Quality Education for a Healthier Scotland Medically Unexplained Symptoms: Current Thinking & Ideas...
42
Quality Education for a Healthier Scotland Medically Unexplained Symptoms: Current Thinking & Ideas for Teaching Dr. Deirdre Holly Research & Training Officer (Health Psychology) Psychology Directorate
-
Upload
delphia-fox -
Category
Documents
-
view
217 -
download
2
Transcript of Quality Education for a Healthier Scotland Medically Unexplained Symptoms: Current Thinking & Ideas...

Quality Education for a Healthier Scotland
Medically Unexplained Symptoms: Current Thinking &
Ideas for Teaching
Dr. Deirdre HollyResearch & Training Officer (Health
Psychology)Psychology Directorate

Quality Education for a Healthier Scotland

Quality Education for a Healthier Scotland
“Persistent and distressing somatic symptoms for which adequate somatic explanation does not reveal sufficient explanatory organic pathology”
-Shaefert et al, 2013

Quality Education for a Healthier Scotland
Vague symptoms, polypharmacology, high distress, insistent and frequent attendees.
Irritable Bowel Syndrome, Chronic Fatigue Syndrome, Fibromyalgia.

Quality Education for a Healthier Scotland
What problems as GPs and trainers do you see?

Quality Education for a Healthier Scotland
Key Figures

Quality Education for a Healthier Scotland
20% of Primary Care consultations
Up to 50% in Secondary Care
High levels of distress and disability
60% also have a diagnosed Long Term Condition
2% of Primary Care patients attend persistently
£3.1 billion cost annually in UK

Quality Education for a Healthier Scotland
What works and what doesn’t?

Quality Education for a Healthier Scotland
Most health professional encounters involve “expert” and “patient”
Problems arise when explanations don’t sit well
Tendency for many health professionals to push the same message
Frustration when the patient resists explanations
Presumption that patient has heard what you’ve said

Quality Education for a Healthier Scotland
Evidence to support CBT-based interventions (Van Dessel et al 2014)
Enhanced generalist care may be helpful (Rosendal et al 2013)
Reassurance/Psychosomatic ideas may not be helpful
Biopsychosocial perpetuation…(formulation vs diagnosis)
Personally relevant, mechanical explanations best (Burton (Ed) 2014)

Quality Education for a Healthier Scotland
Initial Thoughts

Quality Education for a Healthier Scotland
Full physical examination
Physiological aspects of the explanation:
• Pain Mechanisms (sensitisation)• Gut Motility• Vestibular aspects of dizziness

Quality Education for a Healthier Scotland
What not to say...and why

Quality Education for a Healthier Scotland
“Good news, there’s nothing wrong with you!”
“The results of the tests have ruled out anything bad”
“There is not much we can do with these symptoms”
“There could be psychological reasons for all this”
“I’m not sure your symptoms are as bad as you say”
“I’m going to refer you one more time for reassurance”
“You’re absolutely fine, it’s going to be ok”

Quality Education for a Healthier Scotland
How do we avoid this?

Quality Education for a Healthier Scotland
Perpetuating Factors

Quality Education for a Healthier Scotland
Perpetuating factors - Cause vs Perpetuation
Consequence of how symptoms are interpreted:• Avoidance of activity• Low mood and anxiety
Create “vicious cycle” – not a cause, but maintenance
Consequences add to the suffering of the patient

Quality Education for a Healthier Scotland

Quality Education for a Healthier Scotland
“So what do you notice when you’re doing less?”
“How hard is it to cope when you feel down?”
“How can you end up feeling with these worries?”
“What’s happened to your motivation?”
“So one thing affects another, affects another?”

Quality Education for a Healthier Scotland
Good way to validate the patient experience
Can be used to identify intervention strategies
Reflect on success of trying to look for cause

Quality Education for a Healthier Scotland
Move away from psychological cause
Don’t expect to do it all in one session
Personally relevant explanations including physiological elements
Recognise the difference between cause and perpetuation
Reject, collude or empower?

Quality Education for a Healthier Scotland
“...complex interactions of physiological and cognitive processes...”
Neither simple disease syndromes nor a general somatisation disorder are adequate to describe the diversity seen in primary care.
Somatisation is too restrictive a label; ‘functional somatic symptoms’ is a more appropriate term.”
-Burton, 2003

Quality Education for a Healthier Scotland
Core Communication Skills

Quality Education for a Healthier Scotland
Demonstrating genuine empathy
Checking you understand the patient
Summarising the information provided
Reflecting on what has been said
Validating what the patient has said
Checking the patient has picked you up correctly
Getting personally relevant information to use

Quality Education for a Healthier Scotland
How can we enable GP trainees to do this?

Quality Education for a Healthier Scotland
Mapping to RCGP Curriculum
Quality Education for a Healthier Scotland
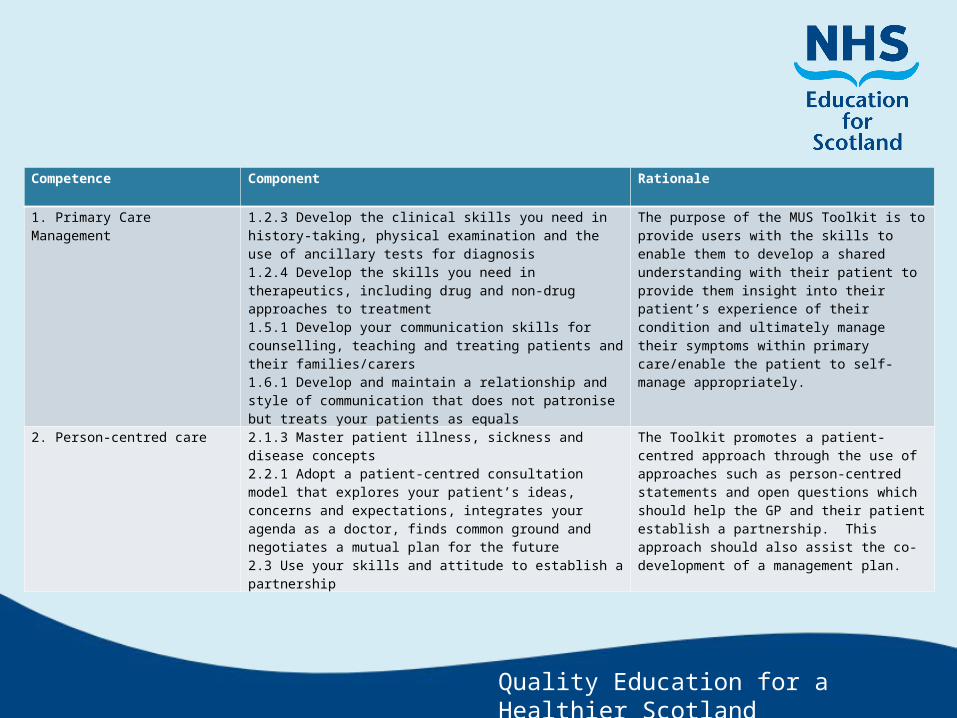
Competence Component Rationale1. Primary Care Management 1.2.3 Develop the clinical skills you need in history-
taking, physical examination and the use of ancillary tests for diagnosis1.2.4 Develop the skills you need in therapeutics, including drug and non-drug approaches to treatment1.5.1 Develop your communication skills for counselling, teaching and treating patients and their families/carers1.6.1 Develop and maintain a relationship and style of communication that does not patronise but treats your patients as equals
The purpose of the MUS Toolkit is to provide users with the skills to enable them to develop a shared understanding with their patient to provide them insight into their patient’s experience of their condition and ultimately manage their symptoms within primary care/enable the patient to self-manage appropriately.
2. Person-centred care 2.1.3 Master patient illness, sickness and disease concepts2.2.1 Adopt a patient-centred consultation model that explores your patient’s ideas, concerns and expectations, integrates your agenda as a doctor, finds common ground and negotiates a mutual plan for the future2.3 Use your skills and attitude to establish a partnership
The Toolkit promotes a patient-centred approach through the use of approaches such as person-centred statements and open questions which should help the GP and their patient establish a partnership. This approach should also assist the co-development of a management plan.

Quality Education for a Healthier Scotland
Section Statements Link to MUS Toolkit3.01 Healthy people: Promoting health and preventing disease
2.5 Negotiate a shared understanding of problems and their management (including self-management), so that patients are empowered to look after their own health and have a commitment to health promotion and self-care2.6 Encourage patients, their carers (and family when appropriate) to access further information and use patient support groups
The MUS toolkit seems to fit well with aspects of person-centred care outlined in these clinical statements due to its emphasis on the use of a shared understanding of symptoms.In addition, the toolkit encourages GPs to support their patients to self-manage their conditions.
3.05 Care of Older Adults 1.9 Have an organisational approach that allows easy access to the primary healthcare team for older people, appropriate timing of appointments and the systematic management of chronic conditions and co-morbidities2.5 Have appropriate communication skills for counselling, teaching and treating patients, their families and carers, recognising the difficulties of communicating with older patients including the slower tempo, possible unreliability or having to rely on the evidence of third parties
The toolkit may have special relevance for elderly patients who tend to present with more LTCs.

Quality Education for a Healthier Scotland
COT Performance Criteria

Quality Education for a Healthier Scotland
PC1 The doctor is seen to demonstrate empathy, warmth and genuineness towards the patient
PC3 The doctor is seen to explicitly elicit the emotional, cognitive and behavioural effects of physical symptoms
PC5 The doctor is seen to bring information about the consequences of persistent symptoms together to demonstrate a “vicious cycle”
PC6 The doctor is seen to help the patient draw conclusions about the “vicious cycle”, exploring the likelihood of further investigations being effective, and the rationale for self management

Quality Education for a Healthier Scotland
Barriers to Implementation

Quality Education for a Healthier Scotland
Believing that referral is a good way of providing reassurance
Believing that referral is an effective management strategy when under pressure

Quality Education for a Healthier Scotland
How can you address these barriers?

Quality Education for a Healthier Scotland
Provide opportunities to master core communication skills
Highlight benefits of being able to manage people with MUS within primary care
Encourage use of approaches suggested within practice in manageable bite size chunks
-use additional resources, where necessary
Use of videos embedded within PESTO
Observation of other’s consultations

Quality Education for a Healthier Scotland
Key Points to Emphasise

Quality Education for a Healthier Scotland
You can’t do everything
Personally relevant explanations can be therapeutic
Providing physiological pathways may help
Keeping and re-appointing the patient can help
No one is advocating the “T” in CBT…
The trials of moving from “diagnosis” to “formulation”
Without core communication skills there’s little point...

Quality Education for a Healthier Scotland
Parting Thoughts...

Quality Education for a Healthier Scotland
How are you going to address this with your trainees?
Think of one way you can change the way you approach MUS with your trainees
How are you going to do this (think SMART)
If that approach doesn’t work what will you do?

Quality Education for a Healthier Scotland
Questions?

Quality Education for a Healthier Scotland

Quality Education for a Healthier Scotland
1. ABC of Medically Unexplained Symptoms. Burton (Ed). 2013. Wiley-Blackwell.
2. Health Behaviour Change (2nd ed.). Mason, P. & Butler, C. (2010).
3. Overcoming Functional Neurological Disorders – A Five Systems Approach. Williams, C. (2011). Hodder Arnold
4. Deary, V., Chalder, T. And Sharpe, M. (2007). The cognitive behavioural model of medically unexplained symptoms: A theoretical and empirical review. Clinical Psychology Review, 27, 781-797.
5. Rosendal M, Blankenstein AH, Morriss R, Fink P, Sharpe M, Burton C. (2013). Enhanced care by generalists for functional somatic symptoms and disorders in primary care (Review). The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Quality Education for a Healthier Scotland
Contacts:David CraigNES Psychology Directorate2 Central Quay 89 Hydepark St.G3 8BW
Deirdre HollyNES Psychology Directorate2 Central Quay 89 Hydepark St.G3 8BW