Pulmonary valve stenosis regurgitation treatment...
35
Transcript of Pulmonary valve stenosis regurgitation treatment...


PULMONIC STENOSIS

Pulmonic stenosis; Etiology Pulmonic stenosis; Etiology
Odenwald T, EXP REV CARDIOVASC THER 2011Odenwald T, EXP REV CARDIOVASC THER 2011
‘…virtually all cases of pulmonary valve stenosis are congenital in origin’

Severity of the pulmonic stenosis; Severity of the pulmonic stenosis;
DefinitionDefinition
ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008
• Severe pulmonic stenosis: Jet velocity
greater than 4 m per second or
maximum gradient greater than 60 mm
Hg

Pulmonic stenosis; Pulmonic stenosis;
Invasive therapeutical optionsInvasive therapeutical options
1. Balloon valvotomy (Guidelines)
2. Percutaneous pulmonic valve
replacement
3. Surgery (homografts, bioprosthetic/
mechanical valves, conduits)

Pulmonic stenosis; Natural history of Pulmonic stenosis; Natural history of
different subgroupsdifferent subgroups
Nadas et al CIRCULATION 1977, ONadas et al CIRCULATION 1977, O’’ Fallon et al CIRCULATION 1993Fallon et al CIRCULATION 1993
�N=564 (total), n=261 (medical), n=303 (surgery)
�22 years follow-up
�Gradients: a) trivial < 25, b) mild 25 to 49, c) moderate
50 to 79, d) severe> 80
�Medically treated group (trivial to moderate gradients)
•14% of patients gradient increase (children<2y and gradients
>40)
•14% significant gradient decrease
• < 20% required valvotomy

Pulmonic stenosis; Natural history of Pulmonic stenosis; Natural history of
different subgroupsdifferent subgroups
Nadas et al CIRCULATION 1977, ONadas et al CIRCULATION 1977, O’’ Fallon et al CIRCULATION 1993Fallon et al CIRCULATION 1993
�Surgery treated group (moderate to severe gradients)
• 1 death
• Insignificant gradient in 90%
• No recurrence of pulmonic stenosis
�Overall
• Pts with gradients < 25 → 96% free of cardiac
operation
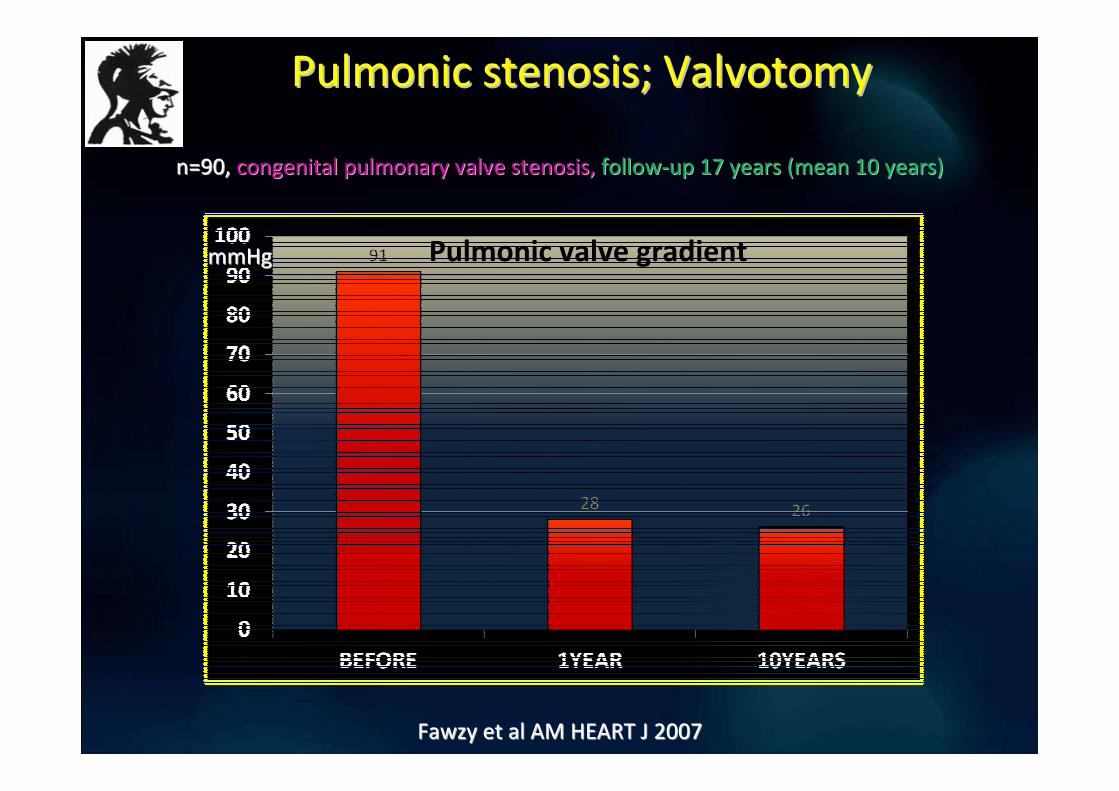
Pulmonic stenosis; ValvotomyPulmonic stenosis; Valvotomy
Fawzy et al AM HEART J 2007Fawzy et al AM HEART J 2007
n=90, n=90, congenital pulmonary valve stenosis, congenital pulmonary valve stenosis, followfollow--up 17 years (mean 10 years)up 17 years (mean 10 years)
mmHgmmHg Pulmonic valve gradient

Pulmonic stenosis; Valvotomy vs SurgeryPulmonic stenosis; Valvotomy vs Surgery
Odenwald et al EXP REV CARDIOVASC THER 2011Odenwald et al EXP REV CARDIOVASC THER 2011
Valvotomy
�Mortality: 3-8%
� Successful reduction of the gradient in 80-90%
�10% restenosis rate in 10 years
Surgery
� Mortality: 0,33-4%
�10 years lifespan for bioprosthetic valves and conduits
� Need for reintervention
� Greater risk for PR and RV dilatation (transannular patch,
conduits)

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
MELODY valve MELODY valve -- MedtronicMedtronic
Odenwald et al EXP REV CARDIOVASC THER 2011Odenwald et al EXP REV CARDIOVASC THER 2011
A trileaflet bovine jugular vein sutured into a platinum–iridium balloon-expandable
stent

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
Edwards Lifesciences SAPIEN
Boone et al CCI 2010Boone et al CCI 2010
Three bovine pericardial leaflets hand-sewn to a tubular, slotted, stainless steel, stent
with fabric sealing cuff covering the lower portion of the stent

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
MELODY vs SAPIEN valveMELODY vs SAPIEN valve
Boone et al CCI 2010Boone et al CCI 2010
Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
Factors to be taken into account Factors to be taken into account
• Size and distensibility of the RVOT/ pulmonary
trunk
• Morphology of the RVOT/pulmonary trunk
• The position of the coronary arteries
Odenwald et al EXP REV CARDIOVASC THER 2011Odenwald et al EXP REV CARDIOVASC THER 2011

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
Selection criteria for MELODY valveSelection criteria for MELODY valve
Size and distensibilitySize and distensibility
Lurz et al Lurz et al Semin Thorac Cardiovasc Surg Pediatr Card Surg Ann 20092009

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
Selection criteria for MELODY valveSelection criteria for MELODY valve
Morphology of the RVOTMorphology of the RVOT
Not suitable for PPVI
Odenwald et al EXP REV CARDIOVASC THER 2011Odenwald et al EXP REV CARDIOVASC THER 2011
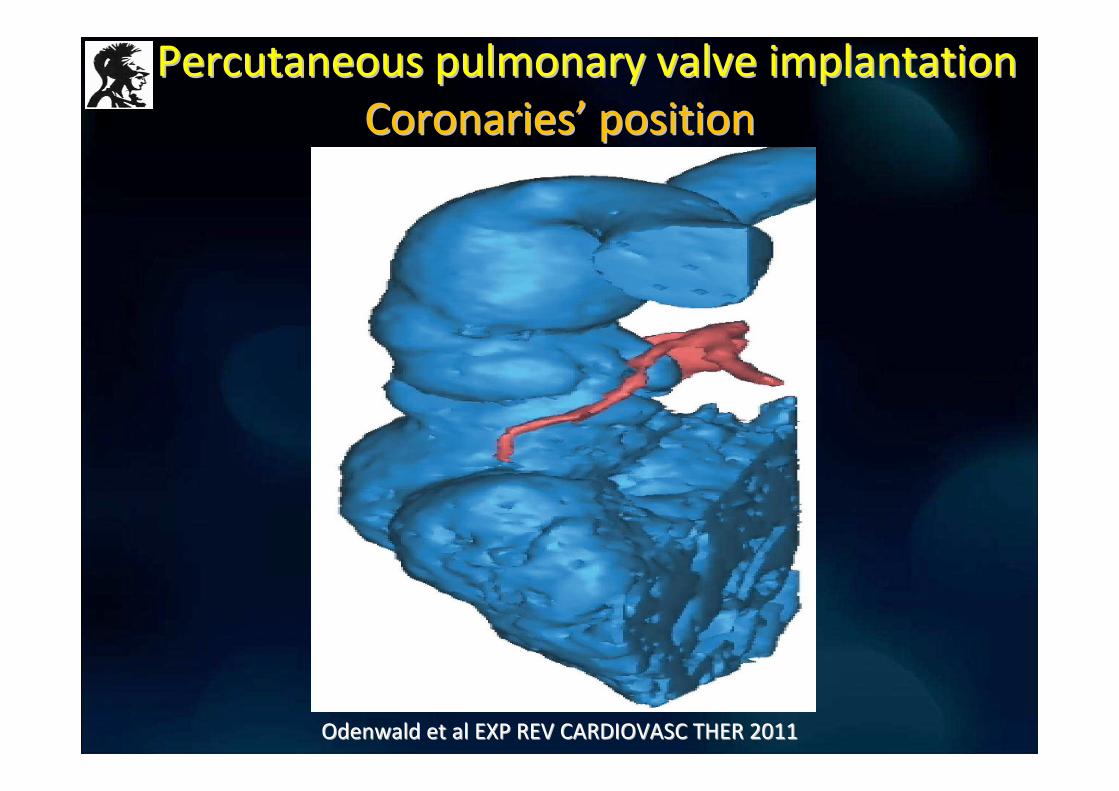
Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
CoronariesCoronaries’’ positionposition
Odenwald et al EXP REV CARDIOVASC THER 2011Odenwald et al EXP REV CARDIOVASC THER 2011

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
MELODY MELODY -- Late resultsLate results
Lurz et al JACC 2011Lurz et al JACC 2011
n=35 PS, n=30 PR, MELODY valve, n=35 PS, n=30 PR, MELODY valve, followfollow--up 1 year up 1 year
1 month 1year
VO2 max improved
only in the PS group
the first month
from 24 to 27
ml/kg/min

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
SAPIEN SAPIEN -- Late resultsLate results
Kenny et al JACC 2011Kenny et al JACC 2011
n=36 dysfunctional RVn=36 dysfunctional RV--PA conduit (severe regurgitation), n=15 severe stenosis, SAPIEN PA conduit (severe regurgitation), n=15 severe stenosis, SAPIEN valve, valve,
followfollow--up 6 months up 6 months
Peak RV-PA gradient

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
MELODY MELODY -- Late resultsLate results
McElhinney et al CIRCULATION 2010et al CIRCULATION 2010
n=136 dysfunctional RVOT conduit or prosthetic valves, n=17 withn=136 dysfunctional RVOT conduit or prosthetic valves, n=17 with Fallot+PS, n=2 PS, MELODY, Fallot+PS, n=2 PS, MELODY,
followfollow--up 2 yearsup 2 years
Peak RV-PA gradient

AHA/ACC GUIDELINESAHA/ACC GUIDELINES
PULMONIC STENOSIS PULMONIC STENOSIS
VALVOTOMYVALVOTOMY
1. In symptomatic adolescent and young adult patients who have:
- exertional dyspnea,
- angina, and
- syncope, or presyncope
an RV–to–pulmonary artery peak-to-peak gradient > 30mmHg (cath)
CLASS I, LEVEL OF EVIDENCE C
2. In asymptomatic adolescent and young adult patients with:
an RV–to–pulmonary artery peak-to-peak gradient > 40mmHg (cath)
ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008

AHA/ACC GUIDELINESAHA/ACC GUIDELINES
PULMONIC STENOSIS PULMONIC STENOSIS
VALVOTOMYVALVOTOMY
CLASS IIb, LEVEL OF EVIDENCE C
In asymptomatic adolescent and young adult patients with:
an RV–to–pulmonary artery peak-to-peak gradient 30-39 mmHg
(cath)
ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008
CLASS III, LEVEL OF EVIDENCE C
In asymptomatic adolescent and young adult patients with:
an RV–to–pulmonary artery peak-to-peak gradient < 30 mmHg (cath)

ESCARDIO GUIDELINESESCARDIO GUIDELINES
Intervention for right ventricular Intervention for right ventricular
outflow tract obstruction outflow tract obstruction
CLASS I, LEVEL OF EVIDENCE C
ESCARDIO Guidelines on Congenital Heart Disease, EUR HEART J 201ESCARDIO Guidelines on Congenital Heart Disease, EUR HEART J 20100
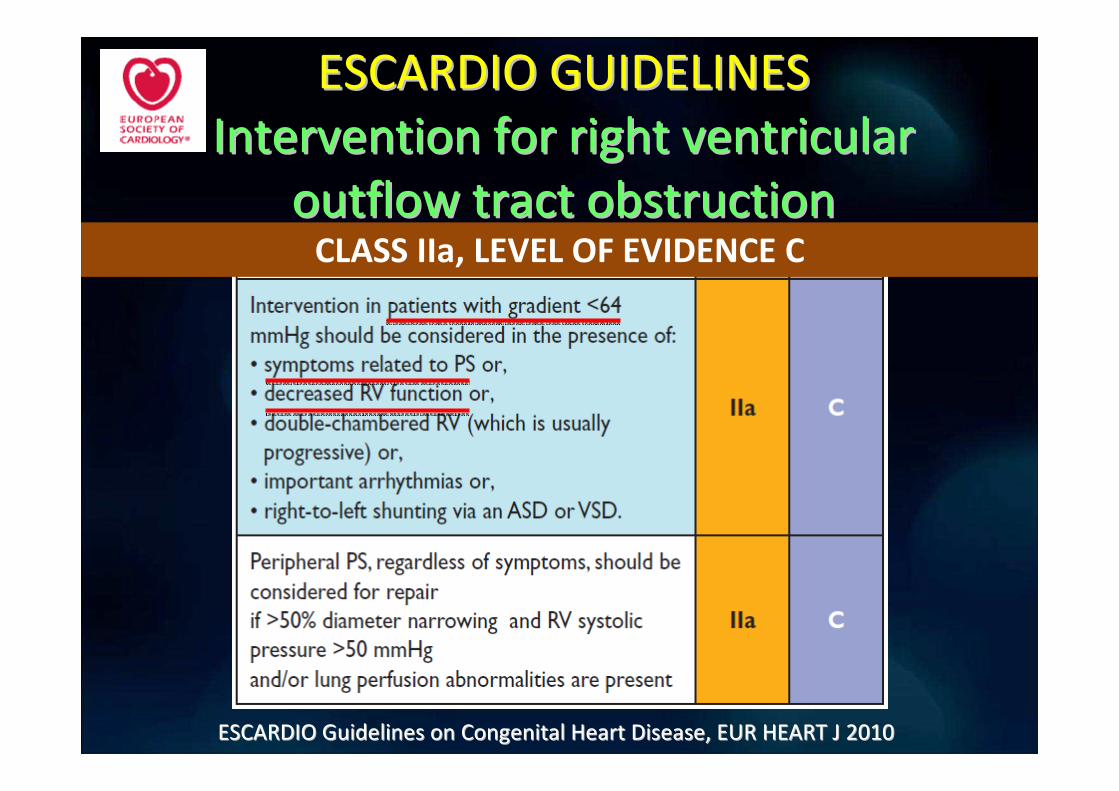
ESCARDIO GUIDELINESESCARDIO GUIDELINES
Intervention for right ventricular Intervention for right ventricular
outflow tract obstruction outflow tract obstruction CLASS IIa, LEVEL OF EVIDENCE C
ESCARDIO Guidelines on Congenital Heart Disease, EUR HEART J 201ESCARDIO Guidelines on Congenital Heart Disease, EUR HEART J 20100

ESCARDIO GUIDELINESESCARDIO GUIDELINES
Intervention for right ventricular Intervention for right ventricular
outflow tract obstruction outflow tract obstruction
•Catheter intervention is recommended for patients with valvular
PS with valves which are not dysplastic (balloon valvotomy) and
with peripheral PS (stent)
•Surgery is recommended for patients with subinfundibular or
infundibular PS and hypoplastic pulmonary annulus, with
dysplastic pulmonary valves (i.e. Noonan’s syndrome), and for
patients with severe PR, TR
•Surgery may be necessary in patients with peripheral PS,
anatomically not amenable for percutaneous therapy
ESCARDIO Guidelines on Congenital Heart Disease, EUR HEART J 201ESCARDIO Guidelines on Congenital Heart Disease, EUR HEART J 20100

PULMONIC REGURGITATION

Pulmonic regurgitation; EtiologyPulmonic regurgitation; Etiology
Fitzerald et al CARD CLIN 2011Fitzerald et al CARD CLIN 2011
1. Dilation of either the pulmonary valve annulus or the
pulmonary artery, secondary to:
i)pulmonary hypertension, ii) idiopathic pulmonary artery
dilation, iii) connective tissue disease
2. Congenital absence of a pulmonary valve leaflet may cause
regurgitation
3. Iatrogenic causes (pulmonary valve trauma related to
balloon valvuloplasty, pulmonary artery catheters, or surgical
repair of congenital heart disease)
Severity of the pulmonic regurgitation; Severity of the pulmonic regurgitation;
DefinitionDefinition
ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008
• Severe pulmonic regurgitation: Color jet
fills outflow tract; dense continuous wave
Doppler signal with a steep deceleration
slope

Pulmonic regurgitation;Pulmonic regurgitation;
Indications for invasive treatmentIndications for invasive treatment
• Patients with NYHA functional class II or III
symptoms and severe pulmonary regurgitation
• For asymptomatic patients, the indications based on
regurgitant fraction, RV end-diastolic or end-systolic
volume, RV ejection fraction and exercise capacity
remain unclear.
ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008ACC/AHA Guidelines on Valvular Heart Disease, CIRCULATION 2008

Pulmonic regurgitation; Pulmonic regurgitation;
Invasive therapeutical optionsInvasive therapeutical options
1. Percutaneous pulmonic valve replacement
2. Surgery (homografts, bioprosthetic/
mechanical valves)

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
MELODY MELODY –– Pulmonic regurgitationPulmonic regurgitation
Vezmar et al, JACC CARDIOVASC INTERV 2010Vezmar et al, JACC CARDIOVASC INTERV 2010
n=28, dysfunctional conduits or homografts, MELODY valve, n=28, dysfunctional conduits or homografts, MELODY valve, followfollow--up 3 yearsup 3 years

Percutaneous pulmonary valve implantationPercutaneous pulmonary valve implantation
MELODY MELODY -- Late resultsLate results
Lurz et al JACC 2011Lurz et al JACC 2011
n=35 PS, n=30 PR, MELODY valve, n=35 PS, n=30 PR, MELODY valve, followfollow--up 1 year up 1 year
1 month 1year
VO2 max improved
only in the PS group
the first month
from 24 to 27
ml/kg/min

ΕυχαριστώΕυχαριστώ πολύπολύ

Back up Back up

CONCLUSIONSCONCLUSIONS
GHZ

Perin E et al, Perin E et al, ACC Scientific Sessions 2012, Chicago, IL ACC Scientific Sessions 2012, Chicago, IL