Public Health Detailing of Primary Care ProvidersDigital+Assets/Provost/... · Public Health...
13
Public Health Detailing of Primary Care Providers New York City’s Experience, 2003–2010 Michelle G. Dresser, MPH, Leslie Short, MPH, Laura Wedemeyer, BA, Victoria Lowerson Bredow, MPH, Rachel Sacks, MPH, Kelly Larson, MPH, Joslyn Levy, MPH, BSN, Lynn D. Silver, MD, MPH Background: Given evidence of widespread underuse of recommended clinical preventive services and chronic disease management, New York City developed the Public Health Detailing Program, a primary care provider outreach initiative to increase uptake of best practices on public health priorities. Purpose: The goal of the study was to evaluate the effectiveness of the Public Health Detailing Program in helping primary care providers and their staff to improve patient care on public health challenges. Methods: An analysis was conducted of reported changes in clinical practice or behavior by examining providers’ retention and implementation of recommendations for campaigns. Results: During each campaign, 170 to 443 providers and 136 to 221 sites were reached. Among providers who responded to questions on changes in their practice behavior, the following signifıcant increases occurred from baseline to follow-up. Screening for clinical preventive services increased, including routinely screening for intimate partner violence (14%– 42%). Clinical management in- creased, such as prescribing longer-lasting supplies of medicine (29%– 42%). Lifestyle modifıcation and behavior change, such as recommending increased physical activity to patients with high cholesterol levels, rose from 52% to 73%. Self-management goal-setting with patients increased, such as using a clinical checkbook to track hemoglobin HbA1c goals (28% to 43%). Conclusions: Data suggest that public health detailing can be effective for linking public health agencies and their recommendations to providers and influencing changes in clinical practice behavior. (Am J Prev Med 2012;42(6S2):S122–S134) © 2012 Published by Elsevier Inc. on behalf of American Journal of Preventive Medicine T he Public Health Detailing Program within the New York City Department of Health and Mental Hygiene (DOHMH) has worked closely with pri- mary care providers and their staff since 2003 to improve patient care by addressing the leading, largely prevent- able, causes of illness, disability, and death. Drawing on evidence indicating that gaps in provider knowledge and the absence of offıce systems contribute to suboptimal care, the Public Health Detailing Program was designed to address these and other issues of care delivery. 1 Public health detailing focuses on neighborhoods facing the greatest health disparities and is part of New York City’s approach to reduce the disproportionate burden of poor health. Public health detailing initiatives center on clinical topics chosen for their anticipated effect on morbidity and mortality and other public health priorities. Al- though the focus is on managing chronic conditions, the program has “detailed” issues ranging from intimate partner violence screening to recruitment for the New York City Medical Reserve Corps, promoting the imple- mentation and use of electronic health records, support- ing exclusive breastfeeding, and improving medication adherence in patients with cardiovascular disease and diabetes. Public health detailing develops its campaigns From the Bureau of Chronic Disease Prevention and Control, New York City Department of Health and Mental Hygiene, New York, New York Address correspondence to: Michelle G. Dresser, MPH, Bureau of Chronic Disease Prevention and Tobacco Control, New York City Depart- ment of Health and Mental Hygiene, 42-09 28 St, CN-46, Queens, NY 11101. E-mail: [email protected]. 0749-3797/$36.00 http://dx.doi.org/10.1016/j.amepre.2012.03.014 S122 Am J Prev Med 2012;42(6S2):S122–S134 © 2012 Published by Elsevier Inc. on behalf of American Journal of Preventive Medicine
-
Upload
phungkhanh -
Category
Documents
-
view
216 -
download
1
Transcript of Public Health Detailing of Primary Care ProvidersDigital+Assets/Provost/... · Public Health...
mpaetc
Public Health Detailingof Primary Care Providers
New York City’s Experience, 2003–2010
Michelle G. Dresser, MPH, Leslie Short, MPH, Laura Wedemeyer, BA,Victoria Lowerson Bredow, MPH, Rachel Sacks, MPH, Kelly Larson, MPH,
Joslyn Levy, MPH, BSN, Lynn D. Silver, MD, MPH
Background: Given evidence of widespread underuse of recommended clinical preventive servicesand chronic disease management, New York City developed the Public Health Detailing Program, aprimary care provider outreach initiative to increase uptake of best practices on public healthpriorities.
Purpose: The goal of the study was to evaluate the effectiveness of the Public Health DetailingProgram in helping primary care providers and their staff to improve patient care on public healthchallenges.
Methods: An analysis was conducted of reported changes in clinical practice or behavior byexamining providers’ retention and implementation of recommendations for campaigns.
Results: During each campaign, 170 to 443 providers and 136 to 221 sites were reached. Amongproviderswho responded to questions on changes in their practice behavior, the following signifıcantincreases occurred from baseline to follow-up. Screening for clinical preventive services increased,including routinely screening for intimate partner violence (14%–42%). Clinical management in-creased, such as prescribing longer-lasting supplies of medicine (29%–42%). Lifestyle modifıcationand behavior change, such as recommending increased physical activity to patients with highcholesterol levels, rose from 52% to 73%. Self-management goal-setting with patients increased, suchas using a clinical checkbook to track hemoglobin HbA1c goals (28% to 43%).
Conclusions: Data suggest that public health detailing can be effective for linking public healthagencies and their recommendations to providers and influencing changes in clinical practicebehavior.(Am J Prev Med 2012;42(6S2):S122–S134) © 2012 Published by Elsevier Inc. on behalf of American Journal ofPreventive Medicine
hgah
tatppYmia
The Public Health Detailing Program within theNew York City Department of Health andMentalHygiene (DOHMH) has worked closely with pri-
ary care providers and their staff since 2003 to improveatient care by addressing the leading, largely prevent-ble, causes of illness, disability, and death. Drawing onvidence indicating that gaps in provider knowledge andhe absence of offıce systems contribute to suboptimalare, the Public Health Detailing Program was designed
From the Bureau of Chronic Disease Prevention and Control, New YorkCity Department of Health and Mental Hygiene, New York, New York
Address correspondence to: Michelle G. Dresser, MPH, Bureau ofChronic Disease Prevention and Tobacco Control, New York City Depart-ment of Health and Mental Hygiene, 42-09 28 St, CN-46, Queens, NY11101. E-mail: [email protected].
d0749-3797/$36.00http://dx.doi.org/10.1016/j.amepre.2012.03.014
S122 Am J PrevMed 2012;42(6S2):S122–S134 ©2012Publishe
to address these and other issues of care delivery.1 Publicealth detailing focuses on neighborhoods facing thereatest health disparities and is part of New York City’spproach to reduce the disproportionate burden of poorealth.Public health detailing initiatives center on clinical
opics chosen for their anticipated effect on morbiditynd mortality and other public health priorities. Al-hough the focus is on managing chronic conditions, therogram has “detailed” issues ranging from intimateartner violence screening to recruitment for the Nework City Medical Reserve Corps, promoting the imple-entation and use of electronic health records, support-
ng exclusive breastfeeding, and improving medicationdherence in patients with cardiovascular disease and
iabetes. Public health detailing develops its campaignsdbyElsevier Inc. on behalf ofAmerican Journal of PreventiveMedicine

totDmau
csrpt
smigtgap
Dbr
foaoacsiw
“stac
tpapap
srciptc
ncV
Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134 S123
J
in collaboration with internal and external clinicalexperts.The program strives to improve primary care physi-
cian practice through one-on-one visits, or “detailing,” awell-known and successful strategy usually associatedwith the pharmaceutical industry.2,3 Whereas most pub-lic health interventions in the primary care setting focuson one condition or disease over time, public health de-tailing has developed a standard methodology for thedelivery of a variety of public health messages. Highlytrained health department representatives promote evi-dence-based, clinical preventive services and chronic dis-ease management by delivering brief, targeted messagesto the entire clinical care team of physicians, physicianassistants, nurse practitioners, nurses, administrators,and other staff.2,4
Through its campaigns, public health detailing sup-ports providers and their staff by (1) outlining and dis-cussing evidence-based key recommendations tailored tospecifıc clinical interventions, (2) providing informationon new public health policies or practice guidelines, and(3) assessing readiness to adopt key recommendationsand supporting clinical tools that best suit the practice.3
The Public Health Detailing Program’s “Action Kits”contain clinical tools, provider resources, and patienteducation materials to promote evidence-based best-practices recommended by the DOHMH, which are thefocus of discussion during offıce visits by representatives.The current paper outlines the results of evaluations from20 different campaigns.
MethodsBetween October 2003 and 2010, the Public Health Detailing Pro-gram completed a total of 49 campaigns. Public Health Detailingused survey data of the leading health indicators by ZIP code toprioritize the geographic areas of East and Central Harlem, SouthBronx, and North and Central Brooklyn as target areas for itscampaigns, although some were expanded citywide. After workinginitially from a list of Medicaid providers, Public Health Detailingsought to identify and subsequently detail all primary care provid-ers working in these geographic areas. Evidence showed that resi-dents in these neighborhoods were more likely than other NewYorkers to have asthma, cancer, HIV/AIDS, diabetes, and heartdisease and to be overweight or obese. These target neighborhoodsare the primary geographic focus of many DOHMH programs.5
The Public Health Detailing Program uses highly trainedHealthDepartment representatives to deliver consistent and repeat mes-saging to providers.3 All representatives are expert communica-ors, andmost have graduate degrees or experience in public healthr are health professionals. Preceding each campaign, representa-ives undergo an intensive week-long training, with expertOHMH faculty, to ensure profıciency in clinical content, com-unicating recommendations and materials, overcoming barriersnd objections, and documentation for evaluation. Representatives
sually visit providers three or four times a year with different eune 2012
ampaigns, so they can develop relationships with them and theirtaff and are seen as a valuable resource from the DOHMH. Thiselationship-building fosters open communication channels andromotes the DOHMH and its resources to providers. No mone-ary incentives were offered for participation.Each representative is assigned between 35 and 45 primary care
ites. A new campaign is implemented approximately every 3 to 4onths and typically lasts 10 to 14weeks.Most campaigns focus on
nternal medicine and family practices; however, some have tar-eted others depending on the topic. For example, the Contracep-ion campaign was expanded to include obstetricians, gynecolo-ists, and pharmacists; the Identifying and Reporting Child Abusend Neglect campaign was limited to family and pediatricractices.The core costs of personnel are covered by the Public Healthetailing Program, but many campaign expenditures are coveredy grants or other DOHMH bureaus, which the program collabo-ates with to improve its sustainability.The Public Health Detailing Program’s communication strategy
ocuses on all staff in the practice—“the total offıce call”—a meth-dology shown to have a positive effect on chronic disease man-gement, testing, and screening.2,3 Campaign messaging centersn key recommendations developed by DOHMH clinical expertsnd is usually limited to amaximumof three recommendations perampaign topic. Key recommendations provide the basis for as-essment questions for evaluation. Representatives are trained tontegrate the recommendations verbatim into their interactionsith providers and staff at each visit.During visits, representatives promote the graphically appealing
Action Kits,” which contain printed clinical tools, provider re-ources, and patient education materials and are designed to havehe look, feel, and quality of a commercially developed product sos to compete with private industry materials (Figure 1).2 The kitontents address the six components of the Chronic Care Model6
in support of informed clinical decision-making, enhanced patientself-management, improved delivery-system design, expanded useof clinical information systems, increased collaboration with com-munity organizations, and heightened understanding of healthsystem issues pertinent to the topic detailed.During each campaign, representatives visit providers and staff
at their assigned sites at least two times.7,8 At these visits, represen-atives introduce and reinforce the key recommendations and cam-aign materials as well as answer any questions from the care teambout the campaign. Representatives collect survey data by askingroviders an identical short set of assessment questions at initialnd follow-up visits. Responses help representatives tailor theirresentation to align with providers’ interests and needs.In addition to the two standard visits, representatives often visit
ites to deliver current and past campaign materials or fulfıll otherequests, such as providing supplemental influenza and pneumo-occal vaccines. Multiple visits to the entire offıce team are anntegral part of the Public Health Detailing Model, providing op-ortunities to reinforce key recommendations, ensuring consis-ency of campaign messaging, and developing relationships withare teams.Of the 24 campaigns carried out in the priority underservedeighborhoods from 2003 to 2010, 20 were studied. Those ex-luded from the analysis were four Influenza and Pneumococcalaccination campaigns, which consisted of only one visit. Provid-
rs’ retention and implementation of key recommendations for
iit
tttmgupttm
rtDfawpaaes
gtYftnmtDequ
S124 Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134
every campaign are evaluated through responses to the assessmentquestions. Changes in clinical practice or behavior aremeasured byproviders’ self-reported status from initial to follow-up visit. At thebeginning of each initial face-to-face visit, representatives reciteassessment questions to providers. At follow-up visits, usually 4 to6 weeks later, representatives attempt to conduct a second assess-mentwith all providers initially visited.Questions are posed to onlylicensed prescribers (physicians, nurse practitioners, and physicianassistants) because they are usually the decision-makers to imple-ment key recommendations and system changes in the practice.On average, three or four assessment questions are designed for
every campaign. The provider is not given a list of answer choices toselect from; rather, he or she states to the representative his or herpractice behavior, and answers are coded in predetermined catego-ries, including “other,” so that all possible answers can be captured.Representatives receive training and practice to code and evaluateeach visit before the campaign begins.Typically, the fırst assessment question examines the hoped-for
effectiveness and uptake of individual campaigns by askingwhether providers use specifıc guidelines for screening or how theyimplement recommended strategies for chronic disease manage-ment. A second question usually determines how providers iden-tify specifıc populations for particular interventions, such as influ-enza and pneumococcal vaccination or screening all patients forintimate partner (domestic) violence. In many campaigns, a third
MEDICATIONADHERENCE
A C T I O N K I TFor HealthCare Providers
and Pharmacists
Helppatients control hypertension,high cholesteroland diabetes
Figure 1. New York City Public Health Detailing ProgramMedication Adherence Action Kit coverNote: Reprinted with permission from the New York City Department of Healthand Mental Hygiene (Copyright 2010).
assessment question explores providers’ choice of standard screen-
ng or testing tools related to the campaign content. Although thiss the standard methodology used to develop the assessment ques-ions, each campaign has its own unique needs.In addition to these questions, representatives ask providers
heir level of adoption or readiness to adopt the key recommenda-ions by obtaining a commitment from the practitioners. Commit-ing to one or more of the DOHMH evidence-based key recom-endations is voluntary on the part of the medical provider and isauged by self-report. Representatives record intended or adoptedse of Public Health Detailing Program Action Kit clinical tools,rovider resources, and patient educationmaterials. They also ratehe receptiveness of providers and staff to the key recommenda-ions and materials on a 6-point scale ranging from “refusal toeet” to “adopted clinical tool(s)/key recommendations.”Representatives record visit data, including assessment question
esponses,material use, and rating scale, on a paper visit record andhen enter them into an electronic database, allowing PublicHealthetailing to analyze campaign data, track campaign reach andrequency, and gauges providers’ interest in the topic and materi-ls. Statistical analysis of the assessment questions is conductedith SPSS 17.0. Chi-square tests are used to determine providerractice change between initial and follow-up visits. The visit datalso include practice information, clinician and staff descriptions,nd visit details. Representatives also record qualitative notes forach visit, observed best practices, and any other comments anduggestions for the Public Health Detailing Program.In addition to the detailing visit, Public Health Detailing Pro-
ram staff collect order information from the DOHMH’s call cen-er, which distributes agency-produced literature throughout Nework City free of charge. With each campaign, select materialsrom the Action Kit are made available through the call center sohat providers and their staff can call to replenish their supply aseeded. Data are specifıcally collected on these materials to deter-inewho is ordering them,whichmaterials are being ordered, and
he quantity and frequency of orders. These data help PublicHealthetailing know which materials continue to be used by practicesven after a campaign ends. A fınal campaign report containing alluantitative and relevant qualitative data is generated and distrib-ted to key stakeholders throughout the DOHMH.
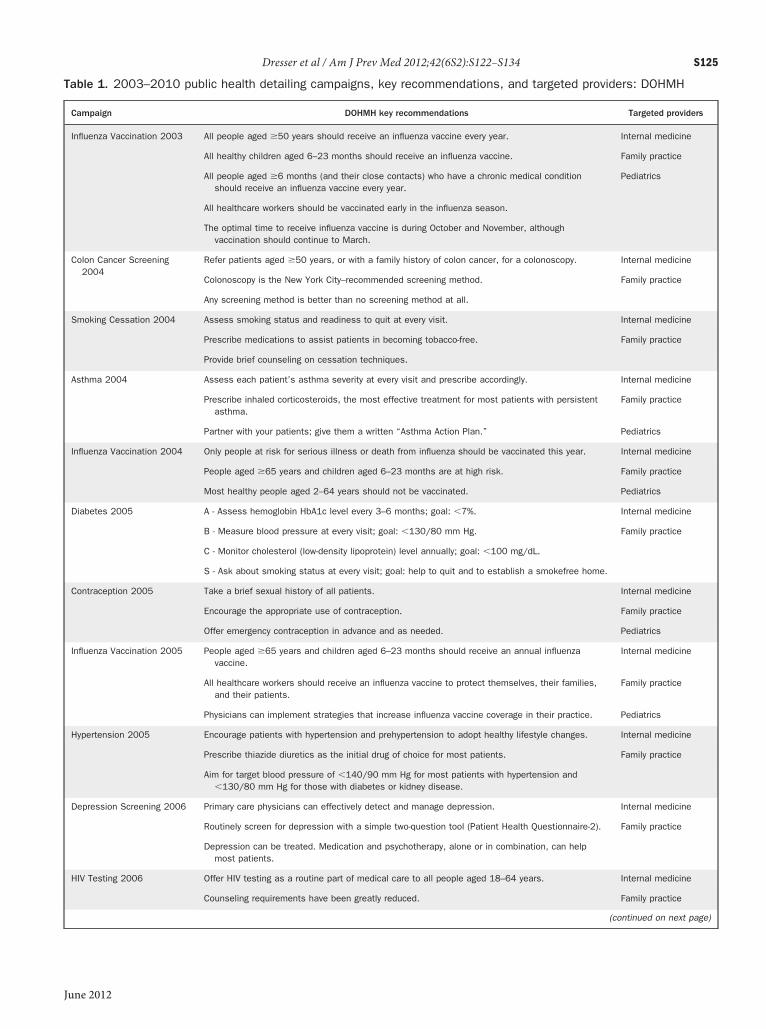
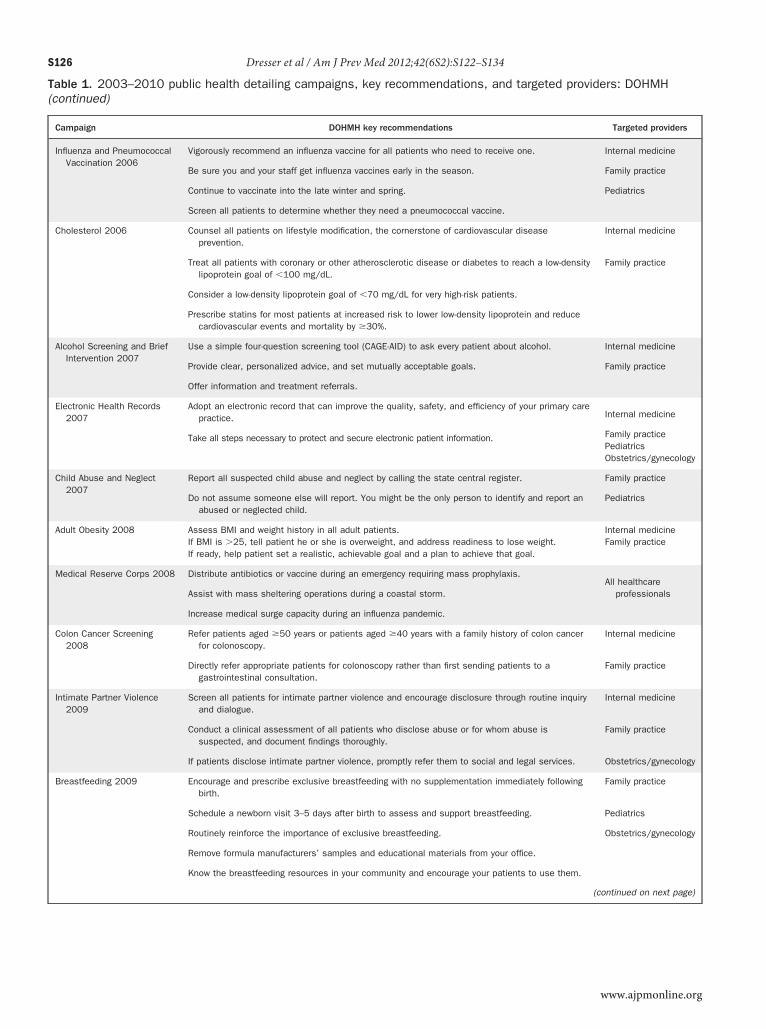
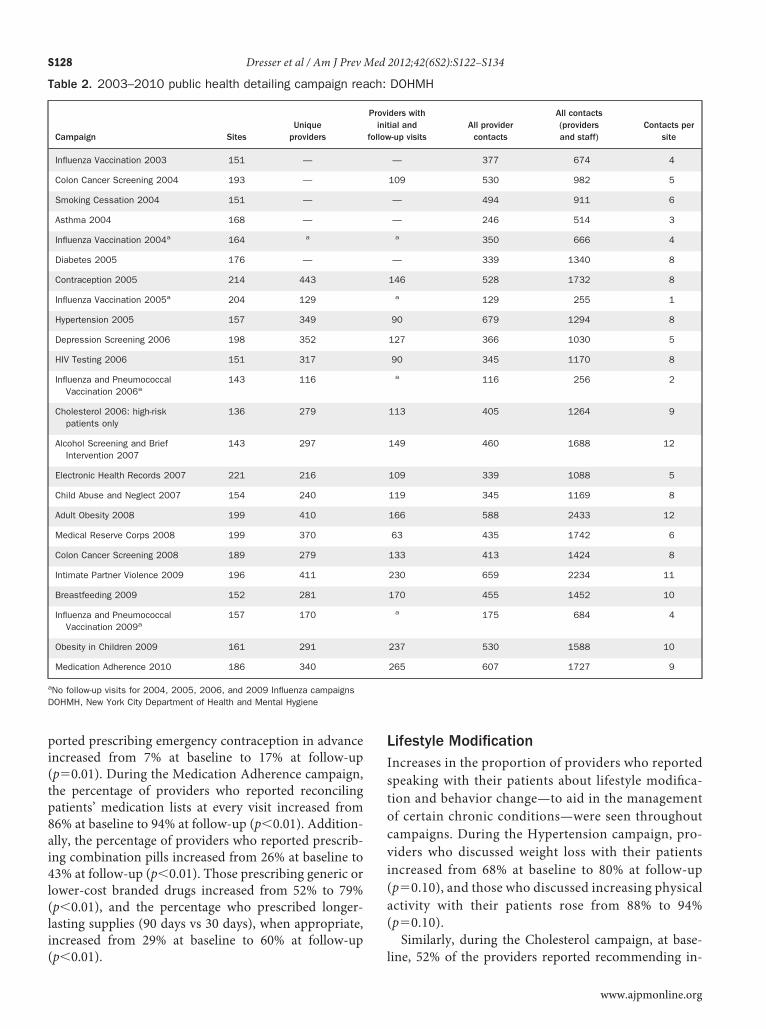
ResultsAll 24 campaigns implemented between 2003 and 2010 inour high-risk neighborhoods and their associated keyrecommendations are outlined in Table 1. The 20 indi-vidual campaigns analyzed for this article reached be-tween 136 and 221 clinical sites, and representatives“detailed” between 170 and 443 providers per cam-paign. In Table 2, the “All Provider Contacts” and “AllContacts (Providers and Staff)” columns indicate thetotal number of detailing visits (initial and follow-upvisits) during the campaign with providers only andwith providers and offıce staff together, respectively.Among all providers who received an initial campaignvisit, on average 45% received a follow-up visit duringthe same campaign (2005–2007: 38% follow-up rate;
2008–2010: 53% follow-up rate).www.ajpmonline.org
Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134 S125
Table 1. 2003–2010 public health detailing campaigns, key recommendations, and targeted providers: DOHMH
Campaign DOHMH key recommendations Targeted providers
Influenza Vaccination 2003 All people aged �50 years should receive an influenza vaccine every year. Internal medicine
All healthy children aged 6–23 months should receive an influenza vaccine. Family practice
All people aged �6 months (and their close contacts) who have a chronic medical conditionshould receive an influenza vaccine every year.
Pediatrics
All healthcare workers should be vaccinated early in the influenza season.
The optimal time to receive influenza vaccine is during October and November, althoughvaccination should continue to March.
Colon Cancer Screening2004
Refer patients aged �50 years, or with a family history of colon cancer, for a colonoscopy. Internal medicine
Colonoscopy is the New York City–recommended screening method. Family practice
Any screening method is better than no screening method at all.
Smoking Cessation 2004 Assess smoking status and readiness to quit at every visit. Internal medicine
Prescribe medications to assist patients in becoming tobacco-free. Family practice
Provide brief counseling on cessation techniques.
Asthma 2004 Assess each patient’s asthma severity at every visit and prescribe accordingly. Internal medicine
Prescribe inhaled corticosteroids, the most effective treatment for most patients with persistentasthma.
Family practice
Partner with your patients; give them a written “Asthma Action Plan.” Pediatrics
Influenza Vaccination 2004 Only people at risk for serious illness or death from influenza should be vaccinated this year. Internal medicine
People aged �65 years and children aged 6–23 months are at high risk. Family practice
Most healthy people aged 2–64 years should not be vaccinated. Pediatrics
Diabetes 2005 A - Assess hemoglobin HbA1c level every 3–6 months; goal: �7%. Internal medicine
B - Measure blood pressure at every visit; goal: �130/80 mm Hg. Family practice
C - Monitor cholesterol (low-density lipoprotein) level annually; goal: �100 mg/dL.
S - Ask about smoking status at every visit; goal: help to quit and to establish a smokefree home.
Contraception 2005 Take a brief sexual history of all patients. Internal medicine
Encourage the appropriate use of contraception. Family practice
Offer emergency contraception in advance and as needed. Pediatrics
Influenza Vaccination 2005 People aged �65 years and children aged 6–23 months should receive an annual influenzavaccine.
Internal medicine
All healthcare workers should receive an influenza vaccine to protect themselves, their families,and their patients.
Family practice
Physicians can implement strategies that increase influenza vaccine coverage in their practice. Pediatrics
Hypertension 2005 Encourage patients with hypertension and prehypertension to adopt healthy lifestyle changes. Internal medicine
Prescribe thiazide diuretics as the initial drug of choice for most patients. Family practice
Aim for target blood pressure of �140/90 mm Hg for most patients with hypertension and�130/80 mm Hg for those with diabetes or kidney disease.
Depression Screening 2006 Primary care physicians can effectively detect and manage depression. Internal medicine
Routinely screen for depression with a simple two-question tool (Patient Health Questionnaire-2). Family practice
Depression can be treated. Medication and psychotherapy, alone or in combination, can helpmost patients.
HIV Testing 2006 Offer HIV testing as a routine part of medical care to all people aged 18–64 years. Internal medicine
Counseling requirements have been greatly reduced. Family practice
(continued on next page)
June 2012
S126 Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134
Table 1. 2003–2010 public health detailing campaigns, key recommendations, and targeted providers: DOHMH(continued)
Campaign DOHMH key recommendations Targeted providers
Influenza and PneumococcalVaccination 2006
Vigorously recommend an influenza vaccine for all patients who need to receive one. Internal medicine
Be sure you and your staff get influenza vaccines early in the season. Family practice
Continue to vaccinate into the late winter and spring. Pediatrics
Screen all patients to determine whether they need a pneumococcal vaccine.
Cholesterol 2006 Counsel all patients on lifestyle modification, the cornerstone of cardiovascular diseaseprevention.
Internal medicine
Treat all patients with coronary or other atherosclerotic disease or diabetes to reach a low-densitylipoprotein goal of �100 mg/dL.
Family practice
Consider a low-density lipoprotein goal of �70 mg/dL for very high-risk patients.
Prescribe statins for most patients at increased risk to lower low-density lipoprotein and reducecardiovascular events and mortality by �30%.
Alcohol Screening and BriefIntervention 2007
Use a simple four-question screening tool (CAGE-AID) to ask every patient about alcohol. Internal medicine
Provide clear, personalized advice, and set mutually acceptable goals. Family practice
Offer information and treatment referrals.
Electronic Health Records2007
Adopt an electronic record that can improve the quality, safety, and efficiency of your primary carepractice.
Take all steps necessary to protect and secure electronic patient information.
Internal medicine
Family practicePediatricsObstetrics/gynecology
Child Abuse and Neglect2007
Report all suspected child abuse and neglect by calling the state central register. Family practice
Do not assume someone else will report. You might be the only person to identify and report anabused or neglected child.
Pediatrics
Adult Obesity 2008 Assess BMI and weight history in all adult patients.If BMI is �25, tell patient he or she is overweight, and address readiness to lose weight.If ready, help patient set a realistic, achievable goal and a plan to achieve that goal.
Internal medicineFamily practice
Medical Reserve Corps 2008 Distribute antibiotics or vaccine during an emergency requiring mass prophylaxis.
Assist with mass sheltering operations during a coastal storm.
Increase medical surge capacity during an influenza pandemic.
All healthcareprofessionals
Colon Cancer Screening2008
Refer patients aged �50 years or patients aged �40 years with a family history of colon cancerfor colonoscopy.
Internal medicine
Directly refer appropriate patients for colonoscopy rather than first sending patients to agastrointestinal consultation.
Family practice
Intimate Partner Violence2009
Screen all patients for intimate partner violence and encourage disclosure through routine inquiryand dialogue.
Internal medicine
Conduct a clinical assessment of all patients who disclose abuse or for whom abuse issuspected, and document findings thoroughly.
Family practice
If patients disclose intimate partner violence, promptly refer them to social and legal services. Obstetrics/gynecology
Breastfeeding 2009 Encourage and prescribe exclusive breastfeeding with no supplementation immediately followingbirth.
Family practice
Schedule a newborn visit 3–5 days after birth to assess and support breastfeeding. Pediatrics
Routinely reinforce the importance of exclusive breastfeeding. Obstetrics/gynecology
Remove formula manufacturers’ samples and educational materials from your office.
Know the breastfeeding resources in your community and encourage your patients to use them.
(continued on next page)
www.ajpmonline.org

Piftnc
pelap7esppl9ci(
Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134 S127
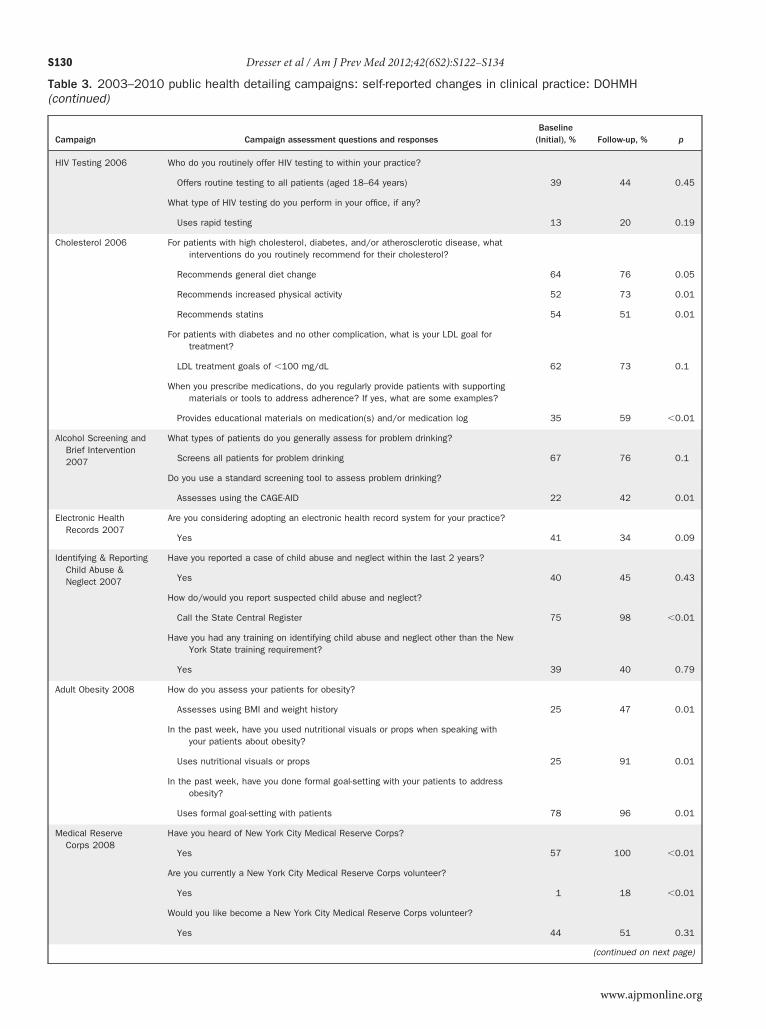
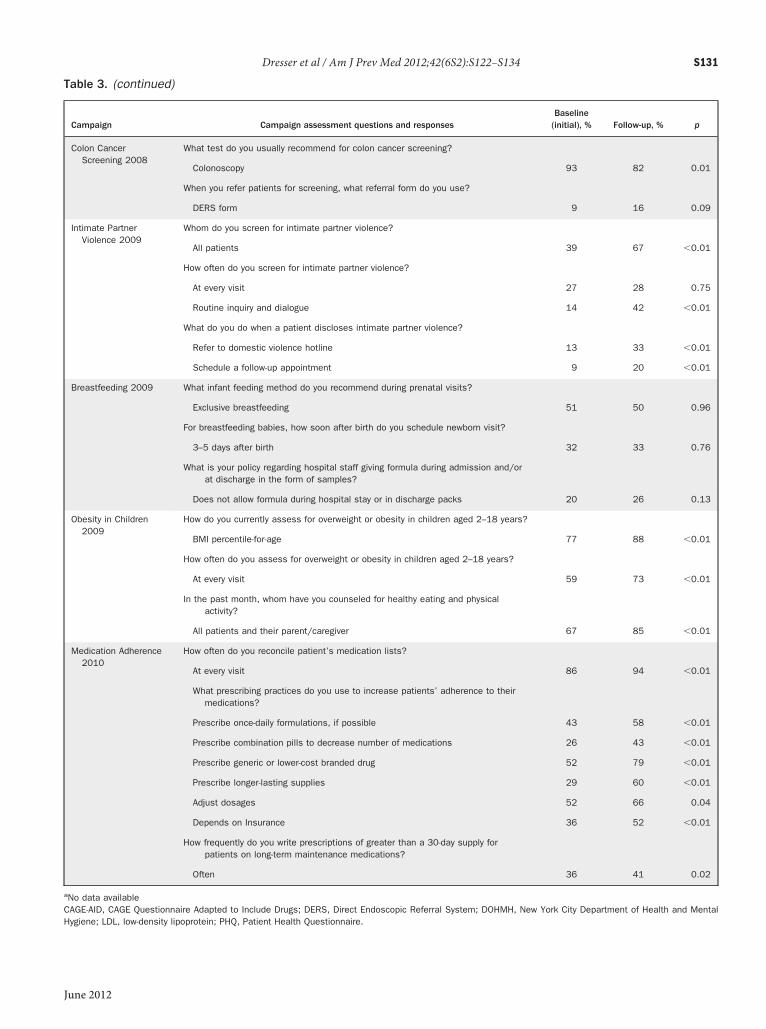
Table 3 illustrates changes in self-reported providerbehavior documented during the individual campaigns.Campaigns worked to improve providers’ practice be-havior to screen patients for clinical preventive servicesand chronic disease management, provide clinical man-agement, and address lifestyle modifıcation and self-management goal-setting with patients. In most cam-paigns, increases were seen among providers whopositively changed their practice behavior from baselineto follow-up.
Screening for Clinical Preventive Services andChronic Disease ManagementSeveral campaigns showed increases among providerswho screened for clinical preventive services. The 2004Colon Cancer campaign showed improvement in theproportion of providers who reported colonoscopy astheir primary screening method for colon cancer, from26% at baseline to 42% at follow-up (p�0.01). Whenrepeated in 2008, an even greater proportion of providersstated that colonoscopy was their preferred screeningmethod 82% to 93% of the time (p�0.01).The Depression campaign showed a marked increase
in the percentage of providers who used the PatientHealth Questionnaire-2,9 from 13% at baseline to 40% atfollow-up (p�0.01). Greater uptake in the use of clinicaltools to assess problem drinking was documented in theAlcohol Screening and Brief Intervention campaign. Atbaseline, 22% of the providers reported using the CAGE
Table 1. (continued)
Campaign DOHMH k
Influenza and PneumococcalVaccination 2009
Strongly recommend the appropriate influen
Screen all patients to determine whether th
Be sure you and your staff get vaccinated ainfluenza as early as possible this fall.
Continue to vaccinate high-risk patients thr
Pneumococcal vaccine should be given to phealth problems.
Obesity in Children 2009 Assess all children and adolescents for ove
Educate children, adolescents, and families
Work with families to set realistic goals for
Medication Adherence 2010 Assess adherence and discuss possible ba
Reconcile your medication lists with the pamedications.
Prescribe once-daily formulations, less-expewhenever possible.
Provide tools such as pill boxes and medicmedications.
DOHMH, New York City Department of Health and Mental Hygiene
Questionnaire Adapted to IncludeDrugs (CAGE-AID)10
June 2012
tool to assess for problemdrinking, and at follow-up, 42%of the providers reported adopting the CAGE-AID tool(p�0.01).10 Among providers visited for the Intimateartner Violence campaign, those who reported screen-ng all patients for intimate partner violence increasedrom 39% at baseline to 67% at follow-up (p�0.01), andhose who reported making screening for intimate part-er violence a part of routine inquiry and dialogue in-reased from 14% to 42% (p�0.01).During the Adult Obesity campaign, the number ofroviders who reported assessing BMI and weight atvery visit rose from 25% at baseline to 47% at fol-ow-up (p�0.01). The Obesity in Children campaignlso showed an increase in providers who assessed BMIercentile-for-age at every visit from 59% at baseline to3% at follow-up (p�|0.01). The proportion of provid-rs addressing chronic disease management washown in the Diabetes campaign. Providers who re-orted setting specifıc clinical management goals foratients to check their hemoglobin HbA1c levels ateast every 6 months increased from 66% at baseline to2% at follow-up (p�0.01), as well as those who indi-ated a target hemoglobin HbA1c level of 7 or lessncreased from 61% at baseline to 83% at follow-upp�0.01).
Clinical ManagementImprovements seen in the provision of clinical manage-ment to patients include changes in prescribing practice.
commendations Targeted providers
ccine(s) for all at-risk patients. Internal medicine
o need pneumococcal vaccination. Family practice
t both the seasonal and the novel H1N1 Obstetrics/gynecology
ut the entire influenza season.
aged �65 years and anyone with long-term
ht and obesity. Family practice
t healthful eating and physical activity. Pediatrics
hy eating and exercise.
to adherence at every patient visit. Internal medicine
list, adjust doses, and eliminate unneeded Family practice
generics, and longer-lasting supplies of medicine
logs to help patients remember to take their
ey re
za va
ey als
gains
ougho
eople
rweig
abou
healt
rriers
tient’s
nsive
ation
During the Contraception campaign, providers who re-
S128 Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134
ported prescribing emergency contraception in advanceincreased from 7% at baseline to 17% at follow-up(p�0.01). During the Medication Adherence campaign,the percentage of providers who reported reconcilingpatients’ medication lists at every visit increased from86% at baseline to 94% at follow-up (p�0.01). Addition-ally, the percentage of providers who reported prescrib-ing combination pills increased from 26% at baseline to43% at follow-up (p�0.01). Those prescribing generic orlower-cost branded drugs increased from 52% to 79%(p�0.01), and the percentage who prescribed longer-lasting supplies (90 days vs 30 days), when appropriate,increased from 29% at baseline to 60% at follow-up
Table 2. 2003–2010 public health detailing campaign rea
Campaign SitesUnique
providers
Influenza Vaccination 2003 151 —
Colon Cancer Screening 2004 193 —
Smoking Cessation 2004 151 —
Asthma 2004 168 —
Influenza Vaccination 2004a 164 a
Diabetes 2005 176 —
Contraception 2005 214 443
Influenza Vaccination 2005a 204 129
Hypertension 2005 157 349
Depression Screening 2006 198 352
HIV Testing 2006 151 317
Influenza and PneumococcalVaccination 2006a
143 116
Cholesterol 2006: high-riskpatients only
136 279
Alcohol Screening and BriefIntervention 2007
143 297
Electronic Health Records 2007 221 216
Child Abuse and Neglect 2007 154 240
Adult Obesity 2008 199 410
Medical Reserve Corps 2008 199 370
Colon Cancer Screening 2008 189 279
Intimate Partner Violence 2009 196 411
Breastfeeding 2009 152 281
Influenza and PneumococcalVaccination 2009a
157 170
Obesity in Children 2009 161 291
Medication Adherence 2010 186 340
aNo follow-up visits for 2004, 2005, 2006, and 2009 Influenza campaignsDOHMH, New York City Department of Health and Mental Hygiene
(p�0.01).
Lifestyle ModificationIncreases in the proportion of providers who reportedspeaking with their patients about lifestyle modifıca-tion and behavior change—to aid in the managementof certain chronic conditions—were seen throughoutcampaigns. During the Hypertension campaign, pro-viders who discussed weight loss with their patientsincreased from 68% at baseline to 80% at follow-up(p�0.10), and those who discussed increasing physicalactivity with their patients rose from 88% to 94%(p�0.10).Similarly, during the Cholesterol campaign, at base-
DOHMH
ders withial and-up visits
All providercontacts
All contacts(providersand staff)
Contacts persite
— 377 674 4
109 530 982 5
— 494 911 6
— 246 514 3
a 350 666 4
— 339 1340 8
146 528 1732 8
a 129 255 1
90 679 1294 8
127 366 1030 5
90 345 1170 8
a 116 256 2
113 405 1264 9
149 460 1688 12
109 339 1088 5
119 345 1169 8
166 588 2433 12
63 435 1742 6
133 413 1424 8
230 659 2234 11
170 455 1452 10
a 175 684 4
237 530 1588 10
265 607 1727 9
ch:
Proviinit
follow
line, 52% of the providers reported recommending in-
www.ajpmonline.org

Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134 S129
Table 3. 2003–2010 public health detailing campaigns: self-reported changes in clinical practice: DOHMH
Campaign Campaign assessment questions and responsesBaseline
(initial), % Follow-up, % p
Influenza andPneumococcalVaccination 2003
Who do you offer flu vaccines to?
To patients in all groups under the CDC recommendation 94 99 0.02
Do you use an office system to prompt you to offer flu vaccine to patients at thetime of their visit?
Use office system as reminder to offer flu vaccine 54 67 0.04
Colon CancerScreening 2004
What primary screening method do you recommend for colon cancer?
Colonoscopy as primary method 26 42 0.01
What is the clinic’s policy/practice regarding colon cancer screening?
Has an office system in place to promote colon cancer screening 52 62 0.01
Smoking Cessation2004
How often do you assess smoking status?
Assess smoking status at every visit 42 a —
Asthma 2004 For patients with asthma, do you indicate a level of severity on their chart?
Yes 68 a —
How do you usually assess severity?
History, spirometry, or peak flow at time of visit 72 a —
Do you usually prescribe controller medications for patients with persistent asthma?
Yes 96 a —
What type of controller medication do you most often prescribe?
Inhaled corticosteroids 85 a —
Do you routinely provide patients with a written self-management plan?
Yes/sometimes 50 a —
Diabetes 2005 What are your specific clinical management goals for hemoglobin HbA1c?
At least every 6 months 66 92 �0.01
HbA1c target level �7% 61 83 �0.01
What tools/systems do you use to track patients who are meeting their goals?
Checkbook (clinical tracking tool developed by the DOHMH) 28 43 �0.01
Contraception 2005 How is sexual history documented?
Has an office system to document sexual history 15 21 0.17
Do you ever prescribe emergency contraception in advance?
Advance prescribing of emergency contraception 7 17 0.01
Hypertension 2005 What lifestyle changes do you routinely discuss with your patients with high bloodpressure?
Discusses lifestyle change with patients re: weight loss 68 80 0.1
Discusses lifestyle change with patients re: physical activity 88 94 0.1
For which patients with hypertension do you recommend home blood pressuremonitoring?
Recommends for self-motivated patients 23 27 0.1
Depression Screening2006
What type of patients do you generally screen for depression?
Screens all patients as part of routine screening 41 40 0.1
Do you use a standard instrument to screen for depression?
Uses PHQ-2 and/or PHQ-9 to screen for depression 13 40 0.01
(continued on next page)
June 2012
S130 Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134
Table 3. 2003–2010 public health detailing campaigns: self-reported changes in clinical practice: DOHMH(continued)
Campaign Campaign assessment questions and responsesBaseline
(Initial), % Follow-up, % p
HIV Testing 2006 Who do you routinely offer HIV testing to within your practice?
Offers routine testing to all patients (aged 18–64 years) 39 44 0.45
What type of HIV testing do you perform in your office, if any?
Uses rapid testing 13 20 0.19
Cholesterol 2006 For patients with high cholesterol, diabetes, and/or atherosclerotic disease, whatinterventions do you routinely recommend for their cholesterol?
Recommends general diet change 64 76 0.05
Recommends increased physical activity 52 73 0.01
Recommends statins 54 51 0.01
For patients with diabetes and no other complication, what is your LDL goal fortreatment?
LDL treatment goals of �100 mg/dL 62 73 0.1
When you prescribe medications, do you regularly provide patients with supportingmaterials or tools to address adherence? If yes, what are some examples?
Provides educational materials on medication(s) and/or medication log 35 59 �0.01
Alcohol Screening andBrief Intervention2007
What types of patients do you generally assess for problem drinking?
Screens all patients for problem drinking 67 76 0.1
Do you use a standard screening tool to assess problem drinking?
Assesses using the CAGE-AID 22 42 0.01
Electronic HealthRecords 2007
Are you considering adopting an electronic health record system for your practice?
Yes 41 34 0.09
Identifying & ReportingChild Abuse &Neglect 2007
Have you reported a case of child abuse and neglect within the last 2 years?
Yes 40 45 0.43
How do/would you report suspected child abuse and neglect?
Call the State Central Register 75 98 �0.01
Have you had any training on identifying child abuse and neglect other than the NewYork State training requirement?
Yes 39 40 0.79
Adult Obesity 2008 How do you assess your patients for obesity?
Assesses using BMI and weight history 25 47 0.01
In the past week, have you used nutritional visuals or props when speaking withyour patients about obesity?
Uses nutritional visuals or props 25 91 0.01
In the past week, have you done formal goal-setting with your patients to addressobesity?
Uses formal goal-setting with patients 78 96 0.01
Medical ReserveCorps 2008
Have you heard of New York City Medical Reserve Corps?
Yes 57 100 �0.01
Are you currently a New York City Medical Reserve Corps volunteer?
Yes 1 18 �0.01
Would you like become a New York City Medical Reserve Corps volunteer?
Yes 44 51 0.31
(continued on next page)
www.ajpmonline.org
Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134 S131
Table 3. (continued)
Campaign Campaign assessment questions and responsesBaseline
(initial), % Follow-up, % p
Colon CancerScreening 2008
What test do you usually recommend for colon cancer screening?
Colonoscopy 93 82 0.01
When you refer patients for screening, what referral form do you use?
DERS form 9 16 0.09
Intimate PartnerViolence 2009
Whom do you screen for intimate partner violence?
All patients 39 67 �0.01
How often do you screen for intimate partner violence?
At every visit 27 28 0.75
Routine inquiry and dialogue 14 42 �0.01
What do you do when a patient discloses intimate partner violence?
Refer to domestic violence hotline 13 33 �0.01
Schedule a follow-up appointment 9 20 �0.01
Breastfeeding 2009 What infant feeding method do you recommend during prenatal visits?
Exclusive breastfeeding 51 50 0.96
For breastfeeding babies, how soon after birth do you schedule newborn visit?
3–5 days after birth 32 33 0.76
What is your policy regarding hospital staff giving formula during admission and/orat discharge in the form of samples?
Does not allow formula during hospital stay or in discharge packs 20 26 0.13
Obesity in Children2009
How do you currently assess for overweight or obesity in children aged 2–18 years?
BMI percentile-for-age 77 88 �0.01
How often do you assess for overweight or obesity in children aged 2–18 years?
At every visit 59 73 �0.01
In the past month, whom have you counseled for healthy eating and physicalactivity?
All patients and their parent/caregiver 67 85 �0.01
Medication Adherence2010
How often do you reconcile patient’s medication lists?
At every visit 86 94 �0.01
What prescribing practices do you use to increase patients’ adherence to theirmedications?
Prescribe once-daily formulations, if possible 43 58 �0.01
Prescribe combination pills to decrease number of medications 26 43 �0.01
Prescribe generic or lower-cost branded drug 52 79 �0.01
Prescribe longer-lasting supplies 29 60 �0.01
Adjust dosages 52 66 0.04
Depends on Insurance 36 52 �0.01
How frequently do you write prescriptions of greater than a 30-day supply forpatients on long-term maintenance medications?
Often 36 41 0.02
aNo data available
CAGE-AID, CAGE Questionnaire Adapted to Include Drugs; DERS, Direct Endoscopic Referral System; DOHMH, New York City Department of Health and MentalHygiene; LDL, low-density lipoprotein; PHQ, Patient Health Questionnaire.June 2012

S132 Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134
creased physical activity to patients with high cholesterollevels, whereas 73% reported doing so at follow-up(p�0.01). At baseline, 64% of the providers reportedroutinely recommending diet change to patients withhigh cholesterol value. At follow-up, this proportion in-creased to 76% (p�0.05). Additionally, during the Obe-sity in Children campaign, providers who reported coun-seling all pediatric patients and their caregivers forhealthy eating andphysical activity increased from67%atbaseline to 85% at follow-up (p�0.01).
Self-Management Goal-SettingIn several campaigns, providers reported an increaseduse of self-management goal-setting with their patients.During the Diabetes campaign, the percentage of provid-ers who reported using a “checkbook-style” diary withpatients to track their hemoglobin HbA1c level increasedfrom 28% at baseline to 43% at follow-up (p�0.01). Datafrom the Adult Obesity campaign showed that almost allproviders used goal-setting strategies for weight loss withtheir patients: from 78% at baseline to 96% at follow-up(p�0.01). Those reporting use of nutritional visuals orprops when speaking about obesity management in-creased from 25% at baseline to 91% at follow-up(p�0.01).
DiscussionBy establishing open channels of communication; pro-viding valuable information, evidence-based tools, re-sources, and patient education materials; and buildingstrong relationships with primary care team membersin high-need neighborhoods, the Public Health Detail-ing Program has developed a successful strategy forcommunicating public health recommendations toclinical care teams. Results of the campaign evaluationindicate that representatives are highly skilled at facil-itating conversations and gaining agreements to im-plement the DOHMH’s recommendations. In the earlydays of the program, occasionally providers wouldreject visits, at times confusing them with regulatoryactivities of other agencies, but by 2010, all practices inthe target communities were routinely receiving visits.Evaluation data from individual public health detailing
campaigns suggest potential effectiveness of this model,which involves repeat, personal visits to offıce teams, aswell as the importance of clear, consistent messagingaround key clinical recommendations. All of the re-sponding providers indicated that the detailing visitshave changed their practice in a positive way, and 73% ofpractices implemented clinical tools (including 15% whoadopted an electronic health record into their practice),
key recommendations, and patient education materials.Care teams reported that they value these tools and re-sources to help reinforce key recommendations, initiateconversations, improvemutual understanding, and facil-itate goal-setting with their patients during and aftercampaigns.Since the inception of the Public Health Detailing Pro-
gram, providers have allotted more time to each visit.Initially, visits lasted an average of 12 minutes, but by2010, visits increased to an average of 17 minutes, anindication of the providers’ interest in the topic and areflection of the relationships representatives developedwith the practices throughout the years.An essential ingredient is having highly trained,
knowledgeable representatives consistently working di-rectly with providers.11 Literature shows that this multi-faceted approach is an effective strategy for influencingprovider attitudes and behavior and is more effectivethan certain other types of educational outreach. “Aca-demic detailing” linked with other educational strategiesmay be the most effective paired intervention, becauseprint-only or mailing interventions generally have notbeen found to be effective in modifying physicianbehavior.12,13
Public health detailing serves as a bridge between theDOHMH and community providers, creating a two-way flow of information. The valuable qualitative andquantitative feedback from providers has been used bythe DOHMH to guide clinical interventions and pro-grammatic initiatives.Economic sustainability of public health programs, in
times of recession, continues to pose a challenge. Publichealth detailing has an average cost in New York City ofapproximately $95 per contact, of which $40 is for staff.Similar programs ideally might be fınanced by organiza-tions to which savings would accrue as a result of im-proved care, such as Medicaid or Medicare, which there-fore have direct interest in their continuity. Because thePublic Health Detailing Program is run by a local healthdepartment—focusing on population health—and iswithout the evident fınancial interests private insurersmight have, this appears to be a source of credibility forthe program’s recommendations.
LimitationsAs stated above, the Public Health Detailing Program’sreach varied among the different campaigns. Fluctua-tion in the program’s reach for number of sites visitedand providers seen varied on several factors, includinglength of the campaign, size of the target group ofproviders, variation in staff size, and provider or staffreceptivity to messaging. However, a general trend ofan increasing number of contacts per site has contin-
ued since the Public Health Detailing Program imple-www.ajpmonline.org

Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134 S133
mented its fırst campaigns. Sites’ increasing familiaritywith the program and representatives’ improving com-munication skills over the last several years enhancedthe reach at each site and reduced wait time to see keyoffıce staff and providers.Loss of follow-up visits with the same providers during
the course of individual campaigns was another limita-tion of the Public Health Detailing Program. Providersand staff often work at multiple sites on certain days andhours of the week, so the number of providers reached atfollow-up is always lower than the number reached dur-ing initial visits. Strategies were implemented to increasethe percentage match of initial and follow-up visits, par-ticularly with physicians, nurse practitioners, and physi-cian assistants, to 80% or higher, a goal subsequentlyachieved with at least two campaigns.Changes in the data structure since the program began
also limited the conclusions drawn from these results.Some of the early campaigns did not capture data in thesame format, and data were unavailable for a few cam-paigns. Most important, this evaluation relied on pro-vider self-reported practices. Self-report may fail to accu-rately reflect providers’ actual clinical behavior. Use ofclinical data to verify changes in clinical practicewould bean important complement to assess effectiveness of thisprogram.The power of electronic medical records also could be
used to assess the effect of campaigns on clinical practice.When the Public Health Detailing Program began, elec-tronic medical records were not as widely used as today,and they should be used for evaluating this and otherclinical systems improvement efforts. However, counsel-ing and provider–patient conversations around a diseasetopic and self-management goal-setting are often not ad-equately captured in the patient record. Patient exit sur-veys or other mechanisms to evaluate the messages pa-tients received during an offıce visit, as well as which onesthey intend to act on, would be another possible evalua-tion approach for the program.Finally, the extent to which the assessed practices
would have changed in the absence of the Public HealthDetailing Program effort is unknown. Providers are reg-ularly exposed to numerous opportunities thatmay influ-ence the way they practice medicine, such as continuingeducation courses, medical journals, conferences, andother means by which evidence-based recommendationsand materials can be acquired. These factors alone, or inconjunction with public health detailing, could have af-fected clinical practice and behavior.
ConclusionOverall, the Public Health Detailing Program has been
received very positively by the medical community in theJune 2012
underserved communities prioritized by the program.Despite the limitations noted, evaluation data based onprovider self-report suggest that public health detailingcan be an effective strategy for linking public health agen-cies and their recommendations tomedical providers andstaff as well as assisting in the development of futureprogram and policy initiatives. The professional relation-ships developed between the providers and their staff andthe DOHMH permit a dialogue described by Avorn:
These conversations enable a talented communicatorto understand the physician’s current practices, be-liefs, and attitudes, making it possible to tailor abehavior-change message specifıcally to that individ-ual’s decision-making process.11
Other public health agencies may fınd this approach forpromoting important clinical practices a useful strategyto assist in improving population health.
Publication of this article was supported by the U.S. DHHSHealth Resources and Services Administration (HRSA) and theNIH National Institute on Minority Health and HealthDisparities.The authors thank Tamara Dumanovsky, PhD, for her ex-
pertise and feedback as the former Director of Research andEvaluation for the Bureau of Chronic Disease Prevention andControl at the New York City Department of Health andMen-tal Hygiene as well as the many Health Department represen-tatives for their detailing throughout the years.Human participant protection was not required because this
review of the literature did not involve human participants.No fınancial disclosures were reported by the authors of this
paper.
References1. Wagner EH, Austin BT, Von KorffM. Improving outcomes in chronic
illness. Manag Care Q. 1996;4(2):12–25.2. Larson K, Levy J, Rome MG, Matte TD, Silver LD, Frieden TR. Public
health detailing: a strategy to improve the delivery of clinical preventiveservices in New York City. Public Health Rep. 2006;121(3):228–234.
3. Soumerai SB, Avorn J. Principles of educational outreach (‘academicdetailing’) to improve clinical decision making. JAMA. 1990;263(4):549–556.
4. Shojania KG, Ranji SR, McDonald KM, et al. Effects of quality im-provement strategies for type 2 diabetes on glycemic control: a meta-regression analysis. JAMA. 2006;296(4):427–440.
5. New York City Department of Health and Mental Hygiene. CommunityHealth Profıles. 2006. www.nyc.gov/html/doh/html/data/data.shtml.
6. Bodenheimer T, Wagner EH, Grumbach K. Improving primary carefor patients with chronic illness. JAMA. 2002;288(14):1775–1779.
7. Sheinfeld Gorin S, Gemson D, Ashford A, et al. Cancer educationamong primary care physicians in an underserved community. Am JPrev Med. 2000;19(1):53–58.
8. Boom JA, Nelson CS, Laufman LE, Kohrt AE, Kozinetz CA. Im-
provement in provider immunization knowledge and behaviors
1
1
1
1
S134 Dresser et al / Am J Prev Med 2012;42(6S2):S122–S134
following a peer education intervention. Clin Pediatr (Phila).2007;46(8):706–717.
9. Spitzer RL, Kroenke K, Williams JBW. Validation and utility of aself-report version of PRIME-MD: the PHQ primary care study. Pri-maryCare Evaluation of Mental Disorders. Patient Health Question-naire. JAMA. 1999;282(18):1737–1744.
0. Petit J, Sederer LI. Brief intervention for alcohol problems. New YorkCity Department of Health andMental Hygiene. City Health Informa-
tion. 2006;25(10):71–78.1. Avorn J. Transforming trial results into practice change: the fınaltranslational hurdle: comment on “Impact of the ALLHAT/JNC7 Dis-semination Project on thiazide-type diuretic use”. Arch Intern Med.2010;170(10):858–860.
2. Avorn J, Soumerai SB. Improving drug-therapy decisions througheducational outreach: a randomized controlled trial of academicallybased “detailing.” N Engl J Med. 1983;308(24):1457–1463.
3. Heffner JE. Altering physician behavior to improve clinical perfor-
mance. Top Health Inf Manage. 2001;22(2):1–9.www.ajpmonline.org