Pulmonary manifestations of early schistosome infection among nonimmune travelers
5
Pulmonary Manifestations of Early Schistosome Infection among Nonimmune Travelers Eli Schwartz, MD, DTMH, Judith Rozenman, MD, Marina Perelman, MD PURPOSE: The clinical aspects of acute pulmonary schistoso- miasis among nonimmune patients have not been well charac- terized. METHODS: We evaluated 8 patients who presented with pul- monary symptoms and abnormal chest radiographs after recent travel to Africa. Diagnosis was based on the detection of schis- tosomal eggs or positive serology. RESULTS: Of 60 patients evaluated in our center for schisto- somiasis during a 3-year period, 8 (6 with Schistosoma hemato- bium, 2 with S. mansoni) had pulmonary symptoms. These symptoms appeared 3 to 6 weeks after exposure and consisted of dry cough and shortness of breath without concurrent fever. The mean (6 SD) eosinophil count was 4020 6 1400 per mmL. Chest radiography revealed multiple small nodules in 7 pa- tients; in 1 patient, a diffuse interstitial infiltrate was also seen. Computerized tomographic scans of the chest were obtained in 4 patients; the scans confirmed the nodular pattern and de- tected a greater number of nodules. A transbronchial biopsy in 1 patient revealed eosinophilic pneumonia without detection of larva or eggs. CONCLUSION: Pulmonary manifestations during the early stage of schistosomal infection may occur with either S. hema- tobium or S. mansoni infection. These manifestations may rep- resent an immunologic process, as is thought to be responsible for the febrile systemic response (Katayama fever) to acute infection. Am J Med. 2000;109:718 –722. q2000 by Excerpta Medica, Inc. S chistosomiasis affects more than 200 million people in more than 70 countries, mainly in places where the socioeconomic conditions are substandard (1). Its clinical manifestations can be divided into three stages. The first stage is characterized by an immediate skin reaction, occurring within 24 hours after skin pene- tration by the cercaria and manifesting as a pruritic pap- ular rash (“swimmer’s itch”). Second, there may be an acute febrile stage, Katayama fever, that occurs 3 to 8 weeks after infection during the maturation of the adult worm, primarily in patients infected with Schistosoma ja- ponicum or S. mansoni. The late stage, or chronic schisto- somiasis, appears months to years after infection, result- ing from granuloma formation around the schistosoma eggs that are retained in tissues (1). Unlike the clinical course of schistosome infection in indigenous tropical populations, the clinical picture of this disease among nonimmune patients is poorly under- stood. Katayama fever, for example, is a febrile manifes- tation in nonimmune patients; its other symptoms and signs include headache, cough, arthralgia, hepatospleno- megaly, and marked eosinophilia. Although a short pe- riod of cough may occur during Katayama fever, primar- ily in S. mansoni infections (2,3), pulmonary signs and symptoms have not been reported as prominent features of the acute phase of the disease, especially in the absence of the other features of Katayama fever. We present the clinical and radiologic findings in a series of nonimmune travelers who experienced prolonged pulmonary symp- toms after infection with S. hematobium or S. mansoni. MATERIAL AND METHODS Charts of patients evaluated between June 1996 and June 1999 at the Center for Geographic Medicine, Sheba Med- ical Center, were reviewed for the diagnosis of schistoso- miasis. The records of nonimmune travelers (those with- out previous exposure to a schistosoma-endemic area) who had pulmonary symptoms and abnormal chest ra- diographs were further examined. Medical histories in- cluded the travel itineraries, whether there was exposure to fresh water, the time of exposure, and time to appear- ance of pulmonary symptoms. As part of their routine evaluation, each patient had provided a stool and urine sample for ova and parasite examination. Blood speci- mens had been obtained to screen for schistosome anti- bodies by enzyme-linked immunosorbent assay (FAST- ELISA) and immunoblot confirmation (performed by the Division of Parasitic Diseases, Centers for Disease Control, Atlanta, Georgia) (4). The diagnosis of schisto- some infection was based on documentation of eggs in the urine or stool, or a positive schistosome serologic test. RESULTS Of 60 patients with schistosomiasis seen during the 3-year period, 8 were identified with respiratory prob- Accepted for publication Aug 29, 2000. From the The Center for Geographic Medicine and Department of Medicine C (Dr Schwartz), the Department of Radiology (Dr Rozen- man), and the Department of Pathology (Dr Perelman), Sheba Medical Center, Tel-Hashomer, and Sackler School of Medicine, Tel-Aviv Uni- versity, Tel-Aviv, Israel. Reprint requests to Eli Schwartz, MD, DTMH, The Center for Geo- graphic Medicine and Department of Medicine C, Chaim Sheba Medi- cal Center, Tel Hashomer, Israel 52621; fax: 9725302011; e-mail: [email protected] 718 q2000 by Excerpta Medica, Inc. 0002-9343/00/$–see front matter All rights reserved. PII S0002-9343(00)00619-7
-
Upload
eli-schwartz -
Category
Documents
-
view
213 -
download
1
Transcript of Pulmonary manifestations of early schistosome infection among nonimmune travelers

Pulmonary Manifestations of Early SchistosomeInfection among Nonimmune Travelers
Eli Schwartz, MD, DTMH, Judith Rozenman, MD, Marina Perelman, MD
PURPOSE: The clinical aspects of acute pulmonary schistoso-miasis among nonimmune patients have not been well charac-terized.METHODS: We evaluated 8 patients who presented with pul-monary symptoms and abnormal chest radiographs after recenttravel to Africa. Diagnosis was based on the detection of schis-tosomal eggs or positive serology.RESULTS: Of 60 patients evaluated in our center for schisto-somiasis during a 3-year period, 8 (6 with Schistosoma hemato-bium, 2 with S. mansoni) had pulmonary symptoms. Thesesymptoms appeared 3 to 6 weeks after exposure and consisted ofdry cough and shortness of breath without concurrent fever.The mean (6 SD) eosinophil count was 4020 6 1400 per mmL.Chest radiography revealed multiple small nodules in 7 pa-
tients; in 1 patient, a diffuse interstitial infiltrate was also seen.Computerized tomographic scans of the chest were obtained in4 patients; the scans confirmed the nodular pattern and de-tected a greater number of nodules. A transbronchial biopsy in1 patient revealed eosinophilic pneumonia without detection oflarva or eggs.CONCLUSION: Pulmonary manifestations during the earlystage of schistosomal infection may occur with either S. hema-tobium or S. mansoni infection. These manifestations may rep-resent an immunologic process, as is thought to be responsiblefor the febrile systemic response (Katayama fever) to acuteinfection. Am J Med. 2000;109:718 –722. q2000 by ExcerptaMedica, Inc.
Schistosomiasis affects more than 200 million peoplein more than 70 countries, mainly in places wherethe socioeconomic conditions are substandard (1).
Its clinical manifestations can be divided into threestages. The first stage is characterized by an immediateskin reaction, occurring within 24 hours after skin pene-tration by the cercaria and manifesting as a pruritic pap-ular rash (“swimmer’s itch”). Second, there may be anacute febrile stage, Katayama fever, that occurs 3 to 8weeks after infection during the maturation of the adultworm, primarily in patients infected with Schistosoma ja-ponicum or S. mansoni. The late stage, or chronic schisto-somiasis, appears months to years after infection, result-ing from granuloma formation around the schistosomaeggs that are retained in tissues (1).
Unlike the clinical course of schistosome infection inindigenous tropical populations, the clinical picture ofthis disease among nonimmune patients is poorly under-stood. Katayama fever, for example, is a febrile manifes-tation in nonimmune patients; its other symptoms andsigns include headache, cough, arthralgia, hepatospleno-megaly, and marked eosinophilia. Although a short pe-riod of cough may occur during Katayama fever, primar-ily in S. mansoni infections (2,3), pulmonary signs and
symptoms have not been reported as prominent featuresof the acute phase of the disease, especially in the absenceof the other features of Katayama fever. We present theclinical and radiologic findings in a series of nonimmunetravelers who experienced prolonged pulmonary symp-toms after infection with S. hematobium or S. mansoni.
MATERIAL AND METHODS
Charts of patients evaluated between June 1996 and June1999 at the Center for Geographic Medicine, Sheba Med-ical Center, were reviewed for the diagnosis of schistoso-miasis. The records of nonimmune travelers (those with-out previous exposure to a schistosoma-endemic area)who had pulmonary symptoms and abnormal chest ra-diographs were further examined. Medical histories in-cluded the travel itineraries, whether there was exposureto fresh water, the time of exposure, and time to appear-ance of pulmonary symptoms. As part of their routineevaluation, each patient had provided a stool and urinesample for ova and parasite examination. Blood speci-mens had been obtained to screen for schistosome anti-bodies by enzyme-linked immunosorbent assay (FAST-ELISA) and immunoblot confirmation (performed bythe Division of Parasitic Diseases, Centers for DiseaseControl, Atlanta, Georgia) (4). The diagnosis of schisto-some infection was based on documentation of eggs inthe urine or stool, or a positive schistosome serologic test.
RESULTS
Of 60 patients with schistosomiasis seen during the3-year period, 8 were identified with respiratory prob-
Accepted for publication Aug 29, 2000.From the The Center for Geographic Medicine and Department of
Medicine C (Dr Schwartz), the Department of Radiology (Dr Rozen-man), and the Department of Pathology (Dr Perelman), Sheba MedicalCenter, Tel-Hashomer, and Sackler School of Medicine, Tel-Aviv Uni-versity, Tel-Aviv, Israel.
Reprint requests to Eli Schwartz, MD, DTMH, The Center for Geo-graphic Medicine and Department of Medicine C, Chaim Sheba Medi-cal Center, Tel Hashomer, Israel 52621; fax: 9725302011; e-mail:[email protected]
718 q2000 by Excerpta Medica, Inc. 0002-9343/00/$–see front matterAll rights reserved. PII S0002-9343(00)00619-7
lems and abnormal chest radiographs (Table). All 8 hadtraveled to Africa, including 6 who had been exposedwhile swimming in Lake Malawi. The other 2 patients hadonly one exposure each in slow-flowing rivers. Six had S.hematobium infection, and 2 were infected with S. man-soni. The patients were between the ages of 23 and 30years, which reflects the age of Israeli travelers to Africa,except patient 4 (age 45 years), who was a long-term ex-patriate and was infected after one exposure in the VoltaRiver in Ghana.
The interval between exposure and the beginning ofsymptoms was 3 to 6 weeks, although the diagnosis wasnot confirmed for at least 1 month in all of the patients.All 8 patients reported shortness of breath and a drycough, particularly while recumbent. None were febrile,but all recalled a short febrile episode of 2 to 3 days beforethe onset of symptoms, with a maximum temperature of398 C. One patient also had urticaria that was treated withantihistamines before the development of his pulmonarysymptoms.
Physical examination of the patients was unremark-able, although a prolonged expiratory phase was noted in2 patients. Laboratory data revealed mild leukocytosis,with mean (6 SD) percent eosinophilia of 37% 6 9% andmean total eosinophil count of 4020 6 1400 per mmL.
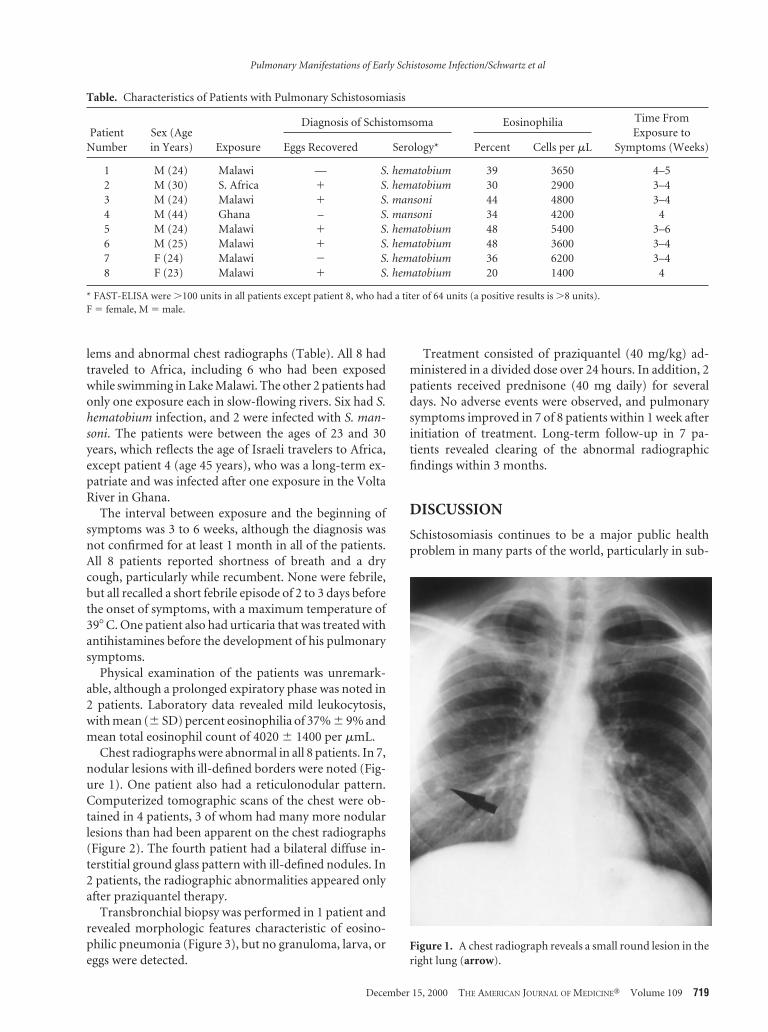
Chest radiographs were abnormal in all 8 patients. In 7,nodular lesions with ill-defined borders were noted (Fig-ure 1). One patient also had a reticulonodular pattern.Computerized tomographic scans of the chest were ob-tained in 4 patients, 3 of whom had many more nodularlesions than had been apparent on the chest radiographs(Figure 2). The fourth patient had a bilateral diffuse in-terstitial ground glass pattern with ill-defined nodules. In2 patients, the radiographic abnormalities appeared onlyafter praziquantel therapy.
Transbronchial biopsy was performed in 1 patient andrevealed morphologic features characteristic of eosino-philic pneumonia (Figure 3), but no granuloma, larva, oreggs were detected.
Treatment consisted of praziquantel (40 mg/kg) ad-ministered in a divided dose over 24 hours. In addition, 2patients received prednisone (40 mg daily) for severaldays. No adverse events were observed, and pulmonarysymptoms improved in 7 of 8 patients within 1 week afterinitiation of treatment. Long-term follow-up in 7 pa-tients revealed clearing of the abnormal radiographicfindings within 3 months.
DISCUSSION
Schistosomiasis continues to be a major public healthproblem in many parts of the world, particularly in sub-
Figure 1. A chest radiograph reveals a small round lesion in theright lung (arrow).
Table. Characteristics of Patients with Pulmonary Schistosomiasis
PatientNumber
Sex (Agein Years) Exposure
Diagnosis of Schistomsoma Eosinophilia Time FromExposure to
Symptoms (Weeks)Eggs Recovered Serology* Percent Cells per mL
1 M (24) Malawi — S. hematobium 39 3650 4–52 M (30) S. Africa 1 S. hematobium 30 2900 3–43 M (24) Malawi 1 S. mansoni 44 4800 3–44 M (44) Ghana – S. mansoni 34 4200 45 M (24) Malawi 1 S. hematobium 48 5400 3–66 M (25) Malawi 1 S. hematobium 48 3600 3–47 F (24) Malawi 2 S. hematobium 36 6200 3–48 F (23) Malawi 1 S. hematobium 20 1400 4
* FAST-ELISA were .100 units in all patients except patient 8, who had a titer of 64 units (a positive results is .8 units).F 5 female, M 5 male.
Pulmonary Manifestations of Early Schistosome Infection/Schwartz et al
December 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109 719

Saharan Africa. The type of chronic disease and end-organinvolvement depends on the schistosome species in-volved, with S. mansoni and S. japonicum affecting thehepatic portal system and S. hematobium affecting thegenitourinary system.
Pulmonary involvement is uncommon but has beendescribed among populations living in endemic areas.Abnormal migration of the eggs of S. mansoni from theportal system through porto-caval shunts, or from thevesicle veins in S. hematobium, may result in ectopic dep-osition of eggs in the pulmonary beds (5). The patholog-ical changes seen in the lungs are primarily the result ofgranuloma formation around these eggs. After manyyears, fibrosis ensues, leading to pulmonary hypertensionand cor pulmonale (6).
The pathological process seen in the lungs of the non-immune patients in our series would be expected to bedifferent. Pulmonary involvement occurred relativelyearly after infection and was reversible. The infiltrates inthese patients were probably not related to schistosomalmigration through the lungs, which typically occurs 5 to 7days after penetration. In our patients, symptoms beganabout 1 month after exposure, and the radiographic eval-uations were performed 4 to 12 weeks after exposure. It istherefore more likely that the pulmonary processes wereimmunologically mediated, similar to those seen in otherforms of eosinophilic pneumonias, in which an incitingagent elsewhere in the body (for example, the intestine) isresponsible (7).
The pathophysiology of acute schistosomiasis in non-immune patients is poorly understood (8). Diaz-Rivera et
al (2) performed serial liver biopsies in US soldiers after S.mansoni infection and demonstrated diffuse eosinophilicinfiltration and pseudotubercle formation. In our pa-tients, the one transbronchial biopsy that was performedrevealed eosinophilic infiltration of the airspaces and eo-sinophilic abscesses, suggesting an immunologic process.In support of this hypothesis, symptoms were also seen inpatients in whom eggs were not detected in the stool.Furthermore, 2 patients developed radiologic findingsonly after treatment was instituted. Treatment is a knownfactor in antigenic stimulation (9) and may be accompa-nied by clinical deterioration (10). Thus, the symptomsare more likely attributable to antigenic stimulationrather than to ectopic egg migration.
Katayama fever is also the result of an immunologicprocess occurring in nonimmune patients. It occurs 3 to8 weeks after infection and is considered to be related toeggs production by adult worms. The syndrome was ini-tially described in Japanese patients after infection with S.japonicum and was later recognized in patients with S.mansoni (2).
There have been a few recent case reports of pulmo-nary infiltrates in febrile patients with acute schistosomi-asis (11,12). The pulmonary syndrome that we have de-scribed is not entirely consistent with Katayama fever,because our patients were infected primarily with S. he-matobium and were not febrile while they had pulmonarysymptoms.
The clinical manifestations of acute schistosomiasismay result from the same immunologic process as Katay-ama fever and may include fever, urticaria, arthralgia,
Figure 2. A computerized tomographic scan through the bifurcation of the trachea shows multiple lesions of different sizes in both lungs.
Pulmonary Manifestations of Early Schistosome Infection/Schwartz et al
720 December 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109

Figure 3. (Top) A transbronchial biopsy specimen shows alveolar spaces (asterisks) filled with numerous eosinophils and macro-phages in association with an interstitial infiltrate and hyperplasia of type two pneumocytes lining the alveolar septae (arrowheads).A focus of intra-alveolar organization is seen in the right upper field (hematoxylin and eosin 3200). (Bottom) Higher magnificationdemonstrates the intra-alveolar infiltrate composed of numerous eosinophils and macrophages (hematoxylin and eosin 3400).
Pulmonary Manifestations of Early Schistosome Infection/Schwartz et al
December 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109 721

hepatosplenomegaly, hepatitis, eosinophilia, and pulmo-nary disease. This syndrome affects nonimmune patients,begins 3 to 4 weeks after infection, and may manifest forseveral months. The pulmonary process was identified inpatients with infection resulting from S. hematobium andS. mansoni, the most common in Africa (13), but proba-bly can occur with infection resulting from other species.
Praziquantel is known to be effective against the adultworm, but its effects in acute schistosomiasis are not clear(8). In this series, almost all patients appeared to improvesoon after receiving the drug, but we cannot rule out thatimprovement may have been the result of the self-limitednature of the process or because several patients receivedconcurrent steroids.
ACKNOWLEDGMENTThe authors thank Dr. Phyllis Kozarsky for her thorough andcritical review of the manuscript, Ms. Marianna Wilson, Divi-sion of Parasitic Diseases at the Center for Disease Control At-lanta, for performing the serology tests, and Dr. Marty Cetronfor his valuable comments.
REFERENCES1. Mahmoud AAF, Abdel Wahab MF. Schistosomiasis. In: Warren
KS, Mahmoud AAF, eds. Tropical, and Geographical Medicine, 2nded. New York: McGraw-Hill, 1990:470 – 471.
2. Diaz-Rivera E, Ramos-Morales RS, Koppisch E, et al. Acute Man-son’s schistosomiasis. Am J Med. 1956;18:918 –943.
3. Hiatt RA, Sotomayor ZR, Sanches G, et al. Factors in the pathogen-esis of acute schistosomiasis mansoni. J Infect Dis. 1979;139:659 –666.
4. Cetron MS, Chitsulo L, Sullivan JJ, et al. Schistosomiasis in LakeMalawi. Lancet. 1996;348:1274 –1278.
5. Morris W, Knauer M. Cardiopulmonary manifestation of schisto-somiasis. Sem Res Inf. 1997;12:159 –170.
6. Phillips JF, Cockril H, Jorge E, Stiener R. Radiologic evaluation ofpatients with schistosomiasis. Radiology. 1975;114:31–37.
7. Lucas SB, Schwartz DA, Hasleton PS. Parasitic lung disease. In:Spencer H, Hasleton PS, eds. Spencer’s Pathology of the Lung, 5th ed.New York: McGraw-Hill, 1996:327–332.
8. Nash TE, Cheever AW, Ottessen EA, Cook JA. Schistosome infec-tion in humans; perspective and recent findings. Ann Int Med. 1982;97:740 –754.
9. Harnett W, Kusel JR. Increased exposure of parasite antigens at thesurface of adult Schistosoma mansoni exposed to praziquantel invitro. Parasitology. 1986;93:401– 405.
10. Harris AD, Cook GC. Acute schistosomiasis (katayama fever): clin-ical deterioration after chemotherapy. J Infection. 1987;14:159–161.
11. Colebunders R, Verstraeten T, Van Gompel A, et al. Acute schisto-somiasis in travelers returning from Mali. J Travel Med. 1995;2:235–238.
12. Cooke GS, Lavlani A, Gleeson FV, Conlon CP. Acute pulmonaryschistosomiasis in travelers returning from lake Malawi, sub-Sa-haran Africa. Clin Inf Dis. 1999;29:836 – 839.
13. World Health Organization. Atlas of the global distribution ofschistosomiasis. Parasitic disease programme, World Health Orga-nization, 1987.
Pulmonary Manifestations of Early Schistosome Infection/Schwartz et al
722 December 15, 2000 THE AMERICAN JOURNAL OF MEDICINEt Volume 109