Public health emergencies DR. MADHUR VERMA PGIMS ROHTAK
63
Dr. Madhur Verma PG JR II DEPTT OF COMMUNITY MEDICINE
-
Upload
madhur-verma -
Category
Health & Medicine
-
view
204 -
download
1
Transcript of Public health emergencies DR. MADHUR VERMA PGIMS ROHTAK
Dr. Madhur Verma
PG JR II
DEPTT OF COMMUNITY MEDICINE
LEARNING OBJECTIVES
1. Introduction
2. Public health emergency & PHEIC
3. Criteria for decision-making in verification and
notification of public health events.
4. Public health emergency preparedness(PHEP)
5. Situation at the time of emergency
6. Epidemiologic methods at the time of PHE
7. Role of hospitals during a PHE
8. Conclusion
INTRODUCTION
Since beginning of the last decade, near the time
anthrax attacked the world, a substantial amount of money
has been spent by majority of the countries to increase their
ability to prepare for, and respond to, public health
emergencies.
Yet, despite reports suggesting that progress has been
made, it is unclear whether these investments have left
the nation better prepared to respond to a bioterrorist
attack, pandemic influenza, or any other large-scale
public health emergency.
This situation is not because of a shortage of measures
of preparedness. Hence, there arises a need to be
prepared to any kind of such situations dangerous to the
mankind known as public health emergencies.
PUBLIC HEALTH EMERGENCY
PHE is defined as “an emergency need for health care
[medical] services to respond to a disaster, significant
outbreak of an infectious disease, bioterrorist attack or
other significant or catastrophic event.”
The definition is also aligned with the all-hazards approach to
preparedness instead of focusing on a “disaster du jour” and
thus allows for the optimal development of capabilities across
scenarios and better prepares communities for the broad
spectrum of potential risks.
PHIEC – Public Health Emergency
of International Concern
An extraordinary event which is determined, as provided in these Regulations:
i. to constitute a public health risk to other Member States through international spread of disease and
ii. to potentially require a coordinated international response.
The Director General -WHO declares PHEIC
The expansive definitions of "disease", "event", "public
health risk" the IHR (2005) cover a wide range of public
health risks of potential international concern:
• whether biological, chemical or radio nuclear in origin or
source, and
• whether potentially transmitted by:
persons (e.g. SARS, influenza, polio, Ebola),
goods, food, animals (including zoonotic disease risks),
vectors (e.g. plague, yellow fever, West Nile fever), or the
environment (e.g. radio nuclear releases, chemical spills
or
other contamination).

Alert and Response Operations
Detection
Verification
Risk assessment
Response
Events that may constitute a
Public Health Emergency of International Concern need:
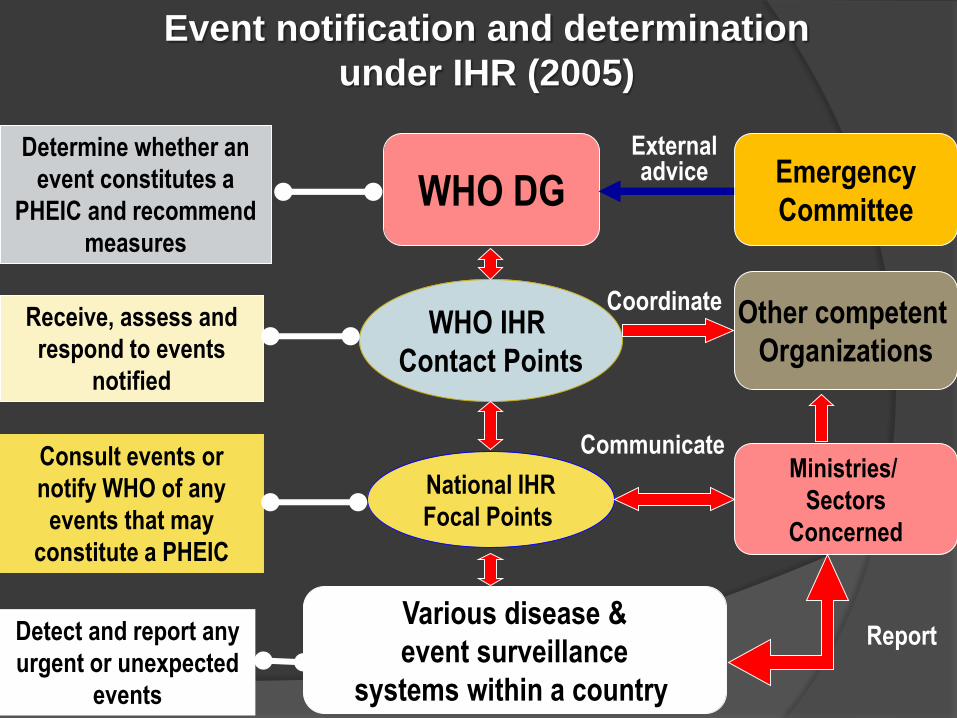
Event notification and determination
under IHR (2005)
WHO DG
Various disease &
event surveillance
systems within a country
National IHR
Focal Points
WHO IHR
Contact Points
Emergency
Committee
Other competent
Organizations
Detect and report any
urgent or unexpected
events
Consult events or
notify WHO of any
events that may
constitute a PHEIC
Receive, assess and
respond to events
notified
Ministries/
Sectors
Concerned
Determine whether an
event constitutes a
PHEIC and recommend
measures
Externaladvice
Coordinate
Communicate
Report
NOTIFICATION
Does not imply that an event is a PHEIC
Just “telling WHO about an event”
No immediate consequences for country
Know about the event from other sources
Start assessing the event without country’s official
notification
8/31/2014 10
Event notification
Any event that may constitute a Public Health Emergency of International Concern (PHEIC)
Within 24 hours of assessment
By the most efficient means of communication
Continue to provide WHO with detailed information
Does NOT mean a real “PHEIC”
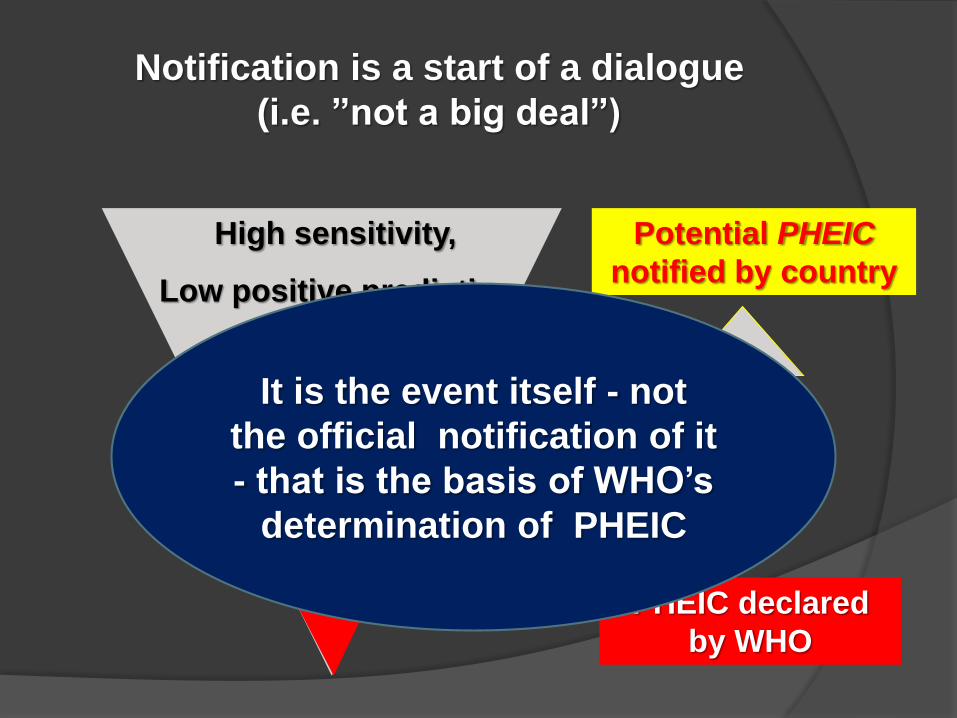
Notification is a start of a dialogue
(i.e. ”not a big deal”)
Potential PHEIC
notified by country
PHEIC declared
by WHO
Dia
log
ue
High sensitivity,
Low positive predictive
value
It is the event itself - not
the official notification of it
- that is the basis of WHO’s
determination of PHEIC
Benefits of early Notification
1. Confidential dialogue
2. IHR protection against unjustified measures
3. Assistance by WHO and other countries
WHO will know sooner or later anyway
8/31/2014 13
Verification of events
Value unofficial sources of information for early alert
WHO requests for verification of potential public health events of international importance
Member States provide initial reply within 24 hours and provision of information
On-site assessment, when necessary
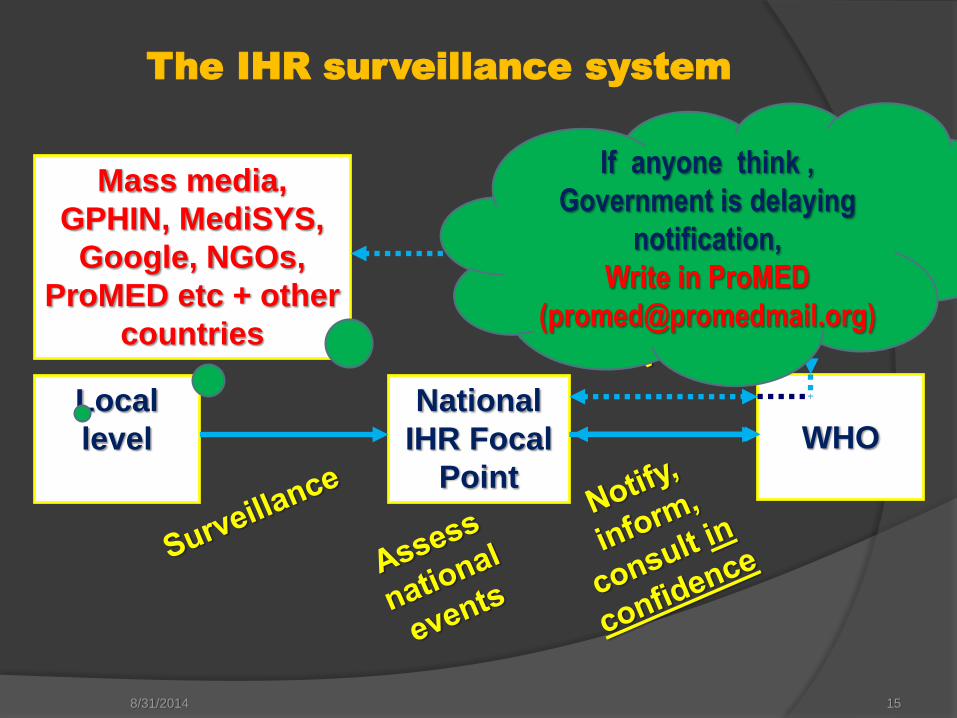
The IHR surveillance system
8/31/2014 15
National
IHR Focal
Point
WHOLocal
level
Mass media,
GPHIN, MediSYS,
Google, NGOs,
ProMED etc + other
countries
If anyone think ,
Government is delaying
notification,
Write in ProMED
Disease List
Four diseases (a single case is notifiable):
Smallpox, Poliomyelitis, human influenza (caused by a
new subtype), SARS
Utilization of the decision instrument:
Cholera, plague, viral haemorrhagic fevers, yellow
fever, …
Diseases of regional concern: dengue fever,
meningococcal diseases…

CONTENTS
INTRODUCTION
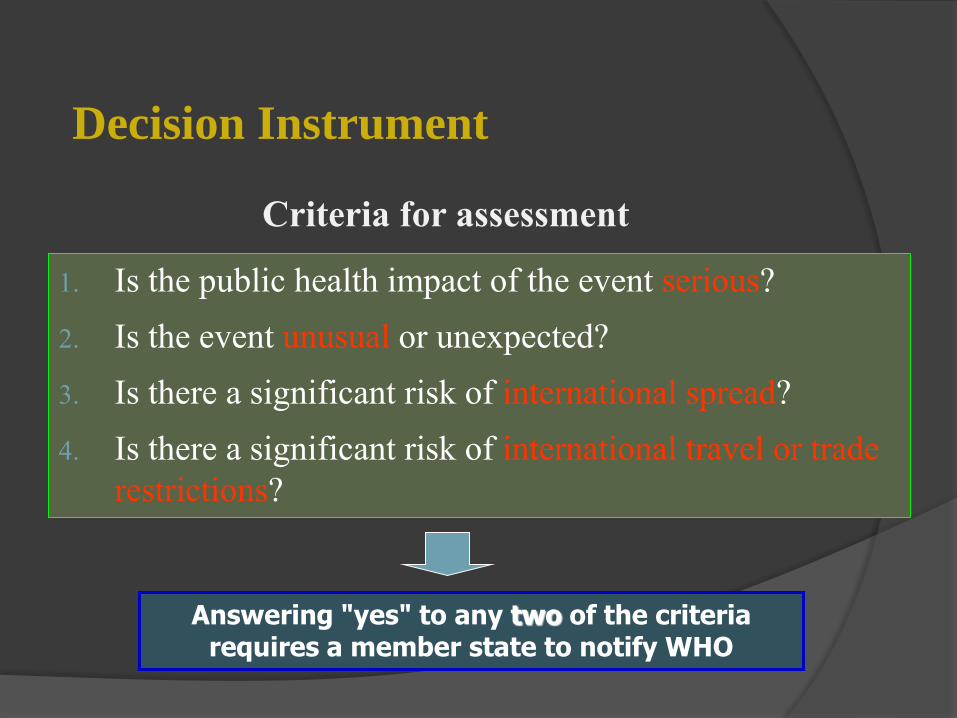
Decision Instrument
1. Is the public health impact of the event serious?
2. Is the event unusual or unexpected?
3. Is there a significant risk of international spread?
4. Is there a significant risk of international travel or trade
restrictions?
Answering "yes" to any two of the criteria requires a member state to notify WHO
Criteria for assessment
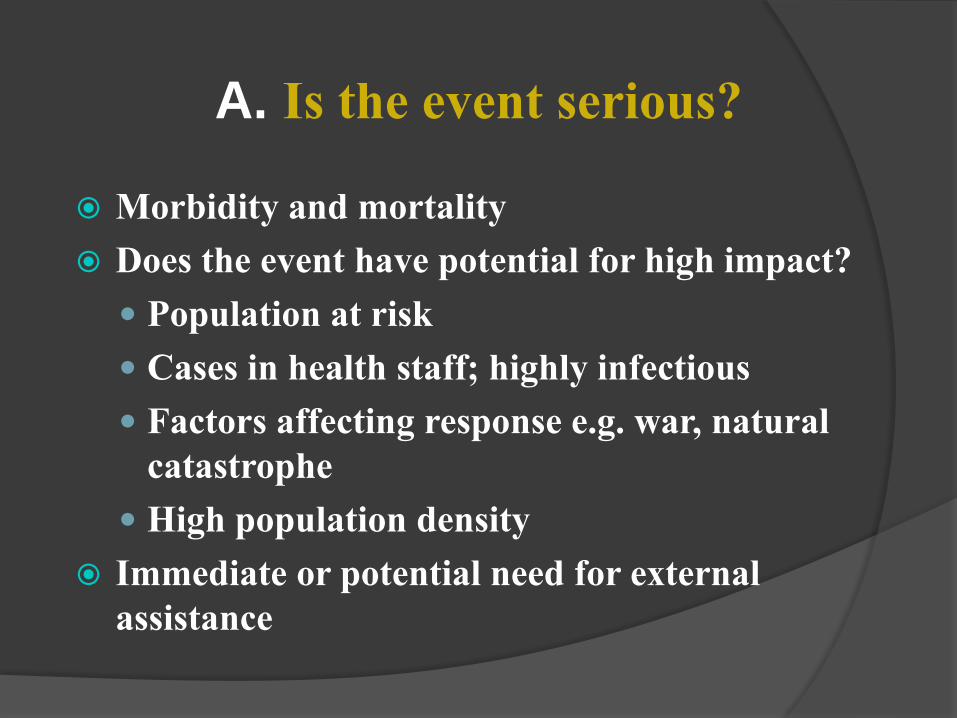
A. Is the event serious?
Morbidity and mortality
Does the event have potential for high impact?
Population at risk
Cases in health staff; highly infectious
Factors affecting response e.g. war, natural
catastrophe
High population density
Immediate or potential need for external
assistance
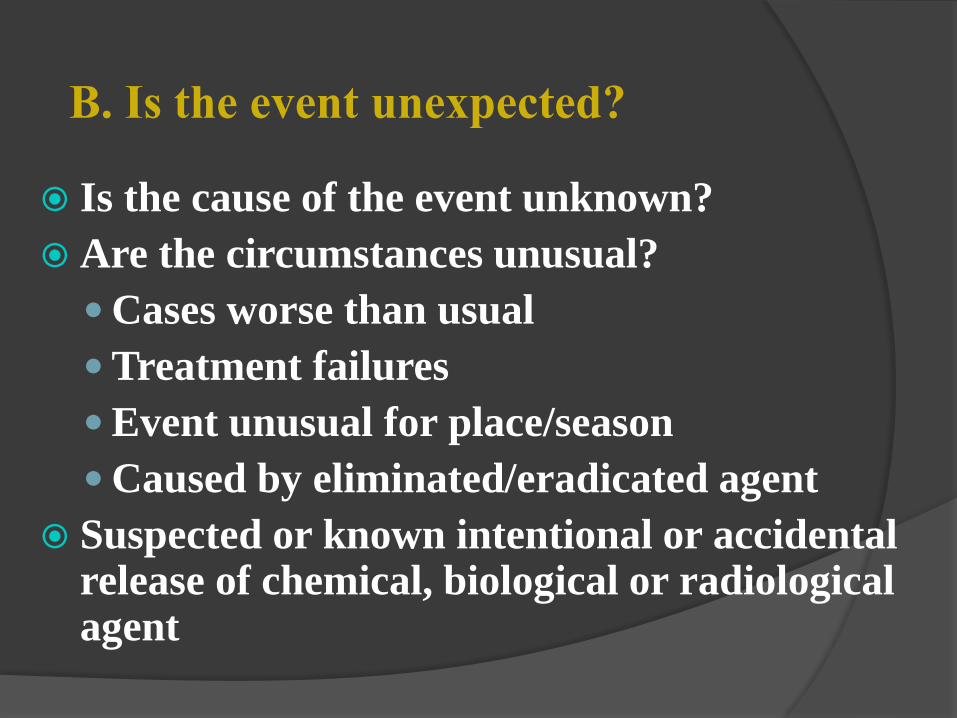
B. Is the event unexpected?
Is the cause of the event unknown?
Are the circumstances unusual?
Cases worse than usual
Treatment failures
Event unusual for place/season
Caused by eliminated/eradicated agent
Suspected or known intentional or accidental release of chemical, biological or radiological agent

C. Is the event likely to spread internationally?
Similar cases in other countries where it was
unexpected?
Factors alerting to cross-border implications?
Caused by epidemic-prone organism
Source suspected/ known to be related to food
import/export
Index case with international travel history
In area with international tourism/ traffic, person or
goods
In border areas with limited capacity for control
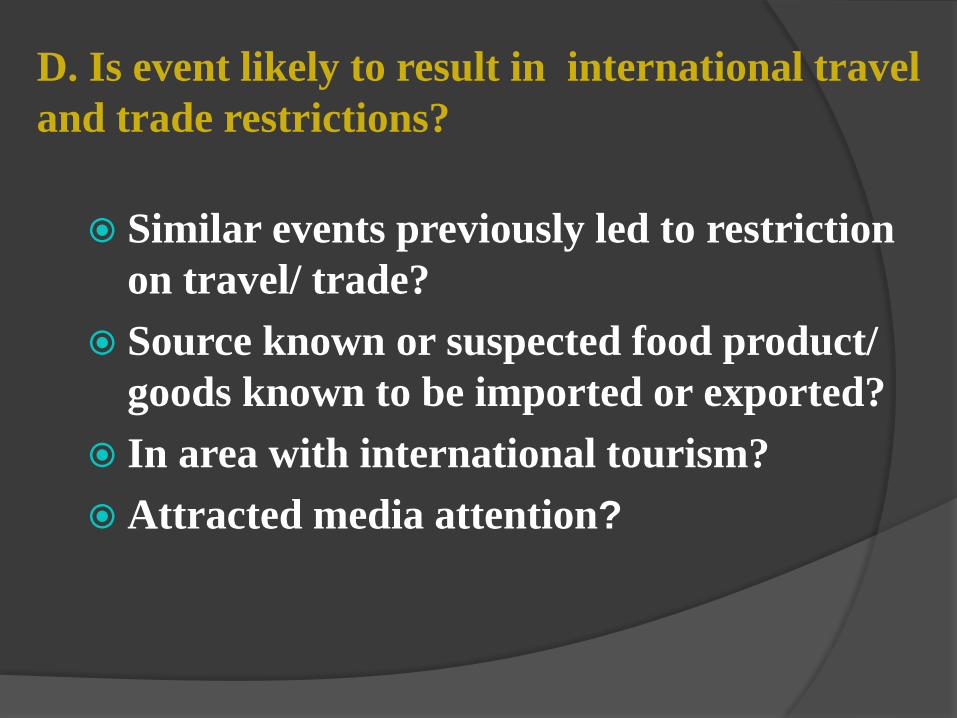
D. Is event likely to result in international travel
and trade restrictions?
Similar events previously led to restriction
on travel/ trade?
Source known or suspected food product/
goods known to be imported or exported?
In area with international tourism?
Attracted media attention?
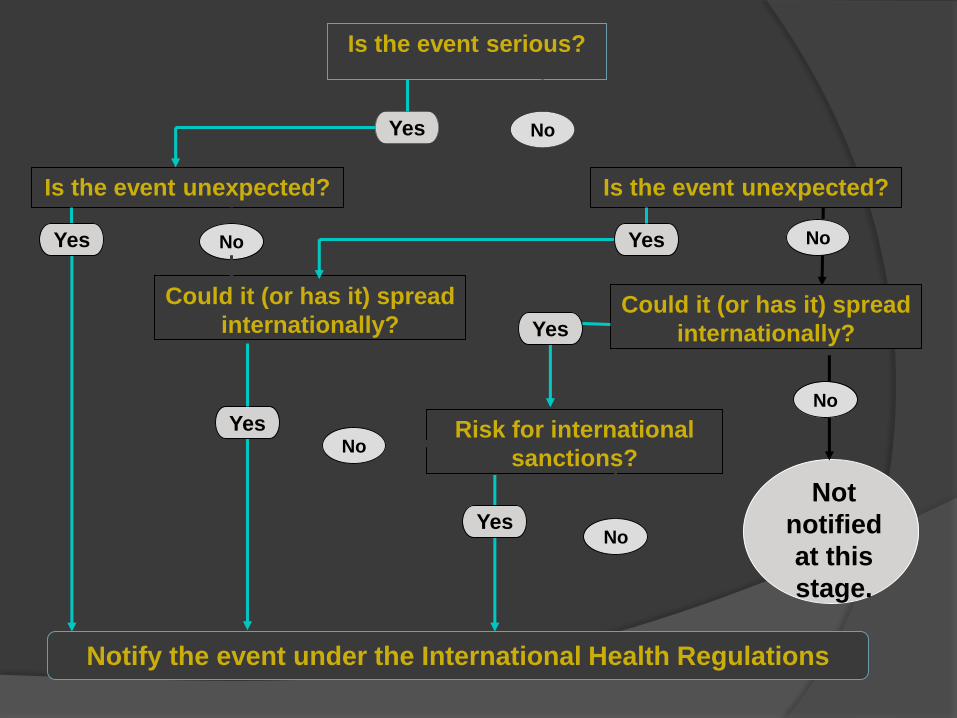
Is the event serious?
Is the event unexpected?
Could it (or has it) spread
internationally?
Risk for international
sanctions?
Not
notified
at this
stage.
No
Notify the event under the International Health Regulations
YesNo
No
No
Is the event unexpected?
Yes
Yes
Yes
Yes
No
Could it (or has it) spread
internationally?Yes
No
Combinations of answers
requiring notification
Serious and unexpected
Serious and risk for international spread
Serious and risk for international
restrictions
Unexpected and risk for international
spread
Unexpected and risk for international
restrictions
Public health threats are always present.
These threats can anytime lead to the onset of public
health incidents.
Being prepared to prevent, respond to, and rapidly
recover from public health threats is critical for protecting
and securing our nation’s public health.
But we face multiple challenges, including an ever-
evolving list of public health threats.
Strong state and local public health systems are the
cornerstone of an effective public health response.
How can we reduce the risk?
Risk reduction can be done in two ways:
A. Preparedness:
B. Mitigation.
PUBLIC HEALTH
EMERGENCY
PREPAREDNESS (PHEP)Preparedness encompasses all those measures taken
before a disaster event which are aimed at
minimizing loss of life,
disruption of critical services and damage when the
disaster occurs.
Thus, preparedness is a protective process which
enables governments, communities and individuals to
respond rapidly to disaster situation and cope with
them effectively.
Preparedness includes
development of emergency response plans
effective warning systems,
maintenance of inventories,
training of manpower etc.
involves a coordinated and continuous process of planning and implementation that relies on measuring performance and taking corrective action.
Mitigation
encompasses all measures taken to reduce both the effect of
hazards itself and the vulnerable conditions in order to reduce
the losses in a future disaster.
Examples of mitigation measures include:
making earthquake resistant buildings,
water management in drought prone areas, management of
rivers to prevent floods etc
PHEP is not a steady state; it requires
continuous improvement, including frequent
testing of plans through drills and exercises and
the formulation and execution of corrective
action plans.
PHEP also includes the practice of improving
the health and resiliency of communities.
ELEMENTS OF PUBLIC HEALTH
EMERGENCY PREPAREDNESS
1. Health risk assessment. Identify the hazards and vulnerabilities (e.g., community health assessment, populations at risk, high-hazard industries, physical structures of importance) that will form the basis of planning.
2. Legal climate. Identify and address issues concerning legal authority and liability barriers to effectively monitor, prevent, or respond to a public health emergency.
3. Roles and responsibilities. Clearly define, assign, and test responsibilities in all sectors, at all levels of government, and with all individuals and ensure each group’s integration.
4. Incident Command System. Develop, test, and improve
decision making and response capability using an
integrated Incident Command System (ICS) at all response
levels.
5. Public engagement. Educate, engage, and mobilize the
public to be full and active participants in PHEP
6. Epidemiology functions. Maintain and improve the
systems to monitor, detect, and investigate potential
hazards, particularly those that are environmental,
radiological, toxic, or infectious.
7. Laboratory functions. Maintain and improve the systems to
test for potential hazards, particularly those that are
environmental, radiological, toxic, or infectious.
8. Countermeasures and mitigation strategies.
Develop, test, and improve community mitigation
strategies (e.g., isolation and quarantine, social
distancing ) and countermeasure distribution strategies
when appropriate.
9. Mass health care. Develop, test, and improve the
capability to provide mass health care services.
10. Public information and communication. Develop,
practice, and improve the capability to rapidly
provide accurate and credible information to the public in
culturally appropriate ways.
11. Robust supply chain. Identify critical resources for public
health emergency response and practice and improve the
ability to deliver these resources throughout the supply chain.
B. Expert and fully staffed workforce1.Operations-ready workers and volunteers.
Develop and maintain a public health and health
care workforce that has the skills and capabilities
to perform optimally in a public health emergency.
2. Leadership. Train, recruit, and develop public
health leaders (e.g., to mobilize resources, engage
the community, develop interagency relationships,
communicate with the public).
C. Accountability and quality improvement
1. Testing operational capabilities. Practice,
review, report on, and improve public health
emergency preparedness by regularly using
real public health events, supplemented with
drills and exercises when appropriate.
2. Performance management Implement a
performance management and accountability
system.
3. Financial tracking Develop, test, and improve
charge capture, accounting, and other financial
systems to track resources and ensure
adequate and timely reimbursement.
Epidemiologic Methods in Disasters
After a disaster (Reconstruction Phase):
Conducting post-disaster epidemiologic follow-up studies
Identifying risk factors for death & injury
Planning strategies & specific interventions to reduce impact-related morbidity &mortality.
Evaluating effectiveness of interventions
Conducting descriptive & analytical studies
Planning medical & public health response to futurEdisasters
Conducting long-term follow-up of rehabilitation /reconstruction activities
AT THE TIME
OF
EMERGENCY
MAJOR AREAS TO BE STRESSED
UPON 1. Health systems and infrastructure
2. Emergency health services
3. Reproductive health care
4. Emergency mental health and psychosocial support
5. Epidemiology and surveillance
6. Control of communicable diseases
7. Water, sanitation and hygiene in emergencies
8. Food and nutrition
9. Management(Financial management for humanitarian response)
Health systems and infrastructure
Essential tasks: prioritizing health services1. Conduct an initial assessment;
2. Identify the major causes of morbidity and mortality;
There are three major sources of disease among the
displaced:
a. Diseases Arising in camps because of unhealthy living
conditions (e.g acute respiratory infections, diarrhoea,
and measles).
The risk of acquiring these diseases is increased by
malnutrition;
b. Within a new environment against which
displaced persons might lack immunity
(e.g., malaria or meningitis);
c. Imported by displaced persons from a previous
environment (e.g. TB,
HIV/AIDS, body lice, parasites) or that is
unique to their population (e.g., sickle cell
disease). These diseases are
usually less common causes of morbidity and
mortality than others
3. Use evidence-based intervention to address major causes of
morbidity and mortality; Triangulate the information collected
in the assessment.
Triangulation is a technique for minimizing biases in the
information collected during the initial assessment
4. Develop a health information system to identify epidemics and guide changes needed in interventions.
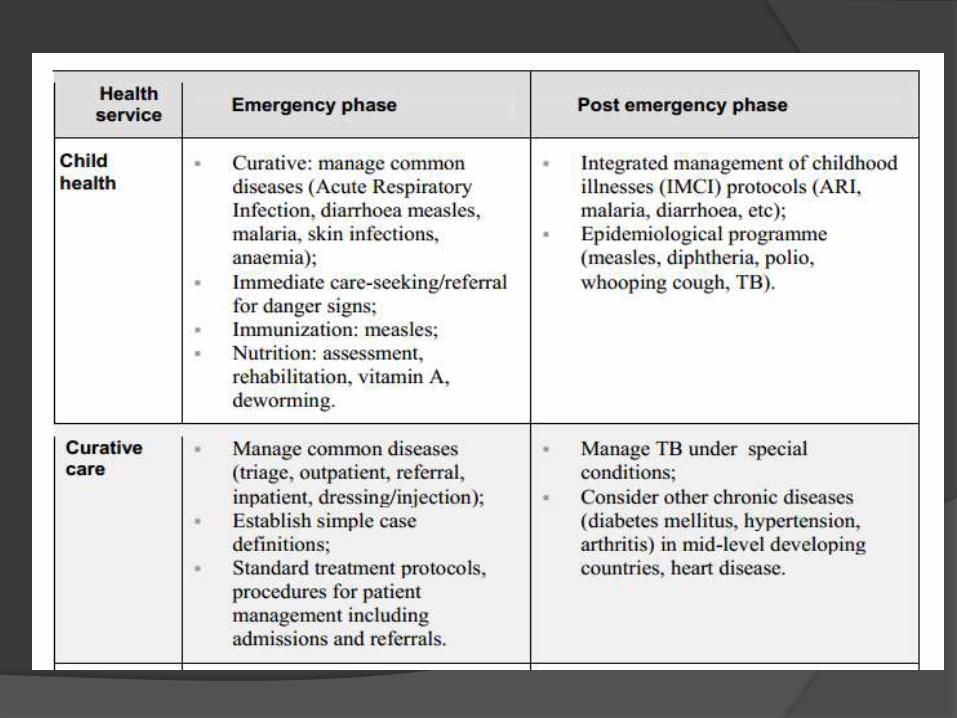
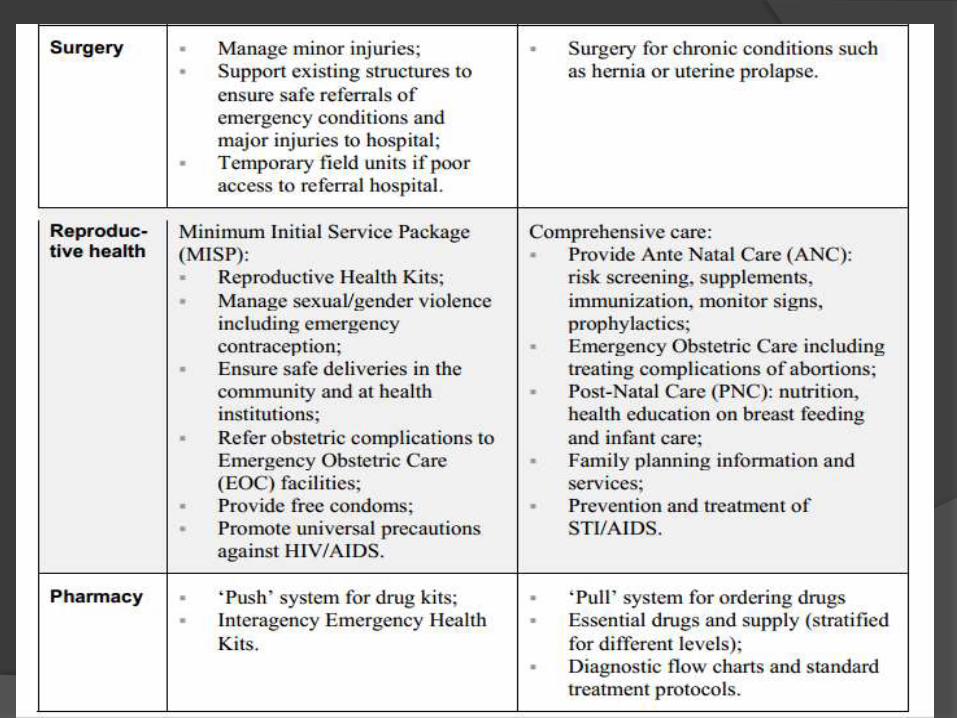
Introduce interventions in phases. Some services must be introduced during the acute
emergency phase while others should be planned but not implemented until the postemergency phase.
Essential tasks:
ensure access to health services
ƒIdentify vulnerable groups and their specific needs;
ƒ Organise services to improve access to vulnerable groups;
ƒ Involve community members and other concerned groups
in the initial assessment and in the design and
development of interventions; and
ƒ Seek women’s views about health problems and ways to
improve health services.
ƒThere is active collaboration with other sectors in the
design and implementation of priority health
interventions, including water and sanitation, food
security, nutrition, shelter and protection.
ƒThe Crude Mortality Rate (CMR) & The Under-Five
Mortality Rate (U5MR) is maintained at, or reduced to,
less than twice the baseline rate documented for the
population prior to the disaster.
Essential tasks: post-
emergency phase
Task 1: Continue to evolve the health
information system and interventions as
indicated
Task 2: Increase capacity of the
community and local health leaders to
design/redesign and implement of health
services
Task 3: Utilise the referral system
established by the lead health authority
Task 4: Whenever possible, base health
services and interventions on
scientifically sound methods
Task 5: Utilise technologies that are
appropriate and socially and culturally
acceptable
Essential tasks: Post-
emergency phase
Task 1: Ensure equity
Task 2: Utilise an inter-sector approach
Task 3: Expand health promotion and
prevention services
Challenges for
Epidemiologists
Applying epidemiologic methods in the context of:
Physical destruction
Public fear
Social disruption
Lack of infrastructure for data collection
Time urgency
Movement of populations
Lack of local support and expertise
Selecting study designs:
Cross-sectional:Studies of frequencies of deaths, illnesses, injuries,adverse health affectsLimited by absence of population counts
Case-control:Best study to determine risk factors, eliminateconfounding, study interactions among multiplefactorsLimited by definition of specific outcomes, issues ofselection of cases & controls
Longitudinal:Studies document incidence and estimate magnitudeof risk Limited by logistics of mounting a study in apost-disaster environment and subject follow-up
Need standardized protocols for data collectionimmediately following disaster
Need standardized terminology, technologies, methodsand procedures
Need operational research to inventory medicalsupplies and determine
1) actual needs,
2) local capacity,
3) needs met by national/international communities
Need evaluation studies to determine efficiency andeffectiveness of relief efforts and emergencyinterventions
Challenges for Epidemiologists Need databases for epidemiologic research based
on existing disaster information systems
Need to identify injury prevention interventions
Need to improve timely and appropriate medical care following disaster (search & rescue, emergency medical services, importing skilled providers, evacuating the injured)
Need measures to quickly reestablish local health care system at full operating capacity soon after disaster
Challenges for Epidemiologists
Need uniform disaster-related injury definitions and classification scheme
Need investigations of disease transmission following disasters and public health measures to mitigate disease risk
Need to study problems associated with massive influx of relief supplies and relief personnel
Need cost-benefit and cost-effectiveness analyses
Role of Hospitals in Disasters/PHE
Hospitals are central to provide emergency
care when a disaster strike the society.
What constitutes a disaster/PHE for a
hospital?
Whenever a hospital or a health care facility is confronted
by a situation where it has to provide care to a large
number of patients in limited time, which is beyond its
normal capacity, constitute a disaster for the said hospital.
In others words when the resources of the hospitals are
over-whelmed beyond its normal capacity and additional
contingency measure are required to control the event, the
hospital can be said to be in a disaster situation.
Assessment of the capacity of a hospital to respond to a
given emergency situation can be assessed by the following
two ways:
Hospital Treatment Capacity (HTC), is defined as the
number of casualties that can be treated in the hospital in
an hour and is usually calculated as 3% of total number of
beds
Hospital Surgical Capacity (HSC) is Hospital Surgical
Capacity (HSC) the number of seriously injured patients
that can be operated upon within a 12-hour period i.e.
HSC= Number of operation rooms x 7x 0.25 operations/12
hrs.
A. Based on the Number of Casualties
( for 1000
bedded 30 hospital)
According To WHO: The Mass Casualty Emergencies
can be categorized in one of the following ways:
Category 1 : Up to thirty patients
belonging to a single accident or
any other emergency, coming to a
hospital casualty at one time.Category 2: Thirty to fifty patients
Category 3: More than fifty patients
Categorisation Of Patients Based on TYPE OF
CASUALTIES:
Category A: Patients in critical condition
Category B: Patients in serious but not life threatening
condition
Category C: Walking , but wounded.
Categorization of the CONTINGENCY PLAN into three classes :
Class A: The plan can be put into practice withoutany disruption to the normal and routine work of theinstitution.
Class B:The plan can be put into practice with minordisruption to the day to day functioning of the hospitaland with some readjustments. The plan may beupgraded to C if the numbers of casualties increase.
Class C:There would be definite disruption of routinework. Major readjustments would be required inhospital
functioning, inpatient treatment, duty arrangements
Organization of Health Delivery System in Disaster/ Emergency situations
Pre-Hospital Management:: To render first aid to victims at the spot of disaster and their transportation to nearby
hospital as an essential part of life saving measures.
a) First aid Parties & Posts(static and mobile)
b) Ambulance service
c) Mobile Surgical Units.
Emergency Hospital Organization
a) Emergency Hospital Services (including critical care facilities)
b) Emergency Surgical Services
c) Emergency Transfusion Services
CONCLUSION
The absence of a clear definition of PHEP makes it
difficult to determine whether the nation is better prepared
to respond to a bioterrorist attack or major disease
outbreak now than it was nearly a decade ago.
Moreover, without an agreed-upon definition,
policymakers and other stakeholders will continue to
struggle to determine what it will take to get ready for
such attacks and outbreaks , as well as how to prioritize
future investments.
The definition presented here provides a concise, broadly
applicable vision of what a prepared community looks like,
along with a short list of actionable and measurable steps
for attaining that vision.
At the most general level, the definition and action-
oriented elements can help provide a set of shared terms
for discussion among various governmental and
nongovernmental actors about what exactly is involved in
enhanced community preparedness.

THANK YOU