
Dual Medical Psychotherapy General ... - School of Psychiatry

Psychotherapy in Contemporary Psychiatry: an essential treatment Prof Anthony W Bateman Hon Professor in Psychotherapy University of Copenhagen

Psychiatry is Psychotherapy
n Neurobiology, psychology, social cognition and relationships interweave to disrupt mental processing
n Mental Disorders require complex treatment to optimize outcome
n The person of the treater is essential n Psychiatry is a relational enterprise

Psychiatry and Psychotherapy
n Psychiatry Ø Biological Ø Psychological Ø Social Ø cultural
n Symptoms, syndromes, Diagnosis
n Mental Illness n Medication
n Psychotherapy Ø Talking – indiv, group,
family Ø Relationships Ø Emotions Ø Cognitions
n Psychological processes
n Less diagnostic and more dimensional

The Nature of
Attachment

The social brain
mPFC
n 1. Medial prefrontal cortex Ø Mentalising proper
o Implicit ability to infer mental states such as beliefs, feelings and desires
Fletcher et al., 1995; Gallagher et al., 2000; Gilbert et al., 2006 (meta-analysis)

The social brain
mPFC
pSTS/TPJ n 2. pSTS/TPJ
Ø Prediction o Biological motion, eye
gaze
Ø Perspective-taking o Different physical points
of view
Pelphrey et al., 2004a,b; Kawawaki et al., 2006 (review); Mitchell 2007

The social brain
mPFC
pSTS/TPJ n 3. Amygdala Ø Attaching reward
values to stimuli o ‘Approach’ vs. ‘avoid’
Ø Facial expressions
Dolan 2002; LeDoux 2000; Winston et al., 2002; Phelps et al., 2000, 2003
Amygdala

The social brain
mPFC
pSTS/TPJ
Temporal pole
n 4. Temporal poles Ø Social scripts,
complex event knowledge
Funnell, 2001; Damasio et al., 2004; Moll et al., 2001, 2002, 2005 (review)
Amygdala

Shared neural circuits for mentalizing about the self and others (Lombardo et al., 2009; J. Cog. Neurosc.)
Self mental state
Other mental state
Overlapping for Self and Other

The mesocorticolimbic dopaminergic reward circuit in addiction process
Amygdala/ bed nucleus of
ST

Baron-Cohen’s (2005) model of the social brain
The Emotion Detector - Left inferior frontal gyrus - Mirror neurons
The Intention Detector - Right medial prefrontal cortex - inferior frontal cortex - Bilateral anterior cingulate - Superior temporal gyrus
Eye Direction Detector - Posterior superior temporal sulcus
Shared Attention Mechanism - Bilateral anterior cingulate - Medial prefrontal cortex - Body of caudate nucleus
The Empathising System - Fusiform gyrus - Amygdala - Orbito-frontal cortex
Theory of Mind Mechanism - Medial prefrontal cortex - Superior temporal gyrus - Temporo-parietal junction
EMOTION UNDERSTANDING BELIEF-DESIRE REASONING

How Attachment Links to Affect Regulation
DISTRESS/FEAR
Exposure to Threat
Proximity seeking
Activation of attachment
The forming of an attachment bond
Down Regulation of Emotions EPISTEMIC
TRUST
BONDING

own baby pictures minus other baby pictures own baby pictures minus houses
HEALTHY MOTHERS OF FIRST INFANTS
N=13
HEALTHY FATHERS OF
FIRST INFANTS
N=8
THALAMUS - BG FACE-OBJECT VISUAL CORTEX
BASAL GANGLIA AMYGDALA
THALAMUS - BG AMYGDALA MIDBRAIN FACE-OBJECT VISUAL CORTEX
CINGULATE CINGULATE
THALAMUS - BG AMYGDALA MIDBRAIN
CINGULATE
Swain et al.,
Crying Neutral Smiling
Do Different Affective States Trigger the Attachment System Equally?

Own: Own: HappyHappy(OH)(OH)
Unknown: Unknown: HappyHappy(UH)(UH)
Unknown:Unknown:SadSad(US)(US)
Own: Own: NeutralNeutral
(ON)(ON)
Own: Own: SadSad(OS)(OS)
Unknown:Unknown:NeutralNeutral
(UN)(UN)
2 sec2 sec
2 sec2 sec
2 sec2 sec
2 sec2 sec
2 sec2 sec
2 sec2 sec
22––6 sec random6 sec randominterinter--stimulus stimulus
intervalinterval
AFFECT
IDENTITY
USOSSad
UNONNeutral
UHOHHappy
Unknown Baby
Own Baby
AFFECT
IDENTITY
USOSSad
UNONNeutral
UHOHHappy
Unknown Baby
Own Baby
STIMULUSSTIMULUSTYPESTYPES
What’s in a Smile? Maternal Brain Responses to Infant Facial
Cues (Strathearn L, Li J, Fonagy P, Montague PR)

Brain response of mothers viewing their own baby’s face
-4 -2 0 2 4 6 8 10 12
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
-4 -2 0 2 4 6 8 10 12 -4 -2 0 2 4 6 8 10 12
HAPPYHAPPY NEUTRALNEUTRAL SADSAD
A. Dorsal putamen
B. Substantia nigra Own baby faceOwn baby face
Time from baby face presentation (sec)
fMR
I res
pons
e (%
BO
LD s
igna
l +/-
se)
Unknown baby faceUnknown baby face
**
* *
**
*
*

-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
R Ventral Striatum R Insula
% s
igna
l cha
nge
Secure Insecure/Dismissing
(t=3.0, P<0.01) (t= -3.9, P<0.0005)
mPFC
y=11 -1.5
-1-0.5
00.5
11.5
22.5
33.5
44.5
5
R Ventral Striatum R mPFC
% s
igna
l cha
nge
(t=3.1, P<0.005) (t=3.0, P<0.01) x=-6
Insula
VS
VS
y=6 y=16
A
B
Maternal security and hemodynamic change
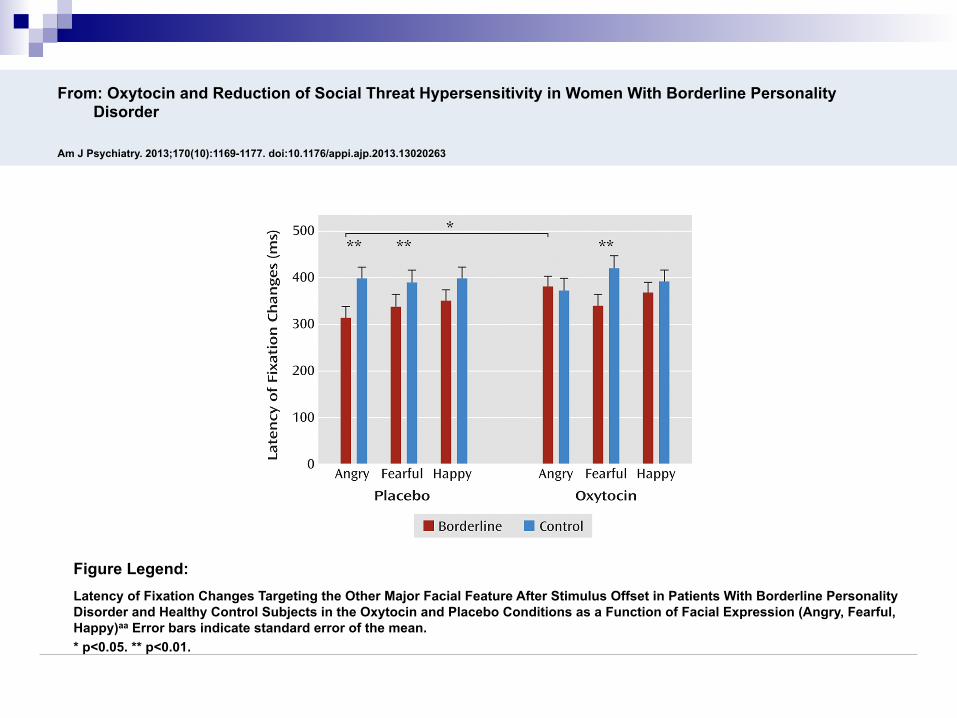
From: Oxytocin and Reduction of Social Threat Hypersensitivity in Women With Borderline Personality Disorder
Am J Psychiatry. 2013;170(10):1169-1177. doi:10.1176/appi.ajp.2013.13020263
Latency of Fixation Changes Targeting the Other Major Facial Feature After Stimulus Offset in Patients With Borderline Personality Disorder and Healthy Control Subjects in the Oxytocin and Placebo Conditions as a Function of Facial Expression (Angry, Fearful, Happy)aa Error bars indicate standard error of the mean. * p<0.05. ** p<0.01.
Figure Legend:

Assurances Game Payoff Matrix
Participant Partner Strategy A
(cooperate)
Strategy B (defect)
Strategy A (cooperate)
You get $6 Your partner gets $6
You get $4 Your partner gets $0
Strategy B
(defect)
You get $0 Your partner gets $4
You get $2 Your partner gets $2
(Kollock, 1998; Kelley et al., 2003)

Response to partner’s hypothetical cooperation in Assurances Game
“Cooperate”
“Defect”
Group x Oxytocin: F(1, 23)=4.82, p < .05 (Bartz et al)
0
0.5
1
1.5
2
2.5
BPD Normal Control
PlaceboOxytocin
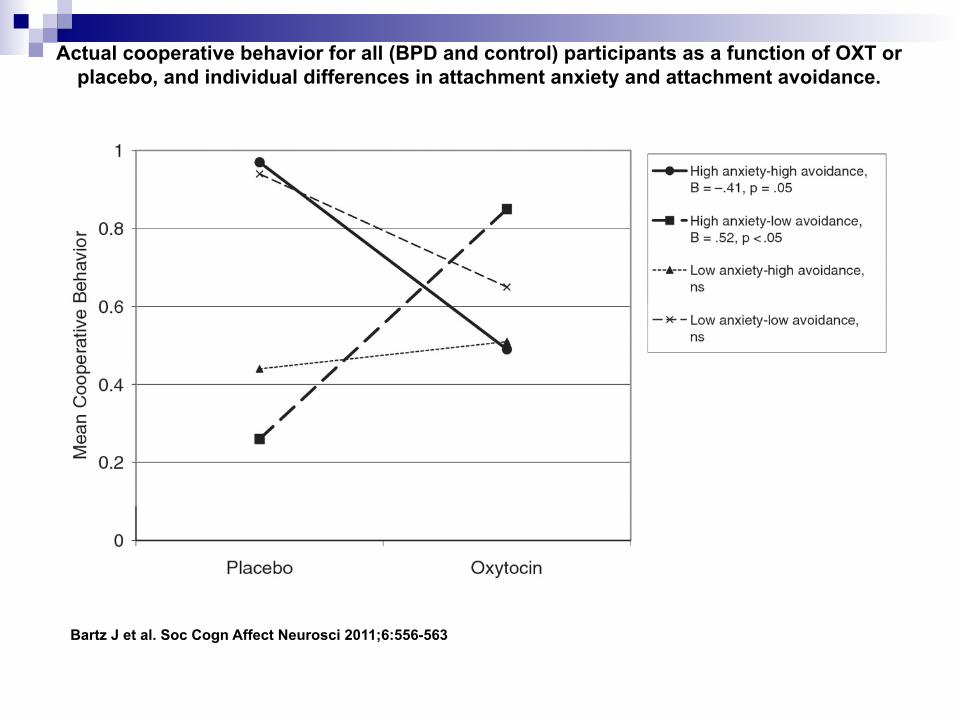
Actual cooperative behavior for all (BPD and control) participants as a function of OXT or placebo, and individual differences in attachment anxiety and attachment avoidance.
Bartz J et al. Soc Cogn Affect Neurosci 2011;6:556-563

Oxytocin and performance on Mind in the Eyes test (Domes et al., 2008)
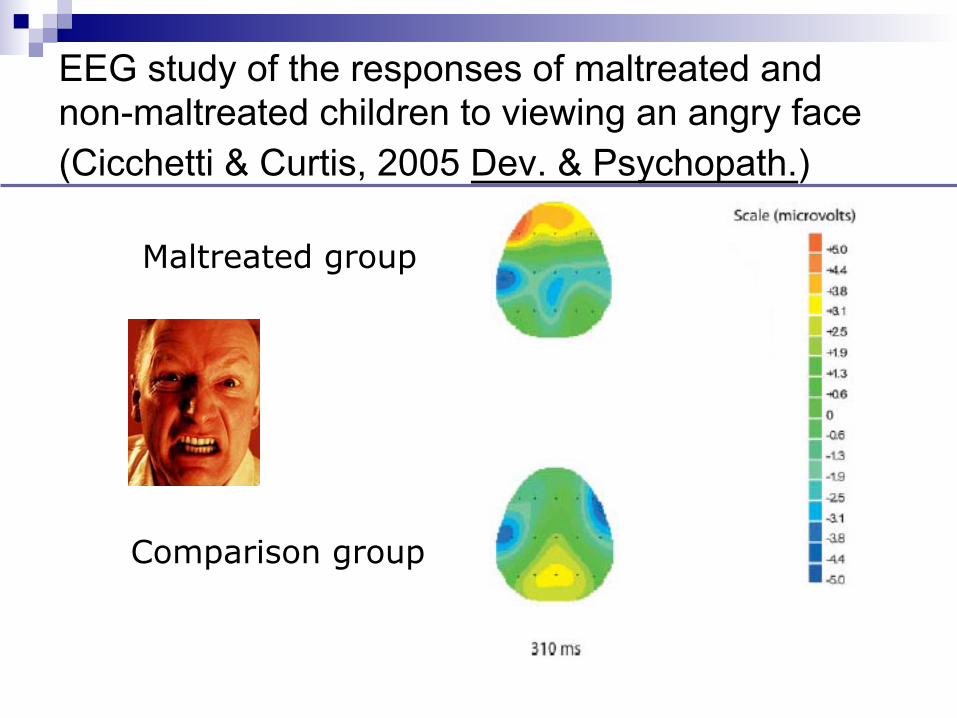
EEG study of the responses of maltreated and non-maltreated children to viewing an angry face (Cicchetti & Curtis, 2005 Dev. & Psychopath.)
Normal child Abused child Maltreated group
Comparison group

Disordered Attachment in
BPD
How Attachment Links to Affect Regulation
DISTRESS/FEAR
Exposure to Threat
Proximity seeking
Activation of attachment
The forming of an attachment bond
Down Regulation of Emotions BONDING
BONDING

The two-dimensional space defined by attachment anxiety and avoidance, showing Bartholomew’s 4 categories
High avoidance
-ve view of other
Low avoidance
+ve view of other
Low anxiety
+ve view of self
High anxiety
-ve view of self
Dismissing avoidant
Fearful avoidant
Secure Preoccupied
0
1
2
3
4
5
6
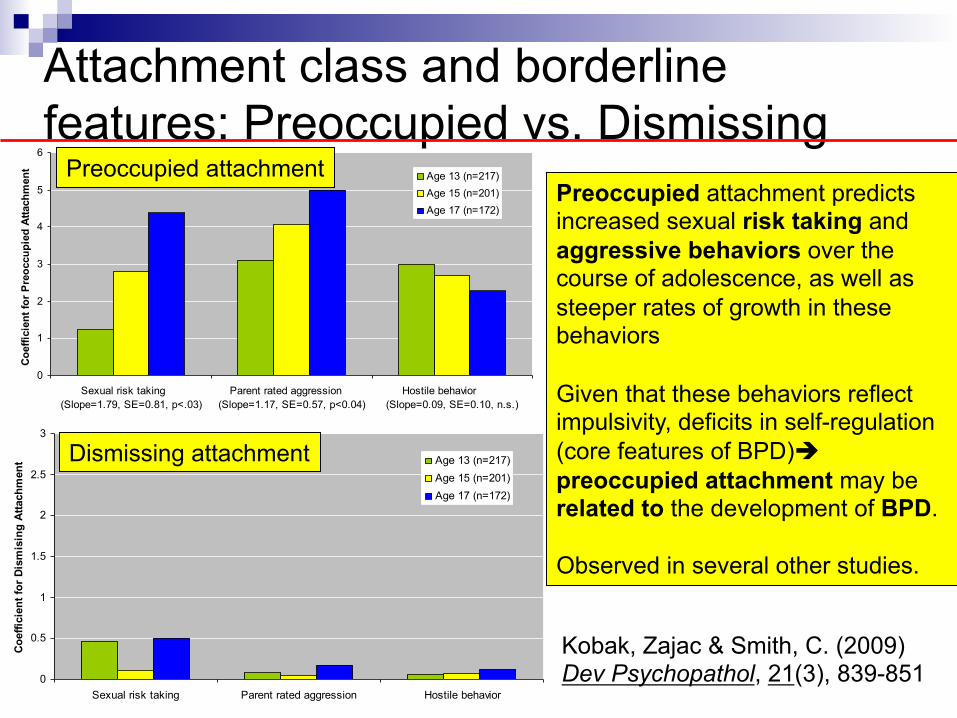
Sexual risk taking (Slope=1.79, SE=0.81, p<.03)
Parent rated aggression (Slope=1.17, SE=0.57, p<0.04)
Hostile behavior (Slope=0.09, SE=0.10, n.s.)
Coef
ficie
nt fo
r Pre
occu
pied
Atta
chm
ent
Age 13 (n=217)Age 15 (n=201)Age 17 (n=172)
0
0.5
1
1.5
2
2.5
3
Sexual risk taking Parent rated aggression Hostile behavior
Coef
ficie
nt fo
r Dis
mis
ing
Atta
chm
ent Age 13 (n=217)
Age 15 (n=201)Age 17 (n=172)
Preoccupied attachment
Attachment class and borderline features: Preoccupied vs. Dismissing
Dismissing attachment
Preoccupied attachment predicts increased sexual risk taking and aggressive behaviors over the course of adolescence, as well as steeper rates of growth in these behaviors Given that these behaviors reflect impulsivity, deficits in self-regulation (core features of BPD)è preoccupied attachment may be related to the development of BPD. Observed in several other studies.
Kobak, Zajac & Smith, C. (2009) Dev Psychopathol, 21(3), 839-851

0
1
2
3
4
5
6
Secure Preoccupied Fearful Dismissing
Commmunity Controls (n=64)
MDD (n=64)
BPD (n=109)
Self-Reported Attachment Styles, and Borderline Personality Disorder
Mea
n sc
ore
Choi-Kain et al., J Nerv Ment Dis 2009;197: 816–821

0.0
10.020.0
30.0
40.0
50.060.0
70.0
80.0
CommmunityControls
MDD BPD
Neither Preoccupied nor FearfulEither Preoccupied or FearfulBoth Preoccupied and Fearful
Self-Reported Attachment Styles, and Borderline Personality Disorder
Per
cent
5 o
r hig
her
Choi-Kain et al., J Nerv Ment Dis 2009;197: 816–821

Adult attachment, personality traits, and borderline personality disorder features in young adults Scott, Levy, & Pincus Journal of Personality Disorders, 23(3), 258–280, 2009
Structural model standardized solution
• Trait impulsivity and negative affect fully account for the relationship between attachment anxiety and BPD symptoms in young adults. • Impulsivity and negative affect may lead to BPD when they occur in the context of high levels of attachment anxiety.
Negative Affect
Impulsivity
BPD FEATURES
Attachment Anxiety
1,401 participants all 18+ years

Disordered Social interaction and neurobiology in
BPD

n PI: P. Read Montague Jnr. n Co-Investigators: Carla Sharp, Brooks King-
Casas, Peter Fonagy, Laura Lomax-Bream n Aim: To identify reliable neural signature for BPD n Total patients screened è assessed è scanned:
Ø BPD: 1,060 è 224è62 Ø Mood control: 622 è235è22 Ø Normal control: 877è398è116
n So far analysed data from 42 BPD and 26 control
Trust in Borderline Personality Disorder (H-17348)

X 3
Investor Trustee
$20
A dynamic version of the Trust game (10 rounds) BPD: The absence of Basic Trust
Camerer & Weigelt, (Econometrica, 1988) Berg, Dickhaut & McCabe (Games and Economic Behavior, 1995)
King-Casas, Sharp, Fonagy, Lomax and Montague (in preparation)

Average Repayment:
repay everything
repay nothing
repay investment (33%)
*King-Casas et al, in preparation
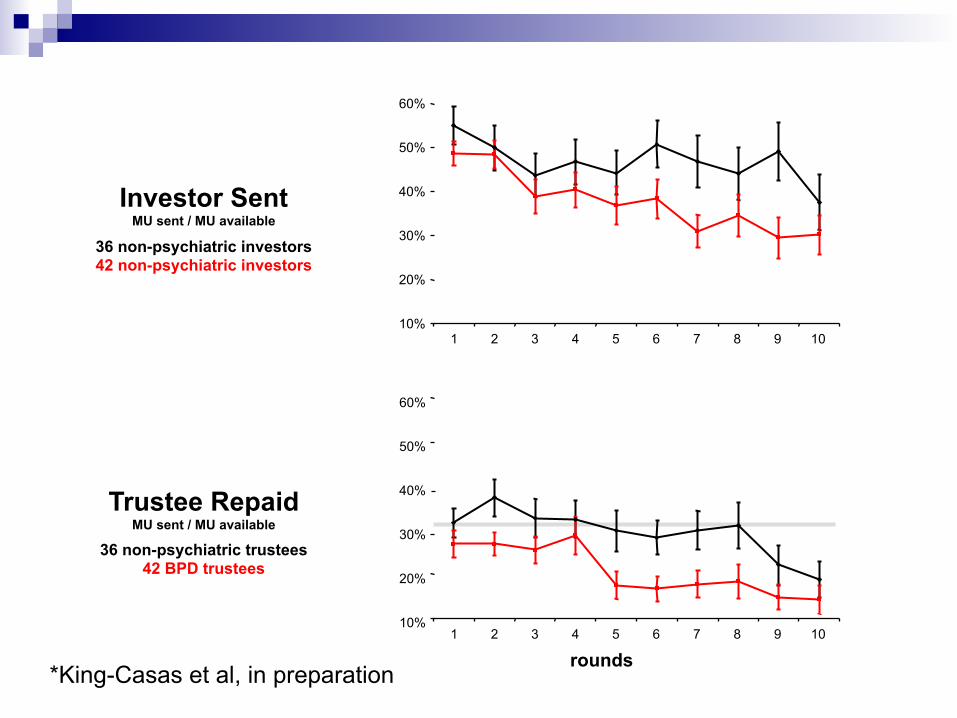
Investor Sent MU sent / MU available
36 non-psychiatric investors 42 non-psychiatric investors
Trustee Repaid MU sent / MU available
rounds
60%
50%
40%
30%
20%
10% 1 3 4 7 9 5 6 8 10 2
60%
50%
40%
30%
20%
10% 1 3 4 7 9 5 6 8 10 2
36 non-psychiatric trustees 42 BPD trustees
*King-Casas et al, in preparation

BPD (N = 42)
Healthy Control (N = 26)
King-Casas, Fonagy, Sharp, Lomax and Read,
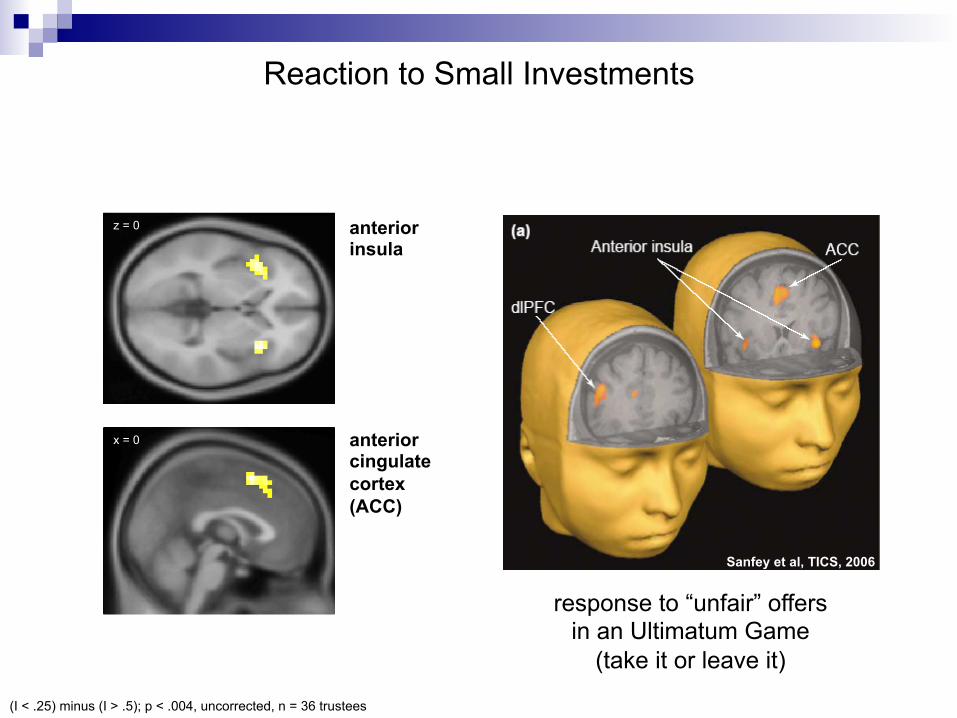
z = 0
x = 0
Reaction to Small Investments
(I < .25) minus (I > .5); p < .004, uncorrected, n = 36 trustees
anterior insula
anterior cingulate cortex (ACC)
Sanfey et al, TICS, 2006
response to “unfair” offers in an Ultimatum Game
(take it or leave it)
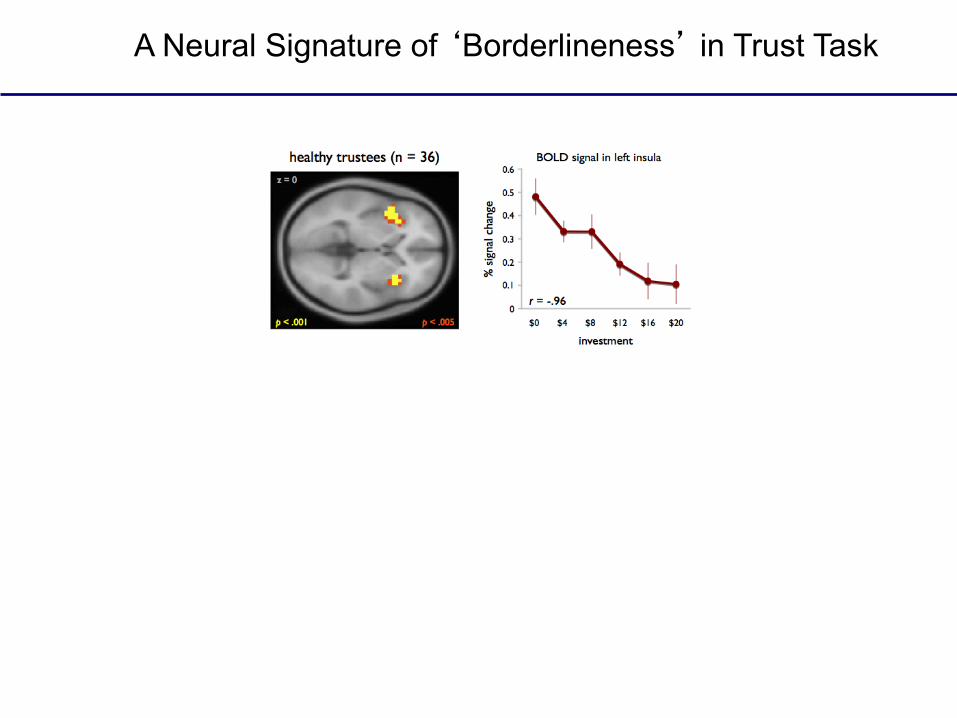
A Neural Signature of ‘Borderlineness’ in Trust Task

Diathesis-stress theories of BPD etiology n Theories suggesting an interaction between a
child’s genetic vulnerability and adverse experiences in the family environment Ø Crowell SE, Beauchaine TP, McCauley E, Smith CJ, Stevens AL, Sylvers P.
Psychological, autonomic, and serotonergic correlates of parasuicide among adolescent girls. Development and Psychopathology 2005;17(4):1105-1127.
Ø Fonagy P, Target M, Gergely G. Attachment and borderline personality disorder - A theory and some evidence. Psychiatric Clinics of North America 2000;23(1):103-+.
Ø Gunderson JG, Lyons-Ruth K. BPD'S interpersonal hypersensitivity phenotype: A gene-environment-developmental model. Journal of Personality Disorders 2008;22(1):22-41.
Ø Paris J. The development of impulsivity and suicidality in borderline personality disorder. Development and Psychopathology 2005;17(4):1091-1104.
Ø Zanarini MC, Frankenburg FR. The essential nature of borderline psychopathology. Journal of Personality Disorders 2007;21(5):518-535.
A Test of Diathesis-Stress Theories of the Etiology of Borderline Personality Disorder in a Birth Cohort of 12 Year Old Children
n Objective. To test if children with a positive family history of psychiatric disorder were more vulnerable to developing borderline personality symptoms following exposure to physical maltreatment and maternal negative expressed emotion.
n Design. Prospective longitudinal cohort study of a nationally representative birth cohort in Great Britain.
n Participants. 1,116 families with twins were followed from birth to age 12 years (retention 96%).
n Main Outcome Measure. Dimensional borderline personality symptoms and dichotomous extreme borderline group membership (dimensional symptoms ≥95th percentile).
Belsky, D., Caspi, A., Arseneault, L., Bleidorn, W., Fonagy, P., Goodman, M., et al. (2012). A Test of Diathesis-Stress Theories of the Etiology of Borderline Personality Disorder in a Birth Cohort of 12 Year Old Children. Development and Psychopathology.24, 251-65.
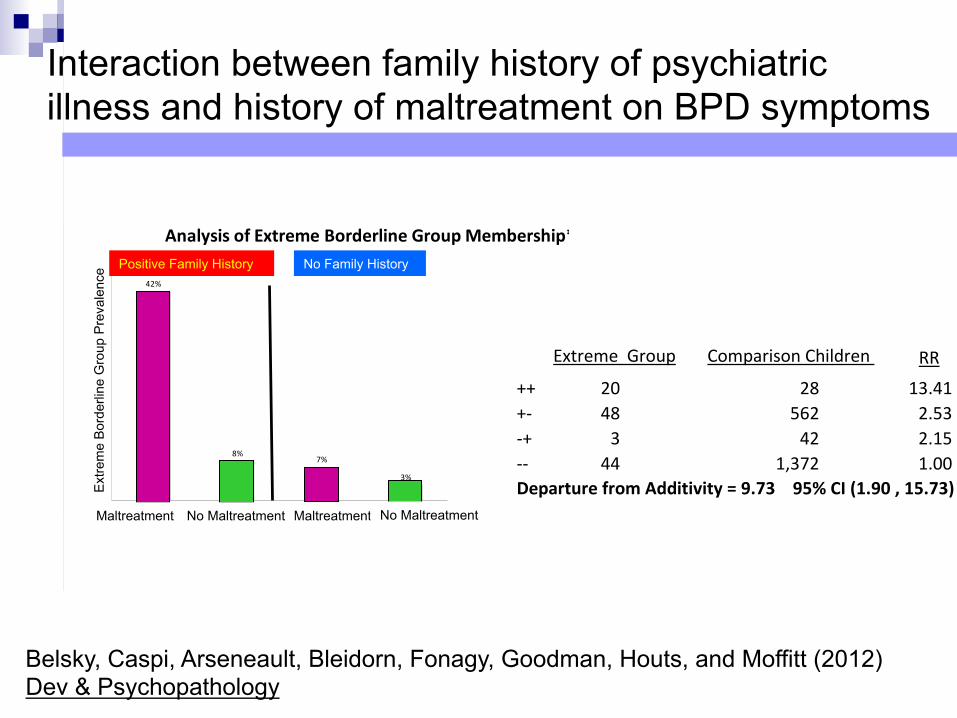
Figure 2. Diathesis-‐Stress Interaction Between Family History of Psychiatric Illness and Physical Maltreatment: The figure shows diathesis-‐stress interaction in analyses of the dimensional outcome of borderline personality related characteristics (Panel A) and the dichotomous outcome of extreme borderline group (Panel B). The convergence between these analyses indicates the interaction is not an artifact of measurement scale.
42%
8%7%
3%Extrem
e Borde
rline
Group
Prevalence
Positive Family History No Family History
Maltreatment MaltreatmentNo Maltreatment No Maltreatment
**++ Children with both risk factors, +-‐ children with positive family history only, -‐+ children with maltreatment only, -‐-‐ children with neither risk factor; Risk Ratios calculated relative to children with neither risk factor. Departure from additivity = RR[++]-‐(RR[+-‐] + RR[-‐+] -‐1). 95% confidence intervals were adjusted for non-‐independence of twin data. Confidence interval for departure from additivity estimated from 100 bootstrap repetitions.
Panel B. Analysis of Extreme Borderline Group Membership**
Extreme Group Comparison Children RR 95% CI
++ 20 28 13.41 (8.16 , 22.04)+-‐ 48 562 2.53 (1.64 , 3.92)-‐+ 3 42 2.15 (0.69 , 6.71)-‐-‐ 44 1,372 1.00Departure from Additivity = 9.73 95% CI (1.90 , 15.73)
0
4
8
12
Dimen
siona
l Borde
rline
Personality R
elated Cha
racteristics Scale Score
Maltreatment No Maltreatment Maltreatment No Maltreatment
Positive Family History No Family History
*Error bars in the graph reflect standard errors of means, adjusted for non-‐independence of twin data. Model I is an ordinary least squares regression of borderline personality related characteristics on physical maltreatment and family history. Model II adds an interaction between family history and maltreatment. Model III is a twin-‐difference analysis. A family history coefficient cannot be estimated in a twin-‐difference analysis, which controls for this and all other family-‐level factors, child sex, and child age. Model IV is a twin difference analysis including the interaction between family history and maltreatment. The interaction term from this model indexes the degree to which a difference between twins in maltreatment status is a stronger predictor of the difference between those twins in borderline symptoms in families with positive psychiatric history. Standard errors in models I and II were adjusted to account for non-‐independence of twin data. 12 of the 32 twin-‐pairs discordant for maltreatment had positive family history of psychiatric illness.
Model
Test of Diathesis-‐Stress Interaction, Between Families
I. 3.77 (0.000) 1.53 (0.000)
II. 2.09 (0.008) 1.36 (0.000) 3.33 (0.017)Test of Diathesis-‐Stress Interaction, Within Families (Twin Difference)
III. 1.65 (0.023)
IV. 0.16 (0.440) 3.84 (0.011)
Coefficient (p-‐value)Family History
-‐-‐
-‐-‐
Maltreatment Interaction
-‐-‐
Panel A. Analysis of Dimensional Borderline Personality Related Characteristics Scale Score*
Interaction between family history of psychiatric illness and history of maltreatment on BPD symptoms
Maltreatment No Maltreatment No Maltreatment Maltreatment
Ext
rem
e B
orde
rline
Gro
up P
reva
lenc
e Positive Family History No Family History
Belsky, Caspi, Arseneault, Bleidorn, Fonagy, Goodman, Houts, and Moffitt (2012) Dev & Psychopathology

Antecedents and co-morbidities of BPD related characteristics in 12 year old children (Belsky et al., 2012)
Characteristics of Children in the Extreme Borderline Group and
Comparison Children:
Means and 95% Confidence Intervals(a)
Correlations (Pearson’s r) Between Child Characteristics and Borderline Personality Related
Characteristics:__r_ 95% CI ___
Figure 1. Psychiatric Antecedents and Comorbidities of Borderline Personality Related Characteristics in 12 Year Old Children
Extreme Borderline Group (N=122)
Comparison Group (N=2,019)
Standardized Score for Child Characteristics
*p<0.05, ***p<0.001. (a) All variables were standardized to Mean = 0, SD = 1. Correlations were estimated as standardized regression coefficients. Error bars for means represent 95% confidence intervals. All estimates were adjusted for non-‐independence of twin data
Child Characteristics 5 Years Cognitive Functioning (5 yrs) IQ Executive Function Theory of Mind
Behavioral and Affective Probs (5 yrs) Interviewer Rating of Temperament Lack of Control Approach Inhibition
Mother & Teacher Rating of Impulsivity, Behavioral & Emotional Problems
Impulsivity (Mother Rating) (Teacher Rating)
Externalizing Problems (Mother Rating) (Teacher Rating)
Internalizing Problems (Mother Rating) (Teacher Rating)
Co-Occurring Psychiatric Problems at Age 12 Years
Conduct Disorder Depression Anxiety Psychotic Symptoms
BPD Group Control

Are there psychiatric conditions that require psychiatry and psychotherapy? Schizophrenia Depression/Anxiety

Family interventions in schizophrenia

Expressed emotion
n Concept originally developed in 1950’s as a generic measure of the ‘emotional climate’ in a family
n Standardized interview about family functioning (no attempt to directly elicit emotional responses)
n Operationalized ratings of various aspects of emotional expression

Expressed emotion in schizophrenia
n Early studies demonstrated the relapse was associated with : Ø critical comments Ø hostility Ø emotional overinvolvement
n Such ‘high EE’ associated with higher relapse rates, particularly with high face-to-face contact of the patient with a ‘high EE’ relative

01020304050607080
Re
lap
se R
ate
(%
)
Med+ Med- Med+ Med-
Low EEHigh EE
Relapse rates : expressed emotion, contact and medication
High Contact Low Contact
After Hirsch & Weinberger (1995)

Cochrane review on family interventions: inclusion
n Interventions for relatives or carers of those with schizophrenia or schizoaffective disorder
n Interventions tested in RCT n Intervention of at least 5 sessions, not
confined to inpatients n All included studies needed to meet
Cochrane quality criteria

Cochrane family interventions review: included studies
Not RCTs<5 sessions
Inadequate data Included
studies
Other exclusions
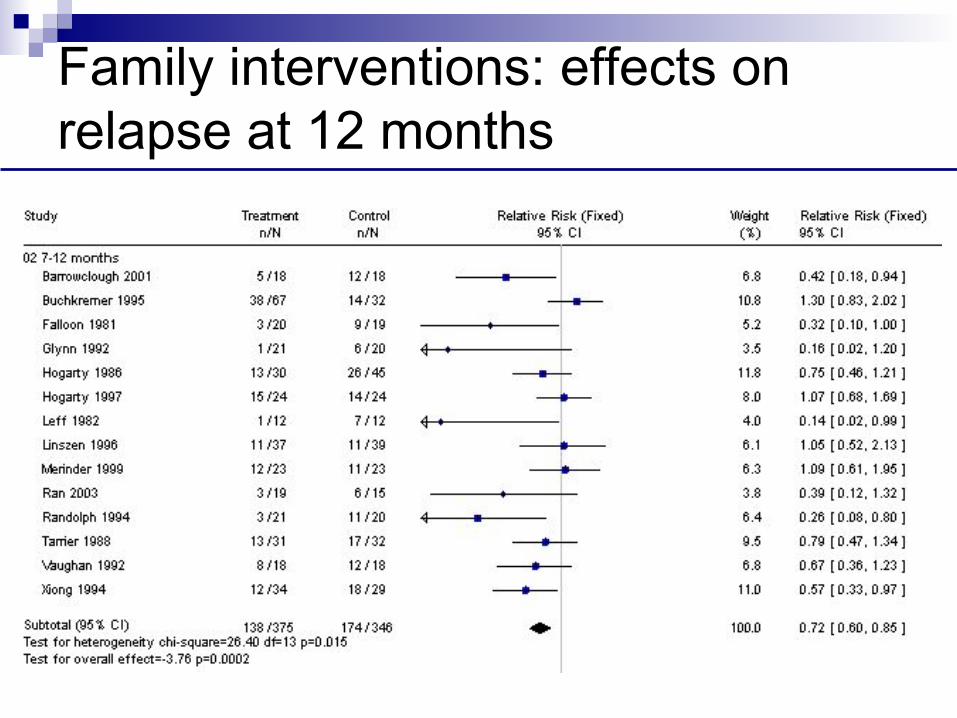
Family interventions: effects on relapse at 12 months

What does EE measure?
EXPRESSED EMOTION
SUBJECTIVE BURDEN
PATIENT’S SYMPTOMS
CARER’S PERSONALITY
King et al (2003)

What does EE measure?
EXPRESSED EMOTION
SUBJECTIVE BURDEN
PATIENT’S SYMPTOMS
CARER’S PERSONALITY
King et al (2003)

Mothers’ critical comments
CRITICAL COMMENTS
R2=0.24
SUBJECTIVE BURDEN
EXCITEMENT SYMPTOMS
NEUROTICISM
King et al (2003)
0.21 (p<0.10)
-.37
.36
.15
.04

Mothers’ over-involvement
CRITICAL COMMENTS
R2=0.25
SUBJECTIVE BURDEN
DYSPHORIA SYMPTOMS
CONSCIENT-IOUSNESS
King et al (2003)
0.04
.45
.17
.05
.21

Adherence Interventions
n Simplify regime n Depot n Psychoeducation of patient and carers n Psychological interventions n N.B. only 50% of patients with
schizophrenia think they take medication out of choice ‘v’ 95% of medical patients

Depression

Pharmacological + Psychological
n Norwegian naturalistic treatment study1 n Depression/anxiety in general practice n Best outcome for antidepressant +
counselling n Does this mean that general practice
patients should be taking antidepressants and having counselling?!
n Malt, UF et al (1999) The Norwegian naturalistic treatment study of depression in general practice (NORDEP) - 1 randomised double blind study BMJ 318:1180-84

Medication and Depression
n Medicalization of human distress n Limited evidence for aminergic theory of
depression n Safety of anti-depressants and side-effects n Recent data on young people led to
recommendations not to prescribe in children
n NICE guidelines suggest increasing caution in prescribing

Economic Impact of Psychotherapy Gabbard, GG et al (1997) The economic impact of psychotherapy: a review Am J Psychiatry 154, 147-155 n 18 studies with economic data n Beneficial economic impact on costs for a
variety of patients with severe disorders – schizophrenia, affective disorder, BPD
n Impact on work performance n Reduce duration and frequency of
psychiatric hospitalization n Best evidence for schizophrenia

Economic impact of psychotherapy
n Cost offset Ø Reduction in medical care Ø Reduction in psychiatric service use
n Cost-effectiveness Ø Quality of life Ø Quantity of life Ø Employment and productivity Ø Not same as ‘cheap’ but of ‘high value’


Costs of anti-depressants in NHS Hollinghurst et al (2005) Opportunity costs of antidepressant prescribing in England: analysis of routine data. BMJ 330 999-1000. n Costs of antidepressants £380 million in 2002 n 2.8x increase since 1991 allowing for inflation n Increase entirely due to SSRIs n This would employ >7000 psychotherapists who
could give 1.54 million treatment courses of 6 sessions each year or 0.51 if 18 sessions
n 2.43 million treatment sessions if Graduate workers trained to treat depression.

Stepped-Care for Depression - NICE
Step 1: GP, practice nurse Assessment Recognition
Mild depression
Moderate or severe depression
Treatment-resistant, recurrent, atypical and psychotic depression,
and those at significant risk
Risk to life, severe self-neglect
Step 2: Primary care team, primary care mental health
worker
Watchful waiting, guided self-help, computerised CBT, exercise, brief
psychological interventions
Step 3: Primary care team, primary care mental health
worker
Medication, psychological interventions, social support
Step 4: Mental health specialists including crisis
teams
Medication, complex psychological interventions,
combined treatments
Step 5: Inpatient care, crisis teams
Medication, combined treatments, ECT

NICE Guidelines for depression
n Initial presentation of severe depression • When patients present initially with severe depression, a
combination of antidepressants and individual CBT should be considered as the combination is more cost-effective than either treatment on its own. IPT may also be considered if preferred. B
n Couple-focused therapy • Couple-focused therapy should be considered for patients with
depression who have a regular partner and who have not benefited from a brief individual intervention. An adequate course of couple-focused therapy should be 15 to 20 sessions over 5 to 6 months. B
n Psychodynamic psychotherapy • Psychodynamic psychotherapy may be considered for the
treatment of the complex comorbidities that may be present along with depression. C

Psychotherapy alone ‘v’ psychotherapy plus pharmacotherapy Thase et al (1997) Archives of General Psychiatry 54: 1009-1015
n ‘Mega-analysis’ n 243 ‘v’ 352 patients n Recovery rates for 16 weeks therapy n Psychotherapy - cbt/pi/ipt

OUTCOME
n Less severe depression -equivalence
n Severe depression - significant difference for combined treatment


Fig. 3 Differences of BOLD responses to a priori categorized high arousal negative stimuli between BPD-patients and controls before ( t 2) and after ( t 5) DBT-treatment assessed by two sample t -tests ( p = 0,005, k = 20, uncorrected).
Knut Schnell , Sabine C. Herpertz
Effects of dialectic-behavioral-therapy on the neural correlates of affective hyperarousal in borderline personality disorder
Journal of Psychiatric Research Volume 41, Issue 10 2007 837 - 847
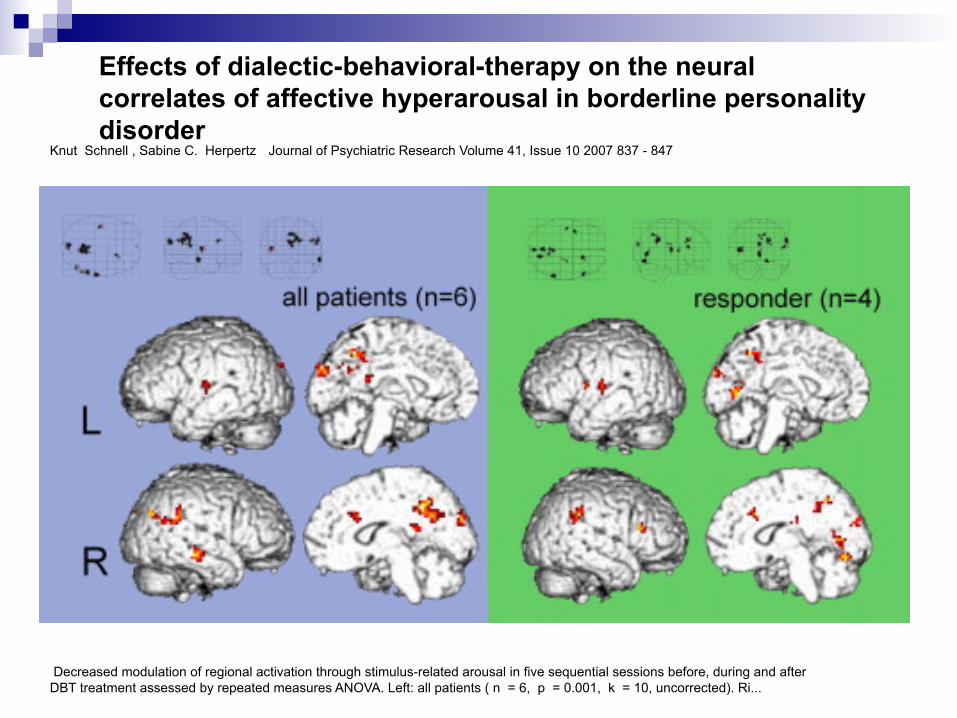
Decreased modulation of regional activation through stimulus-related arousal in five sequential sessions before, during and after DBT treatment assessed by repeated measures ANOVA. Left: all patients ( n = 6, p = 0.001, k = 10, uncorrected). Ri...
Knut Schnell , Sabine C. Herpertz
Effects of dialectic-behavioral-therapy on the neural correlates of affective hyperarousal in borderline personality disorder
Journal of Psychiatric Research Volume 41, Issue 10 2007 837 - 847

Chronic Psychiatric Conditions – non-psychotic

High utilizers of psychiatric services Guthrie et al(1999) Archives of General Psychiatry 56; 519-526
n Non-responsive to 6 months general treatment
n Mean duration of illness 5 years n 75% depression




OUTCOME
Treatment significantly better than controls in:
n Psychological distress n Social functioning n Reduction in health care use n Cost recouped in 6 months

Area all psychotherapies
the same?

What happens when you ask a room of psychotherapists whose approach is the most effective?
77
OK. What time will you be home tomorrow??
What can be done to end this unseemly behaviour?
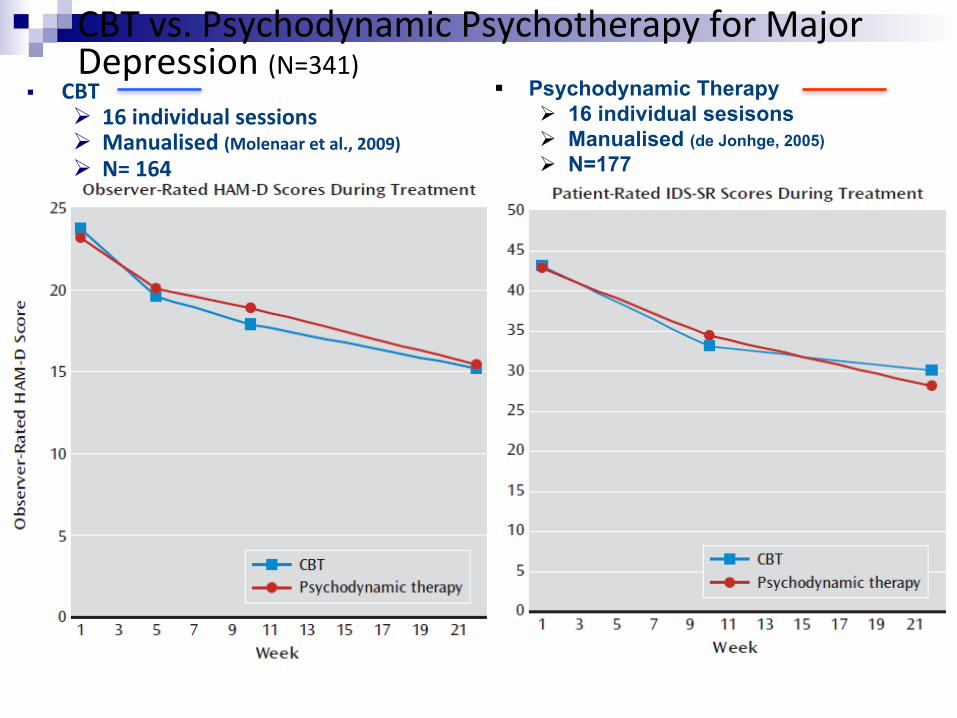
CBT vs. Psychodynamic Psychotherapy for Major Depression (N=341)
§ CBT Ø 16 individual sessions Ø Manualised (Molenaar et al., 2009) Ø N= 164
§ Psychodynamic Therapy Ø 16 individual sesisons Ø Manualised (de Jonhge, 2005) Ø N=177
Driesen et al., 2012

OutpaSents with anorexia nervosa (ANTOP) study Lancet, 2013
Lost 28%
PDT N=80
CBT N=80
TAU N=82
Lost 18% Lost 44%

Body weight and end of treatment, 3-‐months and 12-‐months follow-‐up
Outpatients with anorexia nervosa (ANTOP) study Lancet, 2013
“Common factors” research in psychotherapy
n TradiSonal common factors n Common principles n Cross modality predictors

The ParadigmaSc Common Factor n Centrality of the therapeuFc relaFonship
Ø establishment of a strong working alliance, o My therapist and I have figured out a good way to work on my sad or angry emoSons.
o My therapist and I work well together on things that bother or upset me Ø therapist capacity for understanding
o My therapist really understands what bothers or upsets me o I feel uncomfortable talking about my thoughts and feelings with my therapist
Ø feeling supported and cared about o I don’t get much support from my therapist (reversed) o I feel like my therapist is on my side and tries to help me
Ø agreement between paSent and therapist on treatment goals. o I use my 4me with my therapist to make changes in my thoughts and behavior
o I would rather not work on my problems or issues with my therapist

The working alliance controversy Castonguay et al. (1996) Depressed paSents treated with CBT
n implies technique needs to be pracSsed mindful of the interpersonal context
• alliance significantly associated with outcome • greater focus on distorted thinking associated
with poorer outcomes • effect disappears if alliance levels controlled for
took measures of: • level of alliance
• therapist focus on distorted thinking

TherapeuSc Alliance Predicts Symptom Improvement Session by Session Falkenström et al., (2013) Journal of Counseling Psychology
A sample of 646 patients (76% women, 24% men) in primary care psychotherapy Administered the Working Alliance Inventory and CORE session by session,

Reciprocal Influence of Alliance to the Group and Outcome in Day Treatment for EaSng Disorders
Tasca & Lampard (2012) Journal of Counseling Psychology 59, 507–517
SO WHY DOES IMPROVED ALLIANCE IN SESSIONt-1 LEAD TO IMPROVEMENT IN SESSIONt?

Understanding benefit from working alliance n Is it to do with learning about oneself?
Ø Most unlikely because improvement occurs between end of session and beginning of next session
n So what is it about working alliance that actually improves the paFent? Ø a bizarre delayed reverse causality? Ø aLachment mediated – but through what process? Ø opening up a social learning process that benefits the paSent between sessions

The Impact of Therapists on Treatment Outcome
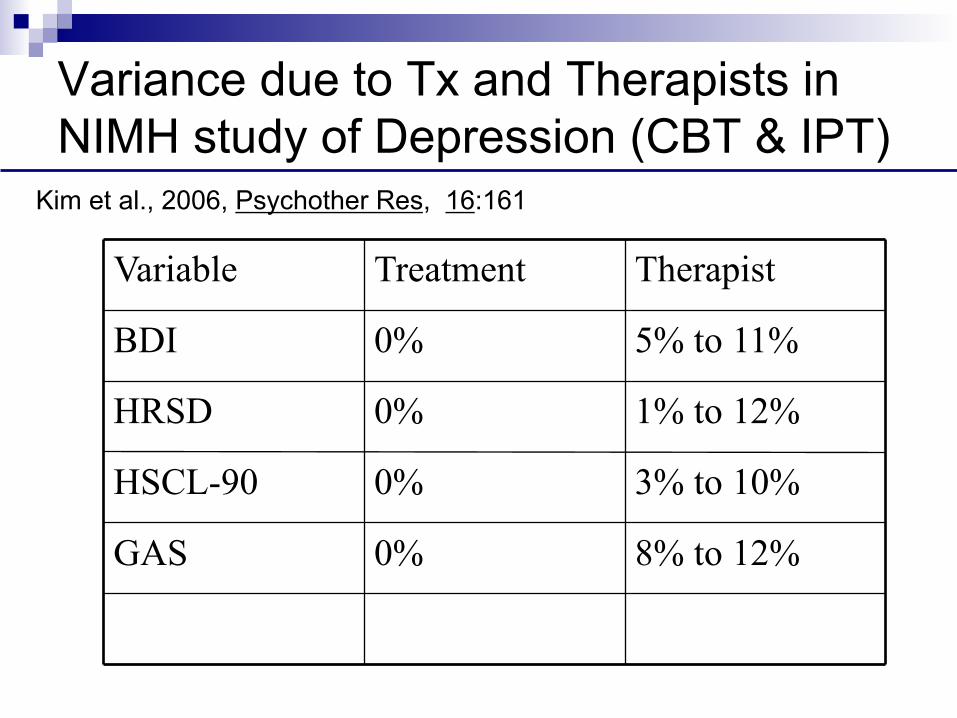
Variance due to Tx and Therapists in NIMH study of Depression (CBT & IPT)
8% to 12%
0% GAS
3% to 10% 0% HSCL-90
1% to 12% 0% HRSD
5% to 11% 0% BDI
Therapist Treatment Variable
Kim et al., 2006, Psychother Res, 16:161
Variance due to therapists in practice Wampold & Brown, JCCP, 2005 n 581 Therapists, 6146 heterogeneous
patients n Diagnosis, degree, experience: 0% variance n Medication: 1% (but also dependent on
psychotherapist) n Provider: 5% n Top quartile produced twice the effect of the
lowest quartile in subsequent year

Impact of individual therapists in routine practice Okiishi et al. 2006 (J Clin Psychol 62:9, 1157)
n 6,499 patients seen by 71 therapists
n therapists had to see at least 15 clients Ø on average saw 92
n number of sessions: range 1-203; mean 8.7
n therapists saw equivalent range of clients in terms of disturbance & presentation
n HLM used to compare ‘trajectories’ (recovery
curves) of patients using OQ45

Clients of Some Therapists Improve Faster or Slower Than Others
Session number
Scor
e on
OQ
45

n Slope of Improvement Across Therapists Unaffected by:
• therapist experience
• gender
• type of training
Ø counselling psychology, clinical psychology, social work, marital/family therapist
• orientation
Ø CBT, humanistic, psychodynamic

Outcomes for Best and Worst Performing Therapists
recovered improved deteriorated
top 10% therapists
22.4% 21.5% 5.2%
bottom 10% therapists
10.6% 17.4% 10.5%
Incidence of Harmful Effects n estimates are that 5-10% of therapy clients
deteriorate • across all orientations, client groups, modalities • in RCTs of ‘empirically supported treatments’
n rates higher than in control groups • e.g. NIMH reanalysis (Ogles et al. 1995) • 13/162 (8%) deteriorated, all in active treatments
n in Lambert’s work therapists tend to be poor at: Ø predicting who will do badly Ø recognising failing therapies

Reducing the Harmful Effects of Psychotherapy: The work of Lambert (2009) n Across studies the rate of observed deterioration in
psychotherapy was 10-25% with young people n Some therapists have rates of deterioration of
around 50% and their treatment is NEVER associated with recovery
n Introduction of outcome tracking (session by session monitoring) Ø Early warning when patient goes off trajectory
n Therapists randomized to feedback vs no-feedback Ø Deterioration reduced by 50% Ø Recovery improves by 50% Ø Average therapy is shorter Ø Patients who show early negative response receive
longer and more effective treatment

Do no harm… outcomes informed care
n Most therapists see themselves as better than average:
Dew & Riemer (2003, 16th Annual Research Conference, University of South Florida)
n Outcomes informed care may be a critical way of linking the EBP approach and practice based evidence
• 143 counselors asked to grade their job performance on scale from A+ to F • 66% rate themselves as A or better • none rated themselves as below average
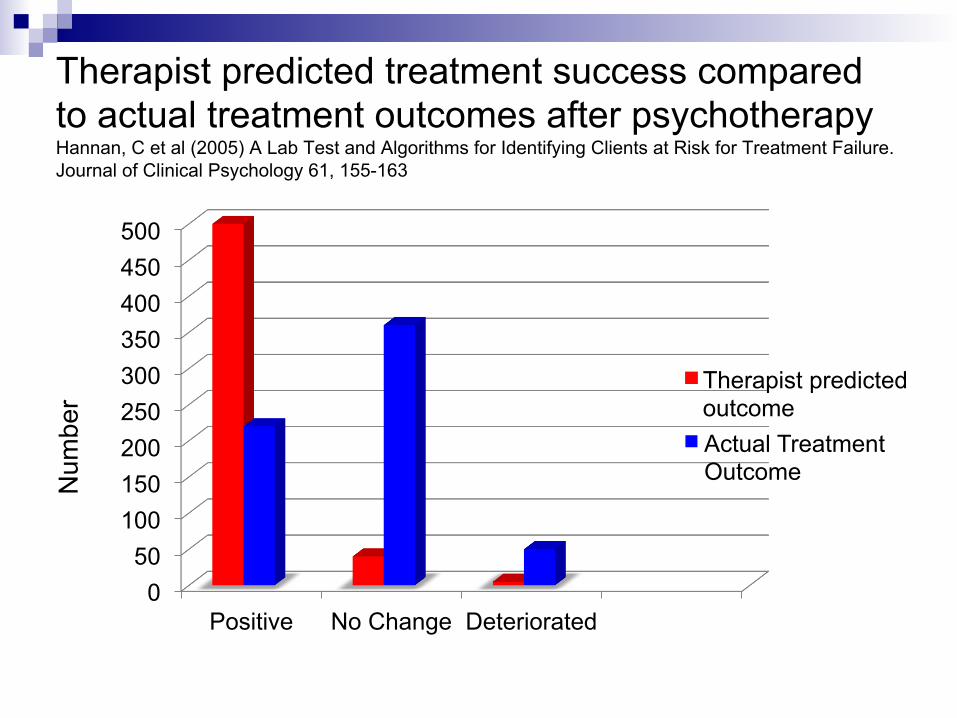
Therapist predicted treatment success compared to actual treatment outcomes after psychotherapy Hannan, C et al (2005) A Lab Test and Algorithms for Identifying Clients at Risk for Treatment Failure. Journal of Clinical Psychology 61, 155-163
0 50
100 150 200 250 300 350 400 450 500
Positive No Change Deteriorated
Therapist predicted outcome Actual Treatment Outcome N
umbe
r
2
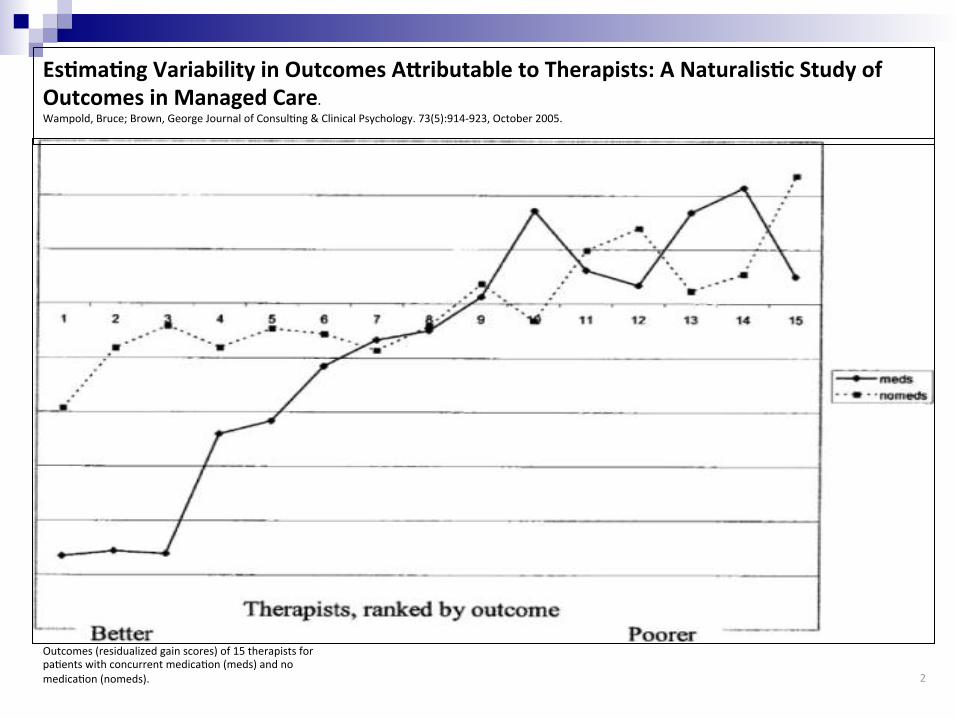
EsFmaFng Variability in Outcomes ALributable to Therapists: A NaturalisFc Study of Outcomes in Managed Care. Wampold, Bruce; Brown, George Journal of ConsulSng & Clinical Psychology. 73(5):914-‐923, October 2005.
Outcomes (residualized gain scores) of 15 therapists for paSents with concurrent medicaSon (meds) and no medicaSon (nomeds).

BDI residual gain score as a function of type of treatment (PLA-CM v. IMI-CM) for each psychiatrist (1–9). Note that lower scores indicate better outcomes; negative residualized gain scores indicate better than average outcomes.
Kevin M. McKay , Zac E. Imel , Bruce E. Wampold Journal of Affective Disorders Volume 92, Issues 2–3 2006 287 - 290
Psychiatrist effects in the psychopharmacological treatment of depression

Psychiatry is Psychotherapy
n Neurobiology, psychology, social cognition and relationships interweave to disrupt mental processing
n Mental Disorders require complex treatment to optimize outcome
n The person of the treater is essential n Psychiatry is a relational enterprise


















