Pyogenic Coccus Pyogenic Coccus. Staphylococci The Staphylococci.
98
Pyogenic Coccu Pyogenic Coccu s s
-
Upload
briana-ilene-hicks -
Category
Documents
-
view
225 -
download
3
Transcript of Pyogenic Coccus Pyogenic Coccus. Staphylococci The Staphylococci.

Pyogenic CoccusPyogenic Coccus



The StaphylococciStaphylococci

Morphology & Identification
Gram positiveGram positive Facultative anaerobesFacultative anaerobes Grape like-clustersGrape like-clusters Catalase positiveCatalase positive Major components of normal flora Major components of normal flora
skinskin nosenose

Gram Positive cocci - staphylococci
Pus

Catalase test(过氧化氢酶)
(-) (+)

Pathogenesis & Immunity of Staphylococcus aureus

Antigenic Structure
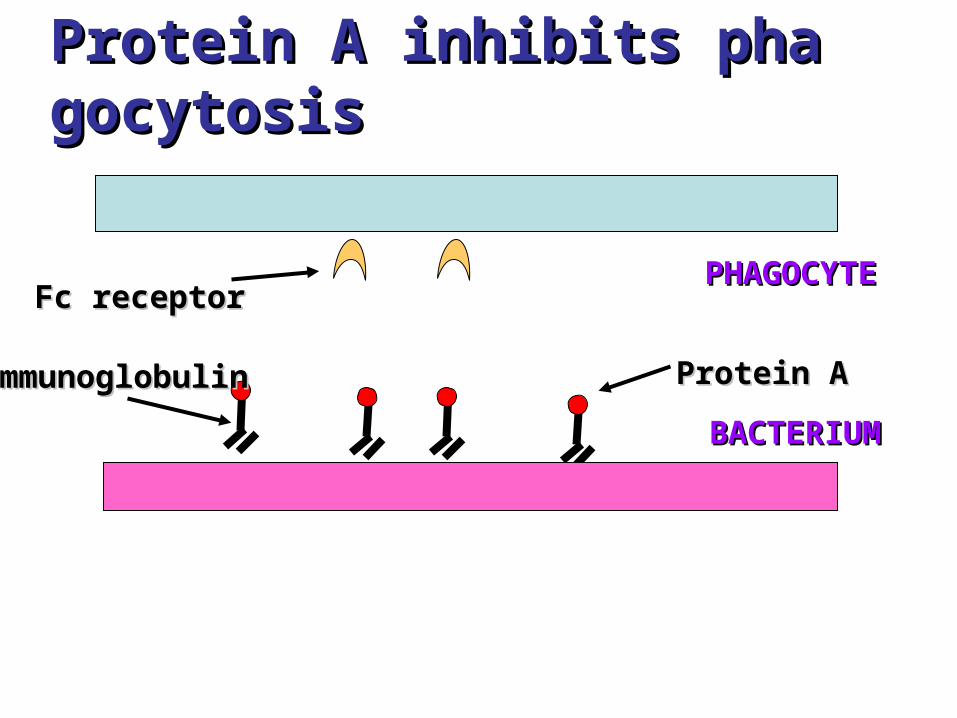
Protein A inhibits phagocytProtein A inhibits phagocytosisosis
Protein AProtein Aimmunoglobulinimmunoglobulin
Fc receptorFc receptor
BACTERIUM BACTERIUM
PHAGOCYTEPHAGOCYTE

Toxins & Enzymes
• Catalase• Coagulase• Hyaluronidase and Lipase ipase • Hemolysin or sphingomyelinase Csphingomyelinase C• Leukocidin• Exfoliative Toxin• Toxic Shock Syndrome Toxin (superantigen)• Enterotoxins

Pathogenesis
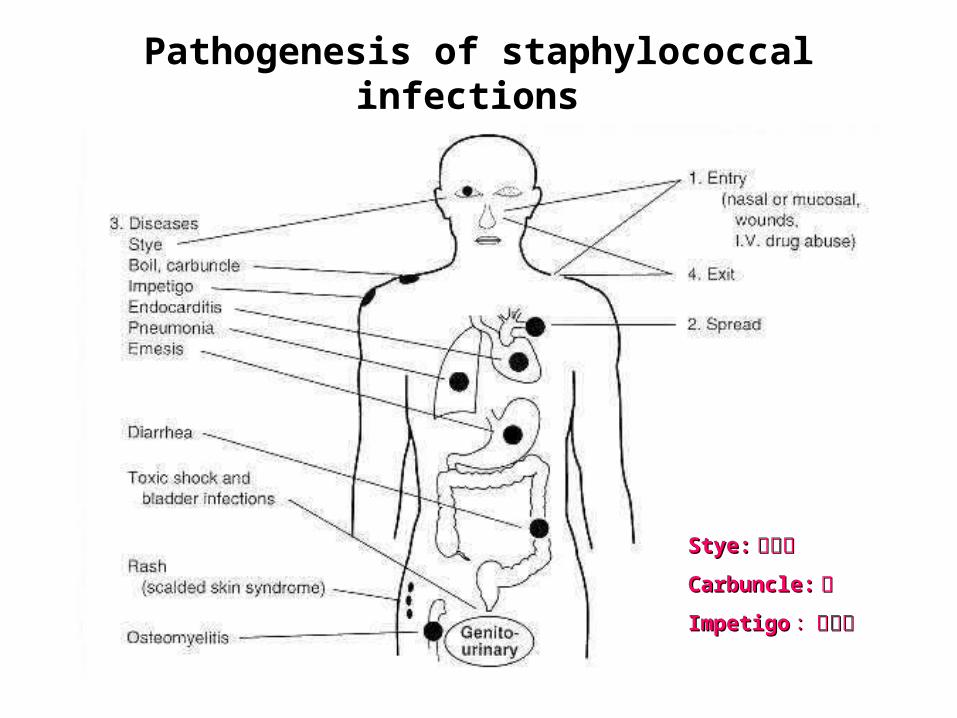
Pathogenesis of staphylococcal infections
Stye:Stye:麦粒肿麦粒肿
Carbuncle:Carbuncle:痈痈
ImpetigoImpetigo :脓疱疮:脓疱疮

Infections associated with indwelling Infections associated with indwelling devicesdevices

Superantigens and the non-specific stiSuperantigens and the non-specific stimulation of T cells mulation of T cells

Clinical Findings-Clinical Findings- Suppurative• A. (Skin) A. (Skin) Furuncle; Protein A, Leukocidin, Hemolysin Furuncle; Protein A, Leukocidin, Hemolysin Stye; lipase Stye; lipase Impetigo; contagious Impetigo; contagious Epidermal necrolysis Epidermal necrolysis Exfoliative Dermatitis (6,7,8); Exfoliative toxin Exfoliative Dermatitis (6,7,8); Exfoliative toxin Mastitis Mastitis Abscess (deep tissue); granulation; coagulasAbscess (deep tissue); granulation; coagulas
e, hyaluronidase (burn, wound) e, hyaluronidase (burn, wound) • B. Systemic B. Systemic : : Bactermia (from abscess, wound, Bactermia (from abscess, wound,
burn) burn) , , Osteomyelitis (tibia) Osteomyelitis (tibia) ,,Pneumonia Pneumonia


Clinical Findings-Clinical Findings- Food poisonFood poisoninging
• not a human infectionnot a human infection
• food contaminated from humans food contaminated from humans
– growth growth
– enterotoxinenterotoxin
• onset and recovery both occur within onset and recovery both occur within few hoursfew hours
• VomitingVomiting/ / nauseanausea/ / diarrheadiarrhea/ / abdominabdominal al //painpain

Toxic shock syndromeToxic shock syndrome
• feverfever• scarlatiniformscarlatiniform
rashrash• desquamationdesquamation• vomitingvomiting• diarrheadiarrhea• myalgiasmyalgias

S. aureusS. aureus
• babiesbabies–scalded skin syndromscalded skin syndrom
ee* exfoliatinexfoliatin

Pseudomembranous ColitisPseudomembranous Colitis
Laboratory
• A. Direct examination; Gram Stain • B. Primary media; BAP • C. Differential Tests. 1. Mannitol Salts 2. Coagulase 3. DNase • D. Phage typing • E. Antibiotic Sensitivity (plasmid, B lactamase) • penicillin /methicillin/vancomycin

GRAM POSITIVE COCCI
S. aureus hemolyticmannitol yellow
+ -Staphylococcus (Clusters) Streptococcus (pairs & chains)
Catalase
• BETA: Bacitracin S.pyogenes (group A)
CAMP/Hippurate S. agalactiae (group B)
HemolysisCoagulase
S. epidermidisnonhemolytic (usually)mannitol white
(2) ALPHA: Optochin/Bile Solubility S. pneumoniae
• GAMMA: Bile Esculin 6.5% NaCl Group D* Enterococcus
Bile Esculin 6.5% NaCl Group D* Non-Enterococcus
(*can also be beta or alpha hemolytic)
Note: Strep. viridansare alpha hemolytic andnegat ive for all the testsbelow
+
++
++
+
+
-
-
Summary Figure (Identification Scheme)
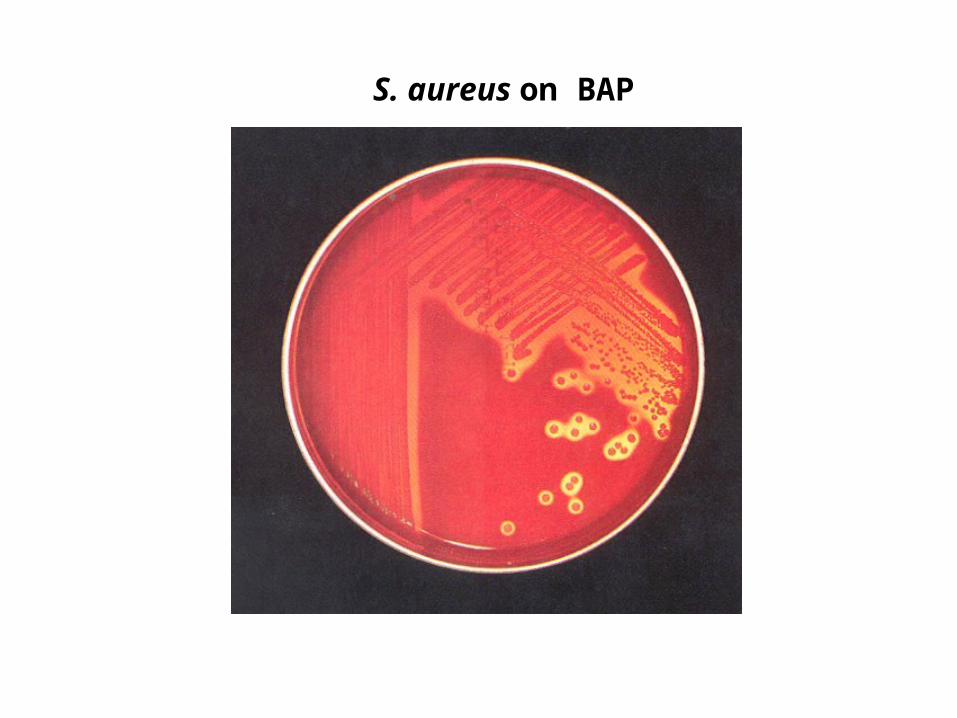
S. aureus on BAP

Mannitol Salt Agar

DNase test
0.1% Toluidine blue O
(+): Pink
1N HCl (+) :

S. aureus on potassium tellurite agar
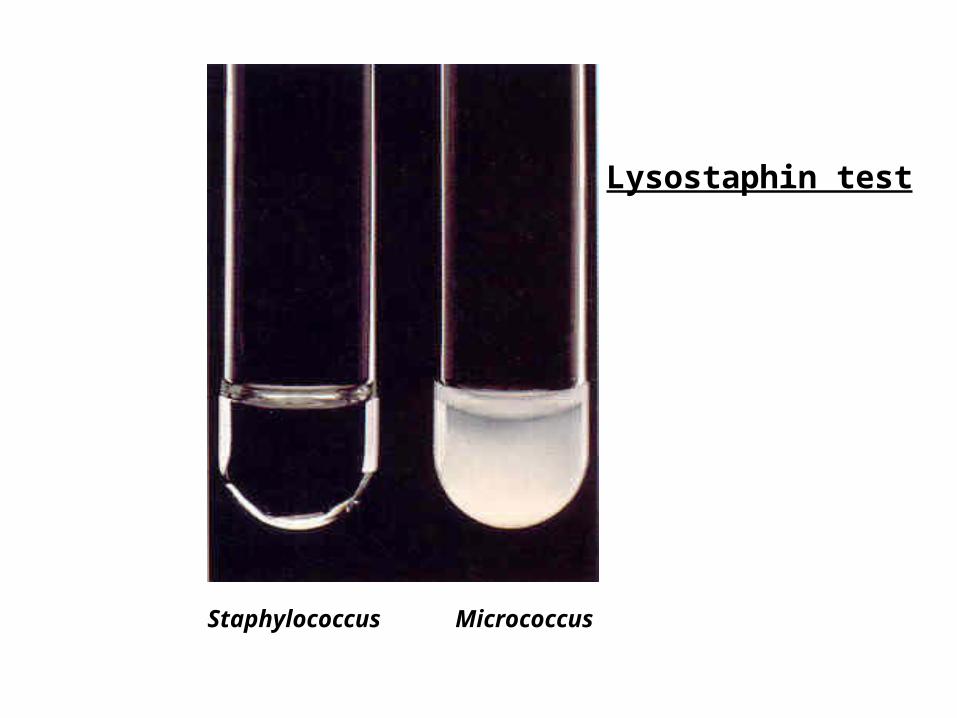
Lysostaphin test
Staphylococcus Micrococcus

API STAPH Kit

Staphylococcus epidermidisStaphylococcus epidermidis
• major component skin floramajor component skin flora• opportunistic infections opportunistic infections
– less common than less common than S.aureusS.aureus• nosocomial infectionsnosocomial infections
– heart valvesheart valves• IdentificationIdentification
– Non-hemolytic Non-hemolytic ((sheep blood agarsheep blood agar))– Does not ferment mannitolDoes not ferment mannitol– Non-pigmented Non-pigmented – Coagulase-negativeCoagulase-negative
Staphylococcus saprophytiStaphylococcus saprophyticuscus
• urinary tract infectionsurinary tract infections
• coagulase-negative coagulase-negative – not differentiated from not differentiated from S. epidermidisS. epidermidis

The Streptococcus


Streptococcus


Morphology & Identification
• facultative anaerobefacultative anaerobe• Gram-positiveGram-positive• ChainsChains or pairsor pairs• CatalaseCatalase negativenegative (staphylococci are catalase positive)(staphylococci are catalase positive)

Cell surface structure of S pyogenes and extracellular substances

S. pyogenesS. pyogenes
fibronectinfibronectin
lipoteichoic acidlipoteichoic acidF-proteinF-protein
epithelial cellsepithelial cells

M proteinM protein
• major target major target – natural immunitynatural immunity
• strain variationstrain variation– antigenicityantigenicity
• re-infectionre-infection– occurs with different strainoccurs with different strain

M protein M protein
M proteinM protein
fibrinogenfibrinogen
rrr
peptidoglycanpeptidoglycan
rrr
IgGIgG
Complement Complement IMMUNEIMMUNE
NON-IMMUNENON-IMMUNE

CapsulesCapsules
• Anti-phagocyticAnti-phagocytic– mucoid strainsmucoid strains
• Streptococci Streptococci • Lancefield Lancefield groupsgroups
*one or more species per groupone or more species per group*surface antigenssurface antigens

groupable streptococcistreptococci
• A, B and DA, B and D–most importantmost important
• C, G, F C, G, F –rarerare

Non-groupableNon-groupable
• S. pneumoniaeS. pneumoniae–pneumonia pneumonia
• viridans streptococciviridans streptococci–e.g.e.g. S. mutans S. mutans
* dental cariesdental caries

Toxins & Enzymes

Hemolysis
alpha
beta
gamma

Classofication of Streptococci of Particular Medical Interest

Pathogenesis of S pyogenes infections.

• Group A streptococcal infections affect Group A streptococcal infections affect all ages peak incidence at 5-15 years of all ages peak incidence at 5-15 years of ageage

S. pyogenes -suppurative. pyogenes -suppurative
• non-invasive non-invasive – pharyngitis pharyngitis – skin infection, impetigoskin infection, impetigo
• invasive bacteremia invasive bacteremia
– toxic shock-like syndrome toxic shock-like syndrome
– "flesh eating" bacteria"flesh eating" bacteria
– pyrogenic toxinpyrogenic toxin

Pyrogenic toxin
• superantigensuperantigen
• T cell mitogen T cell mitogen
• activates immune systemactivates immune system

Scarlet feverScarlet fever
• rash rash • erythrogenic toxinerythrogenic toxin
non-suppurative• rheumatic fever
– inflammatory diseaseinflammatory disease– life threateninglife threatening– chronic sequalaechronic sequalae
• fever fever • heart heart • jointsjoints
• rheumatic NOT rheumatoid arthritisrheumatic NOT rheumatoid arthritis

Rheumatic fever -etiologyRheumatic fever -etiology
M protein M protein – cross-reacts heart myosin cross-reacts heart myosin – autoimmunityautoimmunity
cell wall antigens cell wall antigens – poorly digested poorly digested in vivoin vivo– persist indefinitelypersist indefinitely

Rheumatic feverRheumatic fever

Acute glomerulonephritisAcute glomerulonephritis
• immune complex disease of kidneyimmune complex disease of kidney

Group B streptococcusGroup B streptococcus
• neonatal meningitisneonatal meningitis
• septicemiasepticemia
• transmission transmission – vaginal floravaginal flora

Group B streptococcus - Group B streptococcus - identificationidentification
hemolysishemolysis
• hippurate hydrolysishippurate hydrolysis
• CAMP reactionCAMP reaction
– increases increases hemolysis of hemolysis of S. aureusS. aureus

Group D streptococcusGroup D streptococcus
• Growth on bile esculin agarGrowth on bile esculin agar– black precipitate black precipitate
• 6.5% saline6.5% saline• growgrow
– enterococcienterococci• no growth no growth
– non-enterococcinon-enterococci

EnterococciEnterococci
• distantly related to other streptococcidistantly related to other streptococci• genus genus EnterococcusEnterococcus • gut floragut flora
– urinary tract infection urinary tract infection • fecal contaminationfecal contamination
– opportunistic infectionsopportunistic infections• particularly endocarditisparticularly endocarditis
• most common most common E. (S.) faecalisE. (S.) faecalis

EnterococciEnterococci
• resistant to many antibiotics resistant to many antibiotics – including vancomycinincluding vancomycin
• terminal D-ala replaced by D-lactate terminal D-ala replaced by D-lactate

Viridans streptococciViridans streptococci• diverse species diverse species • oral oral • dental cariesdental caries hemolytic and negative for other tests hemolytic and negative for other tests • non-groupable.non-groupable.• includes includes S. mutansS. mutans
– endocarditis endocarditis
– tooth extractiontooth extraction

Diagnostic Laboratory Test
Post-infectious diagnosis Post-infectious diagnosis (serology)(serology)
• antibodies to streptolysin O antibodies to streptolysin O • important if delayed clinical sequeimportant if delayed clinical seque
lae occurlae occur

MMT T RR
SerotypingSerotyping

S. pneumoniae - diplococci

S. pneumoniae Virulence factorVirulence factorss
• a. a. capsule: capsule: It is antiphagocytic, inhibiting entrapment and It is antiphagocytic, inhibiting entrapment and phagocytosis where type-specific opsonic antibody is absphagocytosis where type-specific opsonic antibody is absent. Non-capsulate mutants are avirulent in experimental ent. Non-capsulate mutants are avirulent in experimental animals.animals.
• b. pneumolysin: b. pneumolysin: It suppresses phagocytic oxidative bIt suppresses phagocytic oxidative burst. It is a membrane-damaging toxin. Thus it can deurst. It is a membrane-damaging toxin. Thus it can destroys red blood cells and possibly ciliated epithelial stroys red blood cells and possibly ciliated epithelial cells. cells.
• c. Surface protein adhesinand secretory IgA protease:c. Surface protein adhesinand secretory IgA protease: The biologic effects are to help The biologic effects are to help S.pneumoniaeS.pneumoniae for the for the colonization and migration.colonization and migration.
• d.Teichoic acid and the Peptidoglycan fragment, phod.Teichoic acid and the Peptidoglycan fragment, phosphorylchorine : sphorylchorine : They can mediate the mobilization oThey can mediate the mobilization of inflammatory cells to the focus of infection and cauf inflammatory cells to the focus of infection and cause the tissue destruction/complement activationse the tissue destruction/complement activation

CapsuleCapsule
• prominent prominent – virulent strains virulent strains
• anti-phagocyticanti-phagocytic• carbohydrate antigens carbohydrate antigens
– vary among strainsvary among strains
• immunity immunity – serotype specificserotype specific
• vaccine contains multiple serotypevaccine contains multiple serotypess
• only for susceptible populationonly for susceptible population

clinic finding • leading cause pneumonialeading cause pneumonia
– particularly young and oldparticularly young and old– after damage to upper respiratory tractafter damage to upper respiratory tract
**e.g. following viral infectione.g. following viral infection• bacteremiabacteremia• meningitismeningitis• middle ear infections (otitis media)middle ear infections (otitis media)
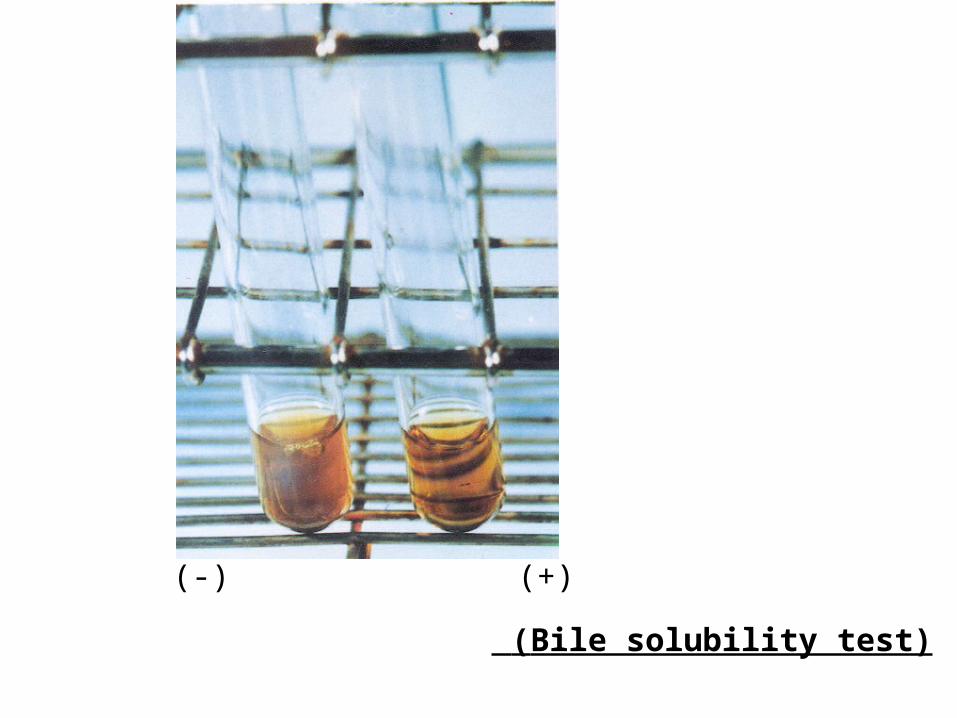
(Bile solubility test)
(-) (+)

Autolysis - identificationAutolysis - identification
BileBile
peptidoglycanpeptidoglycan
cell cell membranemembranelipoteichoic acidlipoteichoic acid
teichoic acidteichoic acid-choline-choline
autolysinautolysin

Not optochin sensitive
optochin sensitive
IdentificationIdentification
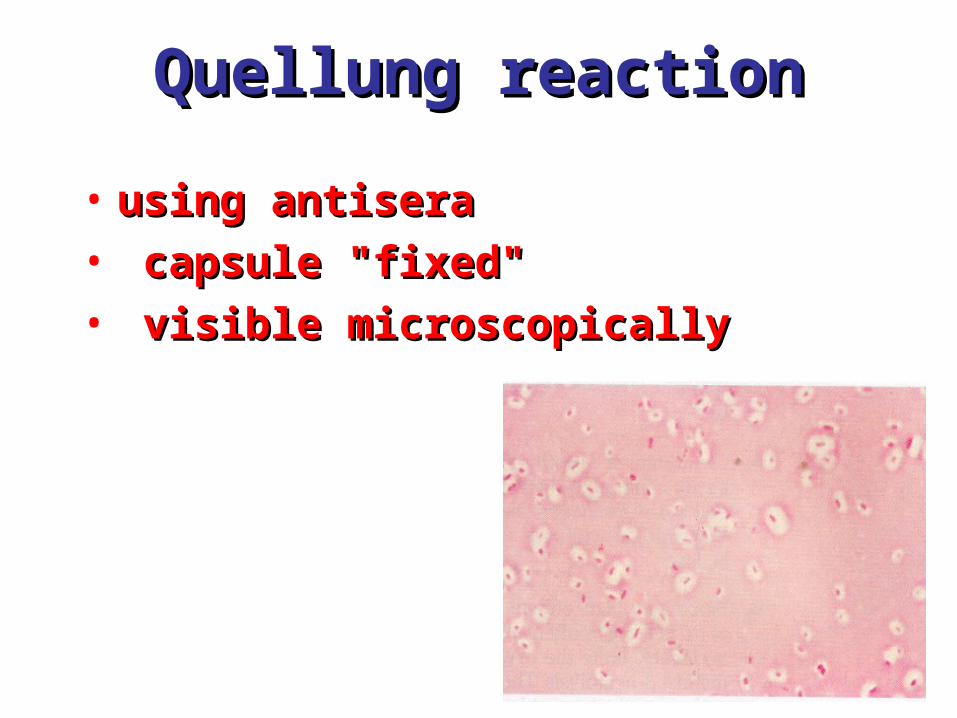
Quellung reactionQuellung reaction
• using antisera using antisera
• capsule "fixed" capsule "fixed"
• visible microscopicallyvisible microscopically

Streptex antiserum

Latex agglutination - streptococci

GRAM POSITIVE COCCI
S. aureus hemolyticmannitol yellow
+ -Staphylococcus (Clusters) Streptococcus (pairs & chains)
Catalase
• BETA: Bacitracin S.pyogenes (group A)
CAMP/Hippurate S. agalactiae (group B)
HemolysisCoagulase
S. epidermidisnonhemolytic (usually)mannitol white
(2) ALPHA: Optochin/Bile Solubility S. pneumoniae
• GAMMA: Bile Esculin 6.5% NaCl Group D* Enterococcus
Bile Esculin 6.5% NaCl Group D* Non-Enterococcus
(*can also be beta or alpha hemolytic)
Note: Strep. viridansare alpha hemolytic andnegat ive for all the testsbelow
+
++
++
+
+
-
-
Summary Figure (Identification Scheme)

Prevention and TreatmentPrevention and Treatment
• Immunity ; 14 capsule types miImmunity ; 14 capsule types mixedxed vaccine vaccine
• MMost strains susceptible to peniost strains susceptible to penicillin cillin , but , but resistance is commo resistance is commonn
NEISSERIANEISSERIA
Neisseria gonorrhoeae

• Gram negative Gram negative • diplococci (pairs of cocci)diplococci (pairs of cocci)• oxidase positiveoxidase positive
• cultureculture• Thayer Martin. Thayer Martin.
– selective selective – chocolate agarchocolate agar
* heated blood (brown)heated blood (brown)
NeisseriaNeisseria

Capsule
LPS
N. meningitidis
Virulence FactorsSimilar, but –Differencesin utilization
HemolysinIgA protease
PILIOpacity (OPA) proteinsOuter Membrane Proteins
N. gonorrhoeae
LPS
PILIOpacity (OPA) proteinsOuter Membrane Proteins
IgA protease
NO capsuleNO hemolysinX

• After 2-14 daysAfter 2-14 days •FFound only in manound only in man• GGonorrheaonorrhea: : second most comm second most common venereal diseaseon venereal disease
N. gonorrhoeae N. gonorrhoeae the "gonococcus"the "gonococcus"

Neisseria gonorrhoeae
Using the Gram stain in patient specimens, the organisms are most often observedin polymorphonuclear leukocytes
Gram stain of pure culture Urethral exudate

Neisseria gonorrhoeae

Pili = key in anchorage of organisms to mucosal epithelium.Nonpiliated gonococci are avirulent
Porin proteins (Por) = prevent phagolysosome fusion & allow intracellular survival [ also called protein I]
Opacity proteins (Opa) = binding of organisms to epithelium[also called protein II]
Reduction-modifiable proteins (Rmp) = protection against bactericidal antibodies [ also called protein III]
Neisseria gonorrhoeae
OUTER MEMBRANE PROTEINS

Neisseria gonorrhoeae
Symptomatic infections are notably PURULENT
Urethritis

Neisseria gonorrhoeae
Symptomatic infections are notably PURULENT
Bartholin’s Duct

Neisseria gonorrhoeae
Purulent conjunctivitis
Ophthalmia neonatorum Infection in newborns during vaginal delivery


Neisseria gonorrhoeae
Disseminated gonococcal infection (DGI). Fever, polyarthritis (or monoarticular septic arthritis), and/or dermatitis(pustules on a hemorrhagic base).

SmearSmear
• polymorphonuclear cellpolymorphonuclear cell
• Gram negative cocciGram negative cocci
many in cellsmany in cells
• CultureCulture

• lactamase-resistant cephalosporinlactamase-resistant cephalosporin– e.g. ceftriaxonee.g. ceftriaxone
• resistant strains resistant strains – common common – produce produce lactamases lactamases– destroy penicillindestroy penicillin
Antibiotic therapyAntibiotic therapy
N. meningitidisN. meningitidis (the "meningococcus")

N. meningitidisN. meningitidis
• resides in man only resides in man only • usually sporadic cases usually sporadic cases
– mostly young childrenmostly young children• outbreaks outbreaks
– adults adults – crowded conditions crowded conditions
* e.g. army barrackse.g. army barracks
NeisseriaNeisseria meningitidismeningitidis
upper respiratory tractupper respiratory tract infection infection – adhesion pili adhesion pili
bloodstreambloodstream
brainbrain

Meningococcal meninigitisMeningococcal meninigitis
• 1-4 1-4 daysdays• SSecond most common meningitis econd most common meningitis
– pneumococcus, most common pneumococcus, most common • FFatal if untreated atal if untreated • RResponds well to antibiotic therapesponds well to antibiotic therap
yy– penicillin penicillin
Laboratory DiagnosisLaboratory Diagnosis
• spinal fluid spinal fluid – Gram negative diplococci Gram negative diplococci
within polymorphonuclear cellswithin polymorphonuclear cells– meningococcal antigens meningococcal antigens
• CultureCulture– Thayer Martin agarThayer Martin agar

Prevention - Prevention - CapsuleCapsule
• capsulecapsule– inhibit phagocytosisinhibit phagocytosis
• anti-capsular antibodiesanti-capsular antibodies– stop infectionstop infection
• antigenic variationantigenic variation– serogroupsserogroups
• vaccine vaccine – multiple serogroups multiple serogroups


![[Mikrobiologi] It 5 - Coccus - Khs](https://static.fdocuments.in/doc/165x107/55cf920d550346f57b930bd5/mikrobiologi-it-5-coccus-khs.jpg)