Ptosis not ptosisSHORT - mercyeye.com · When is Ptosis not “just” Ptosis? Cat Burkat, MD, ......
21
1/22/15 1 When is Ptosis not “just” Ptosis? Cat Burkat, MD, FACS Associate Professor Oculoplastic, Facial Cosmetic, & Orbital Surgery University of Wisconsin- Madison March 7, 2015 Typical Ptosis • Complains of drooping – Heavy lid, fatigue, has to lift lid manually • MRD low, approaches pupil • Droopy lid triad: 1. Skin excess 2. Levator muscle dehiscence (Involutional ptosis) 3. Brow/forehead ptosis
Transcript of Ptosis not ptosisSHORT - mercyeye.com · When is Ptosis not “just” Ptosis? Cat Burkat, MD, ......

1/22/15
1
When is Ptosis not “just” Ptosis?
Cat Burkat, MD, FACS Associate Professor
Oculoplastic, Facial Cosmetic, & Orbital Surgery
University of Wisconsin- Madison
March 7, 2015
Typical Ptosis
• Complains of drooping – Heavy lid, fatigue, has to lift lid
manually
• MRD low, approaches pupil • Droopy lid triad:
1. Skin excess 2. Levator muscle dehiscence
(Involutional ptosis) 3. Brow/forehead ptosis

1/22/15
2
So…we all sag as we age
When can’t we blame it on age?
• 52 yo M with progressive RUL ptosis over 1 year - Hard to put contacts in OD
• Motility, pupils, SLE nl • MRD 0.5 mm OD, 4 mm OS • LVF 11 mm OD, 16 mm OS • Recommend internal ptosis repair
Case

1/22/15
3
• Intraoperative findings: – Eversion – Thick lid
H&E. 40x
H&E. 10x Case
• Diagnosis: RUL ptosis-- yes… but – MRD 0.5 mm OD, 4 mm OS – LVF 11 mm OD, 16 mm OS
• Levator dehiscence alone (which can occur with CL use) should =normal levator function!
Patient:
Ptosis with poor levator function was due to infiltration of levator muscle from lymphoma

1/22/15
4
• Levator function: – Normal ≥ 15mm – Must negate forehead
movement
• 43 yo M, never seen MD for 30 yrs, with eyelid drooping and “lumps” OU.
– puffy lids
• Pupils, motility, LVF nl • Proptosis
Case
• S-shaped eyelid contour:
Ø Suggests lacrimal gland involvement
Ø Palpate!

1/22/15
5
• Palpate – Firm large smooth masses – Proptosis – Ptosis
• Think LG etiologies • Concurrent pneumonia?
Case
• Patient: BUL ptosis yes… but with S-shaped eyelid contour
– Lacrimal gland enlargement causes mechanical ptosis effect
Case

1/22/15
6
Case
• 48 yo F with several mos drooping RUL • VA, pupils, motility, SLE nl • No proptosis
• No erythema, tenderness • ?Just aging fat?
Case • 48 yo F with several mos drooping RUL • VA, pupils, motility, SLE nl • No proptosis • No erythema, tenderness • ?Just aging fat?
• Dx: Lymphoma
TOUCH the lids! Patient: RUL ptosis…yes, but firm smooth oval subQ discrete mass
- normal fat prolapse = nondiscrete and without a border

1/22/15
7
Lymphoma
• #1 most common malignant orbital tumor in adults – Age 50-70
• Insidious onset - painless proptosis, ptosis, diplopia, lid edema • Lacrimal gland is most common orbital site involved
– Up to 50% arise in lacrimal fossa • Bilateral occurrence common (17%)
• Orbital presentation – Anterior orbit – Subconjunctival salmon patch – “Putty-like molding” around structures rather
than invasion • usually vision / EOM’s remain intact
• Predilection for superior/anterior orbit → downward globe displacement
MANAGEMENT • INCISIONAL BIOPSY: fresh specimen for immunocytochemistry +
formalin specimen • Labs: Chem panel, LFT, Alk phos, CT abd/pelvis/chest, bone marrow bx • Chemotherapy • Radiotherapy
– Localized orbital adnexal disease (Achieves local control and may prevent spread)
Lymphoma

1/22/15
8
Lymphoma • Only 20-30% have h/o previous or concomitant systemic disease • 20% of pt with lymphoid tumors of conjunctiva,
35% of pt with orbital tumors, & 67% with eyelid disease will eventually develop systemic
lymphoma PROGNOSIS • Visual prognosis good unless radiation retinopathy • All with localized lesions need LIFELONG follow-up for
development of systemic disease
Case • 6 yo F “bumped heads
with student”, shortly after had RUL swelling. Eye pressure and headaches.
• Rash, fatigue, fevers – ER dx: URI
• VAcc: 20/20 OU • Pupils: equal, reactive,
no RAPD • Motility: limited upgaze,
hypoglobus

1/22/15
9
Case • 69 yo WF awoke one AM
with left eyelid drooping. • No h/o trauma,
discharge, pain. • VAcc: 20/30 OU • Pupils: equal, reactive,
no RAPD • Motility: full OU • SLE, IOP: nl
• PO antibiotics by PCP
Case
• H(93.5): 16 OD, 15 OS • Resistance to retropulsion OS • Brawny thickened LLL

1/22/15
10
• CT orbits: dx: “pre- and post-septal cellulitis” – Ill-defined LLL diffuse enhancement – Inferior rectus – No bony involvement – Bilateral maxillary sinus disease
Case
PMH on review • PMH:
– HTN – GERD – Breast CA-dx 1980
• S/p mastectomy 1984, 1993 • No h/o metastases
Patient: LUL ptosis yes… but also lower lid elevation (or reverse ptosis), eyelid thickening, enophthalmos
- If you don’t ask about the remote history, they often won’t tell
- Ptosis in this pt due to enophthalmos
1/22/15
11
Metastasis to the Orbit • Accounts for ≈ 10% of all orbital neoplasms. (5% hematogenous,
5% from adjacent structures)
• What is the most common malignancy to spread to orbit? – Breast Cancer (42%) – Lung Carcinoma (11%) – Unknown Primary Cancer (11%) – Prostate (8%) – Melanoma (5%) Average survival after dx is 9 months
• 25% of metastatic tumors to the orbit are the initial presentation
– Metastatic neuroblastoma – Leukemia, lymphoma
• In pediatric population, metastatic disease is far less common
Enophthalmos
• 10% of metastatic cases – 80% breast cancer – Contraction of fibroblasts in the scirrhous tumor →
posterior traction on globe
• Breast > GI > prostate, lung

1/22/15
12
Case
• 64 yo M with droopy RUL x 3 wks after picked up new glasses. Also complains of intermittent diplopia before then.
• No dysarthria, systemic weakness
• VA: 20/40 OD, 20/20 OS
• Pupils, motility nl. Orthotropic
• MRD minus 2mm OD, +1mm OS
• LVF 12mm OU
• Diagnosis: RUL ptosis-- yes… but – MRD minus 2mm OD, +1mm OS – Acute onset – Intermittent diplopia preceding
• Levator dehiscence alone should = slowly progressive ptosis
Patient: Variable measurements or true fluctuating symptoms should warrant additional evaluation

1/22/15
13
Ice Pack test • Cheap, safe, quick bedside test • Apply ice to closed lids for 2–5 minutes
– Positive if improvement of diplopia or elevation of MRD by 2 mm – Physiological theory: by cooling skeletal muscle fibers (below 28˚C), the activity of acetylcholinesterases is inhibited
Previous pt: MRD minus 2mm OD, +1mm OS After ice test: MRD +1.5mm OD, +1mm OS
Another Case of MG
• Ice test: – Much over 3 minutes, reduction of muscle fiber temperature below 22˚C may reduce contractile force of the muscle potential false-negative result
• Acetylcholine receptor antibody test
potential false-negative? Patient:
Ptosis due to neuromuscular junction abnormality resulting in decreased muscle contraction
1/22/15
14
Case
• 28 yr old F with ptosis “since she was little” worsening over past yr, resulting in neck pain
– Adopted chin-up position – Severe ptosis BUL – Levator function 4-5mm – Motility nl – No lagophthalmos – Bell’s phenomenon
decreased
• Severe ptosis BUL – MRD minus 2mm OU
• Levator function 4-5 mm • Bell’s phenomenon
decreased
• 3 siblings all have similar appearances
Blepharophimosis-Ptosis- Epicanthus Inversus Syndrome:
Short vertical & horizontal palpebral fissure
Epicanthus inversus lower lid fold Telecanthus
Flat nasal bridge High arched brows
Ectropion Nystagmus, strabismus
Case
Dx: congenital ptosis?

1/22/15
15
Blepharophimosis-Ptosis- Epicanthus Inversus Syndrome
• 4-6% of congenital ptosis • Autosomal dominant inheritance
– FOXL2 gene mutation • May be associated with female infertility
or congenital heart disease
• Surgical options: – None – Limited elevation due to high risk
lagophthalmos – Frontalis sling – Stepwise approach- telecanthus, epicanthal
fold, ectropion, ptosis last
• Diagnosis: BUL ptosis-- yes… but – Minus MRD – LVF 4-5 mm OU – high arched brows – “small eye openings”
• Ask for family history or photos
Patient:
Ptosis with poor levator function due to hypoplasia of levator muscle (myogenic)
1/22/15
16
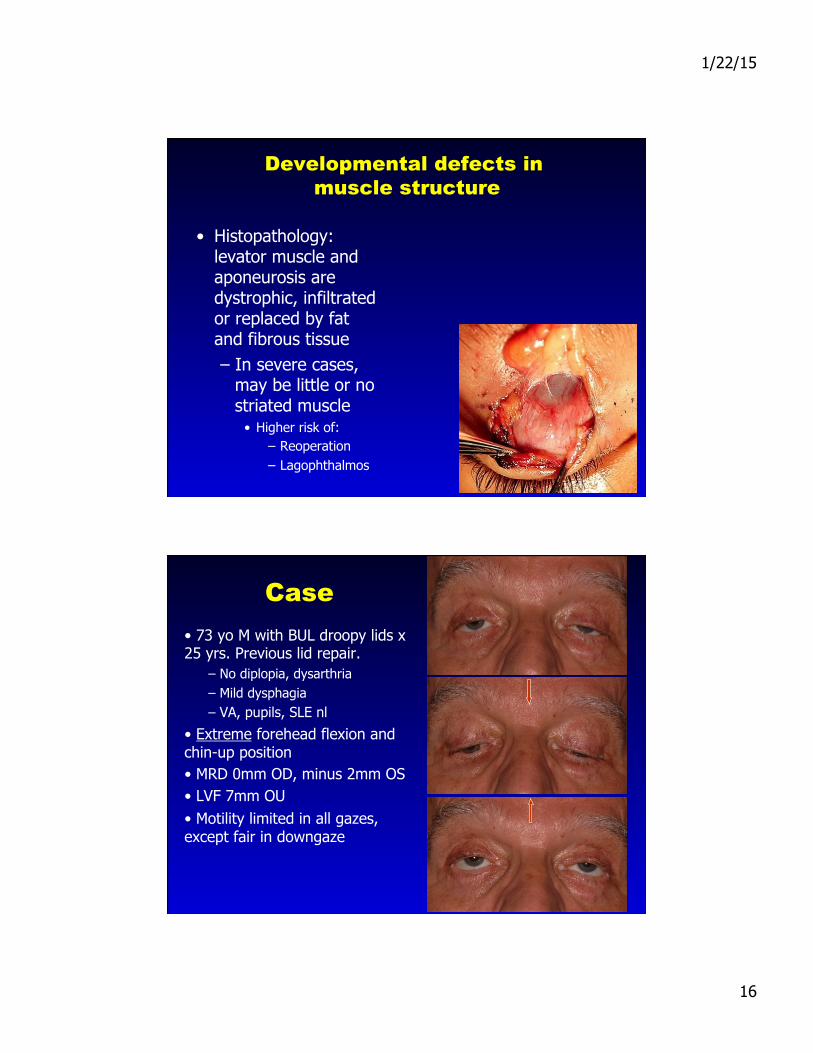
Developmental defects in muscle structure
• Histopathology: levator muscle and aponeurosis are dystrophic, infiltrated or replaced by fat and fibrous tissue – In severe cases,
may be little or no striated muscle
• Higher risk of: – Reoperation – Lagophthalmos
Case • 73 yo M with BUL droopy lids x 25 yrs. Previous lid repair.
– No diplopia, dysarthria – Mild dysphagia – VA, pupils, SLE nl
• Extreme forehead flexion and chin-up position • MRD 0mm OD, minus 2mm OS • LVF 7mm OU • Motility limited in all gazes, except fair in downgaze
1/22/15
17
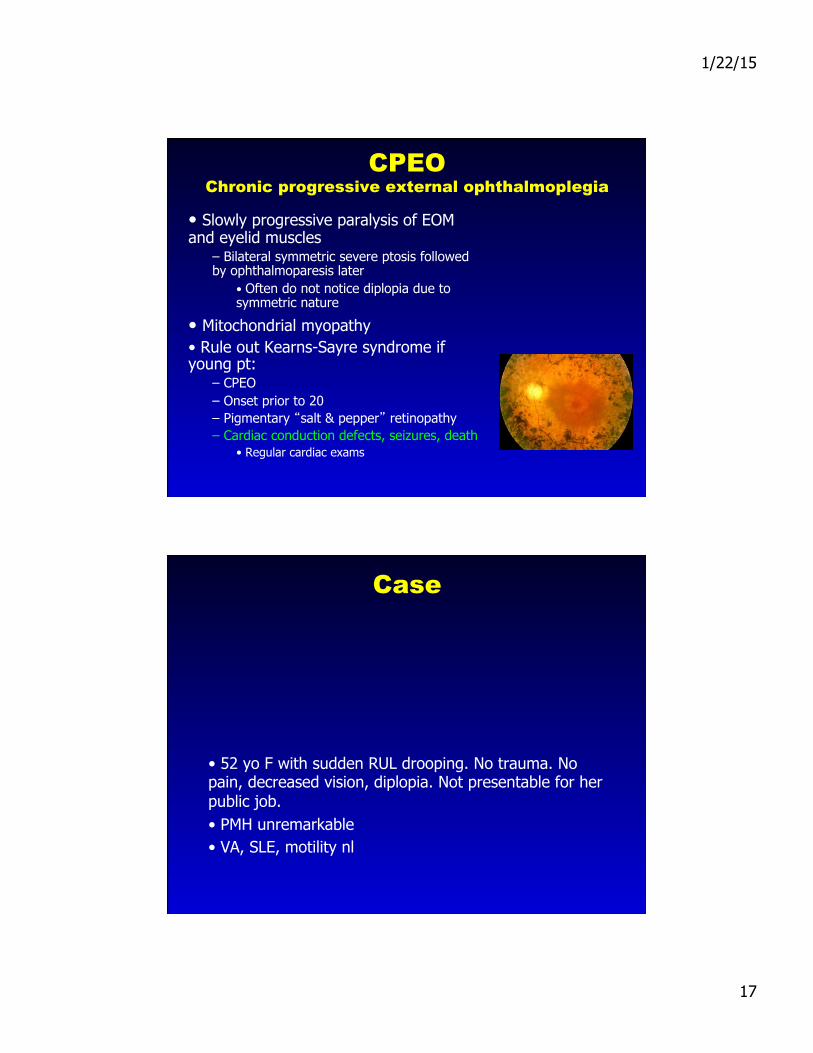
CPEO Chronic progressive external ophthalmoplegia
• Slowly progressive paralysis of EOM and eyelid muscles
– Bilateral symmetric severe ptosis followed by ophthalmoparesis later
• Often do not notice diplopia due to symmetric nature
• Mitochondrial myopathy • Rule out Kearns-Sayre syndrome if young pt:
– CPEO – Onset prior to 20 – Pigmentary “salt & pepper” retinopathy – Cardiac conduction defects, seizures, death
• Regular cardiac exams
Case
• 52 yo F with sudden RUL drooping. No trauma. No pain, decreased vision, diplopia. Not presentable for her public job. • PMH unremarkable • VA, SLE, motility nl

1/22/15
18
Dx: RUL ptosis but…
• Ptosis • Reverse ptosis • Miosis • Other findings: anhidrosis, anisocoria worse in dark
Patient: Ptosis due to Horner’s Syndrome. Don’t forget the exam basics!
Sympathetically-innervated Muller’s muscle and inferior retractors
Case
• 58 yo F with OS drooping, FBS and redness x 2 mos • Hx of multiple nonhealing corneal ulcers • PMH bipolar disorder with psychosis • VA: HM OS • Corneal scar and pannus • Loss of lashes
Definitely not just ptosis!

1/22/15
19
• Differential Dx: – Conjunctival intraepithelial neoplasia – Sebaceous cell carcinoma – Lymphoproliferative process – Severe follicular conjunctivitis
• Pseudotrachoma
• Histopathology: – conjunctival lichen simplex chronicus
• Referred to as the “scratch-itch-scratch” lichenification cycle
– pruritus is dominant symptom
Patient: Loss of lashes at uneven lengths suggests self-induced behaviors causing ptosis

1/22/15
20
Case • Unilateral ptosis over several months
• Pseudoptosis due to retraction of opposite side
– Thyroid disease is most common cause of unilateral or bilateral proptosis/retraction
Atypical Ptosis “Clues”
Symptoms: • Diplopia • Pain • Decreased vision • Lump • Swelling, redness • Rapid onset
Exam findings: • Levator function • Motility • Pupils • Proptosis • Mass • S-shaped lid contour • Disc edema, retinal changes

1/22/15
21
Summary
• Not all ptosis is “just ptosis” from levator dehiscence
• Often will present with other clues • Get close • Knowledge and exam skills • Diagnosis of these diseases can often be the initial
presentation of disease, and can be life-saving (malignancy, MG, Kearns-
Sayre, OPD, Horner’s)