QUICK REFERENCE GUIDE · Web viewMost MSSA are sensitive to meticillin, cephalosporins and...
35
STAPHYLOCOCCUS AUREUS (MRSA & MSSA) MANAGEMENT POLICY Version 12 Name of responsible (ratifying) committee Infection Prevention Management Committee Date ratified 05 April 2019 Document Manager (job title) Infection Prevention Management Committee Date issued 12 June 2019 Review date 11 June 2021 Electronic location Infection Prevention and Control Policies Related Procedural Documents Trust Policies: Hand Hygiene policy Isolation Policy Standard Precautions policy Decontamination policy Key Words (to aid with searching) MRSA, MSSA Staphylococcus aureus, staph aureus Version Tracking Version Date Brief Summary of Changes Author Staphylococcus aureus (MSSA, MRSA) Management Policy Version: 12 Issue Date: 12 June 2019 Review date: 11 June 2021 (unless requirements change) Page 1 of 35 Working together to drive excellence in care for our patients and communities
Transcript of QUICK REFERENCE GUIDE · Web viewMost MSSA are sensitive to meticillin, cephalosporins and...

STAPHYLOCOCCUS AUREUS (MRSA & MSSA) MANAGEMENT POLICY
Version 12
Name of responsible (ratifying) committee Infection Prevention Management Committee
Date ratified 05 April 2019
Document Manager (job title) Infection Prevention Management Committee
Date issued 12 June 2019
Review date 11 June 2021
Electronic location Infection Prevention and Control Policies
Related Procedural Documents
Trust Policies:Hand Hygiene policyIsolation PolicyStandard Precautions policyDecontamination policy
Key Words (to aid with searching) MRSA, MSSA Staphylococcus aureus, staph aureus
Version TrackingVersion Date Ratified Brief Summary of Changes Author
12 05/04/2019 Re-introduction of Hibiscrub as first line suppression therapy
Changes to orthopaedic and renal pathways
IPT
11 17/03/2017 Amendment to MRSA screening for elective orthopaedic patients
IPT
10 28/01/2015 Previously ‘Interim Staphylococcus Aureus Policy’ New elective pathway and renal dialysis pathway
diagrams
Infection Prevention
CONTENTSStaphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 1 of 26
Working together to drive excellence in care for our patients and communities
our patients and communities

1. INTRODUCTION.............................................................................................................................42. PURPOSE.......................................................................................................................................43. SCOPE............................................................................................................................................44. DEFINITIONS.................................................................................................................................45. DUTIES AND RESPONSIBILITIES................................................................................................56. PROCESS.......................................................................................................................................57. TRAINING REQUIREMENTS.......................................................................................................178. REFERENCES AND ASSOCIATED DOCUMENTATION............................................................179. EQUALITY IMPACT STATEMENT...............................................................................................1810. MONITORING COMPLIANCE WITH PROCEDURAL DOCUMENTS.........................................19Appendix 1...........................................................................................................................................20Appendix 2...........................................................................................................................................22EQUALITY IMPACT SCREENING TOOL...........................................................................................24
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 2 of 26

QUICK REFERENCE GUIDE
Screening for MRSA: Not all elective patients need to be screened for MRSA. Some elective specialties are required to screen all patients due to the prevalence and risk of MRSA in their populations. Other elective specialties only need to screen patients with specific risk factors for MRSA. See section 6.7 for relevant screening requirements and risk assessments.
All patients admitted as emergencies must be screened for MRSA at the time of admission. Patients attending the Emergency Department but not needing admission do not require screening.
Screening for S. aureus should be performed using a dry charcoal swab (one swab per site)Screening Sites:
Anterior nares (all patients) the same swab should be used for both nostrils Groin (inpatients only) the same swab should be used for both groins Wounds/skin lesions if multiple lesions, swab representative sample Intravenous devices do not disturb covered/dressed sites unless site looks infected Urinary catheters specimen of urine should also be obtained
All emergency admissions (and admissions to ICU) must be given topical S aureus protection until their screening results are known:
1st Line Suppression: Hibiscrub or Octenisan wash once daily until screening results known
Confirmed MRSA positive patients should receive suppression therapy under the guidance of the Infection Prevention Team:
1st Line Suppression: Mupirocin 2% applied to the inner surface of each nostril 3 times a day for 5 days Chlorhexidine Gluconate 4% (Hibiscrub) or Octenisan once daily for 5 days
2nd Line Suppression (for Mupirocin Resistant Strains): Naseptin applied to the inner surface of each nostril 4 times a day for 10 days Chlorhexidine Gluconate 4% (Hibiscrub) or Octenisan once daily for 10 days
Octenisan washes should only be used if the patient has a chronic skin condition or is intolerant / allergic to Chlorhexidine.
Once a patient is confirmed MRSA positive they should always be assumed to have a continuing positive status irrespective of current screening results. There is no requirement to obtain 3 negative screens post suppression therapy. The patient should be screened weekly after suppression therapy but assumed to remain positive
The purpose of suppression therapy is to achieve a short-term reduction in skin +/- nasal flora. Patients should not be given more than two courses of full suppression therapy in six months.
Patients with nasal or skin carriage of MSSA, or MSSA Blood Stream Infection do not routinely need to be isolated.Where possible, all patients with MRSA positive isolates should be placed in side rooms. High Staphylococcal dispersers must, without exception, take priority for side rooms:
MRSA positive sputum with productive cough MRSA positive tracheostomy MRSA/MSSA positive with severe skin shedding (e.g. severe eczema, psoriasis) MRSA positive in uncovered discharging wound
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 3 of 26

1. INTRODUCTION
Meticillin Sensitive Staphylococcus aureus (MSSA) and Meticillin Resistant Staphylococcus aureus (MRSA) are types of S. aureus bacteria present in community and healthcare settings capable of causing significant healthcare associated infection (HCAI).
2. PURPOSE
This policy defines the actions taken by Portsmouth Hospitals NHS Trust to reduce the transmission of S. aureus within relevant acute and community environments by reducing or managing their reservoirs and preventing onwards transmission. This policy will inform all hospital workers of their individual responsibilities to effectively manage S. aureus. This policy should be read in conjunction with the Standard Precautions, Hand Hygiene and Isolation policies.
3. SCOPE
This policy applies to all Portsmouth Hospitals NHS Trust staff, health and non-healthcare, including agency, bank and locum staff, as well as contractors and external agencies.
‘In the event of an infection outbreak, flu pandemic or major incident, the Trust recognises that it may not be possible to adhere to all aspects of this document. In such circumstances, staff should take advice from their manager and all possible action must be taken to maintain ongoing patient and staff safety’
4. DEFINITIONS Colonisation: Presence of S. aureus (often nose, sputum, urine, faeces, open wounds or on the skin) without the presence of symptoms or clinical manifestations of illness or infection. A colonized individual may transmit the organism to another person. Suppression Therapy: Temporary suppression of the S. aureus carrier state through use of topical agents (e.g. Chlorhexidine or Octenisan washes +/- antimicrobial nasal cream). This decreases the risk of transmission to others. Infection: Invasion and multiplication of S. aureus in tissue with the manifestation of clinical symptoms of infections such as increased white blood cell counts, fever, lesions, furuncles, drainage from a break in skin continuity and erythema. Infection warrants treatment. Mode of Transmission: The method by which S. aureus is spread into the environment and to other persons. S. aureus are transmitted primarily by direct person-to-person contact (i.e. from the hands of one individual to a susceptible individual). Contaminated bed linen, surfaces, medical equipment and high levels of environmental dust also play a significant role in transmission.
Meticillin Resistant Staphylococcus aureus (MRSA): A gram-positive bacteria, found on approximately 3% of the general population and up to 7% of hospital patients that is not inhibited by meticillin or oxacillin and many other antimicrobials. Meticillin Sensitive Staphylococcus aureus (MSSA): A gram-positive bacterial, carried by approximately 50% of the healthy adult population at any one time (20% persistent carriers, 60% intermittent carriers, 20% non carriers). Most MSSA are sensitive to meticillin, cephalosporins and oxacillin. MSSA is a common cause of localised skin and soft tissue infections or serious disease like discitis, osteomyelitis, septic arthritis, endocarditis, pneumonia or systemic sepsis.
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 4 of 26

5. DUTIES AND RESPONSIBILITIES
Infection Prevention Team: Review and update MRSA/MSSA policy Give additional advice regarding the management of patients with MRSA/MSSA Include MRSA/MSSA in all induction and update training for clinical staff Promote good practice and challenge poor practice
Microbiologists: Alert Infection Prevention Team and clinical teams (where appropriate) of patients with
clinically significant MRSA/MSSA infections Follow the antimicrobial prescribing policy for patients with or at risk of MRSA/MSSA
Patient Flow / Duty Hospital Managers: Facilitate placement of patients with MRSA into appropriate isolation rooms Escalate difficulties in management/placement of MRSA/MSSA patients to the Infection
Prevention Team Ensure effective communication of patients risk and carriage status
Matrons / Ward Managers: Must establish a culture of compliance with infection prevention practice across their units Ensure admission and weekly screening for MRSA occurs as per policy Promote good practice and challenge poor practice
Medical Staff: Ensure compliance with infection prevention and antimicrobial prescribing policies Ensure prudent antimicrobial prescribing and stringent use/removal of indwelling devices Follow advice of the Infection Prevention Team relating to patients with MRSA/MSSA
All Healthcare Staff: Must be familiar with and adhere to the relevant infection prevention policies to reduce the
risk of cross infection of patients Must adhere to the full terms and conditions documented in this policy Refer to the infection prevention team if unable to follow the policy guidelines Must check the MRSA status of their patient prior to any invasive procedure
6. PROCESS
6.1 General Principles:Standard precautions, including strict hand hygiene and appropriate use of personal protective equipment should be applied to all patients without exception, regardless of known S. aureus colonisation or infection (refer to standard precautions and hand hygiene policy).
6.2 Screening of patients:Screening for S. aureus should be performed using a dry charcoal swab (one swab per site)
6.2.1 Screening Sites: Anterior nares (all patients) the same swab should be used for both nostrils Groin (inpatients only) the same swab should be used for both groins Wounds/skin lesions if multiple lesions, swab representative sample Intravenous devices do not disturb covered/dressed sites unless site looks infected Urinary catheters specimen of urine should also be obtained
6.3 Suppression Therapy:
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 5 of 26

The purpose of suppression therapy is to achieve a short-term reduction in skin +/- nasal flora to protect the patient during specific events in their admission (e.g. immediately on admission for blood cultures, lines, catheterisation etc. and for certain invasive procedures thereafter). The goal is not to achieve long-term eradication and patients should not be given more than two courses of full suppression therapy in six months to try and achieve this.
6.4 Directions for Administering Suppressive Agents:Suppression therapy should be prescribed on the patients medication chart or as an out-patient prescription and clearly limited in duration, dependent on the agent used
6.4.1 Topical Washes:Hibiscrub (Chlorhexidine 4%) is an antimicrobial wash suitable only for adults and should not be used on patients with hibiscrub allergy or infected, dry, or flaking skin.
Octenisan is a gentle, non-perfumed antimicrobial wash, suitable for use in all age groups (including neonates greater than 28 weeks gestation) and those with eczema and psoriasis.
Patients should wash once daily for 5 days as follows:- Days 1 and 5 wash the whole body, neck, face and hair- Days 2, 3 and 4 wash the whole body, neck and face
Patients should use approximately 50mls of Octenisan or Hibiscrub per wash Patient should wet their skin prior to application of Octenisan or Hibiscrub Octenisan or Hibiscrub should not be diluted in washing water – it must be applied neat Special attention should be paid to sites such as axillae, groin, perineum and buttock areas
or other skin folds Fresh towels and facecloths should be used each day A daily change of bedding and clothing is required and should occur at the same time as the patient washes with Hibiscrub or Octenisan Suppression should be discontinued immediately and the IPCT contacted if the patient
experiences excessive skin irritation or allergic reaction
6.4.2 Nasal Creams:Mupirocin and Naseptin are antimicrobial ointments for use in the nasal passages.Repeated or prolonged courses of Mupirocin or Naseptin must be avoided due to possible development of resistance.
General Directions: Using a clean finger, the patient should wipe a pea-sized amount of ointment around the
inside of each nostril and squeeze their nose Patients should be able to taste the ointment at the back of their throat. If they cannot, they
should apply a small amount of extra cream
6.5 Ongoing S. aureus status:Suppression therapy is designed to reduce the burden of S. aureus on a patient’s skin. It is highly unlikely to achieve long-term eradication and a large number of patients will have detectable levels of S. aureus within one year of treatment. Once a patient is MRSA positive they should always be assumed to have a continuing positive status irrespective of current screening results. Repeated courses of suppression should not be offered unless the patient is undergoing invasive procedures. There is no requirement to obtain 3 negative screens post suppression therapy. The
patient should be screened weekly after suppression therapy but assumed to remain positive
6.6 Continuation of suppression therapy after discharge:Confirmed MRSA positive patients discharged before completing suppression therapy should complete the remainder of their course in the community. Suppression therapy should be clearly written on the TTO chart and documented in the discharge letter.
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 6 of 26

6.7 ELECTIVE SURGICAL PATHWAY:All relevant patients booked as electives should be screened for MRSA. At present, there is no requirement to risk assess or routinely screen patients for MSSA, with the exception of patients undergoing spinal surgery.
The following specialties must screen all elective cases for MRSA prior to procedures:
Cardiology Clinical haematology Gastroenterology Medical oncology
Nephrology Obstetrics (caesareans) Pain relief Plastic surgery Renal surgery
Rheumatology Transplant surgery Trauma and orthopaedics Urology Vascular surgery
The following specialties only need to screen patients identified as high risk:
Breast surgery Colorectal surgery Day case dental Dermatology ENT Elderly medicine Endocrinology
Endoscopy General medicine General surgery Gynaecology Hepatobiliary Neurology Obstetrics (ex caesareans)
Ophthalmology Oral surgery Orthodontics Paediatric medicine Radiotherapy Rehabilitation Thoracic medicine Upper GI surgery
6.7.1 Risk Assessment: A patient is regarded as ‘high risk’ for the carriage or acquisition of MRSA if they fulfill one or more of the following criteria: Have been MRSA positive at any point in the past Had a previous admission to any healthcare facility in the last 6 months Have been admitted from a residential home (inc Nursing Homes, Military Barracks, HM Prisons) Have been admitted with indwelling devices (inc urinary catheters, PICC, tunneled lines) Have chronic open wound(s) (skin breaks, pressure sores, ulcers) or cellulitis Have any chronic skin condition (inc psoriasis, eczema, dermatitis) Have been or are an IV drug user Have been or are a healthcare worker Are admitted for a high risk procedure (joint replacement or implant surgery)
‘High risk’ patients must be identified at the point of pre-operative assessment or clerking. Patients with none of the above risk factors are considered to be ‘low risk’ for the carriage or acquisition of MRSA.
Screening of elective patients should occur no greater than 6 weeks prior to surgery. For elective orthopaedic patients; if the surgery is cancelled and the patient screened negative for MRSA and has no high risk factors, a further screen is not required. However, the patient should be offered suppression therapy on the day of surgery. If the patient does fall in the high risk category they will require rescreening.
For those patients seen in pre-operative assessment more than 7 days before surgery: Screening should be performed and a result obtained. Confirmed positive patients should
then be treated with Hibiscrub/Bactroban or Octenisan/Bactroban if sensitive or intolerant to chlorhexidine in the 5 days leading up to surgery, completing their suppression course on the day of surgery. No repeat screening is required prior to surgery and the patient should be treated as colonised for the purposes of theatre – appropriate intra-operative antibiotics covering MRSA should be used
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 7 of 26

Confirmed MRSA positive patients under the guidance of the Infection Prevention Team:
1st Line Suppression: Mupirocin 2% applied to the inner surface of each nostril 3 times a day for 5 days Chlorhexidine Gluconate 4% (Hibiscrub) or Octenisan once daily for 5 days
2nd Line Suppression (for Mupirocin Resistant Strains): Naseptin applied to the inner surface of each nostril 4 times a day for 10 days Chlorhexidine Gluconate 4% (Hibiscrub) or Octenisan once daily for 10 days
Octenisan washes should only be used if the patient has a chronic skin condition or is intolerant / allergic to Chlorhexidine.
For those patients seen in pre-operative assessment less than 7 days before surgery: Patients should be screened, risk assessed (see criteria 6.7.1), with patients deemed as
high risk given antimicrobial wash to start immediately in order to complete as many days as possible prior to surgery
For patients that cannot be screened prior to surgery, a screen should be obtained on the day of surgery and a risk assessment (see criteria above) performed. High-risk patients should receive an antimicrobial wash prior to going to the operating theatre.
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 8 of 26

As part of Elective Pre-Operative Assessment for patients assessed as high risk of MRSA carriage:
1st Line Suppression: Chlorhexidine Gluconate 4% (Hibiscrub) or Octenisan once daily for 5 days
6.8 EMERGENCY ADMISSION PATHWAY:
6.8.1 Screening for MRSA:All patients admitted as emergencies must be screened for MRSA at the time of admission. Patients attending the Emergency Department but not needing admission do not require screening. For minimum screening requirements see section 6.2.1
As part of the Emergency Admission Pathway for all emergency admissions prior to screening results or any admission to ICU:
1st Line Suppression: Hibiscrub or Octenisan wash once daily until screening results known
Confirmed MRSA positive patients under the guidance of the Infection Prevention Team:
1st Line Suppression: Mupirocin 2% applied to the inner surface of each nostril 3 times a day for 5 days Hibiscrub or Octenisan wash once daily for 5 days (see appendix 2)
2nd Line Suppression (for Mupirocin Resistant Strains): Naseptin applied to the inner surface of each nostril 4 times a day for 10 days
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 9 of 26

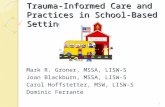
Wash your face with undiluted Hibiscrub – especially around the nose, avoiding your eyes and ears
Use a clean sponge, work downwards and wash well around your armpits.
Continue washing downwards and wash well around the groin area.
Rinse yourself off under the shower.
Now repeat steps 1 to 4, but this time start with your hair.
Hibiscrub or Octenisan wash once daily for 10 days
Octenisan washes should only be used if the patient has a chronic skin condition or is intolerant / allergic to Chlorhexidine.
6.8.2
Instructions for using Hibiscrub Wash
1.
2.
3.
4.
5.
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 10 of 26

After a final rinse, dry yourself thoroughly with a clean towel and put on clean clothes.
6.
Instructions for using Octenisan Wash
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 11 of 26

Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 12 of 26
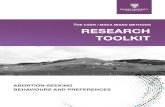
Continue daily Hibiscrub washes
Rescreen every 7 days or on designated ward
screening day
Wait for Admission Screening Results
Positive MRSA Screen
Negative MRSA Screen
Rescreen every 7 days or on designated ward
screening day
Positive MRSA ScreenStart full suppression therapy for 5 days
Mupirocin 2% (Bactroban) nasal ointment 3 times daily
Hibiscrub or Octenisan body wash once daily
48-72 HOURS
Negative MRSA ScreenOption to discontinue Hibiscrub or Octenisan
washes. If patient has chronic wounds, eczema/psoriasis or invasive procedures
planned, suppression may be continued with no time limit
4 HOURSStart Daily Hibiscrub or Octenisan Washes (every patient) – pre-
prescribed as aboveOnce daily body wash 30-50mLs used undiluted over whole body
(do not use nasal Bactroban)
1 HOUREmergency Admission
Routine admission swabs (every patient)Nose & Groin & Site of Infection (e.g. wound[s])

6.9 RENAL DIALYSIS PATHWAY:
Patients receiving Renal Hemodialysis should be screened every 6 months for MRSA and MSSA. If the result is MRSA/MSSA positive, the patient should be offered a full course of suppression for five days following the positive culture result. The patient should be assumed to remain MRSA/MSSA positive despite treatment.
6.10 Isolation and transmission precautions for MRSA and MSSA:Healthcare staff must provide patients and families with appropriate verbal and written information about MRSA or MSSA and explain the need for isolation and transmission precautions where indicated. Written information can be obtained from Infection Prevention.It is important that all relevant staff involved in patient care is aware of the patient’s MRSA/MSSA status and of the infection prevention and control precautions required to reduce the risk of transmission. It is the responsibility of ward staff to inform other departments of the patients MRSA/MSSA status.
Standard precautions should be applied to all patients, routinely.Patients with nasal or skin carriage of MSSA, or MSSA Blood Stream Infection (BSI) do not routinely need to be isolated.Where possible, all patients with MRSA positive isolates should be placed in side rooms. High Staphylococcal dispersers must, without exception, take priority for side rooms: MRSA positive sputum with productive cough
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 13 of 26
Negative MRSA Screen
Hibiscrub washes prior to HD
Screen every 6 months, manage as positive /
isolate / barrier
Positive MRSA Screen
Screen every 6 months
Positive MRSA ScreenStart full suppression therapy for 5 days
Mupirocin 2% (Bactroban) nasal ointment 3 times daily
Hibiscrub or Octenisan body wash once daily
Established HaemodialysisRoutine swabs
Nose & Groin & Site of Infection (e.g. wound[s])

MRSA positive tracheostomy MRSA/MSSA positive with severe skin shedding (e.g. severe eczema, psoriasis) MRSA positive in uncovered discharging wound
6.10.1 Patient movement – internal:The movement of patients with MRSA should be minimised to reduce the risk of cross infection. Where patients need to change specialties or attend departments for essential investigations, the risk posed to other patients should be managed by strict infection control procedures.Staff who are transferring patients must ensure that: The receiving area is aware of the patient’s MRSA status The receiving area has the appropriate level of isolation nursing available The patient is wearing clean / fresh clothes and is on a bed with clean linen Lesions are covered with an impermeable dressing wherever possible All transfer equipment is decontaminated before and after transfer
Portering staff who transfer patients do not need to wear gloves. They MUST cleanse their hands before and after the transfer using soap and water or alcohol hand gel
6.10.2 Patient movement - external/discharge: MRSA is not a valid reason for delaying appropriate care, interventions, transfer or
discharge. These should occur when clinically appropriate Prior to transfer to other healthcare facilities (e.g. hospitals, residential care homes, etc)
the receiving facility must be notified of the individual’s MRSA status Specialised care relating to the patients MRSA status (e.g. wound management,
suppression therapy, and antibiotic therapy) should be discussed by the patient’s physician with relevant agencies (e.g. GP, community Infection Prevention Team, District Nurses) prior to discharge.
Transfer / referral letters must clearly state the MRSA status of the patient Carriage of MRSA is not a valid reason for exclusion from residential care homes Staff are encouraged to contact the IPCT (7700 6261) to discuss problems relating to
delay in discharge due to MRSA status
6.10.3 Patient movement - deceased patients:No additional precautions are required
6.10.4 During the Patient Stay:All patients should: be actively encouraged to keep the bed space free from clutter to enable cleaning be actively discouraged from touching wounds be actively encouraged to observe good hand hygiene at every opportunity including
using the alcohol hand gel at the bedside be encouraged to challenge poor hand hygiene practice
6.10.5 Visitors and MRSA/MSSA:Visitors of patients with MRSA/MSSA are encouraged Visitors must wash/decontaminate their hands before entering the clinical area and
immediately prior to leaving, Alcohol hand rub gel is suitable for visibly clean hands Protective clothing does not need to be worn unless a visitor is providing hands-on care
6.10.6 MRSA/MSSA in the Operating Theatre: Apart from rigorous surgical skin preparation, no additional precautions are required for MSSA.Every effort should be made to reduce the risk of MRSA colonisation or infection before surgery or procedures. A patient’s MRSA status should not prejudice their surgical management.
MRSA positive patients can be scheduled for surgery at any time on the list, providing the required level of decontamination can be achieved between cases
Rigorous surgical skin preparation using 2% Chlorhexidine 70% Isopropyl alcohol should be observed
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 14 of 26

At the end of every surgical procedure with an MRSA positive patient, anaesthetic and any other equipment must be decontaminated with 1000ppm of Actichlor plus. Refer to Trust Decontamination Manual. Extra time may need to be allocated for procedures to allow appropriate cleaning of area
Equipment and the staff attending the patient should be kept to the minimal level without compromising the patient safety or care. All equipment must be cleaned after each MRSA case
Lesions not involved in the surgical procedure should be covered with an impermeable dressing
Discuss with a medical microbiologist the need for specific antibiotic prophylactic cover – see Trust antibiotic policy – surgical prophylaxis
MRSA positive patients in recovery must be segregated wherever feasible and nursed by dedicated staff adhering to isolation procedures
6.10.7 Environmental Cleaning:The management of the environment and equipment should be considered central to minimising the spread of MRSA/MSSA. Cleaning regimens should focus on the elimination of dust and the removal of fomites (see decontamination policy)
6.10.8 Terminal Cleaning on patient discharge / transfer / deathMRSA (or potential MRSA) contaminated patient areas must be cleaned / disinfected after the patient’s discharge. Within PHT between the hours of 0800 – 2100 ‘Terminal Cleans’ are provided by Domestic Services via Engie helpdesk on Ext 7700 6321.Areas situated off-site (not QA hospital) are to request cleaning as per their local procedure.
6.10.9 Out of Hours Terminal Cleaning:Patient areas vacated outside of Domestic Services hours must be cleaned by Clinical staff. The ‘Terminal Clean’ includes:
The cleaning and disinfection of the bed space using a chlorine and detergent based product at 1000ppm of Actichlor plus. The equipment within the bed space includes: The bed – mattress, pillows, bed frame and bed rails. Pillows and mattress covers should
be checked for damage and changed if necessary. (Therapy beds may need specialist cleaning in accordance with the manufacturer’s/hirer’s instructions)
High and low level dusting Washing of floors The bedside locker The over bed table The chair The patient call buzzer Any plastic patient files stored at end of bed The alcohol gel dispenser Any extra equipment that is no longer required should be removed and stored after
cleaning and disinfection Patientline equipment must be wiped over with a soap and water wipe only and foam ear
pads replaced
6.10.10 Completion of Clean:The bed is then safe to admit another patient; however the Engie helpdesk must be informed that a ‘Terminal Clean’ requires completion. This would include: The removal and laundering of curtains including shower curtains Cleaning of the floors Damp dusting of the wider area including radiators and shelves Walls do not require cleaning unless physically contaminated
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 15 of 26

6.11 VISA (Vancomycin intermediate S. aureus) GISA (Glycopeptide intermediate S. aureus) VRSA (Vancomycin resistant S. aureus):VISA / GISA and VRSA infections are still relatively rare and typically occur in patients with MRSA colonisation/infection after persistent exposure to glycopeptides. It is prudent to assume that VISA/GISA (and by inference VRSA) is as transmissible as MRSA in the healthcare setting. The care and management of the patient must be discussed with a medical microbiologist or IPCT before the patient is admitted or as soon as the infection is discovered.In addition to the standards outlined in this policy for MRSA management the following must be applied: The patient must be admitted / transferred to a side room within a specialised area
depending on the patient’s clinical needs The number of staff looking after the patient must be reduced to the minimum in line with
the needs of the patient. These staff must not look after any other patient during the shift or do another concurrent shift without showering and changing uniform
Single use gloves and aprons must be worn at all times whilst in the room Door to the room MUST BE SHUT at all times
6.12 MRSA and MSSA Blood Stream Infection (BSI):The Trust is actively engaged in the mandatory surveillance and reduction MRSA and MSSA BSI inline with national and local targets. The Trust is required to report all cases of MRSA or MSSA BSI acquired >48 hours after admission. A Post Infection Review (PIR) will be undertaken for all MRSA BSI jointly by clinicians and the infection prevention team to identify learning in these cases. The IPCT will notify clinicians of the need for a PIR.
6.13 Staff Screening for Staphylococcus aureus (MRSA or MSSA):The following primarily refers to MRSA colonisation of staff but may be used for screening for MSSA if required
6.13.1 General Principles:Staff members, particularly those involved in direct clinical care, are likely to come into contact with a wide range of organisms, including MRSA as part of their normal daily work. Staff must, therefore, apply standard precautions to all patient interaction, including strict hand hygiene and appropriate use of PPE, to prevent transient acquisition and onwards spread of any bacteria.
Persistent MRSA carriage in staff members who act as a reservoir for the bacteria is less common and regular or routine screening of staff members is not thought to be useful.
Where screening is undertaken, staff can be assured that the process will be: confidential transparent fair and impartial as far as possible, non-detrimental to the persons career pathway
6.13.2 Pre-employment screening: Pre-employment screening of staff members is not routinely required. However, where there is a history of colonisation, the applicant may be screened through the Occupational Health Department (OHD) and suppression given prior to commencing employment if found to be positive.
6.13.3 Staff Screening: Screening of staff for MRSA will only be undertaken if there is unexplained and persistent onwards transmission of MRSA within an area and all other active control measures have failed.The purpose of screening is to identify and eradicate any potential reservoir of MRSA which may be contributing to onwards transmission.
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 16 of 26

Staff screening will be initiated on the advice of the Infection Prevention Team and undertaken by the OHD, who will co-ordinate screening and subsequent management as required
Staff are reminded that it is a disciplinary offence to look up their own or other peoples screening results
Staff must not carry out their own screening as it can be difficult to distinguish between transient and persistent carriage.
6.13.4 Process:
The Infection Prevention Team will identify the extent and scope of screening. This will normally be limited to staff members involved in direct patient care
Staff will receive prior written notice of the intention to screen, along with a copy of the screening protocol which clearly identifies each stage of the process
Staff will be asked to undertake a short questionnaire to identify any skin lesions (eczema, psoriasis, dermatitis, paronychia etc.) or any recent courses of antibiotic treatment
All screens will be taken prior to the staff starting their shift and before any patient contact has occurred to minimise the risk of identifying transient carriage
Screening sites will depend on the epidemiology of the MRSA cases but will usually include specimens for the nasal passages, throat and any areas of broken skin (eczema, psoriasis, dermatitis etc).
6.13.5 Management of Colonised Staff Members Confirmed positive isolates from staff members will be managed confidentially through
the OHD. However, isolates will be sent for epidemiological typing via the microbiology department and individual case discussion may occur involving OHD, IPCT and Infection Control Doctor (ICD)
The action taken will depend upon the site of colonisation of MRSA and the clinical area and duties of the staff member
Colonised staff who are required to take time off work will be considered medically suspended and not on sick or annual leave. Treatment will be funded by Portsmouth Hospitals NHS Trust
6.13.6 Nasal Colonisation alone: Where nasal colonisation only is detected, staff members will be asked to undergo 5 days of topical treatment with nasal mupirocin (or equivalent) and Hibiscrub or Octenisan wash and will not be excluded from work.
6.13.7 Throat carriage: will initially be treated with antibacterial throat wash and dental gel (in conjunction with mupirocin and Hibiscrub or Octenisan) and staff members will not be excluded from work unless they have an active cough.
6.13.8 Colonised/Infected Lesions: Staff members with infected or colonised hand lesions, which render effective hand hygiene impossible, should be referred to OHD/dermatology, and should be off work or removed from clinical duties whilst receiving treatment. An individual risk assessment will be required for staff colonised with MRSA at other sites (e.g. local infections in non-exposed areas).
6.13.9 Subsequent Management: Colonised staff members will be re-screened for MRSA 2-7 days after treatment. If found
to be negative, 2 further screens, one week apart over a three week period will be obtained to ensure clearance. Successful clearance will be defined as 3 negative screens each taken one week apart. A routine follow up screen will be offered at 6 months to ensure persistent success
If initial decolonisation is unsuccessful, a second attempt will be made. In consultation with the ICD, regimes may be modified dependent on the site of colonisation and any
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 17 of 26

underlying medical conditions. This may involve usage of systemic (oral) antibiotics and involvement of other specialists
Persistently colonised staff members will be managed on a case by case basis. A multi-disciplinary team consisting of OHD, the IPCT & ICD and HR will undertake an assessment of risk of transmission to patients cared for by the staff member. Whilst every effort will be made to support the staff member to continue practicing in their current role, patient safety is paramount and consequently it may be necessary to make appropriate adjustments to the role of the staff member. As a last resort, in the unlikely event of persistent colonisation at a site posing a significant risk of ongoing transmission of infection to patients, re-deployment of the staff member may be considered in consultation with senior line management via existing Trust HR frameworks
6.13.10 Health & Safety:If a staff member is sent off work because of an MRSA infection likely to have been acquired at work, the incident needs to be reported under RIDDOR (Reporting of Injuries, Diseases and Dangerous Occurrences Regulations, 1995). This should be done in consultation with the OHD. Reporting is not required for colonisation.
7. TRAINING REQUIREMENTS
a. Clinical and non-clinical staff to receive practical hand hygiene training on induction and every 2 years thereafter (Infection Prevention Team)
b. Clinical and non-clinical staff to receive face-to-face induction training on aspects of infection prevention & MSSA/MRSA (Infection Prevention Team)
c. Update training to be delivered as part of Patient Safety & Quality Days, departmental and drop in days, Link Advisor days and Senior Doctors Training (Infection Prevention Team)
8. REFERENCES AND ASSOCIATED DOCUMENTATION
Centres for Disease Control and Prevention. Staphylococcus aureus resistant to vancomycin – United States, J Am Med Assoc 2002; 288: 824-825.
Cepeda JA, Whitehouse T, Cooper B, et al. Isolation of patients in single rooms or cohorts to reduce spread of MRSA in intensive-care units: prospective two centre study. Lancet 2005; 365: 295-304.
Coia, et al, Guidelines for the control and prevention of meticillin-resistant Staphylococcus aureus (MRSA) in healthcare facilities Journal of Hospital Infection, Volume 63, Supplement 1, May 2006, Pages1-44 The Joint Working Party of the British Society of Antimicrobial Chemotherapy, the Hospital Infection Society, and the Infection Control Nurses Association
Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, Duckworth G, Lai R, Ebrahim S. Isolation measures in the hospital management of methicillin resistant Staphylococcus aureus (MRSA): systematic review of the literature. BMJ 2004; 329:
Department of Health (2008) The Health and Social Care Act 2008: Code of Practice on the prevention and control of infections and related guidance. Department of Health, December 2010. London. HMSO
Geffers C, Farr BM. Risk of transmission of nosocomial methicillin-resistant Staphylococcus aureus (MRSA) from patients colonized with MRSA. Infect Control Hosp Epidemiol 2005; 26: 114-5.
Guidelines for the Treatment of Meticillin-Resistant Staphylococcus aureus (MRSA) In publication J Hosp Infect 2005
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 18 of 26

Guidelines for the Control and prevention of Meticillin-Resistant Staphylococcus aureus (MRSA) In publication J Hosp Infect 2005
Loveday et al (2014). epic3: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. Journal of Hospital Infection 86S1 (2014) S1–S70
National Institute for Health and Care Excellence. Infection prevention and control. Issued: April 2014 NICE quality standard 61
Salgado CD, Farr BM and Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis 2003; 36: 131-139.
9. EQUALITY IMPACT STATEMENTPortsmouth Hospitals NHS Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds.
This policy has been assessed accordingly
Our values are the core of what Portsmouth Hospitals NHS Trust is and what we cherish. They are beliefs that manifest in the behaviours our employees display in the workplace. Our Values were developed after listening to our staff. They bring the Trust closer to its vision to be the best hospital, providing the best care by the best people and ensure that our patients are at the centre of all we do.We are committed to promoting a culture founded on these values which form the ‘heart’ of our Trust:
Respect and dignityQuality of careWorking togetherEfficiency
This policy should be read and implemented with the Trust Values in mind at all times.
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 19 of 26

10.MONITORING COMPLIANCE WITH PROCEDURAL DOCUMENTS
This document will be monitored to ensure it is effective and to assurance compliance.
Minimum requirement to be
monitored
Lead Tool Frequency of Report of Compliance
Reporting arrangements Lead(s) for acting on Recommendations
Monthly reporting of MSSA and MRSA
bacteraemias (post 48 hours) to Trust
board
IPCT Trust Board Report
Monthly Policy audit report to: Trust Board, HoN, MM,
Consultants, Ward Managers, IPMC
C Mitchell, SLN
Weekly reporting of MSSA/MRSA
bacteraemias to divisions
IPCT Weekly CSC Infection Prevention Dashboard
Weekly Policy audit report to: HoN, MM, Consultants,
Ward Managers
SLN, MM, Consultants
Daily monitoring of MRSA acquisition and reporting via
SLE system
IPCT DATIX As required Policy audit report to: HoN, MM, Consultants,
Ward Managers
SLN, MM, Consultants, Ward Managers
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 20 of 26

Appendix 1
MRSA/MSSA Avoidance/Suppression Regime
Before you read this, you may find it helpful to read the booklet ‘MRSA - Wash it Away’ / ‘MRSA – Information for Patients in Hospital’ / MSSA – Patient Information
MRSA (Meticillin-Resistant Staphylococcus aureus) or MSSA (Meticillin-Sensitive Staphylococcus aureus)The hospital has confirmed that you have, or are higher risk of having MRSA or MSSA on your skin or up your nose. We have decided to treat this to reduce the risk of complications. This is known as suppression.Please read this sheet carefully and follow all of the instructions. If you need help to do this, please ask a nurse / carer / relative to assist you.
What should I do?You will be given a special soap to wash with and some nasal cream to put up your nose. You should use both for 5 days.
Wash all over with the special soap once a day for 5 days Put the cream up your nose 3 times a day for 5 days
What is the special soap?The special soap is called Hibiscrub. It is a pink, non-perfumed soap containing chlorhexidine. You should not use it if you have an allergy to chlorhexidine (alternatives are available). Hibiscrub should not be used on children.
How often should I use the special soap? You should wash your whole body using this special soap neat once a day for 5 days.
How do I use this special soap? You can use the special soap in the bath or shower Do not dilute the soap in water but use it neat on a washcloth Wet your face and body first, then wash all over, leaving the soap on your skin for at least 1 minute. Pay special attention to your face, armpits and groin but do not use inside the body. You should use a clean face cloth each day Wash you hair with the special soap on days 1 and 5 of treatment. You can use your normal shampoo/conditioner in between
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 21 of 26

Clean towels and fresh clothes should be used after washing. Bed sheets, pillows and nightclothes should be changed daily
What is the ointment that I put up my nose?The ointment is called Mupirocin (Bactroban®). It is an antibiotic ointment. It does not contain penicillin. You should not use the ointment if you are allergic to Mupirocin or paraffin cream.
How do I use this ointment?Using a clean finger, you should wipe a pea-sized amount of ointment around the inside of each nostril and squeeze your nose. You should be able to taste the ointment in the back of your throat when you have finished. If you cannot, you should apply a small amount of extra cream. You must wash your hands after this.
How often should I put the ointment up my nose? You should put the ointment up your nose three times a day for 5 days.
Are there any risks to me?The ointment sometimes causes irritation to the skin in your nose. If this happens, stop using the ointment and talk to a member of staff.
After 5 days, your treatment is complete. You should not use the nasal cream for longer than this time. You can continue to use the special soap if you wish to. Unless you remain in hospital we will not routinely re-swab you for MRSA.
Further Information:
Infection Prevention & Control Department – Portsmouth Hospitals NHS Trust
telephone 02392 286000 x6261
Public Health England:https://www.gov.uk/government/organisations/public-health-england
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 22 of 26

Appendix 2
MRSA/MSSA Avoidance/Suppression Regime
Before you read this, you may find it helpful to read the booklet ‘MRSA - Wash it Away’ / ‘MRSA – Information for Patients in Hospital’ / MSSA – Patient Information
MRSA (Meticillin-Resistant Staphylococcus aureus) or MSSA (Meticillin-Sensitive Staphylococcus aureus)The hospital has confirmed that you have, or are higher risk of having MRSA or MSSA on your skin or up your nose. We have decided to treat this to reduce the risk of complications. This is known as suppression.Please read this sheet carefully and follow all of the instructions. If you need help to do this, please ask a nurse / carer / relative to assist you.
What should I do?You will be given a special soap to wash with and some nasal cream to put up your nose. You should use both for 5 days.
Wash all over with the special soap once a day for 5 days Put the cream up your nose 3 times a day for 5 days
What is the special soap?The special soap is called Octenisan. It is a clear, non-perfumed soap and comes in a 150ml bottle. It can be used even if you have dry skin, eczema or psoriasis.
How often should I use the special soap? You should wash your whole body using this special soap neat once a day for 5 days.
How do I use this special soap? You can use the special soap in the bath or shower Do not dilute the soap in water but use it neat on a washcloth Wet your face and body first, then wash all over, leaving the soap on your skin for at least 1 minute. Pay special attention to your face, armpits and groin but do not use inside the body. You should use a clean face cloth each day
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 23 of 26

Wash you hair with the special soap on days 1 and 5 of treatment. You can use your normal shampoo/conditioner in between Clean towels and fresh clothes should be used after washing. Bed sheets, pillows and nightclothes should be changed daily
What is the ointment that I put up my nose?The ointment is called Mupirocin (Bactroban®). It is an antibiotic ointment. It does not contain penicillin. You should not use the ointment if you are allergic to Mupirocin or paraffin cream.
How do I use this ointment?Using a clean finger, you should wipe a pea-sized amount of ointment around the inside of each nostril and squeeze your nose. You should be able to taste the ointment in the back of your throat when you have finished. If you cannot, you should apply a small amount of extra cream. You must wash your hands after this.
How often should I put the ointment up my nose? You should put the ointment up your nose three times a day for 5 days.
Are there any risks to me?The ointment sometimes causes irritation to the skin in your nose. If this happens, stop using the ointment and talk to a member of staff.
After 5 days, your treatment is complete. You should not use the nasal cream for longer than this time. You can continue to use the special soap if you wish to. Unless you remain in hospital we will not routinely re-swab you for MRSA.
Further Information:
Infection Prevention & Control Department – Portsmouth Hospitals NHS Trust
telephone 02392 286000 x6261
Public Health England:https://www.gov.uk/government/organisations/public-health-england
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 24 of 26

EQUALITY IMPACT SCREENING TOOLTo be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval for service and policy changes/amendments.
Stage 1 - Screening
Title of Procedural Document: Staphylococcus aureus (MRSA and MSSA) Management Policy
Date of assessment 10/06/2019 Responsible Department
Infection Prevention
Name of person completing assessment
Kathryn Noble Job Title Infection Prevention Manager/Analyst
Does the policy/function affect one group less or more favourably than another on the basis of :
Yes/No Comments
Age No
DisabilityLearning disability; physical disability; sensory impairment and/or mental health problems e.g. dementia
No
Ethnic Origin (including gypsies and travellers) No
Gender reassignment No
Pregnancy or Maternity No
Race No
Sex No
Religion and Belief No
Sexual Orientation No
If the answer to any of the above questions is NO, the EIA is complete. If YES, a full impact assessment is required: go on to stage 2, page 2
More Information can be found be following the link below
www.legislation.gov.uk/ukpga/2010/15/contents
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 25 of 26

Stage 2 – Full Impact Assessment
What is the impact Level of Impact
Mitigating Actions(what needs to be done to minimise /
remove the impact)
Responsible Officer
Monitoring of Actions
The monitoring of actions to mitigate any impact will be undertaken at the appropriate level
Specialty Procedural Document: Specialty Governance CommitteeClinical Service Centre Procedural Document: Clinical Service Centre Governance CommitteeCorporate Procedural Document: Relevant Corporate Committee
All actions will be further monitored as part of reporting schedule to the Equality and Diversity Committee
Staphylococcus aureus (MSSA, MRSA) Management PolicyVersion: 12Issue Date: 12 June 2019Review date: 11 June 2021 (unless requirements change) Page 26 of 26