Psychopharmacologic Consultant Neuronetics X · Strawn et al. Depression & Anxiety. 2015 |Locher,...
17
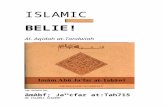
Jeffrey R. Strawn, MD 6/22/2019 1 Recent Advances in the Psychopharmacologic Treatment of Pediatric Anxiety: Tailoring Treatments and Enhancing Outcomes Jeffrey R. Strawn, MD, FAACAP Associate Professor of Psychiatry and Pediatrics University of Cincinnati Cincinnati Children’s Hospital Medical Center Disclosures of Potential Conflicts Source Research Funding Advisor/ Consultant Speaker’s Bureau Books, Intellectual Property In-kind Services Stock or Equity Neuronetics X Allergan X Lundbeck X National Institutes of Health (NIMH) X National Institutes of Health (NIEHS) X Springer Publishing X UpToDate X Assurex/ Genesight X X CMEology X Disclosure: Off Label Medication Use will be Discussed The following are FDA-approved antidepressants in children and adolescents Class Medication Age (years) SSRI 6 7 8 9 10 11 12 13-17 Citalopram NONE Escitalopram NONE MDD Fluoxetine OCD NONE MDD Fluvoxamine NONE OCD Paroxetine NONE Sertraline OCD Vilazodone NONE Vortioxetine NONE SSNRI Duloxetine GAD Desvenlafaxine NONE Venlafaxine NONE Atypical Antidepressant Bupropion NONE Mirtazapine NONE Trazodone NONE Anxiety
Transcript of Psychopharmacologic Consultant Neuronetics X · Strawn et al. Depression & Anxiety. 2015 |Locher,...

Jeffrey R. Strawn, MD 6/22/2019
1
Recent Advances in the Psychopharmacologic
Treatment of Pediatric Anxiety: Tailoring Treatments and
Enhancing OutcomesJeffrey R. Strawn, MD, FAACAP
Associate Professor of Psychiatry and PediatricsUniversity of Cincinnati
Cincinnati Children’s Hospital Medical Center
Disclosures of Potential ConflictsSource Research
FundingAdvisor/
ConsultantSpeaker’s Bureau Books, Intellectual
PropertyIn-kind
ServicesStock or Equity
Neuronetics X
Allergan X
Lundbeck X
National Institutes of Health (NIMH)
X
National Institutes of Health (NIEHS)
X
Springer Publishing X
UpToDate X
Assurex/Genesight
X X
CMEology X
Disclosure: Off Label Medication Use will be DiscussedThe following are FDA-approved antidepressants in children and adolescents
Class Medication Age (years)
SSRI
6 7 8 9 10 11 12 13-17
Citalopram NONEEscitalopram NONE MDD
Fluoxetine OCDNONE MDD
Fluvoxamine NONE OCD
Paroxetine NONE
Sertraline OCD
Vilazodone NONE
Vortioxetine NONE
SSNRI
Duloxetine GAD
Desvenlafaxine NONE
Venlafaxine NONE
Atypical Antidepressant
Bupropion NONE
Mirtazapine NONE
Trazodone NONE
Anxiety

Jeffrey R. Strawn, MD 6/22/2019
2
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers
Variability in Treatment Response Current Approach: Assumptions

Jeffrey R. Strawn, MD 6/22/2019
3
Precision Medicine Precision TxGen
Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers
Psychopharmacologic Treatment of Anxiety in Pediatric Patients
General Principles
Pediatric GAD: Fixed-Dose Sertraline
0 1 2 3 4 5 6 7 8 9Week
20
15
10
5
0
Hamilton
Anxiety Rating Scale
Rynn MA, Siqueland L, Rickels K. Placebo-controlled trial of sertraline in the treatment of children with generalized anxiety disorder. Am J Psychiatry. 2001;158(12):2008-14.
In most pediatric anxiety studies, SSRI/SNRI separates from placebo between week 2 and week 4

Jeffrey R. Strawn, MD 6/22/2019
4
• Age– 6 to 17 years
• Randomization– Venlafaxine (N=157) or placebo
(N=163) for 8 weeks. • Primary outcome measure
– Composite score for GAD section of a modified version of the K-SADS for School-Age Children
• Results– Pooled analysis, venlafaxine
• Venlafaxine > placebo for decrease in K-SADS GAD score (–17.4 vs –12.7).
– CGI Response• venlafaxine > placebo (69% vs
48%).
Pediatric GAD: Venlafaxine XR
Rynn, et al. Efficacy and safety of extended-release venlafaxine in the treatment of generalized anxiety disorder in children and adolescents: two placebo-controlled trials. Am J Psychiatry. 2007;164(2):290-300.
Baseline 1 2 3 4 5 6 7 8
40
35
30
25
Raw
Sco
re o
n N
ine
Del
inea
ted
Item
s fo
r GAD
Fr
om C
olum
bia
K-SA
DS
Pediatric GAD: Duloxetine• Patients• 7-17 years of age
– Duloxetine, 12.6 ± 3 years– Placebo, 12.2 ± 3 years
• Inclusion– Moderate severity GAD
• Outcome– Change in PARS Severity for
GAD– Change in PARS (total)
Strawn, Prakash, Zhang, et al. A randomized, placebo-controlled study of duloxetine for the treatment of children and adolescents with generalized anxiety disorder. J Am Acad Child & Adolescent Psychiatry. 2015;54:283-93.
-12
-7
-2
3 Duloxetine (N=135)Placebo (N=133)
LS M
ean
Cha
nge
Week0 1 2 4 7 10 LOCF
-0.50.51.52.53.54.55.56.5
Weight (kg) Diastolic BP (mm Hg)Systolic BP (mm Hg) Pulse (bpm)
Duloxetine (N=135)Placebo (N=137)
Mea
n C
hang
e fro
m
Base
line
durin
g Ac
ute
Trea
tmen
t
Adolescent GAD: Escitalopram vs. Placebo
Strawn et al, 2019 (unpublished)
• Patients– 12-17 years of age
• Dosing– Forced-Flexible– 5 mg qAM x 2 days then 10 mg qAM x 7 days then 15
mg qAM until week 4 at which time escitalopramcould be increased to 20 mg qAM.
• Inclusion– Moderate severity GAD, no MDD– Stable psychotherapy
• Outcome– Change in PARS from baseline to endpoint– CGI-I and CGI-S
Baseline Characteristics Escitalopramn=26
Placebon=25
Age, years Mean (SD) 14.8 (1.7) 14.9 (1.6) Sex, n (%) Female 20 (77) 19 (76) Race, n (%) Asian 0 (0) 2 (8) Black & African American 1 (4) 1 (4) Caucasian 23 (88) 20 (80) Other 2 (8) 2 (8) IQ Score (SD) 106 (12) 105 (10) PARS Score Mean (SD) 18 (2) 17 (2) CDRS Score Mean (SD) 33(4) 32(6) Comorbidity Separation anxiety, n (%) 4 (15) 5 (20) Panic disorder, n (%) 13 (50) 15 (60) Agoraphobia, n (%) 7 (27) 7 (28) ADHD, n (%) 5 (19) 4 (16) Strawn et al, 2019 (unpublished)
−12
−8
−4
0
0 2 4 6 8Treatment Week
Cha
nge
in P
ARS
Scor
e
p=0.01p<0.001
p=0.002
p<0.001p<0.001
Adolescent GAD: Escitalopram vs. Placebo

Jeffrey R. Strawn, MD 6/22/2019
5
Guanfacine ER in Pediatric Anxiety• Dx: GAD, separation anxiety
disorder, social anxiety disorder.• No ADHD, no MDD, no BP• N = 83• Age 6-17 (mean: 12±3)• 1-6 mg/day, 3:1 randomization• 32 sites
Strawn JR, Compton S, Robertson B, Albano AM, Hamdani M, Rynn MA. J. Child & Adolesc. Psychopharm. 2017;27(1):29-37.
Predicting Treatment Response in Pediatric Anxiety
The Impact of Comorbidity
CAMS: Predictors of RemissionSocial Anxiety/Social Phobia & Age
Ginsburg et al. Remission After Acute Treatment in Children and Adolescents with Anxiety Disorders: Findings From the CAMS. Journal of Consulting and Clinical Psychology. 2011;79(6):806–813
0102030405060708090 No SoP
SoP
Rem
issi
on b
y C
GI-S
Sco
re (%
)
01020304050607080
Age 7-11 yearsAge 12-17 years
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers

Jeffrey R. Strawn, MD 6/22/2019
6
Predicting Treatment Response in Pediatric Anxiety
The Impact of Metabolism
Citalopram & EscitalopramMetabolism and Outcome Relevance
CitalopramN-oxide
2C193A42D6
r-desmethyl-citalopram
s-desmethyl-citalopram
2C193A42D6
s-didesmethyl-citalopram
r-didesmethyl-citalopram
2D6
2D6
2D6Amineoxidase
Amineoxidase
S-Citalopram
R-Citalopram
Adolescent Escitalopram ResponsePharmacogenomic Predictors
Strawn et al. Unpublished data.
Normal metabolizers, n=10Intermediate metabolizers, n=10
Adolescent Escitalopram ResponseLevels in Adolescent GAD
Strawn et al. Unpublished data.
Non-adherent with treatment secondary to side effects

Jeffrey R. Strawn, MD 6/22/2019
7
Adolescent Escitalopram ResponsePharmacogenomic Predictors
Strawn et al. Unpublished data.
Normal metabolizers, n=10Intermediate metabolizers, n=10
5‐HT Transporter GeneSLC6A4 or 5HTT or SERT
• Encoded by the SLC6A4 gene
• Responsible for the reuptake of 5-HT into the presynaptic neuron
• SSRIs inhibit this process, resulting in increased 5-HT being present at the synaptic junction
α2
SSRI
SSRI
5‐HT Transporter GeneSLC6A4 or 5HTT or SERT
• Meta-analyses of the association between 5-HTTTR polymorphism and SSRI efficacy for adult MDD (15 studies, N=1435) (Horstmann et al, 2009)– s/s variant lower remission rates (p<0.0001)– s/s and s/l variants had lower response rates
SSRI
α2
SSRI
s/s l/ls/l
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers

Jeffrey R. Strawn, MD 6/22/2019
8
Predicting Time to Response inPediatric Anxiety
How long should an SSRI trial last?
CAMS: Probability of Response in Pediatric Anxiety Disorders
If no improvement by wk 8 with sertraline, 3:1 odds against additional improvement
Strawn et al. Placebo response in pediatric anxiety disorders: results from the Child/Adolescent Anxiety Multimodal Study (CAMS). Journal of Child and Adolescent Psychopharmacology. 2017;27(6):501-508.
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers
Predicting Response in Pediatric Anxiety
Not all antidepressants are the same

Jeffrey R. Strawn, MD 6/22/2019
9
Meta-Analysis: Antidepressant Efficacy
Effect Size=0.62, p=0.002Weighted d proportional to 5-HT selectivity, p=0.02
Strawn et al. Depression & Anxiety. 2015 | Locher, et al. JAMA Psychiatry. 2017Wang et al. JAMA Pediatrics. 2017 | Dobson et al. J Clin Psychiatry 2019 (in press)
SSRI Effect Size: 0.65SNRI Effect Size: 0.45
SSRI Effect Size: 0.71SNRI Effect Size: 0.41
SSR
ISN
RI
Serotonergic Selectivity
R² = 0.7621
0
0.25
0.5
0.75
1
1.25
1.5
1.75
0 500 1000 1500
fluvoxamine
duloxetine
venlafaxine
sertraline
Ki NE/Ki 5-HT (Serotonergic Specificity)
Effe
ct S
ize
fluoxetineparoxetine
P = 0.010
Strawn et al. Depression & Anxiety. 2015;32(3):149-57
Network Meta-Analysis: Medication EfficacySSRIs, SNRIs and alpha-2 agonists are more effective than placebo in producing ‘treatment response’
Dobson ET, Bloch M, Strawn JR. Network meta-analysis: efficacy and tolerability of pharmacotherapy for pediatric anxiety disorders. Journal of Clinical Psychiatry. 2019;80(1):17r12064.
Network Meta-Analysis: Medication Efficacy
Dobson ET, Bloch M, Strawn JR. Network meta-analysis: efficacy and tolerability of pharmacotherapy for pediatric anxiety disorders. Journal of Clinical Psychiatry. 2019;80(1):17r12064.

Jeffrey R. Strawn, MD 6/22/2019
10
Antidepressant Response in Pediatric Anxiety Disorders
SSNRI
SSRIHigh dose
SSRI
Low dose SSRI
Strawn JR, Mills JA, Sauley B, Welge JA. The impact of antidepressant dose and class on treatment response in pediatric anxiety disorders: a meta-analysis. Journal of the American Academy of Child & Adolescent Psychiatry. 2018;57(4):235–244.
SSRIs produce faster and greater improvement in anxiety symptoms
Antidepressant Dose and Response
Wehry AM, Dulemba SE, Ramsey L, Strawn JR. Pharmacogenomic Testing in Child & Adolescent Psychiatry: an Evidence-Based Review. Current Problems in Pediatrics and Adolescent Health Care 2018
Predicting Placebo Response in Pediatric Anxiety
Expectation is Critical
CAMS: Placebo Response and its Relevance for Clinicians
• Change in PARS score over the course of 12 weeks of treatment was best predicted by:– Separation anxiety disorder
(strongest predictor)– parent expectations for
treatment success– child expectations for treatment
success
Strawn JR, Dobson ET, Mills JA, Cornwall GJ, et al. Placebo Response in Pediatric Anxiety Disorders: Results from the Child/Adolescent Anxiety Multimodal Study. J Child Adolesc Psychopharmacol. 2017

Jeffrey R. Strawn, MD 6/22/2019
11
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers
Meta-Analysis: SSRI and SNRI Adverse Events in Pediatric Patients
Mills and Strawn, 2019, under review
Predicting Antidepressant Side Effects in Anxiety
Activation
Activation
Activation
Impulsivity
Insomnia
Restlessness
Hyperactivity
Irritability
Disinhibition
Luft MJ, Lamy M, DelBello MP, McNamara RK, Strawn JR. Antidepressant-induced activation in children and adolescents: risk, recognition and management. Current Problems in Pediatrics and Adolescent Health Care. 2018;48(2):50-62.

Jeffrey R. Strawn, MD 6/22/2019
12
Activation and Drug Level• Antidepressant-related activation emerges
early in treatment or following an increase in dose (Reinblatt et al. 2009).
• Symptoms resolve when the dose is decreased or medication is discontinued (Riddle et al. 1990; Wilens et al. 2003).– Consistent with one prospective study of
fluvoxamine in which higher plasma fluvoxamine concentrations were associated with a greater likelihood of activation in anxious youth (Reinblatt et al, 2009, right).
• The rate of symptom resolution is related to the rate of activation symptom onset (Wilenset al. 2003).
Activation
No Activation
Luft et al. Antidepressant-induced activation in children and adolescents: risk, recognition and management. Current Problems in Pediatrics and Adolescent Health Care. 2018.
Antidepressants and Activation in Youth with Anxiety Disorders
Reinblatt et al. J Child Adolesc Psychopharmacol. 2009;19(2):119–126.
Fluvoxam
ine level
(ng/mL)
No activation
Activation
0 200
4
00 600
800
Activation and Antidepressant Class in Anxious Children & Adolescents
• SSRIs are more likely to produce activation compared to placebo.• SNRIs do not differ from placebo in terms of the likelihood of producing
activation.
Mills and Strawn, in preparation.
Prob
ability SSRI SNRIs
placebo placebo
p=0.001 p=0.074
Activation and Antidepressant Class in Anxious Children & Adolescents
• SSRIs are more likely to produce activation than SNRIs (p<0.0001)– Odds against H0: 17:1
Mills and Strawn, in preparation.
SSRI
SNRI
Activation Rate
p=0.0001
Prob
ability
Prob
ability

Jeffrey R. Strawn, MD 6/22/2019
13
Escitalopram-Related ActivationANOVA for trend p=0.029
Aldrich et al. Influence of CYP2C19 metabolizer status on escitalopram/citalopram tolerability and response in youth with anxiety and depressive disorders. Frontiers in Pharmacology 2019 (in press).
Clinical Recommendations for Managing Activation
• Rule out general medical condition • Evaluate potential contributors
– Diagnosis/Comorbidity• ADHD, manic symptoms?
– Family factors that perpetuate anxiety (e.g., accommodation)
– occult substance use, – medication adherence,
• Decrease in dose of SSRI• Consider change to another SSRI or SNRI• Consider individual or family psychotherapy• May consider short-term adjunctive benzodiazepines for
activation
Luft et al. Antidepressant-Induced Activation in Children and Adolescents: Risk, Recognition and Management. Current Problems in Pediatrics and Adolescent Health Care. 2017
Predicting Antidepressant Side EffectsWeight Gain
Antidepressant-Related Side EffectsWeight Gain and SSRIs
Calarge et al. Body composition in adolescents during treatment with selective serotonin Reuptake Inhibitors. Pediatrics 2017;140(1) :e20163943
0
0.05
0.1
0.15
0.2
0.25
0.3
BMI z-score fat mass index z-score lean body mass index z-score
CitalopramFluoxetineSertraline
p<0.0005
p<0.05p=0.05
p<0.0005 p<0.0005

Jeffrey R. Strawn, MD 6/22/2019
14
Escitalopram-Related Weight Gain
Ramsey et al. Racial differences in escitalopram/citalopram-related weight gain in children and adolescents: a natural language processing-based electronic medical record study. J Child & Adolescent Psychopharmacology. 2019 (in press)
Log-rank test for trend p=0.018
Aldrich et al. Influence of CYP2C19 metabolizer status on escitalopram/citalopram tolerability and response in youth with anxiety and depressive disorders. Frontiers in Pharmacology 2019(10):99.
Escitalopram-Related Weight Gain
Predicting Treatment-Emergent Suicidality and Self Harm in
Antidepressant-Treated Youth Dose and Medication
Antidepressants & Self-Harm• \\
Miller M, Swanson SA, Azrael D, Pate V, Sturmer T. Antidepressant Dose, Age, and the Risk of Deliberate Self-harm. JAMA Internal Medicine 2014 174(6):899-909
Modal doses:citalopram 20 mg/daysertraline 50 mg/dayfluoxetine 20 mg/day

Jeffrey R. Strawn, MD 6/22/2019
15
Antidepressants & Suicidality in Pediatric Anxiety Disorders
• \\
Dobson ET, Bloch M, Strawn JR. Network meta-analysis: efficacy and tolerability of pharmacotherapy for pediatric anxiety disorders. Journal of Clinical Psychiatry. 2019;80(1):17r12064.
Treatment-emergent suicidality was significantly greater in paroxetine-treated patients compared to those receiving sertraline (logOR: 43.5, 95% CrI: [10.1 to 96.0]), placebo (logOR: 19.5, 95% CrI: [1.7 to 60.4]), and duloxetine (logOR: 20.3, 95% CrI: [1.5 to 67.7]).
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
Psychotherapy
Biomarkers
Precision Tx
Gen Psychopharm
PGx
Time course
Comparing meds
Placebo
Side Effects
Dosing
PsychotherapyBiomarkers
Predicting Psychotherapy Response in Pediatric Anxiety
The Impact of Age and Modality

Jeffrey R. Strawn, MD 6/22/2019
16
Significant linear discontinuity in slope following onset of exposure in CBT
Peris, et al. Trajectories of Change in Youth Anxiety during CBT J Consult Clin Psychol. 2015; 83(2): 239–252.
Onset of cognitiveRestructuring
component of CBT
Onset of exposure exercises
Is exposure “the”
improves symptoms?
Is exposure “the” component of CBT that
improves symptoms?
Trajectory varies by treatment and age
Peris, et al. Trajectories of Change in Youth Anxiety during CBT J Consult Clin Psychol. 2015; 83(2): 239–252.
Onset of cognitiverestructuring component
of CBT
Onset of exposure exercises
Does SSRI treatment
of CBT?
Does SSRI treatment augment the cog effect
of CBT?Are children, compared
with CBT?
Are children, compared to adolescents benefitting more from exposure when treated with CBT?
Predicting Psychotherapy Response in Pediatric Anxiety
The Impact of Comorbidity
ADHD Co-morbidity and Treatment Outcome in CAMS
• ADHD diagnosis moderated acute tx response and remission rates.
• Youth with co-occurring ADHD fared worse in the CBT condition.
– When was CBT administered?• After school
– When were stimulants more likely to have been administered?
• morning• No differences in other tx conditions.• ODD diagnosis did not moderate or predict any
treatment outcomes
Ollendick T. Treatment outcomes in anxious youth with and without comorbid ADHD in the CAMS. Anxiety & Depresive Disorders Association of America, Chicago, IL, March, 2014
CBT
ADHD
12
3
6
9

Jeffrey R. Strawn, MD 6/22/2019
17
Predicting Psychotherapy or Pharmacotherapy Response in
Pediatric AnxietyThe Impact of Severity
Anxiety Severity and Remission• Child & Adolescent
Multimodal Study– Sertraline– Sertraline + CBT– CBT– Placebo
• The most severely anxious youth probably require combined treatment (CBT+SSRI) to achieve the best outcomes.
Taylor JH et al. Monotherapy Insufficient in Severe Anxiety? Predictors and Moderators in the Child/Adolescent Anxiety Multimodal Study. Journal of Clinical Child & Adolescent Psychology. 2018. 47:2, 266-281.
02468
10121416
Severe Anxiety Moderate Anxiety
SertralineCBTSertraline+CBT
NN
T fo
r rem
issi
on
Conclusions• SSRIs/SNRIs are effective treatments for anxiety disorders
– SSRIs associated with greater and faster improvement. – Adequate trial = 6 weeks.
• Psychotherapy is effective for pediatric anxiety disorders– Comorbid conditions affect engagement and liklihood of success and require optimizing of
comorbiditiy-specific treatment. • Antidepressant side effects in adolescents
– activation may be related to drug level and metabolism. – SSRIs are associated with more activation compared to SNRIs. – Citalopram is associated with weight gain in youth with anxiety/depressive disorders
• Pharmacogenetic markers of medication metabolism suggest:– Slower metabolism may be associated with greater weight gain and activation – Extreme metabolizers (e.g., very slow and very fast) are more likely to discontinue medication– SSRI dose requires adjustment in extreme metabolizers to produce similar exposure to normal
metabolizers.
AcknowledgmentsUniversity of Cincinnati• Heidi Schroeder, BS• Melissa P. DelBello, MD, MS• Sara Varney, BS• Sarah Mossman, MA• Jeffrey Mills, PhD• Marissa Luft, BS• Eric Dobson, MD*
Duke University• Moira Rynn, MD• Scott Compton, MD
Cincinnati Children’s• Sergio Delgado, MD• Kim Cecil, PhD• Laura Ramsey, PhD• Ethan Poweleit, BS
Ann & Robert H. Lurie Children’s Hospital• John Walkup, MD
Columbia University• Amir Levine, MD
*Now MUSC










![Genetic Testing and Treatment: Part 1, …...• 40‐50% for limb‐girdle muscular dystrophy on exome sequencing [Ghaoui et al, JAMA Neurol 2015;72:1424‐1432] [Reddy et al, J Hum](https://static.fdocuments.in/doc/165x107/5f3730805b1a5c148c428f1e/genetic-testing-and-treatment-part-1-a-40a50-for-limbagirdle-muscular.jpg)