Psychosocial Test # 1 Review - Weebly€¦ · Web viewPsychosocial Test # 1 Review . Psychosocial...
22
Psychosocial Test # 1 Review Psychosocial Nursing ● Psychosocial Nursing ○ Interventions to assist individuals, families, groups who are having difficulty dealing with emotions and who are having trouble coping with the emotional aspects of illness with life crises that affect health and lives and disorders ○ Focus on effects of stress ○ How to help folks to function at their maximum wellness ● Psychosocial Nursing Care ○ Care for individuals, families, groups, communities ○ Focus on effects of stress ○ How to help folks to function at their maximum wellness ○ Health promotion & maintenance ○ Screening ○ Assessment ○ Stress & Stress Management ○ Crisis & Crisis Intervention ○ Cope with emotions that influence health ○ Cope with emotional aspects of illness ○ Create a therapeutic environment or “milieu” for healing ○ Promote self-care & independence ○ Administer medications/treatments & monitor the effects ○ Provide client education ○ Evaluate client progress in goal attainment ● Psychosocial Nursing Roles ○ Caregivers ○ Counselors (As a nurse should be able to do general counseling) ○ Educators ○ Managers ○ Consultants ○ Researchers ○ Advocates/Liaisons for your patient ○ They practice everywhere- acute inpatient, critical care, community, in a practice, mobile health clinic, hospice, department of mental health in community clinic, school nurse, etc. ● Healer Characteristics ○ Gentleness of spirit ○ Compassion for others ○ Respect for the dignity of others ○ Respect for the choices of others ○ Mindfulness of the potential of the healing act to release the healing energies of the other ● Centering ○ focusing; helping to capture the frontal lobe ○ Pick a focal point (looking at something) to help to center ○ Anxiety, anger are transferable so make sure you aren’t picking that up from pt ○ Have a neutral facial affect ○ Breathe in through nose and out through mouth, less frontal lobe becoming anxious
Transcript of Psychosocial Test # 1 Review - Weebly€¦ · Web viewPsychosocial Test # 1 Review . Psychosocial...
Psychosocial Test # 1 Review
Psychosocial Nursing● Psychosocial Nursing
○ Interventions to assist individuals, families, groups who are having difficulty dealing with emotions and who are having trouble coping with the emotional aspects of illness with life crises that affect health and lives and disorders
○ Focus on effects of stress ○ How to help folks to function at their maximum wellness
● Psychosocial Nursing Care ○ Care for individuals, families, groups, communities○ Focus on effects of stress ○ How to help folks to function at their maximum wellness ○ Health promotion & maintenance○ Screening○ Assessment ○ Stress & Stress Management○ Crisis & Crisis Intervention○ Cope with emotions that influence health○ Cope with emotional aspects of illness○ Create a therapeutic environment or “milieu” for healing ○ Promote self-care & independence○ Administer medications/treatments & monitor the effects ○ Provide client education ○ Evaluate client progress in goal attainment
● Psychosocial Nursing Roles○ Caregivers○ Counselors (As a nurse should be able to do general counseling) ○ Educators○ Managers○ Consultants○ Researchers○ Advocates/Liaisons for your patient ○ They practice everywhere- acute inpatient, critical care, community, in a practice, mobile
health clinic, hospice, department of mental health in community clinic, school nurse, etc.● Healer Characteristics
○ Gentleness of spirit○ Compassion for others○ Respect for the dignity of others○ Respect for the choices of others○ Mindfulness of the potential of the healing act to release the healing energies of the other
● Centering○ focusing; helping to capture the frontal lobe○ Pick a focal point (looking at something) to help to center○ Anxiety, anger are transferable so make sure you aren’t picking that up from pt○ Have a neutral facial affect○ Breathe in through nose and out through mouth, less frontal lobe becoming anxious
● Healing Listening○ Truly engaged with pt○ Taking in everything they share with you ○ Not jumping ahead and thinking about what you’ll say back
Mind-Body-Spirit ● Alternative medicine [also known as health care practices]● Complementary medicine [also known as health care practices]● Holistic Care● MIND: cognition (thoughts), perception (how do they see it), memory, judgment, regulation &
control of emotions and impulses● BODY: the whole of all anatomical parts and physiological functions ● SPIRIT: the vital center, the essence of the whole being● Common Uses for Alternative Therapies
○ Pain
○ Insomnia○ Stress & Anxiety○ Depression ○ Mental (cognitive) decline
● Complementary/Alternative Systems of Health Care○ Ethnocultural practices ○ Folk remedies: ask what pt is using
■ Chicken soup→ cold ■ Honey → decreases allergies ■ Green tea → antioxidants ■ Apples → vitamin C
○ Herbal medications: ask what pt is taking; be aware of variation from batch to batch and company to company
○ FDA vs. German Formulary ■ German Formulary: rates and evaluates herbal products ■ The US doesn’t have the same quality control
○ Teaching Points for Patients■ Complement vs alternative
● Therapies and practices are called alternative when used alone or with other alternative therapies
● Therapies are called complementary when used with conventional therapies■ Choose reliable source■ Choose reliable form--tincture, freeze-dried■ More is NOT better!■ Watch for allergic/adverse reactions■ Inform Health Care Providers
● Spiritual needs/practices ○ Needs: meaning/purpose, faith, hope, love forgiveness○ Religion○ Application
■ Spiritual Assessment ■ Nursing Dxs
● Spiritual Distress/Risk for Spiritual Distress○ Is the state in which the individual or group experiences or is at risk of
experiencing a disturbance in the belief or value system which provides strength, hope and meaning to life (NANDA)
● Impaired Religiosity/Risk for Impaired Religiosity ● Hopelessness
■ Nursing CareVideo Notes
● Video used medical care → think health care!● Mind-body-spirit approach● Hope influences physical health→ expand to all aspects of health● Your body reacts to what’s in your mind● Thoughts & feelings impact patients’...
○ health ○ illness○ acute pain○ chronic pain○ infection○ onset of premature labor○ wound healing (low stress group healed 9 days faster)○ preparation for surgery (listened for 1 week to audio recording)○ response to painful procedure (lumbar puncture)○ reaction to life stresses○ immune function
● Benefits of mind-body-spirit approach○ decreased fear & anxiety○ relaxation○ less pain○ faster healing cost saving
● Examples of complementary treatments○ centering & relaxation○ breathing○ touch○ visualization/guided imagery○ yoga○ meditation○ prayer○ exercise especially outdoors
● Treatments○ individuals respond differently○ personal reactivity varies○ use a variety of techniques○ treatment effect can be measured (EEG, MRI, decreased VS, muscle relaxation)○ use analogy patients are familiar with such as a dimmer switch○ practice improves response
● Group○ sharing○ support○ education○ skill building
● Family involvement & supportNurse-Patient Relationship
● Social vs therapeutic ○ Caring○ Mutuality○ Empathy vs. sympathy
■ Empathy is trying to put yourself in their shoes (you empathize with someone)■ Sympathy is just feeling sorry for them (you sympathize for someone)
○ Trust○ Unconditional acceptance○ Authenticity
■ Own the way you feel ○ Consistency
■ Tell them you will be back in 5-10 minutes and if you can’t then you send someone to let the pt know
■ Consistency builds trust ○ Respect○ Genuineness
■ Don’t try to fake that you care about them○ Rapport
■ Some people will trust you immediately, but others will take time○ Empowerment
■ Stay calm● Therapeutic contract
○ Is a time-bound alliance between nurse and patient, consciously entered into and characterized by respect, acceptance, empathy and genuineness.
Phases of NP Relationship ● Pre-interaction
○ Only phase when it is just the nurse alone → no pt in this phase○ Goal: explore self perceptions, and build knowledge/skills○ Tasks:
■ Building knowledge base■ Building skills■ Obtaining information about the client■ Explore personal beliefs, feelings, etc. ■ Analyze personal strengths and challenges
● Orientation ○ when the nurse and pt first come together ○ Goals: establish trust and formulate contract for intervention○ Roles:
■ Nurse as stranger■ Client as stranger ■ Acknowledge the pt (introduce yourself), Duration (set structure), Explain (what you
are going to be doing), Thank the pt ○ tasks:
■ Establish rapport with pt ● When you introduce yourself you decide what information you’re going to
share with the patient ■ Demonstrate acceptance of the pt■ Begin to develop trust■ Assess pts strengths & limitations■ Formulate nursing diagnosis■ Set mutually agreeable goals for pt and relationship■ Develop realistic plan of action for meeting goals■ Exploring feelings of both nurse & pt —anxiety!■ Establishing therapeutic boundaries■ Establishing a contract for intervention that details the expectations & responsibilities
of the nurse & pt○ Therapeutic Communication
■ Treat the patient as an adult and interact with them on that level ■ Things we say can come across “parent-like” and corresponding style to that is the
child’s response ● Don’t ask “did you finish your breakfast?” ● Ask “How was your breakfast today?”
■ Child part of us is the part that enjoys things and gets in the moment ● “I don’t want to eat that, I hate that”
■ Offering general leads■ Clarifying■ Accepting■ Silence■ Seeking clarification■ Exploring■ Encouraging comparisons
○ Indicators of Completion?■ Initial trust develops■ Pt verbalizes some thoughts & feelings■ Pt identifies needs, problems, areas for growth■ Strengths assessed■ Challenges assessed■ Goals for the relationship are established
● Working Phase○ Goal: Promote patient change ○ Nursing Roles:
■ Resource person■ Teacher - education ■ Leader■ Surrogate
● Family is across the country and can’t be there to hold their hand but you are there and can be there for them
■ Advocate
■ Counselor○ Tasks
■ Gather data on sx, feelings, relationships, past history, history of present health concern
■ Focus on here & now● Spend time on history, but then on focus is forward
■ Maintain trust & rapport ■ Promote pt insight and perception of reality■ Explore past attempts to cope with problem(s) and outcomes ■ Assist pt to identify alternative coping strategies■ Develop action plan & implement ■ Overcome resistance behaviors of pt as level of anxiety rises in response to
discussion of painful issues■ Continuous evaluation of progress toward goal attainment
○ Barriers within the pt ■ Transference - pt has strong feelings toward you as the nurse based on prior
experiences with other people in their life● Unconscious; don’t realize they’re doing it● Strongly positive or negative
■ Resistance - driving forces to change; do something you don’t necessarily want to do; not as easy
● We hope the driving forces are stronger than resistant● Strongest = when pt first admitted, when pt in crisis
■ Boundaries - Boundary violations & Limit Setting ○ Barriers within the nurse
■ Countertransference - happens for us as the nurse● Ex: Positive = always in the room, taking extra time, going extra mile for
them, may remind you of someone you have a positive relationship with■ Self Disclosure
○ Therapeutic Communication■ Explore outcomes of past coping strategies■ Examine alternatives■ Assist pt to reframe beliefs■ Role play – rehearse new ways
● Have them explain to you■ Interpretation – use sparingly!
● When you tell pt what you think■ Address issues directly/confrontation -- be gentle!!
○ Indicators of Completion?■ Change in appearance■ Uses new strategies to cope with anxiety
● Ask “how did that go?”■ Time is noticed during the 1:1 -- “know it’s about time for you to leave?”
● Signal that the time is coming to a close■ Recognizes nurse as unique person■ Associates what is being discussed with past 1:1 (if applicable)■ Resistance decreases
● Termination ○ When start to prepare pt? “I am going to be your nurse from 7 am to tonight, i’ll be your
nurse until you’re discharged”○ Goal:
■ Evaluate goal attainment - pt always goes first to describe what they’ve attained, then YOU add additional info
■ Ensure therapeutic closure & positive experience for the patient ○ Roles: same as working phase ○ Tasks
■ Bringing therapeutic relationship to an end when: ● progress has been made toward mutually set goals● plan for continuing care or for assistance during stressful life experiences is
mutually established by nurse & client ● feelings about termination are explored & recognized
○ Therapeutic Communication■ Pt reviews what has been accomplished■ Nurse reviews what has been accomplished■ Explore feelings about separation■ Discuss plans for future
● Follow up appointments ● Medication and discharge teaching ● Anticipatory guidance : “What will you do if…”
○ If something is wrong, determine the course of action → go to ER, urgent care, etc.
■ Express own feelings ○ Issues?
■ May see the return of s/sx ■ Increase in s/sx ■ Development of new s/sx (new s/sx means they get to stay) ■ separation anxiety
○ Indicators of Completion?■ Demonstrates new thoughts, feelings, behaviors■ Anxiety is low■ Knows s/s when should contact hcp■ Can identify resources ■ Discharge
Therapeutic Communication● Verbal
○ words ○ paralanguage
■ VOLUME: are they hard of hearing? ■ RATE: fast, medium, slow■ RHYTHM: regular rhythm
● Form a connection b/t pt and nurse ■ PITCH OF SPEECH
● Anxious: higher ● Nonverbal
○ 80-90% of all communication is nonverbal ○ Eye Gaze
■ Most powerful form of nonverbal com■ Sustain, but do not stare■ Note what the patient was sharing when they looked away/at you■ Often when people look up they are thinking ■ Up and to left → telling the truth■ Up and to right → could be making things up■ When adults close eyes, may be about to share significant information
○ Facial Affect- neutral■ With older adults, sad can be confused with angry due to wrinkles
○ Hand Gestures■ Manipulators- manipulate body ■ Illustrators-such as moving hands
● Helps with encoding and decoding of speech■ Emblems- universal gestures
● Thumbs up- positive emblem● Number 1
○ Silent Pauses in Speech■ Very powerful ■ Learn to become comfortable with silence ■ Some need more time to respond than others■ Often times, after a period of silence, when the pt breaks the silence, what they say
is significant■ Never interrupt
○ Proxemics (personal space)
■ Intimate distance= 0-18 inches- length of arm■ Personal distance= 18 inches - 4 ft■ Social distance= 4-12 ft■ Public distance= exceeds 12 ft■ Sitting across is aggressive ■ 90 degree angle is best■ Lean slightly forward to be engaged
○ Artifacts - Clothing, Jewelry■ Body art, dress
● Meta-communication - relationship aspects (Warm and caring? Uncomfortable?)● Body Language (NVB) communication blockers● Active Listening
○ Actively listening and focusing on the pt → continually assessing them ○ Things that affect active listening: tired, zoning out, hungry, distraction, how your feeling
(what’s going on with you), time limitations (feeling rushed), pain○ Focusing objective and empathic attention on all behaviors expressed
■ Both client and nurse verbal and nonverbal behaviors■ Listen for content■ Observe for process
○ Purpose■ Minimizes distractions■ Conveys interest■ Conveys objectivity
○ General Outcomes■ Contributes to effective NPR■ Encourages trust■ Provides information about client■ Identifies patient level of functioning■ Identifies themes or cues to patient behavior problems
● Relevant to pt needs both cognitive & emotional → Thought needs and emotional needs● Purposeful & direct● Able to be understood by pt/family● Culturally sensitive● Congruent (V & NV)
○ It goes together ○ Emotional tone fits the words that you say
● Encourages response by pt● Repeated as needed for pt’s understanding● Communication Facilitators
○ Some of us take in information best visually or auditorily■ Listen to what the pt is saying ■ Using a lot of “I see” or hearing words or are they tactile (kinesthetic learners)■ If you can mirror that then it will help you to establish rapport
○ Present focus (here & now)○ Reinforce strengths○ Confront & set limits
■ Directly addressing → bringing it to the other person’s attention○ Redirection
■ Bringing things back to topic○ Modeling
■ Healthy communication and interaction ○ Humor
■ Need to be very sensitive, so that you are laughing WITH the person and you aren’t laughing AT them
○ Offering information■ Pt teaching
○ Don’t reflect back too much ○ Testing - not okay to give the patient your phone number
■ Not healthy for the patient or the nurse■ If patient gets the email, let your instructor know in order to reset the professional
boundary ● Feedback
○ Giving information about how an individual is perceived by another○ Descriptive; not evaluative
○ Focuses on patient behavior○ Specific rather than general○ Directed toward behavior the patient is able to modify○ Most useful when given immediately ○ Start with positive
● Barriers ○ Environment: Noise, privacy, temperature, crowded○ Within the patient: stubborn, personal characteristics, sad, anxious, angry, pain ○ Within the nurse: same things for the nurse as well
● Assertive Communication (more info in week 2 notes) ○ Behavior that enables individuals to…
■ Act in their own best interests■ Stand up for themselves without undue anxiety■ Express their honest feelings comfortably■ Exercise their own rights without denying the rights of others
○ Honesty is basic to assertive behavior and is expressed in a manner that promotes self-respect and respect for others
● short version of the Truth Model ○ “When you….”○ “I feel…”○ “Because…”○ “Would you or In the future, would you…”
● Nurse’s Personal Qualities & areas for self assessmentCultural Sensitivity & cultural competence
● Giger & Davidhizar (1988)○ All of these impact nurse/pt relationship○ Communication- Verbal, paralanguage, nonverbal – eye gaze, touch○ Space- Particularly the comfort level related to personal space - comfort in conversation,
proximity to others, body movement, perception of space.○ Social Organizations - Patterns of cultural behavior learned through enculturation.
Recognize and accept that individuals from culturally diverse backgrounds may desire varying degrees of acculturation into the dominant culture. Life cycle factors must be considered.
○ Time- Concept of the passage of time, duration of time, and points in time.○ Environmental Control- Abilities of persons to control nature. Health practices, values,
definitions of health and illness.○ Biological Variation- Racially related body structure, skin color, hair texture, and other
physical characteristics; enzymatic and genetic variations; electrocardiographic patterns; susceptibility to disease; nutritional preferences and deficiencies, and psychological characteristics.
● Boyle and Andrews (1989)○ History of the origins of the patient's' culture. ○ Value orientations, including view of the world,
ethics, and norms and standards of behavior as well as attitudes about time, work, money, education, beauty, strength, and change.
○ Interpersonal relationships, including family patterns, demeanor, and roles and relationships.
○ Communication patterns and forms.○ Religion and magic.○ Social systems, including economic values,
political systems, and educational patterns.○ Diet and food habits.○ Health and illness belief systems, including
behaviors, decision making, and use of healthcare providers.
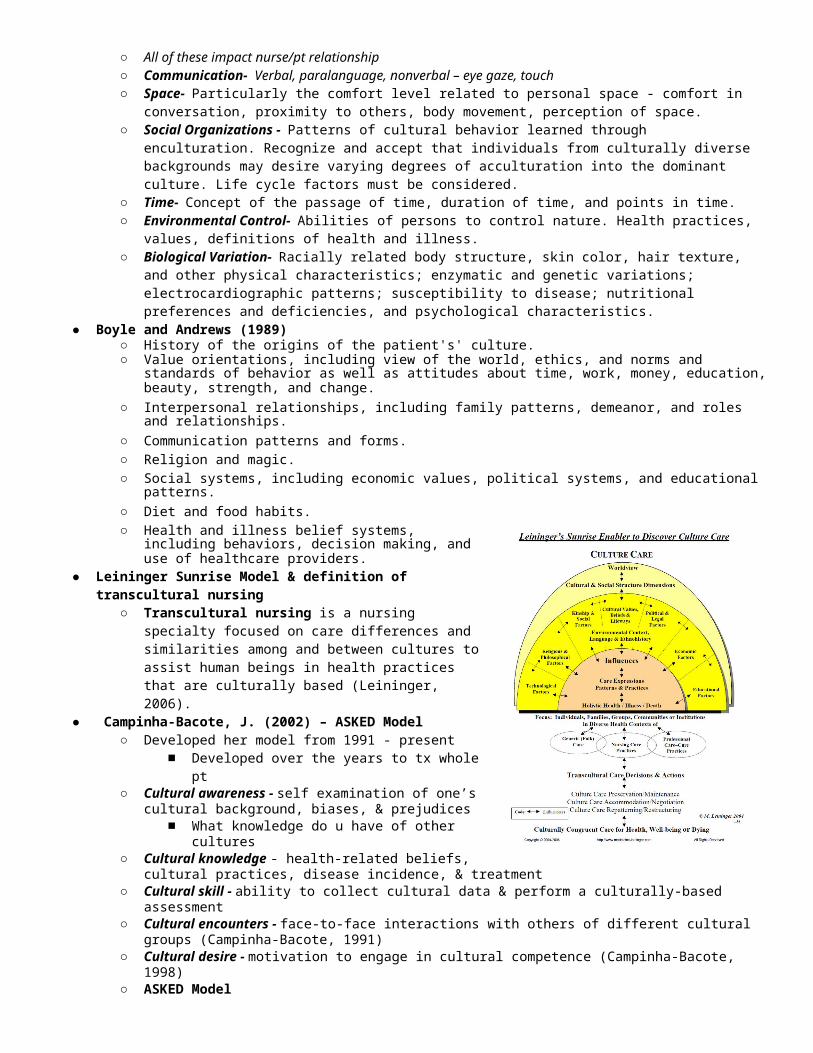
● Leininger Sunrise Model & definition of transcultural nursing
○ Transcultural nursing is a nursing specialty focused on care differences and similarities among and between cultures to assist human
beings in health practices that are culturally based (Leininger, 2006). ● Campinha-Bacote, J. (2002) – ASKED Model
○ Developed her model from 1991 - present■ Developed over the years to tx whole pt
○ Cultural awareness - self examination of one’s cultural background, biases, & prejudices■ What knowledge do u have of other cultures
○ Cultural knowledge - health-related beliefs, cultural practices, disease incidence, & treatment
○ Cultural skill - ability to collect cultural data & perform a culturally-based assessment○ Cultural encounters - face-to-face interactions with others of different cultural groups
(Campinha-Bacote, 1991)○ Cultural desire - motivation to engage in cultural competence (Campinha-Bacote, 1998)○ ASKED Model
■ A wareness: Am I aware of my biases and prejudices towards other cultural groups, as well as racism and other "isms" in healthcare?
■ S kill: Do I have the skill of conducting a cultural assessment in a sensitive manner?■ K nowledge: Am I knowledgeable about the worldviews of different cultural and
ethnic groups, as well as knowledge in the field of biocultural ecology?■ E ncounters: Do I seek out face-to-face and other types of interactions with
individuals who are different from myself?■ D esire: Do I really "want to" become culturally competent?
● American Association of Colleges of Nursing (2008) – review 5 competencies○ Competency 1: Apply knowledge of social and cultural factors that affect nursing and
health care across multiple contexts.○ Competency 2: Use relevant data sources and best evidence in providing culturally
competent care.○ Competency 3: Promote achievement of safe and quality outcomes of care for diverse
populations.○ Competency 4: Advocate for social justice, including commitment to the health of
vulnerable populations and the elimination of health disparities.○ Competency 5: Participate in continuous cultural competence development.
● Nursing Student Challenges – stages 1-4○ Stage One:
■ Selective inattention■ Obsession with detail■ Dissociation of theory from practice■ Avoidance behavior
○ Stage Two:■ Over identification with clients■ Unable to identify client's problems because of denial■ Concrete thinking
○ Stage Three:■ Hostility toward staff and/or faculty■ Feelings of anger, frustration, omnipotence
○ Stage Four:■ Get a better sense of awareness ■ Anxiety decreases■ Accepts client, listens actively, use nursing process■ Interact with them in a therapeutic way
Communication with Special Populations ● Interpreters
○ Thank the interpreter for providing services. This is the only time you should directly address the interpreter until the end of the session
○ Make sure room is evenly lit and that light isn’t glaring in patient’s eyes○ Place the interpreter beside & slightly behind the nurse so that the patient can see both of
you at the same time○ Face the patient directly for the greeting & the entire conversation○ Keep hands away from face, especially your mouth○ Use gestures to show the pt. where to sit or what to do○ Directly address the patient, “Mrs. Jones, How are you feeling today” vs “Please ask the
patient how she is feeling today.” ○ Speak normally & clearly; don’t shout or over enunciate○ Avoid or explain health care terms○ Clearly express a change in topic○ Validate the pts. Understanding periodically○ At the end of the interpreting, thank the interpreter
● Language
○ Avoid selecting an interpreter from a rival faction or group○ Avoid selecting an interpreter from a sex, ages or socioeconomic groups that would prevent
open communication○ Avoid using family members as it may affect what the person does/does not translate or
disclosure○ If no interpreter available, then:
■ Use a calm, friendly manner■ Pantomime (gestures)■ Make a picture board of basic needs■ AT&T has an interpreter line■ Google translate or other free app
● Visually Impaired/Blind○ Things to know:
■ While many persons who are blind can use Braille, the majority of persons who are blind do not.
■ The definition of legally blind is 20/200 vision with best correction. Many more persons who are considered blind have some sight, rather than no sight at all.
■ Many persons who are blind are quite mobile and independent. Some people who are blind view blindness not as a disability as much as an inconvenience.
■ The pt takes your arm and you lead them ■ 2200 with correction → legal blindness■ They don’t view it as a disability but as an inconvenience
○ Things to do:■ Introduce yourself. Identify who you are and what your job or role is. Give the person
verbal information that is visually obvious to those who can see. ■ Tell them when you have brought new items into their environment, describing what
they are and, most importantly, where you have put them. ■ Lead someone who is blind only after they have accepted your offer to do so. Allow
them to hold your arm rather than you holding their arm. It is important to let them control their own movements.
■ Be descriptive when giving directions. Saying “Over there” has little meaning to someone who cannot see you point. “Four doors after turning right from the elevator” would be much more helpful.
■ Describe things from their perspective, not yours. Some persons who are blind use a “clock” reference for things directly in front of them such as a meal. For example, something could be positioned at three o’clock (directly in front and close). Before using this strategy, ask the person if this is useful to them.
○ Things to consider:■ Persons who are blind have a long history of being patronized and talked to as if they
were children. They have been told more often what to do rather than asked what they would prefer doing. This attitude is not acceptable towards any person.
■ Persons who are blind and/or visually impaired are by and large much more independent than most people realize. Many times negotiating the physical environment is less frustrating than trying to communicate with persons who are not sensitive to their needs.
○ Things to avoid:■ Do not interact with a guide dog while it is working (in harness).
● Don’t pet it or interact with it ■ Do not move items (furniture, personal items) after the person has learned their
position. This can be frustrating and, in some cases, dangerous for the person. ■ Do not use references that are visually oriented like, “Over there near the green
plant.” ● Speech Impediments
○ Things to know:■ There are many reasons for having difficulty with speech. Deafness, cerebral palsy,
stroke, head injury, physical malformation of speech mechanisms and general speech impairments are just a few.
■ It is not unusual in stressful situations for someone’s speech to become harder to understand.
○ Things to do:■ Consider writing as an alternative means of communication. Use a computer
terminal, or a Telecommunications Device for the Deaf (TDD/TTY), or plain paper and pencil.
■ If you do not understand what the person is saying, bring it to his/her attention immediately and ask how the two of you may better communicate.
■ If no solution to the communication problem can be worked out with you and the person, consider asking if there is someone who could translate or interpret what is being said.
■ If it is a stressful situation, try to stay calm. If you are in a public area with many distractions, consider moving to a quiet or private location.
○ Things to consider:■ Many persons with difficulty in speech find themselves in situations where people
treat them as if they are drunk, retarded or mentally ill. They are accustomed to being avoided, ignored and even hung up on by phone.
■ Accessibility for persons with difficulty in speech lies within your power. Your understanding, patience and communication skills are as important to someone with a speech impairment as a ramp or grab bar is to someone who uses a wheelchair.
○ Things to avoid:■ Do not become impatient or exasperated with the communication. ■ Do not finish peoples’ sentences for them. ■ Do not pretend to understand them when you really do not.
● Deaf/Hard of Hearing○ Things to know:
■ Members of the Deaf community see their deafness as natural■ Deaf and hearing-impaired persons are entering the workplace in record numbers. ■ Not all persons who are deaf cannot speak. ■ Not all persons who are deaf lip-read. ■ Sign language is not another form of English; it is an official language with its own
grammar, syntax and rules. ■ Not all persons who are deaf use sign language. ■ Lip-reading, while helpful without sound clues, is only 30%-45% effective, and
sometimes less. ■ More persons who are deaf or hearing impaired have some hearing rather than no
hearing at all. ■ Not all persons who are deaf write and read well. ■ Long conversations with persons who lip-read can be very fatiguing to the ■ Find out how the person communicates best. ■ If the person reads lips, speak in a normal, not exaggerated way. Short, simple
sentences are best. ■ Be aware of situations where a person may be waiting for a service (transportation, a
table, the start of an activity) where the common way to communicate is an announcement or the calling of the person’s name. Make sure you take notes when someone cannot hear you and develop an alternative way of notifying them.
■ Gain their attention before starting a conversation. ■ If the person lip-reads, avoid blocking their view of your face. Make sure the lighting
is good. ■ If there is some doubt in your mind whether they understood you correctly, rephrase
your statement and ask them if you have been understood. ■ If the person uses an interpreter, address the person, not the interpreter. ■ Ask if they hear better on one side or another. ■ Communicate better with simple, short questions ■ Approach slowly and from the front so you can see how they are reacting to you
○ Things to Consider:■ When someone asks, “What did you say?” the answers, “Never mind,” “Nothing,” or
“It’s not important,” are very common replies. These are insulting and demeaning, because they communicate that the person is not worth the effort of repeating yourself.
■ Persons who deal very well one-on-one in communication may have a hard time with two or more speakers, especially if there are many interruptions and interjections.
■ Showing impatience to someone who is deaf or hearing impaired may cause someone who is less assertive to back off from telling you of his/her needs.
■ Consider writing as an alternative means of communication. Use a computer terminal, or a Telecommunications Device for the Deaf (TDD/TTY), or plain paper and pencil.
○ Things to avoid:■ Make sure there are no physical barriers between you and the person while in
conversation. ■ If the person is using hearing aids, avoid conversations in large, open and noisy
surroundings. ■ Do not become impatient or exasperated with the person if it takes longer to
communicate. ● Self
○ Self Concept
■ The part of the self that lies within the conscious awareness ■ All that a person perceives, knows, values, feels, hold to be true about his/her
identity ■ Our ideas about who we actually are ■ Dimensions - physical, psychological (emotional), social, spiritual ■ Stable and Dynamic ■ Insecurity peaks in adolescence ■ Influenced by sex, birth order, culture
● Sexual influences on self concept: women are stereotyped as more emotional and vocal than men
● Birth order and self concept: first child is more in control and under more pressure to succeed, youngest child is known as being spoiled
■ Physical—body image and understanding of physiological functioning■ Psychological—identity, cognitive (thinking), perceptual (sensory), emotional
(feelings)■ Social—roles we assume■ Spiritual—connection with higher power(s); finding meaning and purpose in life
○ Assessment■ Physical : body image and understanding of physiological functioning■ Psychological : identity, cognitive (thinking), perceptual (sensory), emotional
(feelings)■ Social : roles ■ Spiritual : connection with higher power(s); finding meaning and purpose in life
○ Ideal Self■ The me I would like to be■ The me I think I ought to be■ Initially, ideal self is learned from parents view of what is ideal self; is influenced next
by teachers and school, then peers, is replaced by individual’s view● Get a lot of feedback from family members / peers etc. which can be positive
or negative. Have to remember that children grow out before they group up. ■ Selects friends that resemble self ideal vs self concept
● We choose friends that we want to be like, not the ones we think we are similar to
■ By age 6-7 relates to competition with others○ Self Esteem
■ Overlap of how i see myself and my self ideal ● The more overlap, the higher the self esteem● The less overlap, the lower the self esteem
■ Individual personal judgment about one’s own worth■ By age 2, child experiences sense of self esteem■ Self esteem is key to behavior■ Self esteem influences thinking processes, emotions, behaviors, desires, values,
goals■ Is global and specific
○ Personality■ “Enduring and inflexible pattern of long duration that lead to significant distress or
impairment and are not due to use of substances or another medical condition.” (DSM 5, 2013)
■ Influenced by temperament (inborn personality characteristics) and the environment■ Automatic responses to the world
● non - thinking ● Touch the hot stove and pull back - a reaction ● As a nurse, we have to control these because our reactions can offend
patients
■ Conscious & unconscious■ Means to adapting to a particular environment and its cultural, ethnic and community
standards● Personality influences your adaptation to the environment
○ Personal Identity■ Perceptual, cognitive, emotional images we have of ourselves■ Perception—how we make sense of reality■ Reality oriented—relationship between inner view and external view■ Perceptual processes are influenced by early parental actions & influence the
development of self concept○ Sullivan
■ Good me - most of us- feeling good about ourselves, we can do things, confident■ Bad me - hearing that you are stupid from parents, too slow, too fast
● Preferable to not me■ Not me - children get inconsistent messages for the same behavior
● Bring home a test grade, one day “great” and next “horrible you are stupid”○ Equilibrium-Disequilibrium
■ People constantly are looking for a balance between themselves and the environment
■ When they are out of balance, it triggers need for nursing interventions● Self awareness, self evaluation, formulating realistic goals, commiting to goals
■ Equilibrium: Driving force to maintain harmony between self and environment■ Disequilibrium: Experience of disharmony between self and environment■ Interventions
● Increase self awareness● Self exploration● Self evaluation● Formulate realistic goals● Commitment to goals via action
○ Self Awareness○ Self respect ○ Self confidence ○ Roles
Human Growth & Development ● Freud
○ Freud believed basic character was formed by age 5 years.○ ID, EGO, SUPEREGO Functions
■ ID: pleasure principle ● What you are born wit ● Part of you that is impulsive, irrational● Not concerned with consequences
■ EGO: mediator ● Appears about the 4th or 5th month of life● Reality tester and the problem solver
■ SUPEREGO: current part of us● Age 3-6 ● Develops through interactions with parents● Ego ideal → how I should be or how I ought to be
○ Conscious, unconscious & preconscious ■ conscious: everything you can recall about yourself■ unconscious: material you don’t yet know about yourself or it may be thoughts,
feelings, experiences that get locked in “an emotional closet”● If you have a really bad experience, it might be too horrible to think about it
so you push it out of the conscious awareness
● Not until you encounter something familiar about that experience that you begin to remember again
● In therapy, you work to uncover these feelings■ preconscious: just below the surface and you don’t automatically remember it, but
you can pull it back up if you need to (Things are in the suppression) ○ Psychosexual Stages:
■ Oral● Child is focused on oral pleasures (sucking)● Too much or too little gratification can result in an Oral Fixation or Oral
Personality which is evidenced by a preoccupation with oral activities● Individuals may become overly dependent upon others, gullible, and
perpetual followers● They may also fight these urges and develop pessimism and aggression
toward others. ● Overeating or drinking, abuse substances, chewing on things
■ Anal● Child’s focus of pleasure in this stage is on eliminating and retaining feces● Child has to learn to control anal stimulation (holding on and letting go)● After effects of an anal fixation during this stage can result in an obsession
with cleanliness, perfection, and control (anal retentive)● On the opposite end of the spectrum, they may become messy and
disorganized (anal expulsive).■ Phallic
● Pleasure zone switches to the genitals.● During this stage boy develops unconscious sexual desires for his mother.● He becomes rivals with his father and sees him as competition for the
mother’s affection.● Boys also develop a fear that their father will punish them for these feelings,
such as by castrating them. This group of feelings is known as Oedipus Complex
● Out of fear of castration and due to the strong competition of his father, boys eventually decide to identify with him rather than fight him.
■ Latent● Stage of relative stability● Sexual urges remain repressed and children’s energy is directed toward
asexual pursuits such as school, athletics, and play mostly with same sex peers.
■ Genital● Final stage of psychosexual development begins at the start of puberty when
sexual urges are once again awakened.● Through the lessons learned during the previous stages, adolescents direct
their sexual urges onto opposite sex peers, with the primary focus of pleasure is the genitals
● Erikson’s Developmental Stages○ Trust vs. Mistrust (birth - 18 mos)
■ Goal is attachment to mother and parents, then others ■ Trust - gives baby sense of faith and hope; baby cries, someone responds (Trust) ■ Mistrust - cry and only sometimes respond, develop sense of mistrust ■ Adults - difficulty relating to other people; suspicious and fearful
○ Autonomy vs. Shame & Doubt (18 mo – 3 yrs)■ Autonomy - “I can do it” sense of internal control and confidence in meeting goals ■ Not successful - feel a lot of shame and doubt; lack self confidence and feel
controlled by others ■ Have a sense of external control; “I’m not in charge of my life”
○ Initiative vs. Guilt (3 – 6 yrs)■ Initiative - goal is to develop a sense of purpose and ability to initiate and direct one’s
actions ● Ex. - see a cup on the stairs, pick it up and throw it away
■ Guilt - cannot address every situation; feeling guilty = feeling inadequate ● Apologize for things they have no control over
● Scared to try new things ○ Industry vs. Inferiority (6 – 12 yrs)
■ Achieving a sense of self confidence by learning and performing tasks successfully (industry)
■ Work ethic ■ If you have learning challenges, you may feel inferior at this time because they’re not
learning at the same rate as others. ■ School performance is critical ■ Industry- feeling of superiority
○ Identity vs. Role Confusion (12 – 20 yrs)■ Identity: goal is to integrate all the tasks that are previously mastered in other stages
into a secure sense of self; try out lots of things■ Role confusion: when trying out a lot of things doesn’t work, and they feel like they
don’t fit in ○ Intimacy vs. Isolation (20 – 30 yrs)
■ “Urge to merge” ■ Intimacy: aking commitments ■ Isolation problems:
● Person is very isolated and interacts only with themselves, gets to work. Goes to cubical. Eats in front of TV. etc.
● Other pattern is multiple relationships but short term ones ■ Intimacy: lasting relationships with others, causes and institutions, not necessarily a
one-on- one thing ○ Generativity vs. Stagnation (30 – 65 yrs)
■ Generativity: Fulfilling life goals and nurturing the next generation ■ Stagnation: when you’re not growing “you figure it out on your own” ■ Sandwich generation: having children and aging
○ Ego Integrity vs. Despair (65 yrs – end of life)■ Ego Integrity: when one looks back on their life and hopefully sees overall that it has
value and worth; they feel fulfilled; don’t fear death■ Despair: depression, anger, and loneliness; dissatisfied when they look back on their
life● Piaget’s Stages of Cognitive Development
○ Sensorimotor (0-2): the child begins to interact with the environment ○ Preoperational (2-6,7): the child begins to represent the world symbolically ○ Concrete operations (7-11,12): the child learns rules like conservation ○ Formal operations (12-adulthood): the adolescent can transcend the concrete situation
and think about the future
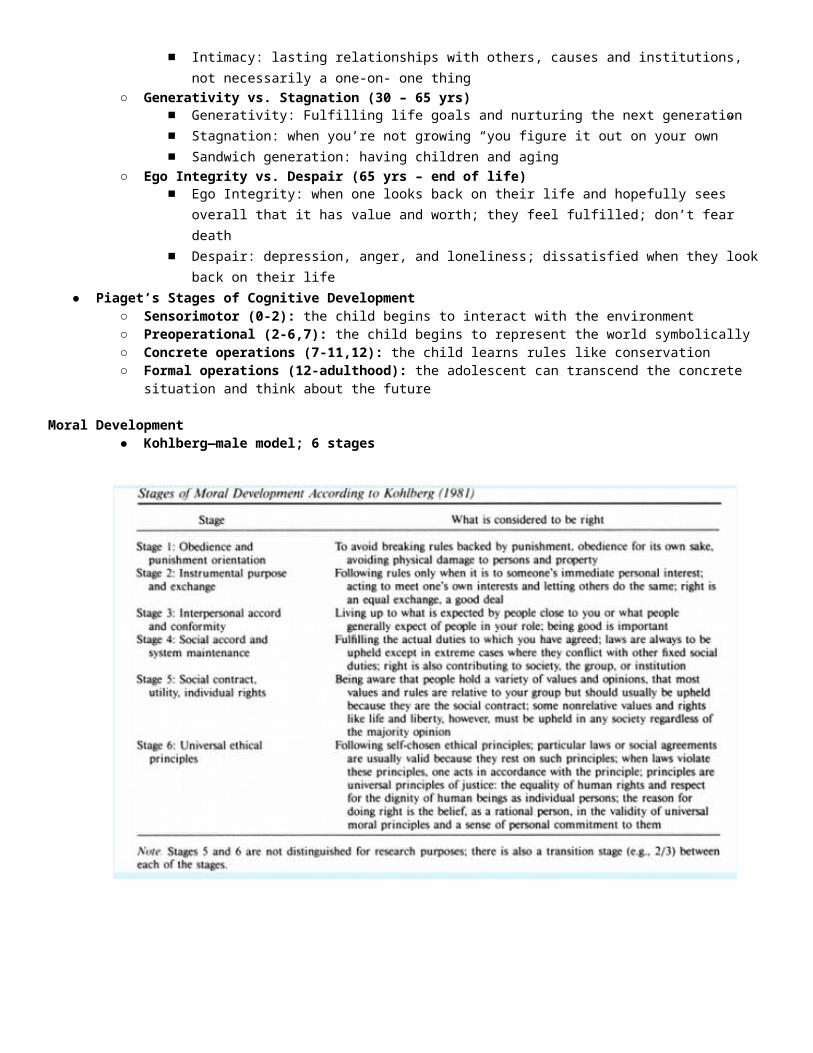
Moral Development● Kohlberg—male model; 6 stages
● Gilligan-model based on women○ how are decisions made?
● Sullivan○ Development based on interpersonal relationships○ Basis of Peplau’s Phases of N-P Relationship○ Anxiety, Needs Satisfaction, Security, Self-system ○ Infancy (birth – 18 mos)○ Childhood (18 mos – 6 yrs)○ Juvenile (6 – 9 yrs)○ Preadolescence (9 – 12 yrs)○ Early adolescence (12 – 14 yrs)○ Late adolescence (14 – 21 yrs)○ Relevance to Nursing Practice
■ Peplau’s focus on relationship development and phases of Nurse-Patient Relationship is based on Sullivan’s work
● Maslow ○ Physiological ○ Safety &
Security○ Love &
Belonging ○ Esteem ○ Self-
actualization
Video Notes – The First Year● Oral stage! Everything goes to
baby’s mouth!● Best learning is
interacting with parents – eye contact, cuddling, touch, talking stimulates hearing & brain development
● Newborn’s best vision within 7”● Baby’s language is body movements● Mimic (role modeling begins in infancy)● When babies are overwhelmed, they shut down● Some babies aren’t “lookers” and natural parental response is to cut down on eye gaze; parents
need to work with baby to develop eye gaze as this is important life skill for interacting with peers & adults, e.g. parents of peers, teachers, coaches, etc.
● Many dads and some moms have difficulty with & need to develop skills in recognizing newborn’s subtle cues and what to do when baby cries
● Men tend to be more physical with babies ● Crying
○ Crying is primary way babies communicate their needs○ Most difficult aspect of baby behavior for parents to cope with○ All babies have fussy times during the day; often 5-6 PM when parents are tired too; some
babies are fussy most of the time and never seem totally happy ● 4 Trait types
○ Average : baby’s responses are consistent, predictable○ Quiet : watches others, takes information in at slower pace○ Active : lots of energy; interested in surroundings; like to explore ○ Hypersensitive : vulnerable to stimulation, e.g. tag on back of shirt, loud talking/noises;
careful not to over stimulate● Babies should sleep on their back “Back to Sleep” ● Developmental milestones
○ Range for achievement of milestones ○ Vocalization (babbling, cooing to da da, ma ma, oh oh) should increase in frequency○ 8 months
■ stranger anxiety■ don’t intrude on baby’s personal space■ caution - direct eye gaze & loud talking
○ Motor ■ 4-7 months: rolls both ways (front to back & back to front); rolls to move■ 6 months: sits well unsupported■ 7-9 months: pull ups, stands holding on■ Crawls
● 9 months● bilateral movement very important for left & right brain development!
■ Cruises● 10 months● pulling to a stand and moves around while holding on
■ 1 year: walks● Parental fatigue & exhaustion● Couple time is very important as baby’s’ needs & time dominate
● Caregivers○ feelings of guilt & jealousy common○ many moms cry and feel distress when leave infants, esp. first time○ talk with caregiver about milestone information – what does parent want & not want shared○ spend 15 – 30 minutes with baby when first get home & then do other tasks to reestablish
relationship, will be less fussy rest of the evening ● Limit setting
○ Discipline is teaching○ Parents should discuss approach○ Differences in approaches/methods can cause issues between parents
● Power Struggle ○ Cooperation & negotiation○ if resolved using physical means earlier in life, becomes more difficult as child grows bigger
because at some point, child will likely be physically larger/stronger