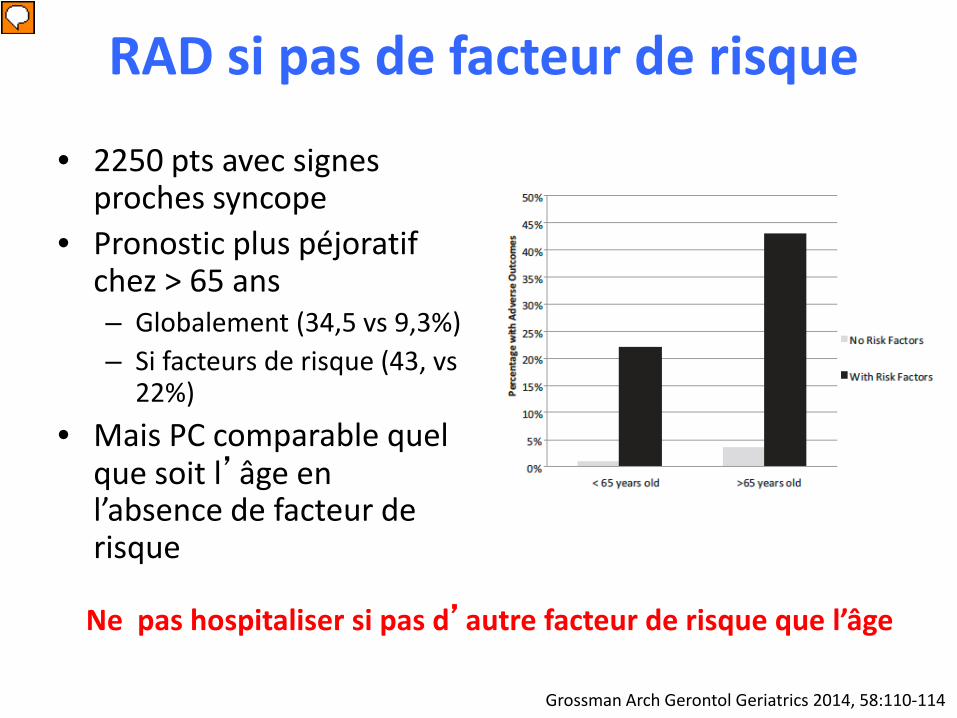
RAD si pas de facteur de risque
Grossman Arch Gerontol Geriatrics 2014, 58:110-114
• 2250 pts avec signes proches syncope
• Pronostic plus péjoratif chez > 65 ans– Globalement (34,5 vs 9,3%)– Si facteurs de risque (43, vs
22%)• Mais PC comparable quel
que soit l’âge en l’absence de facteur de risque
Ne pas hospitaliser si pas d’autre facteur de risque que l’âge
Présentateur
Commentaires de présentation
Age is often a predictor for morbidity and mortality. Although we previously proposed risk factors for adverse outcome in syncope, after accounting for the presence of these risk factors, it is unclear whether age is an independent risk factor for adverse outcomes in syncope. Our objective was to determine whether age is an independent risk factor for adverse outcome following a syncopal episode. We conducted a prospective, observational study enrolling consecutive patients with syncope. Adverse outcome/critical intervention included hemorrhage, myocardial infarction/percutaneous coronary intervention, dysrhythmia, antidysrhythmic alteration, pacemaker/defibrillator placement, sepsis, stroke, death, pulmonary embolus or carotid stenosis. Outcomes were identified by chart review and 30- day follow-up. We found that of 575 patients, adverse events occurred in 24%. Overall, 35% with risk factors had adverse outcomes compared to 1.6% without risks. Age 65 were more likely to have adverse outcomes: 34.5% versus 9.3%, p < 0.001. Similarly, among patients with risk factors, elderly patients had more adverse outcomes: 43%; 36–50% versus 22%; 16–30%, p < 0.001. However, among patients with no predefined risks, there were no statistical differences: 3.6%; 0.28–13% versus 1%; 0.04– 3.8%. This was confirmed in a regression model accounting for the interaction between age > 65 and risk factors. Although the elderly with syncope are at greater risk for adverse outcomes overall and in patients with risk factors, age 65 alone was not a predictor of adverse outcome in syncopal patients without risk factors. Based on this data, it may be safe to discharge home from the ED patients with syncope, but without risk factors, regardless of age.

Syncopes : points particuliers
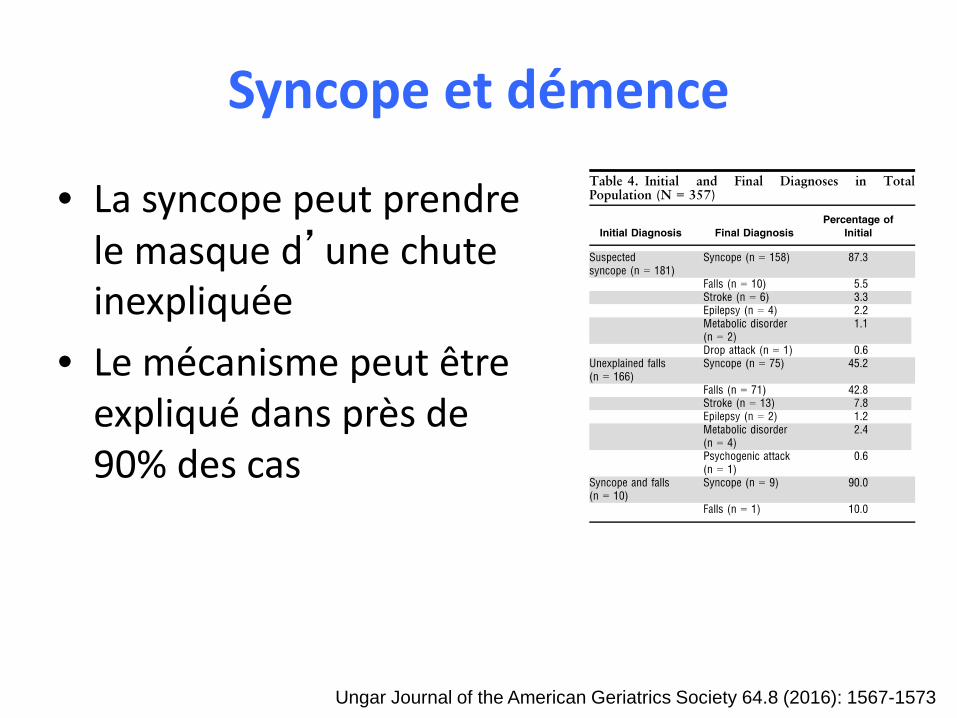
Syncope et démence
• La syncope peut prendre le masque d’une chute inexpliquée
• Le mécanisme peut être expliqué dans près de 90% des cas
Ungar Journal of the American Geriatrics Society 64.8 (2016): 1567-1573
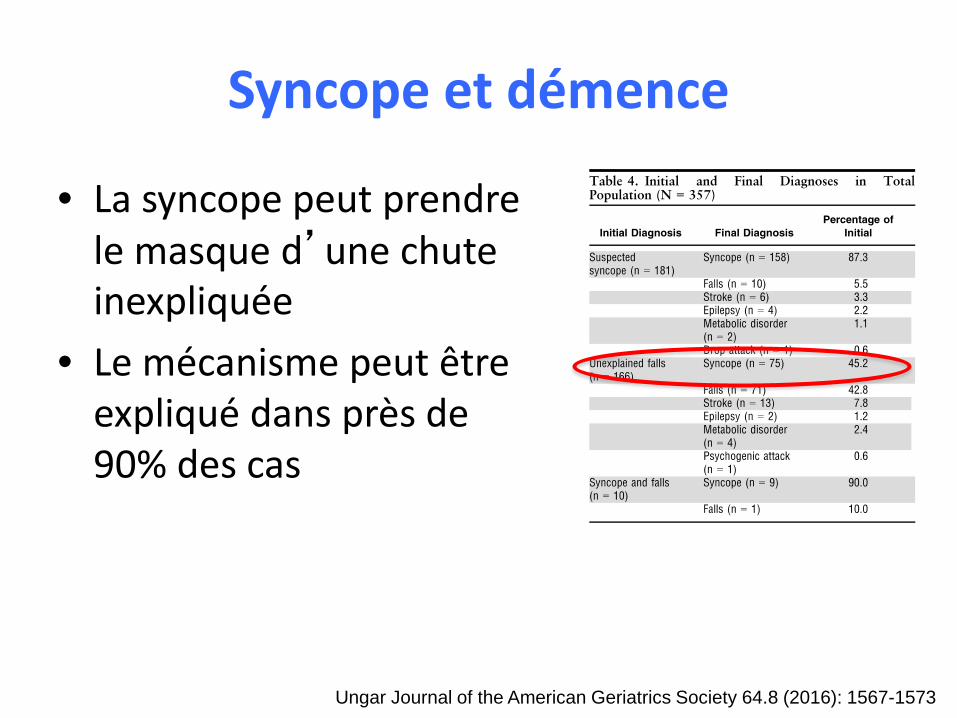
Syncope et démence
• La syncope peut prendre le masque d’une chute inexpliquée
• Le mécanisme peut être expliqué dans près de 90% des cas
Ungar Journal of the American Geriatrics Society 64.8 (2016): 1567-1573
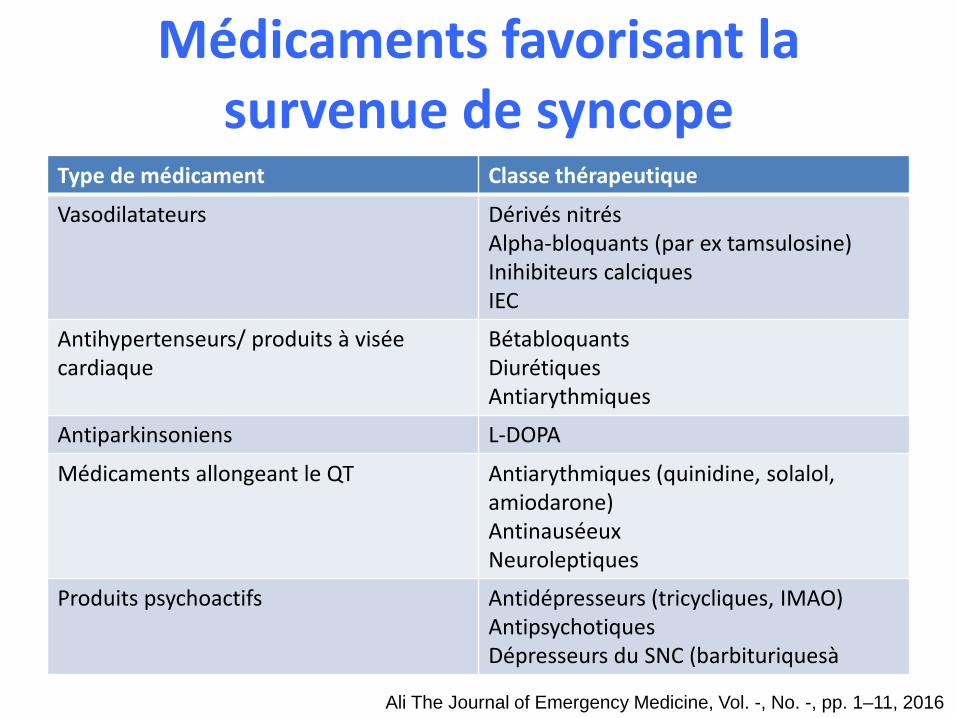
Médicaments favorisant la survenue de syncope
Type de médicament Classe thérapeutique
Vasodilatateurs Dérivés nitrésAlpha-bloquants (par ex tamsulosine)Inihibiteurs calciquesIEC
Antihypertenseurs/ produits à visée cardiaque
BétabloquantsDiurétiquesAntiarythmiques
Antiparkinsoniens L-DOPA
Médicaments allongeant le QT Antiarythmiques (quinidine, solalol, amiodarone)AntinauséeuxNeuroleptiques
Produits psychoactifs Antidépresseurs (tricycliques, IMAO)AntipsychotiquesDépresseurs du SNC (barbituriquesà
Ali The Journal of Emergency Medicine, Vol. -, No. -, pp. 1–11, 2016
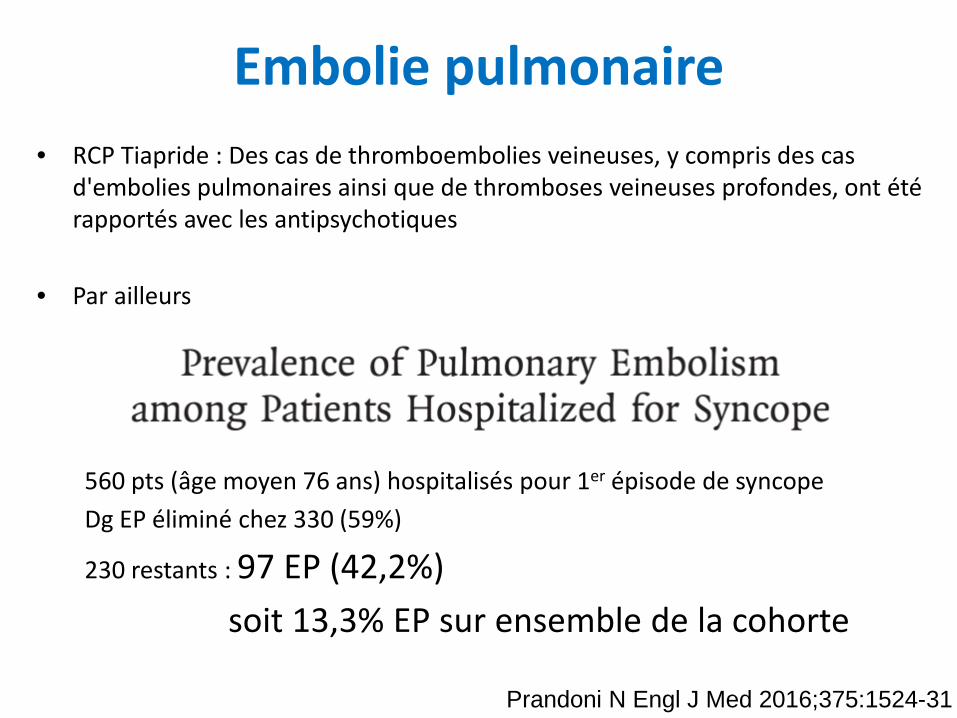
Embolie pulmonaire• RCP Tiapride : Des cas de thromboembolies veineuses, y compris des cas
d'embolies pulmonaires ainsi que de thromboses veineuses profondes, ont été rapportés avec les antipsychotiques
• Par ailleurs
560 pts (âge moyen 76 ans) hospitalisés pour 1er épisode de syncopeDg EP éliminé chez 330 (59%)
230 restants : 97 EP (42,2%) soit 13,3% EP sur ensemble de la cohorte
Prandoni N Engl J Med 2016;375:1524-31
Syncope : points clés• Les patients présentant un présyncope devraient être évalués de manière similaire à ceux qui
présentent une syncope. • Les patients présentant une syncope devraient avoir une recherche d’hypoTA orthostatique
et un ECG 12 dérivations.• Les examens complémentaires et d'imagerie ne devraient être demandés pour les patients
atteints de syncope que s’ils sont cliniquement indiqués par l’interrogatoire et et l'examen clinique.
• Les patients présentant une syncope doivent être hospitalisés en cas de signes d'insuffisance cardiaque, de maladies cardiaques structurelles, d’anomalies ECG ou d’ATCD familiaux de mort subite.
• Les patients atteints de syncope présentant un faible risque de complication (par ex symptômes compatibles avec syncope vasovagale ou par hypotension orthostatique, absence d'antécédents cardiaques, absence d'antécédents familiaux de décès cardiaque et ECG norma) peuvent être suivis en toute sécurité sans autre exploration ou traitement.
• Les enregistreurs implantables augmentent le rendement diagnostique, réduisent le temps de diagnostic et sont rentables en cas de doute sur une syncope cardiaque et ou en cas de syncope inexpliquée.
D’après Runser Am Fam Physician. 2017;95(5):303-312

Quelques références• Pertes de connaissance transitoires et malaises de l’adulte . Benjamin Cretin. 2014
Doin• Task Force for the Diagnosis and Management of Syncope, European Society of
Cardiology, European Heart Rhythm Association, Heart Failure Association, Heart Rhythm Society. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J 2009;30:2631-2671
• Pertes de connaissance brèves de l’adulte : prise en charge diagnostique et thérapeutique des syncopes. HAS 2008
• Guidelines on the management of valvular heart disease (version 2012). The Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal (2012) 33, 2451–2496
•






![[Product Monograph Template - Standard] · risk of hypotension, syncope, stroke, hyperkalemia and deterioration of renal function, including renal failure, in patients with diabetes](https://static.fdocuments.in/doc/165x107/5fcc59668fec3146ca0b382e/product-monograph-template-standard-risk-of-hypotension-syncope-stroke-hyperkalemia.jpg)



![[Product Monograph Template - Standard]COZAAR, or of angiotensin-converting-enzyme inhibitors (ACEIs) with aliskiren increases the risk of hypotension, syncope, stroke, hyperkalemia](https://static.fdocuments.in/doc/165x107/5f06a1677e708231d418f329/product-monograph-template-standard-cozaar-or-of-angiotensin-converting-enzyme.jpg)