Quality and creativity in coding 4th Nordic Casemix Conference Helsinki, 3 June 2010 Jens Lind...
35
Quality and creativity in coding 4th Nordic Casemix Conference Helsinki, 3 June 2010 Jens Lind Knudsen Ministry of Interior and Health, Denmark
-
Upload
christiana-daniels -
Category
Documents
-
view
215 -
download
1
Transcript of Quality and creativity in coding 4th Nordic Casemix Conference Helsinki, 3 June 2010 Jens Lind...

Quality and creativity in coding
4th Nordic Casemix ConferenceHelsinki, 3 June 2010
Jens Lind KnudsenMinistry of Interior and Health, Denmark

4th Nordic Casemix Conference, Helsinki 2010
The quality of DRG depends on many factors
Good coding
Good code classifications
Good cost data
Good systems for collecting the data
Good DRG classifications
Good studies on the data
Good systems to disseminate the results
Good ways to follow up on the results
Dedicated staffs to develop and maintain all this!

4th Nordic Casemix Conference, Helsinki 2010
Quality of the systems around coding
1. You should be able to code what you do!
2. It should be easy to find the codes!
3. Cooperate with the medical associations!
4. The DRG classification must not provide incentives to poor coding!
5. Clear and transparent DRG classification!
6. Ongoing evaluation of the quality of coding!

4th Nordic Casemix Conference, Helsinki 20104
1. You should be able to code what you do!
The Nordic DRG classifications are based on diagnoses (IDC10) and procedures: Surgical procedures
(Nordic Classification of Surgical Procedures)
Treatment procedures(National classifications)
Examination procedures(National classifications)
etc.

4th Nordic Casemix Conference, Helsinki 201014 November 2009 5
1. You should be able to code what you do!
Classifications must be kept up to date constantly!
It must be possible to open new codes- quickly and easily!
It must be possible to place new codes in the DRG classification as the codes are opened!
The Danish code classifications are updated four times a year – with a corresponding update of the DRG classification!

4th Nordic Casemix Conference, Helsinki 2010
2. It must be easy to find the codes!
Simple access tocode classifications!
Easy-to-use coding guidelinesthat fit in the coat pocket!
It must be easy to code well!
Central authorities setsthe principles!
Let the medical societiesdevelop the guidelines!
4th Nordic Casemix Conference, Helsinki 2010
3. Cooperating with the medical societies
When constructing DRGs we should emphasize1. The groups must be meaningful clinically 2. The groups must be homogeneous as to
resources3. Not TO many groups…
When choosing between two good solutions to a classification problem in DkDRG, we often choose the more meaningful clinically.
4th Nordic Casemix Conference, Helsinki 20108
3. Cooperating with the medical societies
The Ministry collaborates closely with all medical associations when developing and maintaining the DRG classification.
The Danish hospitals are providing the data for the calculation of the cost weights.
Result: The hospitals and the doctors are
accepting the measure!
They have made the measure themselves!

4th Nordic Casemix Conference, Helsinki 2010
3. Cooperating with the medical societies
Cost per discharge/visit Length of stay
% o
f dis
charg
es/
vis
its
% o
f dis
charg
es/
vis
its
Complicated reconstruction, knee
Other surgical procedures, back

4th Nordic Casemix Conference, Helsinki 2010
Cost per discharge/visit Length of stay
% o
f dis
charg
es/
vis
its
% o
f dis
charg
es/
vis
its
Complicated reconstruction, knee
Other surgical procedures, back
3. Cooperating with the medical societies
ongoing process

4th Nordic Casemix Conference, Helsinki 201014 November 2009 11
4. No incentives to bad coding in DRG classifications!
In Denmark secondary diagnoses should be coded if they are “clinical relevant”.
Whether a diagnosis is clinical relevant or not is up to the physician to decide.
Some doctors will see a diagnosis as relevant – others will see it as not relevant.
Whether a secondary diagnosis is coded or not can be random.

4th Nordic Casemix Conference, Helsinki 201014 November 2009 12
4. No incentives to bad coding in DRG classifications!
If the hospital is funded with a DRG system where secondary diagnoses might result in higher rates – there is an incentive to code diagnoses with a small indication.
Denmark chose to base complication splits mainly on procedures.
Splits on procedures can outline hospitals with highly specialised procedures.

4th Nordic Casemix Conference, Helsinki 201014 November 2009 13
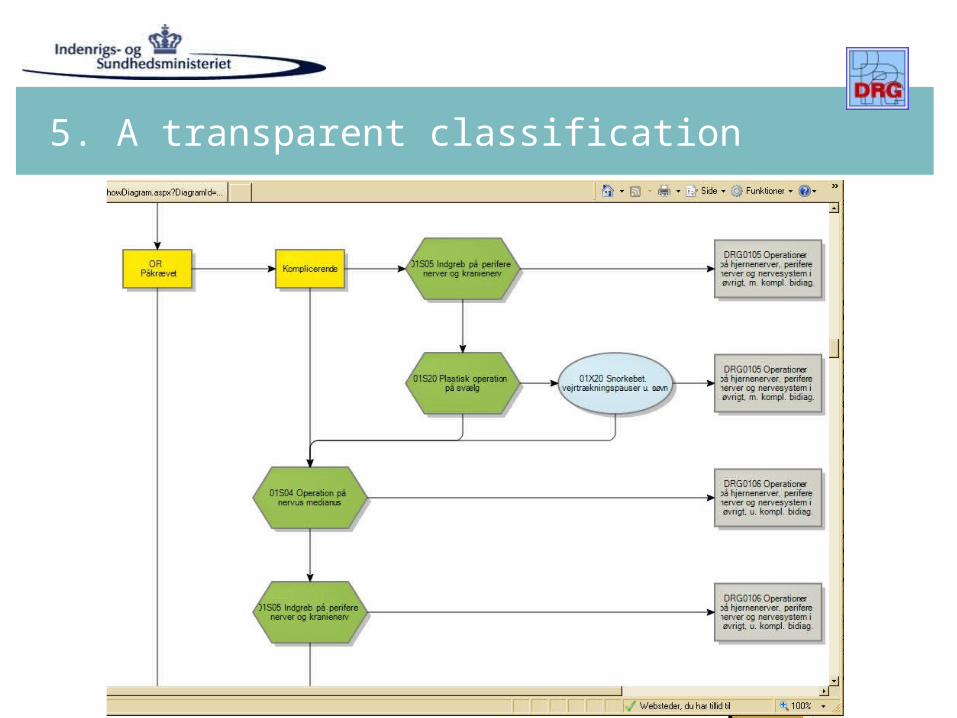
5. A transparent classification
In Denmark the DkDRG system moves around 145 billion DKK (20 billion Euros).
An instrument that moves so much money must be transparent.
If we want the patients classified correctly in the DRGs, we must make it easy for the doctors to choose the necessary and sufficient diagnoses for a correct grouping.
4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification

4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification

4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification(?)

4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification

4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification

4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification

4th Nordic Casemix Conference, Helsinki 2010
5. A transparent classification(?)

4th Nordic Casemix Conference, Helsinki 201014 November 2009 21
5. A transparent classification
Non-transparency in the classification can lead to inefficient coding practices.
In Denmark we are working on removing the build-in complication feature from DkDRG from 2012.

4th Nordic Casemix Conference, Helsinki 2010
6. Ongoing evaluation of the coding
confidence is good
control is better

4th Nordic Casemix Conference, Helsinki 2010
6. Ongoing evaluation of the coding
confidence is good
control may be better
cooperation is even better
partnership may be best

4th Nordic Casemix Conference, Helsinki 201014 November 2009 24
6. Ongoing evaluation of the coding
Four main scenarios of bad coding:1. Under-coding (to few codes)
2. Over-coding (to many correct, but unnecessary codes)
3. Up-coding (fraud, with an effect on DRG rates)
4. Errors (ends up in DRGs for errors)
The evaluation should continuously follow at least these four scenarios.

4th Nordic Casemix Conference, Helsinki 2010
New born babies
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
New born babies – healthy or not?
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
New born babies – healthy or not?
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
New born babies – healthy or not?
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
New born babies – healthy or not?
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
New born babies – healthy or not?
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
New born babies – healthy or not?
Discharges, new born 2009 %
Hospitalhealth probl
minor probl healthy total
health probl
minor probl healthy tot
Rigshospitalet, Copenhagen 1.166 149 3.201 4.516 25,8 3,3 70,9 100
University Hospital, province 1.531 189 2.302 4.022 38,1 4,7 57,2 100
University Hospital, province 990 157 4.088 5.235 18,9 3,0 78,1 100
Major hospital, Copenhagen 916 479 4.525 5.920 15,5 8,1 76,4 100
Major hospital, Copenhagen 720 0 2.113 2.833 25,4 0,0 74,6 100
Minor hospital, Copenhagen 517 176 1.537 2.230 23,2 7,9 68,9 100
Major hospital, province 990 557 2.207 3.754 26,4 14,8 58,8 100
Minor hospital, province 184 149 731 1.064 17,3 14,0 68,7 100
Minor hospital, province 350 231 937 1.518 23,1 15,2 61,7 100
other major / minor hospitals 8.590 2.469 25.944 37.003 23,2 6,7 70,1 100
Total15.95
4 4.55647.58
568.09
5 23,4 6,7 69,9 100Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
Discharges MDC 14 – no. of diagnoses
Hospitalno of
dischargesAverage no diagnoses
Rigshospitalet, Copenhagen 4.694 4,3
University hospital, province 4.117 8,7
University hospital, province 6.847 5,5
Major hospital, Copenhagen 5.899 6,9
Major hospital, Copenhagen 3.167 3,3
Major hospital, province 8.940 5,9
Major hospital, province 5.801 4,5
Other major / minor hospitals 38.287 5,1
Total 77.752 5,4Discharges 2009, DkDRG 2010

4th Nordic Casemix Conference, Helsinki 2010
Discharges MDC 14 – no. of diagnoses
Hospitalno of
dischargesAverage no diagnoses
Rigshospitalet, Copenhagen 4.694 4,3
University hospital, province 4.117 8,7
University hospital, province 6.847 5,5
Major hospital, Copenhagen 5.899 6,9
Major hospital, Copenhagen 3.167 3,3
Major hospital, province 8.940 5,9
Major hospital, province 5.801 4,5
Other major / minor hospitals 38.287 5,1
Total 77.752 5,4
35.996
Total no ofdiagnoses
5,4 => 22.232
3,3 => 15.744
Discharges 2009, DkDRG 2010
4th Nordic Casemix Conference, Helsinki 2010
Quality and creativity in coding
1. You should be able to code what you do!
2. It should be easy to find the codes!
3. Cooperate with the medical associations!
4. The DRG classification must not provide incentives to poor coding!
5. Clear and transparent DRG classification!
6. Ongoing evaluation of the quality of coding!

4th Nordic Casemix Conference, Helsinki 201014 November 2009 35
Thank you
Thank you!Jens Lind Knudsen