Pulmonary Project
150
Rehabilitation Systems Pulmonary Care & Rehabilitation Program Implementation Manual
-
Upload
roger-campbell-ms-lion -
Category
Documents
-
view
68 -
download
1
Transcript of Pulmonary Project
Rehabilitation Systems
Pulmonary Care & Rehabilitation Program Implementation Manual

2 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Table of Contents
Overview of Common Pulmonary Conditions ............................................................ 6
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) .................................................... 6 ALPHA-1 ANTITRYPSIN DEFICIENCY ................................................................................ 13 PERSISTENT ASTHMA .................................................................................................... 13 BOOP ......................................................................................................................... 15 BRONCHIECTASIS .......................................................................................................... 17 CYSTIC FIBROSIS (CF) .................................................................................................. 18 IDIOPATHIC PULMONARY FIBROSIS (IPF) ......................................................................... 20 OCCUPATIONAL LUNG DISEASE ....................................................................................... 21 SARCOIDOSIS ............................................................................................................... 22 CHEST WALL DISEASE .................................................................................................. 23 NORMAL STRUCTURE AND FUNCTION ............................................................................. 23 LUNG CANCER .............................................................................................................. 25 PRIMARY VERSUS SECONDARY LUNG CANCER ................................................................ 26 TYPES OF LUNG CANCER............................................................................................... 26
Staging, Diagnostic, Treatment, and Special Considerations ................................. 30
DEFINITIONS ................................................................................................................. 30 PATHOGENESIS AND PATHOLOGY ................................................................................... 31 DIAGNOSIS ................................................................................................................... 31 CLASSIFICATION OF SEVERITY........................................................................................ 32 STAGING OF DISEASE SEVERITY .................................................................................... 34 NATURAL HISTORY AND PROGNOSIS OF COPD ............................................................... 34 SLEEP AND COPD ........................................................................................................ 35 HYPOXEMIA DURING SLEEP IN COPD ............................................................................. 35 COPD AND OBSTRUCTIVE SLEEP APNEA SYNDROME ...................................................... 35
Treatment ..................................................................................................................... 36
TREATMENT OF STABLE COPD ...................................................................................... 36 RECOMMENDATIONS BY PROFESSIONAL SOCIETIES* FOR ................................................. 37 MANAGEMENT OF STABLE COPD .................................................................................. 37 BRONCHODILATORS ...................................................................................................... 39 CORTICOSTEROIDS ....................................................................................................... 40 IMMUNIZATIONS ............................................................................................................ 40 ANTIBIOTICS ................................................................................................................. 41 MUCOKINETIC AGENTS .................................................................................................. 41
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 3
OTHERS ....................................................................................................................... 41
Treatment of Acute Exacerbations of COPD ............................................................. 43
MANAGEMENT OF ACUTE EXACERBATIONS OF COPD ...................................................... 43 OXYGEN THERAPY ........................................................................................................ 44 BRONCHODILATORS ....................................................................................................... 44 ANTIBIOTICS.................................................................................................................. 44 CORTICOSTEROIDS ........................................................................................................ 44 NONINVASIVE POSITIVE PRESSURE VENTILATION AND MECHANICAL VENTILATION .............. 45 OTHERS ....................................................................................................................... 45 CONCLUSION ................................................................................................................ 45 SUMMARY ..................................................................................................................... 45 SUGGESTED READINGS ................................................................................................. 46
Introducing Pulmonary Rehabilitation ....................................................................... 51
Pulmonary Rehab Inclusion Criteria .......................................................................... 52
COPD Rehabilitation Patient Assessment Form ....................................................... 56
Physical Functioning Score (PFS) .............................................................................. 60
Health-Related Quality of Life Survey ........................................................................ 61
Example List of Goals for Pulmonary Patients ......................................................... 62
(MET) to Functional Task Conversions ...................................................................... 63
6 - MINUTE WALK TEST (6MWT) ................................................................................ 65
R P E / FT ...................................................................................................................... 66
DYSPNEA ..................................................................................................................... 67
Speed, Distance, Energy Conversion Chart .............................................................. 68
Plan of Treatment / Exercise Prescription and Progression .................................... 69
COMPONENTS OF AN EXERCISE PRESCRIPTION ............................................................... 70 EXERCISE DOSE – RESPONSE RELATIONSHIP .................................................................. 71 WITH A GRADUAL UPSLOPE IN PROGRESSION ................................................................. 71 GENERAL AEROBIC EXERCISE RECOMMENDATIONS ......................................................... 72 INCREMENTAL EXERCISE PROGRESSION ......................................................................... 73 WORK-REST RATIO ....................................................................................................... 74 FUNDAMENTALS OF RESISTANCE TRAINING: PROGRESSION AND EXERCISE PRESCRIPTION . 74
Individual Therapeutic Session, SOAP note format ................................................. 75 4 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
SOAP NOTE ............................................................................................................... 77
Pulmonary Patient Education ..................................................................................... 78
Early Warning Signs of Respiratory Exacerbations ................................................. 80
Five-Finger Fly-By Assessment ................................................................................. 81
Exacerbation / Distress Interventions ....................................................................... 82
Energy Conservation .................................................................................................. 85
Relaxation and Stress Management .......................................................................... 87
Dietary Guidelines for Pulmonary Patients ............................................................... 89
Pulmonary Rehabilitation Case Study ....................................................................... 93
Breathing Retraining ................................................................................................... 99
Chest Physical Therapy ............................................................................................ 103
Oxygen Delivery Systems ......................................................................................... 108
COPD Medications .................................................................................................... 112
Pulmonary Rehabilitation goals-building blocks for writing functional goals ..... 112
Common (MET) to Functional Task Conversions (Short List) ............................... 113
The Compendium of Physical Activities Tracking Guide (Long List) ................... 119
Pulmonary Rehabilitation Progress Report ........................................................... 132
NOTES ................................................................................ Error! Bookmark not defined.
Course Evaluation ..................................................................................................... 136
COPD Glossary .......................................................................................................... 140
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 5

OVERVIEW OF COMMON PULMONARY CONDITIONS
Chronic Obstructive Pulmonary Disease (COPD) Pulmonary diseases are becoming more important causes of morbidity and mortality in the modern world, with COPD being the most common and a major cause of lung-related death and disability. In the United States, COPD accounted for 119,000 deaths in 2000, ranking it the fourth leading cause of death and the only major disease among the top 10 that continues to increase. Mortality data tend to underestimate the impact of COPD because it is more likely to be listed as contributory rather than the underlying cause of death, and is often not listed at all. Between 1980 and 2000, death rates for COPD increased 282% for women compared to 13% for men. Also in 2000, the number of women dying from COPD exceeded the number of men.
JAMA. 2005; 294 (10) : 1255-1259 Chronic obstructive pulmonary disease (COPD) is a lung disease characterized by chronic obstruction of lung airflow that interferes with normal breathing and is not fully reversible. The more familiar terms 'chronic bronchitis' and 'emphysema' are no longer used, but are now included within the COPD diagnosis. COPD is not simply a "smoker's cough" but an under-diagnosed, life-threatening lung disease. A COPD diagnosis should be considered in any patient who has symptoms of cough, sputum production, or dyspnea (difficult or labored breathing), and/or a history of exposure to risk factors for the disease. Where spirometry is unavailable, the diagnosis of COPD should be made using all available tools. Clinical symptoms and signs, such as abnormal shortness of breath and increased forced expiratory time, can be used to help with the diagnosis. A low 6 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
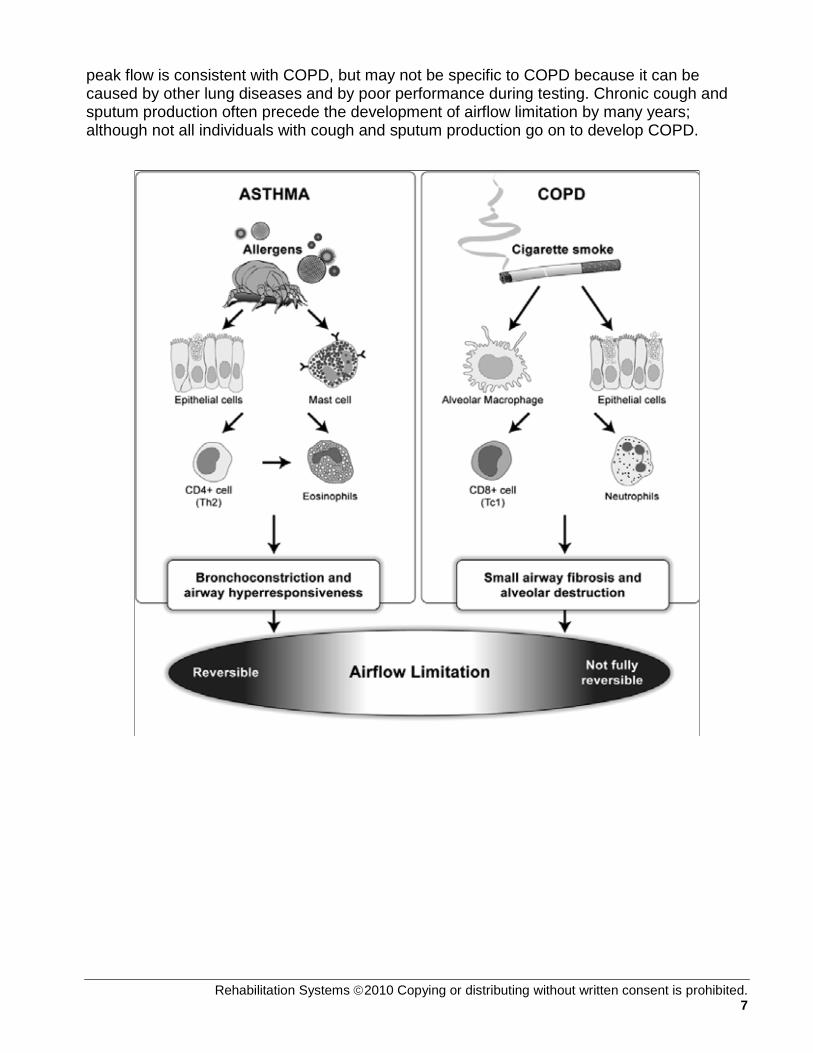
peak flow is consistent with COPD, but may not be specific to COPD because it can be caused by other lung diseases and by poor performance during testing. Chronic cough and sputum production often precede the development of airflow limitation by many years; although not all individuals with cough and sputum production go on to develop COPD.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 7

COPD is a progressive disease that makes it hard to breathe. COPD can cause coughing that produces large amounts of mucus, wheezing, shortness of breath, chest tightness, and other symptoms. Cigarette smoking is the leading cause of COPD. Most people who have COPD smoke or used to smoke. Long-term exposure to other lung irritants, such as air pollution, chemical fumes, or dust, also may contribute to COPD.
8 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

The air that you breathe goes down your windpipe into tubes in your lungs called bronchial tubes, or airways.
Slide A shows the location of the respiratory structures in the body. Slide B is an enlarged image of airways, alveoli, and the capillaries. Slide C shows the location of gas exchange between the capillaries and alveoli. The airways are shaped like an upside-down tree with many branches. At the end of the branches are tiny air sacs called alveoli. The airways and air sacs are elastic. When you breathe in, each air sac fills up with air like a small balloon. When you breathe out, the air sac deflates and the air goes out. In COPD, less air flows in and out of the airways because of one or more of the following: The airways and air sacs lose their elastic quality. The walls between many of the air sacs are destroyed. The walls of the airways become thick and inflamed (swollen). The airways make more mucus than usual, which tends to clog the airways. Healthy Alveoli and Damaged Alveoli
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 9
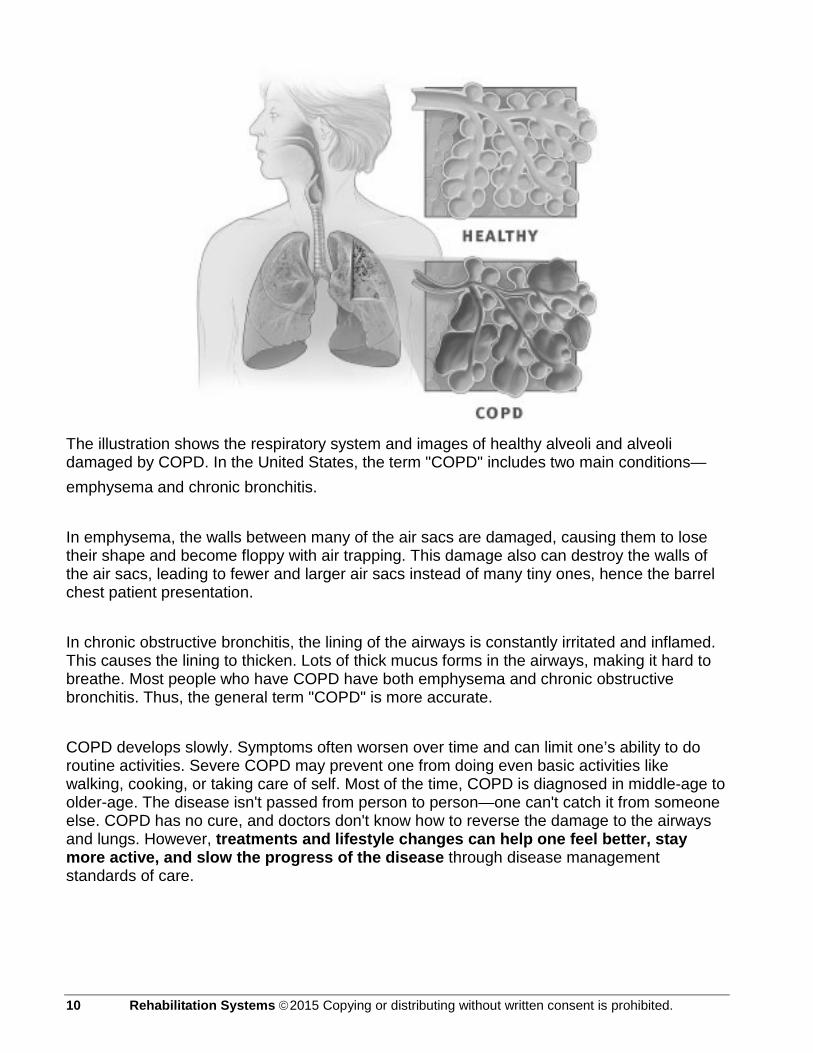
The illustration shows the respiratory system and images of healthy alveoli and alveoli damaged by COPD. In the United States, the term "COPD" includes two main conditions— emphysema and chronic bronchitis. In emphysema, the walls between many of the air sacs are damaged, causing them to lose their shape and become floppy with air trapping. This damage also can destroy the walls of the air sacs, leading to fewer and larger air sacs instead of many tiny ones, hence the barrel chest patient presentation. In chronic obstructive bronchitis, the lining of the airways is constantly irritated and inflamed. This causes the lining to thicken. Lots of thick mucus forms in the airways, making it hard to breathe. Most people who have COPD have both emphysema and chronic obstructive bronchitis. Thus, the general term "COPD" is more accurate. COPD develops slowly. Symptoms often worsen over time and can limit one’s ability to do routine activities. Severe COPD may prevent one from doing even basic activities like walking, cooking, or taking care of self. Most of the time, COPD is diagnosed in middle-age to older-age. The disease isn't passed from person to person—one can't catch it from someone else. COPD has no cure, and doctors don't know how to reverse the damage to the airways and lungs. However, treatments and lifestyle changes can help one feel better, stay more active, and slow the progress of the disease through disease management standards of care.
10 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 11

12 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Alpha-1 Antitrypsin Deficiency Alpha-1 antitrypsin deficiency, or A1A deficiency, is a condition that raises your risk for certain types of lung disease, especially if you smoke. A1A deficiency is an inherited condition; it's passed in the genes from parents to children. Some people who have severe A1A deficiency develop emphysema, often when they're only in their forties or fifties. Emphysema is a serious lung disease in which damage to the airways makes it hard to breathe. A smaller number of people who have A1A deficiency have cirrhosis and other serious liver diseases. Cirrhosis is a disease in which the liver is scarred. This prevents the liver from working properly. In people who have A1A deficiency, cirrhosis and other liver diseases usually occur in infancy and early childhood. A very small number of people who have A1T deficiency have a rare type of skin disease called necrotizing panniculitis. This skin disease can cause painful lumps under or on the surface of the skin. Alpha-1 antitrypsin, is a protein made in the liver. Normally, the protein goes into the bloodstream and helps protect the body's organs from the harmful effects of other proteins. One of the main organs it protects is the lungs. A1A deficiency occurs when the A1A proteins made in the liver aren't the right shape. They get stuck inside liver cells and can't get into the bloodstream. Because not enough A1A protein travels to the lungs to protect them, the risk of lung disease increases. Also, because too many A1A proteins are stuck in the liver, liver disease can develop.
Persistent Asthma Persistent asthma is a chronic inflammatory pulmonary disorder that is characterized by reversible obstruction of the airways. The underlying cause of the increasing prevalence of asthma is unknown. However, the airway inflammation that is noted in asthma is due to an immune-mediated process in which inflammatory cells and inflammatory mediators enter airway tissues to cause disease. Many cell-mediated immunologic factors participate in the inflammatory process of asthma. The most important inflammatory cells involved are eosinophils, mast cells, and T lymphocytes. Important aspects that define asthma include airway hyperresponsiveness and bronchoconstriction. Airway hyperresponsiveness refers to an increased tendency of the asthmatic airway to react to a variety of stimuli that would not cause a response in a normal airway. These asthma triggers can cause an asthma attack in an inflamed airway. Bronchoconstriction refers to a narrowing of the airways that causes obstruction of airflow (sometimes termed airflow limitation). The bronchoconstriction of asthma is unique because it is at least partly reversible, either spontaneously or with treatment. When inflamed airways respond to an asthma trigger through bronchoconstriction, the characteristic symptoms of asthma appear namely wheezing, cough, and chest tightness or dyspnea. Wheezing is due to airflow limitation, causing a high-pitched whistling sound, which is usually heard on expiration, but it may also be heard on inspiration. Cough probably results from stimulation of sensory nerves in the airways by inflammatory mediators that are released by various inflammatory cells involved in asthma. Chest tightness or dyspnea is the sensation associated with the increased work needed to breathe when the airways are constricted that patients often feel.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 13
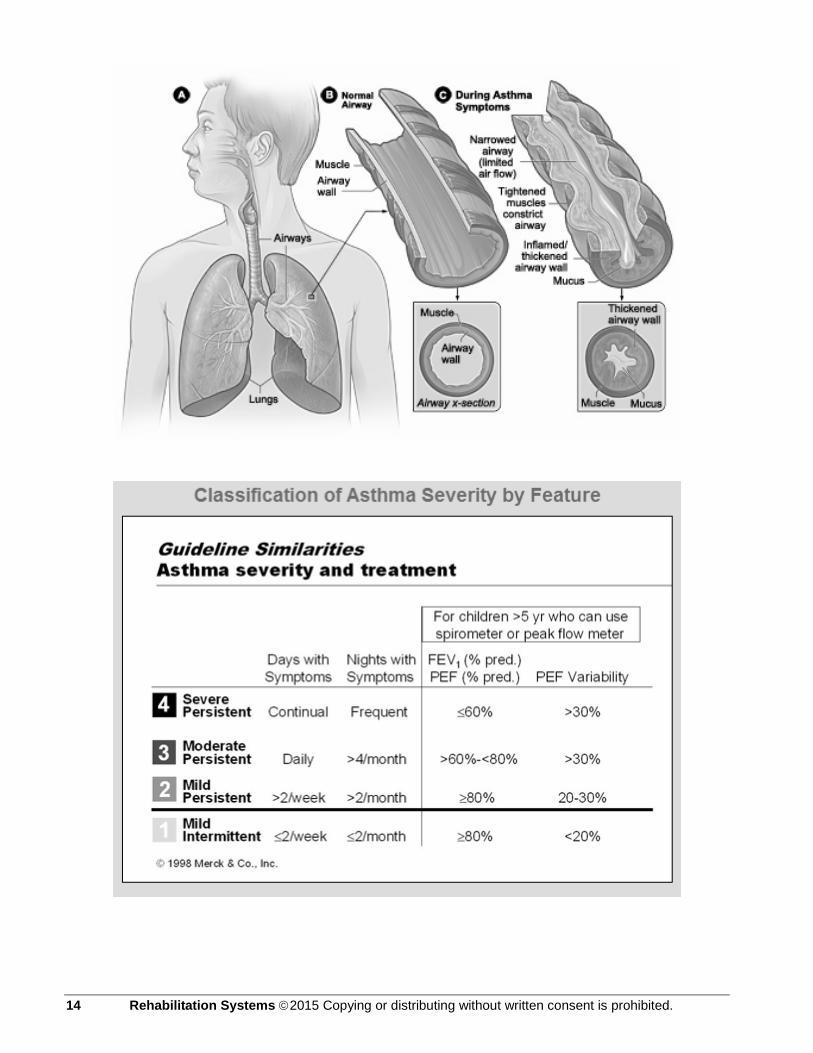
14 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
BOOP Bronchiolitis Obliterans Organizing Pneumonia. BOOP is inflammation in the lungs. Bronchiolitis is inflammation of the very small airways called the bronchioles, less than one millimeter in diameter. There are over 200,000 of these airways. Obliterans means that the inflammation in these small airways completely fills the bronchioles and obliterates the opening of the airway with inflammation. Organizing is a term used to describe the pattern of the inflammation cells. Pneumonia means that the lung is filled with inflammation, where the blood takes up oxygen. The rounded structures where this occurs are called alveoli. There are millions of them. If unfolded, they create an area the size of a tennis court. Dr. Epler first reported BOOP in 1985. Dr. Epler reported about 50 individuals who developed a flu-like illness, "crackles" in the lungs, and lung function tests that showed a decreased lung capacity and a decreased diffusion of oxygen into the blood. The chest x-ray showed "patchy shadows" in both lungs. Dr. Epler named this illness bronchiolitis obliterans organizing pneumonia (BOOP) because this is the pattern seen by the pathologists - doctors who examine lung tissue material. Some colleagues refer to it as Epler's pneumonia. Most of the time, about 80% of the time, the cause of BOOP is not known and referred to as idiopathic BOOP. BOOP may be caused by an infection such as a virus or unusual bacteria can cause BOOP. There has been a report of BOOP caused by the malaria parasite. BOOP may be caused by medications. These include some anti-cancer medications - rituximab therapy for non-Hodgkin's lymphoma.
Conditions and circumstances that have been shown to be associated with BOOP include: • A heart-lung, lung or bone marrow transplant • infection by a virus or unusual bacteria • Anti-cancer medications such as chemo therapy • Long term use of antibiotics • Illicit use of cocaine • Some connective tissue disorders such as lupus and rheumatoid arthritis • Exposure to toxins and fumes, especially NO2 and old textile dye processes
There are miscellaneous causes or associated disorders. Almost every month, there are new reports. For example, BOOP occurs after radiation therapy for breast cancer. BOOP is associated with lymphoma or other cancers. BOOP has occurred in textile workers exposed to an unusual type of textile dye. Remarkably, a high dose of L-Tryptophan, a popular supplement among health enthusiasts for use in sleep and pain disorders, can cause BOOP. There has been a report of BOOP from exposure to a high concentration of mold dust.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 15

BOOP may also be secondary to an underlying lung disease. For example, BOOP may be the inflammation associated with idiopathic pulmonary fibrosis (IPF), which is also called usual interstitial pneumonia (UIP). This is a progressive scarring lung disease. Anyone, anywhere in the world can get BOOP. It occurs in both men and women equally. It usually develops between the ages of 40 years and 60 years. It can occur in children and in patients over 80 years old. BOOP may occur at any time of the year.
16 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
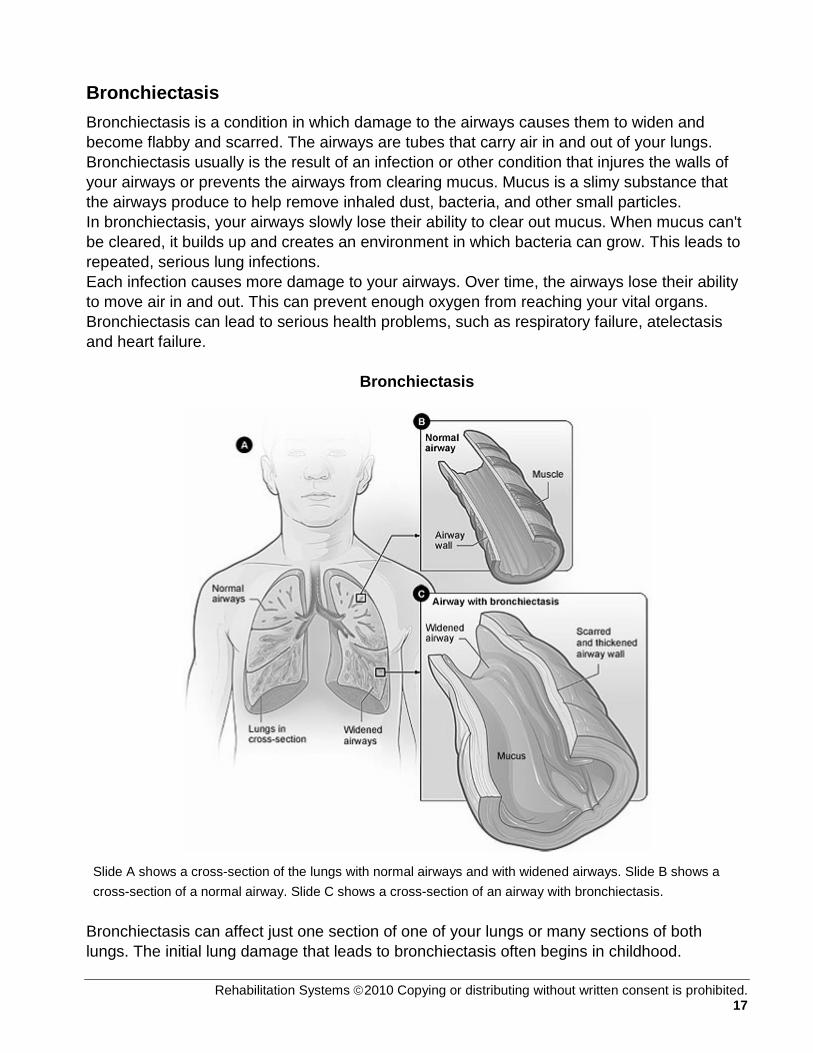
Bronchiectasis Bronchiectasis is a condition in which damage to the airways causes them to widen and become flabby and scarred. The airways are tubes that carry air in and out of your lungs. Bronchiectasis usually is the result of an infection or other condition that injures the walls of your airways or prevents the airways from clearing mucus. Mucus is a slimy substance that the airways produce to help remove inhaled dust, bacteria, and other small particles. In bronchiectasis, your airways slowly lose their ability to clear out mucus. When mucus can't be cleared, it builds up and creates an environment in which bacteria can grow. This leads to repeated, serious lung infections. Each infection causes more damage to your airways. Over time, the airways lose their ability to move air in and out. This can prevent enough oxygen from reaching your vital organs. Bronchiectasis can lead to serious health problems, such as respiratory failure, atelectasis and heart failure.
Bronchiectasis
Slide A shows a cross-section of the lungs with normal airways and with widened airways. Slide B shows a cross-section of a normal airway. Slide C shows a cross-section of an airway with bronchiectasis.
Bronchiectasis can affect just one section of one of your lungs or many sections of both lungs. The initial lung damage that leads to bronchiectasis often begins in childhood.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 17

However, symptoms may not appear until months or even years after you start having repeated lung infections. In the United States, common childhood infections, such as whooping cough and measles, used to cause many cases of bronchiectasis. However, these causes are now less common due to the use of vaccines and antibiotics. Now, in the United States, bronchiectasis usually is due to an underlying medical condition that injures the airway walls or prevents the airways from clearing mucus. Examples of such conditions include cystic fibrosis and primary ciliary dyskinesia.
Cystic Fibrosis (CF) Cystic fibrosis, or CF, is an inherited disease of your secretory glands, including the glands that make mucus and sweat. People who have CF inherit two faulty CF genes—one from each parent. The parents likely don't have the disease themselves. CF mostly affects the lungs, pancreas, liver, intestines, sinuses, and sex organs.
Mucus is a substance made by the lining of some body tissues. Normally, mucus is a slippery, watery substance. It keeps the linings of certain organs moist and prevents them from drying out or getting infected. However, if one has CF, the mucus becomes thick and sticky. The mucus builds up in one’s lungs and blocks the airways. The buildup of mucus makes it easy for bacteria to grow. This leads to repeated, serious lung infections. Over time, these infections can severely damage the lungs. The thick, sticky mucus also can block tubes, or ducts, in the pancreas. As a result, the digestive enzymes that the pancreas makes can't reach the small intestine.
18 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

These enzymes help break down the food that one eats. Without them, the intestines can't fully absorb fats and proteins. This can cause vitamin deficiency and malnutrition because nutrients leave the body unused. It also can cause bulky stools, intestinal gas, a swollen belly from severe constipation, and pain or discomfort. CF also causes the sweat to become very salty. As a result, the body loses large amounts of salt when one sweats. This can upset the balance of minerals in the blood and cause a number of health problems. Examples include dehydration, increased heart rate, tiredness, weakness, decreased blood pressure, heat stroke, and, rarely, death. If one has CF, they are also at increased risk for diabetes or osteoporosis. CF also causes infertility in men, and it can make it harder for women to get pregnant. The symptoms and severity of CF vary from person to person. Some people who have CF have serious lung and digestive problems. Other people have more mild disease that doesn't show up until they're adolescents or adults. The symptoms and severity of CF also vary over time. Sometimes, one will have few symptoms. Other times, the symptoms may become more severe. As the disease gets worse, one will have more severe symptoms more often. Lung function often starts to decline in early childhood in people who have CF. Over time, permanent damage to the lungs can cause severe breathing problems. Respiratory failure is the most common cause of death in people who have CF. As treatments for CF continue to improve, so does life expectancy for those who have the disease. Today, some people who have CF are living into their forties, fifties, or older. Early treatment for CF can improve both your quality of life and lifespan. Such early treatment includes nutritional and respiratory therapies, medicines, exercise rehabilitation, and deliberate physical activity plans.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 19

Idiopathic Pulmonary Fibrosis (IPF) Pulmonary fibrosis is a condition in which tissue deep in the lungs becomes thick and stiff, or scarred, over time. The development of the scarred tissue is called fibrosis. As the lung tissue becomes thicker, the lungs lose their ability to move oxygen into the bloodstream. As a result, one’s brain and other organs don't get the oxygen they need. In some cases, doctors can find out what is causing the fibrosis. But in most cases, they can't find a cause. They call these cases idiopathic pulmonary fibrosis (IPF). IPF is a serious condition. About 200,000 Americans have it. About 50,000 new cases are diagnosed each year. IPF mostly affects people who are 50 to 75 years of age. IPF varies from person to person. In some people, the lung tissue quickly becomes thick and stiff. In others, the process is much slower. In some people, the condition stays the same for years. IPF has no cure yet. Many people live only about 3 to 5 years after diagnosis. The most common cause of death related to IPF is respiratory failure. Other causes include:
• Pulmonary hypertension • Heart failure • Pulmonary embolism • Pneumonia • Lung Cancer
Some people may be more likely to develop IPF because of their genes (the basic units of heredity). If more than one member of your family has IPF, the condition is called familial idiopathic pulmonary fibrosis. Today, scientists are beginning to understand more about what causes IPF, and they can diagnose it more quickly. They also are studying several medicines that may slow the progress of the disease. These efforts should improve the lifespan and quality of life for people who have IPF. In IPF, lung tissue becomes scarred. The scarring typically starts at the edges of the lungs and progresses towards the center of the lungs, making it more and more difficult for a person to breathe. Unfortunately, IPF is a disabling disease that can be fatal.
20 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Occupational lung disease Occupational lung diseases are a branch of occupational diseases concerned primarily with work related exposures to harmful substances, be they dusts or gases, and the subsequent pulmonary disorders that may occur as a result. Substances known to cause lung disease include coal dust, asbestos, silicon and barium. An occupational disease is any chronic ailment that occurs as a result of work or occupational activity. An occupational disease is typically identified when it is shown that it is more prevalent in a given body of workers than in the general population, or in other worker populations. Occupational hazards that are of a traumatic nature (such as falls by roofers) are not considered to be occupational diseases.
U.S. Department of Labor's Mine Safety and Health Administration (MSHA) Mandated plans for reducing Black Lung Disease. 12-03-09.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 21

Sarcoidosis Sarcoidosis is a disease of unknown cause that leads to inflammation. It can affect various organs in the body. Normally, your immune system defends your body against foreign or harmful substances. For example, it sends special cells to protect organs that are in danger. These cells release chemicals that recruit other cells to isolate and destroy the harmful substance. Inflammation occurs during this process. Once the harmful substance is destroyed, the cells and the inflammation dissipate. In people who have sarcoidosis, the inflammation doesn't go away. Instead, some of the immune system cells cluster to form lumps called granulomas in various organs in your body.
Sarcoidosis can affect any organ in your body. However, it's more likely to occur in some organs than in others. The disease usually starts in the lungs, skin, and/or lymph nodes (especially the lymph nodes in your chest). The disease also often affects the eyes and the liver. Although less common, sarcoidosis can affect the heart and brain, leading to serious complications. If many granulomas form in an organ, they can affect how the organ works. This can cause signs and symptoms. Signs and symptoms vary depending on which organs are affected. Many people who have sarcoidosis have no symptoms or mild symptoms. Lofgren's syndrome is a classic set of signs and symptoms that is typical in some people who have sarcoidosis. Lofgren's syndrome may cause fever, enlarged lymph nodes, arthritis (usually in the ankles), and/or erythema nodosum. Erythema nodosum is a rash of red or reddish-purple bumps on your ankles and shins. The rash may be warm and tender to the touch.
The outcome of sarcoidosis varies. Many people recover from the disease with few or no long-term problems. More than half of the people who have sarcoidosis have remission within 3 years of diagnosis. Two-thirds of people who have the disease have remission within 10 years of diagnosis. People who have Lofgren's syndrome usually have remission. Relapse 1 or more years after remission occurs in less than 5 percent of patients. Sarcoidosis leads to organ damage in about one-third of the people diagnosed with the disease. Damage may occur over many years and involve more than one organ. Rarely, sarcoidosis can be fatal. Death usually is the result of complications with the lungs, heart, or brain.
22 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Chest Wall Disease The chest wall is a critical component of the respiratory pump. Diseases that alter the structure of the chest wall affect the function of the pump, and may result in respiratory compromise or failure. The components of the chest wall include the bony structures (ribs, spine), respiratory muscles, and nerves connecting the central nervous system with the respiratory muscles. Chest wall structure and physiology and diseases that affect the bony portion of the chest wall will be reviewed here. Included are discussions of the following conditions: Ankylosing spondylitis Congenital deformities Flail chest Kyphoscoliosis Fibrothorax Obesity and ascites Chest wall tumors
Normal Structure and Function The rib cage and vertebral column form the boundaries of the chest wall superiorly and laterally, while the diaphragm constitutes the inferior component. Changes in the intra-abdominal contents or compliance of the abdominal wall alter the mechanical properties of the chest wall through their effects on the motion of the diaphragm. The external boundary of the lower chest wall is the lower border of the rib cage, but internally, this boundary overlaps with the diaphragm, which covers as much as one-half of the rib cage at residual volume (RV). By virtue of this "zone of apposition" between the diaphragm and the ribs, the rib cage is exposed both to abdominal and pleural pressures, such that the normal function of the chest wall depends on the intricate interaction of the two spaces. The mechanics of the chest wall are described by a pressure-volume curve.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 23

In the upright position, the resting volume of the chest wall is approximately 75 percent of vital capacity (VC). The rib cage recoils outward when the volume is smaller and recoils inward when the volume is larger. In contrast, the resting volume of the respiratory system as a whole — the functional residual capacity (FRC) — is approximately 35 percent of VC. This measure takes into account the mechanical properties of the chest wall plus the inward recoil of the lung.
24 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Lung Cancer Lung cancer is the uncontrolled growth of abnormal cells in one or both lungs. These abnormal cells do not carry out the functions of normal cells and do not develop into healthy lung tissue. As they grow, the abnormal cells can form tumors and impede the function of the lung, which is to provide oxygen to the body via the blood. There are different types of lung cancer and each type is treated differently. THE GENETIC BASIS OF LUNG CANCER All cells in the body contain the genetic material called deoxyribonucleic acid (DNA). Every time a mature cell divides into two daughter cells, it replicates its DNA exactly. The daughter cells are clones of the original cell, identical in every way. It is in this way that our bodies continually replenish themselves. Old cells die off and the next generation takes their place. A cancer begins with an error, or mutation, in a cell's DNA. DNA mutations can be caused by the normal aging process or through environmental factors, such as cigarette smoke or breathing in asbestos. Researchers have found that it takes a series of genetic changes to create a lung cancer cell. Before becoming fully cancerous, cells can be precancerous, which means they have some irregularities (mutations) but still function as lung cells. However, precancerous changes may signify progression toward cancer. When a cell with a genetic mutation divides, it passes along its abnormal genes to the two daughter cells, which then divide into four cells with errors in their DNA and so on. Once a cell has a genetic mutation, it may develop more. With each new mutation, the cell becomes more irregular and may not be as effective in carrying out their function in lung tissue. At a later stage of disease, some cells can migrate away from the main tumor and start growing in other parts of the body. These sites are called metastases. Series of Genetic Changes For lung cancer to develop, suppressor genes (genes that normally serve as the brakes on cellular growth), and oncogenes (genes that encourage the cell to divide), have become mutated. Unlimited growth, in the face of no mechanism to stop or slow the growth, is what fuels the cancer. Other genetic changes occur in cancer as well. Researchers have pinpointed changes to specific genes that contribute to the disease and hope one day to develop specific agents to act on these changes before they can snowball into cancer. Already, some targeted therapies and chemoprevention agents have been developed that work this way.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 25

Primary versus Secondary Lung Cancer Primary lung cancer starts in the lungs. The cancer cells are abnormal lung cells. Sometimes, people will have cancer from another part of their body travel, or metastasize, to their lungs. This is called secondary lung cancer, because the lungs are secondary compared to the original, primary, and location of the cancer. Secondary lung cancer is not lung cancer, but rather the type of cancer from its original site, such as breast cancer. Secondary lung cancer will be treated differently than primary lung cancer, because it is a different disease.
Types of Lung Cancer There are two main types of lung cancer, non-small cell lung cancer and small cell lung cancer. These names refer to how the cancers look under a microscope to a pathologist. Most cancers are non-small cell. There are subtypes of non-small cell lung cancer. Because different types of lung cancer are treated differently, oncologists will determine exactly what treatment is best. NON-SMALL CELL LUNG CANCER (NSCLC) NSCLC accounts for about 80% of lung cancers. There are different types of NSCLC, including
• Squamous cell carcinoma (also called epidermoid carcinoma). This is the most common type of NSCLC. It forms in the lining of the bronchial tubes and is the most common type of lung cancer in men.
• Adenocarcinoma. This cancer is found in the glands of the lungs that produce mucus. This is the most common type of lung cancer in women and also among people who have not smoked.
• Bronchioalveolar carcinoma. This is a rare subset of adenocarcinoma. It forms near the lungs' air sacs. Recent clinical research has shown that this type of cancer responds more effectively to Targeted therapies -Targeted therapies: These therapies include monoclonal antibodies, anti-angiogenesis drugs, and growth factor inhibitors, are designed to treat only the cancer cells, thus sparing normal cells from damage.
• Large-cell undifferentiated carcinoma. This cancer forms near the surface, or outer edges, of the lungs. It can grow rapidly.
SMALL CELL LUNG CANCER (SCLC) SCLC accounts for about 20% of all lung cancers. Although the cells are small, they multiply quickly and form large tumors that can spread throughout the body. Smoking is almost always the cause of SCLC.
26 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
References: Jaeschke R, O’Byrne PM, Mejza F, et al. The safety of long-acting beta-agonists among patients with asthma using inhaled corticosteroids: systematic review and metaanalysis. Am J Respir Crit Care Med. 2008; 178:1009-16. Results of the above SMART study have prompted greater scrutiny of long-acting beta-agonist use. This meta-analysis suggests these medications do not reduce or increase the risk of asthma-related admits or all-cause mortality when administered concomitantly with inhaled corticosteroids. The analysis was not able to address risk based on race or in children. Nelson HS, Weiss ST, Bleecker ER, et al, SMART Study Group. The salmeterol multicenter asthma research trial. Chest 2006; 130:928. This randomized, double-blinded, placebo-controlled, observational study (N= 26,355) showed a small, but statistically significant increase in respiratory-related and asthma-related deaths for the population receiving salmeterol. It is uncertain whether poor outcomes were due to physiologic treatment effects, genetic factors, lack of concomitant inhaled corticosteroid use, or patient behaviors. Jaeschke R, O’Byrne PM, Mejza F, et al. The safety of long-acting beta-agonists among patients with asthma using inhaled corticosteroids: systematic review and metaanalysis. Am J Respir Crit Care Med. 2008; 178:1009-16. Results of the above SMART study have prompted greater scrutiny of long-acting beta-agonist use. This meta-analysis suggests these medications do not reduce or increase the risk of asthma-related admits or all-cause mortality when administered concomitantly with inhaled corticosteroids. The analysis was not able to address risk based on race or in children. Haahtala T, Jarvinen M, Kava T, et al. Comparison of a beta-agonist, terbutaline, with an inhaled corticosteroid, budesonide, in newly detected asthma. New Engl J Med 1991; 325:388-92. This randomized, blinded comparison of the above two drugs was important in establishing inhaled corticosteroids as the first line treatment for asthma. Lazarus SC, Boushey HA, Fahy JV et al. Long-acting beta2-agonist monotherapy vs. continued therapy with inhaled corticosteroids in patients with persistent asthma: a RCT. JAMA 2001;285:2583-93. Switching from low dose ICS to long-acting beta2-agonist in patients with well-controlled, persistent asthma increased the risk of treatment failure and asthma exacerbations. Niewoehner DE, Rice K, Cote C, et al. Prevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator. Ann Intern Med 2005;143:317-26. A large multi-center RCT of VA patients with moderate to severe COPD (mean baseline FEV1 36%) found tiotropium reduced the proportion of patients with 1 or more exacerbations during 6 months of treatment vs. placebo (27.9 % vs. 32.3 %). These results support using tiotropium in COPD patients with moderate to severe obstruction and frequent exacerbations. Global strategy for the diagnosis, management, and prevention of COPD: GOLD workshop summary. For the most current 2008 version of these influential guidelines go to: http://www.goldcopd.com Pryor JA. Physiotherapy for airway clearance in adults. Eur Respir J 1999;14:1418-24. Somewhat cursory overview of common airway clearance techniques used in the setting of CF, neuromuscular disease, and other diseases associated with impaired secretion clearance. The author also touches on the paucity of evidence supporting the superiority of any one approach. Pryor JA. Physiotherapy for airway clearance in adults. Eur Respir J 1999;14:1418-24. Somewhat cursory overview of common airway clearance techniques used in the setting of CF, neuromuscular disease, and other diseases associated with impaired secretion clearance. The author also touches on the paucity of evidence supporting the superiority of any one approach. Fuchs HJ, Borowitz DS, Christiansen DH, et al. Effect of aerosolized recombinant human DNase on exacerbations of respiratory symptoms and on pulmonary function in patients with cystic fibrosis: the Pulmozyme Study Group. N Engl J Med 1994;331:637-42. Large RCT found patients receiving a 24-week course of Pulmozyme had an improvement in FEV1 of 5% compared to placebo and decreased exacerbation rate (28 vs. 37% in placebo group). Ramsey BW, Pepe MS, Quan JM, et al. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med 1999;340:23-9. Study found use of TOBI on alternating months improved lung function, decreased bacterial burden, and decreased the relative risk of hospitalization. The rate of acquired tobramycin resistance was about 7% over 24 weeks. Saiman L, Marshall BC, Mayer-Hamblett N, et al. Azithromycin in patients with cystic fibrosis chronically infected with pseudomonas aeruginosa. JAMA 2003;290:1749-56. Large multicenter RCT of 6 months
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 27

duration found chronic azithromycin resulted in a 4.4% improvement in FEV1% predicted compared to a 1.8% decline in placebo. The azithromycin group had fewer exacerbations and gained more weight. Balfour-Lynn IM, Lees B, Hall P, et al. Multicenter randomized controlled trial of withdrawal of inhaled corticosteroids in cystic fibrosis. Am J Respir Crit Care Med 2006; 173:1356-62. This study of 171 children and adults with mean baseline FEV1 of 76% predicted found no difference in to time to 1st exacerbation, or use of rescue bronchodilators and antibiotics over the first 6 months of withdrawing inhaled steroid. These results suggest that many CF patients may be able to safely discontinue inhaled steroids. Aaron SD, Vandemheen KL, Ferris W, et al. Combination antibiotic susceptibility testing to treat exacerbations of cystic fibrosis associated with multiresistant bacteria: a randomised, double-blind, controlled clinical trial. Lancet 2005; 366:463-71. This study of 132 CF patients found selection of intravenous antibiotics based on multiple combination bactericidal susceptibility testing did not reduce the time to next exacerbation compared to antibiotic selection based on conventional culture and sensitivity tests and there was no difference in the rate of treatment failure. Elkins MR, Robinson M, Rose BR, et al. A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N Engl J Med 2006; 354:229-40. This study of 164 children and adults with CF found the combination of bronchodilator and 7% saline neb bid had only a modest impact on pulmonary function but reduced exacerbations (76% exacerbation free vs. 62% placebo, p = .03). These results may not be applicable to patients on more aggressive baseline regimens than the study population. American Thoracic Society/European Respiratory Society international multidisciplinary consensus classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2002;165:277-304. Written to standardize the diagnostic criteria and terminology for idiopathic interstitial pneumonias, this article nicely summarizes the clinical, radiologic, and histologic features of the ILD alphabet soup. Mathieson JR, Mayo JR, Staples CA, Muller NL. Chronic diffuse infiltrative lung disease: comparison of diagnostic accuracy of CT and chest radiography. Radiology 1989;171:111-6. First study to assess accuracy of CT-based diagnosis for patients with ILD. Correctly diagnosed UIP in 89% of cases, sarcoid in 77% of cases, and were, for the most part, less accurate in diagnosing less common diseases. Includes an interesting table of the frequency of selected CT findings observed among the 5 most common ILDs in the study (e.g. pleural fluid/thickening seen in only 9% of UIP cases). Epler GR, Colby TV, McCloud TC, et al. Bronchiolitis obliterans organizing pneumonia. New Engl J Med 1985;312:152-8. Classic article describing idiopathic BOOP (cryptogenic organizing pneumonia) Lazor R, Vandevenne A, Pelletier A, et al. Cryptogenic organizing pneumonia: characteristics of relapses in a series of 48 patients. Am J Respir Crit Care Med 2000; 162:571-7. This retrospective case series provides insight on the clinical course of COP and has had a large influence on the way corticosteroids are used to treat COP. 58% of patients experienced a relapse, 82% of which occurred within 1 year of the initial episode. Two-thirds of patients were on corticosteroids at the time of first relapse; only 1 patient was on > 20 mg/day of prednisone. Delayed treatment was a risk factor for relapse. Relapses did not affect longer term outcome. Demedts M, Behr J, Buhl R, et al, IFIGENIA Study Group. High-dose acetylcysteine in idiopathic pulmonary fibrosis. N Engl J Med. 2005; 353:2229-42. Multi-center, double-blind, randomized, placebo-controlled study (N=182) which determined (after one year) that high-dose oral acetylcysteine added to standard therapy (prednisone and azathioprine) resulted in modest benefit in terms of preserving vital capacity and DLCO but offered no survival advantage. A large proportion of patients dropped out of the study and there is concern that acetylcysteine prevented azathioprine toxicity rather than treated IPF. Martinez FJ, Safrin S, Weycker D, et al. The clinical course of patients with idiopathic pulmonary fibrosis. Ann Intern Med 2005;142:963-7. This retrospective study of 168 patients with mild to moderate disease from the placebo arm of the IFN-gamma 1b study found minimal change in physiologic variables among survivors during the 72 weeks of follow-up. 19% of patients died of IPF-related causes, of whom 47% experienced rapid clinical deterioration. These results indicate IPF exacerbations in patients with milder disease are not uncommon, which has implications for listing for lung transplantation. Flaherty KR, King TE, Raghu G et al. Idiopathic interstitial pneumonia: what is the effect of a multidisciplinary approach to diagnosis? Am J Respir Crit Care Med 2004;170:904-10. This study found radiologists and clinicians with expertise in ILD reliably diagnose IPF without a lung biopsy when the clinical and imaging features are typical of IPF. Combining clinical, radiographic, and pathologic information heavily influenced the final diagnostic impression in non-IPF cases. Histology results had the greatest influence in these instances, but pathologists altered or clarified their diagnosis 19% of the time after receiving radiographic and clinical information.
28 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Raghu G, Brown KK, Bradford WZ et al . A placebo controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis. N Engl J Med 2004;350:125-33. A RCT of Gamma-1b IFN involving 330 patients found no difference in progression-free survival, pulmonary function, or quality of life in patients with IPF unresponsive to corticosteroid therapy. A trend towards enhanced survival in adherent patients with less severe lung impairment (FVC >62 % predicted) prompted the INSPIRE trial which is in progress. Baughman RP, Costabel U, du Bois RM. Treatment of sarcoidosis. Clin Chest Med 2008; 29:533-48. Offers some additional information since the 1999 ATS/ERS statement on sarcoidosis. Additional articles in this issue of Clin Chest Med cover other aspects of sarcoidosis. United States. Surgeon General's Advisory Committee on Smoking and Health, and United States. Public Health Service. Office of the Surgeon General. "Smoking and Health." United States. Public Health Service. Office of the Surgeon General, 1964. Official Report This landmark U.S. Surgeon General’s report added to the growing international recognition of the multiple hazards of cigarette smoking. Tockman MS, Anthonisen NR, Wright EC, et al. Airways obstruction and the risk for lung cancer. Annals Intern Med 1987;106:512-8. This study found smokers with COPD had about a 5-fold risk of developing lung cancer compared to smokers without COPD. The more severe the COPD, the greater the risk. Goldstraw P, Crowley J, Chansky K, et al. The IASLC lung cancer staging project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007; 2:706-14. This proposal was subsequently adopted as the new standard for TNM staging effective January, 2009. Major changes in the new edition include reclassification of satellite pulmonary nodules and malignant effusions. Silvestri G, Gould M, Margolis M, et al. Noninvasive staging of non-small cell lung cancer. Chest 2007;132:178S-201S. ACCP evidence-based clinical practice guidelines (2nd Edition) reviewing the evidence for staging of non-small cell lung cancer with CT and PET scanning. Detterbeck F, Jantz M, Wallace M, et al. Invasive mediastinal staging of lung cancer. Chest 2007; 202S-220S. ACCP evidence-based clinical practice guidelines (2nd Edition) reviewing the sensitivity and specificity of various tissue sampling techniques: TTNA, TBNA, EBUS, EUS, VATS, Chamberlain procedure, mediastinoscopy and extended cervical mediastinoscopy. Fontana RS, Sanderson DR, Taylor WF, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Mayo Clinic study. Am Rev Respir Dis 1984;130:561-5. Also includes a summary of the combined results of the Mayo, Sloan-Kettering, and Johns Hopkins study sites on pp 565-70. Melamed MR, Flehinger BJ, Zaman MB, et al. Screening for lung cancer: results of the Memorial Sloan-Kettering study in New York. Chest 1984;86:44-53. Frost JK, Ball WC, Levin ML, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Johns Hopkins study. Am Rev Respir Dis 1984;130:549-54 Kubik A, Parkin DM, Khlat M, et al. Lack of benefit from semi-annual screening for cancer of the lung: follow-up of a randomized controlled trial on a population of high-risk males in Czechoslavakia. Int J Cancer 1990;45:26-33.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 29
STAGING, DIAGNOSTIC, TREATMENT, AND SPECIAL CONSIDERATIONS Recently, chronic obstructive pulmonary disease (COPD) has gained interest as a major public health concern and is currently the focus of intense research because of its persistently increasing prevalence, mortality, and disease burden. COPD was responsible for more than 2.5 million deaths worldwide in the year 2000 alone and currently ranks as the fourth leading cause of death in the United States, surpassed only by heart disease, cancer, and cerebrovascular disease. Furthermore, COPD is projected to have the fifth leading burden of disease worldwide by the year 2020. COPD is one of the leading causes of disability worldwide and is the only disease for which the prevalence and mortality rates continue to rise. This document presents a concise overview of COPD. We address its definition, prevalence and epidemiology, pathology and pathophysiology, diagnosis, therapy, and outcomes. Also, because of recent insights regarding the relation between COPD and sleep disorders, we include a discussion on sleep and COPD.
Definitions
COPD is broadly defined and encompasses several clinical and pathologic entities, namely emphysema and chronic bronchitis. Evidence of airflow obstruction that is chronic, progressive, and for the most part fixed, characterizes COPD. Notwithstanding the presence of irreversible airflow obstruction in COPD, most individuals (∼60% to 70%) demonstrate a reversible component of airflow obstruction when tested repeatedly.
Emphysema is specifically defined in pathologic terms as “alveolar wall destruction with irreversible enlargement of the air spaces distal to the terminal bronchioles and without evidence of fibrosis.”
Chronic bronchitis is defined as “productive cough that is present for a period of three months in each of two consecutive years in the absence of another identifiable cause of excessive sputum production.”
Whereas the American Thoracic Society (ATS), British Thoracic Society (BTS), and European Respiratory Society (ERS) definitions of COPD emphasize chronic bronchitis and emphysema, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) proposes a definition of COPD that focuses on the progressive nature of airflow limitation and its association with abnormal inflammatory response of the lungs to various noxious particles or gases. According to the GOLD document, COPD is defined as “a disease state characterized by airflow limitation that is not fully reversible. The airflow limitation is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases.”
30 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Pathogenesis and Pathology
As indicated in the definition of emphysema, the pathologic hallmark is elastin breakdown with resultant loss of alveolar wall integrity. This process is triggered by the exposure of a susceptible individual to noxious particles and gases. Cigarette smoke remains the main causative agent, involved in more than 90% of cases; however, other gases and particles have been shown to play a role in pathogenesis, which is a result of an inflammatory process. In contrast to the eosinophilic inflammation seen in asthma, the predominant inflammatory cell is the neutrophil. Macrophages and CD8+ T lymphocytes are increased in the various parts of the lungs, and several mediators, including leukotriene B4, interleukin 8, and tumor necrosis factor, contribute to the inflammatory process.
Oxidative stress is regarded as another important process in the pathogenesis of COPD, and altered protease/antiprotease balance, at least in individuals with severe deficiency of alpha-1 antitrypsin, has been shown to predispose to a panacinar form of emphysema. Individuals with severe deficiency of alpha-1 antitrypsin may develop emphysema at an early age (e.g., by the fourth decade), in contrast to the “usual” emphysema, which typically begins in the sixth decade.
The pathologic hallmark of chronic bronchitis is an increase in goblet cell size and number that leads to excessive mucus secretion. Airflow obstruction and emphysematous change are frequent but not universal accompaniments. When COPD is complicated by hypoxemia, intimal and vascular smooth muscle thickening may cause pulmonary hypertension, which is a late and poor prognostic development in COPD.
Diagnosis
The diagnosis of COPD is suggested by findings on history or physical examination, or both, and is confirmed by laboratory tests, usually with a supportive risk factor (e.g., familial COPD or cigarette exposure, or both). Spirometry is indispensable in establishing the diagnosis because it is a standardized and reproducible test that objectively confirms the presence of airflow obstruction. Characteristically, spirometry shows a decreased forced expiratory volume in 1 second (FEV1) and FEV1/forced vital capacity (FVC) ratio. Evidence of reversible airflow obstruction, defined as a post-bronchodilator rise of FEV1 and/or FVC by 12% and 200 mL, is present in up to two thirds of patients with serial testing. Measurement of the diffusing capacity for carbon monoxide (DLCO) may help differentiate between emphysema and chronic bronchitis. Specifically, in the context of fixed airflow obstruction, a decreased diffusing capacity indicates a loss of alveolar-capillary units, which suggests emphysema. Deficiency of α1 antitrypsin is an uncommon cause of emphysema that continues to be under-recognized by practicing clinicians. The clinical recognition of patients with this condition is also based on clinical suspicion, but as outlined in the American Thoracic Society/European Respiratory Society (ATS/ERS) evidence-based standards document, specific circumstances should prompt suspicion of α1-antitrypsin deficiency. They include emphysema occurring in a young individual (age 45 or younger) or without obvious risk factors (e.g., smoking or occupational exposure) or with prominent basilar emphysema on imaging, necrotizing panniculitis, antineutrophil cytoplasmic antibody (C-ANCA)–positive vasculitis, bronchiectasis of undetermined etiology, otherwise unexplained liver disease, or a family history of any one of these conditions, especially siblings of PI*ZZ individuals.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 31

The most common symptoms and signs include cough, dyspnea on exertion, and increased phlegm production. Additional signs and symptoms include wheezing, prolonged expiration with pursed-lip breathing, barrel chest, use of accessory muscles of breathing and, in advanced cases, cyanosis, evidence of right heart failure, and peripheral edema. A chest radiograph (CXR) is usually obtained to exclude other etiologies but may show hyperinflation and flattening of the diaphragms with increased retrosternal space on the lateral view, and hyperlucency reflecting oligemia. The chest radiograph is an insensitive test for diagnosing emphysema and is abnormal only when emphysema is relatively advanced. In contrast, high-resolution computed tomography (CT) scanning is far more sensitive and specific than CXR for diagnosing emphysema and readily identifies bullae and blebs that are the consequences of alveolar breakdown. However, save its role in selecting the proper candidate for lung volume reduction surgery (LVRS), the additional data from CT rarely alter therapy, making CT scanning not indicated for routine clinical use.
Classification of Severity
Because the degree of FEV1 reduction has prognostic implications and correlates with mortality and morbidity, a staging system based on the degree of airflow obstruction has been proposed by the different societal guidelines. As reviewed in, staging of disease severity, four groups—the ATS, the ERS, the BTS, and GOLD—have developed staging systems for COPD based on the value of FEV1 percent predicted. All systems propose three-stage classifications of COPD, although the FEV1 criteria vary among systems.
32 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 33

Staging of Disease Severity Disease Severity FEV1 Predicted
ATS ERS BTS GOLD
Stage 0: at risk – – – Normal Chronic symptoms (cough, sputum production) Stage I: mild ≥50% ≥70% ≥60% ≥80% With or without chronic symptoms Stage II: moderate 35-49% 50-69% 40-59% 50%-79% With or without chronic symptoms Stage III: severe <35% <50% <40% 30%-49% With or without chronic symptoms Stage IV: very severe – – – <30% or <50% with chronic respiratory failure
ATS, American Thoracic Society; BTS, British Thoracic Society; ERS, European Respiratory Society; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
More recently, in the context that one major purpose of staging systems is to establish prognosis, attention has focused on the additive value of assessing weight (i.e., body mass index), dyspnea, and exercise capacity (i.e., the 6-minute walk distance), to FEV1 in staging COPD. Indeed, the resultant index called BODE (for Body mass index, Obstruction, Dyspnea, and Exercise capacity) has been shown to better predict survival in COPD than FEV1 alone. BODE scores of 0 to 10 (most impaired) are stratified into four quartiles, which discriminate mortality risk better than FEV1 alone.
Natural History and Prognosis of COPD
Several factors influence the natural history and affect survival in patients with COPD. These factors include age, smoking status, pulmonary artery pressure, resting heart rate, body mass index (BMI), airway responsiveness, hypoxemia, dyspnea, exercise capacity, and most importantly, the level of FEV1, which remains the single best predictor of prognosis.
More fully discussed in the section on treatment, few interventions have been shown to change the natural history of COPD. Specifically, survival can be improved by use of supplemental oxygen by those hypoxemic on room air, by allocation to smoking cessation, and—in selected individuals—by lung volume reduction surgery.
Acute exacerbations of COPD (AECOPD) are a significant contributor to mortality. For example, in the SUPPORT study of patients with AECOPD admitted to the hospital, of 1016 inpatients admitted with hypercapnic respiratory failure, 89% survived the acute hospitalization, but only 51% were alive at 2 years. Patient characteristics associated with mortality at 6 months included increased severity of illness, lower body mass index, older age, poor prior functional status, lower Pao2/Fio2 (inspired fraction of oxygen), and lower serum albumin. However, congestive heart failure and cor pulmonale were associated with longer survival time at 6 months, and this was attributed to the effective therapy available for
34 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

the management of these conditions. The overall severity of illness on the third day of hospitalization, as measured by the Apache III score, was the most important independent predictor of survival at 6 months.
Notably, in another study of individuals with AECOPD, the development of hypercapnia during an acute exacerbation of COPD appeared not to affect the risk of death with AECOPD. Specifically, in a prospective study involving 85 patients admitted with acute exacerbation and followed for 5 years, the mortality rate was not significantly different between hypercapnic and eucapnic individuals. In contrast, patients with chronic hypercapnia demonstrated a much poorer outcome, with only an 11% 5-year survival rate. Notwithstanding these insights, well-designed studies and controlled trials are necessary to improve our ability to predict the outcomes for patients afflicted with this disease.
Sleep and COPD
In the context of a growing understanding of sleep and the interactions between disorders of sleep and COPD, this section reviews the mechanism of hypoxemia in sleep and the overlap between COPD and obstructive sleep apnea syndrome (OSAS).
Hypoxemia during Sleep in COPD
Under normal circumstances, sleep results in a decrease in ventilation and in chemo-responsiveness to the arterial partial pressure of carbon dioxide (Paco2). The decreased ventilation appears to be almost entirely related to a drop in tidal volume. Normally, this decrease in tidal volume does not result in hypoxemia, because the drop in the arterial partial pressure of oxygen (Pao2) occurs on the flat portion of the oxyhemoglobin dissociation curve, thereby preserving the oxygen saturation (Sao2). However, in patients with COPD, whose oxygenation during wakefulness may already be on the steep portion of the oxyhemoglobin dissociation curve, hypoxemia during sleep may occur as tidal volume falls. The most pronounced hypoxemia occurs during the rapid eye movement (REM) stage of sleep because of the generalized muscle hypotonia that accompanies REM sleep. REM-associated hypoxemia may reach critically low levels, especially in patients with already borderline waking oxygenation, with potentially deleterious clinical consequences such as cardiac dysrhythmias, pulmonary hypertension, and polycythemia. Hypoxemia during sleep in COPD is primarily a result of hypoventilation, but it is also caused by a decrease in functional residual capacity (FRC), and to worsening ventilation/perfusion ( / ) mismatch.
COPD and Obstructive Sleep Apnea Syndrome
The co-occurrence of COPD and obstructive sleep apnea syndrome (OSAS), also referred to as the “overlap syndrome,” involves a minority of COPD patients but identifying these individuals is important because their nocturnal hypoxemia tends to be more pronounced, leading to a greater likelihood of adverse clinical events. It follows that in patients with the overlap syndrome, therapy must be directed at their COPD and at the OSAS.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 35

TREATMENT
Treatment of Stable COPD
Once the diagnosis of COPD is established and the stage of the disease is determined, attention turns to patient education and risk factor modification, to pharmacologic and nonpharmacologic methods needed to ameliorate the signs and symptoms of COPD, and to optimizing patients' longevity and functional status.
Patient education is an essential component of treatment because it facilitates reduction of risk factors and improves the individual patient's ability to cope with the disease. Education requires a team approach that includes, in addition to the physician and the patient, home health nurses, social workers, physical therapists, occupational therapists, and others. In addition to risk-factor reduction, education should provide a basic, simple-to-understand overview of COPD, its pathophysiology, medications and their proper use, and instructions on when to seek help. Discussing end-of-life issues and establishing advance directives are facilitated by the educational process, especially when applied in the setting of pulmonary rehabilitation.
Smoking cessation is a cornerstone of patient education and confers many benefits, including slowing the accelerated rate of FEV1 decline among smokers, improvements in symptoms, and lessening the risk of lung cancer. For example, data from the Lung Health Study (LHS) show that in the sustained nonsmokers over that 11-year study, the rate of FEV1 decline slowed to 30 mL per year in men and 22 mL per year in women compared with the 66 mL per year and 54 mL per year decline in continuing male and female smokers, respectively. The result was that 38% of continuing smokers had an FEV1 <60% of predicted normal at 11 years compared with only 10% of sustained quitters. Aggressive smoking cessation intervention with counseling and nicotine patch allowed 22% of LHS participants to achieve sustained smoking cessation over 5 years, and 93% of these individuals were still abstinent at 11 years.
Available strategies for smoking cessation include nicotine replacement, available in gum, patch, inhaler or nasal spray; bupropion (an antidepressant), smoking-cessation programs, varenicline, counseling, and combinations of these. Randomized, controlled trials suggest that the combination of nicotine replacement and bupropion confers greater likelihood of achieving smoke-free status than either therapy alone. Use of the partial acetylcholine receptor agonist, varenicline, appears to allow higher rates of smoking cessation than does buproprion.
Beyond education and smoking cessation, the goals of pharmacologic and nonpharmacologic treatments are to enhance survival, quality of life, and functional status, and to lessen mortality. As seen below, available treatments include bronchodila-tors, corticosteroids, immunizations, antibiotics, mucokinetics, and others.
36 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Recommendations by Professional Societies* for Management of Stable COPD
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 37

38 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Bronchodilators
Bronchodilators are a mainstay of COPD treatment, and include β-adrenergic agonists, anticholinergics, and methylxanthines. β-adrenergic agonists are effective in alleviating symptoms and improving exercise capacity, and can produce significant increases in FEV1. Their effect is achieved through smooth muscle relaxation, resulting in improved lung emptying, reduced thoracic gas volume and residual volume, and lessened dynamic hyperinflation. As such, it is believed that the increase in exercise tolerance and reduction in symptoms of breathlessness are primarily a result of an improvement in inspiratory capacity rather than an increase in FEV1. Oral theophylline has been shown to lessen dyspnea and improve the health-related quality of life (QOL) despite lack of significant rise in FEV1, with improvements believed to be a result of increased respiratory muscle performance. However, the narrow therapeutic index of methylxanthines and their potential for adverse drug-drug interactions, has hindered their widespread use. Long-acting formulations have allowed more consistent and stable plasma levels, thereby mitigating the problem.
Recently, newly-developed oral, highly selective phosphodiesterase-4 (PDE-4) inhibitors roflumilast and cilomilast, have shown promise in the management of stable COPD. Specifically, a randomized, double-blind study involving more than 1400 patients with moderate-to-severe COPD compared patients assigned to receive 250 mg of roflumilast, 500 mg of roflumilast, or placebo over a period of 24 weeks. The primary end points were post-bronchodilator FEV1 and health-related QOL. Secondary end points included the rate of COPD exacerbations. Although there was no significant difference in the post-bronchodilator FEV1 in the treatment arms, both were superior to placebo (P < .0001). Similar findings were reported in the health-related QOL and rate of exacerbations with an acceptable safety profile. 32 Similarly, cilomilast was compared with placebo in a double-blind, placebo-controlled, parallel group trial. Here, patients were assigned to cilomilast 15 mg orally twice daily versus placebo, and followed for 24 weeks. Change from baseline FEV1 and St. George's Respiratory Questionnaire (SGRQ) scores were the primary end points, with the rate of COPD exacerbations as the main secondary end point. Again, cilomilast was statistically superior to placebo in all study end points, with mild-to-moderate adverse events that were self limited. 33 As promising as these studies seem, more studies are needed before these new PDE-4 inhibitors become part of the standard therapy of the stable COPD patient.
In the early stages of COPD (e.g., stage I), a short-acting β-adrenergic agonist (e.g., albuterol, terbutaline, etc.) or an anticholinergic is used on an as-needed basis. As the disease progresses (e.g., stages II and III), regular use of one or more bronchodilators is frequently recommended. Some data suggest that a combination of albuterol and ipratropium bromide provides better bronchodilation than either agent alone. In 2004, the United States Food and Drug Administration approved a new anticholinergic agent, tiotropium, for the long-term, once daily, maintenance treatment of bronchospasm associated with stable COPD, including chronic bronchitis and emphysema. Although this is the same indication granted to ipratropium, tiotropium has shown significant advantages over ipratropium, both pharmacologically and clinically. Specifically, tiotropium blocks the M1-M5 muscarinic receptors with a 6- to 20-fold greater affinity than ipratropium and for a more prolonged period of time and dissociates more rapidly from the M2 receptor associated with acetylcholine release, thereby conferring theoretical advantages over ipratropium. These advantages were shown in clinical trials comparing the two agents. Specifically, tiotropium demonstrated significantly greater bronchodilation than ipratropium and users experienced less dyspnea,
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 39
fewer acute exacerbations, reduced albuterol use, and improved nocturnal oxygen saturation. Furthermore, when compared with long-acting β2 agonists, tiotropium provided greater bronchodilation and reduced dyspnea than salmeterol. A large double-blind, placebo-controlled trial showed a significantly greater reduction in yearly incidence as well as delay to first COPD exacerbation compared with either salmeterol or placebo.
Corticosteroids
Although widely used, oral and inhaled corticosteroids have a limited role in managing patients with stable COPD. Several groups suggest brief trials of oral corticosteroids for patients with stable COPD. For example, the BTS suggests a course of oral prednisone (e.g., 30 mg daily) taken for 2 weeks, or a course of inhaled steroid (e.g., beclomethasone 500 mg twice daily or the equivalent) taken for 6 weeks. Similarly, the ERS suggests a trial of corticosteroids (e.g., 0.4 to 0.6 mg/kg/day) taken for 2 to 4 weeks. Patients with significant FEV1 responses are considered candidates for long-term inhaled corticosteroids. At the same time, four randomized, placebo-controlled trials of inhaled corticosteroids in patients with COPD have shown no effect on the rate of FEV1 decline, although one study suggested that steroid recipients experienced fewer COPD exacerbations than non recipients.
A more recent trial was conducted comparing the effect of the salmeterol/fluticasone combination with either agent alone and with placebo, and found that the combination therapy was significantly more effective than sole therapy with the long-acting bronchodilator, or fluticasone, or placebo in patients with COPD. Specifically, the TRISTAN study, a 52-week, randomized, placebo-controlled study involving 1465 patients with moderate-to-severe COPD showed significant improvement in FEV1 in the salmeterol/fluticasone combination versus salmeterol (treatment difference of 73 mL, P < 0.0001), fluticasone (treatment difference of 95 mL, P < 0.0001), and placebo (treatment difference of 133 mL, P < 0.0001). Other benefits included a decrease in the use of rescue medications in the combination group as well as a significant improvement in health status as defined by the St. George's Respiratory Questionnaire compared with the fluticasone, but not the salmeterol group. Finally, the rate of moderate and severe exacerbations was reduced by 25% in the combination group compared with placebo. This finding becomes all the more significant in the context that severe acute exacerbations have an independent negative impact on prognosis, with increased mortality associated with the frequency of severe exacerbations. Specifically, in a prospective cohort of 304 men with severe COPD (mean FEV1, 46% predicted), older age, carbon dioxide (CO2) tension, and acute exacerbation of COPD represented independent indicators of poor prognosis, with patients with three or more exacerbations showing the greatest mortality risk. Finally, whether the combination of an inhaled corticosteroid and long-term bronchodilator enhances survival in patients with COPD is the subject of ongoing research.
Immunizations
Yearly prophylactic immunization with the influenza vaccine has been shown to reduce the incidence of influenza by 76% and is strongly recommended. Immunization once with the 23-polyvalent pneumococcal vaccine in individuals with COPD or, in the special case of individuals with immunodeficiency or those with splenectomy, every 5 years, is also recommended.
40 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Antibiotics
Prophylactic antibiotics have not shown benefit in the management of stable COPD and are not recommended.
Mucokinetic Agents
Mucoactive agents are varied and include ambroxol, erdosteine, carbocysteine, iodinated glycerol, N-acetylcysteine, surfactant, and others, all of which have been studied with conflicting results. However, a Cochrane systematic review of 23 randomized, controlled trials in Europe and the United States associates the long-term use (>2 months) of oral mucolytics with a reduction in acute COPD exacerbations and days of illness, and suggests the consideration of these agents in patients with recurrent, prolonged, severe COPD exacerbations. Still, the latest guidelines by the ATS and BTS do not recommend the routine use of mucoactive agents in the management of chronic COPD.
Others
Antitussives containing narcotics and other therapies, such as inhaled nitric oxide, may be harmful. Their use in COPD is contraindicated. In the specific case of alpha-1 antitrypsin deficiency, intravenous augmentation therapy with pooled human plasma antiprotease can raise serum levels of alpha-1 antitrypsin above a protective threshold value (11 micromolar). Available evidence suggests that augmentation therapy can slow the rate of FEV1 decline in individuals with severe deficiency of alpha-1 antitrypsin (e.g., with the PI*ZZ phenotype) and established airflow obstruction of moderate severity (e.g., FEV1 30% to 65% predicted). Currently available α1-proteinase inhibitors in the United States include Prolastin (Talecris, Research Triangle, North Carolina), Aralast (Baxter Healthcare, Deerfield, Illinois), and Zemaira (ZLB Behring, King of Prussia, Pennsylvania).
Nonpharmacologic treatment of COPD includes pulmonary rehabilitation, long-term oxygen therapy (LTOT), ventilatory support, and lung volume reduction surgery (LVRS). Pulmonary rehabilitation is recommended at all stages by all available guidelines. Aerobic lower extremity training can improve exercise endurance, dyspnea, health care use, and overall quality of life. Upper extremity exercise and respiratory muscle training also appear helpful.
Long-term oxygen therapy for patients with hypoxemia has been shown to improve survival in eligible patients with COPD. Criteria for prescribing LTOT include a Pao2 <55 mm Hg or Sao2 <88% with or without increased Paco2, or Pao2 between 55 and 59 mm Hg or Sao2 <89%, with right-sided failure reflected by evidence of pulmonary hypertension or polycythemia (e.g., hematocrit >55%).
Nocturnal noninvasive ventilatory support still has an unproven role in managing patients with stable COPD. Lung volume reduction surgery (LVRS) involves the resection of 20% to 35% of the emphysematous lung to improve lung mechanics. The procedure was first proposed by Brantigan and Mueller in the late 1940s, but was abandoned then because of unacceptably high associated mortality. More recently, available randomized, controlled trials show that LVRS is contraindicated in individuals with severely impaired lung function (e.g., FEV1 <20% predicted, homogeneous emphysema or lung diffusing capacity, or both, for carbon monoxide <20% predicted), but that LVRS recipients with moderate degrees of airflow obstruction may experience an improved FEV1, walking distance, and quality of life. In the recently published
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 41

results of the National Emphysema Treatment Trial, a randomized controlled trial of LVRS versus medical therapy (including rehabilitation) in which 1218 individuals with moderate COPD (FEV1 <45% predicted) were enrolled, the LVRS group overall experienced improved disease-specific quality of life and exercise capacity compared with the medically managed group. 20 On the other hand, the LVRS group had similar rates of survival as the medically managed group. In subsets defined by pre-specified exploration, a survival advantage was observed in the subgroup of patients with predominantly upper lobe emphysema and low baseline (i.e., post-rehabilitation) exercise capacity (defined as a maximal workload at <25 watts for women and 40 watts for men).
Finally, lung transplantation is an option for patients with severe airflow obstruction and functional impairment. The five-year actuarial survival rate for patients undergoing single-lung transplantation for COPD is 43.2%. Selection criteria include an FEV1 <25% predicted and/or a Paco2 >55 mm Hg or cor pulmonale, or both.
42 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

TREATMENT OF ACUTE EXACERBATIONS OF COPD
Acute exacerbation of COPD (AECOPD) represents an acute worsening of the patient's baseline condition, generally characterized by worsened dyspnea and increased volume and purulence of sputum. Depending on the severity of baseline COPD, additional derangements may become manifest, such as hypoxemia, worsening hypercapnia, cor pulmonale with worsening lower extremity edema, or altered mental status. The main goals of treating AECOPD are to restore the individual to his or her previous stable baseline and to prevent or reduce the likelihood of recurrence. This requires identification of the precipitating factor or condition and its reversal or amelioration while optimizing gas exchange and improving the individual patient's symptoms. Treatment modalities similar to the ones used in stable COPD are used in managing acute exacerbations. These include oxygen therapy, bronchodilators, antibiotics, corticosteroids, mechanical ventilation, and others.
Recommendations by Professional Societies for Management of Acute Exacerbations of COPD
American Thoracic Society
European Respiratory Society
British Thoracic Society
Global Initiative for Chronic Obstructive
Lung Disease Bronchodilators
Recommended: ß 2 agonists ± anticholinergics; IV aminophylline if inadequate response
Recommended: ß 2 agonists ± anticholinergics; methylxanthines if needed as second-line therapy in severe exacerbations
Recommended: ß 2 agonists ± anticholinergics; IV aminophylline if inadequate response
Recommended: ß 2 agonist dose increase ± anticholinergics ± IV aminophylline depending on disease severity
Corticosteroids
Oral or systemic Oral or systemic empirically
7-14 days of systemic steroids Systemic steroids
Antibiotics
Narrow-spectrum antibiotic; broad spectrum if no response
Inexpensive antibiotic empirically for 7-14 days; if ineffective, choice guided by sputum culture
Common oral antibiotics usually adequate Broader spectrum if no response or if more severe exacerbation
Empirically with increased sputum volume and purulence based on local sensitivity patterns to usual pathogens
Oxygen Therapy
Raise PaO2 >60 mm Hg
Keep SaO2 >90% and/or PaO2 ≥60 mm Hg. Avoid PaCO2 rise by >10 mm Hg or pH drop to <7.25
Raise PaO2 to ≥50 mm Hg while avoiding pH <7.26
Keep SaO2 >90% and PaO2 >60 mm Hg
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 43

Ventilatory Support
NIPPV or invasive mechanical ventilation based on criteria
NIPPV in appropriate patients
NIPPV or invasive mechanical ventilation if pH <7.26 with rising PaCO2 despite controlled oxygen therapy
NIPPV or invasive mechanical ventilation based on selection and exclusion criteria.
Chest Physiotherapy If sputum volume is >25 mL/day
Help in clearance of secretions Not recommended May be beneficial in
certain circumstances
Oxygen Therapy
The role of oxygen therapy is to correct the hypoxemia that usually accompanies the AECOPD. The end point is to maintain oxygen tension at approximately 60 to 65 mm Hg, thereby assuring near-maximal hemoglobin saturation while minimizing the potential for deleterious hypercapnia. Hypercapnia complicating supplemental oxygen is mainly a result of ventilation-perfusion mismatch, with generally smaller contributions of depression of the respiratory drive and the Haldane effect.
Bronchodilators
Bronchodilators are widely used in AECOPD, and β-adrenergic agonists and anticholinergics are first-line therapies. As in stable COPD, both can improve airflow in AECOPD, and although recommendations vary, combined therapy is often recommended. β-adrenergic agonists have a quicker onset of action, whereas anticholinergics have a more favorable side-effect profile. Because of their potential side effects, as well as their limited benefit, methylxanthines are used mostly as second-line therapy.
Antibiotics
Antibiotics play a favorable role in treating AECOPD, especially in the setting of increased volume and purulence of phlegm. A narrow-spectrum antibiotic (e.g., amoxicillin, trimethoprim-sulfamethoxazole, doxycycline, etc.) is often recommended as first-line therapy, although use of a beta-lactam/beta-lactamase combination has been recommended in patients with severe AECOPD, and fluoroquinolones have been recorded in individuals suspected to be colonized with Pseudomonas aeruginosa. 8 The optimal duration of treatment is still unclear, although most guidelines recommend treating for between 7 and 14 days.
Corticosteroids
Randomized clinical trials generally support the use of systemic corticosteroids to enhance airflow and to lessen treatment failure in AECOPD. Prolonged therapy beyond 2 weeks confers no additional benefits, with 5 to 10 days being the likeliest optimal duration. 66–68
44 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Noninvasive Positive Pressure Ventilation and Mechanical Ventilation
Noninvasive positive pressure ventilation (NIPPV) is emerging as a preferred method of ventilation in adequately selected patients with acute respiratory acidemia. This mode is currently used in the treatment of acute respiratory failure of many causes, including COPD. Appropriate patient selection is critical to assure the success of NIPPV. Poor candidates are those with acute respiratory arrest, altered mental status with agitation or lack of cooperation, distorted facial anatomy preventing adequate mask application, cardiovascular instability, or excessive secretions, or both. NIPPV improves symptomatic and physiologic variables, reduces the need for intubation, hospital stay, and mortality, and does not use additional resources.
For patients who do not qualify for NIPPV and/or show evidence of worsening respiratory failure and life-threatening acidemia despite NIPPV, intubation and mechanical ventilation are indicated. This method of ventilation carries numerous risks and complications, including ventilator-acquired pneumonia and barotrauma. Adequate ventilator management is necessary, and every effort should be undertaken to minimize the duration of mechanical ventilation.
Others
Mucolytics, expectorants, and chest physiotherapy have not been shown to improve the outcome and are not recommended.
Conclusion
Overall, COPD poses a common and significant clinical challenge for patients and clinicians alike. Clinicians' expert knowledge regarding diagnosis and management can enhance patients' longevity and quality of life.
Summary
• Chronic obstructive pulmonary disease is emerging as a major cause of morbidity and mortality in the United States. COPD currently is the fourth leading cause of death among Americans.
• Chronic obstructive pulmonary disease is under-recognized overall, as is alpha-1 antitrypsin deficiency, a genetic predisposition to COPD.
• Among the available therapies for COPD, many can improve symptoms (e.g., bronchodilators, pulmonary rehabilitation). Three treatments—smoking cessation, supplemental oxygen used for 24 hours a day, and lung volume reduction surgery—have been shown to prolong life in appropriately selected COPD individuals.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 45

Suggested Readings
• AACP/AACVPR Pulmonary Rehabilitation Guidelines Panel. Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based guidelines. Chest. 112: 1997; 1363-1396.
• American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease.
• American Thoracic Society/European Respiratory Society Statement. Standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med. 168: 2003; 818-900.
• Anthonisen NR, Connett JE, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. The Lung Health Study Research Group. Am J Respir Crit Care Med. 166: 2002; 675-679.
• Maurer JR, Frost AE, Estenne M. International guidelines for the selection of lung transplant candidates. The International Society for Heart and Lung Transplantation, the American Thoracic Society, the American Society of Transplant Physicians, the European Respiratory Society. Transplantation. 66: 1998; 951-956.
• National Emphysema Treatment Trial Research Group. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 348: 2003; 2059-2073.
• Pauwels RA, Buist AS, Calverley PM. GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 163: 2001; 1256-1276.
• Pauwels RA, Lofdahl CG , Laitinen LA. Long-term treatment with inhaled budesonide in persons with mild chronic obstructive pulmonary disease who continue smoking. European Respiratory Society Study on Chronic Obstructive Pulmonary Disease. N Engl J Med. 340: 1999; 1948-1953.
• Sutherland ER, Cherniack RM. Management of chronic obstructive pulmonary disease. N Engl J Med. 350: 2004; 2689-2697.
• The Lung Health Study Research Group . Effect of inhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary disease. N Engl J Med. 343: 2000; 1902-1909.
46 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

References
Murray CJL, Lopez AD, Mathers CD, Stein C: The global burden of disease 2000 project: aims, methods and data sources. Global Programme on Evidence for Health Policy Discussion Paper No. 36. Geneva, World Health Organization, 2001.
National Heart, Lung, and Blood Institute: 2007 NHLBI Morbidity and Mortality Chartbook. Available at http://www.nhlbi.nih.gov/resources/docs/cht-book.htm (accessed Deceember 27, 2007).
World Health Organization: World Health Report 2000: Health systems: Improving performance. Available at http://www.who.int/whr/2000/en/ (accessed December 27, 2007).
Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990– 2020: Global Burden of Disease Study. Lancet. 349: 1997; 1498-1504.
American Thoracic Society/European Respiratory Society Task Force: Standards for the diagnosis and management of patients with COPD [Internet]. Version 1.2. New York, American Thoracic Society, 2004 (updated September 8, 2005). PDF available for download at http://www.thoracic.org/sections/copd/ (accessed December 27, 2007).
Siafakas NM, Vermeire P , Pride NB. , for the European Respiratory Society Task Force: Optimal assessment and management of chronic obstructive pulmonary disease (COPD). Eur Respir J. 8: 1995; 1398-1420.
BTS guidelines for the management of chronic obstructive pulmonary disease. Thorax. 52: 1997; S1-S28.
Pauwels RA, Buist AS , Calverley PM. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 163: 2001; 1256-1276.
Hurd S. The impact of COPD on lung health worldwide: Epidemiology and incidence. Chest. 117: 2000; 1S-4S.
Sullivan SD, Ramsey SD , Lee TA. The economic burden of COPD. Chest. 117: 2000; 5S-9S.
Keatings VM, Collins PD , Scott DM , Barnes PJ. Differences in interleukin-8 and tumor necrosis factor-alpha in induced sputum from patients with chronic obstructive pulmonary disease or asthma. Am J Respir Crit Care Med. 153: 1996; 530-534.
Repine JE, Bast A , Lankhorst I. Oxidative stress in chronic obstructive pulmonary disease. Oxidative Stress Study Group. Am J Respir Crit Care Med. 156: 1997; 341-357.
Standards for the diagnosis and management of individuals with α1-antitrypsin deficiency. Am J Respir Crit Care Med. 168: 2003; 818-900.
Stoller JK, Sandhaus RA , Turino G. Delay in diagnosis of α1-antitrypsin deficiency: A continuing problem. Chest. 128: 2005; 1989-1994.
Campos MA, Wanner A , Zhang G , Sandhaus RA. Trends in the diagnosis of symptomatic patients with α1-antitrypsin deficiency between 1968 and 2003. Chest. 128: 2005; 1179-1186.
Celli BR, Cote CG , Marin JM. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 350: 2004; 1005-1012.
Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: A clinical trial. Ann Intern Med. 93: 1980; 391-398.
Anthonisen NR, Connett JE , Kiley JP. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA. 272: 1994; 1497-1505.
Anthonisen NR, Skeans MA , Wise RA. The effects of a smoking cessation intervention on 14.5-year mortality: A randomized clinical trial. Ann Intern Med. 142: 2005; 233-239.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 47
A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 348: 2003; 2059-2073.
Connors AF, Dawson NV , Thomas C. Outcomes following acute exacerbation of severe chronic obstructive lung disease. Am J Respir Crit Care Med. 154: 1996; 959-967.
Costello R, Deegan P , Fitzpatrick M , McNicholas WT. Reversible hypercapnia in chronic obstructive pulmonary disease: A distinct pattern of respiratory failure with a favorable prognosis. Am J Med. 102: 1997; 239-244.
Roberts CM, Barnes S , Lowe D. Evidence for a link between mortality in acute COPD and hospital type and resources. Thorax. 57: 2002; 137-141.
Gay PC. Chronic obstructive pulmonary disease and sleep. Respiratory Care. 49: 2004; 39-51.
McNicholas WT. Impact of sleep on ventilation and gas exchange in chronic lung disease. Monaldi Arch Chest Dis. 59: 2003; 212-215.
Anthonisen NR, Connett JE , Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. The Lung Health Study Research Group. Am J Respir Crit Care Med. 166: 2002; 675-679.
Sutherland ER, Cherniack RM. Management of chronic obstructive pulmonary disease. N Engl J Med. 350: 2004; 2689-2697.
Celli BR. Pulmonary rehabilitation in patients with COPD. Am J Respir Crit Care Med. 152: 1995; 861-864.
Heffner JE, Fahy B , Hilling L , Barbieri C. Outcomes of advance directive education of pulmonary rehabilitation patients. Am J Respir Crit Care Med. 155: 1997; 1055-1059.
Gonzales D, Rennard SI , Nides M. Varenicline Phase 3 Study Group. Varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: A randomized controlled trial. JAMA. 296: 2006; 47-55.
Jorenby DE, Leischow SJ , Nides MA. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med. 340: 1999; 685-691.
Rabe KF, Bateman ED , O'Donnell D. Roflumilast—an oral anti-inflammatory treatment for chronic obstructive pulmonary disease: A randomized controlled trial. Lancet. 366: 2005; 563-571.
Rennard SI, Schachter N , Strek M. Cilomilast for COPD: Results of a 6-month, placebo-controlled study of a potent, selective inhibitor of phosphodiesterase 4. Chest. 129: 2006; 56-66.
Ferguson GT, Cherniack RM. Management of chronic obstructive pulmonary disease. N Engl J Med. 328: 1993; 1017-1022.
In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. Chest. 105: 1994; 1411-1419.
Routine nebulized ipratropium and albuterol together are better than either alone in COPD. Chest. 112: 1997; 1514-1521.
FDC Reports.. 66: 2004; 18.
Panning CA, DeBisschop M. Tiotropium: An inhaled, long-acting anticholinergic drug for chronic obstructive pulmonary disease. Pharmacotherapy. 23: 2003; 183-189.
van Noord JA, Bantje TA , Eland ME. A randomised controlled comparison of tiotropium and ipratropium in the treatment of chronic obstructive pulmonary disease. Thorax. 55: 2000; 289-294.
Vincken W, van Noord JA , Greefhorst AP. Improved health outcomes in patients with COPD during 1 year's treatment with tiotropium. Eur Respir J. 19: 2002; 209-216.
McNicholas WT, Calverley PM , Lee A , Edwards JC. Long-acting inhaled anticholinergic therapy improves sleeping oxygen saturation in COPD. Eur Respir J. 23: 2004; 825-831.
48 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Brusasco V, Hodder R , Miravitlles M. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD. Thorax. 58: 2003; 399-404.
Pauwels RA, Lofdahl CG , Laitinen LA. Long-term treatment with inhaled budesonide in persons with mild chronic obstructive pulmonary disease who continue smoking. European Respiratory Society Study on Chronic Obstructive Pulmonary Disease. N Engl J Med. 340: 1999; 1948-1953.
Burge PS, Calverley PM , Jones PW. Randomised, double blind, placebo controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: The ISOLDE trial. BMJ. 320: 2000; 1297-1303.
Vestbo J, Sorensen T , Lange P. Long-term effect of inhaled budesonide in mild and moderate chronic obstructive pulmonary disease: A randomised controlled trial. Lancet. 353: 1999; 1819-1823.
Effect of inhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary disease. N Engl J Med. 343: 2000; 1902-1909.
Calverley P, Pauwels R , Vestbo J. Trial of Inhaled Steroids and Long-acting β2-Agonists Study Group: Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: A randomised controlled trial. Lancet. 361: 2003; 449-456.
Soler-Cataluna JJ, Martinez-Garcia MA , Roman Sanchez P. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 60: 2005; 925-931.
Vestbo J. The TORCH (towards a revolution in COPD health) survival study protocol. Eur Resp J. 24: 2004; 206-210.
Nichol KL, Margolis KL , Wuorenma J , Von Sternberg T. The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med. 331: 1994; 778-784.
Koivula I, Sten M , Leinonen M , Makela PH. Clinical efficacy of pneumococcal vaccine in the elderly: A randomized, single-blind population-based trial. Am J Med. 103: 1997; 281-290.
Prevention and control of influenza: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 48: 1999; 1-28.
Poole PJ, Black PN. Mucolytic agents for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2006;
Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based guidelines. Chest. 112: 1997; 1363-1396.
Brantigan OC, Mueller E. Surgical treatment of pulmonary emphysema. Am Surg. 23: 1957; 789-794.
Patients at high risk of death after lung-volume-reduction surgery. N Engl J Med. 345: 2001; 1075-1083.
Geddes D, Davies M , Koyama H. Effect of lung-volume-reduction surgery in patients with severe emphysema. N Engl J Med. 343: 2000; 239-245.
Goldstein RS, Todd TRJ , Guyatt G. Influence of lung volume reduction surgery (LVRS) on health related quality of life in patients with chronic obstructive pulmonary disease. Thorax. 58: 2003; 405-410.
Bennett LE, Keck BM , Daily OP. Worldwide thoracic organ transplantation: A report from the UNOS/ISHLT International Registry for Thoracic Organ Transplantation. Clin Transpl. 31: 2000; 44.
Maurer JR, Frost AE , Estenne M. International guidelines for the selection of lung transplant candidates. The International Society for Heart and Lung Transplantation, the American Thoracic Society, the American Society of Transplant Physicians, the European Respiratory Society. Transplantation. 66: 1998; 951-956.
International Society for Heart and Lung Transplantation: Available at http://www.ishlt.org
McCrory DC, Brown C , Gelfand SE , Bach PB. Management of acute exacerbations of COPD: A summary and appraisal of the published evidence. Chest. 119: 2001; 1190-1209.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 49

Stoller JK. Acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 346: 2002; 988-994.
Anthonisen NR, Manfreda J , Warren CP. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med.. 106: 1987; 196-204.
Stockley RA, O'Brien C , Pye A , Hill SL. Relationship of sputum color to nature and outpatient management of acute exacerbation of COPD. Chest. 117: 2000; 1638-1645.
Niewoehner DE, Erbland ML , Deupree RH. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 340: 1999; 1941-1947.
Davies L, Angus RM , Calverley PM. Oral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: A prospective randomised controlled trial. Lancet. 354: 1999; 456-460.
Thompson WH, Nielson CP , Carvalho P. Controlled trial of oral prednisone in outpatients with acute COPD exacerbation. Am J Respir Crit Care Med. 154: 1996; 407-412.
Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 163: 2001; 540-577.
Noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med. 163: 2001; 283-291.
Kramer N, Meyer TJ , Meharg J. Randomized, prospective trial of noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med. 151: 1995; 1799-1806.
50 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
INTRODUCING PULMONARY REHABILITATION
What is pulmonary rehabilitation? Pulmonary Rehabilitation (PR) is a multidisciplinary approach to improving the functional status and quality of life of people with chronic lung disease. Endurance and strength exercise training is the cornerstone of pulmonary rehabilitation. Along with exercise comes patient education that increases understanding of the disease process, improved coping skills, and a focus on empowering the patient for self-management.
What are the expected outcomes of pulmonary rehabilitation? Patients may expect to realize specific outcomes such as; fewer emergency room visits, lower re hospitalization rates, increased functional ability, independence and self-care. Program graduates typically return to activities of daily living sooner and maintain a higher Quality of Life.
What do ruling societies say about pulmonary rehabilitation? Dr. Andrew Ries, MD, MPH, FCCP, chair of the pulmonary rehabilitation guidelines committee with the American College of Chest Physicians. “The primary goal of pulmonary rehabilitation is to restore the patient to the highest possible level of independent function. We want patients to become more physically active and to learn more about their disease, treatment options, and how to cope.” Pulmonary rehabilitation can include exercise training, education, instruction in various respiratory techniques, and psychosocial support. Research shows that pulmonary rehabilitation is appropriate for any stable patient with COPD who is disabled by respiratory symptoms.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 51
PULMONARY REHAB INCLUSION CRITERIA
Restrictive Diseases • Interstitial diseases
o Interstitial fibrosis o Occupational or environmental lung disease
• Sarcoidosis o Chest wall diseases o Kyphoscoliosis
• Ankylosing spondylitis o Neuromuscular diseases o Parkinson’s disease o Post-polio syndrome o Amyotrophic lateral sclerosis o Diaphragmatic dysfunction o Multiple sclerosis o Post-tuberculosis syndrome
Obstructive Diseases • COPD (including alpha-1 antitrypsin
deficiency) • Persistent asthma • Bronchiectasis • Cystic fibrosis • Bronchiolitis obliterans
Other conditions • Lung cancer • Pre and post thoracic and abdominal surgery • Pre and post lung transplantation • Pre and post lung volume reduction surgery • Ventilatory dependency • Pediatric patients with respiratory disease • Obesity related respiratory disease
Demonstrated Outcomes of Pulmonary Rehabilitation • Reduced respiratory symptoms (dyspnea, fatigue) • Increased exercise performance • Increased knowledge about pulmonary disease and its management • Enhanced ability to perform activities of daily living • Improved health-related quality of life • Improved psychosocial symptoms (reversal of anxiety and depression, increased self-
efficacy) • Reduced hospitalizations and use of medical resources • Return to work or leisure activities
52 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
COPD REHABILITATION PATIENT ASSESSMENT FORM Patient Information Name:__________________________________________________ Date: ________________ Address:________________________________________________ Phone: ______________ Emergency Contact:_______________________________________ Phone: ______________ Age: ________ Sex: ________ Weight: ________ Height:__________ Marital status: _________ Occupation:_____________________________ Retired?_________ Disabled?_____________ Insurance provider: _______________________________________ Sessions allowed: ______ Diagnosis: ______________________________________________ Date of Dx: ___________ Primary Care Provider: ____________________ Referring Physician: ____________________
History Food allergies: ______________________ Medication allergies:_______________________ # of hospitalizations in past year:________________ # of days in hospital: ______________ # of ER visits in last year due to breathing problems: ________________________________ # of acute COPD exacerbations in past year: _______________________________________ Physical Limitation (sensory, stroke, surgeries): _____________________________________
Medical Problems Do you have or have you ever had: Bronchitis_____Pneumonia_____TB_____Cancer______ Blood Clot in Lungs______Pleurisy______Family History of Respiratory Disease:_____ Tobacco Use: _________Pack/Years: _________Quit Date: _________ Secondhand Smoke: _____
Have You Ever Been Exposed To: Asbestos Dust _____ Paint Fumes_____ Farm Dust/Pesticides _____ Plastic Fumes_____ Welding / Mining Dust _____ Solvent Fumes _____ Other Dust _____ Other Fumes _____
Medications Medication Compliance: Y/N Spacer: Y/N Needs Training: Y/N Are you currently taking Antidepressants: Y/N Name:_________________________ Are you currently taking Anxiolytics: Y/N Name:______________________________
56 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Symptoms Do You Ever Have Chest Pain? __________Location:_________________ Type of Pain: ________________________Frequency:________________ # Of Colds /Year: ____Flu Vaccines Each Year: ____Pneumonia Vaccines Each Year: ____ Cough Y/N Frequency: _______________Sputum Y/N Describe: ______________ Wheeze Y/N Cause: __________________Dyspnea Y/N Cause: ______________ Fluid Retention Y/N Where: ________________________________________________ Dyspnea scale for grading the degree breathlessness 1 = least severe, 5 = most sever #:_________ 1. Not troubled by breathlessness except during strenuous exercise 2. Short of breath when hurrying or walking up a slight hill 3. Walks slower than contemporaries on the level because of breathlessness 4. Stops for breath after about 100 yards or after a few minutes on the level 5. Too breathless to leave the house, or breathless when dressing or undressing
SOB Most Difficulty: Morning AM or PM Bedtime Oxygen Therapy Y/N FIO2:________When:_________Home Respiratory Therapy Y/N What type of home respiratory therapy? ___________________________________________ Pursed Lip Breathing_____ Diaphragmatic Breathing_____ Accessory Muscle Use in Breathing_____
Sleep Hygiene #Hours: _______Pillows Used: ______Sleep Disturbances: ______What Kind: ____________ Do you snore, or does your spouse say you snore?: __________ Do you wake up to breathe?_____ Do you stop breathing during sleep? _________ Do you feel rested in the morning?________ Do you need to take naps daily? ________ Do you take medication to help you sleep? ___________
Activities of Daily Living Are you able to care for yourself? _________ Are you able to care for your home?________ Do you exercise? Y/N Type of exercise & how often: _____________________________ Do you have exercise equipment? Y/N Type: _____________________________________ Special interests & hobbies: ____________________________________________________ Does breathing difficulty keep you from your activities? _____Do you live alone? _____ Do you have transportation? ______ Do you need assistive devices? _____ If so, which devices? ___________________________________________________________
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 57

Dietary History Do you have trouble eating? Y/N Why? ________________________________________ Do You Have Difficulty Gaining or Losing Weight? ___________________________________ Special Diet? _________________________________________________________________ Appetite: ________Good________Fair________Poor_______Is this usual for you? ________ Vitamins: Y/N Restaurants per week? _________________________________________ Do you consume alcohol? Y/N How much?________________________________________ Psychosocial Assessment Present Temperament: (Angry, Worried, Sad, Impatient, Frustrated, Depressed, Anxious, Calm, Content, Cheerful, Happy)_______________________________________________________________ Stressors / Fears /Concerns: _____________________________________________________ Relaxation techniques you us_____________________________________________________ What is your most difficult adjustment since being diagnosed with lung disease? _____________________________________________________________________________ Do you forget often? Y/N Do you have a support system? Y/N Who?________________ Do you understand your diagnosis? ________________________________________________ How motivated are you to achieve better health? _____________________________________
List One Long Term Goal ____________________________________________________________________________
List three measurable goals to accomplish in rehabilitation: 1.___________________________________________________________________________ 2.___________________________________________________________________________ 3.___________________________________________________________________________
58 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Physical Assessment Functional Capacity & MET Level: (6:00 Min Walk Test):_______________________________
LAB DATA PFT DATE: _______________ FVC: ______________________________________ FEV1:______________________________________ FEV1/FVC: __________________________________ DLCO: _____________________________________ TLC (sb) ____________________________________
ABG DATE: ______________ pH: ________________________________________ pCO2:______________________________________ pO2:_______________________________________ %Sa02:_____________________________________ FI02:_______________________________________
_______________________________________/_____________ Therapist: Date:
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 59

PHYSICAL FUNCTIONING SCORE (PFS)
SF-36® Health Survey TO BE COMPLETED BY THE PATIENT
Name: ____________________________________ Date: __________________________
A Physical Functioning raw score of (21) is converted as follows: (21 – 10) ---------------- X 100 = 55 20 PRE PROGRAM: SF-36 PF Score: _______ POST PROGRAM: SF-36 PF Score: _______
The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much? (Please circle one number on each line.)
Activities Yes, limited a lot
Yes, limited a little
Not limited at all
1. Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports.
1 2 3
2. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf.
1 2 3
3. Lifting or carrying groceries. 1 2 3 4. Climbing several flights of stairs. 1 2 3 5. Climbing one flight of stairs. 1 2 3 6. Bending, kneeling, or stooping. 1 2 3 7. Walking more than a mile. 1 2 3 8. Walking several blocks. 1 2 3 9. Walking one block. 1 2 3 10. Bathing or dressing yourself. 1 2 3
www.rehabsys.com
60 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
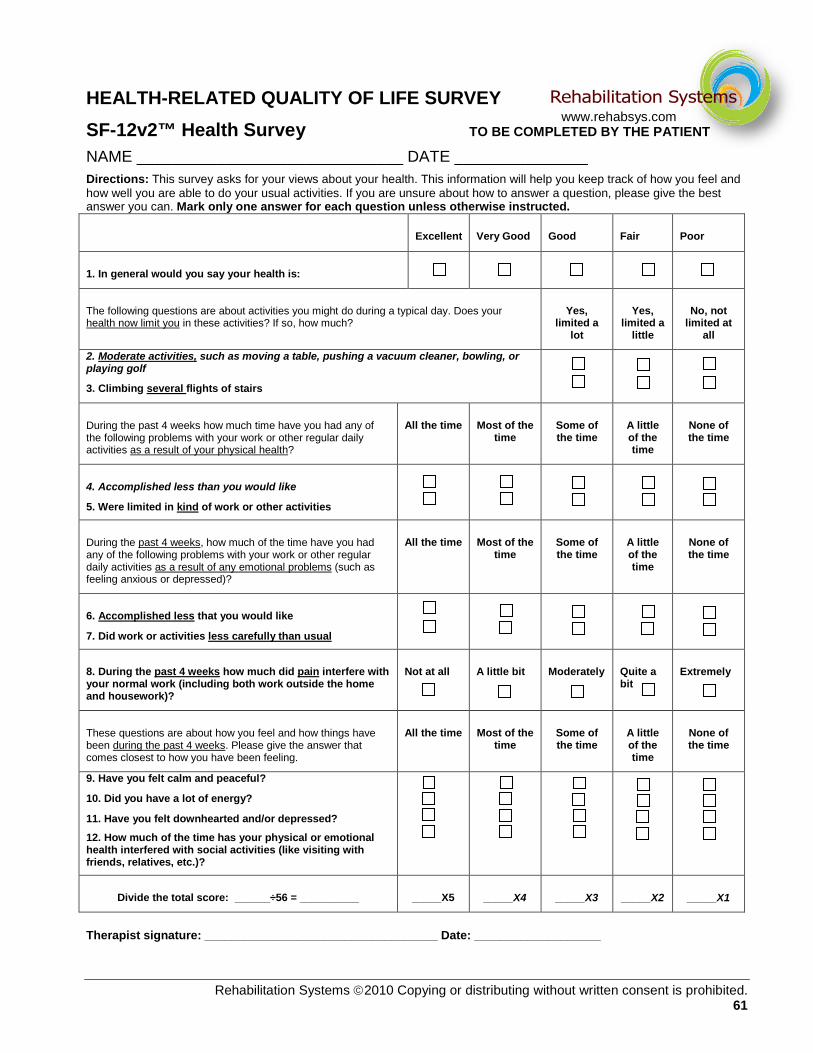
HEALTH-RELATED QUALITY OF LIFE SURVEY SF-12v2™ Health Survey TO BE COMPLETED BY THE PATIENT
NAME ______________________________ DATE _______________ Directions: This survey asks for your views about your health. This information will help you keep track of how you feel and how well you are able to do your usual activities. If you are unsure about how to answer a question, please give the best answer you can. Mark only one answer for each question unless otherwise instructed.
Excellent Very Good Good Fair Poor
1. In general would you say your health is:
The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much?
Yes, limited a
lot
Yes, limited a
little
No, not limited at
all
2. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf
3. Climbing several flights of stairs
During the past 4 weeks how much time have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
All the time Most of the time
Some of the time
A little of the time
None of the time
4. Accomplished less than you would like
5. Were limited in kind of work or other activities
During the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling anxious or depressed)?
All the time Most of the time
Some of the time
A little of the time
None of the time
6. Accomplished less that you would like
7. Did work or activities less carefully than usual
8. During the past 4 weeks how much did pain interfere with your normal work (including both work outside the home and housework)?
Not at all A little bit Moderately Quite a bit
Extremely
These questions are about how you feel and how things have been during the past 4 weeks. Please give the answer that comes closest to how you have been feeling.
All the time Most of the time
Some of the time
A little of the time
None of the time
9. Have you felt calm and peaceful?
10. Did you have a lot of energy?
11. Have you felt downhearted and/or depressed?
12. How much of the time has your physical or emotional health interfered with social activities (like visiting with friends, relatives, etc.)?
Divide the total score: ______÷56 = __________ _____X5 _____X4 _____X3 _____X2 _____X1
Therapist signature: ___________________________________ Date: ___________________
www.rehabsys.com
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 61
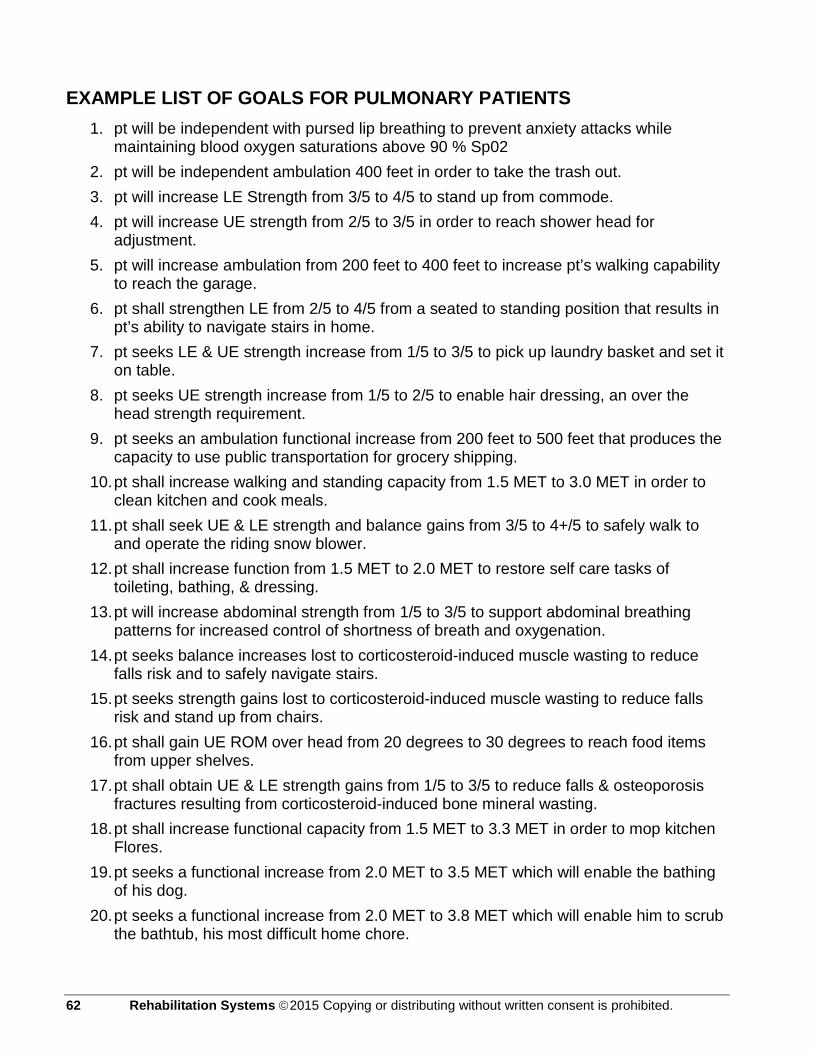
EXAMPLE LIST OF GOALS FOR PULMONARY PATIENTS 1. pt will be independent with pursed lip breathing to prevent anxiety attacks while
maintaining blood oxygen saturations above 90 % Sp02 2. pt will be independent ambulation 400 feet in order to take the trash out. 3. pt will increase LE Strength from 3/5 to 4/5 to stand up from commode. 4. pt will increase UE strength from 2/5 to 3/5 in order to reach shower head for
adjustment. 5. pt will increase ambulation from 200 feet to 400 feet to increase pt’s walking capability
to reach the garage. 6. pt shall strengthen LE from 2/5 to 4/5 from a seated to standing position that results in
pt’s ability to navigate stairs in home. 7. pt seeks LE & UE strength increase from 1/5 to 3/5 to pick up laundry basket and set it
on table. 8. pt seeks UE strength increase from 1/5 to 2/5 to enable hair dressing, an over the
head strength requirement. 9. pt seeks an ambulation functional increase from 200 feet to 500 feet that produces the
capacity to use public transportation for grocery shipping. 10. pt shall increase walking and standing capacity from 1.5 MET to 3.0 MET in order to
clean kitchen and cook meals. 11. pt shall seek UE & LE strength and balance gains from 3/5 to 4+/5 to safely walk to
and operate the riding snow blower. 12. pt shall increase function from 1.5 MET to 2.0 MET to restore self care tasks of
toileting, bathing, & dressing. 13. pt will increase abdominal strength from 1/5 to 3/5 to support abdominal breathing
patterns for increased control of shortness of breath and oxygenation. 14. pt seeks balance increases lost to corticosteroid-induced muscle wasting to reduce
falls risk and to safely navigate stairs. 15. pt seeks strength gains lost to corticosteroid-induced muscle wasting to reduce falls
risk and stand up from chairs. 16. pt shall gain UE ROM over head from 20 degrees to 30 degrees to reach food items
from upper shelves. 17. pt shall obtain UE & LE strength gains from 1/5 to 3/5 to reduce falls & osteoporosis
fractures resulting from corticosteroid-induced bone mineral wasting. 18. pt shall increase functional capacity from 1.5 MET to 3.3 MET in order to mop kitchen
Flores. 19. pt seeks a functional increase from 2.0 MET to 3.5 MET which will enable the bathing
of his dog. 20. pt seeks a functional increase from 2.0 MET to 3.8 MET which will enable him to scrub
the bathtub, his most difficult home chore.
62 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
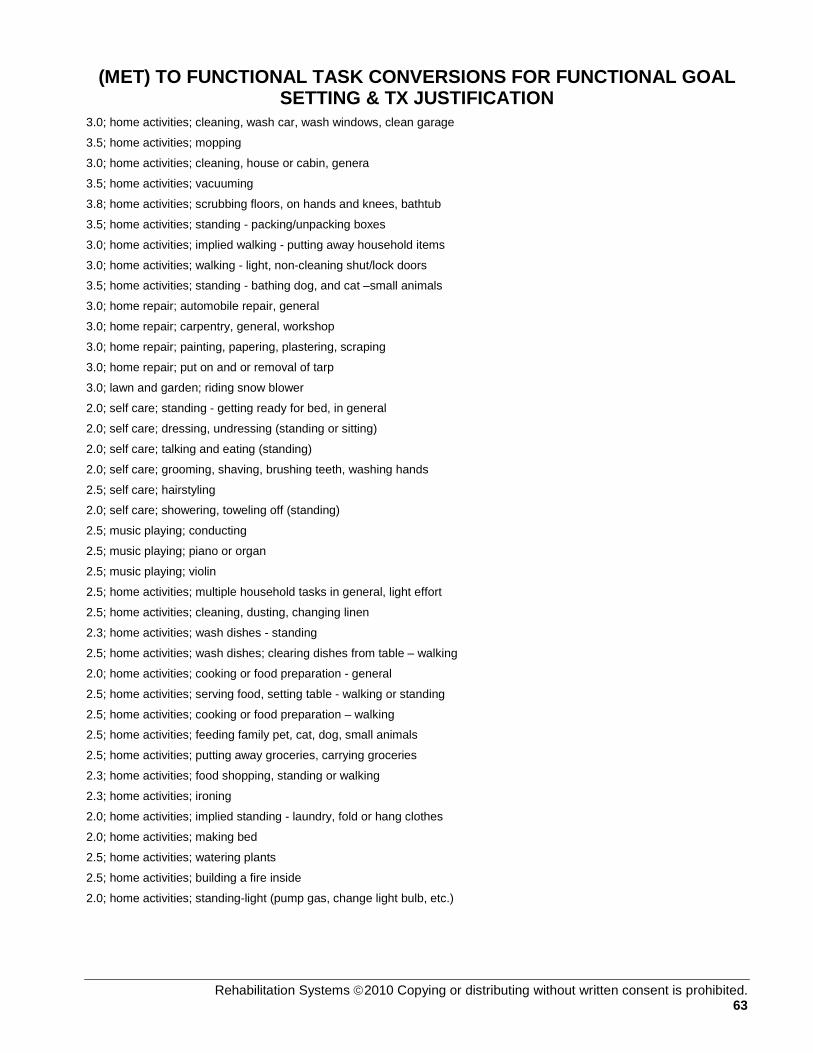
(MET) TO FUNCTIONAL TASK CONVERSIONS FOR FUNCTIONAL GOAL SETTING & TX JUSTIFICATION
3.0; home activities; cleaning, wash car, wash windows, clean garage
3.5; home activities; mopping
3.0; home activities; cleaning, house or cabin, genera
3.5; home activities; vacuuming
3.8; home activities; scrubbing floors, on hands and knees, bathtub
3.5; home activities; standing - packing/unpacking boxes
3.0; home activities; implied walking - putting away household items
3.0; home activities; walking - light, non-cleaning shut/lock doors
3.5; home activities; standing - bathing dog, and cat –small animals
3.0; home repair; automobile repair, general
3.0; home repair; carpentry, general, workshop
3.0; home repair; painting, papering, plastering, scraping
3.0; home repair; put on and or removal of tarp
3.0; lawn and garden; riding snow blower
2.0; self care; standing - getting ready for bed, in general
2.0; self care; dressing, undressing (standing or sitting)
2.0; self care; talking and eating (standing)
2.0; self care; grooming, shaving, brushing teeth, washing hands
2.5; self care; hairstyling
2.0; self care; showering, toweling off (standing)
2.5; music playing; conducting
2.5; music playing; piano or organ
2.5; music playing; violin
2.5; home activities; multiple household tasks in general, light effort
2.5; home activities; cleaning, dusting, changing linen
2.3; home activities; wash dishes - standing
2.5; home activities; wash dishes; clearing dishes from table – walking
2.0; home activities; cooking or food preparation - general
2.5; home activities; serving food, setting table - walking or standing
2.5; home activities; cooking or food preparation – walking
2.5; home activities; feeding family pet, cat, dog, small animals
2.5; home activities; putting away groceries, carrying groceries
2.3; home activities; food shopping, standing or walking
2.3; home activities; ironing
2.0; home activities; implied standing - laundry, fold or hang clothes
2.0; home activities; making bed
2.5; home activities; watering plants
2.5; home activities; building a fire inside
2.0; home activities; standing-light (pump gas, change light bulb, etc.)
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 63

Department of Health and Human Services Healthcare Financing Administration
FORM HCFA-700 (11-91) Part A _______ Part B________ Other______
PLAN OF PROGRESS FOR REHABILITATION (Complete for INITIAL CLAIMS ONLY)
1. Patient’s LAST NAME
FIRST NAME M.I. 2. PROVIDER NUMBER 3. HICN
4. PROVIDER NAME 5. MEDICAL REC NUMBER (OPTIONAL)
6. ONSET DATE 7. SOC DATE
8. TYPE □ Physical Therapy
9. PRIMARY DIAGNOSIS Pertinent Medical DX)
10. TREATMENT DIAGNOSIS 11. Visits From SOC
12. PLAN of TREATMENT/FUNCTIONAL GOALS 13. Freq/Duration (3/wk X 4 wk)
GOALS (Short term)
OUTCOME (Long term)
PLAN Skilled services required:
1)
1)
__Bed Mobility __Transfer training __Gait training __Balance re-ed __Therapeutic ex.
Specify OTHER:
__ROM Contracture mgmt. __W/C training __Muscle re-ed __Energy cons. Modalities
__Pt/caregiver training __Home program __Equipment needs __Safety skills __Other (specify)
2)
3)
2)
4)
5)
14. SIGNATURE
(professional establishing POC, including professional designation)
15. CERTIFICATION FROM ______________ THROUGH_______________N/A ___________
16. I CERTIFY THE NEED FOR THESE SERVICES FURNISHED UNDER THIS PLAN OF TREATMENT AND WHILE UNDER MY CARE Physician signature: ____________________________________
Date: 17. ON FILE (print/type physician name)
18. INITIAL ASSESSMENT age_____ M/F Rehab potential_______________
19. PRIOR HOSPITALIZATION ____________ to___________ N/A_____
20. HX and level of function at start of care:
21. 6-MINUTE WALK TEST ASSESSMENT
Min tolerated
Distance
Heart Rate
% spO2
RPE
Dyspnea
FiO2
22. Tx Justification:
23. Signature (Or name of professional, including professional designation.)
24. Date
25. Service Dates
FROM _____________ THROUGH _____________
64 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
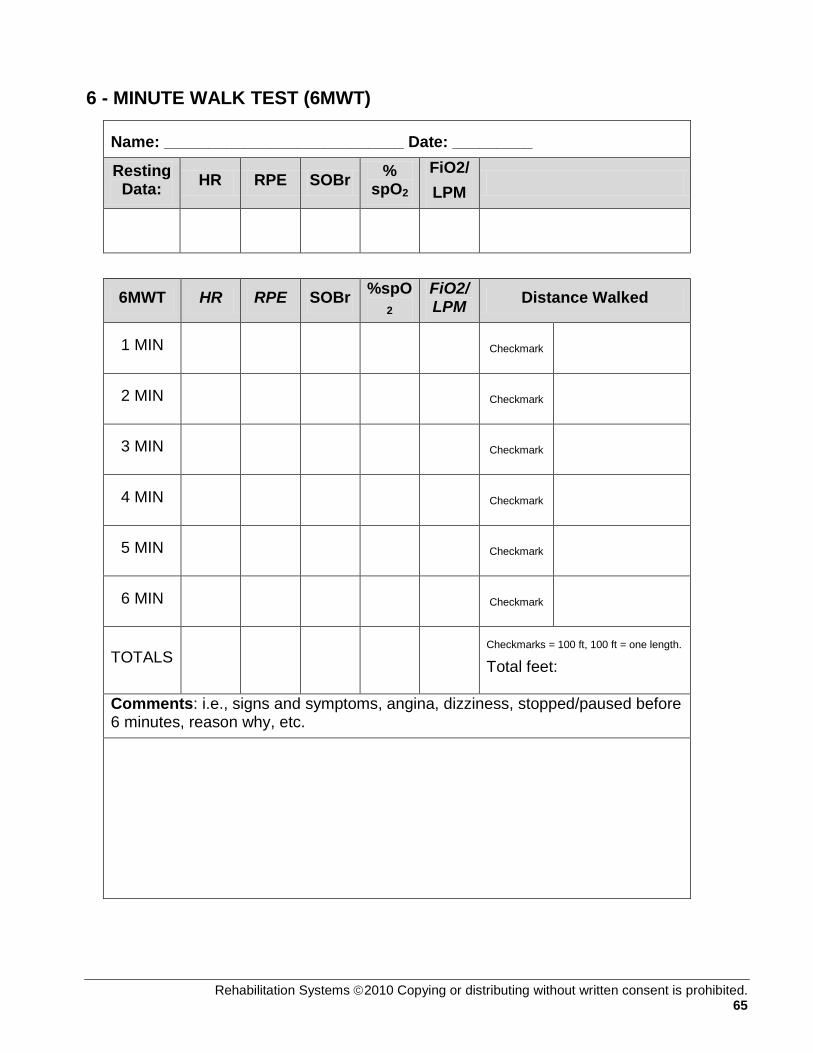
6 - MINUTE WALK TEST (6MWT)
Name: ___________________________ Date: _________
Resting Data: HR RPE SOBr %
spO2 FiO2/ LPM
6MWT HR RPE SOBr %spO2
FiO2/LPM Distance Walked
1 MIN
Checkmark
2 MIN
Checkmark
3 MIN
Checkmark
4 MIN
Checkmark
5 MIN
Checkmark
6 MIN
Checkmark
TOTALS
Checkmarks = 100 ft, 100 ft = one length. Total feet:
Comments: i.e., signs and symptoms, angina, dizziness, stopped/paused before 6 minutes, reason why, etc.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 65

R P E / FT Ratings of Perceived Exertion / Ratings of Fatigue Threshold
How hard are you working? How much are you fatigued?
MODIFIED 10 POINT BORG SCALE
0 Nothing at all 0.5 Very, very slight (just noticeable) 1 Very slight 2 Slight (light) 3 Moderate 4 Somewhat severe 5 Severe (heavy) 6 7 Very severe 8 9 10 Very, very severe (maximal)
66 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
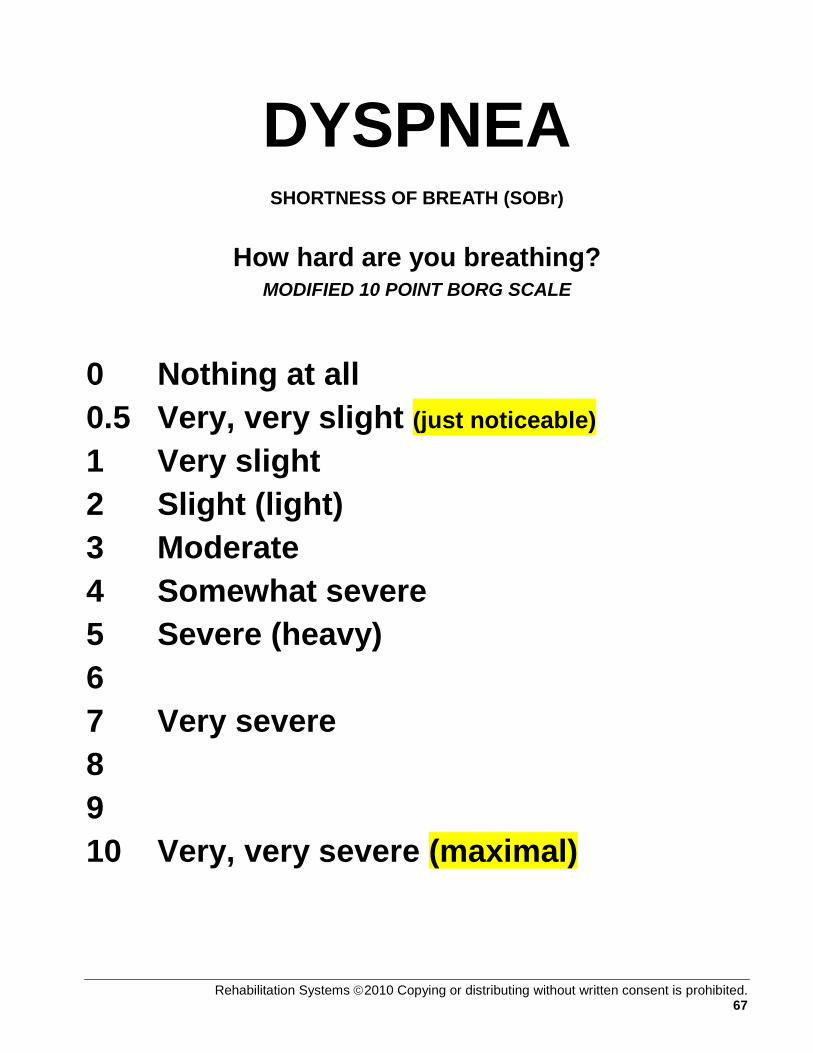
DYSPNEA SHORTNESS OF BREATH (SOBr)
How hard are you breathing? MODIFIED 10 POINT BORG SCALE
0 Nothing at all 0.5 Very, very slight (just noticeable)
1 Very slight 2 Slight (light) 3 Moderate 4 Somewhat severe 5 Severe (heavy) 6 7 Very severe 8 9 10 Very, very severe (maximal)
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 67
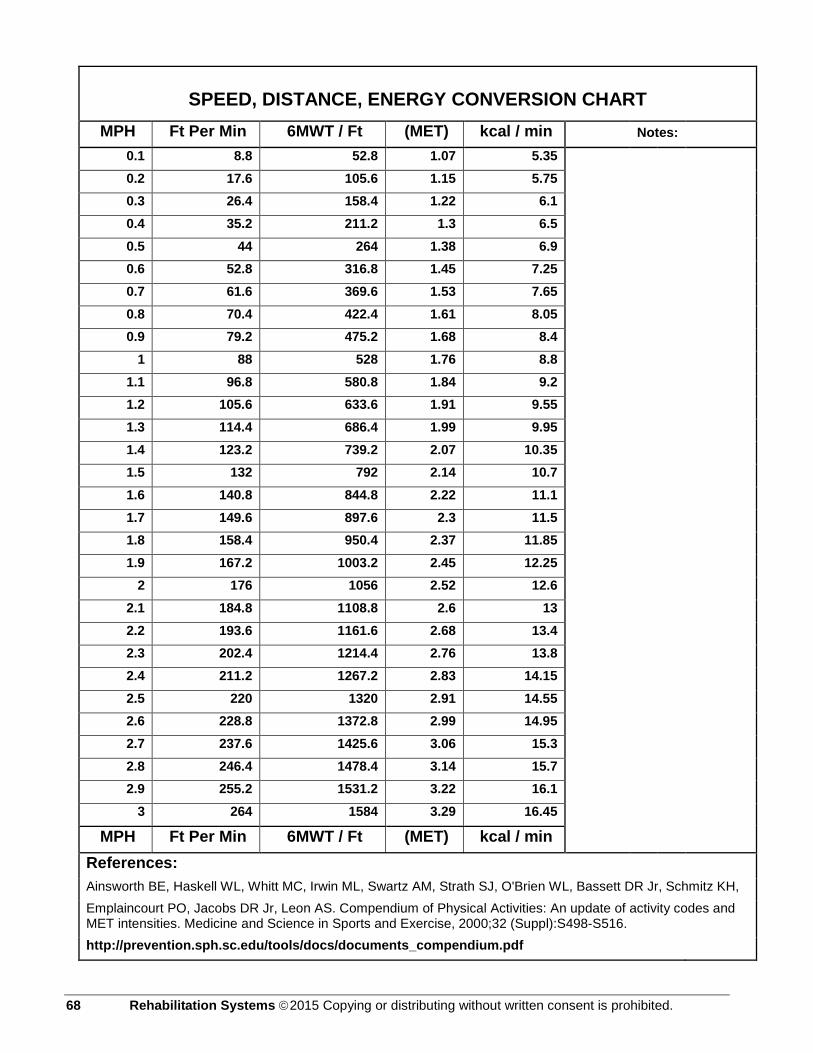
SPEED, DISTANCE, ENERGY CONVERSION CHART MPH Ft Per Min 6MWT / Ft (MET) kcal / min Notes:
0.1 8.8 52.8 1.07 5.35 0.2 17.6 105.6 1.15 5.75 0.3 26.4 158.4 1.22 6.1 0.4 35.2 211.2 1.3 6.5 0.5 44 264 1.38 6.9 0.6 52.8 316.8 1.45 7.25 0.7 61.6 369.6 1.53 7.65 0.8 70.4 422.4 1.61 8.05 0.9 79.2 475.2 1.68 8.4
1 88 528 1.76 8.8 1.1 96.8 580.8 1.84 9.2 1.2 105.6 633.6 1.91 9.55 1.3 114.4 686.4 1.99 9.95 1.4 123.2 739.2 2.07 10.35 1.5 132 792 2.14 10.7 1.6 140.8 844.8 2.22 11.1 1.7 149.6 897.6 2.3 11.5 1.8 158.4 950.4 2.37 11.85 1.9 167.2 1003.2 2.45 12.25
2 176 1056 2.52 12.6 2.1 184.8 1108.8 2.6 13 2.2 193.6 1161.6 2.68 13.4 2.3 202.4 1214.4 2.76 13.8 2.4 211.2 1267.2 2.83 14.15 2.5 220 1320 2.91 14.55 2.6 228.8 1372.8 2.99 14.95 2.7 237.6 1425.6 3.06 15.3 2.8 246.4 1478.4 3.14 15.7 2.9 255.2 1531.2 3.22 16.1
3 264 1584 3.29 16.45
MPH Ft Per Min 6MWT / Ft (MET) kcal / min
References:
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett DR Jr, Schmitz KH, Emplaincourt PO, Jacobs DR Jr, Leon AS. Compendium of Physical Activities: An update of activity codes and MET intensities. Medicine and Science in Sports and Exercise, 2000;32 (Suppl):S498-S516. http://prevention.sph.sc.edu/tools/docs/documents_compendium.pdf
68 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

PLAN OF TREATMENT / EXERCISE PRESCRIPTION AND PROGRESSION Principle In patients with COPD, disability is primarily a result of progressive deconditioning. As the disease progresses, limited ventilatory capacity makes exertion unpleasant and leads to an increasingly sedentary lifestyle. Shortness of breath (breathlessness) and exercise intolerance are the most incapacitating symptoms patients develop. A counter-measure to progressive functional decline in patients with COPD is exercise training. For moderate to severe COPD patients, moderate-intensity aerobic exercise training should be performed to maintain endurance, strength, and function. The goal of exercise at this time is to maintain function and prevent the loss of endurance and strength. COPD treatments exhaust physical and emotional reserves, so the goal of moderate-intensity aerobic exercise training is to maintain these resources. COPD patient are easily fatigued but appear to benefit from moderate-intensity aerobic activities. Moderate-intensity aerobic exercise during this time improves strength and endurance and assists in countering signs and symptoms associated with psychosocial ills. Additionally, special modifications in the type of exercise performed may be required if orthopedic limitations, such as range of motion deficits, occur as a result of surgery, accidents or other orthopedic limitations. For “Lung Cancer” patients, irreversible destruction of the lungs is the hallmark of COPD which accompanies or precedes lung cancer. Significant ventilation-perfusion mismatch occurs, impairing maximal gas exchange. Additionally, the work of breathing is increased secondary to increased airway resistance and hyperinflation. Increased muscle mass and a better vascular system will help improve peripheral extraction of oxygen, which will lead to better physical activity. Evaluate the patients need for bronchodilator therapy, mucolytics or supplemental oxygen during exercise. Therapists will find that frequent follow-up, encouragement and reassurance are integral to the success of the rehabilitation process. Progress in exercise tolerance may be minimal in this population, however diligent participation can reduce respiratory symptoms, reverse anxiety and depression, and increase the ability to perform activities of daily living. Purpose It has clearly been demonstrated that exercise is beneficial for patients who have COPD. Structured exercise protocols and less demanding protocols for very low level COPD patients alike produced significant improvement in exercise tolerance, decreased minute ventilation and improved dyspnea. Although exercise may not lengthen life expectancy, it has been shown to improve the quality of life and therefore should be an integral adjunctive treatment for all pulmonary patients.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 69
Components of an Exercise Prescription An exercise prescription generally includes the following specific recommendations:
• Type of exercise or activity (i.e. strength training, walking, cycling, swimming, chopping wood, fishing, cleaning house, washing the car…)
• Specific workloads (i.e. MPH, MET, FPM-walking speed, Kcal/min, ) • Duration-(variable) and frequency-(fixed:3 X Wk) of the activity or exercise session • Intensity guidelines – Target heart rate (THR) range and estimated rate of (RPE),
(SOBr), (Fatigue). Precautions or contraindications regarding oxygen saturation such as: Keep oxygen saturation > 88% Sp02 at all times during the therapeutic exercise session or an orthopedic, cardiac or co-morbidity concern may require close supervision. The 6 Minute Walk Test (6MWT) is used to establish the exercise prescription of the patient in both the in & out patient setting. Many COPD patients will not likely complete the full (6MWT). However, the information collected from the test is valuable. Special attention should be paid to Oxygen Saturation (%Sp02), Ratings of Perceived Exertion (RPE), Dyspnea (SOBr), Heart Rate (HR), and Fraction of Inspired Oxygen or Liters Per Minute (Fi02/ LPM) when identifying exercise intensity. Subjective vs. Objective Measurements Subjective measurements are (RPE), (SOBr) (Fatigue) Objective measurements are (HR), (%Sp02), (Fi02/LPM). Low stress threshold V. High stress threshold (Resiliency) Low stress threshold is categorized by high subjective ratings with low objective measurements. High stress threshold is categorized by low subjective ratings with high objective measurements. If the Heart Rate remains low 80 to 100 and RPR-FT/SOBr are high between 6 and 7, one may conclude that the patient has a lower stress threshold or deconditioned functional capacity and is appropriate to start at a lower intensity level of RPR/SOBr of 2 to 3. Conversely, if the patient achieves a Heart Rate of 100 to 120 and reports an RPE-FT/SOBr of 3 to 4, this patient has a higher stress threshold and is appropriate to start at a moderate intensity level of RPE-FT/SOBr of 3 to 4. Procedure Sure and safe progression is consistently achieved in the COPD diseased population with incremental increases in prescriptive exercise intensity, type, and duration. Start Low and Go Slow.
70 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Exercise Dose – Response Relationship
With A Gradual Upslope in Progression
Moderate Intensity (Better for Outpatient programs) Medicare B, Outpatient Programs-(OP). (OP Clinic, ALF, ILF, Home)
Low Intensity (Better for Inpatient programs) Medicare A, RUG, Inpatient Programs. (SNF, HHA)
Exercise to promote functional independence Activity to maintain function or prevent deconditioning
Accumulate 60 minutes 3 to 4 days per week. RPE 4-6 on 10 point scale. Typically: Out Patient Programs.
Accumulate 15-25 minutes of activity that is well-tolerated three times a day, 4 to 5 days per week and gradually increase exercise time and intensity, RPE 2-4 on 10 point scale. Typically: In Patient Programs.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 71
General Aerobic Exercise Recommendations Parameter Recommendation and Comment Mode
Most exercises involving large muscle groups are appropriate, but walking, cycling, and NuStep, are especially recommended. The key is to modify exercise mode based on acute or chronic treatment effects of pulmonary exacerbations.
Frequency At least 3 times/wk, but daily exercise may be preferable for severely deconditioned inpatients performing lighter-intensity and shorter-duration exercises.
Intensity Moderate intensity, depending on patient's current fitness level and severity of side effects from treatments. Guidelines include 50%-75% VO2max or HRreserve, 60%-70% HRmax, or an RPE of 4-6. HRreserve is the best guideline if HRmax is estimated rather than measured.*
Duration At least 20-30 min of continuous activity, but this goal may require multiple intermittent shorter bouts (eg, 5-10 min) with rest intervals in deconditioned patients or those experiencing severe side effects of treatment.
Progression Initial progression should be in frequency and duration. Only when these goals are met should intensity be increased. Progression should be slower and more gradual for deconditioned patients or those with severe side effects of treatment.
72 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
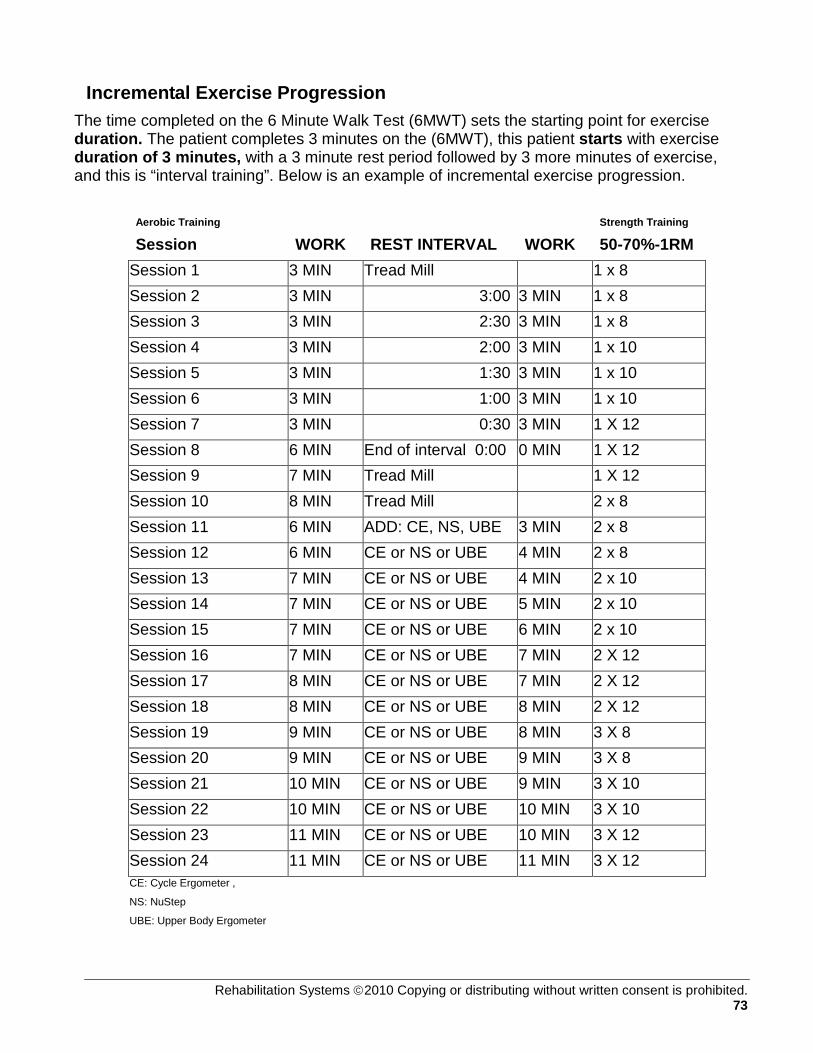
Incremental Exercise Progression The time completed on the 6 Minute Walk Test (6MWT) sets the starting point for exercise duration. The patient completes 3 minutes on the (6MWT), this patient starts with exercise duration of 3 minutes, with a 3 minute rest period followed by 3 more minutes of exercise, and this is “interval training”. Below is an example of incremental exercise progression.
Aerobic Training
Session WORK REST INTERVAL WORK Strength Training
50-70%-1RM Session 1 3 MIN Tread Mill 1 x 8 Session 2 3 MIN 3:00 3 MIN 1 x 8 Session 3 3 MIN 2:30 3 MIN 1 x 8 Session 4 3 MIN 2:00 3 MIN 1 x 10 Session 5 3 MIN 1:30 3 MIN 1 x 10 Session 6 3 MIN 1:00 3 MIN 1 x 10 Session 7 3 MIN 0:30 3 MIN 1 X 12 Session 8 6 MIN End of interval 0:00 0 MIN 1 X 12 Session 9 7 MIN Tread Mill 1 X 12 Session 10 8 MIN Tread Mill 2 x 8 Session 11 6 MIN ADD: CE, NS, UBE 3 MIN 2 x 8 Session 12 6 MIN CE or NS or UBE 4 MIN 2 x 8 Session 13 7 MIN CE or NS or UBE 4 MIN 2 x 10 Session 14 7 MIN CE or NS or UBE 5 MIN 2 x 10 Session 15 7 MIN CE or NS or UBE 6 MIN 2 x 10 Session 16 7 MIN CE or NS or UBE 7 MIN 2 X 12 Session 17 8 MIN CE or NS or UBE 7 MIN 2 X 12 Session 18 8 MIN CE or NS or UBE 8 MIN 2 X 12 Session 19 9 MIN CE or NS or UBE 8 MIN 3 X 8 Session 20 9 MIN CE or NS or UBE 9 MIN 3 X 8 Session 21 10 MIN CE or NS or UBE 9 MIN 3 X 10 Session 22 10 MIN CE or NS or UBE 10 MIN 3 X 10 Session 23 11 MIN CE or NS or UBE 10 MIN 3 X 12 Session 24 11 MIN CE or NS or UBE 11 MIN 3 X 12 CE: Cycle Ergometer ,
NS: NuStep
UBE: Upper Body Ergometer
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 73
Work-Rest Ratio The Work-Rest-Ratio (WRR) as a method of interval training serves best at the beginning of the low level patients program and should follow the One-to-One (1:1) (WRR) rule, i.e., Work 3 minutes: Rest 3 minutes: Work 3 minutes. The Work-Rest-Ratio-Interval (WRRI) should decrease in 30 second increments from threptic session to therapeutic session or as the patient tolerates without fatigue hangovers. Once the (WRRI) has been closed, the therapist may add one (1) minute of exercise duration per exercise session or as the patient tolerates without fatigue hangovers. (Causing a “Fatigue Hangover” is a cardinal sin) The optimal aerobic activity segment should seek to reach the following “Best Case Scenario”. GOAL: Best Case Scenario; 15 minutes walking/treadmill, 15 minutes cycling, with 20 minutes of upper and lower extremity strength training exercises. Prescribing exercise in the chronic diseased population requires a significant amount of planning and encouragement. The exercise prescription should proceed gradually since most individuals are extremely limited in the amount of exercise tolerated secondary to deconditioning, dyspnea, exertional distress or hypersensitivity to exertion. References United States Army Center for Health Promotion and Preventive Medicine 5158 Blackhawk Road. Aberdeen Proving Ground, Maryland 21010-5403 MAJ Robert L. Gauer, MD, FACSM, LTC Francis G. O.Connor, MD, FACSM COL Willis B. Campbell, MD, Ph.D., MPH, FACSM Fundamentals of Resistance Training: Progression and Exercise Prescription KRAEMER, WILLIAM J.; RATAMESS, NICHOLAS A. Medicine & Science in Sports & Exercise: April 2004 - Volume 36 - Issue 4 - pp 674-688 Is the 6 Min Walk Test An Acceptable Measure of Progression in Cardiac Rehabilitation Programmes? Derman, E W FACSM; Dreyer, L A; Schwellnus, M P FACSM; Noakes, T D FACSM. Medicine & Science in Sports & Exercise: May 2001 - Volume 33 - Issue 5 - p S319 H15g Free Communication/Poster Adults With Chronic Diseases and Disabilities Exercise in Rehabilitation Medicine, 2nd Edition Sliwa, James A. D.O. Medicine & Science in Sports & Exercise: November 2006 - Volume 38 - Issue 11 - p 2036
74 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
INDIVIDUAL THERAPEUTIC SESSION, SOAP NOTE FORMAT Principle Each therapeutic session is an opportunity to provide exercise in a controlled and monitored environment, and education that not only enhances exercise, but also improves all aspects of function. Each session will build on the previous session in both fitness and knowledge. Purpose Exercise sessions should focus on individual needs and aim to progress the patient to a higher level of functioning. Patient goals should be discussed and reviewed at various points throughout the sessions to assist in measuring progress. Documentation during each session also helps both therapists and patients measure success.
Procedure
Subjective Record subjective information that the patient reports, such as, how they are feeling or sleeping.
Objective Record a productive chough, or sleep disturbance such as waking up to breathe.
Measurements • HR (Heart Rate) • BP (Blood Pressure) • % spO2 • RPE/SOBr/Fatigue
Physiological Changes During Exercise
What do these measurements mean? You expect the heart rate to increase with exertion. You should also see an increase in blood pressure with exercise. Oxygen usage will increase, but the % sp O2 should remain above 88% at all times during exercise. Any sudden change in any of the baseline measurements or subjective reporting indicates a need to decrease or even stop the exercise. Monitoring changes will allow you to determine whether to increase or decrease the intensity of the therapeutic session or seek medical attention from the patient’s physician.
Aerobic Exercise There are various modes that can be used for aerobic exercise. Ideally two modes of aerobic exercise will provide variety if the patient can tolerate the exercise duration. The treadmill is the most important mode of aerobic training as it easily translates into ADL's and functional independence.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 75

• All aerobic exercise must begin with a 3 min warm up and conclude with a 3 min cool down at minimal loads.
• Aerobic training requires only one warm up and one cool down. Transitioning between equipment is exempt from WU & CD workloads.
• COPD patients often have balance and falls-risk issues so they must be monitored for safety while on exercise equipment. As a rule, most COPD patients will require balance and gait training to counter the lean tissue waisting that occurs from chronic corticoid steroid use.
Resistance Exercise
Resistance exercise is patient dependent; therefore, adjusting intensity, and volume should be considered based on patient needs, ability, and history.
• Resistance exercise is very important for LE & UE as it translates into ADL's.
• Resistance exercise is an emerging research focus for COPD patients as it’s revealing functional outcomes equivalent to aerobic exercise training.
• Resistance exercise progression is outlined in the following guidelines: o Sets & Reps:
1x8, 1x10, 1x12, 2x8, 2x10, 2x12, 3x8, 3x10, 3x12.
• ROM exercise may be “medically necessary”, thus, ROM therapy should be carefully attended to.
Patient Education
Exercise sessions will include education associated with your condition. Successive education will build on previous education. You will be asked to read about the benefits of exercise and proper exercise, and you will be given tips for making everyday tasks easier.
• 8 sessions should be taught and documented. • Patient education is a partnership, ask the patient to pre-read, and then
cover the section & answer questions once a week in a 15-minute lesson session.
Follow-up Complete SOAP notes and documentation.
Assessment Document how the patient tolerated the exercise session using intensity, duration, frequency, and mode (IDFM).
Plan Document goals and/or changes for the next session using IDFM.
Measurements Allow the patient to cool down, and then collect final measurements and compare to baseline measurements. The resting heart rate should be within 8 beats of the baseline.
76 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

SOAP NOTE
Pulmonary Rehabilitation
Session # Patient Name: Date:
Subjective: Patient feels (check one) О Good О Fair О Poor
Objective:
Resting Measurements Aerobic Exercise
Start Tx End Tx Requirement Type Duration Int HR BP %
SpO2 FiO2
HR HR <100 to DC
Warm up (3 Min)
BP BP <200/110
%spO2
%spO2
>88%
FiO2 FiO2 Keep % spO2 >88
Education: Notes:
Cool Down (3 Min) RPE/DYSP/Fatigue (1-10)
Strength Training Sets (1-3) Reps (8-12) Load (lbs)
Leg Press Chest Press Overhead Press Pull Downs Rowing
Assessment:
Planning:
Therapist
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 77

PULMONARY PATIENT EDUCATION The patient education resource is produced by the American College of Chest Physicians. The following outline will guide you through weekly education objectives throughout the duration of the entire program.
WEEK Initial & Date Patient Activities & Education Outline Checklist 1 Orientation: COPD Patient Evaluation, H&P 1 6 Min Walk Test, SF~36 HQOL Survey. ACCP Education Book- 1 Important Steps 1: Quit Smoking. 2 Important Steps 2: Flu & pneumonia shots. 3 Important Steps 3: Medications, pages 12 - 20. 3 Important Steps 3: Medications, pages 21-28. 4 Important Steps 4: Exercise and Nutrition. 5 Important steps 5: Energy Conservation and Stress Control 6 Important steps 6: Control Your Breathing 6 Develop the Home Exercise Program (HEP) 7 Important step 7: Use Oxygen Therapy 8 Important step 8: Manage Acute Exacerbation
12 6 Min Walk Test/SF-36 HQoL Survey 12 Progress letter written and mailed to referring practitioner. 14 Follow-up phone call on HEP and pt’s continued progress.
Notes:
78 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 79
EARLY WARNING SIGNS OF RESPIRATORY EXACERBATIONS Early detection of exacerbation can prevent or interrupt a serious bout of illness and or a hospital admission. A change or increase in the symptoms you often have may be the only early warning sign. You may notice one or more of the following:
• An increase or decrease in the amount of sputum produced
• An increase in the thickness or stickiness of sputum
• A change in sputum color to yellow or green or the presence of blood in the sputum
• An increase in the severity of shortness of breath, cough and/or wheezing
• A general feeling of ill health
• Ankle swelling
• Forgetfulness, confusion, slurring of speech and sleepiness
• Trouble sleeping
• Using more pillows or sleeping in a chair instead of a bed to avoid shortness of breath
• An unexplained increase or decrease in weight
• Increased feeling of fatigue and lack of energy that continues
• A lack of sexual drive
• Increasing morning headaches, dizzy spells, restlessness
Symptoms do not go away when they are ignored. Therefore, knowing when to call your health care provider is very important in managing your chronic lung disease. It is very important for you to work with your health care provider to determine the best treatment for signs and symptoms of COPD.
80 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
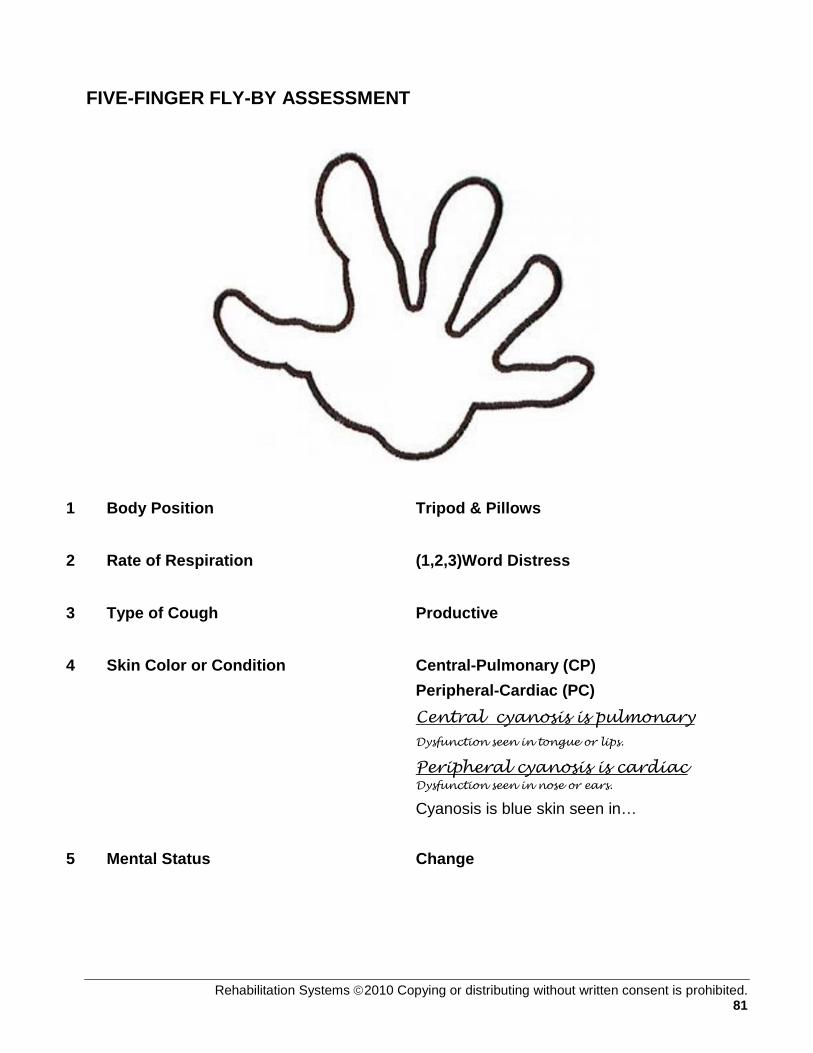
FIVE-FINGER FLY-BY ASSESSMENT
1 Body Position Tripod & Pillows
2 Rate of Respiration (1,2,3)Word Distress
3 Type of Cough Productive
4 Skin Color or Condition Central-Pulmonary (CP) Peripheral-Cardiac (PC) Central cyanosis is pulmonary Dysfunction seen in tongue or lips.
Peripheral cyanosis is cardiac Dysfunction seen in nose or ears.
Cyanosis is blue skin seen in…
5 Mental Status Change
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 81

EXACERBATION / DISTRESS INTERVENTIONS
Body Positioning Severe distress. SOB SCALE 7-10
Excessive accessory muscle use. Tripod body position. The patient is unable to breathe unless maintaining a sitting position.
Orthopnea The number of pillows a patient uses to rest comfortably is another indicator of respiratory. Note whether the patient uses one-, two-, three-, or four-pillows to rest. An increase in the number of pillows to rest indicates an increase in dyspnea.
Interventions
1. Administer oxygen to keep oxygen saturation at 88% or higher. 2. Encourage the patient to employ energy conservation efforts. 3. Encourage the patient to employ more efficient breathing techniques.
Accessory muscle use
Employing accessory muscles to improve oxygenation can drain valuable energy reserves. Assisting the patient in using available resources effectively may decrease the possibility of exacerbation.
Interventions
1. Encourage pursed-lip breathing to slow rapid respiration and reduce collapse of airways during exhalation. See Breathing Retraining procedure.
2. Sit patient at the edge of the bed with arms folded and resting on a bedside table. This will promote expansion of the lungs and assist the accessory muscles to perform more efficiently.
3. If needed, encourage proper diaphragmatic breathing by pushing in on abdomen during exhalation. The belly should expand outward with inspiration.
4. Place hands on the trapezius muscles to encourage patient to drop the shoulders and expand the lungs in the correct direction for more efficient use.
82 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Rate of Respirations Severe distress SOB SCALE 7-10.
This level is indicated if the patient can only speak a few words without a pause. This is identified as “two-word” or “three-word” distress. A change from a rapid rate to a slow rate in a patient with respiratory distress suggests extreme fatigue and the possibility of respiratory arrest.
Interventions
1. Administer oxygen to keep oxygen saturation at 88% or higher. 2. Encourage the patient to employ energy conservation efforts. If breathing
effort does not return to normal perform a more focused assessment to determine status of possible exacerbation.
3. Encourage the patient to employ more efficient breathing techniques.
Type of Cough Ineffective cough, Severe distress. SOB SCALE 7-10.
The patient lies in bed with poor intake of air resulting in small ineffective coughs. The airway is not cleared and the patient begins to appear fatigued, and has increasing anxiety.
Interventions
1. Administer oxygen to keep oxygen saturation at 88% or higher. Humidify air if more than three liters per minute are administered.
2. Ensure adequate fluid intake of 2 to 3 liters per day to liquefy secretions. 3. Staged breathing.
i. The patient should assume a sitting position, or the head of the bed should be raised to 45 degrees, with head slightly flexed, shoulders relaxed, knee’s flexed, feet on the floor, if possible, and forearms supported by a pillow. The patient then drops the head and bends forward while using slow, pursed-lip breathing to exhale. Sitting up again, the patient uses diaphragmatic breathing to inhale slowly and deeply. Repeating this breathing pattern three to four times should facilitate mobilization of secretions.
4. Huff coughing. i. Before initiating a cough, the patient should take a deep abdominal
breath, bend slightly forward, and then huff cough (cough three to four times on exhalation). The patient may need to splint the thorax or abdomen to achieve a maximum cough.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 83

Skin color or condition Cyanosis. Severe distress. SOB SCALE 7-10.
Peripheral cyanosis is associated with cardiac dysfunction. Peripheral cyanosis is noted by a bluish or purplish tinge at the extremities or in the nose or ears. When assessing capillary refill time, there is no blanching of the nail bed. Central cyanosis is more closely associated with pulmonary function. Central cyanosis is noted by a bluish or purplish tinge to the central areas such as the tongue, conjunctivae, or inner surface of the lips. The nail beds may appear cyanotic, but blanch under pressure and refill time is normal. Pallor, mottled, or glossy skin indicates chronic decreased arterial perfusion.
Interventions
1. Administer oxygen to keep oxygen saturation at 88% or higher. 2. Encourage the patient to employ energy conservation efforts. If breathing
effort does not return to normal perform a more focused assessment to determine status of possible exacerbation.
3. Encourage the patient to employ more efficient breathing techniques, (see Breathing Retraining).
4. If peripheral cyanosis is evident transport the patient to the nearest Emergency Department and contact the physician.
Mental Status Mild to severe. Severe distress. SOB SCALE 7-10.
Any changes in mental status such as agitation, combative behavior, confusion, or decreased level of consciousness require immediate intervention because this change may indicate the onset of rapid deterioration.
Interventions
1. Administer oxygen to keep oxygen saturation at 88% or higher. 2. Encourage the patient to employ energy conservation efforts, (see Energy
Conservation). 3. Encourage the patient to employ more efficient breathing techniques, (see
Breathing Retraining). 4. If mental status does not improve or continues to deteriorate, transport the
patient to the nearest Emergency Department and contact the physician.
84 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
ENERGY CONSERVATION
Principle Energy conservation consists of tasks that are utilized to minimize energy expenditure in the patient with low or no reserves for maintaining basic life support. Conservation methods can be used with patients who struggle with daily tasks due to a chronic condition such as COPD or CHF. Methods can be used when a patient is unable to breathe within normal limits for that patient, and is using alternative breathing techniques that will further drain reserves and lead to distress or exacerbation.
Purpose Rehabilitation and nursing personnel can assist the patient in performing energy conservation tasks to relieve expenditure of reserves when a patient is working hard to breathe. Assisting the patient to conserve energy will bring control back to the patient, prevent exacerbation, and diminish the need for emergency care.
Procedure
Activity intolerance Decreased tolerance is evident when a patient is unable to complete ADL’s without assistance.
Interventions
1. Assist patients to avoid excessive tiring by combining activities when possible to shorten time involved to complete tasks.
2. Locate needed items for personal grooming within easy reach such as on a bedside table, to avoid standing for long periods of time.
3. Stop activities or exercise that produce excessive shortness of breath or tachycardia.
4. Allow for adequate rest periods between activities. 5. Make use of comfort measures that promote rest, such as massage,
encouraging personal items of comfort, changing locations away from drafts, improving lighting, etc.
6. Teach the patient to rate fatigue level on a scale of 0-10. See Modified 10 Point Borg Scale.
7. Save large tasks for when the patient has a low level of fatigue such as a score of 0-2.
8. Small tasks can be accomplished with monitoring during medium levels of fatigue such as from 3-6.
9. For greater fatigue levels rating 7 or higher, provide rest opportunities and monitor for potential breathing difficulties (see Five-Finger Fly-By Assessment and Exacerbation Interventions).
10. Continually identify priorities and eliminate non-essential activities.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 85

Anxiety and irritability Low oxygen levels can cause a patient to become anxious and/or irritable. The change in disposition from calm to irritable increases energy expenditure and can lead to distress.
Interventions
1. Make an effort to reduce anxiety and irritability that can drain reserves. 2. Reduce stressors and respond promptly to patient’s concerns. 3. Accept irritability without provoking further aggressive responses. 4. Provide appropriate encouragement for progress.
Altered Body Positioning while effective for mild or moderate respiratory distress, tripod positions are not encouraged for severe respiratory distress. When the patient has to support the body in an upright position using arm strength, fatigue will occur quickly and the patient will lose valuable energy needed for basic survival.
Interventions Use a High Fowler’s position or dangle at the bedside with arms folded across a bedside table. Use of these positions will decrease the amount of work it takes to stay upright with the chest expanded for better lung efficiency.
Altered secretion clearance the elderly, and those with chronic respiratory conditions, have decreased ability to mobilize secretions. This can lead to infection and can quickly tire a person already struggling to breathe. Interventions Energy conservation methods can be applied to coughing, called stage-controlled coughing. Teach the patient to use a huff-cough method, by huffing several times with exhalation to promote secretion movement and then one strong cough. (See Exacerbation Interventions and Breathing Retraining procedures for details.)
References Finlayson, M., Shevil, E., Luo, P., Chen, H. Y., & Mathiowetz, V. (2007). Effects of cognition on quiz performance, behavior change, and vitality after energy conservation course among people with multiple sclerosis. International Journal of MS Care, 9, 13‐21. Fisk, J. D., Ritvo, P. G., Ross, L, Haase, D. A., Marrie, T. J., & Schlech, W. F. (1994). Measuring the functional impact of fatigue: Initial validation of the fatigue impact scale. Clinical Infectious Diseases, 18 (Suppl 1), S79‐83. Mallik, P. S., Finlayson, M., Mathiowetz, V., & Fogg, L. (2005). Psychometric evaluation of the Energy Conservation Strategies Survey. Clinical Rehabilitation, 19, 583‐543. Carpenito, L.J., (2002), Handbook of Nursing Diagnosis and Nursing Diagnosis, Application to Clinical Practice, J.B. Lippincott Co.
86 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
RELAXATION AND STRESS MANAGEMENT Principle Relaxation and stress management will help increase the quality of life. Stress can have negative effects on the body, such as decreased energy, hypertension, blood sugar imbalances, and impaired cognitive function. Purpose The purpose of this module is to help educate and incorporate stress and relaxation techniques into our patient’s lives. Procedure The word stress is derived from the Latin work stringer which means to “draw tight.” Long term or prolonged stress is a serious threat to a person’s emotional and physical health. As stress increases or the number of stressors increase a person’s ability to effectively adapt is decreases. Stress can be defined as any type of change that causes physical, emotional or psychological strain. Stress causes the body to release a hormone called cortisol. Prolonged high levels of cortisol can lead to heart disease and other health problems. Cortisol is an important hormone in the body, secreted by the adrenal glands and is involved in the following functions:
• Glucose metabolism • Regulation of blood pressure • Insulin release for blood sugar maintenance • Immune function • Inflammatory response
Cortisol normally is present in the body at higher levels in the morning and at its lowest at night. Although stress isn’t the only reason that cortisol is secreted into the bloodstream, it is termed “the stress hormone” because it’s also secreted in higher levels during the body’s ‘fight or flight’ response to stress. Cortisol is accountable for several stress-related changes in the body. While cortisol is important and a helpful part of the body’s response to stress, it’s important that the body’s relaxation response be activated so the body’s functions can return to homeostasis. Higher and more prolonged levels of cortisol in the bloodstream have been shown to have negative effects, such as:
• Impaired cognitive performance • Suppressed thyroid function • Blood sugar imbalances such as hyperglycemia • Decreased bone density • Decrease in muscle tissue • Higher blood pressure
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 87

Lowered immunity and inflammatory responses in the body To keep cortisol levels healthy and under control, the body’s relaxation response should be activated after the fight or flight response occurs. You can learn to relax your body with various stress management techniques, and you can encourage lifestyle changes in order to keep the body from reacting to stress in the first place. The following have been found by many to be very helpful in relaxing the body and mind, aiding the body in maintaining healthy cortisol levels:
• Guided Imagery • Self-Hypnosis • Exercise • Yoga • Listening to Music • Breathing Exercises • Meditation • Anti-anxiety Medications
Relaxation is a form of control. Cortisol secretion varies among individuals. Studies have shown that people who secrete higher levels of cortisol in response to stress also tend to eat more food, and food that is higher in carbohydrates than people who secrete less cortisol. If you’re more sensitive to stress, it’s especially important for you to learn stress management techniques and maintain a low-stress lifestyle. References
Beck, J. G., Stanley, M. A., Baldwin, L. E., Deagle, E. A., III, and Averill, P. M. Comparison of cognitive therapy and relaxation training for panic disorder. J Consult Clin Psychol 1994;62(4):818-826. Boyce, P. M., Talley, N. J., Balaam, B., Koloski, N. A., and Truman, G. A randomized controlled trial of cognitive behavior therapy, relaxation training, and routine clinical care for the irritable bowel syndrome. Am.J Gastroenterol. 2003;98(10):2209-2218 Linton, D. K., Matteson, M. A. & Maebuis, N. K. (2000). Introductory Nursing Care of Adults. (2nd Ed.). W.B. Saunders Company: Philadelphia. Lewis, S. K., Heitkemper, M. M. & Dirkesen, S.R. (2004). Medical Surgical Nursing. Assessment and Management of Clinical Problems.(6th ed.). Mosby, INC. St. Louis.
McGrady, A. V., Kern-Buell, C., Bush, E., Devonshire, R., Claggett, A. L., and Grubb, B. P. Biofeedback-assisted relaxation therapy in neurocardiogenic syncope: a pilot study. Appl.Psychophysiol.Biofeedback 2003;28(3):183-192.
88 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

DIETARY GUIDELINES FOR PULMONARY PATIENTS Practical Approaches to Nutrition in Patients with COPD
A general approach includes eating foods that you like, and finding ways to eat healthy things that you also like.
Balanced Diet
Most nutritionists recommend a balanced diet. A balanced diet contains calories from a combination of protein, fat (from animal or vegetable sources), and carbohydrates (sugars and starches). A balanced diet should also contain an adequate number of the essential minerals and vitamins. If you are too thin or losing weight, you should try to eat more. This usually means more frequent, small meals. The possible advantage of eating this extra food as protein or fat rather than carbohydrates is discussed below.
Foods to Avoid
There are no special foods you need to avoid. If you produce a lot of phlegm, some people find that milk and other dairy products tend to either make more phlegm or make it thicker. Try reducing dairy products for yourself, since this helps some people but not others. If you like milk and cheese, and this does not seem to make your phlegm worse, then drink and eat them. If you find an increase in phlegm production or phlegm thickness when you eat milk products, then you will want to avoid them. If foods cause a particular problem for you, then avoid them. For example, if a particular food causes you to have gas which may be uncomfortable and distend your stomach and cause you to eat less, and then avoid these foods.
Water and Fluid Intake
Having a high water and fluid intake, in general, is helpful. It may be particularly important in patients with COPD with excessive phlegm production. Liberal drinking of water may allow the body to thin the mucus or phlegm, so that it is easier to cough out. Expensive bottled water has no benefit over tap water. The timing of fluid intake may be important to those patients who have to get up at night to urinate. Drinking more fluid earlier in the day may help avoid extra trips to the bathroom at night. Fluid retention with swelling of the legs can be a problem, particularly for patients with COPD and heart disease. Fluid retention is more a problem of excessive salt intake than excessive fluid intake. Salt causes you to hold the fluid in your body. If you limit salt in your diet, then the water that you drink will not be held in the body but will be eliminated in the urine or by perspiration. If you have fluid retention, the best therapy is limiting salt intake or combing that with a diuretic (“water pill”), not limiting the amount of water you drink. Chronic fluid retention may be more troublesome and should be discussed with your doctor.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 89
Alcohol Excessive amounts of alcohol can be harmful (for anyone). High alcohol levels can interfere with breathing. Ask your doctor for specific guidelines regarding alcohol. Your doctor might tell you to avoid or limit alcoholic beverages. Alcoholic beverages do not have much nutritional value and can interact with the medicines you are taking, especially oral steroids. Too much alcohol might slow your breathing and make it difficult for you to cough up mucus.
Other Considerations
Nutritional needs are tied to other aspects of your health, including your lung problems. Other aspects discussed may allow you to preserve your energy and still maintain your activity. For example, learn to be more efficient (get things done with less work), using the muscles of breathing while you exercise can modify your nutritional needs. If you are losing weight, consider ways to reduce your work of breathing. Consider the use of oxygen if appropriate (if your blood oxygen level is low), and consider balancing the adverse nutritional effects of medications (especially corticosteroids), against the potential beneficial effects.
Anabolic corticosteroids (the same medicine used- or abused- by bodybuilders) and growth hormones have been tested in experimental animals and are beginning to be tested on humans. Studies in patients with COPD are beginning to suggest benefit. More studies are needed in analyzing the use of hormones.
Low Carbohydrate Diets and Food Supplements
If you eat the same amount of calories in the form of carbohydrates (sugar and starches) compared to fat or protein, you will produce relatively more carbon dioxide. Since you eliminate carbon dioxide by breathing, this means you will have to breathe more to get rid of carbon dioxide if your diet is high in carbohydrates. On the other hand, carbohydrates can be converted to energy more quickly than fat or protein. The greater carbon dioxide production from carbohydrate is not usually an important issue for patients with COPD and should not be a major factor in determining the balance between protein, fat, and carbohydrate food sources. An exception might be the patient with severe COPD under stress with an acute episode (acute exacerbation of chronic bronchitis).
The food industry has promoted the use of canned food supplements. Commercial food supplements targeted at patients with COPD are relatively low in carbohydrates and high in protein and fat. These commercial food supplements tend to be relatively expensive. The same effect, a higher intake of calories to counteract weight loss, can be achieved more economically by eating normal food. Food supplements may be useful in selected patients, but even then, less expensive alternatives are usually just as effective.
90 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Vitamins and Other Supplements Most balanced diets contain enough vitamins to meet your basic needs. On the other hand, taking a multi-vitamin is safe and may be helpful. COPD, especially the emphysema part, is a disease thought to involve so-called oxidant injury. This is injury to the body’s tissue (in this case, to the walls of the air sacs in the lungs), which is caused or enhanced by oxygen changing into toxic forms. The toxic forms of oxygen that can cause tissue injury are called free oxygen radicals. So, oxygen that is necessary for life has the potential for causing harm if free oxygen radicals are formed. Antioxidants counteract this effect by either removing or chemically changing the toxic free oxygen radicals. An antioxidant is a chemical or substance that has this ability to scavenge or detoxify these forms of oxygen. Vitamin A and vitamin E are known to have antioxidant effects. Coenzyme Q is also an antioxidant. There is no study that proves that these antioxidants help prevent the progression of lung disease or result in other beneficial or helpful effects. Taken in recommended doses, they are safe (very high doses may cause problems), and they may have some benefit. Special combinations of antioxidants, other vitamins and minerals are available in health food stores but tend to be expensive and have no scientific research to support their widespread use at this time. If you choose to take antioxidants, we recommend the cheapest generic forms available, usually found in any drug store or supermarket.
Frequent, Small Meals
Because of the “war” between the big lungs pushing down and compressing the stomach and a large stomach distended with food or gas pushing up and compressing the lungs, eating frequent small meals (“grazing”) will be more comfortable and allow a greater daily food intake.
Diet and COPD
Food is the fuel for your breathing muscles. A diet composed of a variety of foods within each category is also necessary for maintenance and repair. Many people with COPD do not eat properly because they are short of breath while eating. A professional dietary plan will help immensely. Do not “burn” your breathing muscles for fuel! There are really very few “do not eat” items, and tasteful effective food supplements are available in case you simply cannot eat a nutritious diet. Discuss the possibility of a dietary consultation with your R.N. or physician.
Balanced nutrition is a part of good health. Nutritional needs are tied to other aspects of your health, including your lung problems. Discuss your nutritional concerns with your doctor, a dietician or a nutrition specialist. These specialists are available in most medical centers and medical communities. Try what makes sense to you. Natural foods and generic vitamins are generally as effective as more expensive alternatives. Try to find healthy foods which you also like. Follow the nutritional program that makes you feel the best. Eating should be a source of pleasure. Try to make eating one of your pleasures and not an ordeal.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 91
Reference Frontline Advice for COPD Patients, 2002. Thomas L. Petty, M.D. General Dietary Guidelines for Lung Cancer Patients 2007. Annette Davis, C.N., Jean-Claude Lapraz, M.D. Jean Bokelmann, M.D. Endobiogenic Integrative Medical Center. Fogarty A, Britton J. The role of diet in the etiology of asthma. Clin Exp Allergy. 2000;30:615–627. Tabak C, Smit HA, Heederik D, Ocké MC, Kromhout D. Diet and chronic obstructive pulmonary disease: independent beneficial effects of fruits, whole grains, and alcohol (the MORGEN study). Clin Exp Allergy. 2001;31:747–755.
92 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
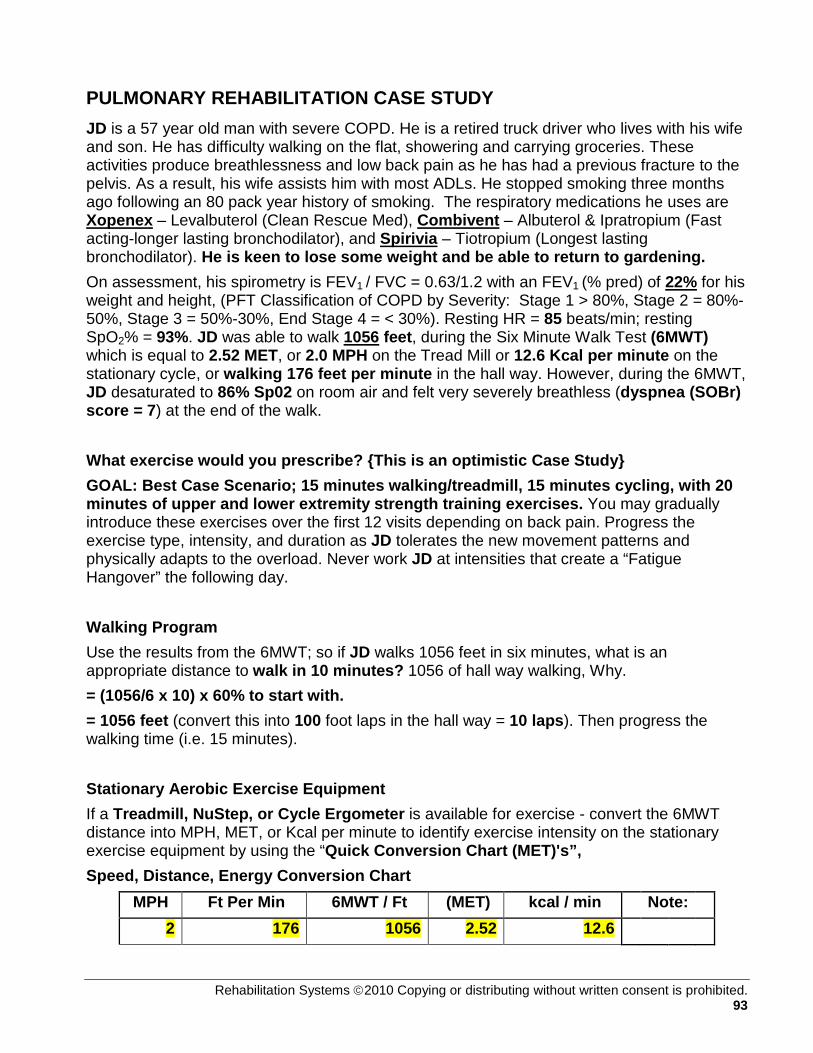
PULMONARY REHABILITATION CASE STUDY JD is a 57 year old man with severe COPD. He is a retired truck driver who lives with his wife and son. He has difficulty walking on the flat, showering and carrying groceries. These activities produce breathlessness and low back pain as he has had a previous fracture to the pelvis. As a result, his wife assists him with most ADLs. He stopped smoking three months ago following an 80 pack year history of smoking. The respiratory medications he uses are Xopenex – Levalbuterol (Clean Rescue Med), Combivent – Albuterol & Ipratropium (Fast acting-longer lasting bronchodilator), and Spirivia – Tiotropium (Longest lasting bronchodilator). He is keen to lose some weight and be able to return to gardening. On assessment, his spirometry is FEV1 / FVC = 0.63/1.2 with an FEV1 (% pred) of 22% for his weight and height, (PFT Classification of COPD by Severity: Stage 1 > 80%, Stage 2 = 80%-50%, Stage 3 = 50%-30%, End Stage 4 = < 30%). Resting HR = 85 beats/min; resting SpO2% = 93%. JD was able to walk 1056 feet, during the Six Minute Walk Test (6MWT) which is equal to 2.52 MET, or 2.0 MPH on the Tread Mill or 12.6 Kcal per minute on the stationary cycle, or walking 176 feet per minute in the hall way. However, during the 6MWT, JD desaturated to 86% Sp02 on room air and felt very severely breathless (dyspnea (SOBr) score = 7) at the end of the walk. What exercise would you prescribe? {This is an optimistic Case Study} GOAL: Best Case Scenario; 15 minutes walking/treadmill, 15 minutes cycling, with 20 minutes of upper and lower extremity strength training exercises. You may gradually introduce these exercises over the first 12 visits depending on back pain. Progress the exercise type, intensity, and duration as JD tolerates the new movement patterns and physically adapts to the overload. Never work JD at intensities that create a “Fatigue Hangover” the following day. Walking Program Use the results from the 6MWT; so if JD walks 1056 feet in six minutes, what is an appropriate distance to walk in 10 minutes? 1056 of hall way walking, Why. = (1056/6 x 10) x 60% to start with. = 1056 feet (convert this into 100 foot laps in the hall way = 10 laps). Then progress the walking time (i.e. 15 minutes). Stationary Aerobic Exercise Equipment If a Treadmill, NuStep, or Cycle Ergometer is available for exercise - convert the 6MWT distance into MPH, MET, or Kcal per minute to identify exercise intensity on the stationary exercise equipment by using the “Quick Conversion Chart (MET)'s”, Speed, Distance, Energy Conversion Chart
MPH Ft Per Min 6MWT / Ft (MET) kcal / min Note: 2 176 1056 2.52 12.6
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 93
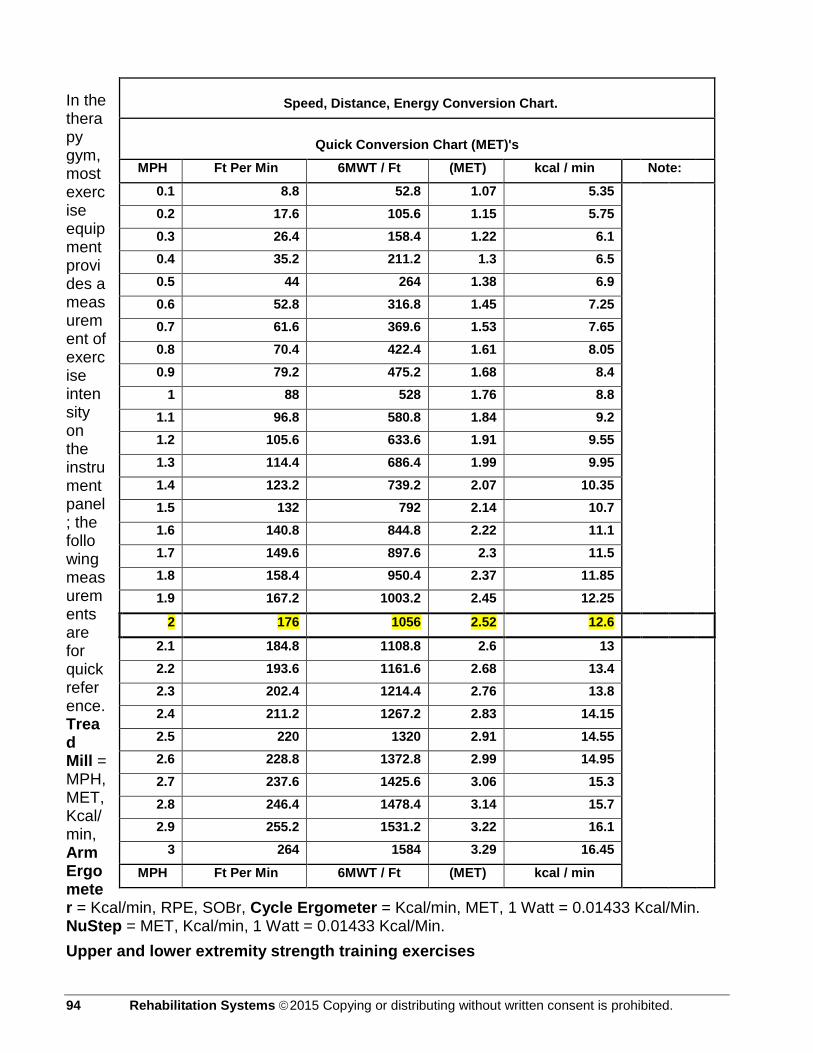
In the therapy gym, most exercise equipment provides a measurement of exercise intensity on the instrument panel; the following measurements are for quick reference. Tread Mill = MPH, MET, Kcal/min, Arm Ergometer = Kcal/min, RPE, SOBr, Cycle Ergometer = Kcal/min, MET, 1 Watt = 0.01433 Kcal/Min. NuStep = MET, Kcal/min, 1 Watt = 0.01433 Kcal/Min. Upper and lower extremity strength training exercises
Speed, Distance, Energy Conversion Chart.
Quick Conversion Chart (MET)'s
MPH Ft Per Min 6MWT / Ft (MET) kcal / min Note:
0.1 8.8 52.8 1.07 5.35 0.2 17.6 105.6 1.15 5.75 0.3 26.4 158.4 1.22 6.1 0.4 35.2 211.2 1.3 6.5 0.5 44 264 1.38 6.9 0.6 52.8 316.8 1.45 7.25 0.7 61.6 369.6 1.53 7.65 0.8 70.4 422.4 1.61 8.05 0.9 79.2 475.2 1.68 8.4
1 88 528 1.76 8.8 1.1 96.8 580.8 1.84 9.2 1.2 105.6 633.6 1.91 9.55 1.3 114.4 686.4 1.99 9.95 1.4 123.2 739.2 2.07 10.35 1.5 132 792 2.14 10.7 1.6 140.8 844.8 2.22 11.1 1.7 149.6 897.6 2.3 11.5 1.8 158.4 950.4 2.37 11.85 1.9 167.2 1003.2 2.45 12.25
2 176 1056 2.52 12.6
2.1 184.8 1108.8 2.6 13 2.2 193.6 1161.6 2.68 13.4 2.3 202.4 1214.4 2.76 13.8 2.4 211.2 1267.2 2.83 14.15 2.5 220 1320 2.91 14.55 2.6 228.8 1372.8 2.99 14.95 2.7 237.6 1425.6 3.06 15.3 2.8 246.4 1478.4 3.14 15.7 2.9 255.2 1531.2 3.22 16.1
3 264 1584 3.29 16.45
MPH Ft Per Min 6MWT / Ft (MET) kcal / min
94 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

After JD becomes accustom to the aerobic exercise of walking in the hall way, tread mill, or peddling the cycle egometer during the first two weeks or after the first 6 sessions, JD will be ready to start his strength training program. The key is to start low and go slow, avoiding fatigue hangovers. For the greatest overall strength gains, JD will participate in “five double joint movement patterns” for muscle group strength development. The five movement patterns are as follows:
Strength training progression is paced as tolerated by JD and the physical limitations of his lower back. JD starts strength training at one (1) Set of eight (8) Repetitions with a weight he can perform without shortness of breath while on 2 – 4 L/min of supplemental oxygen. Special attention is focused on JD’s range of motion with safe and proper form of movement before increasing sets and reps. Strength exercise progression seeks to achieve three (3) Sets of twelve (12) Repetitions before graduation from pulmonary rehabilitation.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 95

JD will benefit from performing these exercises with 2 – 4 liters per minute (L/min) of oxygen supplementation particularly if his breathlessness levels are elevated beyond 4 (somewhat severe) on the Borg scale. Remember to turn up the supplemental oxygen to keep JD’s oxygen saturation, as measured by the pulse oximeter, above 90% Sp02, which is JD’s blood oxygen saturation level. As a matter of contraindication, JD’s oxygen saturation must stay above 88% Sp02 during his therapeutic exercise sessions. The only time JD is allowed, in clinic, to drop his oxygen saturation drop below 88% Sp02 is during the 6MWT, because of the diagnostic need to measure functional capacity in relationship to oxygen usage, thus objectively identifying oxygen supplementation need. Pulse Oximeter A blood-oxygen monitor displays the percentage of arterial hemoglobin in the oxyhemoglobin configuration. Acceptable normal ranges are from 95 to 100 percent, although values down to 90% are common in patients without COPD. With the severity of JD’s COPD, you will need to pay close attention to his oxygen saturation as he will drop below 88% Sp02 with mild exertion.
96 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
The oxygen-haemoglobin dissociation curve, also spelled oxygen-hemoglobin dissociation curve, plots the proportion of hemoglobin in its saturated form on the vertical axis against the prevailing oxygen tension on the horizontal axis. The oxyhemoglobin dissociation curve is an important tool for understanding how our blood carries and releases oxygen. Specifically, the oxyhemoglobin dissociation curve relates oxygen saturation (SO2) and partial pressure of oxygen in the blood (PO2), and is determined by what is called "hemoglobin's affinity for oxygen"; that is, how readily hemoglobin acquires and releases oxygen molecules into the fluid that surrounds it Hemoglobin binds with carbon monoxide 240 times more readily than with oxygen. The presence of carbon monoxide on one of the 4 heme sites causes the oxygen on the other heme sites to bind with greater affinity. This makes it difficult for the hemoglobin to release the oxygen to the tissues and has the effect of shifting the curve to the left. With an increased level of carbon monoxide, a person can suffer from severe hypoxemia while displaying normal %SpO2.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 97
References Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2007;176:532-55. Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance — United States, 1971–2000. MMWR Surveill Summ 2002;51(SS-6):1-16. Babb TG, Viggiano R, Hurley B, Staats B, Rodarte JR. Effect of mild-to-moderate airflow limitation on exercise capacity. J Appl Physiol 1991;70:223-30. Decramer M, De Benedetto F, Del Ponte A, Marinari S. Systemic effects of COPD. Respir Med 2005;99:Suppl B:S3-S10. Skeletal muscle dysfunction in chronic obstructive pulmonary disease: a statement of the American Thoracic Society and European Respiratory Society. Am J Respir Crit Care Med 1999;159:S1-S40. Maltais F, LeBlanc P, Whittom F, et al. Oxidative enzyme activities of the vastus lateralis muscle and the functional status in patients with COPD. Thorax 2000;55: 848-53. Agustí AG, Sauleda J, Miralles C, et al. Skeletal muscle apoptosis and weight loss in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2002;166: 485-9. Casaburi R, Patessio A, Ioli F, Zanaboni S, Donner CF, Wasserman K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am Rev Respir Dis 1991;143:9-18. Pepin V, Saey D, Laviolette L, Maltais F. Exercise capacity in chronic obstructive pulmonary disease: mechanisms of limitation. COPD 2007;4:195-204. Wagner PD. Skeletal muscles in chronic obstructive pulmonary disease: deconditioning, or myopathy? Respirology 2006; 11:681-6. Casaburi R. Exercise training in chronic obstructive lung disease. In: Casaburi R, Petty TL, eds. Principles and practice of pulmonary rehabilitation. Philadelphia: W.B. Saunders, 1993:204-24. Nici L, Donner C, Wouters E, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med 2006;173:1390-413 Porszasz J, Emtner M, Goto S, Somfay A, Whipp BJ, Casaburi R. Exercise training decreases ventilatory requirements and exercise-induced hyperinflation at submaximal intensities in patients with COPD. Chest 2005;128:2025-34. Haas F, Salazar-Schicchi J, Axen K. Desensitization to dyspnea in chronic obstructive pulmonary disease. In: Casaburi R, Petty TL, eds. Principles and practice of pulmonary rehabilitation. Philadelphia: W.B. Saunders, 1993:241-51.
98 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

BREATHING RETRAINING Principle Chronic Obstructive Pulmonary Disease (COPD) is a disease characterized by a limitation of airflow. Airflow limitation occurs as a result of two processes: increased resistance and airway narrowing, wall thickening and fibrosis. Loss of driving pressure results from alveolar destruction (emphysema), causing less elastic decreased driving pressure. Increased resistance is due to airway inflammation leading to recoil of the lung. Decreased attachments to the airways from the alveoli also result in some distal airways undergoing dynamic collapse on exhalation. As lung reserve declines, dyspnea worsens and independent daily activity performance erodes. In the presence of pulmonary dysfunction, air becomes trapped in the lungs, pushing down on the diaphragm. The neck and chest muscles must then assume an increased share of the work of breathing. This significantly increases the consumption of oxygen and energy, and increases shortness of breath. Purpose It should not be assumed that people with chronic lung dysfunction have developed efficient breathing patterns. Encouraging proper breathing skills can greatly aid in minimizing the symptoms that lead to respiratory distress. Self administered breathing techniques can decrease respiratory symptoms and complications, encourage independence, improve physical conditioning and exercise performance, improve emotional well-being, and reduce hospitalizations. Any patient experiencing an alteration of breathing (See Visual Inspection) should be encouraged to utilize proper breathing techniques. The techniques of pursed-lip breathing and diaphragmatic breathing will enable the healthcare provider to assist the patient in controlling symptoms and increasing alveolar oxygenation and ventilation. Procedure
Diaphragmatic Breathing Diaphragmatic breathing improves the effort of respirations by utilizing the most efficient muscle of breathing. It is a large, dome-shaped muscle located at the base of the lungs. The abdominal muscles help move the diaphragm and give more power to empty the lungs. The diaphragm moves down as you breathe in, making the chest size larger so that air can flow into the lungs. With normal functioning lungs, the diaphragm moves upward and reduces the chest size so that air is pushed out of the lungs. COPD may prevent the diaphragm from working effectively. COPD increases the risk of air becoming trapped in the lungs, and pushing down on the diaphragm. The neck and chest muscles must then assume an increased share of the work of breathing. This significantly increases the consumption of oxygen and effort in breathing, which may result in shortness of breath and fatigue. Use of the diaphragm can be improved with proper training and frequent utilization of the technique. Making the patient aware of their current breathing pattern may be helpful in teaching or encouraging a new breathing pattern.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 99

To begin, position the patient on the back with knees bent, or sitting upright in a chair. Place one hand on the diaphragm and ask the patient to relax the abdominal muscles, and then inhale through their nose and feel the diaphragm push against your hand. When the patient is performing the technique properly have them place their own hand on the diaphragm to feel the movement. Utilizing the patient’s hand reinforces the technique of abdominal expansion upon inspiration. The hand on the chest should move very little or not at all. Pursed-lip Breathing Pursed-lip breathing is one of the simplest ways to control shortness of breath. It provides a quick and easy way to slow the pace of breathing, making each breath more effective. Pursing the lips on exhalation creates backpressure on the airways keeping them open. Keeping the airways open improves the removal of carbon dioxide and the inspiration or more oxygen. Patients who learn this technique will be able to catch their breath faster and easier and feel less short of breath. This technique should be used during the difficult part of any activity, such as bending, lifting or stair climbing. It should also be encouraged and monitored when a patient appears to be short of breath. The patient should tighten the abdominal muscles to move the diaphragm up and exhale slowly through the mouth while pursing the lips (like whistling). The air should move smoothly as if blowing a bubble or blowing out a candle. Rate of Inspiration/Expiration During inspiration and exhalation encourage the patient to relax the muscles in the chest and neck as much as possible. Using the accessory muscles to breathe increases anxiety, consumes oxygen at a faster rate, produces fatigue, and decreases the quantity of air inhaled. Controlling the rate of respirations will decrease the risk of respiratory distress. Encourage the patient to control the rate to a normal limit. A rate of 12-24 breaths per minute is acceptable. Greater than 24 breaths per minute is acceptable if the patient is exerting energy, and is maintaining a normal oxygen saturation and heart rate. The rate of inspiration versus expiration should be controlled to a rate of 1:2, or 2:4. To encourage this rate have the patient silently count, “one…two” during inspiration, and “one…two…three…four” during exhalation. Huff-coughing The inflammatory cascade resulting from chronic irritation causes a hyper-secretion of mucous. Other cellular changes and changes in the properties of lung surfactant also contribute to the increased production of mucous. Many patients with COPD have
100 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

developed ineffective coughing patterns that do not adequately clear airways of sputum. The goals of effective coughing are to conserve energy, reduce fatigue, and facilitate removal of secretions. Before initiating a cough, the patient should take a deep abdominal breath, bend slightly forward, and then huff cough. The patient may need to splint the thorax or abdomen to achieve a maximum cough. Assist the patient to assume a sitting position with head slightly flexed, shoulders relaxed, knees flexed, and forearms supported by pillow, and if possible, with feet on the floor. The patient then drops the head and bends forward while using slow, pursed-lip breathing to exhale. Sitting up again, the patient uses diaphragmatic breathing to inhale slowly and deeply. On the next exhalation the patient coughs three to four times. Encourage the patient to repeat these steps three to four times to facilitate mobilization of secretions.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 101

References Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: NHLBI/WHO Workshop Report. Rockville, Md: National Institutes of Health, National Heart, Lung, and Blood Institute; April 2001. NIH Publication No. 2701. Jones AY, Dean E, Chow CCS. Comparison of the oxygen cost of breathing exercises and spontaneous breathing in patients with stable chronic obstructive pulmonary disease. Phys Ther. 2003;83:424–431. Thompson WH, Carvalho P, Souza JP, Charan NB. Effect of expiratory resistive loading on the noninvasive tension-time index in COPD. J Appl Physiol. 2000;89:2007–2014. Hall, D.A., and Faughnan, M.E., (2005). COPD: Approaches to controlling disease and decreasing disability. Retrieved October 29, 2005, Lewis, S.M., Heitkemper, M.M., Dirksen, S.R., (2004), Medical Surgical Nursing, Mosby Co. Tips for Better Breathing, (n.d.). Retrieved October 29, 2005. Cahalin LP, Braga M, Matsuo Y, Hernandez ED. Efficacy of diaphragmatic breathing in persons with chronic obstructive pulmonary disease: a review of the literature. J Cardiopulm Rehabil. 2002;22:7–21.
102 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
CHEST PHYSICAL THERAPY Principle Chest physical therapy is the term for a group of treatments designed to promote expansion of the lungs, and eliminate secretions from the respiratory system. Depending on the circumstances, chest physical therapy may be performed by anyone from a physical therapist to an aid or even a trained member of the patient’s family. People who benefit from chest physical therapy exhibit a wide range of problems that make it difficult to clear secretions from their lungs. Some people who may receive chest physical therapy include people with, cystic fibrosis or neuromuscular diseases like Guillain-Barré syndrome, progressive muscle weakness (myasthenia gravis). People with lung diseases such as bronchitis, pneumonia, or chronic obstructive pulmonary disease (COPD) also benefit from chest physical therapy. People who are likely to aspirate because of diseases such as cerebral palsy or muscular dystrophy also receive chest physical therapy, as do some people who are bedridden, confined to a wheelchair, or who cannot breathe deeply because of postoperative pain. Purpose The purpose of chest physical therapy is to clear the lungs of mucus secretions. Chest physical therapy includes postural drainage, chest percussion, and chest vibration. It is usually done in conjunction with other treatments to mobilize secretions. These other treatments include: exercise, flutter devices, suctioning, nebulizer treatments, and the administration of expectorant drugs. Percussion and drainage uses force and gravity to assist in effectively draining secretions from the lungs and into the central airway where they can either be coughed up or suctioned out. Reasons to avoid chest physical therapy include:
• Acute asthma • Recent heart attack • Pulmonary embolism • Lung abscess • Active hemorrhage • Some spine injuries • Recent surgery • Open wounds, burns, or a tendency to bleed (taking Heparin or Coumadin). • Bleeding from the lungs • Neck or head injuries • Fractured ribs • Collapsed lungs • Damaged chest walls • Tuberculosis
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 103
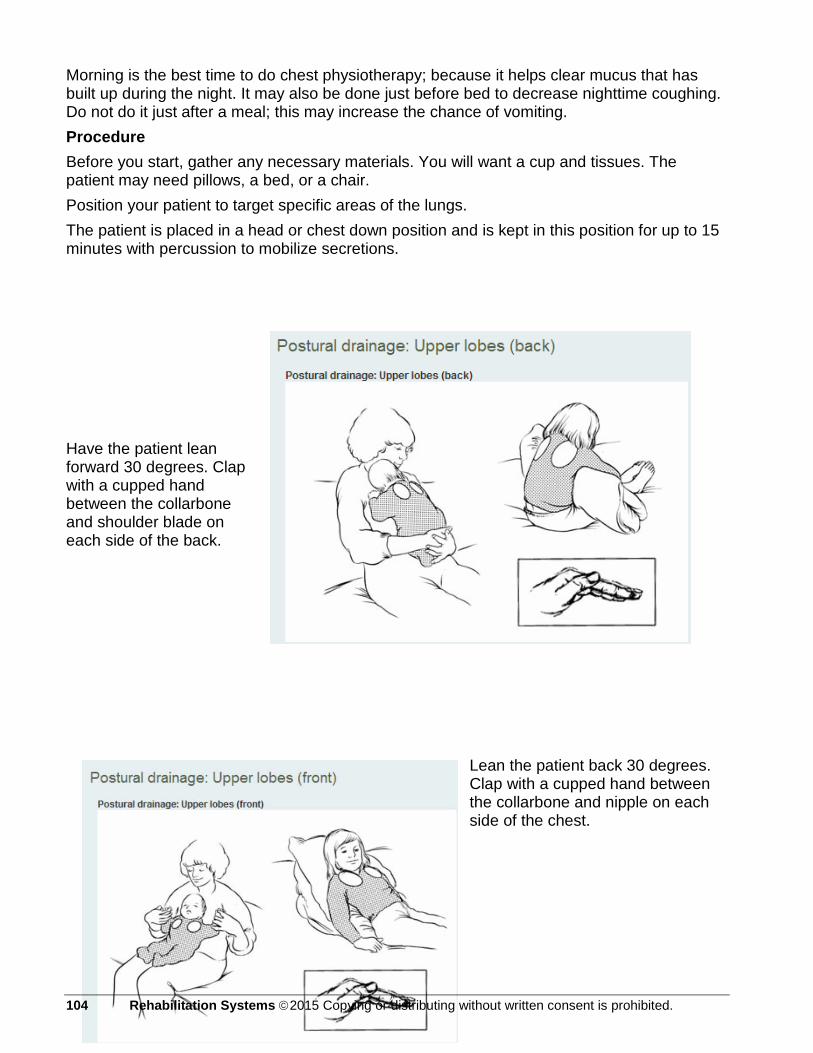
Morning is the best time to do chest physiotherapy; because it helps clear mucus that has built up during the night. It may also be done just before bed to decrease nighttime coughing. Do not do it just after a meal; this may increase the chance of vomiting. Procedure Before you start, gather any necessary materials. You will want a cup and tissues. The patient may need pillows, a bed, or a chair. Position your patient to target specific areas of the lungs. The patient is placed in a head or chest down position and is kept in this position for up to 15 minutes with percussion to mobilize secretions. Have the patient lean forward 30 degrees. Clap with a cupped hand between the collarbone and shoulder blade on each side of the back.
Lean the patient back 30 degrees. Clap with a cupped hand between the collarbone and nipple on each side of the chest.
104 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
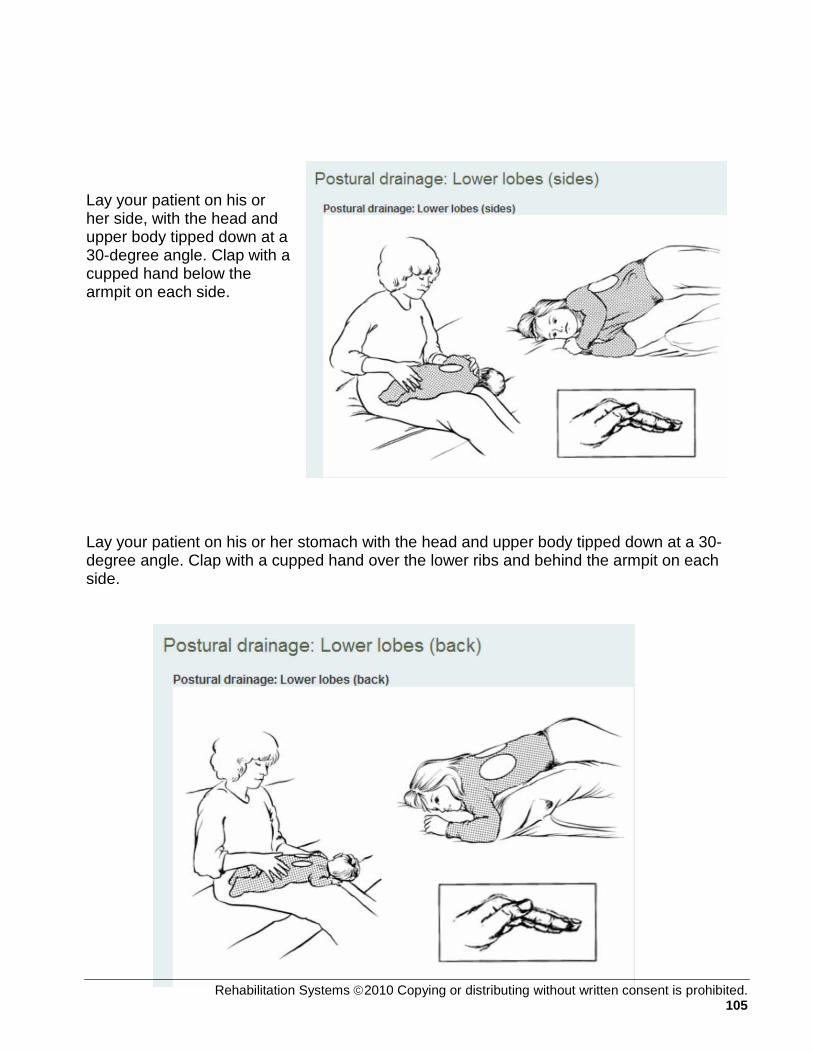
Lay your patient on his or her side, with the head and upper body tipped down at a 30-degree angle. Clap with a cupped hand below the armpit on each side. Lay your patient on his or her stomach with the head and upper body tipped down at a 30-degree angle. Clap with a cupped hand over the lower ribs and behind the armpit on each side.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 105

Clap your patients back or chest with a cupped hand quickly and rhythmically. This loosens the mucus, allowing it to drain. Bend your hand at the wrist and form a cup.
106 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
When you clap, you should hear a hollow sound. If you hear a slapping, your hand is not cupped enough. You may safely clap over the ribs, but do not clap over the kidneys, spine, or female breasts. Do not clap directly on the skin; always cover the area with thin clothing or a cloth. How much force to use while clapping, and how long you clap, depends on the patient. Consider the following:
Younger and smaller patients require less force and time than older and larger patients. Watch the patient for pain and discomfort. If you notice this, you may be using too much force.
Is mucus coming up? If not, you may need more force. After clapping, have your patient cough. Have the patient take a deep breath, and then breathe out forcefully while coughing to produce secretions.
References
1. Webb MSC, Martin JA, Cartlidge PHT, Ng YK, Wright NA. Chest physiotherapy in acute bronchiolitis. Archives of disease in childhood 1985:60(11);1078-9.
2. Nicholas KJ, Dhouieb MO, Marshall TG, et al. An evaluation of chest physiotherapy in the management of acute bronchiolitis: changing clinical practice Physiotherapy 1999;85:669-74
3. Bohe L, Ferrero ME, Cuestas E, Polliotto L, Genoff M. Indications of conventional chest physiotherapy in acute bronchiolitis. Medicina 2004;64(3):198-200.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 107

OXYGEN DELIVERY SYSTEMS Principle Long-term oxygen therapy is widely accepted as the standard treatment for chronic hypoxemia, a condition in which there is an inadequate supply of oxygen in the blood, caused by chronic obstructive pulmonary disease (COPD), and other disorders such as interstitial lung disease. Long-term oxygen therapy will reverse secondary polycythemia, increase body weight, alleviate right heart failure due to cor pulmonale, improve cardiac function, enhance neurophysiological function, improve skeletal-muscle metabolism, boost exercise performance, reduce dyspnea, and enable the patient to perform activities of daily living. These changes are known to promote a higher quality of life for the patient and family. Long-term oxygen therapy improves survival in hypoxemic patients with COPD. While the mechanisms of action responsible for these reductions in mortality are still unknown, it appears that pulmonary hemodynamics are involved. Chronic hypoxemia tends to increase pulmonary artery pressures, yet when the hypoxemia is reversed through oxygen administration, the pulmonary artery pressures lower toward normal levels. This reduction in the pressure load reduces cardiac work and improves oxygen delivery to the tissues. Simply correcting hypoxemia, however, may not prevent tissue hypoxia. Clinicians must be concerned about other physiologic systems’ impact on oxygen transport and delivery to metabolically active tissues. Accordingly, lung function should be optimized, infection should be controlled, and congestive heart failure should be treated. Further, hemoglobin deficiencies must be corrected and optimization of cardiac output must be ensured before oxygen transport by the circulatory system can be maximized. Some clinicians are unduly concerned that oxygen supplementation will lead to respiratory drive depression, or hypercapnia, an increased level of carbon dioxide in the blood, and respiratory acidosis. Consequently, these clinicians may prescribe oxygen inadequately. While carbon dioxide retention does occur, it is often caused by ventilation/perfusion mismatching rather than by respiratory center depression, and it rarely leads to respiratory acidosis. Thus, the therapeutic priority must always be the correction of hypoxemia. Purpose Three types of stationary sources supply supplemental oxygen for Assisted Living Facilities (ALF) / Skilled Nursing Facilities (SNF) and home use: oxygen concentrators, compressed gas cylinders, and liquid oxygen reservoirs. Portable oxygen systems are available for patients who desire to remain ambulatory (and as backup in the event of primary source failure). Over the past three decades, technological advances have refined source and delivery systems. Large cylinders for home use now have been replaced by oxygen concentrators or liquid systems. Portable systems have undergone a transformation from continuous-flow systems that waste oxygen to storage reservoir cannulae and pneumatic or electronic pulsing devices. Steel E cylinders are being replaced by lighter aluminum or composite cylinders. Because portable storage devices can be coupled with oxygen-conserving technologies, the storage reservoir size can be reduced.
108 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Oxygen-Storage Devices The E cylinder is perhaps the most widely distributed and best known. It is routinely used as a backup system for concentrators and liquid oxygen in the event of a system failure. At a flow rate of 2 L/min, the E cylinder will last for about 5.5 hours. This time can be extended, however, through the use of oxygen-conserving technologies. The E cylinder as a primary stationary oxygen source is not practical due to its low storage capacity and overall cost. Oxygen concentrators extract oxygen from room air using a molecular sieve. Concentrators are preferred by the Home Medical Equipment (HME) community for their convenience, low cost, and long interval between service calls. Design innovations and use of new space-age materials have improved concentrator power consumption, minimized noise and heat buildup, enhanced safety and efficiency of operation, and lowered overall costs. Some users still find them noisy, however, and they do add to the patient’s monthly electricity costs. For those in remote areas where electricity provision is unreliable, a concentrator may not be the best choice. Most concentrators produce sufficient flows to cover the typical oxygen prescription of 2 to 3 L/min. For patients who require flow rates of more than 5 L/min, there are specialized concentrators that can deliver up to 10 L/min. Liquid systems have been around for many years and are the most efficient means for storing oxygen. When liquid oxygen is used, 1 L can provide 860 L of oxygen gas, supplying enough oxygen to last 5 days for patients requiring flows of 2 L/min. Liquid oxygen is easily transfilled from stationary reservoirs to portable containers, making it ideal for the ambulatory patient. Recently, liquid modules have incorporated a conserving device, thus creating a highly portable, lightweight system. The disadvantages of liquid oxygen include its higher cost, the tendency of liquid oxygen to evaporate when not being used, and the rare incidence of freezing injuries. Patients must live within the delivery range of the oxygen supplier. For rural patients living outside that radius, the cost of delivery may be prohibitive. Oxygen-Delivery Devices Oxygen is usually administered in one of three ways: using a nasal canula, a transtracheal catheter, or an electronic demand device. There are more than 800,000 patients now receiving long-term oxygen supplementation in the United States. Nasal Cannula Most people receive their oxygen via standard nasal cannula. Although simple and inexpensive, the standard nasal cannula is an inefficient delivery system. The wastefulness of the system is derived from the physiology of respiration. During a normal respiratory cycle, about one fourth to one third of the time is spent in inhalation; the rest of the cycle is exhalation. Because the standard cannula delivers oxygen throughout the entire respiratory cycle, much of that oxygen is wasted. In addition, the last half of inhalation does not reach the alveoli; consequently, up to five sixths of continuously flowing oxygen is lost to the atmosphere. This physiological realization, coupled with economic forces and the need for smaller and lighter systems, has led to the development of conserver technologies.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 109

Reservoir cannulae work by storing oxygen in small reservoirs during exhalation and then releasing that stored oxygen at the beginning of the next inhalation. Two variations of the reservoir cannula are available; one stores oxygen in a reservoir below the nose and one uses a small reservoir at chest level. These cannulae have reduced the use of oxygen by 50% to 75%, compared with standard nasal cannulae, while maintaining the patient’s oxygen saturation at comparable values. They may not be as efficient for mouth breathers, and some individuals find their appearance objectionable. In the event of reservoir failure, the patient can simply use the cannula as a standard flow cannula until it can be replaced. Transtracheal oxygen (TTO) devices, first introduced by Heimlich, deliver oxygen directly through a small catheter inserted into the trachea. Placement of the catheter requires a skilled, experienced physician, good patient selection, and comprehensive support from a nurse and RT. Education is the key to success: patients must learn to clean, maintain, and care for the catheter and stoma. Because of these requirements, the relative number of patients receiving transtracheal oxygen therapy tends to be limited, unfortunately. Transtracheal catheters are more efficient when used in conjunction with a demand-flow device. Transtracheal delivery is known to improve adherence to therapy while conserving oxygen. Patients receiving transtracheal oxygen have improved exercise tolerance, and it has been used with success in patients who have refractory hypoxemia. Continuous Positive Airflow Pressure (CPAP) A system called continuous positive airflow pressure (CPAP) employs a machine weighing about five pounds that fits on a bedside table and supplies a steady stream of air through a tube that connects to a plastic mask. The machine applies sufficient air pressure to prevent the airway tissues from collapsing during sleep. It is not an oxygen-delivery system, but it improves airflow into the lungs and may help reduce hospitalization, particularly when combined with long-term oxygen therapy.
110 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

References Continuous or nocturnal oxygen therapy in hypoxemix chronic obstructive lung disease: A clinical trial, nocturnal oxygen therapy trial group. (1980) Ann Internal Med; 93, 391-398. Eaton, T., Garrett, J.E., and Young, P., (2002). Ambulatory oxygen improves quality of life of COPD patients: A randomized controlled trial. Eur Respir J, 20, 306-322. Report of Medical Research Council Working Party. Long term domiciliary oxygen therapy in chronic cor pulmonale complicating chronic bronchitis and emphysema. (1981) Lancet, 1,681-685. Tiep B., (Editor), Carter, R., (1991).The Physiologic Principles of Oxygen Delivery. Portable Oxygen Therapy: Including Oxygen Conserving Methodology. Mount Kisco,NY: Futura Publishing Company, 81-124. Timms, R.M., Farreed, U.K., and George, A.W., (1985). Hemodynamic response to oxygen therapy in chronic obstructive pulmonary disease. Ann Internal Med 102, 29-36. Weitzenblum, E., Sautegeau, A., Ehrhart, M. et al., (1985). Long-term oxygen therapy can reverse the progression of pulmonary hypertension in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis, 131, 493-498. Zielinski, J., (1999). Effects of long-term oxygen therapy in patients with chronic obstructive pulmonary disease. Curr Opin Pulm Med, 5, 81-87.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 111

COPD MEDICATIONS Principle Patients with COPD receive an array of medications for various symptoms. Dosage and types of medications may be adjusted depending upon the patients’ response to the medication. Expected outcomes and side-effects should be understood prior to administering any medication. The type and dose of medications may change with the season, location changes or other factors. Medications will also vary with triggers such as viral infections, allergens, pollution, cold air, and exercise. For most people with COPD, it takes from several weeks to several months to develop a treatment plan that leads to acceptable symptom control. Observing and reporting response to medications increases the ability to determine effective symptom control. Purpose There are six typical medication types used to treat symptoms of COPD; they are not expected to cure the disease. Types and dosages may require adjustment to maintain or improve symptom control. Accurate documentation and reporting of poor affect, or adverse side-effects will enable physicians to prescribe medications according to the patients’ condition and needs. Medications are presented in categories with expected outcomes and examples. See the quick reference chart attached to the procedure for possible side effects. Bronchodilators
Bronchodilators help reduce the effort of breathing, and are often the first choice for therapy. They dilate the airways to relieve or reduce shortness of breath and wheezing. The three main groups of bronchodilators are:
Beta2-agonists Beta2-agonists work to relieve breathlessness. Short-acting beta2-agonists are often used as a "rescue" medication to open airways quickly, but they can also be taken on a regular basis. If many inhalations of a short-acting bronchodilator are required to relieve symptoms, the addition of a long-acting beta2-agonist should be considered. They come in two varieties: short- and long-acting. Examples of short-acting beta2-agonists are:
(1) Ventolin® and Airomir® (salbutamol); (2) Bricanyl® (terbutaline); (3) Berotec® (fenoterol).
Examples of long-acting beta2-agonists are:
(1) Serevent® (salmeterol); (2) Oxeze® & Foradil® (formoterol).
112 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Anticholinergics Anticholinergics also work to relieve shortness of breath. Anticholinergics seem to be effective in treating COPD–if they are taken on a regular basis. A short-acting beta2-agonist and an anticholinergic can be combined in a single inhaler. For some COPD sufferers, this combination can provide better relief of breathlessness than if the drugs are used separately. For others, the effect is the same, but the combination medication is more convenient. They can be used both regularly and on an "as needed" basis.
Examples of anticholinergics are:
1. Atrovent® (ipratropium) 2. The longest-acting anticholinergic bronchodilator called tiotropium (Spiriva®) has a half-life of 36 hours. It is administered only once daily.
An example of a short-acting beta2-agonist and anticholinergic combination is: (1) Combivent® (salbutamol and ipratropium)
Xanthines
Xanthines are tablets that may help relieve breathlessness. Depending on the person, xanthines can also improve the function of breathing muscles and perhaps reduce inflammation resulting from COPD. These medications can have a relatively high likelihood of causing side effects, such as nausea and heartburn, and can also interact with food and other drugs. Patients may need education regarding the purpose of this important medication and its effects on reducing inflammation. This medication is used on a short-term basis. Nursing interventions can be used to reduce the side effects of nausea and heartburn. Examples of xanthines are:
1. theophylline; 2. Uniphyl®; 3. Theo-Dur®.
Anti-Inflammatory
Anti-inflammatory medications are corticosteroids, usually taken in an inhaled form. They are used to reduce cough and inflammation of the airways. Although they work best for treating asthma, they may be helpful for a small number of COPD sufferers, especially those with the most advanced disease. The main benefit of inhaled corticosteroids seems to be a reduction in the number of COPD flare-ups. Corticosteroids in tablet form (e.g. prednisone) are often used for a few days to help treat COPD flare-ups. Examples of inhaled corticosteroids are:
1. Flovent® (fluticasone); 2. Pulmicort® (budesonide); 3. Qvar® (beclomethasone).
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 109

Some medications combine anti-inflammatories with long-acting beta2-agonists to reduce inflammation, relieve breathlessness and decrease the number of COPD flare-ups. Two such combinations are:
1. Advair® (fluticasone and salmeterol); 2. Symbicort® (budesonide and formoterol).
Antibiotics
Patients with COPD or other respiratory diseases pose a high risk of respiratory infections. Physicians should be notified at the first sign of infection. See Visual Inspection-Character of Cough. Antibiotics are used to treat COPD flare-ups caused by bacterial infections of the airways. Different antibiotics kill different types of bacteria. Although COPD flare-ups can also be frequently caused by viral infections, antibiotics are not helpful against viruses. Examples of antibiotics are:
1. Amoxil®; 2. Avelox®; 3. Biaxin®; 4. Ceclor®;
5. Ceftin®; 6. Cipro®; 7. Clavulin®; 8. Levaquin®;
9. Septra®; 10. Tequin®; 11. Zithromax®.
Vaccines for Flu & Pneumonia
Vaccines can help protect patients against specific strains of flu and pneumonia. Both types of vaccine can be effective in reducing the likelihood of a COPD flare-up. "Flu shots" are given annually; the pneumonia vaccine is usually given only once (although some people may require revaccination). Medical personnel should be vaccinated every year to reduce the risk of vector-borne influenza viruses that can be passed to patients.
Supplemental Oxygen
Lung damage as a result of COPD may make it difficult to get enough oxygen from natural air into the bloodstream. Low blood oxygen levels can cause shortness of breath, a change in mentation, fatigue, irritability, and increased perception of pain. If the blood oxygen level is low, oxygen therapy can help lessen breathlessness and other associated symptoms, and it improves the patients’ ability to participate in therapy, thus increasing functional capacity. See Oxygen Delivery Devices.
Expectorant Expectorants enhance the flow of respiratory tract secretions. The enhanced flow of less viscid secretions lubricates irritated respiratory tract membranes, promotes cilliary action and facilitates the removal of inspissated mucus. As a result, sinus and bronchial drainage is improved and nonproductive coughs become more productive and less frequent. Examples or expectorants are:
1. Guaifenex LA, 2. Humibid, 3. Humibid LA, 4. Giatuss
110 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

References General Medications Guidelines, (2004). Retrieved October 12, 2005, from http://www.cchs.net/health/health-info/docs\2400\246.asp?index=8698. Medications for chronic obstructive pulmonary disease, (2004). http://www.cchs.net What you need to do, (n.d.). Your medications. The American Lung Association. http://www.lung.ca Tussend Expectorants, (1998). Distributed by: Monarch Pharmaceuticals. Manufactured by: King Pharmaceuticals. Retrieved October 14, 2005, from www.kingpharm.com/uploads/ pdf_inserts/Tussend_Expectorant_PI.pdf National Heart, Lung, and Blood Institute: 2007 NHLBI Morbidity and Mortality Chartbook. Available at http://www.nhlbi.nih.gov/resources/docs/cht-book.htm (accessed Deceember 27, 2009).
American Thoracic Society/European Respiratory Society Task Force: Standards for the diagnosis and management of patients with COPD; Version 1.2. New York, American Thoracic Society, 2008. PDF available for download at http://www.thoracic.org/sections/copd/ (accessed December 27, 2009).
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 111

PULMONARY REHABILITATION GOALS-BUILDING BLOCKS FOR WRITING FUNCTIONAL GOALS 1. pt will be independent with pursed lip breathing to prevent anxiety attacks while maintaining blood oxygen saturations above 90 % Sp02 2. pt will be independent ambulation 400 feet in order to take the trash out. 3. pt will increase LE Strength from 3/5 to 4/5 to stand up from commode. 4. pt will increase UE strength from 2/5 to 3/5 in order to reach shower head for adjustment. 5. pt will increase ambulation from 200 feet to 400 feet to increase pt’s walking capability to reach the garage. 6. pt shall strengthen LE from 2/5 to 4/5 from a seated to standing position that results in pt’s ability to navigate stairs in home. 7. pt seeks LE & UE strength increase from 1/5 to 3/5 to pick up laundry basket and set it on table. 8. pt seeks UE strength increase from 1/5 to 2/5 to enable hair dressing, an over the head strength requirement. 9. pt seeks an ambulation functional increase from 200 feet to 500 feet that produces the capacity to use public transportation for grocery shipping. 10. pt shall increase walking and standing capacity from 1.5 MET to 3.0 MET in order to clean kitchen and cook meals. 11. pt shall seek UE & LE strength and balance gains from 3/5 to 4+/5 to safely walk to and operate the riding snow blower. 12. pt shall increase function from 1.5 MET to 2.0 MET to restore self care tasks of toileting, bathing, & dressing. 13. pt will increase abdominal strength from 1/5 to 3/5 to support abdominal breathing patterns for increased control of shortness of breath and oxygenation. 14. pt seeks balance increases lost to corticosteroid-induced muscle wasting to reduce falls risk and to safely navigate stairs. 15. pt seeks strength gains lost to corticosteroid-induced muscle wasting to reduce falls risk and stand up from chairs. 16. pt shall gain UE ROM over head from 20 degrees to 30 degrees to reach food items from upper shelves. 17. pt shall obtain UE & LE strength gains from 1/5 to 3/5 to reduce falls & osteoporosis fractures resulting from corticosteroid-induced bone mineral wasting. 18. pt shall increase functional capacity from 1.5 MET to 3.3 MET in order to mop kitchen Flores. 19. pt seeks a functional increase from 2.0 MET to 3.5 MET which will enable the bathing of his dog. 20. pt seeks a functional increase from 2.0 MET to 3.8 MET which will enable him to scrub the bathtub, his most difficult home chore. 112 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

COMMON (MET) TO FUNCTIONAL TASK CONVERSIONS (SHORT LIST) 3.0; home activities; cleaning, wash car, wash windows, clean garage 3.5; home activities; mopping 3.0; home activities; cleaning, house or cabin, genera 3.5; home activities; vacuuming 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing - packing/unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; lawn and garden; riding snow blower 2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; music playing; conducting 2.5; music playing; piano or organ 2.5; music playing; violin 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside 2.0; home activities; standing-light (pump gas, change light bulb, etc.)
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 113

Writing Functional Goals in Objective, Measurable, and Functional Terms Purpose Physical and Occupational Therapists are required to document patient outcomes on the Department of Health and Human Services Plan of Treatment, 700 & 701, etc. Human physiological outcomes at rest and during activity are well known, translating measurements (MET) allows therapists to apply scientific principles to the assessment of everyday functional capacity. The validity of metabolic equivalents (MET) and it’s relationship to functional capacity or physical activity is central to the Compendium of Physical Activities Tracking Guide. The compendium was developed for use in epidemiologic studies to standardize the assignment of MET intensities in physical activity. The compendium has been used in studies worldwide to assign intensity units MET to physical activity, and to develop innovative ways to assess energy expenditure in physical activity. Principle Functional capacity and the writing of functional goals must relate to activities of daily living for rehabilitation outcome relevance. Goal setting must be a partnership, where the therapist and the patient work together to establish functional short term and outcome goals. Goal setting takes place during the initial evaluation and is documented on the 700/701.
Each therapist needs to identify how they will reach the patients goals in measurable, objective, and functional terms.
Ask yourself, are the goals measurable? Objective? Or functional?
With goals established, the therapist may refer to the: The Compendium of Physical Activities Tracking Guide. Look up the functional goal and record the MET work load required to perform the goal. For example:
“pt will care for home chores such as take the trash out, fix meals, and vacuum floors w/o assistance”
114 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Sample goals from The Compendium of Physical Activities Tracking Guide MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen, taking out trash 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; non-food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside 3.5; home activities; vacuuming
Achieving the desired goals requires a functional capacity of 3.5 MET. However, the patient at the time of evaluation or start of the program demonstrated a functional capacity of 2.0 MET. Therefore, therapists must define the incremental pathway /methods which will progress the patient to the desired functional goals. This is the plan of care (poc), exercise prescription (ep) or plan of treatment (pot). This methodology is documented in the Tx Justification on the 700/710.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 115
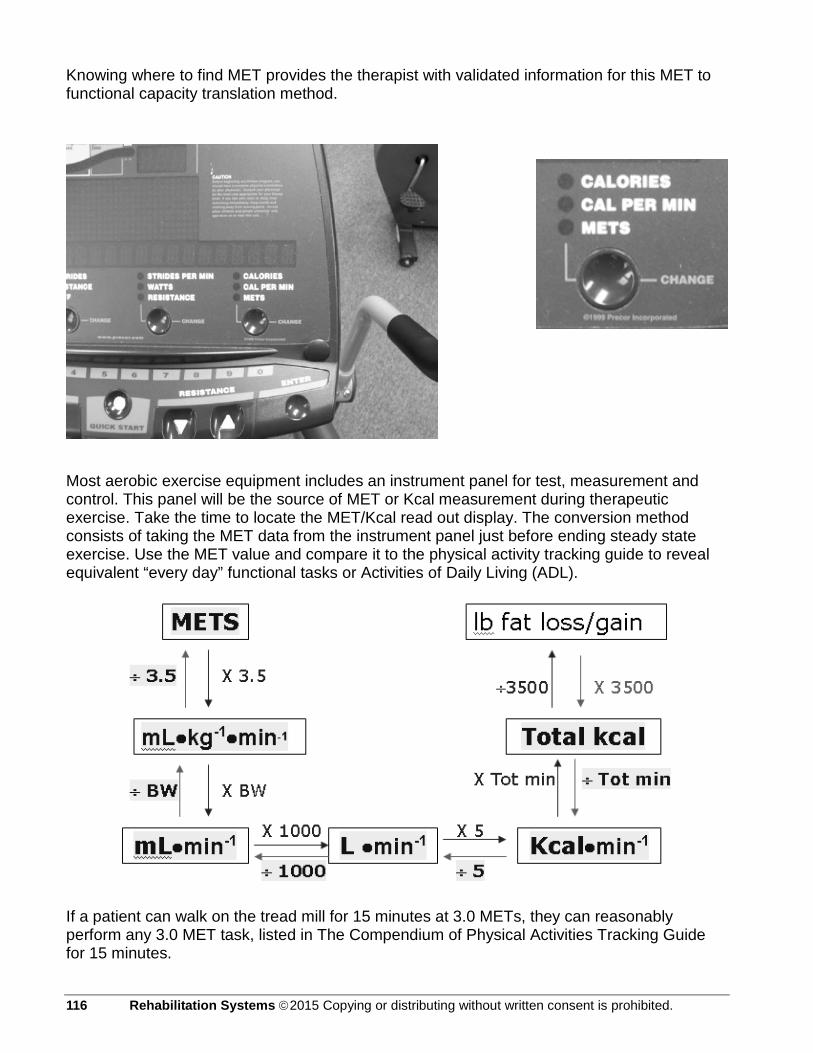
Knowing where to find MET provides the therapist with validated information for this MET to functional capacity translation method.
Most aerobic exercise equipment includes an instrument panel for test, measurement and control. This panel will be the source of MET or Kcal measurement during therapeutic exercise. Take the time to locate the MET/Kcal read out display. The conversion method consists of taking the MET data from the instrument panel just before ending steady state exercise. Use the MET value and compare it to the physical activity tracking guide to reveal equivalent “every day” functional tasks or Activities of Daily Living (ADL).
If a patient can walk on the tread mill for 15 minutes at 3.0 METs, they can reasonably perform any 3.0 MET task, listed in The Compendium of Physical Activities Tracking Guide for 15 minutes.
116 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 117
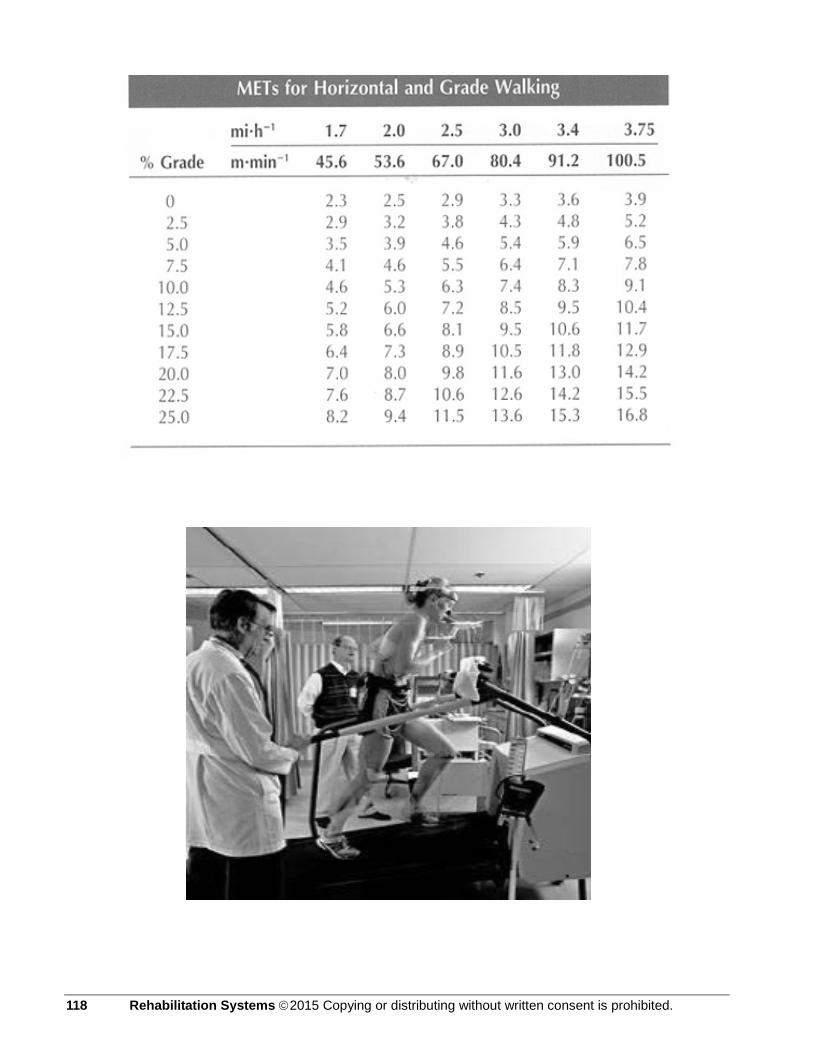
118 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

THE COMPENDIUM OF PHYSICAL ACTIVITIES TRACKING GUIDE (LONG LIST)
Met Level / Category / Functional Task Equivalent 1 to 2 MET LEVEL 0.9; inactivity; quiet sleeping 1.5; home activities; reclining with baby 1.0; inactivity; lying quietly, watching television 1.0; inactivity; lying quietly, doing nothing, lying in bed awake 1.0; inactivity; sitting quietly and watching television 1.0; inactivity; sitting quietly, sitting smoking, listening to music 1.2; inactivity; standing quietly (standing in a line) 1.0; inactivity; reclining in a chair - talking or talking on phone 1.0; inactivity; reclining in a chair – reading 1.0; inactivity; meditating 1.5; lawn and garden; watering lawn or garden, standing or walking 1.5; miscellaneous; sitting - card playing, playing board games 1.8; miscellaneous; sitting - writing, desk work, typing 1.8; miscellaneous; standing - talking or talking on the phone 1.5; miscellaneous; sitting - talking or talking on the phone 1.8; miscellaneous; sitting - studying, general, including reading - writing 1.8; miscellaneous; sitting - class, note-taking or class discussion 1.8; miscellaneous; standing – reading new paper waiting for bus 1.5; miscellaneous; sitting - arts and crafts, light effort 1.8; miscellaneous; standing - arts and crafts, light effort 1.5; miscellaneous; family reunion, genealogy, sitting, talking, eating 1.8; music playing; accordion 1.5; occupation; farming, milking by machine, light effort 1.3; occupation; police, riding in a squad car (sitting) 1.5; occupation; sitting - light office work, general 1.5; occupation; sitting meetings, general, and/or with talking involved 1.5; occupation; typing, electric, manual or computer 1.0; self care; sitting on toilet 1.5; self care; bathing (sitting) 1.5; self care; eating (sitting) 1.0; self care; taking medication, sitting or standing
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 119

MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 1.0; self care; having hair or nails done by someone else, sitting 1.5; sexual activity; active, vigorous effort 1.3; sexual activity; general, moderate effort 1.0; sexual activity; passive, light effort, kissing, hugging 1.0; transportation; riding in a car or truck 1.0; transportation; riding in a bus 1.0; religious activities; sitting in church, attending a ceremony 1.5; religious activities; sitting in church, talking or singing 1.3; religious activities; sitting, reading religious materials at home 1.2; religious activities; standing in church (quietly), standing quietly 1.0; religious activities; kneeling in church/at home (praying) 1.8; religious activities; standing, talking in church 1.5; religious activities; eating at church 1.5; religious activities; typing, electric, manual, or computer 1.5; volunteer activities; sitting - meeting, general 1.5; volunteer activities; sitting - light office work, in general 1.5; volunteer activities; typing, electric, manual, or computer 2 to 3 MET LEVEL 2.5; conditioning exercise; stretching, hatha yoga 2.5; conditioning exercise; mild stretching 2.5; fishing and hunting; fishing from boat, sitting 2.0; fishing and hunting; fishing, ice, sitting 2.5; fishing and hunting; hunting, bow and arrow or crossbow 2.5; fishing and hunting; hunting, duck, wading 2.5; fishing and hunting; pistol shooting or trap shooting, standing 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen, taking out trash 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking
120 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
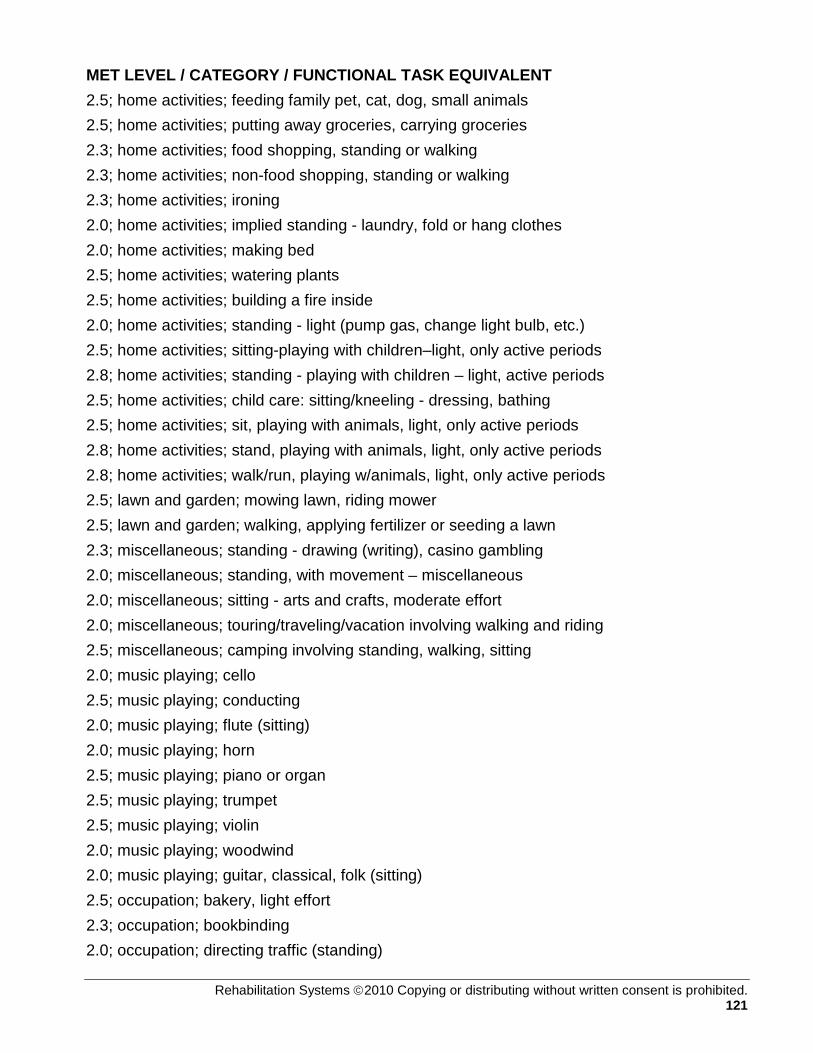
MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; non-food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside 2.0; home activities; standing - light (pump gas, change light bulb, etc.) 2.5; home activities; sitting-playing with children–light, only active periods 2.8; home activities; standing - playing with children – light, active periods 2.5; home activities; child care: sitting/kneeling - dressing, bathing 2.5; home activities; sit, playing with animals, light, only active periods 2.8; home activities; stand, playing with animals, light, only active periods 2.8; home activities; walk/run, playing w/animals, light, only active periods 2.5; lawn and garden; mowing lawn, riding mower 2.5; lawn and garden; walking, applying fertilizer or seeding a lawn 2.3; miscellaneous; standing - drawing (writing), casino gambling 2.0; miscellaneous; standing, with movement – miscellaneous 2.0; miscellaneous; sitting - arts and crafts, moderate effort 2.0; miscellaneous; touring/traveling/vacation involving walking and riding 2.5; miscellaneous; camping involving standing, walking, sitting 2.0; music playing; cello 2.5; music playing; conducting 2.0; music playing; flute (sitting) 2.0; music playing; horn 2.5; music playing; piano or organ 2.5; music playing; trumpet 2.5; music playing; violin 2.0; music playing; woodwind 2.0; music playing; guitar, classical, folk (sitting) 2.5; occupation; bakery, light effort 2.3; occupation; bookbinding 2.0; occupation; directing traffic (standing)
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 121
MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 2.5; occupation; chambermaid, making bed (nursing) 2.5; occupation; custodial work - cleaning sink and toilet, light effort 2.5; occupation; custodial work - dusting, light effort 2.5; occupation; custodial work - vacuuming, light effort 2.0; occupation; farming, moving animals, driving, light effort 2.5; occupation; farming, driving harvester, cutting hay, open irrigation 2.5; occupation; farming, driving tractor 2.6; occupation; horse racing, walking speed 2.3; occupation; printing (standing) 2.5; occupation; police, directing traffic, shouting commands (standing) 2.0; occupation; police, driving a squad car (sitting) 2.5; occupation; shoe repair, general 2.5; occupation; sitting; moderate (riding mower/forklift, crane operation) 2.5; occupation; tailoring, cutting 2.5; occupation; tailoring, general 2.0; occupation; tailoring, hand sewing 2.5; occupation; tailoring, machine sewing 2.0; occupation; walking on job, less than 2.0 mph, very slow 2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; sports; billiards 2.5; sports; croquet 2.5; sports; darts, wall or lawn 2.5; sports; football or baseball, playing catch 2.5; sports; horseback riding, walking 2.0; transportation; automobile or light truck (not a semi) driving 2.0; transportation; flying airplane 2.5; transportation; motor scooter, motorcycle 2.5; walking; bird watching 2.5; walking; pushing or pulling stroller with child or walking with children 2.0; walking; household walking from room to room
122 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 2.0; walking; walking, less than 2.0 mph, level ground, strolling, very slow 2.5; walking; walking, 2.0 mph, level, slow pace, firm surface 2.5; walking; walking from house to car or bus, from car or bus to go places 2.5; walking; walking to neighbor’s house to socialize, visit, or teach 2.8; walking; walking, 2.5 mph, downhill 2.5; water activities; boating, power 2.5; religious activities; sitting, playing an instrument at church 2.0; religious activities; standing, singing in church, active participation 2.0; religious activities; walk/stand to usher for religious purposes 2.5; religious activities; serving food at church 2.0; religious activities; preparing food at church 2.3; religious activities; washing dishes/cleaning kitchen at church 2.5; religious activities; standing - moderate (lifting 50 lbs) 2.5; volunteer activities; sitting - moderate work 2.3; volunteer activities; standing - light work (filing, talking, assembling) 3 to 4 MET LEVEL 3.0; conditioning exercise; bicycling, stationary, 50 watts, very light effort 3.5; conditioning exercise; calisthenics, home exercise, general 3.5; conditioning exercise; rowing, stationary, 50 watts, light effort 3.0; conditioning exercise; weight lifting 3.0; dancing; ballroom, slow (e.g. waltz, foxtrot, slow dancing) 3.0; fishing and hunting; fishing, general 3.5; fishing and hunting; fishing from river bank, standing 3.3; home activities; carpet sweeping, sweeping floors 3.0; home activities; cleaning, wash car, wash windows, clean garage 3.5; home activities; mopping 3.0; home activities; cleaning, house or cabin, genera 3.5; home activities; vacuuming 3.0; home activities; cooking Indian bread on an outside stove 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing - packing/unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 123
MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 3.0; home activities; carrying small children 3.0; home activities; child care: standing - dressing, bathing, grooming 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; home repair; wiring, plumbing 3.0; lawn and garden; riding snow blower 3.5; lawn and garden; trimming shrubs or trees, power cutter 3.0; lawn and garden; picking fruit off trees, picking fruits/vegetables 3.0; lawn and garden; walking/standing - picking up yard, light 3.0; lawn and garden; walking, gathering gardening tools 3.0; miscellaneous; standing - arts and crafts, moderate effort 3.5; miscellaneous; standing - arts and crafts, vigorous effort 3.5; music playing; trombone 3.0; music playing; guitar, rock and roll band (standing) 3.5; music playing; marching band, drum major (walking) 3.5; occupation; carpentry, general 3.0; occupation; custodial work - buffing the floor with electric buffer 3.5; occupation; custodial work - general cleaning, moderate effort 3.5; occupation; custodial work - mopping, moderate effort 3.0; occupation; custodial work - take out trash, moderate effort 3.0; occupation; custodial work - vacuuming, moderate effort 3.5; occupation; electrical work, plumbing work 3.5; occupation; farming, chasing cattle, non-strenuous (walking) 3.0; occupation; farming, milking by hand, moderate effort 3.5; occupation; locksmith 3.0; occupation; machine tooling, welding 3.0; occupation; standing; light/moderate, assemble/repair heavy parts 3.5; occupation; standing; moderate, assembling at fast rate, lifting 50 lbs 3.5; occupation; tailoring, weaving 3.3; occupation; walking on job, 3.0 mph, in office, moderate speed 3.8; occupation; walking on job, 3.5 mph, in office, brisk speed 3.0; occupation; walking, 2.5 mph, slowly and carrying 25 pounds
124 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 3.0; occupation; walking, gathering things at work, ready to leave 3.0; occupation; working in scene shop, theater actor, backstage employee 3.5; sports; archery (non-hunting) 3.0; sports; frisbee playing, general 3.0; sports; golf, miniature, driving range 3.5; sports; golf, using power cart 3.5; sports; horseback riding, saddling horse 3.0; sports; horseshoe pitching, quoits 3.0; sports; shuffleboard, lawn bowling 3.5; sports; trampoline 3.0; sports; volleyball, non-competitive 3.0; transportation; driving heavy truck, tractor, bus 3.5; walking; carrying infant or 15 pound load 3.0; walking; loading /unloading a car 3.0; walking; downstairs 3.0; walking; loading /unloading a car 3.0; walking; walking, 2.5 mph, firm surface 3.3; walking; walking, 3.0 mph, level, moderate pace, 3.8; walking; walking, 3.5 mph, level, brisk, firm surface 3.0; water activities; sailing, boat sailing, windsurfing, ice sailing, general 3.0; water activities; surfing, body or board 3.0; water activities; water volleyball 3.5; winter activities; snowmobiling 3.3; religious activities; walking, 3.0 mph, moderate speed 3.8; religious activities; walking, 3.5 mph, not carrying anything 3.0; religious activities; cleaning church 4 to 5 MET LEVEL 4.0; bicycling; bicycling, <10 mph, leisure, to work or for pleasure 4.8; dancing; ballet or modern, twist, jazz, tap, jitterbug 4.5; dancing; general 4.5; dancing; ballroom, fast (disco, folk, square), line dancing 4.0; fishing and hunting; digging worms, with shovel 4.0; fishing and hunting; fishing from river bank and walking
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 125

MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 4.0; home activities; multiple household tasks all at once, vigorous effort 4.0; home activities; sweeping garage, sidewalk or outside of house 4.0; home activities; walk/run - playing with children – moderate 4.0; home activities; elder care, disabled adult, only active periods 4.0; home activities; walk/run, playing with animals, moderate 4.0; home repair; automobile body work 4.5; home repair; carpentry, finishing or refinishing cabinets or furniture 4.5; home repair; caulking, except log cabin 4.5; home repair; laying or removing carpet 4.5; home repair; laying tile or linoleum, repairing appliances 4.5; home repair; painting 4.5; home repair; sanding floors with a power sander 4.5; home repair; scraping and painting 4.5; home repair; washing fence, painting fence 4.5; lawn and garden; mowing lawn, power mower 4.5; lawn and garden; operating snow blower, walking 4.5; lawn and garden; planting seedlings, shrubs 4.5; lawn and garden; planting trees 4.3; lawn and garden; raking lawn 4.0; lawn and garden; raking roof with snow rake 4.0; lawn and garden; sacking grass, leaves 4.5; lawn and garden; trimming shrubs or trees, manual cutter 4.5; lawn and garden; weeding, cultivating garden 4.0; lawn and garden; gardening, general 4.0; music playing; drums 4.0; music playing; marching band, playing an instrument (walking) 4.0; occupation; bakery, general, moderate effort 4.0; occupation; custodial work – feathering arena floor, moderate effort 4.0; occupation; farming, chasing cattle or other livestock on horseback 4.0; occupation; farming, feeding small animals, milk bottle for calf, goat 4.5; occupation; farming, feeding cattle, horses 4.5; occupation; farming, hauling water for animals, general hauling water 4.5; occupation; forestry, sawing, power 4.0; occupation; forestry, weeding 4.5; occupation; furriery – raise mink for fur coats
126 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 4.0; occupation; machine tooling, tapping and drilling 4.0; occupation; masseur, masseuse, manual therapy (standing) 4.5; occupation; orange grove work 4.0; occupation; police, making an arrest, taking command (standing) 4.0; occupation; lifting items continuously, 10 – 20 lbs, with limited walking 4.0; occupation; tailoring, pressing, starching 4.0; occupation; walking, 3.0 mph, moderately and carrying 25 lbs 4.0; occupation; walking, pushing a wheelchair 4.5; occupation; walking, 3.5 mph, briskly and carrying 25 pounds 4.5; running; jogging on a mini-tramp 4.5; sports; badminton, social singles and doubles, general 4.5; sports; basketball, shooting baskets 4.0; sports; coaching: football, soccer, basketball, baseball, swimming, etc. 4.0; sports; curling 4.5; sports; golf, general 4.5; sports; golf, walking and carrying clubs 4.3; sports; golf, walking and pulling clubs 4.0; sports; gymnastics, general 4.0; sports; softball, officiating 4.0; sports; table tennis, ping pong 4.0; sports; tai chi 4.0; walking; pushing a wheelchair, non-occupational setting 4.0; water activities; swimming, treading water, moderate effort, general 5 to 6 MET LEVEL 5.5; conditioning exercise; health club exercise, general 5.0; dancing; aerobic, low impact 5.5; dancing; ballroom, dancing fast 5.0; fishing and hunting; hunting, general 5.0; home activities; maple syruping/sugar bushing 5.0; home activities; walk/run-playing with children–vigorous 5.0; home activities; walk/run, playing with animals, vigorous 5.0; home repair; caulking, chinking log cabin 5.0; home repair; cleaning gutters
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 127

MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 5.0; home repair; hanging storm windows 5.0; home repair; painting the outside of the house 5.0; home repair; spreading dirt with a shovel 5.0; lawn and garden; carrying, loading or stacking wood 5.0; lawn and garden; clearing land, hauling branches 5.0; lawn and garden; digging sandbox 5.0; lawn and garden; digging, spading, filling garden with compost 5.0; lawn and garden; laying sod 5.5; lawn and garden; mowing lawn, general 5.5; lawn and garden; mowing lawn, walk, power mower 5.5; occupation; construction, outside, remodeling 5.5; occupation; farming, shoveling grain 5.0; occupation; forestry, ax chopping, (SLOW) 5.0; occupation; forestry, hoeing 5.0; occupation; walking, carrying objects about 25 to 49 pounds 5.0; sports; cricket (batting, bowling) 5.0; sports; softball or baseball, fast or slow pitch, general 5.0; sports; tennis, doubles 5.0; walking; using crutches 5.0; walking; walking, 4.0 mph, level, firm surface 5.0; walking; walking, grass track 5.0; water activities; snorkeling 5.5; winter activities; ice skating, moderate effort 5.0; winter activities; skiing, downhill, light effort 6 to 7 MET LEVEL 6.0; bicycling; 10-12 mph 6.0; fishing and hunting; fishing in stream, in waders 6.0; fishing and hunting; hunting, deer, elk, large game 6.0; fishing and hunting; hunting, pheasants or grouse 6.0; home activities; butchering animals 6.0; home activities; moving furniture, household items 6.0; home repair; carpentry, outside house, installing rain gutters 6.0; lawn and garden; chopping wood, splitting logs
128 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 6.0; lawn and garden; gardening with heavy power tools, tilling a garden 6.0; lawn and garden; mowing lawn, walk, hand mower 6.0; lawn and garden; shoveling snow, by hand 6.0; occupation; coal mining, general 6.0; occupation; farming, care of animals (grooming, brushing, shearing) 6.0; occupation; forestry, planting by hand 6.0; occupation; horse grooming 6.5; occupation; horse racing, trotting 6.5; occupation; truck driving, loading and unloading truck 6.0; occupation; using heavy power tools such jackhammers 6.0; sports; boxing, punching bag 6.0; walking; carrying 16 to 24 lb load, upstairs 6.0; walking; hiking, cross country 6.5; walking; marching, rapidly, military 6.0; walking; walking, 3.5 mph, uphill 6.3; walking; walking, 4.5 mph, level, firm surface 6.0; water activities; swimming, leisurely, not lap swimming, general 7 to 8 MET LEVEL 7.5; home activities; carrying groceries upstairs 7.5; home repair; carpentry, sawing hardwood 7.0; occupation; forestry, sawing by hand 7.0; occupation; masonry, concrete 7.0; running; jogging, general 7.0; sports; basketball, officiating 7.0; sports; racquetball, casual, general 7.0; sports; tennis, general 7.0; walking; backpacking 8 to 9 MET LEVEL 8.0; walking; up stairs 8.0; bicycling; bicycling, general 8.0; occupation; carrying heavy loads, such as bricks
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 129
MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 8.0; occupation; farming, baling hay, cleaning barn, vigorous effort 8.0; occupation; fire fighter, hauling hoses on ground 8.5; occupation; shoveling, digging ditches 8.0; running; running, 5 mph (12 min/mile) 8.0; sports; basketball, game 9 to 10 MET LEVEL 9.0; walking; carrying load upstairs, general 9.0; home activities; moving household items upstairs, carrying furniture 9.0; sports; football, competitive 10.0; walking; carrying 50 to 74 lb load, upstairs References
Barbara Ainsworth, William Haskell, Arthur Leon, David Jacobs, Jr., Henry Montoye, James Sallis & Ralph Paffenbarger, Jr. Compendium of physical activities: classification of energy costs of human physical activities. Medicine and Science in Sports and Exercise 25: 71-80, 1993. Wasserman K, Hansen JE, Sue DY, Whipp BJ, Casaburi R. Principles of exercise testing and interpretation, 3rd ed. Baltimore: Lippincott Williams & Wilkins; 1999. Wasserman K. Cardiopulmonary exercise testing and cardiovascular health. Armonk, NY: Futura; 2002. Principles of Exercise Testing and Interpretation; Including Pathophysiology. Karlman Wasserman, James E. Hansen, Darryl Y. Sue, Brian J. Whipp, William W. Stringer, M.D. - 2005 - 585 pages. Sue DY. Integrative cardiopulmonary testing: basis and application. Medicine, Exercise, Nutrition and Health 1994;3:32-35. Whipp BJ, Davis JA, Torres F, et al. A test to determine parameters of aerobic function during exercise. J Appl Physiol: Resp Environ Exerc Physiol 1981;50:217-221 Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 1986;60:2020-2027 Cohen-Solal A. Cardiopulmonary exercise testing in chronic heart failure. In: Wasserman K, ed. Exercise gas exchange in heart disease. Armonk, NY: Futura Publishing Co, 1996:17-35.
130 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Part A Part B Other
Physical Therapy
PLAN Skilled Services Required:GOALS (Short Term) Gait Training ROM/Contracture Mgmt.
Balance Re-ed Home ProgramOutcome (Long Term) Therapeutic ex. Pt/Caregiver Training
Muscle Re-Ed Safety SkillsEnergy Cons. Equipment Needs
Other
N/A
20. INITIAL ASSESSMENT 19. PRIOR HOSPITALIZATION FROM to
Age M / F Rehab Potential
Hx and level of function at start of care:
Min tolerated DistanceHR%SPO2RPEDyspneaFIO2
Min tolerated DistanceHR%SPO2RPEDyspneaFIO2
22. SERVICE DATES FROM THROUGH
FORM HCFA-700 (11-91)
2)
Tx Justification:
15. PHYSICIAN SIGNATURE 16. DATE
N/A
DISCONTINUE SERVICESORCONTINUE SERVICES
18. ON FILE (Print/type physician's name)
N/A
5)
21. FUNCTIONAL LEVEL(end of billing period) PROGRESS REPORT:
3. HICN
10. TREATMENT DIAGNOSIS
6. ONSET DATE 7. SOC DATE
FIRST NAME M.I. 2. PROVIDER NUMBER
4. PROVIDER NAME MEDICAL RECORD NO. (Optional)
DEPARTMENT OF HEALTH AND HUMAN SERVICES
HEALTH CARE FINANCING ADMINISTRATION
(professional establishing POC including professional designation)13. Signature
12. PLAN OF TREATMENT FUNCTIONAL GOALS
PLAN OF TREATMENT FOR OUTPATIENT REHABILITATION (COMPLETE FOR INITIAL CLAIMS ONLY)1. PATIENT'S LAST NAME
14. FREQ/DURATION (e.g. 3/wk x wk.)
11. VISITS FROM SOC
1)
8.TYPE: 9. PRIMARY DIAGNOSIS
2)
1)
From17. Certification
I CERTIFY THE NEED FOR THESE SERVICES FURNISHED UNDER THIS PLAN OF TREATMENT AND WHILE UNDER MY CARE
3)
4)
THROUGH
__
Assessment
____
6 minute walk test
6 minute walk test Assessment
______
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 131
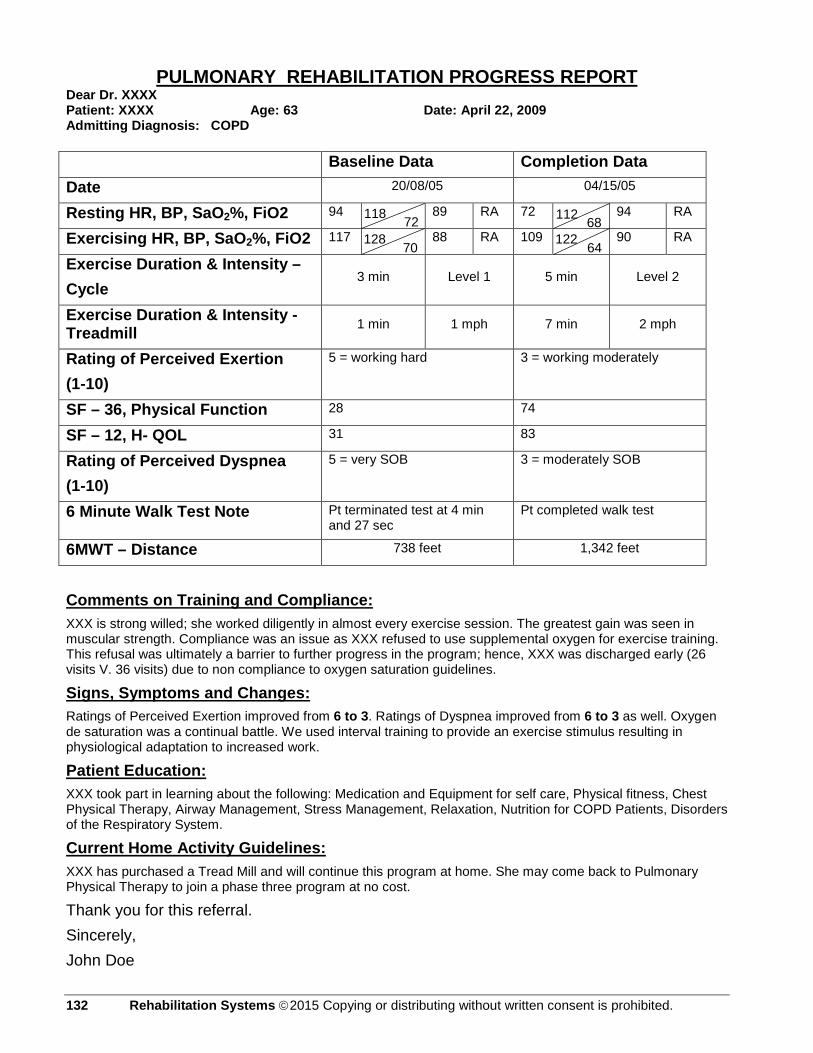
PULMONARY REHABILITATION PROGRESS REPORT Dear Dr. XXXX Patient: XXXX Age: 63 Date: April 22, 2009 Admitting Diagnosis: COPD Baseline Data Completion Data Date 20/08/05 04/15/05
Resting HR, BP, SaO2%, FiO2 94 89 RA 72 94 RA
Exercising HR, BP, SaO2%, FiO2 117 88 RA 109 90 RA
Exercise Duration & Intensity – Cycle
3 min Level 1 5 min Level 2
Exercise Duration & Intensity - Treadmill 1 min 1 mph 7 min 2 mph
Rating of Perceived Exertion (1-10)
5 = working hard 3 = working moderately
SF – 36, Physical Function 28 74
SF – 12, H- QOL 31 83
Rating of Perceived Dyspnea (1-10)
5 = very SOB 3 = moderately SOB
6 Minute Walk Test Note Pt terminated test at 4 min and 27 sec
Pt completed walk test
6MWT – Distance 738 feet 1,342 feet
Comments on Training and Compliance: XXX is strong willed; she worked diligently in almost every exercise session. The greatest gain was seen in muscular strength. Compliance was an issue as XXX refused to use supplemental oxygen for exercise training. This refusal was ultimately a barrier to further progress in the program; hence, XXX was discharged early (26 visits V. 36 visits) due to non compliance to oxygen saturation guidelines.
Signs, Symptoms and Changes: Ratings of Perceived Exertion improved from 6 to 3. Ratings of Dyspnea improved from 6 to 3 as well. Oxygen de saturation was a continual battle. We used interval training to provide an exercise stimulus resulting in physiological adaptation to increased work.
Patient Education: XXX took part in learning about the following: Medication and Equipment for self care, Physical fitness, Chest Physical Therapy, Airway Management, Stress Management, Relaxation, Nutrition for COPD Patients, Disorders of the Respiratory System.
Current Home Activity Guidelines: XXX has purchased a Tread Mill and will continue this program at home. She may come back to Pulmonary Physical Therapy to join a phase three program at no cost.
Thank you for this referral. Sincerely, John Doe
118
72 70
68 64
128
112 122
132 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
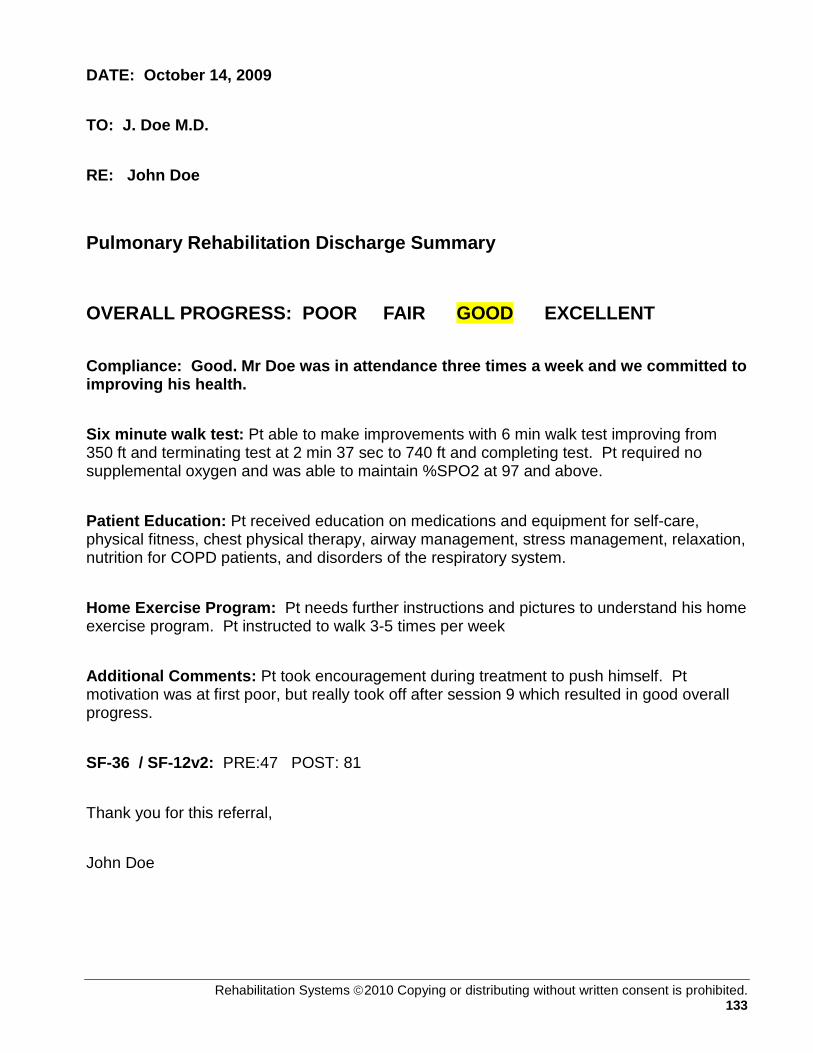
DATE: October 14, 2009 TO: J. Doe M.D. RE: John Doe
Pulmonary Rehabilitation Discharge Summary
OVERALL PROGRESS: POOR FAIR GOOD EXCELLENT Compliance: Good. Mr Doe was in attendance three times a week and we committed to improving his health. Six minute walk test: Pt able to make improvements with 6 min walk test improving from 350 ft and terminating test at 2 min 37 sec to 740 ft and completing test. Pt required no supplemental oxygen and was able to maintain %SPO2 at 97 and above. Patient Education: Pt received education on medications and equipment for self-care, physical fitness, chest physical therapy, airway management, stress management, relaxation, nutrition for COPD patients, and disorders of the respiratory system. Home Exercise Program: Pt needs further instructions and pictures to understand his home exercise program. Pt instructed to walk 3-5 times per week Additional Comments: Pt took encouragement during treatment to push himself. Pt motivation was at first poor, but really took off after session 9 which resulted in good overall progress. SF-36 / SF-12v2: PRE:47 POST: 81 Thank you for this referral, John Doe
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 133

134 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Roger K. Campbell, M.S., CET, MFT-c
Program & Project Manager
Rehabilitation Systems [email protected]
www.rehabsys.com
Mr. Campbell started his exercise science career in 1983 as an Army Master Fitness Trainer, where he physically prepared
troops for combat readiness and sports performance. With the GI Bill, Campbell obtained a Bachelor of Science Degree in
Exercise Science from Utah State University, followed by a Master of Science Degree from the University of Utah, in Clinical
Exercise Physiology. While earning a masters degree, Campbell also served as the Health and Fitness Program Director of
the Murray City Fire Department, which focused on the human performance demands and physical integrity needs of
firefighters.
Campbell's greatest passion however, is working for the functional restoration and independence of medically complex
patients. While serving the University of Utah's Lung Transplant program, Campbell realized that greater restorative
measures could, and should, be implemented to improve functional abilities of patients, and set his focus on their
rehabilitation pathway. Campbell spends his best energies devoted to developing, duplicating, and maintaining specialized
rehabilitation programs. Campbell is the creator of www.gocancerrehab.com, a growing cancer rehabilitation network of
care designed to increase access to restorative services, delivered by nurses, physical and occupational therapists.
Campbell's mission is the duplication of specialized rehabilitation programs in large and small communities alike.
Additionally, Campbell is committed to the educational development of health care professionals as a serving panel member
of the industries-first, accredited Cancer Specialist certification prepared by the American College of Sports Medicine
(ACSM) and the American Cancer Society (ACS).
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 135

COURSE EVALUATION Roger K. Campbell, M.S., CET, MFT-c. www.rehabsys.com, [email protected] The purpose of this evaluation is to gather input so that we may improve this course and how it is taught and therefore help you improve your learning. We are the only ones looking at your responses, and we will report back to you on the feedback received if you desire, you may email us at: [email protected] 1. What are the strongest features of this course? In other words, what contributed most to your learning experience? 2. What specific suggestions do you have for changes that we can make to improve the course or how it is taught? 3. Is the pace of the course: (Too Fast) (Just Right) (Too Slow)
136 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 137

Cong
ratu
latio
ns__
____
____
____
____
____
____
____
has
succ
essf
ully
com
plet
ed th
e Pu
lmon
ary
Reha
bilita
tion
Prog
ram
Im
plem
enta
tion
Cour
se
Utah
CEU
s, 1
6 Co
ntac
t Hou
rs,
Idah
o CE
Us, 1
6 Co
ntac
t Hou
rs,
Nev
ada
CEUs
, 15
Cont
act H
ours
____
____
____
____
____
____
____
__Ro
ger K
. Cam
pbel
l, M
.S.,
CET,
MFT
-cPr
ogra
m D
evel
oper
Spec
ial P
rogr
ams
Canc
er, P
ulm
onar
y, C
HF, D
iabe
tes,
ro
ger@
reha
bsys
.com
ww
w.re
habs
ys.c
om
138 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 139

COPD GLOSSARY
Acute: sudden, usually short-term
Advance directives: legal documents including the Living Will and Durable Power of Attorney for Health Care. A Living Will states what type of treatment you wish to receive in the event that you become physically or mentally unable to communicate your wishes. A Durable Power of Attorney for Health Care authorizes another person to make medical decisions for you when you are unable to do so for yourself. See also Living Will and Durable Power of Attorney for Health Care.
Adverse: undesirable or not expected
Allergen: a substance (such as a food or pollen) that your body perceives as dangerous and can cause an allergic reaction.
Allergy: abnormal reaction to a stimulus called an allergen. Allergy refers to the abnormal response of the airways to inhaled stimuli, such as pollen, or to consumed items, such as foods, that may cause unusual airway reactions and lead to bronchospasm.
Alpha1-antitrypsin (AAT): (also called alpha antiproteinase or AAP). A protective material produced in the liver and transported to the lungs to help combat inflammation. Deficiency states occur as the result of hereditary defects.
Alveoli: thin-walled, small sacs located at the ends of the smallest airways in the lungs where the exchange of oxygen and carbon dioxide takes place.
Antibiotic: medication used to treat infection caused by bacteria. Antibiotics do not protect against viruses and do not prevent the common cold.
Anticholinergics: (also called cholinergic blockers or "maintenance" bronchodilators). This type of medicine helps open (dilate) the bronchial tubes (airways) to help move more air easily into and out of the lungs. Anticholinergics also help clear mucus from the airways. As the airways open, the mucus moves more freely and can therefore be coughed out more easily. Anticholinergics work differently and more slowly than fast-acting bronchodilators.
Antihistamine: medication that prevents symptoms of congestion, watery eyes, sneezing, and itchy, runny nose by blocking histamine receptors.
Anti-inflammatory: medication, such as prednisone, aspirin or steroids, that reduces inflammation and swelling.
Apnea: absence of breathing for more than 10 seconds. See also sleep apnea.
Arterial blood gas test: a blood test that measures oxygen and carbon dioxide in the blood.
140 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

Atelectasis: partial or complete collapse of the lung, usually due to a blockage of the air passages with fluid, mucus or infection. Symptoms include dry cough, chest pain and mild shortness of breath.
Asthma, chronic: a disease of the air passages that carry air in and out of the lungs. Asthma causes the airways to narrow, the lining of the airways to swell and the cells that line the airways to produce more mucus. These changes make breathing difficult and cause a feeling of not getting enough air into the lungs. Common symptoms include shortness of breath, wheezing and excess mucus production.
Bacteria: infectious organisms (germs) that may cause bronchitis or pneumonia.
BIPAP (bi-level positive airway pressure) machine: a breathing machine that uses two pressure levels (inspiratory and expiratory) to provide breathing assistance. This machine is often used for patients with sleep apnea or respiratory failure.
Black pigment: the material that gives damaged human lungs a black and sooty appearance.
Blebs and bullae: localized destruction of portions of the lungs that may compress otherwise useful lung tissues.
Breath sounds: sounds heard through a stethoscope. The intensity of the sound of air moving in and out of the lungs may indicate the amount of obstruction.
Breathing rate: the number of breaths per minute.
Bronchial tubes: branches of the airways (air passages) in the lungs.
Bronchioles: the smallest branches of the airways in the lungs. They connect to the alveoli (air sacs).
Bronchitis, chronic: irritation and inflammation of the lining of the bronchial tubes. The irritation causes coughing and excess amounts of mucus in the airways which can lead to difficulty breathing. Bronchitis is considered chronic when the person has a productive cough (coughs up mucus) and shortness of breath that lasts at least three months each year for at least two years in a row.
Bronchodilator: medication used to relax the muscle bands that tighten around the airways to increase air flow. Bronchodilators also help clear mucus from the lungs.
Bronchodilators, fast-acting: (also called "rescue" or "quick relief" medications). These medications quickly relax muscles that tighten around the airways, making the airways wider, breathing easier, and shortness of breath reduced.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 141
Bronchodilators, long-acting: also called ("maintenance" medications). These medications prevent airway spasms throughout the day and night; they take effect more slowly than fast-acting bronchodilators, but work for a longer period of time.
Bronchospasm: the sudden tightening of the bands of muscle that surround the airways, causing the airways to become narrower. Bronchospasm may result in wheezing.
Cannula: a small plastic tube used to supply extra oxygen through the nose.
Carbon dioxide: a colorless, odorless gas that is formed in tissues of the body and is delivered to the lungs for removal.
Carcinogen: cancer-causing substance.
Chronic: continuing over a certain period of time; long-term.
Cilia: hair-like structures that line the airways in the lungs and help to clean out the airways.
CPAP (continuous positive airway pressure) machine: A breathing machine that provides pressure to keep the upper airways open during breathing. This machine is often used for patients with obstructive sleep apnea.
Clinical trials: research programs conducted with patients to evaluate a new medical treatment, drug or device. The purpose of clinical trials is to find new and improved methods of treating different diseases and special conditions.
Closed mouth technique: a method for inhaling medicine from a metered dose inhaler. The open mouth technique is the preferred method. (See open mouth technique)
Contraindication: any condition which indicates that a particular course of treatment (or exercise) would be inadvisable or cause harm.
Controlled coughing: a technique in which the cough comes from deep within the lungs and has just enough force to loosen and carry mucus through the airways without causing them to narrow and collapse. Controlled coughing saves energy and oxygen.
COPD (chronic obstructive pulmonary disease): COPD is a general term for several lung diseases that includes chronic bronchitis, emphysema and chronic asthma. COPD adds to the work of the heart, since the amount of oxygen that goes to the blood may be reduced. The two primary causes of COPD are cigarette smoking and alpha1 antitrypsin deficiency. Air pollution and occupational dusts may also contribute to COPD, especially if the person exposed to these substances is a smoker.
Cor pulmonale: enlargement of the right side of the heart. Cor pulmonale weakens the heart and causes increased shortness of breath and swelling in the feet and legs. Patients who have chronic COPD with low oxygen levels may develop this condition.
142 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.

CPR (cardiopulmonary resuscitation): a first-aid method to restore breathing and heart action through mouth-to-mouth breathing and chest compression.
Decongestant: Medication that shrinks swollen nasal tissues to relieve symptoms of nasal swelling, congestion and mucus secretion.
Dehydration: excessive loss of water from the body.
Diaphragm: most efficient breathing muscle, located at the base of the lungs.
Diaphragmatic breathing: method of breathing which helps you use the diaphragm correctly so you use less effort and energy to breathe.
Dietitian: A health care professional who specializes in food and nutrition.
Diffusion capacity: a measurement of how much oxygen is carried from your lungs into your bloodstream.
Diuretic: medication that increases urine output. Helps the body get rid of excess fluid. Also called a "water pill."
Dry powder inhaler (DPI): a device for inhaling respiratory medications that come in powder form.
Durable Power of Attorney for health care: a legal document that authorizes another person to make health-care decisions for you if you became physically or mentally unable to make these decisions yourself.
Dyspnea: shortness of breath.
Edema: swelling that may occur in the ankles, feet or legs.
Electrocardiogram (EKG): a tracing of the heart's electrical activity. Can show heart strain and heart disease.
Emphysema: the destruction, or breakdown, of the walls of the alveoli located at the end of the bronchial tubes. The damaged alveoli are not able to exchange oxygen and carbon dioxide between the lungs and the blood. The bronchioles lose their elasticity and collapse during exhalation, trapping air in the lungs. The trapped air keeps fresh air and oxygen from entering the lungs.
Exacerbation: worsening.
Expectorant: medication that helps to thin mucus in the airways so it can be coughed out more easily. These medications should be taken with at least 8 ounces of water.
Exhalation: breathing air out of the lungs; expiration.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 143
Flutter valve: see mucus clearing device
Heart failure: a condition caused by weakening of the heart muscle. The heart is strained and can not pump enough blood. Fluid can build up in the lungs and other parts of the body. Symptoms can include shortness of breath and swelling of the legs, ankles and feet.
(HEP) high-efficiency particulate air filter: a filter which removes particles in the air by forcing it through screens containing microscopic pores.
High blood pressure: a condition (that usually has no symptoms) involving higher than normal pressure of the blood against the blood vessels. High blood pressure increases the risk of developing heart disease, a heart attack and a stroke.
Histamine: a naturally-occurring substance that is released by the immune system after being exposed to an allergen. When you inhale an allergen, mast cells located in the nose and sinus membranes release histamine. Histamine then attaches to receptors on nearby blood vessels, causing them to enlarge (dilate). Histamine also binds to other receptors located in nasal tissues, causing redness, swelling, itching and changes in the secretions.
Holding chamber: see spacer
Home care company: organization that provides many aspects of COPD care in the home, including the use and care of respiratory equipment, teaching, monitoring and review of environment and treatment.
Humidification: the act of moisturizing the air with molecules of water.
Hyperventilation: excessive rate and depth of breathing.
Hypoxia: insufficient oxygen in the tissues, even though blood flow is adequate.
Immune system: the body's defense system that protects us against infections and foreign substances.
IAQ: indoor air quality.
Incentive spirometer: a device that encourages deep inspiration to expand the lungs and improve cough effectiveness.
Indication: reason to use.
Inflammation: a response in the body that may include swelling and redness.
Inhaler: See metered dose inhaler (MDI)
Inspiration: breathing air into the lungs; inhalation.
144 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Intubation: placing a tube in the trachea (wind pipe) to enable artificial breathing; can be a lifesaving procedure.
I/E ratio: inhalation/exhalation ratio, or the relative length of inhalation (breathing in) compared to exhalation (breathing out).
Irritant: substance that is not an allergen (see allergen) but can cause a reaction in the airways or damage the lungs.
Leukotriene modifier: medication that blocks chemicals called leukotrienes in the airways. Leukotrienes occur naturally in the body and cause tightening of airway muscles and production of excess mucus and fluid. Leukotriene modifiers work by blocking leukotrienes and decreasing these reactions. These medications are also helpful in improving airflow and reducing some COPD symptoms.
Living Will: a legal document in which you can state what kind of medical care you desire to receive or what life-support procedures you would like to withhold if you became physically or mentally unable to communicate your wishes.
Lung volume: See total lung capacity
Lung volume reduction surgery: surgery in which damaged areas of the lungs are removed so the remaining portion of the lungs can function better. Lung volume reduction surgery is performed only for people with certain types of COPD, and after careful testing and evaluation.
Lung transplantation: a surgical procedure in which a healthy lung from a donor replaces the recipient's unhealthy lung. Lung transplant as a treatment option for COPD is reserved for carefully selected patients.
Maximal oxygen uptake: a person's highest rate of oxygen consumption. This measurement is usually expressed in milliliters of oxygen per kilogram of body weight per minute.
Medical history: a list of a person's previous illnesses, present conditions, symptoms, medications and health risk factors.
Medical referral: a doctor's recommendation that a patient see a qualified medical professional, often a specialist, to review their health status and determine whether medical treatment is needed or whether a particular course of exercise and/or diet change is safe.
Metabolism: the body's use of oxygen and food to produce energy.
Metered dose inhaler (MDI): small aerosol canister placed in a plastic container that releases a mist of medication when pressed down from the top. This medication can be
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 145
breathed into the airways. Many COPD medications are taken using a MDI.
Monitoring: keeping track of.
Mucolytic agent: medication that thins mucus secretions.
Mucus: a material produced by glands in the airways, nose, sinuses and elsewhere in the body. Mucus cleans and protects certain parts of the body such as the lungs.
Mucus clearing device: a device used to loosen mucus in the airways so it can be coughed up more easily.
Nasal cannula: a light-weight tube with two hollow prongs that fit just inside the nose. Nasal cannulas are used to deliver oxygen.
Nasal spray: medication used to prevent nasal allergy symptoms. Available by prescription or over-the-counter in decongestant, corticosteroid or salt-water solution form.
Nebulizer: a machine that changes liquid medicine into fine droplets (in aerosol or mist form) that are inhaled through a mouthpiece or mask. Nebulizers can be used to deliver bronchodilator (airway-opening) medications such as Albuterol and Atrovent. A nebulizer may be used instead of a metered dose inhaler (MDI). It is powered by a compressed air machine and plugs into an electrical outlet.
Non-steroidal: medication that is not a steroid. Also see steroid.
Open mouth technique: effective method for inhaling medicine from a metered dose inhaler. See closed mouth technique.
Orthopnea: difficulty breathing related to body position, especially shortness of breath while lying on the back. This is often treated by propping the person's head on two or more pillows while lying down.
Oxygen: the essential element in the respiration process to sustain life. This colorless, odorless gas makes up about 21 percent of the air. Oxygen may be prescribed if your lungs are not getting enough oxygen to your blood. Breathing prescribed oxygen increases the amount of oxygen in your blood, reduces the extra work of the heart and decreases shortness of breath.
Oxygen, compressed: a form of prescribed oxygen that is stored in a tank in gas form. A flow meter and a regulator are attached to the tank to adjust the oxygen flow. The compressed oxygen system is generally prescribed when oxygen is not needed all the time, such as only when walking or performing physical activity.
146 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Oxygen, liquid: At very cold temperatures, oxygen changes from a gas to a liquid. When liquid oxygen is warmed, it becomes a gas so that it can be delivered to you. A liquid oxygen system includes a large stationary unit that stays in the home. It also includes a small, portable canister (weighing from 5 to 13 pounds) that can be filled from the stationary unit for trips outside the home.
Oxygen concentrator: an electric oxygen delivery system about the size of a large suitcase. The concentrator extracts some of the air from the room and separates the oxygen from other gases in the air. Oxygen is then delivered to you through a nasal cannula. An oxygen concentrator may be recommended if you need oxygen all the time or while sleeping.
PEP valve: See mucus clearing device
Peak expiratory flow rate: a test used to measure how fast air can be exhaled from the lungs.
Personal best peak expiratory flow (PEF): the highest peak flow number a person can achieve over a 2- to 3-week period when symptoms are under good control. The personal best PEF is the number to which all other peak flow readings will be compared.
Pharynx: the back of the throat through which air passes when you inhale.
Pneumonia: a sudden infection of localized areas of the lungs. Pneumonia often accompanies bronchitis.
Pollen: a fine, powdery substance released by plants and trees.
Positive expiratory therapy valve: see mucus clearing device
Postural drainage: positioning oneself in certain postures to allow gravity to help drain mucus or phlegm from the lungs.
Productive cough: a "wet" cough that may involve coughing up mucus.
Puffer: another term for inhaler or metered dose inhaler.
Pulmonary function tests (PFTS): a series of tests that measure how well air is moving in and out of the lungs and carrying oxygen to the blood stream.
Pulmonary hypertension: a rare lung disorder in which the arteries in the lungs have become narrowed, making it difficult for blood to flow through the vessels.
Pulmonologist: a doctor who specializes in caring for people with lung diseases and breathing problems.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 147
Pulse oximetry: a non-invasive test in which a device that clips on the finger measures the oxygen level in the blood.
Pursed lip breathing: a method of breathing through pursed lips (as if you were blowing on a whistle) to improve breathing patterns.
Relapse: the return of signs and symptoms of an illness after a period of improvement.
Residual volume: the volume of air remaining in the lungs, measured after a maximum expiration.
Respiration: the process of breathing which includes the exchange of gases in the blood (oxygen and carbon dioxide). See inhalation and exhalation.
Respiratory failure: the sudden inability of the lungs to provide normal oxygen delivery or normal carbon dioxide removal.
Respiratory therapist: a health care professional who specializes in assessment, treatment and education for people with lung diseases.
Respiratory therapy department: a hospital department that provides therapies and treatments to patients who have cardiopulmonary problems.
Pulmonary rehabilitation: a program that can help you learn how to breathe easier and improve your quality of life. It includes treatment, exercise training, education and counseling.
Sedentary: not very physically active.
Sleep apnea: a sleep disorder in which a person's breathing stops in intervals that may last from 10 seconds to a minute or longer. When an apneic event occurs, air exchange may be impaired.
Spacer: a tube-like device (also called a holding chamber) used with a metered dose inhaler. The spacer makes it easier to coordinate pressing on the inhaler and breathing in the medicine.
Spirometry: see total lung capacity test
Sputum: mucus or phlegm.
Steroid: medication that reduces swelling and inflammation. Comes in pill and inhaled forms.
Supplement: nutritional: drinks that can be used in addition to meals to increase intake of calories and nutrients.
Theophylline agents: (also called "maintenance" or "long-term control" bronchodilators). These agents open airways, prevent and relieve airway spasms, and prevent night-time cough and shortness of breath. 148 Rehabilitation Systems 2015 Copying or distributing without written consent is prohibited.
Thorax: the muscular and bony structure of the chest.
Tidal volume: the quantity of air inhaled and exhaled in one respiratory cycle during regular breathing.
Total lung capacity test: a test that measures the amount of air in the lungs after a person has breathed in as much as possible.
Trachea: the main airway (windpipe) supplying air to both lungs.
Tracheostomy: a surgical opening made when necessary in the main airway, the trachea.
Vaccine: an injected medication that may stimulate the immune response to protect a person from an infection.
Ventilator: the proper term for a breathing machine used to treat respiratory failure and help support breathing.
Virus: a group of highly contagious infectious agents that cause a variety of colds and chest infections. Viruses are not affected by antibiotics, however the influenza vaccine is effective against the influenza virus.
Vital capacity: maximal breathing capacity; the amount of air that can be expired after a maximum inspiration.
Wheezing: the high-pitched whistling sound of air entering or leaving narrowed airways.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 149