Pulse Healthcare Magazine, Fall 2012
31
IN THIS ISSUE How Change May Unfold in Other Markets • Six Years Later: Seeking Cost Control, Assessing Affiliations How the Payers Are Responding • Attorneys Offer Their Perspectives © 2012 Navigant Consulting, Inc. FALL 2012 Lessons Learned: What Massachusetts' Experience Tells Us HEALTHCARE
Transcript of Pulse Healthcare Magazine, Fall 2012

in this issUEHow Change May Unfold in Other Markets • Six Years Later: Seeking Cost Control, Assessing Affiliations
How the Payers Are Responding • Attorneys Offer Their Perspectives
© 2012 Navigant Consulting, Inc.
FALL 2012
Lessons Learned: What Massachusetts'
Experience Tells Us
H E A L T H C A R E

in this issue
A LETTER FROM DAVE & ALEX
HOW CHANGE MAY UNFOLD IN OTHER MARKETS Navigant Healthcare Managing Directors David Burik and Lisa Rolfe examine the conditions suggesting where change may be implemented most successfully and rank other markets’ “readiness for reform.”
SIX YEARS LATER: SEEKING COST CONTROL, ASSESSING AFFILIATIONS Navigant Healthcare Managing Director Jim Agnew takes a close look at Massachusetts’ experience since its landmark legislation as hospital boards debate the merits of local control vs. a larger system.
HOW PAYERS ARE RESPONDING Navigant Healthcare Managing Director Catherine Sreckovich describes how payers in a favorable policy environment have expanded coverage and introduced risk-based bundled payment approaches.
NAVIGANT NEWS Michael Hill, M.D., and his team, specializing in innovative hospital care transformation consulting, have joined Navigant Healthcare to add to our growing suite of performance improvement solutions.
NAVIGANT ADVISORS OFFER THEIR EXPERTISE
UPCOMING EVENTS
2
4
12
20
27
29
30
Lessons Learned: What Massachusetts' Experience Tells Us
NAVIGANT PULSE FALL 2012 | 1

NAVIGANT PULSE FALL 2012 | 2
Healthcare has been center stage in the legal and political worlds this year, first with the Supreme Court’s landmark decision upholding most of the Accountable Care Act (ACA) and now in an election that could determine whether the law is repealed by a new Congress. But for providers, payers and patients, healthcare’s future already is taking shape far beyond the courthouse or campaign trail – in the marketplace, regardless of who prevails in Washington. The new directional realities, to name just a few, include:
» Fee-for-service losing ground as new payment models become a bigger part of the financing model
» Individual and family insurance replacing commercial group insurance
» Risk moving from employers and insurance companies to patients and providers as healthcare goes from defined benefits to defined contributions
» Reimbursements from Medicare and Medicaid both declining
While the ACA has accelerated certain trends such as the move toward value-based healthcare, competition – not reform – is the major driver in a healthcare landscape that is fundamentally different and much more challenging. Larger health systems have a big edge in this environment, while pressure builds on single-site and
small system providers, not to mention the independent physician practitioners. We are seeing a growing separation of the strategic winners and losers among health systems, with an increase in capital availability for strong performers and tightening of capital for weak ones.
To emerge as one of the winners, we believe providers must navigate strategic challenges with a laser-like focus on “big picture” issues such as cost-effectiveness, clinical excellence and truly integrated relationships between hospitals and physicians. At a minimum, after seeing Medicare margins shrink from positive to negative in less than a decade, providers must lower costs per case and find other ways to at least break even on Medicare volumes. We believe some of the answers will be found at the intersection of performance improvement and clinical effectiveness. As hospitals and physicians align, it is not enough for a health system to just employ doctors. Hospitals and physicians must become clinical collaborators and coordinators of care, with more physicians in leadership positions and more patient-centered clinical operating models.
To help understand how our industry’s transformation will play out, Navigant has intentionally invested in assisting clients in Massachusetts, the nation’s laboratory for healthcare reform. In the six years since the state enacted its version of healthcare reform, we have completed more than 250 engagements with a wide range of physicians, payers, health systems and suppliers.
Alex HunterDave Zito
Clients, Colleagues and Friends:
CONTINUED ON NEXT PAGE
A Letter from Dave & Alex

Based on our experience, we believe the Massachusetts law has been the catalyst for three market forces and trends that are reshaping the healthcare marketplace:
» Increasing provider recapitalization and consolidation. Thinly capitalized and distressed hospitals and physician groups increasingly will seek partnerships, resulting in some transactions that could not have been predicted two years ago.
» An emerging new payment model. Managed care contracts are offering increased incentives to use accountable care tools such as more generics, less high-end imaging and emergency-department avoidance.
» Government fiscal pressures. Large Federal and state budget deficits have exacerbated Medicare and Medicaid solvency issues, forcing payment cuts that demand provider cost reductions.
This edition of Pulse is devoted to what has happened in Massachusetts and the implications for other states and markets. Like the ACA, reform in Massachusetts focused on increasing access to care, not dealing with costs. Surprise! Already-high costs soared higher. This summer the state moved to control costs, but the results of its inability to deal with financial issues earlier offers valuable lessons to providers elsewhere, David Burik and Lisa Rolfe write. David and Lisa also examine the Massachusetts experience to isolate the criteria that help identify which states and markets score highest in
“readiness for reform.” Jim Agnew takes a close look inside the consolidating Massachusetts market to describe how hospital boards are weighing the tradeoffs of local governance versus the advantages of joining a larger system. Catherine Sreckovich offers a perspective on how payers are responding to the Massachusetts law and market forces with a wide variety of risk-based bundled approaches and other initiatives that move away from fee-for-service payments. While every state is different, Catherine foresees that most markets will see continued pressure by regulators to control premiums and health plans’ own pressures to respond by controlling healthcare costs.
As always, Navigant stands ready to design, develop and implement solutions to create high-performing healthcare organizations in today’s volatile environment. We offer the industry’s deepest strategic, clinical and medical group capabilities. In a recent addition, Michael Hill, M.D., founder of EMPATH, an innovative hospital care transformation consultancy, and his team joined Navigant’s Healthcare practice. (See page 27). Our more than 500 consultants collaborated to create the interdisciplinary “Big Platform” solutions rather than a piecemeal approach to our industry’s challenges. We explore not only traditional opportunities for improvement such as labor cost, revenue cycle and supply chain, but also opportunities for pricing transformation, improved care management and creative forms of recapitalization. Please visit our website, www.navigant.com, or contact us directly by phone or email.
Dave ZitoManaging DirectorNavigant Healthcare Practice [email protected] 312.583.5871
Alex HunterManaging DirectorNavigant Healthcare Functional [email protected]
Best regards,
NAVIGANT PULSE FALL 2012 | 3

The Massachusetts Story: Lessons for Other States
KEY POINTS
■ Cost control issues dominate early years of reform
■ ‘Readiness for Reform’ criteria suggest which states will be next
■ Some states will move faster than Federal healthcare reform
By David Burik and Lisa Rolfe
NAVIGANT PULSE FALL 2012 | 4
The multitude of complex regulatory, economic and care delivery factors that led to the Accountable Care Act (ACA) are largely the same factors that led to the sweeping healthcare reform implemented in the state of Massachusetts in 2006. Of course, in the last six years healthcare has become even more volatile with growing levels of uncompensated care, proliferation of new science and technology and the associated escalation of healthcare costs. Still, there is much to be learned from the Massachusetts experience that can serve as a predictive framework of how change might unfold throughout the country. Specifically, the conditions that led to the Massachusetts law, the most effective responses, surprises and other lessons learned can help inform other states, commercial payers, physician groups, health system providers and other industry players as they plan for the impact of reform on their core strategies.
So what were the conditions that led to the Massachusetts law in the first place? As a state that enjoys a tradition of direct engagement with healthcare, Massachusetts had considered many models over many years that could address the issues of:
» Growing levels of uninsured and uncompensated care
» Constrained access to primary care and preventive care services
» A need to reduce overall state healthcare costs
Through the Commonwealth Health Insurance Connector and other reform initiatives, Massachusetts succeeded in providing coverage to more than 95 percent of state residents, and increased access to a broad range of healthcare
NAVIGANT PULSE FALL 2012 | 4
CONTINUED ON NEXT PAGE

services, including primary care and preventive services. These successes built upon the state’s long history of reform efforts across public and private sector groups. While much progress was made on the access front, Massachusetts was largely unsuccessful at containing costs through these initiatives. In fact, the Massachusetts experience showed that when access increases, costs go up. Healthcare spending in Massachusetts is 15 percent higher than the national average,
although premium growth has slowed somewhat. This gap has continued to widen, an issue that the state ultimately will need to address under the ACA through provider payment reform and other significant cost reduction initiatives. (In August, Massachusetts Gov. Deval Patrick signed into law a bill that state lawmakers say could save Massachusetts as much as $200 billion over the next 15 years by pegging healthcare spending at or below the state’s overall rate of growth.)
In Massachusetts and markets around the country, the
uptick in healthcare consolidation that we have been
talking about for years is now happening, with payment
incentives providing a rocket-fuel boost. At the same
time, hospital systems that have grown through past
acquisitions are looking at their corporate organizational
structures and evaluating whether all of the boxes on
their organizational charts contribute to, or inhibit,
their missions. Whether systems are contemplating
acquisitions or integrating operations after acquisitions,
there may be compelling reasons to keep those boxes
and what they represent, including separate boards of
directors and administrative expenses.
Some systems do not want to relinquish local
control for political or mission reasons and prefer
a joint-venture alternative that brings in a capital
partner but retains meaningful local governance.
However, slimmer, leaner organizations generally
will be more successful because systems need to be
nimble to compete effectively. For example, more
academic medical centers are looking to partner
with community hospitals, both to expand their
geographic coverage and reduce costs. In doing
so, they are evolving their structures to be more
competitive against generally lower-cost
community hospital networks.
On the regulatory front, an essential part of market
analysis, as always, is assessing whether a combination
may trigger meaningful antitrust scrutiny. There is a
certain amount of irony in today’s environment. On
the one hand, states and the federal government are
offering incentives for consolidation, while on the
other hand antitrust enforcers increasingly are saying,
“Yes, but don’t get too strong or consolidated.”
That said, in most urban and suburban markets,
there are more than enough competitors and provider
alternatives to sustain a finding that consolidation will
not enable the consolidator to exert undue market
leverage over payers.
Monte Dube is a partner in the Chicago
office and a member of the healthcare
department of the law firm Proskauer Rose
LLP. For almost 30 years, he has worked
exclusively in the health industry, guiding
clients domestically and abroad through the challenges
of new government regulations, changing capital
markets and technology adoption. He can be reached
at [email protected] or 312.962.3533.
Slimmer, Leaner Systems Have an EdgeBy Monte Dube, Proskauer Rose LLP
NAVIGANT PULSE FALL 2012 | 5
CONTINUED ON NEXT PAGE

LESSONS FROM MASSACHUSETTSThe state’s inability to deal with fundamental financial and cost of care issues in the early years of reform offers many important lessons for the healthcare industry under the ACA. These lessons fall into the following general categories:
Size is not the only predictor of contract quality. Through the early days of reform, Blue Cross Blue Shield of Massachusetts plans sustained preferential rate structures with several “quality” providers in the Boston market. Some estimates put these payment differentials as high as 30 percent. The focus of payers and employers was to access “must-have” providers, not to enhance their value. It was not until large employers in the marketplace put pressure on the Blues that payment levels began to level out across the provider community, making cost reduction possible. The next step in achieving significant and lasting cost reductions is in the adoption of significantly different payment methodologies, including innovative cost-sharing and risk-bearing arrangements. Massachusetts’ Blue Cross’ Alternative Quality Product, implemented in 2009, has shown early signs of success in slowing cost-of-care increases while maintaining quality.
Proliferation of academic medicine entrenched in quaternary care may provide additional hurdles to meaningful progress toward cost containment. Massachusetts has a plethora of academic medical centers. This concentration brings significant barriers to cost reduction. While academic providers may have supported the concept of cost reduction, they had fundamental cultural and cost structure issues that limited their ability to make meaningful progress in the early days of the Massachusetts law. On one hand, these centers can accurately be described as job creators that generate economic development. On the other hand, a large percentage of care may be provided in a less-costly setting, leading to healthcare being too expensive and posing a barrier to economic development. It remains to be seen what role the academic medical center of the future can and will play in healthcare cost reduction.
Successful academic medical centers will be those that embrace opportunities to increase efficiencies in the delivery of complex care, while also deploying their teaching, research and clinical missions toward population health management initiatives. These changes may require a fundamental shift in academic culture, faculty incentives and new models for approaching the marketplace (e.g., new roles for community-based providers affiliated with the academic medical center.)
Some level of provider consolidation must occur before real cost containment and value creation can be achieved. It is difficult, if not impossible, for freestanding community hospitals and physician practices to have the assets required to thrive under a reform scenario in a timely manner. Specifically, hospitals and physician groups need to be part of something bigger than a single, stand-alone structure to ensure access to capital, managed care contracting and infrastructure, and fixed cost leverage across multiple sites. In addition, the leadership requirements for succeeding are quite different than the leadership requirements of the past. Future leaders should not be afraid to make the jump to “curve 2” care delivery and the corresponding reallocation of capital, physician incentives and operational priorities. In the future, this leadership will be concentrated in large, complex organizations that will be sufficiently capitalized to move nimbly in executing core strategies. Despite several recent hospital mergers, Boston still is ranked as one of the nation’s 19 least-concentrated health system markets, according to a Navigant estimate of the Herfindahl-Hirschman Index (HHI) used by the U.S. Department of Justice and Federal Trade Commission.
Taxable/private equity participation in the provider market can instigate change. One only has to look at the entry of the private equity firm, Cerberus Capital Management, into the Boston market to see the impact a new, well-capitalized player can have on the pace and nature of market consolidation. In a market previously dominated by large academic players, Cerberus’ acquisition of Caritas Christi Health Care and the resulting
NAVIGANT PULSE FALL 2012 | 6
CONTINUED ON NEXT PAGE

formation of Steward Health Care System significantly changed the landscape of Boston healthcare. Cerberus’ desire for a “big platform” deal led it to invest more than $800 million in the formation of Steward Health Care System – $400 million in acquisition costs and another $400 million in committed capital for information technology investments, physician development and other strategic and operational initiatives. These investments raised the bar in the market for cost containment and other reform-friendly activities.
IS YOUR STATE THE NEXT MASSACHUSETTS?So how do these lessons help predict the future for other states as providers and payers prepare for national healthcare reform? The following conditions suggest a predisposition and perhaps a predictor of where early stages of change may be implemented most successfully. Interestingly enough, many of these conditions are the very same criteria that taxable providers use when evaluating desirability of market entry – a market where they can have a fundamental positive financially accretive outcome.
A political climate “friendly” to taxable providers: Massachusetts is a good example of what can happen when taxable providers become a significant component of the healthcare landscape. With their focus on shareholder value, for-profits can reset the bar in terms of cost of care delivery.
High unemployment: High statewide unemployment means more people will gain access/coverage in the future. This will encourage providers and payers to work together toward the common goal of providing the best possible care under the highest value delivery model.
Exchange progress/experience with Pioneer ACOs: National healthcare reform is likely to unfold most constructively in those states that already have made significant progress on commercial exchange initiatives. Specifically, progress in state exchanges increases the likelihood of people gaining commercial rather than Medicaid coverage, a desired outcome for key stakeholders. To become a Pioneer Accountable
Care Organization, the Centers of Medicare & Medicaid Services must be convinced that the ACO has the infrastructure to successfully manage a medical expense budget. With this criteria, it is not surprising that Massachusetts, with the first phase of reform behind it, has six of the 32 Pioneer ACOs nationwide.
A moderately concentrated commercial payer market: A commercial payer market that is not overly concentrated may enhance the ability of employers and providers to negotiate innovative value or budget-based payment programs with multiple commercial payers.
A moderately consolidated provider market, particularly those with many small to mid-sized Integrated Delivery Networks (IDNs): Provider consolidation will be essential under reform, as the cost of building the infrastructure needed to succeed will most certainly need to be spread over a larger organizational base. Both individual hospitals and small to mid-size IDNs will be especially pressured to consolidate.
Market experience with capitation: States with an existing risk-based presence and, specifically, those with high Medicaid HMO enrollment or a high Medicare Advantage population, will be more likely to be early adopters of the types of risk contracting approaches required. Given this experience, it is likely that the infrastructure required to manage care is farther along in these markets.
High inpatient utilization rates: Markets with above-average utilization rates may have more upside potential to control costs/utilization through accountable care approaches. The exception to this may be in a state that derives these high utilization rates from a high concentration of academic and other quaternary providers.
An adequate supply of physician providers: Access to physician and other non-physician providers is essential as the number of insured increases. This need for sufficient providers is particularly acute in the primary and preventive care specialties.
CONTINUED ON PAGE 9
NAVIGANT PULSE FALL 2012 | 7

Markets Most Ready for Healthcare's Transformation
SeattleSpokane
Portland
Salt Lake City
Denver
Kansas City
Minneapolis
ChicagoSouth Bend
Fort Wayne
IndianapolisDayton
Evansville
MemphisChattanooga
Kingsport
Cincinnati
Columbus
ToledoAkron
Nashville
Birmingham
Columbus
AtlantaAugusta
Savannah
Miami
St. Louis
FlintDetroit
Cleveland
YoungstownPittsburg
AllentownBridgeport
New HavenHartford
Springfield
TrentonPhiladelphia
Harrisburg
Lancaster
Scranton
Knoxville
Washington, DC
Ann Arbor
Eugene
Las Vegas
Phoenix
MaRkET SCORE
Philadelphia-Camden-Wilmington, PA-NJ-DE-MD 2.9
Detroit-Warren-Livonia, MI 2.8
Atlanta-Sandy Springs-Marietta, GA 2.7
Northern NJ 2.7
Seattle-Tacoma-Bellevue, WA 2.7
Augusta-Richmond County, GA-SC 2.6
New Haven-Milford, CT 2.6
Chicago-Joliet-Naperville, IL-IN-WI 2.5
Cincinnati-Middletown, OH-KY-IN 2.4
Cleveland-Elyria-Mentor, OH 2.4
Miami-Fort Lauderdale-Pompano Beach, FL 2.4
Pittsburgh, PA 2.4
Scranton-Wilkes-Barre, PA 2.4
Youngstown-Warren-Boardman, OH-PA 2.4
Allentown-Bethlehem-Easton, PA-NJ 2.4
Bridgeport-Stamford-Norwalk, CT 2.4
Indianapolis-Carmel, IN 2.4
Hartford-West Hartford-East Hartford, CT 2.3
Memphis, TN-MS-AR 2.3
Fort Wayne, IN 2.3
Portland-Vancouver-Hillsboro, OR-WA 2.3
Washington-Arlington-Alexandria, DC-VA-MD-WV 2.3
Harrisburg-Carlisle, PA 2.2
Phoenix-Mesa-Glendale, AZ 2.2
Salt Lake City, UT 2.2
MaRkET SCORE
St. Louis, MO-IL 2.2
Springfield, MA 2.2
Trenton-Ewing, NJ 2.2
Columbus, GA-AL 2.2
Columbus, OH 2.2
Dayton, OH 2.2
Evansville, IN-KY 2.2
Kansas City, MO-KS 2.2
Toledo, OH 2.2
Ann Arbor, MI 2.1
Denver-Aurora-Broomfield, CO 2.1
Kingsport-Bristol-Bristol, TN-VA 2.1
Akron, OH 2.1
Birmingham-Hoover, AL 2.1
Chattanooga, TN-GA 2.1
Eugene-Springfield, OR 2.1
Flint, MI 2.1
Knoxville, TN 2.1
Lancaster, PA 2.1
Las Vegas-Paradise, NV 2.1
Minneapolis-St. Paul-Bloomington, MN-WI 2.1
Nashville-Davidson-Murfreesboro-Franklin, TN 2.1
Savannah, GA 2.1
South Bend-Mishawaka, IN-MI 2.1
Higher scores are based on market characteristics such as a high number of physicians per capita and low hospital and
payer concentration as well as metrics evaluating potential for reform such as high unemployment and hospital usage
rates and familiarity with capitation.
Source: Navigant Healthcare
NAVIGANT PULSE FALL 2012 | 8

Using these criteria and the lessons learned in the Massachusetts experience, Navigant completed a high level “ranking” of how states might be expected to perform under national healthcare reform. Navigant scored 140 MSAs in this analysis, with 49 markets scoring in the top quartile of “readiness for reform.” The top quartile markets are located in 20 states and the District of Columbia, with only 10 of these markets west of the Mississippi River. Examples of high, medium and low “readiness” scores from this analysis are as follows:
“HIGH” READINESSMarkets that scored the highest in their readiness for reform included large urban markets such as Philadelphia, Detroit and Atlanta. These three markets’ moderately concentrated provider communities, combined with the markets’ experience with capitation, are the two most consistent criteria that led to these states’ high scoring.
In the Philadelphia market, payers are proactively approaching the need to reduce costs. Examples include the growth of consumer-driven health plans that have enabled employers to shift rising healthcare costs to employees, and Independence Blue Cross, the market’s largest insurer, which is implementing a number of coordination of care and payment reform initiatives. Additionally, a Philadelphia-area physician group is among 32 Pioneer ACOs selected by CMS to manage care under its new payment initiative. Philadelphia hospitals and health systems are responding to the need to reduce costs by shifting more care to the outpatient setting and forming new community-based partnerships.
In Detroit, unemployment remains high, although the economy is beginning to rebound as the automotive industry stabilizes. The provider market is only moderately consolidated with pressure for greater consolidation, leading to new models for health system collaboration. In fact, many Detroit area health systems have formed ACOs and are negotiating alliances in specialty areas. Taxable dollars are present in the market with Vanguard Health Systems’ acquisition of Detroit Medical Center in 2011.
In Atlanta, both Emory Healthcare and Piedmont Healthcare have made key acquisitions that have provided them with critical mass to build infrastructure required. Additionally, three of the market’s top four health plans are forming patient-centered medical homes and multiple forms of ACOs. These are just a few examples of the types of market activities that might suggest a market’s “high readiness” for national healthcare reform.
“MEDIUM” READINESSMarkets as diverse as Albuquerque, N.M., and Louisville, Ky., scored in the middle of the pack in terms of readiness. In Albuquerque, the large and growing Medicaid market has led to significantly reduced payments to hospitals and physicians. As a result, providers are looking for new ways to attract insured patients, including service expansion into suburban areas. In 2011, New Mexico Gov. Susana Martinez vetoed a bill that would have created a state health insurance exchange initiative and pushed for repeal of Federal healthcare reform legislation. With national reform still moving forward, the Albuquerque market will be forced to explore new models for cost-effective care delivery for its diverse and challenging payer mix.
In the Louisville market, significant provider consolidation has proven difficult, with Kentucky Gov. Steve Beshear rejecting the three-way merger of University of Louisville Hospital, Jewish Hospital & St. Mary’s and Saint Joseph Health System in Lexington. That said, significant opportunities exist as the Louisville physician sector continues its alignment with these large area health systems, which are looking to tap into the infrastructure required to take on new payment methodologies.
“LOW” READINESS Lastly, examples of markets that scored at the low end of the “readiness for reform” analytic include Raleigh, N.C., Baton Rouge, La., and Omaha, Neb. The Raleigh market has seen turmoil in the payer market, exemplified by Aetna’s contract termination with UNC Health Care in 2011. Employers were not willing to be without UNC and switched to other payers, leading to new product
NAVIGANT PULSE FALL 2012 | 9
CONTINUED ON NEXT PAGE

and network offerings. These changes have taken the focus off of true managed care cost savings, and, as a result, providers and payers have some catch-up to do to prepare.
Hospitals and health systems in the Omaha market, while highly consolidated, have not had the reputation of being early adopters of healthcare reform initiatives. Providers have only moderate use of disease management and utilization management programs, although that may be changing with the formation of a market-wide Accountable Care Alliance. That said, economic pressures for healthcare reform are not as strong as in other mid-sized markets, given the relative strength of the local economy.
The Baton Rouge healthcare market faces significant challenges, as the state closed Louisiana State University’s Earl K. Long Medical Center, the market’s safety-net provider, and transferred care to the market’s largest healthcare system, the Franciscan Missionaries of our Lady Health System and its Our Lady of the Lake Regional Medical Center. This has led to major hospital construction initiatives and the need to grow and reorganize the physician community away from small groups and solo practices into larger entities that can more proactively manage the health needs of the region.
These examples show that there will not be a “one-size fits all” strategy for a market to prepare for national healthcare reform.
So what are the implications of the key learnings from Massachusetts and the predictors for which states will be next? The implications can be summarized as follows:
» Some states and markets will move faster than Federal healthcare reform.
» Increased access will increase total costs. Those organizations that focus intensely on lowering per-member cost early on will increase their likelihood of success.
» The pace and level of market consolidation will escalate and new organizational models/legal structures for
IDNs will emerge. Partners HealthCare and Steward Health Care System in Boston are good examples of this evolution. Both have developed a variety of wholly-owned and contractual participation models.
» Continued growth is expected in physician employment, with compensation programs that include risk pools and mirror the value and budget-based payment systems adopted under reform.
» Antitrust and state attorney general activities will evolve as they wrestle with the conflict inherent in balancing pro-competitive behavior with the need for market consolidation to access capital required for infrastructure.
» There will be a premium on management’s ability to manage through the conversion from fee-for-service to value and budget-based compensation.
Providers and other market participants can and should use these Massachusetts lessons and market-specific predictors to refine organizational strategy and operational priorities. At a minimum, organizations should evaluate the readiness of their current structures (e.g., simpler, less complex corporate structures will be preferred) and incentives (e.g., are we incentivizing the “right” behaviors?) under their predicted reform scenario. Additionally, organizations should prepare to collaborate, both horizontally and vertically, with a variety of other market participants that can align around common goals. Whether a market is earlier or later in its stage of reform impact, reform is coming and proactive planning will heighten the probability of organizational success.
For more information on how your state scores under the rankings described in this article, please contact Chris Myers, at [email protected] or 312.583.4161.
NAVIGANT PULSE FALL 2012 | 10
CONTINUED ON NEXT PAGE

About David BurikDavid Burik is a Managing Director at Navigant Healthcare with more than 30 years of consulting experience within all segments of the healthcare industry. His expertise includes the definition and communication of key strategic issues, as well as the successful execution of platform solutions for those issues. He has a bachelor’s degree and master’s degree in finance and hospital health service management from the Kellogg School of Management at Northwestern University. For more information, contact David at [email protected] or 312.583.4148.
About Lisa RolfeLisa Rolfe is a Managing Director at Navigant Healthcare with 20 years of strategic consulting experience and longstanding client relationships within all segments of the healthcare industry. Lisa has a bachelor’s degree in human biology from Stanford University and a master’s degree in business administration, marketing and business policy from the University of Chicago. She currently serves on the Board of Directors at the Michael Rolfe Pancreatic Cancer Foundation. For more information, contact Lisa at [email protected] or 312.583.4154.
NAVIGANT PULSE FALL 2012 | 11

The Massachusetts Story: Six Years Later
KEY POINTS
■ The state seeks to slow costs that are among nation’s highest
■ More hospitals enter strategic partner discussions
■ Hospital boards weigh benefits of local control vs. a larger system
By Jim Agnew
Almost as fast as a Tom Brady quarterback sneak, the Massachusetts State Legislature has once again changed the playing field for the state’s healthcare providers. Legislation enacted this summer targets $200 billion in savings for the state over the next 15 years, tying the state’s healthcare cost increases from 2013 through 2017 to growth in the Massachusetts economy, estimated at 3.6 percent for 2013. For the five years following 2017, the limit is even more aggressive – a half percentage point below growth in the gross state product. In recent years, Massachusetts healthcare spending increases have averaged between 6 and 7 percent, based on $68 billion in total spending in 2010. The new law includes price transparency, increased access to wellness care, mechanisms for certifying Accountable Care Organizations and patient-centered medical homes, incentives to adopt payment methodologies that are alternatives to fee-for-service, and, in the case of state healthcare programs, mandates to expand the number of beneficiaries for whom payment is made based on alternative payment methodologies.
The new bill comes six years after the landmark legislation that created the Massachusetts health reform model, the precursor to the federal Affordability Care Act. It also follows two intermediate changes, in 2008 and 2010, that addressed transparency, mechanisms for understanding cost drivers in the payer and provider communities, expansion of primary care resources, and insurance product redesign to promote cost consciousness in provider selection. While many industry experts applaud the bold measures, healthcare executives and the Massachusetts Hospital Association caution the increased financial burden will deter hospitals from making needed investments in clinical technology, clinical service line expansion, staff development and upgrades to aging infrastructure. Credit rating agency Moody’s Investment Service warned the new cost limits will inhibit hospitals’ revenue growth and reduce their operating flexibility. The report also suggested the money derived from a $225 million one-time assessment on health plans and major healthcare providers and an excise tax on insurers to help
NAVIGANT PULSE FALL 2012 | 12
CONTINUED ON NEXT PAGE

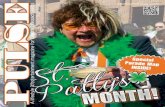
Source: Massachusetts Department of Health 2011
support community hospitals would artificially work to keep smaller, less profitable hospitals in business, while limiting the expansion opportunities for larger hospital groups and hurting their credit standings.
Over the past six years, the Massachusetts health reform legislation was successful in reducing the state’s number of uninsured to less than 2 percent. But the plan did little to slow the growth of healthcare costs that were already among the highest in the nation. A state report last year that found per capita spending in Massachusetts was 15 percent above the national average, noted that private insurance premiums rose between 5 and 10 percent annually. It will be interesting to examine data moving forward as there is some indication both the cost growth and the growth in premiums, especially for the small group market, are beginning to slow.
Historically, the Massachusetts healthcare environment has been dominated by world-class academic institutions, research, strong competitive
activity and high-cost tertiary urban providers. This environment, added to the cost pressures, has been more than enough to create a landscape for hospitals to consider the value of new business models, provider consolidation and risk-based reimbursement models.
In 1990, there were 97 community hospitals operating in the state; today there are 64. Last year, 16 Massachusetts hospitals lost money and two have filed for bankruptcy, according to the state Division of Health Care Finance and Policy. (Quincy Medical Center was sold to Steward Health Care System through the bankruptcy process; North Adams Regional Hospital recently emerged from bankruptcy protection, although its future is still uncertain.)
Massachusetts hospitals and health systems now face the daunting challenge of operating in a new environment where the guardrails are not clearly defined, driving local hospital boards and leadership
Healthcare Spending in Massachusetts: Projections With and Without assumptions about Cost Control Measures
Cost savings over
2013-2022 vs. baseline
projection ($ millions)
2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
$160,000
$140,000
$120,000
$100,000
$80,000
$60,000
$40,000
$20,000
$0
$140,994
$98,539
$197,674
• Baseline projection under current growth
• Growth constrained to GSP until 2017, and GSP - 0.5% from 2018 through 2022
NAVIGANT PULSE FALL 2012 | 13
CONTINUED ON NEXT PAGE

Massachusetts has been a national leader in
healthcare policy since enactment of its landmark
healthcare reform legislation in 2006. After successfully
tackling coverage, it is now, through both public and
private initiatives:
» Addressing coordination to achieve more efficient
care delivery, promotion of financial and other
incentives for quality;
» Recognizing the need to rely on economies of scale
to help finance the intensive infrastructure needed to
support effective population health management;
» And, above all, moving to put in place a true
partnership between patient and caregiver.
The provider landscape is changing to respond to
these initiatives. Each hospital is faced with a strategic
challenge to define for itself the best means to assure
that it is addressing the public policy concerns
described above, and especially how to assure itself a
financially stable base to implement responsive
programs.
What may seem like a kaleidoscope of transactional
activity is in reality a sorting out of differing strategies,
an effort to understand what the right size is for a
coordinated system, and an effort to match the
institution’s culture with that of a potential partner. It is
an exciting, daunting and challenging time.
Steve Weiner chairs the Health Law
Section for Mintz Levin law firm, based
in the Boston office. He has more than
30 years of experience in the
healthcare field as a policy maker,
educator and attorney. He can be reached at
[email protected] or 617.348.1757.
Hospitals Seek Financially Stable BaseBy Steve Weiner, Mintz Levin
teams to make multimillion dollar decisions and develop long-term strategy without a clear vision of the future.
PROVIDER CONSOLIDATION AND RECAPITALIzATIONMassachusetts legislative reform and cost pressures have accelerated the rate at which both community and tertiary hospitals are entering into strategic partner discussions. Many smaller community hospitals are looking for a strong partner to help them weather the financial storm and ensure long-term viability of community access to care. Larger, more financially secure systems are reaching out to expand their market footprint in preparation for population health management and broader risk-based contracting.
One of the most dramatic transactions was the entry of Cerberus Capital Management and its $800 million acquisition of Caritas Christi Health Care, a six-hospital system headquartered in Boston. The result was the formation of Steward Health Care System. The emergence of Steward in the Massachusetts market has increased the opportunities for investor-owned ownership models as an alternative for Massachusetts hospitals to consider. Although Vanguard Health Systems has owned and operated three hospitals in the state, Massachusetts never has been fertile ground for investor-owned providers. That’s now changing: following the Caritas acquisition, Steward has acquired four community acute care hospitals and one long-term acute care hospital in the past 24 months. Each hospital has retained certain reserved
NAVIGANT PULSE FALL 2012 | 14
CONTINUED ON NEXT PAGE

rights and guarantees, including preservation of the hospital for a predetermined number of years, guarantees of capital funding to improve clinical technology, information technology and facility infrastructure and preservation of legacy clinical service lines most important to the communities they serve.
POST-ALIGNMENT INTEGRATIONOne of the most difficult challenges facing health systems is the effort to integrate operations, finance and clinical services after a transaction. Creating of a culture of “systemness” is hard to describe and harder to accomplish. Organizations such as Lowell General Hospital, Steward and Partners HealthCare each are engaged in operations integration with new acquisitions or merger partners. Beginning the post-merger planning efforts, to the extent legally permissible, following the letter of intent or memorandum of understanding phase and before a definitive agreement is completed, is integral for a smooth and successful transition. Lowell began
internal integration planning efforts even while conducting due diligence on its recent transaction with Saints Medical Center. Integration teams began to organize and develop a post-merger model for the new combined organization that addressed the healthcare needs of the greater Lowell community. As the transaction moved toward completion, clinical service line configuration, physician alignment, access to care across multiple campuses, capital formation and a new approach to the system’s vision and mission were all analyzed in detail.
Navigant has been actively engaged with both community hospitals and large health systems to provide strategic advisory and performance improvement resources. In addition, Navigant Capital Advisors has been the financial advisor of record for multiple Massachusetts hospital transactions, supporting both sell-side and buy-side transactions.
Typically, a community hospital board in Massachusetts is faced with a decision of remaining a stand-alone
"We see a national trend of distressed hospitals
looking to affiliate with larger systems, private
equity funds or commercial payers in order to
preserve access to healthcare services in their
communities and obtain the resources to build
comprehensive delivery networks in a cost-
effective manner."
Kevin Lyles, co-chair of
Jones Day's healthcare practice
"Massachusetts’ new health reform law will likely
spur greater consolidation among the state's
hospitals and health systems. A hospital will
need a truly integrated network in order to
achieve the law's stated goals of controlling
healthcare costs without sacrificing the
quality of care."
Travis Jackson, healthcare partner
in Jones Day's Boston office
NAVIGANT PULSE FALL 2012 | 15
CONTINUED ON NEXT PAGE

organization or exploring an affiliated relationship with a clinical/economic partner. As shown in the illustration below, transaction business models are plentiful and each has its pros and cons for both parties. The process begins with the board and leadership team taking a critical view of its value proposition and long-term mission viability under the pressure of reform, revenue compression and competitive threats. This was the initial exercise undertaken by several Massachusetts hospitals, including Morton Hospital, Quincy Medical Center, Northeast Health System, New England Sinai Hospital and Rehabilitation Center and Cooley Dickinson Hospital in their recent transaction activity. Ultimately each determined a partnership/affiliation with another provider was in their community’s best interest.
LOCAL CONTROL VS. SySTEM BENEFITSOne of the early questions faced by community hospital boards is the dilemma of local governance vs. the benefits of joining a larger system. Joining a larger
system through acquisition or merger means the loss of some local control and autonomy. Large scale financial decisions and strategy are managed at the parent board. But that does not preclude input from the local community or hospital. The use of regional boards is widespread across Massachusetts and beyond. These local boards may have responsibility for quality, community needs assessment, medical staff credentialing and fundraising. Board members may believe that the quality-related responsibilities delegated to local hospital board functions are a demotion from their previous authority over financial and business matters. Nothing could be further from the truth. In today’s healthcare reform environment, quality drives revenue.
In many cases members of the regional board make up a percentage of the seats on parent board committees, including strategy, quality, compensation and audit. Today’s health system parent boards understand the value of local governance input from regional boards structured with a governance hierarchy. Based on the transaction negotiations and
NAVIGANT PULSE FALL 2012 | 16
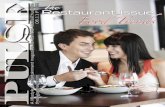
Source: Navigant Healthcare Strategy Practice 2012
Health System Transaction Spectrum
A broad range of potential affiliation structures is available to hospitals and health systems, each influencing
possible benefits. The requirement or desirability for proximity between affiliated units also varies.
Independent, Free-Standing
Contracted Relationship Joint Venture
Management Contract
Joint Operating agreement
Full asset Merger
asset Sale or Long-Term Lease
Specific Clinical Purpose
Back Office Corporate Services
Physician alignment
Risk Sharing
N/a Helpful Required Irrelevant Required Required Required Mixed Helpful Helpful Irrelevant
CONTINUED ON NEXT PAGE
Independent “Loose” Affiliation “Tight” Affiliation
Proximity

reserved powers, there is much flexibility on the design and implementation of hierarchical governance.
The importance of local governance and the value of strategic and financial autonomy are key questions that must be addressed as a first step in any strategic endeavor.
Navigant has identified seven key strengths, with associated drivers of performance, to help boards and
leadership teams in Massachusetts consider their readiness for strategic affiliation or validating their ability to remain a stand-alone organization (see chart below).
The complexity of in-state transactions has allowed both parties significant leverage in structuring terms and conditions that provide mutual benefit. Both not-for-profit and investor-owned transactions have cleared regulatory hurdles with the Massachusetts
StrengthS DriverS
Financial Position, Capital Access and Ability to Make Strategic investments
Debt capacity
Operating margins
Cost position
Strong credit rating
Balance sheet strength
Physician “Platform” Sufficient complement of strategically located, closely
aligned integrated/employed
PCPs with appropriate complement of specialists and sub-specialists
Ability to recruit and retain physicians
Availability of a range of functioning physician alignment vehicles ranging from
JVs to Management Services Organizations to employment
Established, high-performing, critically massed physician enterprise
Competitive Position/vulnerability Presence and strength of other local providers
Competitive encroachment by regional systems
Ability to recruit and retain key clinical and support staff
Ability to be paid appropriately/fairly for services
Market Presence/Position Sufficient critical mass to be a “relevant” provider in the market in terms of:
Size
Market share
Geographic coverage
Differentiated Clinical Service Component
Unique capabilities:
Services
Equipment
Staff
Facilities
Clinical Performance Quality scores
Patient and physician satisfaction
Prepared to deliver accountable care
Patient Access and Preference Access to/presence in avenues of growth and attractive demographics
Strong community support/positive image/presence
Limited outmigration for services available in the community
Seven Strengths to Assess Before Affiliation Providers with them can affiliate or stand alone; providers without
them are likely candidates for affiliation
CONTINUED ON NEXT PAGE
NAVIGANT PULSE FALL 2012 | 17

Department of Public Health and, for the investor-owned transactions, with the Massachusetts Attorney General’s office. Early and often communication with state regulators has been a common theme among all recent transactions. The state has been supportive in providing guidance and objectivity where community benefit and improvement to care delivery can be clearly articulated.
CRITICAL DECISIONSCooley Dickinson Hospital in Northampton, Mass., announced in February 2012 it is affiliating with Massachusetts General Hospital. In a news release, Cooley Dickinson CEO Craig Melin noted that healthcare restructuring away from fee-for-service is happening faster in the state than the rest of the country. In addition, the community hospital said it chose to partner because of decreasing reimbursements, quality care goals and needed infrastructure support for population-based care. "All of this will mean growing operational stress for hospitals and physicians. Organizations that thrive in this world will be those where there is clinical and economic integration among hospitals and physicians for delivery of acute care, chronic care and population-based care," the news release said. "Without a partner, (the Board of) Trustees envisioned that the operational stresses could weaken Cooley Dickinson in the future…."
Many other Massachusetts hospitals now are fully engaged in objective scenario planning to help determine the best strategic options and ultimately who may be the best partner for the future for the benefit of all community stakeholders.
BECOMING COST-COMPETITIVEOne of the most difficult challenges is to continually reduce operating costs to remain competitive in the eyes of commercial payers and ensure a positive bottom line to allow for reinvestment in people, clinical services and infrastructure. For many Massachusetts hospitals, expense reduction has been a roller coaster ride. Initial focus on supply chain, revenue cycle and workforce productivity leads to successful results. But after time, the costs continue
to creep. Massachusetts hospitals have learned that sustainable cost management is an unending battle. Traditional efforts, while helpful, do not deliver the level of improvement required to offset reductions in reimbursements. Hospitals now are turning to clinical reengineering and advanced care management. A new focus on cost per episode of care, using tools such as Prometheus data sets and other informatics tools, is essential. Ultimately, all Massachusetts providers will need to articulate a redefined cost/quality value proposition targeted at multiple stakeholders.
FUTURE FORECASTThe American Hospital Association recently provided guidance for changes in hospital ownership, including mergers, integrated networks or ACOs.
"Hospital leaders must approach potential integration opportunities in a manner that protects the delivery of healthcare services in their communities but recognizes the hospital's need to adapt to the changing environment," the AHA report states. AHA encourages organizations to consider how the partnership will fulfill the hospital's core mission, fall in line with strategic planning, ensure quality of care or avoid potential liabilities.
After a wave of consolidations and new alliances last year, industry leaders say 2012 likely will bring another round of community hospitals partnering with what they hope will be their perfect match.
As for the ACO trend, some community hospitals will merge with larger institutions to build the necessary infrastructure. But Massachusetts healthcare systems that want to form ACOs may have higher priorities than merging with other hospitals: They have to find a way to partner with their physicians, either by employing them or by helping them form clinically integrated networks. They also have to invest in health IT systems to make ACOs work.
Navigant expects the wave of Massachusetts transactions will continue. A number of trends are
NAVIGANT PULSE FALL 2012 | 18
CONTINUED ON NEXT PAGE

becoming more prevalent. Existing stalwart capital providers, as well as newly formed entities, are aggressively pursuing acquisitions. In many cases, new forms of affiliation and partnership are being utilized to combine the resources and balance the needs of the state’s hospitals and systems. Additionally, not-for-profit health systems are evaluating novel approaches to partnerships and ventures to expand their missions. Hospitals across Massachusetts also will begin to explore new avenues of recapitalization without the need to relinquish autonomy or control. Finally, the emergence of cross-vertical transactions between payers, providers and clinicians underscore that the current wave of statewide consolidation is truly without precedent.
With so much uncertainty in the economy and with dramatic healthcare policy shifts looming, Massachusetts residents can probably expect more hospital alliances in the future. When it comes to lowering costs and delivering more efficient and better healthcare, size seems to matter. The era of the stand-alone community hospital may be becoming the exception rather than the rule.
About Jim AgnewJim Agnew is a Managing Director in Navigant Healthcare Strategy Practice. He has 30 years of executive leadership and experience in advisory services, including a unique blend of hospital operations, financial and corporate development expertise that has been tested in both the not-for-profit and investor-owned segments of the healthcare industry. Jim is currently focused on supporting clients engaged in healthcare mergers and acquisitions, pre- and post-merger integration, health system growth strategy and hospital-physician alignment. Prior to Navigant, Jim served in senior leadership positions at HCA and the Bon Secours Health System. He is a Fellow in the American College of Healthcare Executives and frequent guest lecturer at Johns Hopkins, Duke University, ACHE and HFMA on topics related to hospital growth strategy and provider network development. For more information, contact Jim at [email protected] or 617.748.8341.
NAVIGANT PULSE FALL 2012 | 19

The Massachusetts Story: How Payers Are Responding
KEY POINTS
■ A favorable policy environment aids expanded coverage
■ State ‘Connector’ uses leverage to manage cost growth
■ Risk-based bundled payments start replacing fee-for-service
By Catherine Sreckovich
As implementation of the federal Affordable Care Act (ACA) nears, payers are looking to the Massachusetts experience related to its 2006 reform to provide information and caution about healthcare coverage expansions. In considering these experiences, however, it is important to remember that Massachusetts started implementation in a particularly favorable policy environment for expanding coverage. The Massachusetts payer experience, therefore, should be considered in this context. Payers should consider how the policies within each state – policies on Medicaid eligibility and coverage, the makeup of the commercial insurer market, insurance market regulations, unique payer and provider environments and political issues – will influence implementation.
PRE-REFORM MASSACHUSETTSPrior to the 2006 Health Care Reform Act, Massachusetts had taken a number of steps to improve access to health insurance coverage and healthcare services through enhancements to its Medicaid program and insurance market regulation.
Medicaid Massachusetts was one of the states operating under a Federal Section 1115 demonstration waiver that gave it considerable flexibility in operating its Medicaid and Children’s Health Insurance Program (CHIP) programs. Through the waiver, the state pooled funds from a health insurance premium surcharge with state and federal Medicaid funds into a single fund for uncompensated care, which was used to finance and make available safety net services. When the Centers for Medicare & Medicaid Services (CMS) notified the state that it would not extend the waiver upon its June 2006 expiration, putting about $385 million of the state’s $1 billion uncompensated care funding at risk, the state began to consider alternatives that would mesh with private insurance coverage expansions to create greater healthcare coverage access.
Private Insurance Market Specific characteristics of the Massachusetts insurance market created an environment more friendly to reform implementation
NAVIGANT PULSE FALL 2012 | 20
CONTINUED ON NEXT PAGE

and influenced how payers would respond to the reform legislation. For example:
» Uninsured rates (10.6 percent) were low in Massachusetts in comparison to other states.
» Levels of employer-sponsored coverage were high.
» Insurance regulations required guaranteed issue of insurance to individuals and groups and modified community rating.
» Local, non-profit health plans that had historically been rated highly on quality and customer service dominated the market.
» The overall insurance market was less concentrated than in many other states, although there was one large carrier – Blue Cross Blue Shield of Massachusetts – with a significant market share.
IMPLEMENTATION OF HEALTHCARE REFORMHealthcare reform not only created the Commonwealth Health Insurance Connector Authority (Connector)
The transition from fee-for-service payments to value
and/or budget-based payments is already well under
way in Massachusetts. For example, Blue Cross’
Alternative Quality Contract (AQC), in which Steward,
Partners, Atrius and other major provider systems
participate, has, according to a recent Harvard
Medical School Study, in its first year (2009) slowed
the rate of increase in medical expenses and
improved performance on quality measures. All
participating AQC groups met their 2009 budget
targets, and shared in the resulting savings.
Many of these systems also participate in value and/or
budget-based payment arrangements with Harvard
Pilgrim Health Care, Tufts Health Plan and Fallon
Community Health Plan, Massachusetts’ other major
HMOs. Moreover, Steward, Partners, Atrius and three
other Massachusetts systems are among the 32 Pioneer
ACOs that will have the opportunity to share substantial
risk for services to Medicare beneficiaries. According to
the Centers for Medicare & Medicaid Services, the
Pioneer ACO program “is designed for… [systems]
experienced in coordinating care for patients across
care settings… [and will allow them] to move rapidly
from a shared savings payment model to a population-
based payment model.”
As Massachusetts led the nation in expanding health
insurance coverage, Massachusetts payers and
providers are leading the nation in moving from
traditional FFS payments to value and/or budget-
based payments designed to improve quality and slow
the rate of increase in medical expenses and
premiums. This has required a significant commitment
of financial and personnel resources to build the
information technology and other managed care
infrastructure necessary to be successful under value
and/or budget-based payment arrangements. There is
no reason to believe that this preliminary, and we hope
ongoing, success is not replicable in other markets.
Christopher M. Jedrey is a partner in the
law firm of McDermott Will & Emery LLP,
based in the firm’s Boston office. He is
partner-in-charge of its Boston Health
Industry Advisory Practice Group, and
national co-chairman of its Academic Medical
Centers practice. He can be reached at
[email protected] or 617.535.4405.
Move to Value Payments Can Bring SavingsBy Chris Jedrey, McDermott Will & Emery
NAVIGANT PULSE FALL 2012 | 21
CONTINUED ON NEXT PAGE

to oversee the Commonwealth’s Health Insurance Exchange and develop policies for health coverage expansion, but also affected Medicaid and the private insurance market.
Medicaid The state converted the funding for the uncompensated care pool into premium support payments for low-income populations below 300 percent of the federal poverty level. Massachusetts also expanded its Medicaid and SCHIP programs to include children with family incomes up to 300 percent of the federal poverty level.
Private Insurance Market Massachusetts enacted insurance reforms to merge the individual and small group markets to form one risk pool. While the merger resulted in a small increase in insurance premiums, it was moderated by the state’s prior insurance changes aligning the rating and guaranteed issue rules between the two markets. The state required that insurance products be priced the same whether they are marketed inside or outside the Exchange to address the potential for adverse selection. These reforms helped Massachusetts launch and sustain its Exchange with minimal disruption to its insurance markets. In addition, the Connector limited health plans that could operate within the Connector to those applying – and qualifying – for positions as qualified health plans.
POST-IMPLEMENTATIONMedicaid In December 2011, CMS once again renewed the state’s 1115 demonstration waiver. Among the goals of the renewal are to continue to redirect spending on uncompensated care to create Delivery System Transformation Initiatives, designed as incentive payments to support investments in healthcare delivery systems that will support payment reform, and transition away from fee-for-service payments toward alternative payment arrangements that reward high-quality, efficient and integrated systems of care.
Private Insurance Market The Connector used its leverage as a large purchaser to aggressively manage cost growth and produce savings for the state within Commonwealth Care (CommCare), the
subsidized insurance market within the health benefit exchange. CommCare is the access point for subsidized health insurance for approximately 158,000 Massachusetts residents. As such, it is a separate risk pool, with no "outside" market with which to compete. From the inception of CommCare in 2006 through fiscal year 2010, the average annual rate of increase in premiums was held under 5 percent – about half the rate of growth in commercial insurance. The same savings did not occur with CommChoice (small employer, non-subsidized market), which is a relatively small book of business for health plans and where the Connector does not carry the same level of clout.
In 2009, the statutory limitation on health plans’ eligibility for CommCare ended. In this phase of contracting for qualified health plans, the Connector further standardized product designs, so that health plans had to be more innovative to compete based on a level playing field. Some larger carriers with more name recognition lost market share in this price-competitive environment. On the other hand, BMC HealthNet, one of the original managed care organizations in the CommCare program, began offering commercial products through the Connector. Smaller, lesser-known carriers increased market share where consumers could compare products with similar benefits and see, at a glance, which products offered more competitive prices (though there were other factors that influenced a consumer’s decision in purchasing health coverage). In 2009, the Exchange was able to attract the first new insurance carrier – the CeltiCare Health Plan – to enter the Massachusetts market in decades and was successful in garnering lower bids from the other participating plans.
During its 2011-2012 procurement process, the Connector pressed the health plans to produce savings by improving provider contracts, directing members’ care to lower-cost settings, enhancing medical management and improving administrative efficiency. The two plans that offered the lowest rates exclude several high-cost hospitals from their networks, but the Connector determined that all of the health plans’ proposed networks meet the program’s standards for members’ access to care.
NAVIGANT PULSE FALL 2012 | 22
CONTINUED ON NEXT PAGE

The Connector also has managed the cost of CommCare by requiring that new enrollees whose incomes qualify them for fully subsidized coverage (paying no premium) may only choose between the two lowest-cost plan options.
ACCESS VS. COST CONTROLThe focus of healthcare reform in Massachusetts was on expanding access to insurance coverage (not on cost control), and Massachusetts currently has a greater percentage of individuals covered by health insurance than any other state. Health insurance premiums, however, are among the highest in the nation. Per capita spending on healthcare in Massachusetts historically has been the highest in the nation. While the growth in premiums has slowed in recent years, small groups experience the highest growth in rates and rate increases, and overall premium increases continue to outpace inflation. A recent study by the Massachusetts Division of Health Care Policy and Finance concludes that as a result of these trends, group purchasers and individuals are selecting insurance packages with fewer benefits or higher cost-sharing requirements, known as “benefit buy-downs.” This has important implications for providers as well as individuals in terms of access to care.
The state has continued to regulate health plans in an effort to reduce premium rate increases and legislation in 2010 required a Minimum Medical Loss ratio (MLR) of 88 percent in 2011 and 90 percent in 2012 – a financial measurement to encourage health plans to provide value to enrollees by limiting the amount of each premium dollar used to pay overhead expenses. As a result, any reductions in premiums likely will have to result from reductions in medical costs.
The Massachusetts Attorney General’s office, which has authority to review and analyze the reasons why healthcare costs continue to increase faster than general inflation, issued reports in 2010 and 2011 about the increase in healthcare costs. The 2010 report concluded that the healthcare market players – whether insurers, providers, businesses or consumers who pay for health insurance – had not effectively controlled costs because, in part, the
prices negotiated between insurers and providers were not designed to encourage or reward provider efficiency. The 2011 report concluded that the wide variation in payments made by health insurers to providers is not explained by differences in quality of care, the complexity of patients, the proportion of public pay patients or academic status; instead, these wide variations correlated with market leverage: more highly paid providers gained market share at the expense of less costly providers.
As employers have continued to push for more cost-effective products – requesting more limited and tiered networks, high deductible plans, higher up-front deductibles, HMO coinsurance options and benefit buy-down programs – payers in Massachusetts have tried to respond through the development of risk-based bundled payment approaches and other initiatives to move away from fee-for-service payments. Page 24 provides examples of some of these approaches.
Meanwhile, MassHealth has implemented a number of programs within the Medicaid program, also designed to reduce the rate of cost increases, and is continuing to redefine delivery models to provide care that is integrated, coordinated and efficient. For example, MassHealth requires enrollment in managed care for non-institutionalized members under age 65 who do not have other insurance; beneficiaries have a choice of five managed care organizations or the Primary Care Clinician Plan (PCC) Plan. MassHealth also participates in a multi-payer, three-year demonstration project running from April 2011 through April 2014 that includes the PCC Plan, Medicaid and Connector Managed Care Organizations (MCOs), Group Insurance Commission and private payers. This demonstration program covers 46 practice sites, covering approximately 265,000 patients, including 150,000 MassHealth members. The focus of the program is on chronic conditions, including diabetes and pediatric asthma and includes provisions for shared savings.
At the end of July, as part of efforts to limit healthcare cost growth, Massachusetts lawmakers
CONTINUED ON NEXT PAGE
NAVIGANT PULSE FALL 2012 | 23

required Medicaid, the state employee healthcare program and all other state-funded healthcare programs to transition to new healthcare payment methodologies that incentivize the delivery of high-quality, coordinated, efficient and effective healthcare while reducing waste, fraud and abuse. In addition, the new law:
» Promotes transparency and accountability by requiring all healthcare provider systems to register with the state and report regularly on financial performance, market share, cost trends and quality measures;
» Develops a process to track price variation among different healthcare providers over time;
» Establishes a commission to determine and quantify the acceptable and unacceptable factors contributing to price variation among providers.
CONCLUSIONThe potential payer impact of full ACA implementation is difficult to determine because every state is different in terms of its insurance regulations, insurance market and competition,
Blue Cross Blue Shield of Massachusetts launched its
Alternative Quality Contract (AQC) in January 2009. The
AQC is a statewide product that reaches more than 44
percent of the commercial product business. The
objectives of the AQC are to reduce medical spending
growth and improve quality of care and patient
outcomes. BCBS allocates provider groups an annual
budget (risk-adjusted) with a payment differential
based on surplus or deficit, and will pay groups a per
member per month bonus if they meet certain quality
thresholds on ambulatory and inpatient measures.
BCBS Massachusetts introduced Hospital Choice Cost Share
in January 2011. This option offers consumers significantly
lower copayments for choosing any of 53 high-value
hospitals or additional freestanding outpatient centers
for a wide range of services and couples those tiered
copayments with out-of-pocket maximums. More than
40,000 individuals enrolled in this plan in its first few months.
Tufts Health Plan implemented Your Choice plan
options, which incorporate a tiered network with cost-
sharing incentives for members who choose high-quality,
efficient providers.
Harvard Pilgrim Health has implemented risk-based
“global payment” contracts with hospitals and doctors,
reopening contracts with its largest provider groups to
negotiate the new rates and implement new products.
The company established goals to use network and
provider approaches to redirect volume in the short-term
and to reinforce provider change and market
competition in the long-term.
Fallon Community Health Plan has been offering limited
network products. Its Direct Care product offers
consumers average premium savings of 13 percent
compared to its Select Care product, which is itself less
expensive than unlimited products that include all
Massachusetts providers.
Network Health became one of the low-cost CommCare
plans and gained 33 percent market share. It attributed
this performance to holding rates flat by limiting where
patients can receive services, negotiating tougher
contracts with hospitals and providing better oversight of
the sickest patients.
Massachusetts Payers Respond to Push for More Cost-Effective ProductsIn an effort to move away from fee-for-service payments, payers in Massachusetts have developed a
variety of risked-based, bundled payment approaches and other initiatives.
NAVIGANT PULSE FALL 2012 | 24
CONTINUED ON NEXT PAGE

Medicaid eligibility, politics and state willingness to include health plans in greater discussion about the ACA. What is not difficult to predict, however, is the continued pressure by regulators to control premiums and health plans’ own pressures to respond by controlling healthcare costs. The Massachusetts experience suggests that an immediate response is needed to control rising healthcare costs and the tolerance for premium increases may not exist.
Further, even though the ACA includes provisions that address cost control (such as moving from fee-for-service payments to value-based payments for the Medicare population, which includes the creation of integrated delivery systems and better care coordination), they may not create savings quickly enough to make premiums affordable. Payers will need to develop new benefit structures that could potentially reduce coverage and effectively reduce instead of improve access to care. With higher deductibles and coinsurance, providers may need to address increased bad debt or limited coverage of the services they provide. And health plans will have to continue to create competitive products if they operate within the state exchange.
Without meaningful cost reductions, state Medicaid programs will continue to face challenges in paying for services. Even though the federal government will match 90 percent of Medicaid costs for the Medicaid expansion population, states are wrestling with huge Medicaid deficits that are not likely to dissipate by 2014, creating the need to rethink how they finance Medicaid services.
About Catherine SreckovichCatherine Sreckovich is a Managing Director and leads Navigant’s Healthcare Payer Strategy practice. She has extensive experience working with healthcare payers, providers and managed care organizations in the development and review of healthcare delivery and reimbursement systems, healthcare compliance programs, healthcare reform options and healthcare data analysis and litigation support. She has worked with health plans, employers and unions in assessing opportunities for improving health insurance benefit design, the analysis and design of cost containment options, the evaluation of health insurance claims processing operations and the development of claims processing specifications for third-party administrators. She is currently working with states and CMS on the development and implementation of Health Insurance Exchange options. Most recently, Catherine’s practice was engaged as a consultant for the Massachusetts Medicaid Delivery Model Advisory Commission. The commission was established to study comparative costs and benefits of varied care delivery models from the Medicaid program. Contact Catherine at [email protected] or 312.583.5747.
NAVIGANT PULSE FALL 2012 | 25

Navigant news
FOUNDER OF INNOVATIVE CLINICAL TRANSFORMATION CONSULTANCy AND TEAM JOIN NAVIGANTMichael Hill, M.D., founder of EMPATH, an innovative hospital care transformation consulting firm, and his team of seven professionals have joined Navigant’s Healthcare practice. The addition of Dr. Hill, his team and his clinical transformation expertise to Navigant Healthcare’s growing suite of performance improvement solutions will offer Navigant clients further enhancements in creating high-performing healthcare organizations. EMPATH’s client base included more than 100 hospitals nationwide, ranging in size from 200 to 1,000 beds.
Dr. Hill, who joins as a Managing Director, brings to Navigant a comprehensive solution of advisory and workflow expertise, used in conjunction with a technology-enabled tool, to improve the efficiency, service delivery and predictability of hospital operations. The tool is a real-time monitoring and metrics reporting system that identifies substantial operating efficiencies, staffing levels and performance for each of the Key Performance Indicators (KPI) for important areas of the hospital. It is an essential component of the Performance Improvement solution as it enhances the implementation of a system of care that is designed to achieve specified levels of performance.
“The detailed reports identify real-time clinical workflow issues and ensure back-up systems exist to alleviate the process bottleneck,” said Dave Hampshire, Managing Director and leader of the Navigant Healthcare Performance Improvement team. “This clinical transformation solution will
impact hospitals’ patient throughput and overall enhanced operational efficiency, allowing us to deliver a deeper value to our clients.”
The combination of this new solution with Navigant’s current performance improvement strategies allows hospitals to manage capacity with real-time data, to proactively optimize work, and to continuously re-evaluate their efforts.
Dr. Hill founded EMPATH in 1996 after practicing emergency medicine for 15 years and serving as Quality Improvement Director and Medical Director of Operations for Emergency Physicians’ Medical Group. He speaks nationally on reducing Emergency Department patient length of stay and improving ED patient satisfaction. Dr. Hill is past president of the California chapter of the American College of Emergency Physicians.
EMPATH has designed and implemented changes in client operations that decreased inpatient length of stay by more than a day, decreased ED and inpatient cycle times by 30 to 50 percent and increased customer satisfaction scores to above the 90th percentile.
Michael Hill, M.D.
CONTINUED ON NEXT PAGE
NAVIGANT PULSE FALL 2012 | 26

“We have been lucky to work with some of the most innovative hospitals in the country to develop and implement proven solutions that enable a new level of performance and accountability to the market place,” said Dr. Hill. “We believe that Navigant Healthcare is the perfect team to join. Our clients will have access to a national network of more than 500 healthcare consulting professionals who can help us substantially leverage our products and experience. This combination will further assist hospitals in addressing the broader scale impacts of ongoing change in the healthcare industry with a full suite of services.”
Look for further details on the operations maturity model and how we believe it will transform the management of clinical care in an upcoming issue of the Pulse.
For more information, contact Michael Hill at [email protected] or 415.399.2129.
NAVIGANT AT FOREFRONT WITH ADDITION OF NEW ACOSWith the addition of 89 new Medicare Accountable Care Organizations in July – and at least 400 such public and private initiatives underway nationally – Navigant Healthcare has been at the forefront of many of the network development efforts for both payers and providers.
Navigant supports six of the 32 Pioneer ACOs and assists more than 100 health systems and physician organizations with a variety of Center for Medicare and Medicaid Innovation and commercial ACO development initiatives.
The movement to transform into an ACO is no easy task. Navigant offers a unique perspective on not only strategy and design, but also the implementation and operations of high-performing networks and ACOs. Two key observations to date:
Two types – “investors” and “hedgers” – are emerging in the ACO space in response to healthcare reform. The investors believe accountable care is likely, if not inevitable, and are investing to be good at it. Hedgers are hedging their bets and taking steps to not be disadvantaged in the event that accountable care becomes a reality.
Of more immediate concern, there is a lack of credentialed resources that have implemented clinical and financial integration at the point of care at physician practices, hospitals, post-acute care settings and payers.
For more information, please contact Michael Nugent at [email protected] or 312.583.4153 or Melissa Masopust at [email protected] or 312.583.4113.
NAVIGANT PULSE FALL 2012 | 27

Navigant advisors offer their expertiseNavigant is knowledgeable on a variety of healthcare topics that are important to physician practices, healthcare systems and payers. Below are some highlights and links to articles featuring our experts.
MEETING THE CHALLENGE OF CULTURAL CHANGE ON THE PATH TO A HIGH-VALUE FUTURE Navigant Healthcare’s Lisa Rolfe explores the staggering challenges confronting health systems and physicians over the next decade. Opportunities to reduce cost while improving patient care are evident throughout the delivery system. Consider, for example, the opportunity to reduce readmission rates for Medicare patients. Elimination of the 18 percent of total Medicare admissions that are actually readmissions while improving access to patient-centered medical homes could reduce total hospital inpatient activity by more than 25 percent. Effective leaders must address the fundamental behavioral and cultural changes required to effectively move from a fee-for-service to a pay-for-performance delivery system.
POST-ACUTE PARTNERSHIPS TO SUPPORT BUNdLEd PAYMENTS: RISK OR OPPORTUNITY?In this HFMA Payment & Reimbursement Forum article, Navigant Healthcare professionals Rich Bajner, Eric Logue and donna Cameron point to the significant cost containment opportunities in the post-acute realm, suggesting that providers are in a unique position to partner with these organizations to coordinate and manage care, improve outcomes and achieve efficiencies.
INTEGRATED CARE FOR MEDICAID/MEDICARE DUAL ELIGIBLES TAKES OFF This white paper by Navigant Healthcare’s Cheryl Duva and Catherine Sreckovich explores better coordination of healthcare delivery and how spending on dual eligibles has the potential to improve their quality of life and health outcomes while generating tremendous cost savings. This initiative can help bend the cost curve in a meaningful way. Significant programmatic challenges to providing managed care for dual enrollees have resulted in a lack of coordination. Medicare and Medicaid programs have fundamentally different designs that are misaligned in numerous ways, including administrative, reimbursement and data hurdles.
HEALTH BENEFIT EXCHANGES: PREPARATION FOR HOSPITALS Health Benefit Exchanges will not only be the mechanism for the purchasing of health coverage, but they will also be the vehicle that is likely to accelerate the delivery system transformation. This white paper by Navigant Healthcare’s Cheryl Duva, Catherine Sreckovich and Cristine Vogel provides a brief overview of the requirements of Exchanges and how hospitals can begin to prepare for them and the broader impacts of the Accountable Care Act.
For links to these articles and more, visit our Insights & Events page at navigant.com/healthcareinsights
NAVIGANT PULSE FALL 2012 | 28

Upcoming eventsNavigant’s experts speak on a variety of healthcare issues throughout the year. This calendar highlights upcoming events that our experts are participating in across the country.
NOVEMBER 13 – 14Second Annual Health Insurance Exchange Congress
State and Plan Perspectives on Design, Implementation and Ongoing Collaboration for Long-Term Sustainability.
Speaker Cheryl Duva Navigant Healthcare
NOVEMBER 13 – 162012 American Academy of Medical Administrators Annual Conference
“Successful Alignment Models for Physicians and Hospitals”
Speakers Marcel Lisi John Lutz Navigant Healthcare
For links to these events and more, visit our Insights & Events page at navigant.com/insights/events
JANUARy 10 – 12American College of Cardiology Summit
“Excellence – Structures and Governance, Compensation and Performance”
Speakers Jim Palazzo Anthony Long Navigant Healthcare
FEBRUARy 10 – 13
2013 SciQuest NextLevel Conference
Speaker Caroline Kolman Navigant Healthcare
NAVIGANT PULSE FALL 2012 | 29

About NavigantNavigant Healthcare’s 500+ professionals are part of Navigant Consulting, Inc.’s (NySE:NCI) global team of 2,500 employees, dedicated to assisting clients in creating and protecting value in the face of critical business risk and opportunities. These seasoned consulting professionals assist health systems, physician practice groups and payers in designing, developing and implementing integrated solutions that create high-performing healthcare organizations. Through a unique interdisciplinary approach leveraging the depth and breadth of expertise from healthcare executives, clinicians and physicians, the team enables clients to build their capabilities and achieve sustainable peak performance around quality of care, cost, leadership and culture in today’s changing healthcare environment. Through senior level engagement with clients, Navigant professionals combine technical expertise in Disputes and Investigations, Economics, Financial Advisory and Management Consulting, with business pragmatism in the highly regulated Construction, Energy, Financial Services and Healthcare industries.
©2012 Navigant Consulting, Inc. All rights reserved.
Navigant Consulting is not a certified public accounting firm and does not provide audit, attest, or public accounting services.
See navigant.com/licensing for a complete listing of private investigator licenses.
Dave ZitoManaging DirectorNavigant Healthcare Practice [email protected]
Alex HunterManaging DirectorNavigant Healthcare Functional [email protected]
H E A L T H C A R E