Question of Quality Conference 2016 - Jonathan B. Perlin
21
2/29/16 1 Learning Healthcare & Clinical Leadership in an Accountable Environment Jonathan B. Perlin, MD, PhD, MSHA, MACP, FACMI President, Clinical Services Group and Chief Medical Officer HCA / Hospital Corporation of America Chair, American Hospital Association, 2015 Clinical Professor of Medicine & Biomedical Informatics, Vanderbilt University Adjunct Professor of Health Administration, Virginia Commonwealth University Contact: [email protected] It’s a Question of Quality Conference London, England– February 25, 2016 1. US: Accountability, Transparency and Health IT 2. Transformation: Case-Studies from HCA US – Learning & Improving at-Scale: The REDUCE MRSA Trial – Clinical Leadership: Billion-Dollar Babies 3. Harvesting the (Big) “Data-Dividend” Overview
-
Upload
hca-healthcare-uk -
Category
Healthcare
-
view
158 -
download
2
Transcript of Question of Quality Conference 2016 - Jonathan B. Perlin
2/29/16
1
Learning Healthcare & Clinical Leadership in an Accountable Environment
Jonathan B. Perlin, MD, PhD, MSHA, MACP, FACMI
President, Clinical Services Group and Chief Medical Officer HCA / Hospital Corporation of America
Chair, American Hospital Association, 2015 Clinical Professor of Medicine & Biomedical Informatics, Vanderbilt University Adjunct Professor of Health Administration, Virginia Commonwealth University
Contact: [email protected]
It’s a Question of Quality Conference
London, England– February 25, 2016
1. US: Accountability, Transparency and Health IT
2. Transformation: Case-Studies from HCA US – Learning & Improving at-Scale: The REDUCE MRSA Trial
– Clinical Leadership: Billion-Dollar Babies
3. Harvesting the (Big) “Data-Dividend”
Overview
2/29/16
2
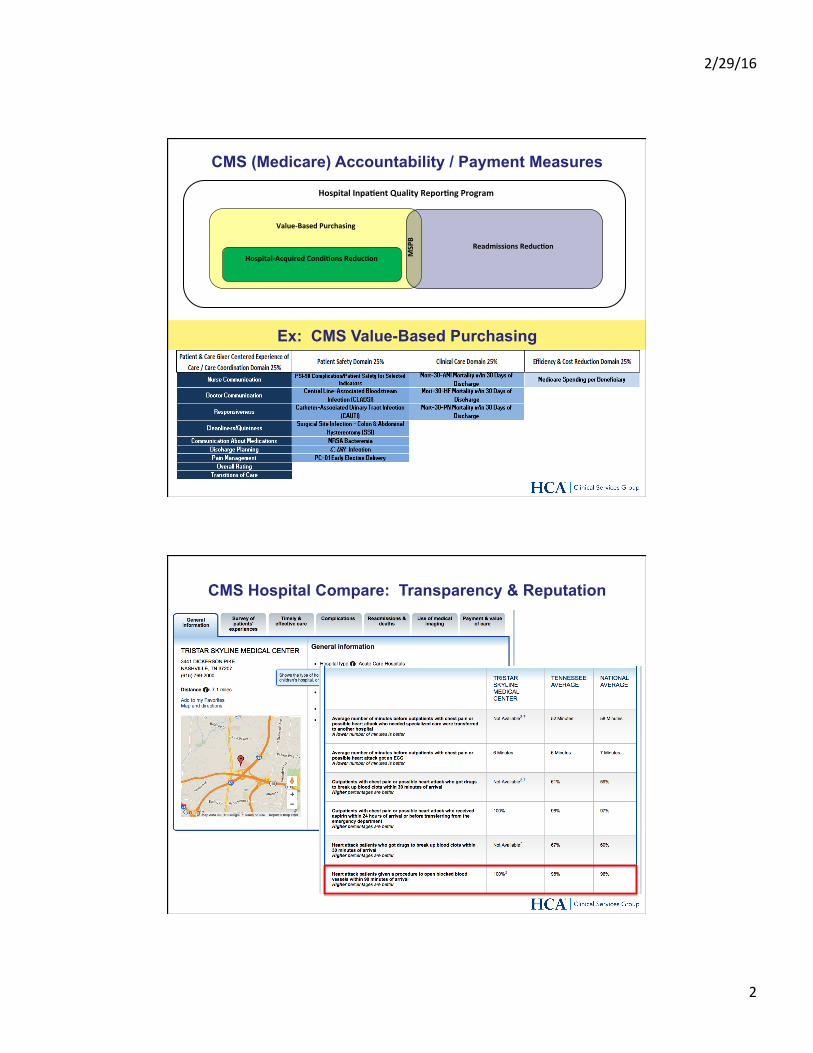
CMS (Medicare) Accountability / Payment Measures
Value-BasedPurchasing
Hospital-AcquiredCondi9onsReduc9onReadmissionsReduc9on
MSPB
HospitalInpa9entQualityRepor9ngProgram
Ex: CMS Value-Based Purchasing
CMS Hospital Compare: Transparency & Reputation
2/29/16
3
• Numerous organizations issue reports ranking and rating hospitals. • Use CMS and proprietary data • Issue reports, provide websites, offer recognition • Some provide a forum for customer/patient reviews • Some are “pay to play”
• Organizational missions include: • Consumer advocacy • Consumer education • Purchaser decision-making • Product sales • Consulting services sales
Third-Party Assessments
L
Third-Party Assessments
Transparency has driven better performance . . . and confusion!
Organizational Responses: - Learning - Celebrating Success
2/29/16
4
BREAKING: CMS and health insurers unveil first set of standardized quality measures By Melanie Evans | February 16, 2016
The CMS and America's Health Insurance Plans, health plans' trade group, announced a new agreement to standardize measures of quality for the nation's doctors. Officials say the measures are necessary as payers and consumers seek to shop for high-quality care.
The agreement—which outlines seven sets of quality measures to be used across public and private payers—is the first to be announced by the Core Quality Measures Collaborative, which includes the CMS, AHIP, the American Academy of Family Physicians and the National Partnership for Women and Families. The National Quality Forum, an endorsement body for industry quality standards, was a technical adviser.
The announcement comes as industry stakeholders and policymakers struggle with how best to identify and reward high-quality healthcare. Measures of quality are increasingly tied to how much doctors and hospitals are paid and HHS said that by 2018 half of Medicare spending outside of managed care would be under contracts with rewards and potential penalties for quality. . .
Tuesday, February 16, 2016
MU is a Programme in the “HITECH” (Health Information Technology for Economic & Clinical Health) of ARRA:
• An “Interstate Highway Program” for Health Information Technology – Envisioned Interoperable Electronic Health Records
• Offered Incentives to Eligible Hospitals & Providers (Doctors) to adopt Electronic Health Records over a rolling four year period to end NLT 2017 – Over $30 BILLION in incentives have been distributed – BTW, Hospitals not achieving MU would ultimately
experience (incapacitating) payment penalties
Health IT: The “Meaningful Use” (MU) Programme
2/29/16
5
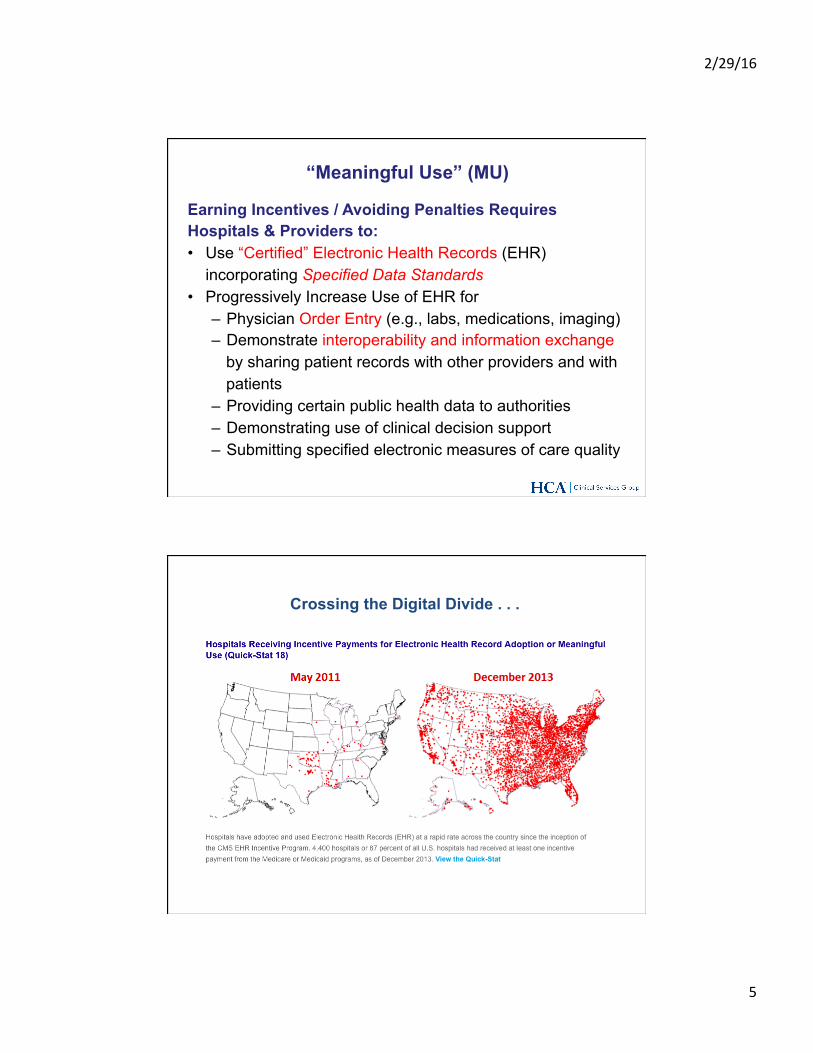
Earning Incentives / Avoiding Penalties Requires Hospitals & Providers to:
• Use “Certified” Electronic Health Records (EHR) incorporating Specified Data Standards
• Progressively Increase Use of EHR for – Physician Order Entry (e.g., labs, medications, imaging) – Demonstrate interoperability and information exchange
by sharing patient records with other providers and with patients
– Providing certain public health data to authorities – Demonstrating use of clinical decision support – Submitting specified electronic measures of care quality
“Meaningful Use” (MU)
Crossing the Digital Divide . . .
2/29/16
6
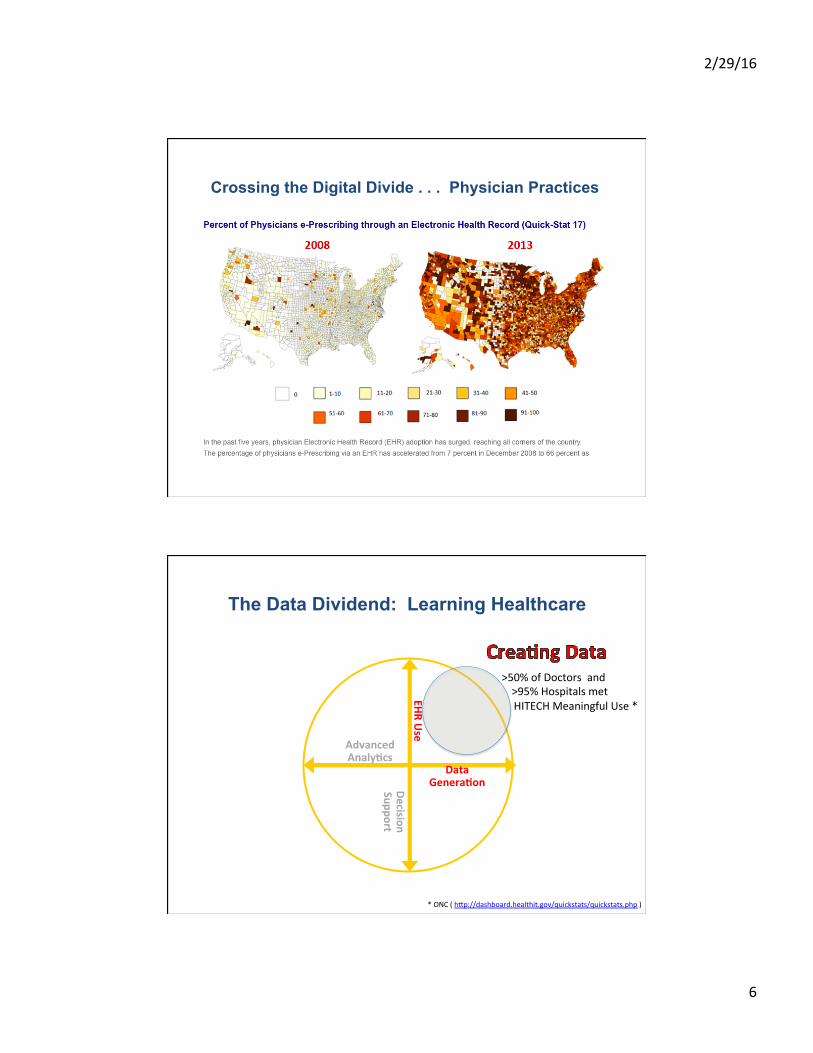
Crossing the Digital Divide . . . Physician Practices
The Data Dividend: Learning Healthcare
EHRUse
DecisionSupport
DataGenera9on
AdvancedAnaly9cs
>50%ofDoctorsand>95%Hospitalsmet
HITECHMeaningfulUse*
*ONC(hKp://dashboard.healthit.gov/quickstats/quickstats.php)
2/29/16
7
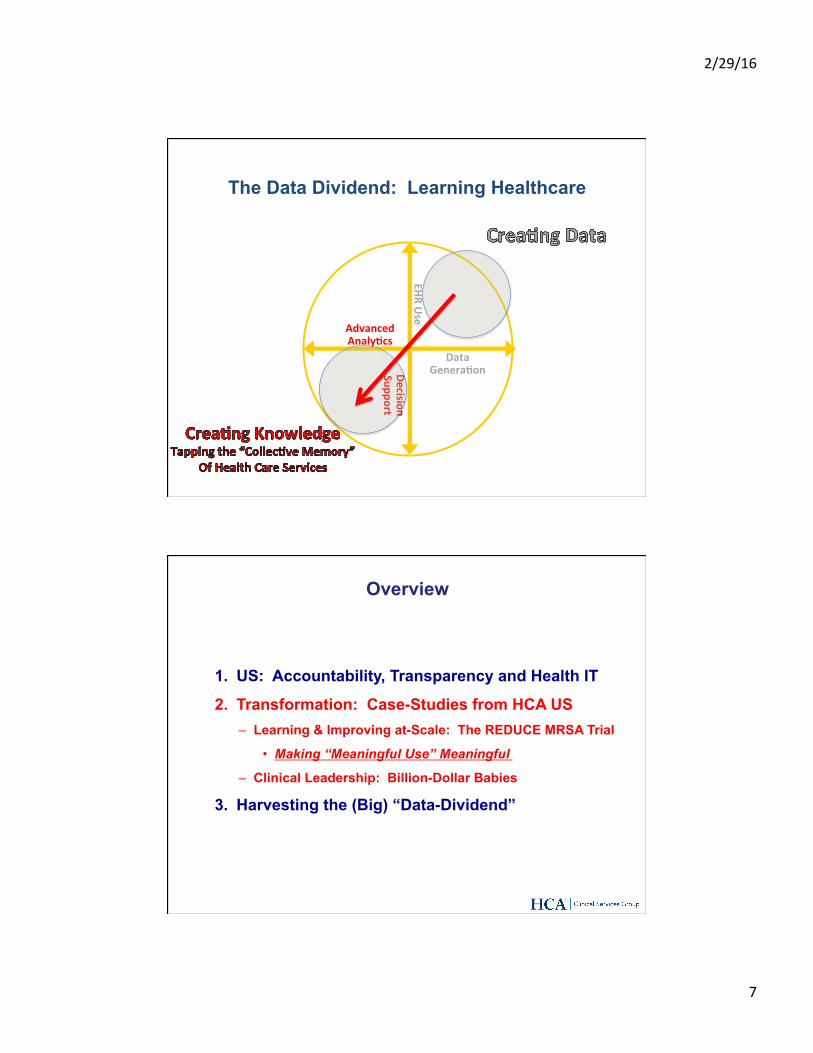
EHRUse
DecisionSupport
DataGenera9on
AdvancedAnaly9cs
The Data Dividend: Learning Healthcare
1. US: Accountability, Transparency and Health IT
2. Transformation: Case-Studies from HCA US – Learning & Improving at-Scale: The REDUCE MRSA Trial
• Making “Meaningful Use” Meaningful
– Clinical Leadership: Billion-Dollar Babies
3. Harvesting the (Big) “Data-Dividend”
Overview
2/29/16
8
Addressing a Significant Problem:
• In the United States, ~ 1 in 20 patients hospitalized will develop a healthcare-associated infection (HAIs)
~ 1.9 – 2.1 million patients infected ~ 80,000 die ~ $20- 30 billion avoidable healthcare expenditures
• Methicillin-resistant Staphylococcus aureus (MRSA), and other Staphylococcus aureus, account for approximately 25% of all deaths from HAIs
The REDUCE MRSA Trial – Background
*Updatedfrom:KlevinsRMetal,PubHlthRep,2007;122:160-6.
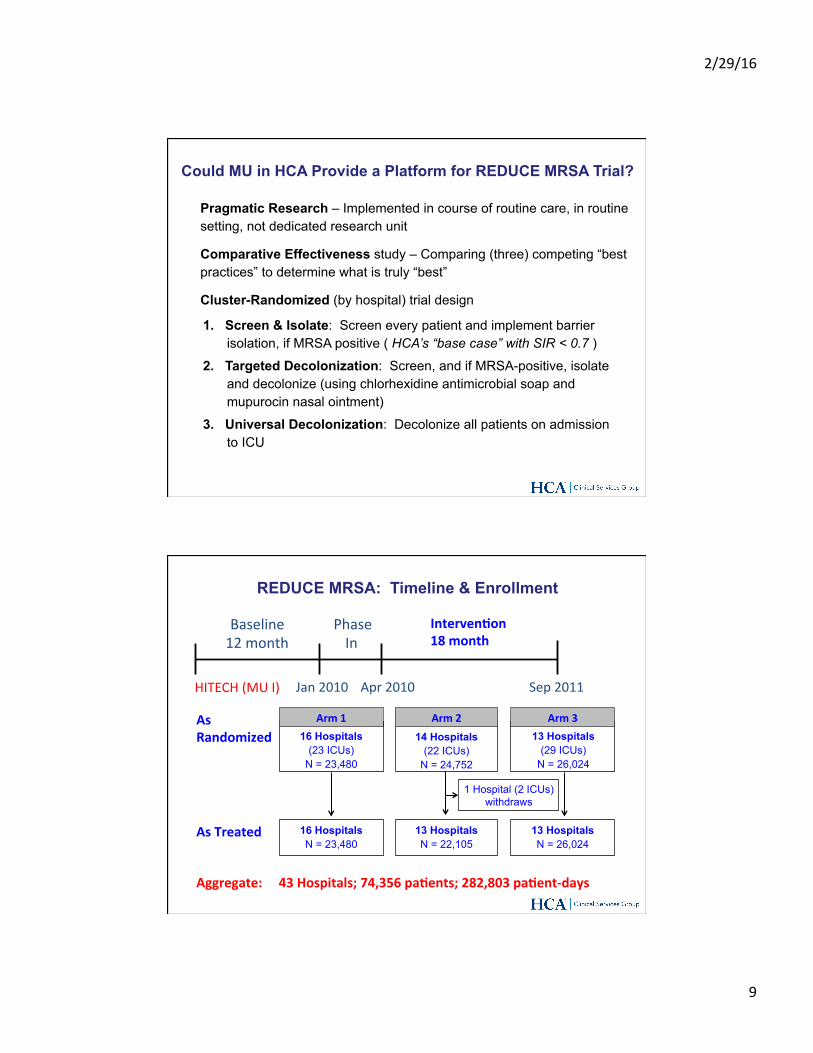
What Might be Learned Across a Large Health System ?
InternaZonalAnchorage
NWGA
NortheastC
TerreHaute
IdahoFalls
ColumbusAtlantaPanhandle**
Orleans
IdahoFalls
Tallahassee
WW
W
LasVegasWW
SanJoseW
WesternIdaho
Utah
SouthernCalifornia
Utah
W
Denver
W
WSanAntonioAusZnDallas/FW
Houston
KansasCity
OklahomaCity
WW
CorpusChrisZ
Brownsville
W
Wichita
W
W
SanAntonioAusZn
Dallas/FtW
Wichita
ElPaso
New
CentralLouisiana
LafayeKe
C No.VA
CRichmondC
SWVACFrankfortC SWVAFrankfortFrankfort
Tampa
NorthCentralFlorida
TreasureCoast
EE
PalmBeach
DadeBroward
JacksonvilleColumbus
Panhandle
TerreHaute
MiddleGATrident/Charleston
GrandStrandAugustaChaKanooga
SWVA
AmericanGroup
NaZonalGroup
CentralLondon
WesternIdaho
SanJose
Houston
KansasCity
NWGAAtlanta
OklahomaCityNashville
25millionpa9entcontactsannuallyApproximately5%ofmajorhospitalservicesinU.S.:
• Admissions >1.6million• PaZentDays >7.6million• Deliveries >0.25million• TotalSurgeries >1.3million• EDVisits >8million
Ø 170Hospitals,120FreestandingSurgery
Centers,>850PhysicianPracZces,>200UrgentCareCentersin23statesandLondon
Ø HospitalsrangefromcomplexterZaryreferral
andacademicmedicalcenterstourbanandsuburbancommunitymedicalcenters
Ø ~215,000employees,including~72,000nursesand30,000alliedhealthprofessionals
Ø >50,000affiliatedphysicians,including>3,300employedphysiciansandpracZZoners
Ø Morethan38,000licensedbeds
2/29/16
9
Pragmatic Research – Implemented in course of routine care, in routine setting, not dedicated research unit
Comparative Effectiveness study – Comparing (three) competing “best practices” to determine what is truly “best”
Cluster-Randomized (by hospital) trial design
1. Screen & Isolate: Screen every patient and implement barrier isolation, if MRSA positive ( HCA’s “base case” with SIR < 0.7 )
2. Targeted Decolonization: Screen, and if MRSA-positive, isolate and decolonize (using chlorhexidine antimicrobial soap and mupurocin nasal ointment)
3. Universal Decolonization: Decolonize all patients on admission to ICU
Could MU in HCA Provide a Platform for REDUCE MRSA Trial?
Aggregate:43Hospitals;74,356pa9ents;282,803pa9ent-days
Arm116 Hospitals
(23 ICUs) N = 23,480
Arm214 Hospitals
(22 ICUs) N = 24,752
Arm313 Hospitals
(29 ICUs) N = 26,024
16 Hospitals N = 23,480
13 Hospitals N = 22,105
13 Hospitals N = 26,024
1 Hospital (2 ICUs) withdraws
AsRandomized
AsTreated
REDUCE MRSA: Timeline & Enrollment
Jan2010 Apr2010 Sep2011
Baseline12month
PhaseIn
Interven9on18month
HITECH(MUI)
2/29/16
10
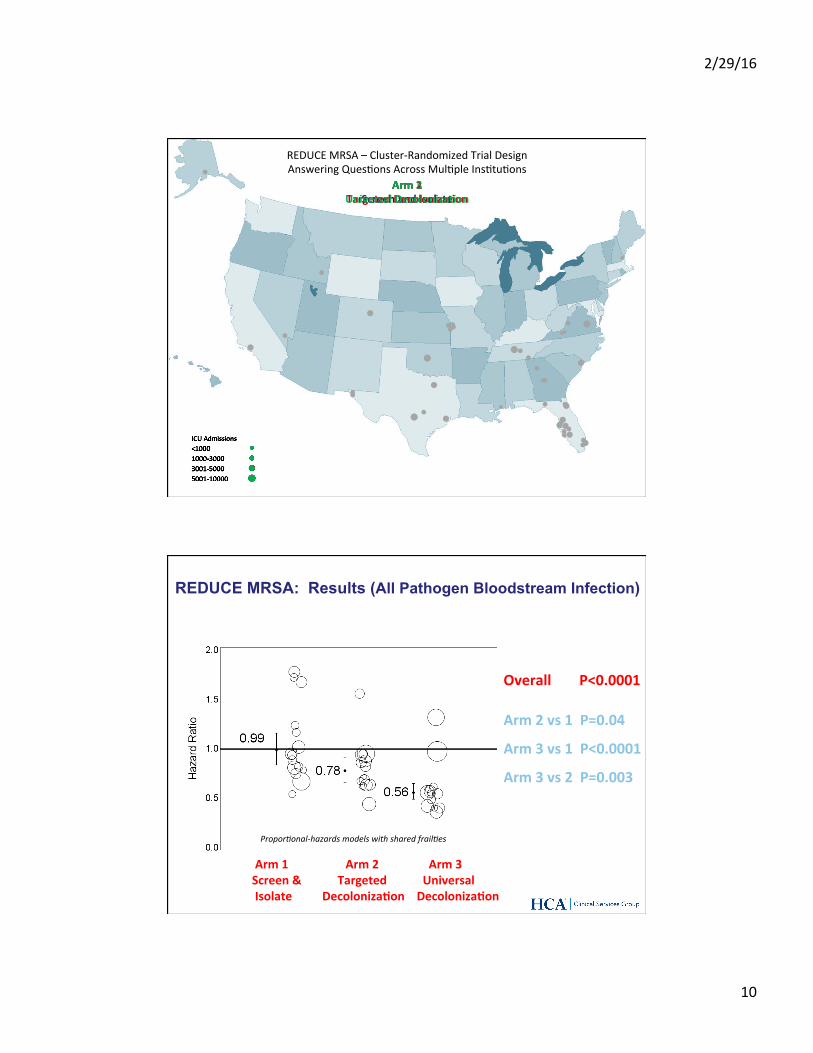
REDUCEMRSA–Cluster-RandomizedTrialDesignAnsweringQuesZonsAcrossMulZpleInsZtuZons
Arm1ScreenandIsolate
Arm2TargetedDecoloniza9on
Arm3UniversalDecoloniza9on
OverallP<0.0001
Arm1Arm2 Arm3Screen&Targeted UniversalIsolateDecoloniza9onDecoloniza9on
Arm2vs1P=0.04
Arm3vs1P<0.0001
Arm3vs2P=0.003
REDUCE MRSA: Results (All Pathogen Bloodstream Infection)
Propor3onal-hazardsmodelswithsharedfrail3es
2/29/16
11
Decolonization reduces all blood stream infections (BSIs) by 44% and MRSA by 37%
• For every 99 patients decolonized, 1 BSI was avoided • Set a new standard for reducing BSIs in ICUs • Policy: Demonstrated that (9) state-mandated
screening were expensive and inappropriate
REDUCE MRSA: Study Findings
• Agency for Healthcare Research and Quality
• CDC Prevention Epicenters Steering Committee
• Harvard Pilgrim Health Care Institute / Harvard Medical School
• Hospital Corporation of America • Rush University • University of California Irvine
REDUCE MRSA: Discussion Fostering a Learning Health System
• REDUCE MRSA notable not only for its outcomes, but
for its methods: • Speed: Did not take one hospital 64 years to amass the
power of the study – it took 43 hospitals 18 months • Implementation: Not conducted by a single-purpose research
team, but by nurses and infection prevention professionals during routing patient care
• Setting: Did not occur in a controlled research unit, but within community hospitals across the country, embedded in routine care . . .
• Because of interoperable health information, REDUCE MRSA efficiently answered real-world questions, in real-world environments, that generalize to real-world situations
2/29/16
12
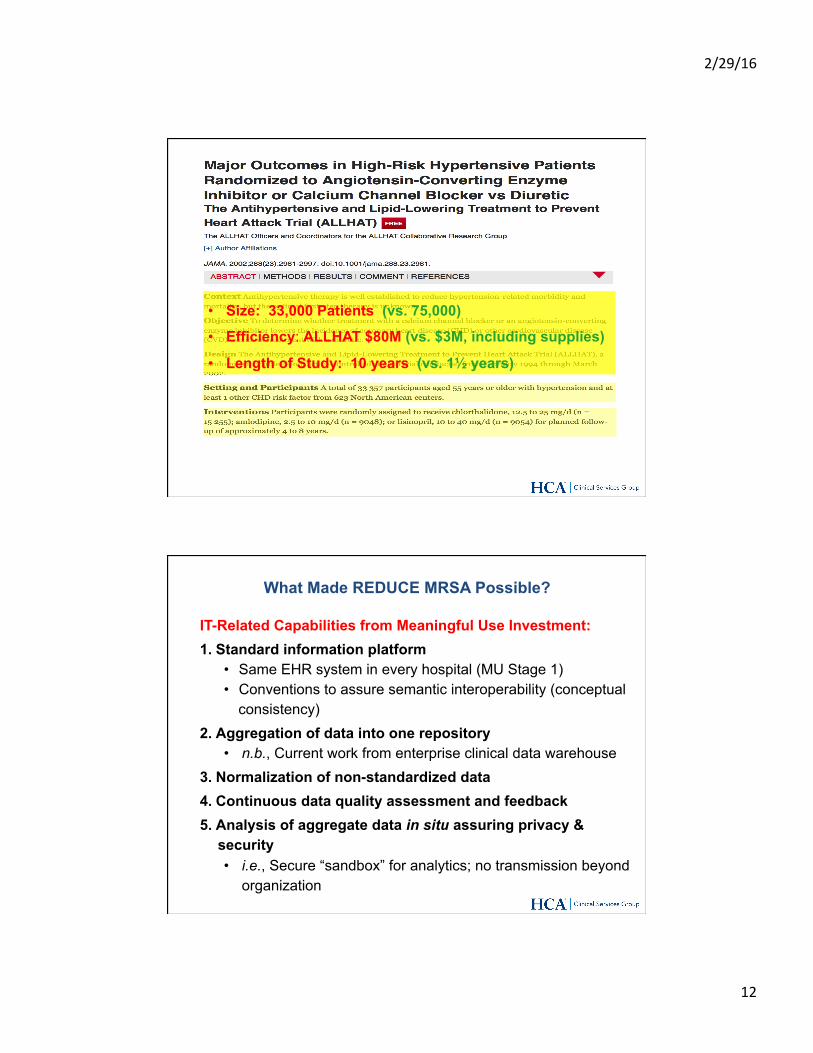
• Size: 33,000 Patients (vs. 75,000)
• Efficiency: ALLHAT $80M (vs. $3M, including supplies)
• Length of Study: 10 years (vs. 1½ years)
IT-Related Capabilities from Meaningful Use Investment: 1. Standard information platform
• Same EHR system in every hospital (MU Stage 1) • Conventions to assure semantic interoperability (conceptual
consistency) 2. Aggregation of data into one repository
• n.b., Current work from enterprise clinical data warehouse 3. Normalization of non-standardized data 4. Continuous data quality assessment and feedback 5. Analysis of aggregate data in situ assuring privacy &
security • i.e., Secure “sandbox” for analytics; no transmission beyond
organization
What Made REDUCE MRSA Possible?
2/29/16
13
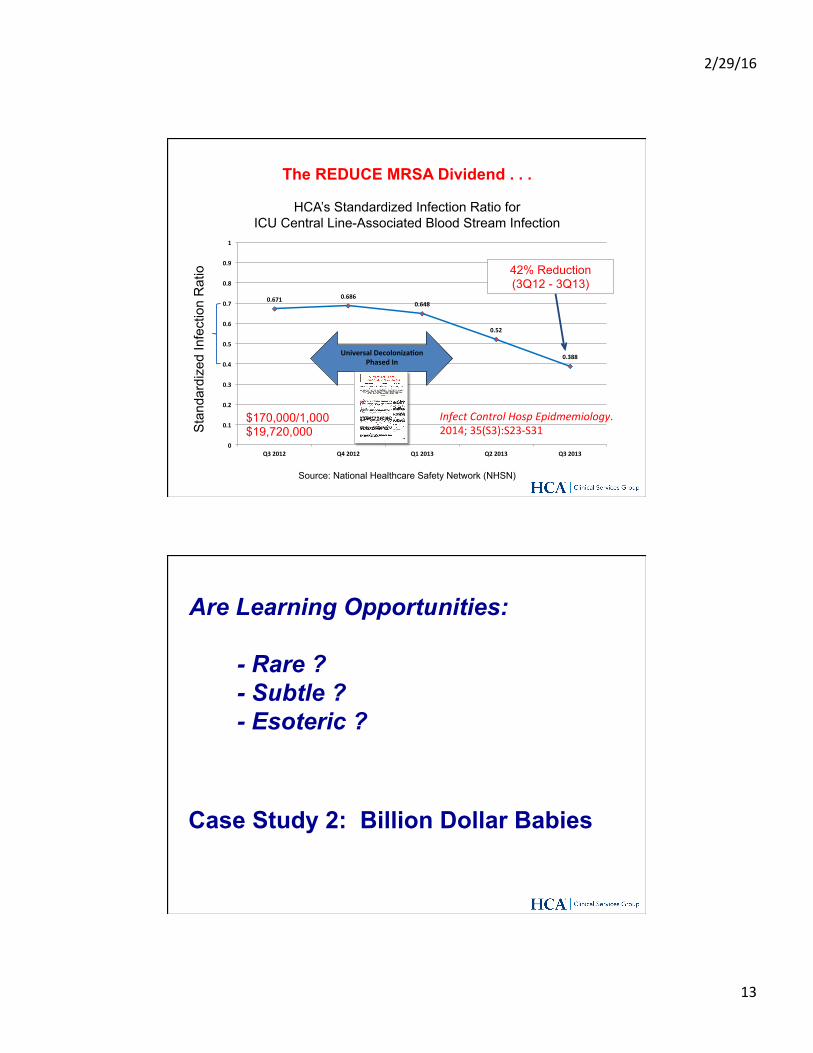
0.671 0.6860.648
0.52
0.388
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Q32012 Q42012 Q12013 Q22013 Q32013
UniversalDecoloniza9onPhasedIn
42% Reduction (3Q12 - 3Q13)
Sta
ndar
dize
d In
fect
ion
Rat
io
Source: National Healthcare Safety Network (NHSN)
HCA’s Standardized Infection Ratio for ICU Central Line-Associated Blood Stream Infection
$170,000/1,000 $19,720,000
InfectControlHospEpidmemiology.2014;35(S3):S23-S31
The REDUCE MRSA Dividend . . .
Are Learning Opportunities: - Rare ?
- Subtle ? - Esoteric ?
Case Study 2: Billion Dollar Babies
2/29/16
14
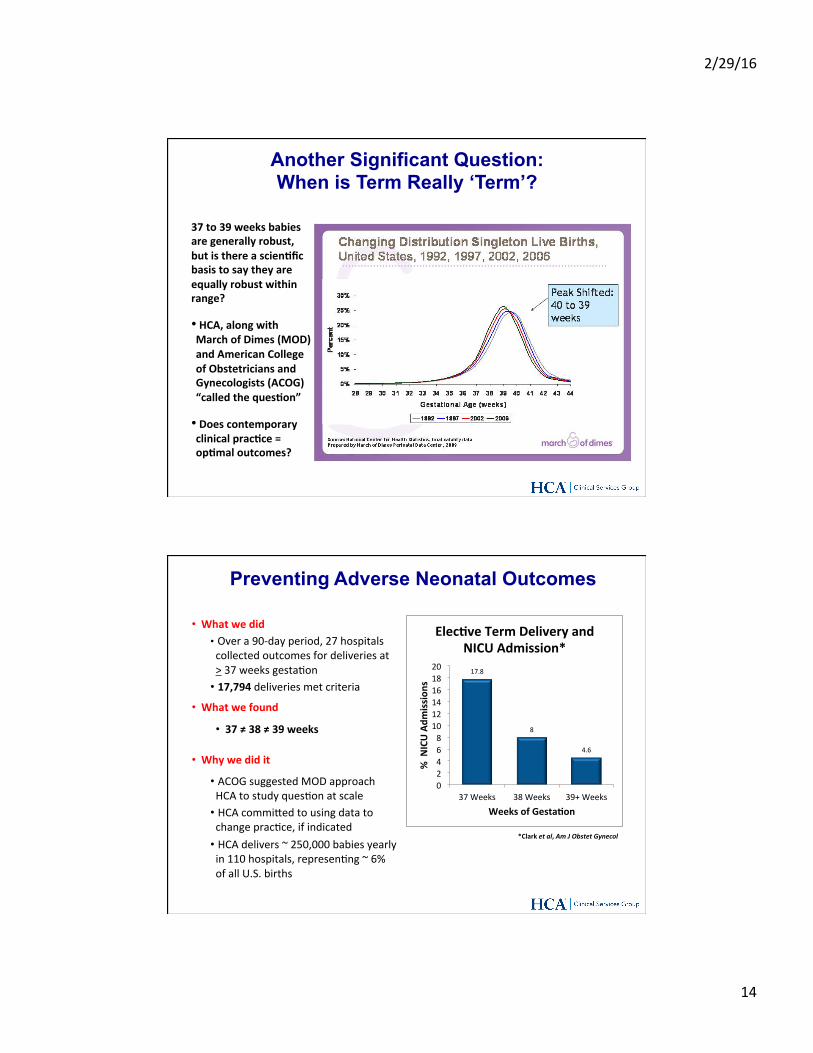
Another Significant Question: When is Term Really ‘Term’?
37to39weeksbabiesaregenerallyrobust,butisthereascien9ficbasistosaytheyareequallyrobustwithinrange?
• HCA,alongwithMarchofDimes(MOD)andAmericanCollegeofObstetriciansandGynecologists(ACOG)“calledtheques9on”
• Doescontemporaryclinicalprac9ce=op9maloutcomes?
• Whatwedid• Overa90-dayperiod,27hospitalscollectedoutcomesfordeliveriesat>37weeksgestaZon
• 17,794deliveriesmetcriteria
• Whatwefound
• 37≠38≠39weeks
• Whywedidit
• ACOGsuggestedMODapproachHCAtostudyquesZonatscale
• HCAcommiKedtousingdatatochangepracZce,ifindicated
• HCAdelivers~250,000babiesyearlyin110hospitals,represenZng~6%ofallU.S.births
*Clarketal,AmJObstetGynecol
17.8
8
4.6
02468101214161820
37Weeks 38Weeks 39+Weeks
%N
ICUAdm
ission
s
WeeksofGesta9on
Elec9veTermDeliveryandNICUAdmission*
PreventingAdverse Neonatal Outcomes
2/29/16
15
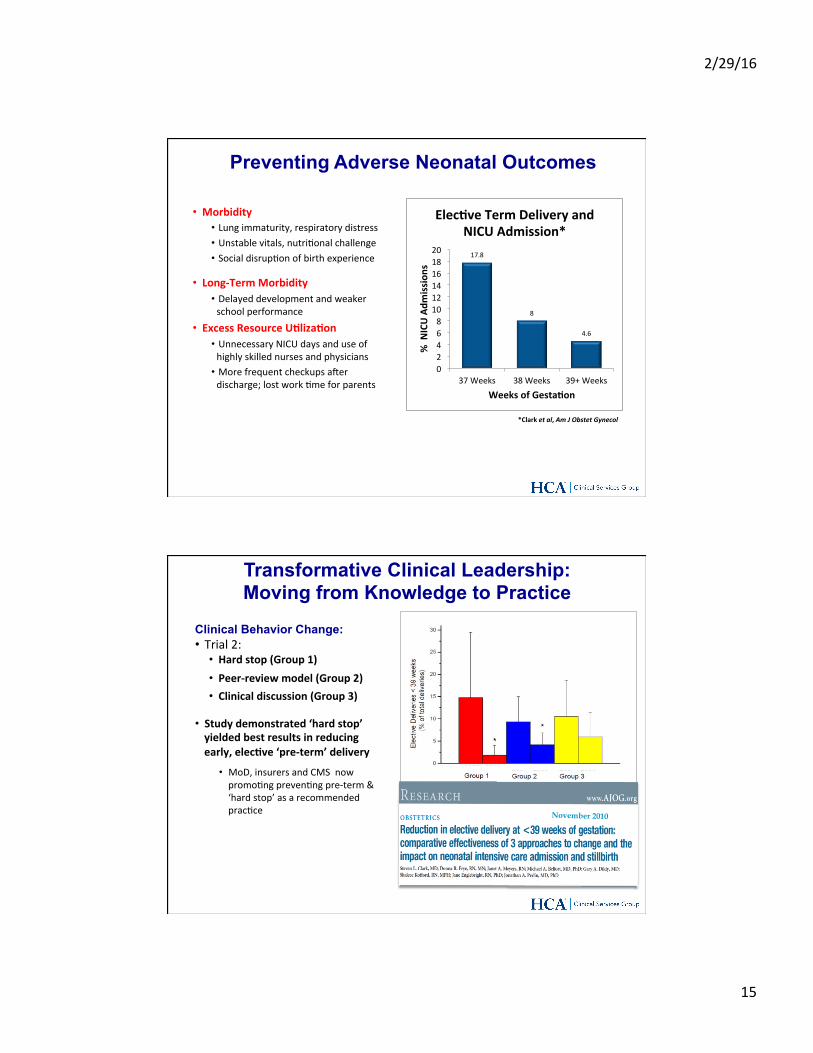
• Morbidity• Lungimmaturity,respiratorydistress• Unstablevitals,nutriZonalchallenge• SocialdisrupZonofbirthexperience
• Long-TermMorbidity• Delayeddevelopmentandweakerschoolperformance
• ExcessResourceU9liza9on• UnnecessaryNICUdaysanduseofhighlyskillednursesandphysicians
• Morefrequentcheckupsamerdischarge;lostworkZmeforparents
17.8
8
4.6
02468101214161820
37Weeks 38Weeks 39+Weeks
%N
ICUAdm
ission
s
WeeksofGesta9on
Elec9veTermDeliveryandNICUAdmission*
*Clarketal,AmJObstetGynecol
PreventingAdverse Neonatal Outcomes
Clinical Behavior Change:• Trial2:
• Hardstop(Group1)• Peer-reviewmodel(Group2)• Clinicaldiscussion(Group3)
• Studydemonstrated‘hardstop’yieldedbestresultsinreducingearly,elec9ve‘pre-term’delivery
• MoD,insurersandCMSnowpromoZngprevenZngpre-term&‘hardstop’asarecommendedpracZce
Transformative Clinical Leadership: Moving from Knowledge to Practice
*Clarketal,AmJObstetGynecol,2010
November 2010
2/29/16
16
Learning opportunities are ubiquitous
Organizational learning has to be intentional • EHR’s don’t yet automate “pattern recognition” (i.e., relationship
between gestational age, complications, type of complications and cost of potentially avoidable services)
Organizational improvement also has to be intentional • Must obligate to using evidence
Clinical behavior change requires clinical leadership • Compelling data change discussion from religion to evidence
Learning / Improvement Opportunities
1. US: Accountability, Transparency and Health IT
2. Transformation: Case-Studies from HCA US – Learning & Improving at-Scale: The REDUCE MRSA Trial
– Clinical Leadership: Billion-Dollar Babies
3. Harvesting the (Big) “Data-Dividend”
Overview

2/29/16
17
What if the results of REDUCE MRSA (of the strategies compared) were already present in data generated by previous care?
• What if trials could have been performed “in silica?” • In 18 minutes, not 18 months ? (REDUCE) • In 9 minutes, not 90 days ? (Pre-term delivery)
What other answers to pressing questions (cost, quality, precision medicine, policy) might exist in the “collective memory” of our healthcare services?
How do we harvest the “Data Dividend?”?
What If REDUCE MRSA Didn’t Require 18 Months?
34
Data sizes: US Library of Congress printed material: 10 Tb HCA: 120 Petabytes (12,000 Libraries of Congress) Google: Best Guess 15 Exabytes (1.5million Libraries of Congress, 100x HCA) Planet volumes: Moon: 2.2E-2 Jupiter: 1.4e3 (63,000 moons) Sun 1.4E6 (63 million moons) Units: Extabyte: 10^18 bytes Petabyte: 10^15 bytes Terrabyte: 10^12 bytes Gigabye: 10^9 bytes Note that the Library of Congress has at least 3 petabytes of digital content
What Could be Learned from the “Digital Dividend?”
2/29/16
18
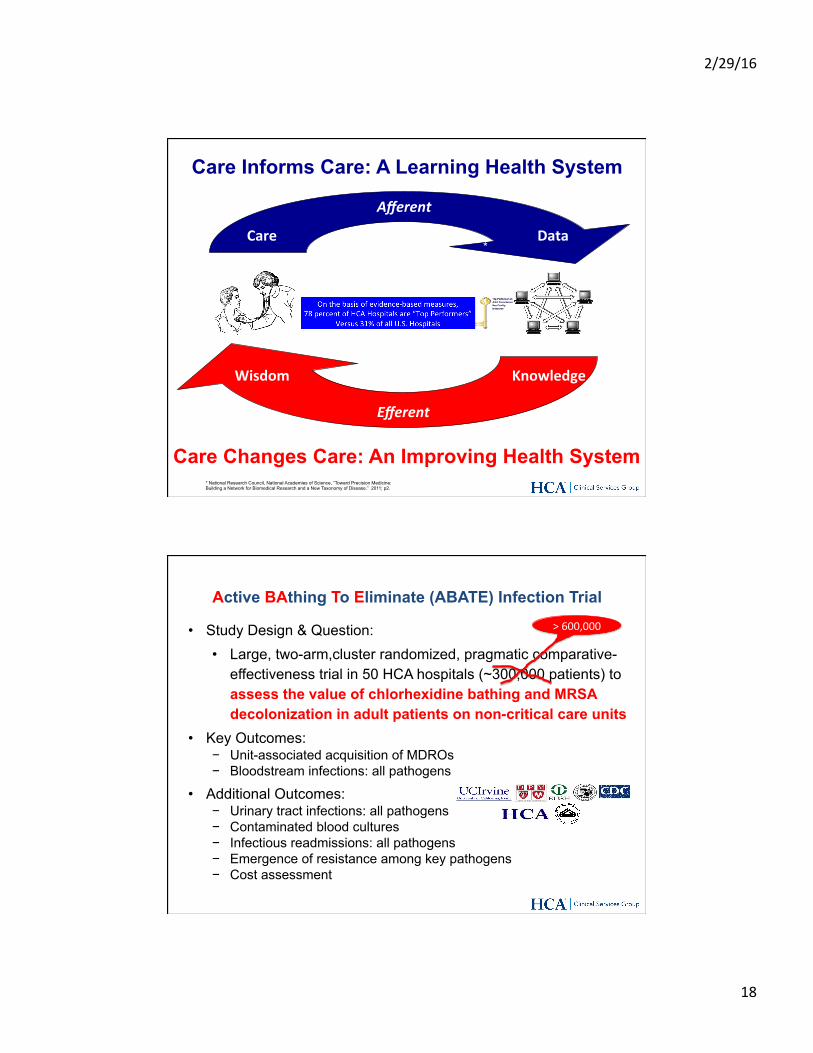
Care Informs Care: A Learning Health System
* National Research Council, National Academies of Science, “Toward Precision Medicine: Building a Network for Biomedical Research and a New Taxonomy of Disease.” 2011; p2.
*
Knowledge
Care Data
Wisdom
Care Changes Care: An Improving Health System
Afferent
Efferent
• Study Design & Question: • Large, two-arm,cluster randomized, pragmatic comparative-
effectiveness trial in 50 HCA hospitals (~300,000 patients) to assess the value of chlorhexidine bathing and MRSA decolonization in adult patients on non-critical care units
• Key Outcomes: − Unit-associated acquisition of MDROs − Bloodstream infections: all pathogens
• Additional Outcomes: − Urinary tract infections: all pathogens − Contaminated blood cultures − Infectious readmissions: all pathogens − Emergence of resistance among key pathogens − Cost assessment
Active BAthing To Eliminate (ABATE) Infection Trial >600,000
2/29/16
19
The “Data Dividend” . . . a Learning & Improvement Engine
The Full Dividend of Transparency, Accountability & Clinical Leadership:
A “Learning Health System”
2/29/16
20
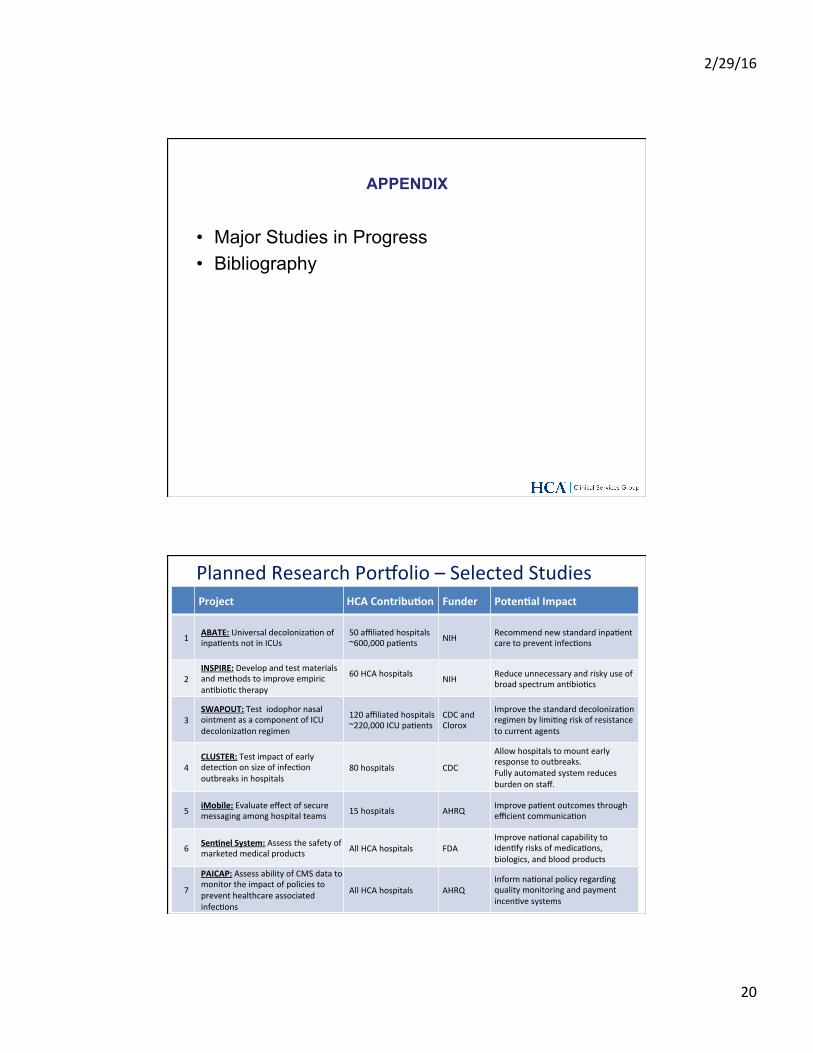
APPENDIX
• Major Studies in Progress • Bibliography
PlannedResearchPorqolio–SelectedStudiesProject HCAContribu9on Funder Poten9alImpact
1 ABATE:UniversaldecolonizaZonofinpaZentsnotinICUs
50affiliatedhospitals~600,000paZents NIH RecommendnewstandardinpaZent
caretopreventinfecZons
2INSPIRE:DevelopandtestmaterialsandmethodstoimproveempiricanZbioZctherapy
60HCAhospitals NIH Reduceunnecessaryandriskyuseof
broadspectrumanZbioZcs
3SWAPOUT:TestiodophornasalointmentasacomponentofICUdecolonizaZonregimen
120affiliatedhospitals~220,000ICUpaZents
CDCandClorox
ImprovethestandarddecolonizaZonregimenbylimiZngriskofresistancetocurrentagents
4CLUSTER:TestimpactofearlydetecZononsizeofinfecZonoutbreaksinhospitals
80hospitals CDC
Allowhospitalstomountearlyresponsetooutbreaks.Fullyautomatedsystemreducesburdenonstaff.
5 iMobile:Evaluateeffectofsecuremessagingamonghospitalteams 15hospitals AHRQ ImprovepaZentoutcomesthrough
efficientcommunicaZon
6 Sen9nelSystem:Assessthesafetyofmarketedmedicalproducts AllHCAhospitals FDA
ImprovenaZonalcapabilitytoidenZfyrisksofmedicaZons,biologics,andbloodproducts
7
PAICAP:AssessabilityofCMSdatatomonitortheimpactofpoliciestopreventhealthcareassociatedinfecZons
AllHCAhospitals AHRQInformnaZonalpolicyregardingqualitymonitoringandpaymentincenZvesystems
2/29/16
21
Bibliography
Platt R, Takvorian S, Septimus E, Hickok J, Moody J, Perlin J, Jernigan J, Huang S. “Cluster Randomized Trials in Comparative Effectiveness Research: Randomizing hospitals to test methods for prevention of healthcare-associated infections.” Medical Care. 2010; 48:s52-57.
Huang SS, Septimus E, Kleinman K ... Perlin JB, Platt R. “Targeted Versus Universal Decolonization to Prevent ICU Infection.” New England Journal of Medicine. 2013; 368:2255-2265. DOI: 10.1056/NEJMoa1207290.
Platt R, Huang SS, Perlin JB. “A Win for the Learning Health System.” May 29, 2013. Commentary, Institute of Medicine, Washington, DC. Available at http://www.iom.edu/WinforLHS;
Huang SS, Septimus E, Avery TR, Lee GM, Hickok J, Weinstein RA, Moody J, Hayden MK, Perlin JB., Platt Richard, Ray GT. “Cost Savings of Universal Decolonization to Prevent ICU Infection: Implications of the REDUCE MRSA Trial.” Infection Control and Hospital Epidemiology. 2014; In Press.
Septimus E, Hayden MK, Kleinman K, Avery TR, Moody J, Weinstein RA, Hickok J, Lankiewicz J, Gombosev A, Haffenreffer K, Kaganov RE, Jernigan JA, Perlin JB, Platt R, Huang SS. “Cost-savings of universal decolonization to prevent intensive care unit infection: implications of the REDUCE MRSA trial.” Infection Control and Hospital Epidemiology. 2014;35(Suppl3):S23-31.
Huang SS, Septimus E, Hayden M, … Perlin JB, Weinstein R. “Effectct of Body Surface Decolonization on Bacteriuria and Candiduria in Intensive Care Units: an Analysis of a Cluster-Randomized Trial.” Lancet Infectious Disease. 2016;16(1):70-9.
©HCAMS,2014
Learning Healthcare & Clinical Leadership in an Accountable Environment
Jonathan B. Perlin, MD, PhD, MSHA, MACP, FACMI
President, Clinical Services Group and Chief Medical Officer HCA / Hospital Corporation of America
Chair, American Hospital Association, 2015 Clinical Professor of Medicine & Biomedical Informatics, Vanderbilt University Adjunct Professor of Health Administration, Virginia Commonwealth University
Contact: [email protected]
It’s a Question of Quality Conference
London, England– February 25, 2016