
Psychological Test Usage: Implications in Professional ... · Professional Psychology: Research a...
14
Professional Psychology: Research a 2000, Vol. 31, No. 2, 141-154 Copyright 2000 by the American Psychological Association, Inc. 0735-7028/00/55.00 DOI: I0.1037//0735-7028.31.2.I41 Psychological Test Usage: Implications in Professional Psychology Wayne J. Camara, Julie S. Nathan, and Antonio E. Puente American Psychological Association Do psychological assessments require more time than third parties and managed care are willing to reimburse? A survey of clinical psychologists and neuropsychologists was conducted to evaluate the current uses of psychological assessment instruments. Respondents reported their use of tests for 8 different areas of assessment, the average time spent in performing various assessment services and other assessment practices. Results suggested that a majority of neuropsychologists devote a substantial portion of their time to assessment, but only 12% of clinical psychologists reported spending more than 10 hr in assessment-related practice each week. The authors describe the typical time required to administer, score, and interpret various tests and assessments; factors that affect the time required to conduct assessments; and provide a current ranking of the most frequently used assessments in clinical and neuropsychology. How long does it take to conduct comprehensive psychological assessments? Does the time required for assessment activities depend on the nature of the assessment and the presenting prob- lems? What assessments are most commonly used and do they differ by the nature and function of the assessment? What are the implications of these issues for psychologists conducting assess- ment services in today's managed care environment? What strat- egies may psychologists invoke to overcome the multiple obstacles imposed by managed care and demonstrate the efficacy and ex- tensiveness of comprehensive assessment practices? We examined these and other related questions through a survey of a sample of clinical and neuropsychologists who conducted assessment activities. Psychological assessment has been a defining practice of pro- fessional psychology since the field's inception. Over the past several decades, national surveys of psychological test usage have enriched our knowledge of the assessment practices of profes- sional psychologists. With the advent of managed care, psycho- logical services such as assessment services are increasingly com- pensated at standard approved rates that may or may not reflect the level of effort and time required to perform these services. In today's managed care environment, research-based knowledge of the time it actually takes clinicians to administer, score, interpret, and write reports could "curb abuse of testing benefits ... we know has gone on" (R. DeLapp, personal communication, Novem- ber 5, 1991). The present study was designed to provide accurate information on current psychological test usage. Louttit and Brown (1947) first documented psychological test usage in 1935 and 1946. Subsequent national surveys to estimate psychological test usage were reported in 1961 (Sundberg, 1961) and 1969 (Lubin, Wallis, & Paine, 1971). Lubin et al. (1971) found that the top 10 most often used tests included 4 projective tech- niques, the Rorschach Psychodiagnostic Test (often called the Inkblot Test), Thematic Apperception Test (TAT), the Draw-A- WAYNE J. CAMARA received his PhD in organizational behavior from the University of Illinois at Urbana-Champaign. He is executive director of research and development at the College Board in New York City. He is also president-elect of the American Psychological Association's (APA's) Division of Evaluation, Measurement, and Statistics. This research was initiated when Dr. Camara was assistant executive director of scientific affairs at AP^. JULIE S. NATHAN received her MSEd in 1998 and will be completing her PhD in school psychology from Fordham University in May 2000. She is currently a clinical psychology intern at Montefiore Medical Center/Albert Einstein College of Medicine. ANTONIO E. PUENTE received his PhD from the University of Georgia. He is professor of psychology at the University of North Carolina at Wilmington and maintains an independent practice limited to clinical neuropsychology. He is a past president of the National Academy of Neuropsychology. THIS RESEARCH WAS CONDUCTED with the support of the APA Practice and Science Directorates. We thank the many psychologists and neuropsy- chologists who assisted in reviewing and commenting on the design of the survey, the study methods, and the definitions and assessment areas used in the study. Specifically, recommendations and reviews of the list of tests and the survey content were provided by Thomas Boll, Gordon Chelune, Lee Anna Clark, Munro Cullum, Elena Eisman, Alan Entin, Larry Fried- man, Douglas Jackson, A. John McSweeney, John Mendoza, Robert Resnick, Gayle Rettig, Cecil Reynolds, Charles Spielberger, Laetitia Thompson, Michael Westerveld, Nancy Wilcockson, and members of the executive committees of Divisions 12 (Clinical Psychology). 40 (Clinical Neuropsychology), and 42 (Psychologists in Independent Practice), as well as members from the Board of Professional Affairs. Russ Newman and William C. Howell allocated staff and provided financial support for the survey and study. Jessica Kohout and Marlene Wicheski coordinated the data collection and mailing. Peter Pfordresher managed the data entry and coding of all survey responses. Georgia Sargeant copyedited the mono- graph. Finally, Geoffrey Reed, Heather Roberts-Fox, Dianne Maranto, and Amy Rabinove assisted in coordinating review and comments from APA governance on the design of this study and the draft and final reports. A MUCH MORE COMPREHENSIVE REPORT of the study, with additional data and analyses, is available as an unpublished manuscript from the APA Practice Directorate (Camara, Nathan, & Puente, 1998). CORRESPONDENCE CONCERNING THIS ARTICLE should be addressed to Wayne J. Camara, College Board, 45 Columbus Avenue, New York, New York 10023. Electronic mail may be sent to [email protected].
Transcript of Psychological Test Usage: Implications in Professional ... · Professional Psychology: Research a...

Professional Psychology: Research a2000, Vol. 31, No. 2, 141-154
Copyright 2000 by the American Psychological Association, Inc.0735-7028/00/55.00 DOI: I0.1037//0735-7028.31.2.I41
Psychological Test Usage: Implications in Professional Psychology
Wayne J. Camara, Julie S. Nathan, and Antonio E. PuenteAmerican Psychological Association
Do psychological assessments require more time than third parties and managed care are willing to
reimburse? A survey of clinical psychologists and neuropsychologists was conducted to evaluate the
current uses of psychological assessment instruments. Respondents reported their use of tests for 8
different areas of assessment, the average time spent in performing various assessment services and other
assessment practices. Results suggested that a majority of neuropsychologists devote a substantial portion
of their time to assessment, but only 12% of clinical psychologists reported spending more than 10 hr in
assessment-related practice each week. The authors describe the typical time required to administer,
score, and interpret various tests and assessments; factors that affect the time required to conduct
assessments; and provide a current ranking of the most frequently used assessments in clinical and
neuropsychology.
How long does it take to conduct comprehensive psychological
assessments? Does the time required for assessment activities
depend on the nature of the assessment and the presenting prob-
lems? What assessments are most commonly used and do they
differ by the nature and function of the assessment? What are the
implications of these issues for psychologists conducting assess-
ment services in today's managed care environment? What strat-
egies may psychologists invoke to overcome the multiple obstacles
imposed by managed care and demonstrate the efficacy and ex-
tensiveness of comprehensive assessment practices? We examined
these and other related questions through a survey of a sample
of clinical and neuropsychologists who conducted assessment
activities.
Psychological assessment has been a defining practice of pro-
fessional psychology since the field's inception. Over the past
several decades, national surveys of psychological test usage have
enriched our knowledge of the assessment practices of profes-
sional psychologists. With the advent of managed care, psycho-
logical services such as assessment services are increasingly com-
pensated at standard approved rates that may or may not reflect the
level of effort and time required to perform these services. In
today's managed care environment, research-based knowledge of
the time it actually takes clinicians to administer, score, interpret,
and write reports could "curb abuse of testing benefits . . . we
know has gone on" (R. DeLapp, personal communication, Novem-
ber 5, 1991). The present study was designed to provide accurate
information on current psychological test usage.
Louttit and Brown (1947) first documented psychological test
usage in 1935 and 1946. Subsequent national surveys to estimate
psychological test usage were reported in 1961 (Sundberg, 1961)
and 1969 (Lubin, Wallis, & Paine, 1971). Lubin et al. (1971) found
that the top 10 most often used tests included 4 projective tech-
niques, the Rorschach Psychodiagnostic Test (often called the
Inkblot Test), Thematic Apperception Test (TAT), the Draw-A-
WAYNE J. CAMARA received his PhD in organizational behavior from the
University of Illinois at Urbana-Champaign. He is executive director of
research and development at the College Board in New York City. He is
also president-elect of the American Psychological Association's (APA's)
Division of Evaluation, Measurement, and Statistics. This research was
initiated when Dr. Camara was assistant executive director of scientific
affairs at AP^.
JULIE S. NATHAN received her MSEd in 1998 and will be completing her
PhD in school psychology from Fordham University in May 2000. She is
currently a clinical psychology intern at Montefiore Medical Center/Albert
Einstein College of Medicine.
ANTONIO E. PUENTE received his PhD from the University of Georgia.
He is professor of psychology at the University of North Carolina at
Wilmington and maintains an independent practice limited to clinical
neuropsychology. He is a past president of the National Academy of
Neuropsychology.
THIS RESEARCH WAS CONDUCTED with the support of the APA Practice and
Science Directorates. We thank the many psychologists and neuropsy-
chologists who assisted in reviewing and commenting on the design of the
survey, the study methods, and the definitions and assessment areas used in
the study. Specifically, recommendations and reviews of the list of tests
and the survey content were provided by Thomas Boll, Gordon Chelune,
Lee Anna Clark, Munro Cullum, Elena Eisman, Alan Entin, Larry Fried-
man, Douglas Jackson, A. John McSweeney, John Mendoza, Robert
Resnick, Gayle Rettig, Cecil Reynolds, Charles Spielberger, Laetitia
Thompson, Michael Westerveld, Nancy Wilcockson, and members of the
executive committees of Divisions 12 (Clinical Psychology). 40 (Clinical
Neuropsychology), and 42 (Psychologists in Independent Practice), as well
as members from the Board of Professional Affairs. Russ Newman and
William C. Howell allocated staff and provided financial support for the
survey and study. Jessica Kohout and Marlene Wicheski coordinated the
data collection and mailing. Peter Pfordresher managed the data entry and
coding of all survey responses. Georgia Sargeant copyedited the mono-
graph. Finally, Geoffrey Reed, Heather Roberts-Fox, Dianne Maranto, and
Amy Rabinove assisted in coordinating review and comments from APA
governance on the design of this study and the draft and final reports.
A MUCH MORE COMPREHENSIVE REPORT of the study, with additional data
and analyses, is available as an unpublished manuscript from the APA
Practice Directorate (Camara, Nathan, & Puente, 1998).
CORRESPONDENCE CONCERNING THIS ARTICLE should be addressed to Wayne
J. Camara, College Board, 45 Columbus Avenue, New York, New York
10023. Electronic mail may be sent to [email protected].

142 CAMARA, NATHAN, AND PUENTE
Person Test (DAP), and the House-Tree-Person (H-T-P) Projec-
tive Technique, as well as 3 intelligence tests, the Wechsler Adult
Intelligence Scale (WAIS), the Wechsler Intelligence Scale for
Children (WISC), and the Stanford-Binet Intelligence Scale. The
others in the top 10 were the Bender Visual Motor Gestalt Test
(hereinafter the Bender Gestalt), the Minnesota Multiphasic Per-
sonality Inventory (MMPI), and Sentence Completion tests.
In the 10-year interval between Sundberg's (1961) and Lubin
et al.'s (1971) studies, intellectual measures such as the WAIS
and WISC began to displace some of the traditional projective
personality assessment instruments, but these were still pre-
ferred over more empirical measures of personality. The MMPI,
in fact, was the only objective personality test found in the
top-10-ranked instruments of both studies. These earlier studies
examined the rank ordering of tests but did not provide any
information regarding specific test usage. In their 1975 survey
of psychological test usage, Brown and McGuire (1976) asked
professionals from community mental health agencies and hos-
pitals not only which tests were used most often but also which
were used most for intellectual versus personality assessments,
and which were used most for different age groups. Brown and
McGuire's (1976) study found little overall change in the
top-ranked tests from 1969 to 1975. The most notable changes
from 1971 to 1975 were the addition of the Slosson Intelligence
Test for Children and Adults and the Kinetic Drawing System
for Family and Schools to the list of most frequently used tests,
and the increase in popularity of the WISC.
Another national survey of psychological test usage was per-
formed in 1982 (Lubin, Larsen, & Matarazzo, 1984). Of the 6
projective techniques ranked in the top 10 in 1969, 5 were still in
the top 10 in 1982, and the MMPI was ranked second in 1982,
demonstrating its steadily increasing use. For the first time, the
Stanford-Binet was not among the top 10 tests used in the 1982
survey, ranking 15th.
Before 1984, surveys on testing practices had been conducted
with members of APA Division 12; however, now surveys of
assessment practice included members of the Association for
Advancement of Behavior Therapy (AABT) and the Society for
Personality Assessment (SPA; O'Roark & Exner, 1989). Re-
sults revealed that projective techniques, specifically the Ror-
schach, TAT, Sentence Completion, and H-T-P tests, were in
the SPA's top 10 most frequently used testing instruments. The
objective personality measures in the top 10 were the MMPI
(ranked third), the Children's Apperception Test (CAT), and the
Sixteen Personality Factor Questionnaire (16PFQ). For cogni-
tive assessment, the Wechsler scales were ranked first, indicat-
ing their growing popularity. The overwhelming majority of
SPA members (90% of those who responded) indicated that
they primarily used assessments for diagnostic purposes, and
53% also used testing as an indicator of what type of therapy
would be most effective.
Addressing a void in the survey research to date, Ball, Archer,
and Imhof (1994) surveyed practitioners for their perceptions of
the time required to administer, score, and interpret psychological
test instruments. They mailed surveys to small samples of clinical
psychologists, neuropsychologists, and SPA members. The instru-
ments listed as typical for test batteries corresponded closely with
the most highly ranked tests in previous surveys (Ball et al., 1994).
Results showed that clinicians in private practice were adminis-
tering longer test batteries than clinicians in primary employment
settings. These data raised questions "as to whether clinical, finan-
cial, or some other consideration may underlie test selection" (Ball
et al., p. 247).
Overall, data suggest surprisingly little substantive change in
the ranking of the most often used (i.e., popular) instruments
over the last several decades. For example, the Stanford-Binet
and the Rorschach have been in the top 20 since 1935. Accord-
ing to Lubin et al. (1984), the rank-order correlation between
ranks in 1969 and 1982 was .89 (p < .001). The use of
projective techniques has persisted in popularity since 1969.
Specifically, the Rorschach, TAT, H-T-P, and DAP tests have
been among the top 10 test instruments used in each decade
(Lubin et al., 1984). The instruments that clinical psychologists
use the most seem to cluster consistently into a core battery that
includes the WAIS or WISC, the MMPI, and several of the
more popular projective tests, including the Rorschach and TAT
(Watkins, 1991). This has not changed much since the 1960s.
Watkins noted that though the data suggest a steady decline in
the percentage of time that practicing psychologists devote to
assessment (from 44% in 1959, down to 22% in 1982 over all
five settings) most of them currently spend a fair portion of
their time conducting assessment services.
The Test Usage Survey
The present study was designed to gather information on the
current use of psychological assessment instruments by clinical
psychologists and neuropsychologists. This study diverged from
previous studies of psychological test usage in several ways. First,
the sample was limited to clinical psychologists and neuropsy-
chologists who reported that assessment services accounted for a
substantial part of their practice. Second, this survey asked more
specific questions, such as (a) the amount of time spent per week
conducting assessments and (b) whether assessments were intel-
lectual, developmental, adaptive-functional, or neuropsychologi-
cal in nature.
Participants included 1,002 members of the National Associa-
tion of Neuropsychology (NAN) and 1,500 clinical psychologists
from the American Psychological Association (APA), randomly
selected from the respective databases of each institution. The
neuropsychologists were randomly selected from among approxi-
mately 2,300 NAN members. The clinical psychologist sample
was randomly selected from a population of approximately 35,000
doctoral members of APA in independent practice who specialize
in providing mental health services as their primary or secondary
positions.
Instrumentation
We mailed all participants the six-page "Survey of Test and
Assessment Use in Professional Psychology." The initial draft of
this survey was reviewed by more than 20 psychologists who were
members of APA Division 40 (Clinical Neuropsychology), Divi-
sion 42 (Psychologists in Independent Practice), and APA gover-

SPECIAL SECTION: PSYCHOLOGICAL TEST USAGE 143
nance groups with expertise in assessment.1 In addition to evalu-
ating the proposed questions, reviewers were asked to study the
draft list of tests and identify additional instruments that should be
added to the list. We pilot tested a revised survey with an addi-
tional 20 practitioners, and they also identified a number of addi-
tional tests to be included in the list of tests for the final survey.
Their comments and suggestions were incorporated, raising the
number of tests for the final survey from 75 to 120.
The survey included items inquiring about (a) the amount of
time devoted to assessment services in a typical week, (b) use of
tests for eight different areas of assessment and the use of specific
assessments, and (c) participant's credentials and experience. Par-
ticipants devoting 4 hr a week or less to assessment services were
asked to stop and return the survey, because the survey designers
felt that individuals who engaged minimally in assessment services
might not have enough recent experience to estimate the time
required for completing different services. Those engaged in as-
sessment services for more than 4 hr per week completed the
remaining survey items.
We asked participants about the use of assessments for eight
different areas of assessment. We decided on these practice areas
for assessment services through a consensus process involving 45
members of APA divisions and governance groups with expertise
in assessment. The areas and brief definitions adapted from the
survey are
1. Adaptive-functional behavior. The assessment of adaptive behavior
is concerned with the degree to which individuals function indepen-
dently and meet satisfactorily the demands of personal and social
responsibility imposed by the culture. Assessments are designed to
determine a person's competence in meeting the independence-related
needs and social demands of the environment (e.g., communication,
daily living skills, socialization, and motor skills). Instruments such as
behavior scales, behavioral checklists, and direct observation are used
to assess independent functioning skills, physical development, lan-
guage development, and academic competencies (Sattler, 1992).
2. Aphasia. Aphasia is the loss or impairment of language due to some
type of brain injury. The purpose of this type of evaluation is to
determine the language areas affected and to provide a starting point
for language retraining. Most aphasia tests describe what the patient
can do, so that remaining functions (not defects) are tested. A typical
aphasia evaluation may include assessments of (a) perception and
recognition of language (auditory and visual); (b) performance of
motor functions pertaining to language (speaking and writing); (c)
ability to use language symbols in reading, handwriting, and mathe-
matics; and (d) formulation and comprehension of prepositional lan-
guage (oral and written; Agranowitz, McKeown, & Nielsen, 1964).
3. Behavioral medicine or rehabilitation. Behavioral medicine is an
"interdisciplinary field concerned with the integration of behavioral
and biomedical science knowledge and techniques relevant to health
and illness and the application of this knowledge and these techniques
to prevention, diagnosis, treatment, and rehabilitation. Assessments
within this domain seek to appraise the medical patient's present
status within the context of the past and within his or her larger social
framework or environment, including current physical and psycho-
social stressors. Objective instruments are used to assess the patient's
overt behaviors and evaluate self-reported feelings and biophysical
processes (Schneiderman & Tapp, 1985).
4. Developmental. Developmental assessment can be characterized as
a process for obtaining clinical information about a child in order to
provide answers to development-related questions and to generate
appropriate intervention strategies. Assessments may entail obtaining
an overall index of development or securing a detailed assessment of
the child's level of functioning across different areas (e.g., motor
development, language development, social development, etc.). The
focus may be on documenting changes over time through repeated
assessments (Johnson & Goldman, 1990).
5. Intellectual or achievement. Intelligence tests assess learning that
occurs in a wide variety of life experiences. Achievement tests are
heavily dependent on formal learning acquired at school or home.
With children, the main goal(s) of intellectual or achievement assess-
ments include determining the nature of the child's learning or be-
havior problems (i.e., the child's strengths and weaknesses in abilities
related to learning). With adults, these assessments are used to deter-
mine the level of intellectual functioning or knowledge in one or more
specific domains (e.g., math, science). Evaluations are usually based
on norms for similar-aged individuals (e.g., young children, older
adults). A comprehensive battery should include a measure of global
intelligence and measures of the information-processing skills in-
volved in comprehension, visualization, memory, reasoning, and
judgment (Sattler, 1992).
6. Neurobehavioral clinical examinations. These instruments are used
to evaluate the extent that individual's social and emotional function-
ing are affected by the brain and potential brain-impaired processes.
The participants are most often adults and young adults who may have
encountered a head injury or are suspected of some degenerative
illness. These assessments are used to examine daily problem-solving
strategies (e.g., daily living tasks, independence) and reasoning abil-
ities as they may be affected by the brain and any brain impairment.
Assessments in this area are similar to those used in more generalized
neuropsychological assessment in that they involve a variety of in-
formal and formal measures about a person's level of neurological
functioning.
7. Neuropsychological assessments. Most participants of these assess-
ments are suspected of having had some type of physical brain injury,
such as a blow to the head, a stroke, or carbon monoxide poisoning.
These assessments rely on many of the same techniques, assumptions,
and theories as do other psychological assessments. The distinction
lies in the focus on brain function as the point of departure (Lezak,
1995). The goal is to be able to evaluate the full range of basic
physical and mental abilities that are controlled directly by the brain.
Reducing the symptomatology of the brain-impaired individual to its
basic processes requires not only a general understanding of the
functional aspects of behavior and cognition but also a specific
understanding of how these functions relate to the brain and to brain
dysfunction in particular (Golden, Zillmer, & Spiers, 1992).
8. Personality-psychopathology. These assessments are usually con-
ducted when a person's behavior problems, emotional difficulties,
social interactions, or ability to function independently become so
significantly disruptive or disrupted that mental health intervention
appears warranted (Knoff, 1986). Personality assessment helps iden-
tify and characterize an individual's social-emotional status and atti-
tudes, behaviors, and reactions to specific and recent or general and
long-existing situations or environments. Personality assessments in-
clude formal or informal observation, interviews, and evaluation
processes addressing an individual's behavior, social-emotional de-
velopment or progress, or self-concept formation.
Respondents indicated the approximate number of times per
year they administer a "full battery" of tests in each of the eight
1 The Board of Professional Affairs, the Board of Scientific Affairs, and
the Committee on Psychological Tests and Assessment.

144 CAMARA, NATHAN, AND PUENTE
designated areas of assessment, and individual tests used. For
example, a participant using tests for intellectual assessment would
indicate the number of times he or she had conducted such assess-
ments in a year, as well as the average time spent for each of the
three assessment services: administration, scoring, and interpreta-
tion. In addition, the questionnaire asked participants to indicate
which tests they had used from a list of 120 individual tests, to
identify which of the eight practice areas the test-was used for, and
to identify the average time spent for each of the three assessment
services. Participants provided information about the mode of
testing (computer or paper and pencil) and were also asked to write
in the names of any additional tests they had used that were not on
the list.
Procedure
We first mailed the "APA Survey" questionnaires in late 1994,
accompanied by a cover letter from the APA president at the time,
Ronald E. Fox, explaining that the purpose of the study was to
estimate the frequency of use of psychological and neuropsycho-
logical assessment and the approximate amount of time required
for assessment services (administration, scoring, and interpreta-
tion). We sent two mailings. We received responses from 1,499
(56%) of the total of 2,700 individuals selected, 933 clinical
psychologists (62% of the sample of 1,500), and 566 neuropsy-
chologists (47% of the sample of 1,200).
Of the 1,499 respondents, 754 of the clinicians and 119 of the
neuropsychologists reported conducting assessment services for
under 5 hr in a typical week; these questionnaires were set aside.
We conducted analyses only on questionnaires from the partici-
pants who engaged in 5 hr or more of assessment-related services
in a typical week. Therefore, 179 clinicians and 447 neuropsy-
chologists qualified for the remaining analyses. Nine additional
tests "written-in" by 5 or more respondents were added to the
initial list of tests, resulting hi a final list of 129 tests used in the
analyses.
We conducted all analyses separately for the clinical psycholo-
gist and neuropsychologist samples. The types and uses of assess-
ments and the assessment services provided by these two groups of
psychologists differ greatly, so responses from these groups are not
combined for any analysis. However, comparisons of the types of
assessment services provided, time required for completing ser-
vices, and frequency and types of assessments used by these
groups are reported later.
Frequency in Conducting Assessments
Table 1 illustrates the number of hours clinical psychologists
and neuropsychologists devote to assessment during a typical
week. As shown in Table 1, more than 80% of clinical psycholo-
gists reported spending less than 5 hr during a typical week in
administering, scoring, reporting, and interpreting psychological
tests, whereas more than 80% of neuropsychologists spend an
average of 5 or more hr per week in providing these assessment
services.
Of the clinical psychologists, approximately 4% of respondents
engage in assessment for 10-14 hr, 15-20 hr, or more than 20 hr
during a typical week, with 7% spending 5-9 hr providing assess-
ment services. More than a third of neuropsychologists spend hi
Table 1
Hours Spent Individually Administering, Scoring, and
Interpreting Psychological Tests During a Typical Week
Clinical
psychologists
Hours
0-45-9
10-1415-20More than 20No response
Total
n
755
62
39
36
374
933
%
81
744
4
100
Neuropsychologists
n
1166292
105188
4
567
%
2111161933
100
excess of 20 hr per week on assessment activities, with another
third of them spending 10—20 hr per week on assessment. The final
31 % devote 10 hr per week or less to assessment.
We conducted the remaining analyses for only those 447
neuropsychologists and 179 clinical psychologists who reported
engaging in assessment activities for 5 hr or more in a typical
week. Table 2 shows that neuropsychologists most often
conduct assessments for purposes of neuropsychological as-
sessment (95%), intellectual-achievement assessment (79%),
personality-psychopathology (79%), and neurobehavioral clinical
assessment (51%). Even so, more than a quarter of all neuropsy-
chologists report conducting assessments for each of the eight
purposes listed in the survey. Table 2 reports the mean and median
number of full test or assessment batteries conducted by neuro-
psychologists who practice in a given assessment area. The median
is by far the better indicator of central tendency for assessment
services provided by neuropsychologists. In seven of the eight
practice areas, approximately 20% of neuropsychologists account
for greater than 50% of assessments being conducted. In these
areas, the mean number of assessments per respondent exceeds the
median by 50% or more.
Among neuropsychologists, there was substantial variation in
the number of times they annually administer a full battery of
assessments in each of the practice areas. For example, for neu-
ropsychological assessment batteries and intellectual-achievement
batteries, some respondents had conducted only a few assessments
annually, whereas one neuropsychologist conducted more than 400
full assessment batteries in the past year. Most of the variation
was due to 10% of neuropsychologists who reported conducting
well more than 200 neuropsychological assessment batteries,
intellectual-achievement batteries, and neurobehavioral clinical
examination batteries annually.
Clinical psychologists involved in assessment services for 5 or
more hr per week are most often involved in personality-
psychopathology testing (93%) and intellectual-achievement test-
ing (88%), followed by neuropsychological assessment (47%),
adaptive-functional behavioral assessment (40%), and develop-
mental assessment (30%). There was substantial variation in the
number of full psychological batteries they administered in some
areas, mostly because of the number of assessments performed by
the most productive 10% to 20% of clinicians in each area. Clinical
psychologists differed most in how often they conducted neuro-
psychological assessments, intellectual-achievement assessments,

SPECIAL SECTION: PSYCHOLOGICAL TEST USAGE 145
Table 2Number and Percentage of Full Assessment Batteries Administered Annually
Clinical psychological
Practice area
Adaptive-functional behavior assessmentAphasiaBehavioral medicine-rehabilitationDevelopmentalIntellectual-achievementNeurobehavioral clinical examinationNeuropsychologic alPersonality-psychopathology
Total
«(%)
72(40)30(17)26(15)53 (30)
158 (88)30(17)84 (47)
166(93)179
Mdn
20.013.513,520.050.030.030.050.0
M
36.328.428.335.987.359.163.680.4
SO
47.846.430.847.0
110.073.5
116.0101.0
n(%)
194 (43)205 (46)127 (28)115(27)354 (79)228(51)427 (95)353 (79)447
Neuropsychological
Mdn
20.025.030.020.060.050.070.050.0
M
36.953.670.346.290.488.996.887.5
SD
54.470.492.291.796.787.991.3
115.0
and personality-psychopathology assessments. Figures 1 and 2illustrate total activity within each assessment area. Assessmentsfor intellectual-achievement, personality-psychopathology, andneuropsychological purposes account for the great majority oftesting for both clinical psychologists and neuropsychologists.
Earlier research reporting on reasons for referral suggested thatmost referrals were requests for a complete assessment, personalityassessment, or intellectual assessment {Lubin et al., 1984). Re-quests in 1982 for a neuropsychological assessment, across the fivesettings, yielded a composite overall low of 3%. In the currentstudy, however, clinical psychologists involved in assessment ser-vices were testing most often for personality-psychopathology
(93%) and intellectual-achievement (88%), followed by neuropsy-chological assessment (47%). Moreover, neuropsychologists weremost often involved in neuropsychological assessment (95%), fol-lowed by intellectual-achievement and personality-psychopathologyassessment (both 79%). These data suggest that neuropsychologicalassessments have become increasingly popular within the last decade.
Given the wide variation in the frequencies and patterns ofassessment services provided by clinicians and neuropsycholo-gists, it is extremely difficult to characterize the "typical amount ofassessment activity" of these practitioners. The median provides amore accurate picture of the amount of assessment activity in theseareas for most practitioners in both groups, yet there is a small
Beh. Med/Rehabilitation2%
AphasiaNeurobehavioral 2%
4%Developmental
5%
Adaptive/Functional
Neuropsychological13%
Intellectual/Achievement34%
Personality/Psychopathology32%
Figure 1. Proportion of assessment services, by area, conducted by clinical psychologists. Beh. Med.behavioral medicine.

146 CAMARA, NATHAN, AND PUENTE
Beh. Med/Rehabilitation6%
Intellectual/Achievement20%
Neurobehavioral13%
Developmental3%
Adapt! w/Functional
Personality/Psychopathology20%
Neurops ychological26%
Figure 2. Proportion of assessment services, by area, conducted by neuropsychologists. fleh, Med.behavioral medicine.
percentage (10%-20%) of practitioners who conduct twice asmany assessments as the typical practitioner in this study. It is alsoimportant to remember that practitioners providing less than 5 hrof assessment services in a typical week, 80% of clinicians, and20% of neuropsychologists already have been excluded from theseanalyses.
Time Required to Administer, Score, and Interpret a FullAssessment Battery
The amount of time required for completing a full psychologicalor neuropsychological assessment battery may vary widely, for anumber of obvious reasons; (a) the number and types of tests usedin an assessment; (b) the mode of administration (e.g., paper andpencil, computer based); (c) the intended use(s) of the assessment(e.g., a quick neurological screening vs. a full neuropsychologicalexamination, a full psychoeducational evaluation vs. a reevalua-tion); (d) the characteristics, symptoms, and abilities of the clientor patient being tested; (e) the setting; and (f) the level of reportingand interpretation required (e.g., written reports, oral briefings,court reports), to name just a few. However, though the timerequirements for specific tests and assessments also were exam-ined, it is also important to provide some estimates of both thenumber of full assessments completed, by area, and the timerequirements for administration, scoring, and interpretation, if weare to understand the general demands of assessment services.
It is rare that clinical psychologists or neuropsychologists useonly one or two tests ia completing an assessment. They are morelikely to use several tests in conducting brief reevaluations or
screenings, or to use an extensive array of tests in completing a fullassessment battery for diagnostic or evaluative purposes. Table 3provides (a) the number of clinicians who administer, score, andinterpret assessments in the eight areas; (b) the average amount oftime (in min) that is required to provide these services for a fullbattery of assessments; and (c) the standard deviation of the timerequired. Table 4 provides an identical breakdown for theneuropsychologists.
First, nearly all clinical psychologists administer, score, andinterpret assessments when conducting a full psychological assess-ment battery. Some have suggested that an increasing proportionof clinicians may be only interpreting assessment results, whilegiving the duties of administration and scoring to another provider(someone with less training who might operate at a lower cost, oranother vendor who provides computehzed administrative ser-vices). Our evidence suggests that most clinicians are directlyresponsible for administering, scoring, and interpreting assess-ments in each assessment area.
Second, test administration required the greatest amount of timein each assessment area, followed closely by the time required forinterpretation and the time required for scoring. We used thefollowing definitions for these services in the instructions includedin the questionnaire:
Administration: time required in the preparation for testing (selectingtests, preparing testing materials and test site) and actual administra-tion of a test or assessment. Do not include time required for the clientto complete self-administered tests.

SPECIAL SECTION: PSYCHOLOGICAL TEST USAOE 147
Table 3
Minutes Required by Clinical Psychologists to Administer, Score, and Interpret a Full Psychological Assessment Battery
Administer
Practice area
Adaptive-functional behavior assessmentAphasiaBehavioral medicine-rehabilitationDevelopmentalIntellectual-achievementNeurobehavioral clinical examinationNeuropsychologicalPersonality— psychopathology
Total
n
59
302452
1563084
162607
M
72.8
77.3151.099.8
115.085.1
208.0104.097.4
Mdn
60.037.5
120.072.5
100.067.5
180.090.0
SD
82.8113.0145.098.168.360.5
144.076.4
n
70302453
1562583
163602
Score
M
34.2
36.245.7
35.131.336.259.4
49.942.0
Mdn
20.017.530.0
30.030.0
20.045.045.0
SD
42.565.858.2
41.332.6
57.860.537.8
n
71
3024
531562885
166613
Interpret
M
47.463.2
107.0
69.665.067.599.187.875.9
Mdn
30.020.060.0
30.045.0
40.060.060.0
SD
58.1147.0159.0113.078.677.4
111.093.6
Scoring: time required to score individual responses and derived
scores (including subscale scores, standardization scores, norm-
referenced scores, or comparisons) and to collaborate with test ad-
ministrator or psychometrician when necessary. When scoring ser-
vices (computer-based scoring or machine scoring) are used, scoring
includes the time required to forward raw test data to the service,
review and verify score reports, and any follow-up interactions re-
quired with the service.
Interpretation and reporting: time required to review raw test data
(quantitative and qualitative) and scoring reports and time required to
synthesize all relevant data (e.g., medical, historical), complete writ-
ten and oral reports, and provide interpretation to client, family, or
referral source. When services provide interpretative reports, interpre-
tation time also includes the review, verification, and elaboration of
the report.
Across assessment areas, administration accounted for 45% of
the overall time required in conducting assessment services. Scor-
ing and interpretation-reporting accounted for 36% and 19%,
respectively. Most notably, there was substantial variation among
practitioners in the time required to administer and interpret full
psychological assessment batteries but less variation in scoring
time.
The time required for clinical psychologists to administer and
interpret-report assessment results differed across assessment ar-
eas, whereas the time required for scoring assessments remained
fairly consistent, across all areas of assessment. Neuropsycholog-
ical assessment consumed the most time, on average requiring
50% more time to administer (M = 208 min, Mdn =180 min) than
the average clinical assessment did. Interpretation and repotting of
results from assessments conducted for behavioral medicine and
rehabilitation purposes, neuropsychological assessment, and per-
sonality or psychopathology assessments consumed substantially
more time than assessments in other areas (an average of 93 min
across these areas compared with an average of 62 min for the
remaining five assessment areas). Most of the variation is due to
the number and choice of tests selected by clinicians for inclusion
in a full psychological battery.
For the neuropsychological sample (see Table 4), the time
required for administering full assessment batteries (55% of the
total time spent providing assessment services) far exceeded the
average time required for scoring (16%) and interpretation-
reporting results (28%). The time required for assessments con-
ducted for neuropsychological purposes or behavioral medicine-
rehabilitation purposes far exceeded the time required for other
uses of assessment. The times required by neuropsychologists for
providing assessment services were more uniform than the times in
the clinical sample, perhaps indicating more uniformity in the
numbers and types of assessment instruments used.
The times required for providing assessment services are sub-
stantially similar across areas for both the clinical and neuropsy-
chological samples but vary widely according to the intended
purpose of the assessment (Camara, Nathan, & Puente, 1998). The
time required to complete a full neuropsychological assessment
battery requires substantially more time than assessments in other
areas. Assessments conducted for personality-psychopathology,
Table 4
Minutes Required by Neuropsychologists to Administer, Score, and Interpret a Full Psychological Assessment Battery
Administer
Practice area
Adaptive-functional behavior assessmentAphasiaBehavioral medicine-rehabilitationDevelopmentalIntellectual-achievementNeurobehavioral clinical examinationNeuropsychologicalPersonality-psychopathology
Total
n
88
202
123114350227
422335
1,961
M
73.660.7
110.0113.0122.080.0
304.0103.0140.83
Mdn
60.045.090.090.0
120.060.0
300.090.0
SD
87.652.177.080.876.367.1
136.097.6
n
87
20312311134820042048
1,940
Score
M
32.223.635.335.833.425.878.5
46.041.74
Mdn
20.015.0
30.030.030.020.060.0
30.0
SD
74.219.024.927.724.822.551.638.7
n
88
202
124
114
350
223
425
3501,976
Interpret
M
48.039.158.259.461.346.8
135.074.971.66
Mdn
30.030.045.030.040.030.0
120.060.0
SD
82.440.044.655.773.938.5
115.078.2

148 CAMARA, NATHAN, AND PUENTE
behavioral medicine-rehabilitation, intellectual-achievement, and clinicians using the Rorschach Psychodiagnostic Test ("inkblot
developmental evaluation purposes required more time on average test") and 107 using the TAT, followed by the H-T-P Protective
than assessments conducted for adaptive-functional behavior. Technique (60 users), Human Figures Drawing Test (49 users),
aphasia, and neurobehavioral clinical purposes. Assessments con- Rotter Incomplete Sentences Blank (45 users), Sentence Comple-
ducted in the latter three areas can often be characterized as briefer (ion Test (40 users), and the CAT (38 users). The Bender Visual
screenings or examinations used to assess behavioral functioning Motor Gestalt Test was the third most frequently used test, with
or specific diagnoses, requiring less time than the more exhaustive 112 users, but this use may be divided among neuropsychological
diagnostic assessments used in the former applications. screening, projective assessment, and intellectual-achievement as-
sessment. Several intelligence and achievement tests were among
Frequency of Use of Individual Tests and Assessments the most frequently used assessments: the WAIS-R, with 151
Table 5 provides a rank-ordered list of the top 20 tests used by users; the W^C-II, with 135 users; ̂ *« Wide Rmie Achieve-clinical psychologists or neuropsychologists who conduct assess- ment Test (WRAT), with 86 users. Finally, a few inventories and
ment services for 5 or more hr in a typical week. Only 161 of the screening tests were also often cited for use by the clinical sample.
179 respondents completed this section of the survey. Clinical Among Aese were me Wechsler Memory Scale—Revised (58
psychologists indicated they used an average of 13.4 (Mdn = 13.0) users>- && Trailmaking Test A&B (52 users), the Conners' Parent
separate tests. The MMPI was the most frequently used test used and Teacher Rating Scales (37 users), and the Vineland Adaptive
by 138 clinical psychologists (more than 86%). The Beck Depres- Behavior Scales (37 users).
sion Inventory (53 users), the Millon Clinical Multiaxial Inventory Respondents were asked to indicate the number of times they
(53 users), and the Millon Adolescent Personality Inventory (38 use (i.e., administer, score, and interpret-report) each test annu-
users) were the next most often cited personality tests. Projective ally. This question attempts to determine the highest utilization
assessments were also used by a majority of respondents, with 124 rate among psychologists using the various tests. Among tests used
Table 5
Frequency and Rank Order of Tests Used by Clinical Psychologists and Neuropsychologists
Clinicalpsychologists
Test
Aphasia Screening Test0
Beck Depression InventoryBender Visual Motor Gestalt TestBoston Naming TestCalifornia Verbal Learning TestCategory TestChildren's Apperception Test (CAT-A)Conners' Parent and Teacher Rating ScalesFAS Word Fluency TestFinger Tapping Test"Grooved Pegboard Test"Halstead-Reitan Neuropsychological Test BatteryHand Dynamometer (Dynamic Hand Grip Strength Test)Hooper Visual Organization TestHouse-Tree-Person (H-T-P) Projective TechniqueHuman Figures Drawing TestMillon Adolescent Clinical InventoryMillon Clinical Multiaxial InventoryMinnesota Multiphasic Personality Inventory (MMPI) I and IIPeabody Picture Vocabulary Test — RevisedRey Complex Figure TestRorschach Inkblot TestRotter Incomplete Sentences BlankSentence Completion TestThematic Apperception Test (TAT)Trail Making Test A&B°Vineland Adaptive Behavior ScalesWechsler Adult Intelligence Scale— Revised (WAIS-R)Wechsler Intelligence Scale for Children — Revised (WlSC-R-ni)Wechsler Memory Scale — RevisedWide Range Achievement Test — Revised and IIIWisconsin Card Sorting Test
Rank
23105
42363116
183729
442344598
1316102
20254
14156
12
181397
33
n
2753
11213182038371722
1227
128
60493853
1383425
124
45
40
1075237
151135588619
Neuropsychologists
Rank
1711258
149
603956
157
2019314156241
2812185142
26
4
44
21639
12
n
156200
96209189203
29
57241228180214136145785535
100359
891961534154
91
246
51
331178257203
196
Total n
186
253208222207223
6794
25825019224114815313810473
153497
123221
1778694
198298
8$482313315289215
Note. Only tests ranked in the top 20 by either the clinical or neuropsychology sample are listed in the table. * A subtest of the Halstead-Reitan and theReitan-Indiana Neuropsychological Batteries. b A subtest of the Halstead-Russell Neuropsychological Evaluation System. c A subtest of the Halstead-Reitan Neuropsychological Battery,
SPECIAL SECTION: PSYCHOLOGICAL TEST USAGE 149
by a substantial portion of the clinical sample, the Bender Qestalt,
the Human Figures Drawing Test, the Rotter Incomplete Sentences
Blank, the MMPI, the Rorschach, and the H-T-P Projective Tech-
nique were used an average of over 65 times across users.
Finally, regarding frequency of test use, the current study sug-
gests very little change since the 1960s. The Rorschach, TAT, and
H-T-P were among the top 10, indicating the sustained popularity
of projectives. Also unchanged from previous research were the
inclusions of the WAIS and WISC, Bender Gestalt, MMPI, and
WRAT in the top 10. One change was the inclusion of the Millon
Clinical Multiaxial Inventory in the top 10. For further details,
Table 5 provides the top rank ordering of tests ranked in the top 20
by either clinical psychologists or neuropsychologists.
Neuropsychologists use an average of 17.6 (Mdn = 15.0) dif-
ferent tests in their assessment practice, with 10% of respondents
using over 30 different tests. Neuropsychologists were much more
likely than clinical psychologists to write in additional tests that
were not on the original list provided in the survey; over 100
respondents wrote in five or more tests. A total of 18 respondents
did not complete this section. Table 5 also provides a rank ordering
of the top 20 tests used by the remaining 430 neuropsychologists.
Overall, a large number of neuropsychological batteries and
individual neuropsychological assessments used for screening spe-
cific functions were used by a large percentage of these respon-
dents: the Wechsler Memory Scale—Revised (257 users), Trail
Making Test A&B (Halstead-Reitan; 246 users), FAS Word Flu-
ency Test (also known as the Controlled Word Association Test,
Spreen & Strauss, 1991; 237 users), Finger Tapping Test2 (228
users), Halstead—Reitan Neuropsychological Test Battery (214 us-
ers), Boston Naming Test (20& users), Category Test (209 users),
Wisconsin Card Sorting Test (196 users), Rey Complex Figures
Test (196 users), California Verbal Learning Test (189 users),
Grooved Pegboard Test3 (180 users), Aphasia Screening Test4
(159 users), Hooper Visual Organization Test (145 users), and the
Hand Dynamometer (Dynamic Grip Strength Test; 136 users).
As with the clinical sample, the MMPI was the most frequently
used test (359 users). Additional personality tests often used by
this sample were the Beck Depression Inventory (200 users) and
the Millon Clinical Multiaxial Inventory (100 users). The Ror-
schach Inkblot Test and the TAT were the most frequently used
projective instruments, with 153 and 91 users, respectively. The
WAIS-R, WRAT, and WISC-H were the most commonly used
intelligence and aptitude tests (with 331, 203, and 178 users,
respectively).
The following several instruments had the highest utilization
rates among all tests used by a substantial percentage (25% or
more) of the sample: Trail Making A&B (Halstead-Reitan),
WAIS-R, MMPI, Wechsler Memory Scale—Revised, Rey Com-
plex Figures Test, FAS Word Fluency Test, and the WRAT. Each
of these was used an average of 90 or more times annually by test
users.
It should be noted that test use varied markedly by assessment
area. The frequency and rank order of tests used within each of the
eight assessment areas show some substantial disparities from the
overall list. For example, the Bender Gestalt, which ranked fifth
among clinical psychologists, was the most frequently used assess-
ment for intellectual and achievement assessments and neurobe-
havioral clinical examinations. Similarly, the Aphasia Screening
Test and the Vineland Adaptive Behavior Scales were the tests
most often used by neuropsychologists when assessment was
conducted for aphasia screening and adaptive-functional behavior.
However, these tests ranked 17th and 44th, respectively, in total
use by neuropsychologists (Camara et al., 1998).
Unfortunately, when the data are sorted by assessment area, the
number of responses in each area is so low that the reliability of the
rankings within many assessment areas is also extremely low.
Fewer than 50 respondents provided specific rankings and
frequency-of-use data for assessments in five of the eight areas,
and between zero and seven tests were used by three or more
respondents for each assessment area. Therefore, results of test use
frequencies and rank ordering lack sufficient reliability to indicate
relative use within these five areas: adaptive-functional behavioral
assessment, aphasia assessment, behavioral medicine and rehabil-
itation, developmental assessment, and neurobehavioral clinical
examinations.
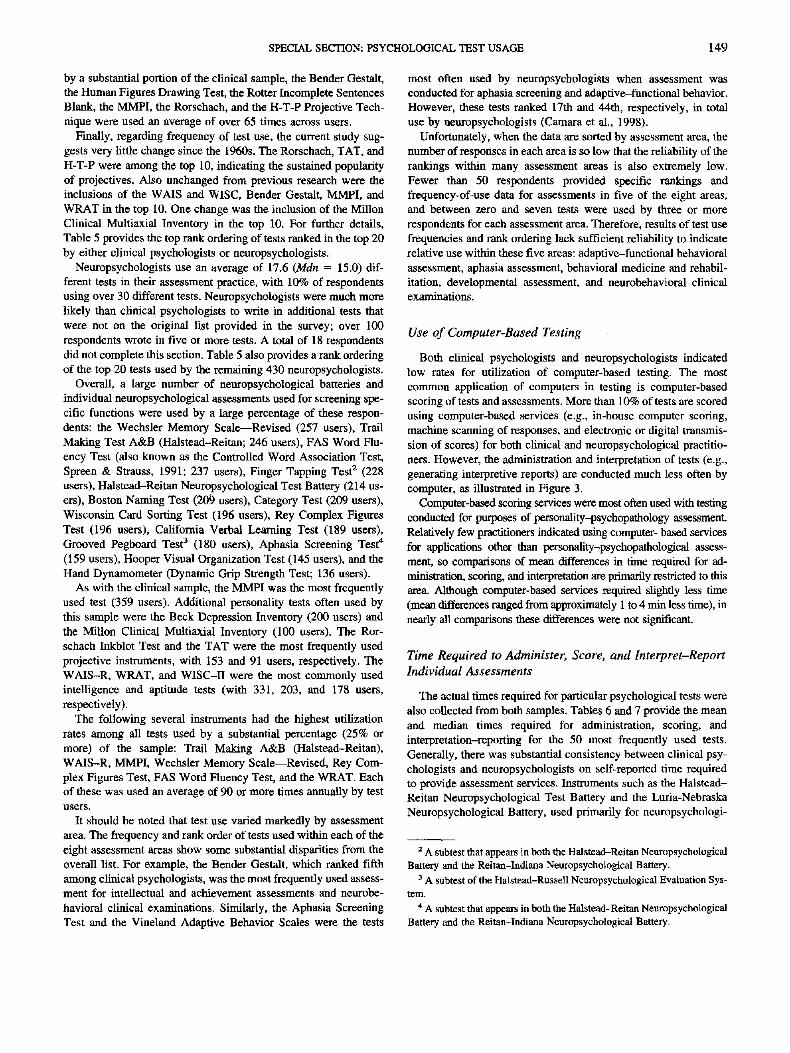
Use of Computer-Based Testing
Both clinical psychologists and neuropsychologists indicated
low rates for utilization of computer-based testing. The most
common application of computers in testing is computer-based
scoring of tests and assessments. More than 10% of tests are scored
using computer-based services (e.g., in-house computer scoring,
machine scanning of responses, and electronic or digital transmis-
sion of scores) for both clinical and neuropsychological practitio-
ners. However, the administration and interpretation of tests (e.g.,
generating interpretive reports) are conducted much less often by
computer, as illustrated in Figure 3.
Computer-based scoring services were most often used with testing
conducted for purposes of personality-psychopathology assessment.
Relatively few practitioners indicated using computer- based services
for applications other man personality-psychopathological assess-
ment, so comparisons of mean differences in time required for ad-
ministration, scoring, and interpretation are primarily restricted to thisarea. Although computer-based services required slightly less time
(mean differences ranged from approximately 1 to 4 min less time), in
nearly all comparisons these differences were not significant.
Time Required to Administer, Score, and Interpret-Report
Individual Assessments
The actual times required for particular psychological tests were
also collected from both samples. Tables 6 and 7 provide the mean
and median times required for administration, scoring, and
interpretation-reporting for the 50 most frequently used tests.
Generally, there was substantial consistency between clinical psy-
chologists and neuropsychologists on self-reported time required
to provide assessment services. Instruments such as the Halstead—Reitan Neuropsychological Test Battery and the Luria-Nebraska
Neuropsychological Battery, used primarily for neuropsychologi-
2 A subtest that appears in both the Halstead-Reitan Neuropsychological
Battery and the Reitan-Indiana Neuropsychological Battery.3 A subtest of the Halstead-Russell Neuropsychological Evaluation Sys-
tem.4 A subtest that appears in both the Halstead-Reitan Nenropsychological
Battery and the Reitan-Indiana Neuropsychological Battery.

150 CAMARA, NATHAN, AND PUENTE
12.0% -f
10.0%-
8.0%-
6.0%-
4.0%-
2.0%-
0.0%
10.4% 10.3%
3.6%
2.4%
1.J
0 Clinical Psychologists
D Neuropsychologists
3.9%
3.1%
Administration Scoring Interpretation
Figure 3. Percentage of testing services conducted with computers.
cal assessments, required the most time for administration, scoring,and interpretation (an average of 6.5 hr and over 4 hr, respec-tively). Next in consumption of time were intelligence tests such asthe Kaufman Assessment Battery for Children, the Stanford-BinetIntelligence Scale, and the various Wechsler scales. The RorschachInkblot Test and the Woodcock-Johnson Psycho-Educational Bat-tery—Revised required, on average, over 2 hr for completion.
Conclusions and Implications for Professional Practice
This study provides a broad survey of the assessment practicesfor clinical psychologists and neuropsychologists today. Nearly80% of neuropsychologists reported providing assessment servicesfor more than 4 hr weekly, with one third of them spending over 20hr per week in this area. Assessment services account for arelatively minor aspect of practice for the over 80% of clinicalpsychologists who spend 4 hr or less each week conducting as-sessment services. However, assessment services are a substantialcomponent of practice for the more than 12% of clinicians whospend 10 or more hr in this practice area.
Patterns of assessment practice reveal that evaluations ofpersonality-psychopathology and intellectual-achievement ac-count for over two thirds of assessments conducted by clinicalpsychologists. Not only do most psychologists conduct assess-ments in these two areas, but the ratio of assessments per psychol-ogist practicing in these areas (87.3 and 80.4 assessments perpractitioner, respectively) far exceeds the ratios in the remainingsix assessment areas. Neuropsychological assessments andadaptive-functional behavior assessments are the next most pop-ular use of psychological testing, with approximately 50% ofclinical psychologists practicing in these areas.
Assessment practice by neuropsychologists is somewhat more var-ied as to area, with neuropsychological, personality-psychopathology,and intellectual-achievement evaluations each accounting for 20%or more of all assessments. Neurobehavioral clinical examinationswere the next most frequent use of assessment, accounting for anadditional 13% of all assessment practice in the field. More thanhalf of all neuropsychologists practice in all of these four assess-ment areas. The ratio of testing among neuropsychologists prac-ticing in assessment areas was consistent across these four areas,ranging from 87.5 to 96.8 assessments per practitioner. In addi-tion, neuropsychologists report taking substantially more time tointerpret-report results from assessments than do clinical psychol-ogists, whereas time required for administration and scoring aremore comparable.
Results from this project have implications for the reimburse-ment of psychological assessment services by third parties andreimbursement-authorization of such services by managed care.This study empirically determined that the mean time required toadminister, score, and interpret a full psychological or neuropsy-chological battery was more than 3.5 hr by experienced clinicalpsychologists and 4.25 hr for neuropsychologists, with additionaltime required for assessments conducted in some practice areas.
Psychological assessment faces enormous obstacles in the cur-rent health care delivery system, ranging from outright refusal toreimburse assessment, difficulties in gaining preauthorization fortesting, or requirements that practitioners use medication for dif-ferential diagnosis (Eisman et al., 1998). Current guidelines issuedby most managed care organizations do not provide separatereimbursement of assessment services, either requiring the psy-chologist to reduce treatment time if assessment services are

SPECIAL SECTION: PSYCHOLOGICAL TEST USAGE 151
Table 6
Minutes Required to Administer, Score, and Interpret Individual Tests: Clinical Psychologists
Test
Aphasia Screening Test"Beck Depression InventoryBender Visual Motor Gestalt TestBoston Naming TestCalifornia Verbal Learning TestCategory TestChild Behavior ChecklistChildren's Apperception Test (CAT- A)Children's Depression InventoryConners' Parent and Teacher Rating ScalesDevelopmental Test of Visual-Motor
IntegrationFAS Word Fluency TestFinger Tapping Test"Grooved Pegboard Test6
Halstead-Reitan Neuropsychological BatteryHand Dynamometer (Dynamic Hand Grip
Strength Test)House-Tree-Person (H-T-P) Projective
TechniqueHuman Figures Drawing TestKaufman Assessment Battery for ChildrenKinetic Drawing System for Family and
School: A HandbookLuria-Nebraska Neuropsychological BatteryMemory Assessment ScalesMillon Adolescent Clinical InventoryMillon Clinical Multiaxial InventoryMinnesota Multiphasic Personality Inventory
(MMPI) I and nMyers-Briggs Type IndicatorPeabody Picture Vocabulary Test — RevisedPersonality Inventory for ChildrenRey Complex Figures Test
Reynolds Adolescent Depression ScaleRoberts Apperception Test for Children
Rorschach Inkblot TestRotter Incomplete Sentences BlankSymptom Checklist-90— Revised
(SCL-90-R)Sentence Completion TestShipley Institute of Living ScaleSixteen Personality Factor QuestionnaireStanford-Binet Intelligence ScaleStrong Interest Inventory (4th Ed.)Stroop Neuropsychological Screening TestTest of Visual-Motor Integration (TVMI)
Thematic Apperception Test (TAT)Trail Making Test A&B°Vineland Adaptive Behavior ScalesVineland Social Maturity ScaleWechsler Adult Intelligence Scale — Revised
(WAIS-R)Wechsler Intelligence Scale for Children —
Revised and m (WISC-R and m)Wechsler Memory Scale — RevisedWide Range Achievement Test — RevisedWisconsin Card Sorting TestWoodcock-Johnson Psycho-Educational
Battery — Revised
No. ofpsychologists
2753
11213182029381437
2017221227
12
604919
2514123853
138103410251125
124
45
1240
11
1522151925
107523713
151
135588619
30
No. of uses peryear
M
30.348.279.141.539.835.754.823.445.757.4
32.6
69.158.571.838.4
56.4
65.573.820.4
66.415.729.027.241.8
66.816.123.729.842.828.429.266.170.8
67.154.0
80.819.620.67.1
52.022.3
47.446.627.410.8
53.1
56.940.768.449.9
55.3
SD
43.0
49.095.152.836.9
36.743.839.080.275.6
34.561.548.051.044.8
62.4
70.681.043.8
63.721.019.2
35.949.2
93.428.2
35.930.940.6
14.725.8
103.9122.6
89.657.8
147.816.524.95.1
39.922.4
86.654.936.19.6
60.4
69.045.4
105.568.3
76.0
Mdn
20.0
25.040.020.0
27.517.5
36.013.520.030.0
24.050.050.0
55.020.0
50.0
40.040.010.0
50.08.0
35.015.0
24.5
36.05.0
10.020.040.0
25.020.032.535.0
40.030.040.020.010.05.0
50.015.020.026.019.010.0
25.0
30.020.030.030.0
30.0
Min to administer
M
24.8
11.115.718.830.643.0
13.136.2
11.611.2
19.2
15.112.5
8.5237.8
6.3
17.314.7
70.3
14.0126.853.814.819.4
29.814.022.95.5
19.916.839.845.316.6
15.215.315.936.168.825.015.315.538.414.3
51.124.6
78.6
82.448.731.931.3
90.5
SD
11.9
10.07.9
11.811.913.517.918.58.0
15.6
24.227.59.64.1
135.5
3.1
7.78.1
23.9
6.362.1
19.917.321.6
37.012.610.57.28.8
16.517.420.612.2
16.410.513.036.731.123.56.14.3
19.28.7
19.710.7
22.1
25.725.320.2
12.6
68.6
Mdn
20.0
10.015.015.0
30.045.0
10.030.010.010.0
15.07.0
10.0
10.0240.0
5.0
15.015.060.0
15.0120.0
50.010.010.0
10.010.020.0
2.520.010.035.045.015.0
12.515.0
10.030.0
60.015.015.015.0
30.012.545.020.0
75.0
80.045.030.030.0
72.5
Min to score
M
11.48.2
11.38.8
16.713.120.019.29.6
12.2
13.08.36.24.7
57.3
4.9
11.012.3
27.1
8.134.317.5
16.018.8
21.918.012.421.514.9
12.321.644.812.1
10.312.010.516.322.6
137.7
10.511.619.59.5
25.715.4
22.9
24.719.615.720.4
33.4
SD
7.37.27.57.48.68.7
11.221.1
5.07.3
12.514.13.22.4
36.5
2.7
10.613.824.5
11.323.6
5.013.816.2
16.512.16.5
15.68.37.2
15.931.712.2
8.810.2
7.68.3
11.0349.3
6.94.7
19.910.312.414.2
15.7
18.511.211.4
16.0
22.9
Mdn
10.05.0
10.05.0
15.010.020.015.010.010.0
10.05.05.05.0
60.0
5.0
10.010.020.0
5.030.015.015.015.0
20.017.510.020.010.010.020.037.510.0
10.010.010.015.020.05.0
10.010.015.05.0
30.010.0
20.0
20.015.015.015.0
30.0
Min to interpret
M
14.112.512.39.6
34.620.323.329.710.414.7
12.37.67.84.9
81.9
5.3
15.014.137.1
13.353.921.332.429.3
36.146.015.4
20.524.217.333.850.617.8
22.521.818.425.0
31.330.013.912.934.213.826.613.2
35.3
39.223.517.7
19.3
36.9
SD
9.914.08.97.4
69.816.916.129.06.5
11.2
9.07.56.12.0
74.7
2.6
8.59.6
30.2
10.033.88.6
17.8
17.3
32.947.710.913.460.018.122.845.712.1
18.517.618.717.9
21.519.98.4
11.429.425.716.910.1
40.1
44.1
14.514.514.1
28.2
Mdn
10.010,010.010.0
17.515.020.027.510.010.0
10.05.05.05.0
60.0
5.0
15.010.030.0
10.052.520.030.0
25.0
30.027.515.015.010.0
10.030.030.015.0
15.015.015.020.0
30.020.010.010.030.010.030.010.0
30.0
30.020.015.015.0
30.0
Note. Only the top 50 most popular tests were included in this table.• A subtest of the Halstead-Reitan and the Reitan-Indiana Neuropsychological Batteries. b A subtest of the Halstead-Russell NeuropsychologicalEvaluation System. " A subtest of the Halstead-Reitan Neuropsychological Battery.

152 CAMARA, NATHAN, AND PUENTE
Table 7
Minutes Required to Administer, Score, and Interpret Individual Tests: Neuropsychologists
Test
Aphasia Screening Test"Beck Depression InventoryBender Visual Motor Gestalt TestBenton Judgment of Line Orientation TestBenton Revised Visual Retention TestBoston Diagnostic Aphasia ExaminationBoston Naming TestCalifornia Verbal Learning TestCategory TestChild Behavior ChecklistConners' Parent and Teacher Rating ScalesDementia Rating ScaleDevelopmental Test of Visual-Motor
IntegrationFinger Tapping TestGrooved Pegboard Testb
Halstead-Reitan Neuropsychological BatteryHand Dynamometer (Dynamic Hand Grip
Strength Test)Hooper Visual Organization TestHouse-Tree-Person (H-T-P) Projective
TechniqueHuman Figures Drawing TestLuria-Nebraska Neuropsychological BatteryMemory Assessment ScalesMUlon Clinical Multiaxial InventoryMinnesota Multiphasic Personality Inventory
(MMPI) I and 11Neuropsychological Questionnaire
(Adult Form)Paced Auditory Serial Addition TestPeabody Picture Vocabulary Test — RevisedPeabody Individual Achievement
Test — RevisedRey Complex Figures TestRhythm Test"Rorschach Inkblot TestRotter Incomplete Sentences BlankSymptom Checklist-90— Revised (SCL-90-R)Sensory Perceptual Examination"Sentence Completion TestShipley Institute of Living ScaleSpeech Sounds Perception Testc
Stroop Neuropsychological Screening TestTactile Finger Localization TestTactile Performance TestThematic Apperception Test (TAT)Test of Visual-Motor IntegrationTrail Making Test A&B°Vineland Adaptive Behavior ScalesWechsler Adult Intelligence Scale — Revised
(WAIS-R)Wechsler Memory Scale — RevisedWechsler Intelligence Scale for Children —
Revised and HI (WISC-R and HI)Wide Range Achievement Test — RevisedWisconsin Card Sorting TestWoodcock-Johnson Psycho-Educational
Battery — Revised
No. ofpsychologists
15920096908066
2091892035257
120
43
228
180214
136145
78556450
100
359
49
110
89
50
196
79153
414387545775
11848769173
24651
331257
178
203196
58
No.
M
69.069.268.650.354.134.1
81.371.959.883.359.446.4
62.678.377.867.1
66.0
63.5
55.960.3
24.043.652.3
94.3
88.660.247.6
43.692.770.754.4
76.956.788.2
75.166.366.6
60.970.561.540.243.999.228.9
94.593.1
59.7
89.177.5
51.2
of uses peryear
SD
88.2
84.985.564.080.041.585.865.669.4
114.0
89.551.8
66.8
81.874.576.1
67.1
70.1
53.757.641.7
51.162.0
121.8
97.368.566.5
54.2
91.277.771.3
103.953.397.3
119.597.279.457.093.373.6
45.252.192.633.7
92.085.9
63.688.469.3
47.9
Mdn
35.0
42.540.030.030.020.050.050.035.050.0
40.025.0
37.5
50.050.040.0
40.0
50.0
35.042.512.022.540.0
50.0
50.0
40.020.0
20.070.040.035.037.550.050.037.527.535.050.030.035.025.020.070.015.0
70.060.0
30.051.050.0
30.0
Min
M
21.510.416.515.718.246.816.832.4
38.110.0
8.338.3
14.7
12.68.8
250.0
7.3
13.7
19.714.8
160.251.522.3
38.5
27.2
22.722.1
42.7
17.712.147.412.212.723.113.418.318.7
11.79.8
34.637.316.911.545.0
83.453.3
81.630.830.3
80.2
to administer
SD
19.89.2
14.36.4
15.336.7
15.315.718.916.3
8.018.4
5.9
18.75.0
136.5
6.77.6
22.58.7
94.922.121.8
44.5
27.911.99.9
24.010.06.1
20.6
12.812.130.212.810.022.5
10.26.8
29.919.7
16.315.124.7
35.1
23.0
30.119.315.0
58.6
Mdn
15.010.015.015.015.040.0
15.030.035.05.05.0
35.0
15.010.010.0
240.0
5.010.0
15.015.0
157.550.015.0
15.0
20.0
20.020.0
40.015.010.045.05.0
10.020.010.020.015.0
10.010.030.030.015.010.040.0
90.060.0
75.030.030.0
60.0
Min to score
M
9.55.9
11.45.9
12.619.8
7.617.210.213.89.9
13.8
12.25.04.8
54.4
4.36.5
12.29.8
46.519.419.2
24.7
10.4
9.710.3
16.314.45.7
47.78.0
15.66.86.6
11.4
6.38.44.09.4
20.5
11.66.1
19.8
24.621.4
21.813.1
16.8
22.5
SO
8.84.57.94.1
8.715.5
6.1
11.06.58.25.27.3
8.33.14.6
37.6
2.96.2
10.98.1
42.210.021.5
54.9
12.76.4
6.1
11.38.6
3.835.97.99.95.69.36.24.48.23.35.1
22.3
10.37.8
11.9
29.211.0
11.37.4
11.7
11.2
Mdn
5.05.0
10.05.0
10.015.0
5.015.010.012.5
10.015.0
10.05.05.0
60.0
5.05.0
10.010.030.020.015.0
15.0
10.0
10.010.0
15.015.05.0
40.05.0
15.05.0
10.010.05.05.05.0
10.015.010.05.0
15.0
20.020.0
20.010.0
15.0
20.0
Min to interpret
M
13.2
9.514.6
7.910.922.7
9.317.013.113.112.119.1
10.37.06.2
95.3
5.88.8
16.912.062.120.827.2
30.4
23.310.311.6
16.712.27.6
45.012.912.410.5
17.511.67.9
10.66.3
12.627.810.58.0
33.0
29.3
21.6
29.914.614.3
31.4
SD
11.99.2
30.85.69.1
22.7
7.715.88.9
10.39.4
15.2
11.15.44.0
94.4
4.57.1
11.08.4
56.712.323.7
21.4
23.37.38.5
12.19.4
5.3
41.97.37.6
7.612.26.86.48.75.18.0
24.516.46.5
43.5
23.914.5
24.611.2
9.5
30.2
Mdn
10.05.0
10.05.0
10.015.08.0
15.010.010.0
10.015.0
10.0
5.05.0
60.0
5.05.0
15.010.045.020.020.0
30.0
15.010.010.0
12.510.05.0
30.015.0
10.010.0
15.010.05.0
10.05.0
10.025.0
5.05.0
15.0
25.020.0
25.010.0
10.0
20.0
Note. Only the top 50 most popular tests were included in this table.a A subtest of the Halstead-Reitan and the Reitan-Indiana Neuropsychological Batteries. b A subtest of the Halstead-Russell NeuropsychologicalEvaluation System. c A subtest of the Halstead-Reitan Neuropsychological Battery.

SPECIAL SECTION: PSYCHOLOGICAL TEST USAGE 153
provided, to "eat these costs," or to simply pass on costs to the
client. Other managed care organizations stipulate that behavioral
interviews are the only necessary diagnostic assessment because
the Diagnostic and Statistical Manual of Mental Disorders (4th
ed.; DSM-IV; American Psychiatric Association, 1994) makes no
reference to other psychological or neuropsychological assess-
ments (Eisman et al., 1998).
When assessment services are reimbursed limits of less than 2 hr
are most typical. Such guidelines from managed care are clearly
inconsistent with the empirical research from this study demon-
strating that comprehensive assessment services require approxi-
mately 4 or more hr of time by a trained professional. Because
practitioners can be reimbursed for the actual time required to
conduct comprehensive assessment services under existing man-
aged care guidelines there is a danger that assessment services will
be dramatically restrained or eliminated from intake and treatment
planning. This study showed that less than 12% of clinical psy-
chologists spend 5 or more hr on assessment services. In the future,
fewer practitioners may engage in such services for less time than
currently reported. Clinical psychologists may also reduce the
number of assessments used and possibly reduce the time ex-
pended in interpretation and reporting of results if reimbursement
is not provided.
The economic barriers created under managed care may con-
tinue to reduce the quality of assessment services and the extent
that such services are provided in some areas (e.g., intake, diag-
nosis, treatment planning). There are several general strategies that
the profession of psychology and individual practitioners can
consider to more directly affect these economic and health care
policy issues.
First, practitioners must be creative in incorporating assessment
as a central component within their interventions and treatments so
that is not considered an option or supplemental service that must
be justified and added onto reimbursement for treatment. Assess-
ment services are often medical necessities and not an option.
Practitioners should view and portray assessments as an integral
component of effective treatment planning and mental health in-
terventions. Practitioners should explore ways of incorporating and
describing such services as a component of treatment plans.
Second, evidence of the efficacy of psychological and neuro-
psychological assessment in the treatment of patients and the
disposition of treatment is needed. Barlow (1994) and Broskowski
(1995) observed that in the present managed care era, mental
health services that do not have strong empirical support are not
likely to be reimbursed. Practitioners must be able to justify the
benefits of comprehensive assessment services in terms of treat-
ment focus, treatment duration, and cost-to-benefit ratio. Has a
comprehensive assessment aided in the initial diagnosis and effec-
tiveness of treatment planning in ways that both focus the subse-
quent psychological interventions and reduce the overall length of
treatment for a client? Has assessment been effectively used to
inform treatment and make the necessary adjustments throughout
the intervention, or to provide summative evidence of the efficacy
of treatment? Practitioners can advance such arguments with man-
aged care by submitting case records and other data that support
the effectiveness of assessment practices. Evidence demonstrating
that assessment services in diagnosis or treatment have been ef-
fective in reducing the duration of treatment or reducing the
recidivism of mental health problems will be viewed as compelling
by managed care because of its economic relevance.
An APA task force has recently summarized evidence of the
benefits of psychological assessment in assessing current function-
ing, in confirming or disconfirming clinical impressions, in dif-
ferential diagnosis, in identifying appropriate treatments, in mon-
itoring treatment, in risk management, and as a therapeutic inter-
vention (Meyer et al., 1998). More constructive interactions with
mental health care systems are needed to reduce the misunder-
standings and biases against assessment and to help define criteria
for medical necessity of assessment services. Just as practitioners
must advance such evidence when arguing for the reimbursement
of assessment services, the profession must advocate more force-
fully with the use of such evidence of the effectiveness and utility
of assessment services in addressing mental health problems.
Finally, assessment services must be viewed as a more inte-
grated component of professional practice rather than an indepen-
dent service. Practice guidelines, and discussion of such guide-
lines, issued by the Agency for Health Care Policy and Research
(AHCPR), the American Psychiatric Association, and a Task
Force of APA's Division 12 generally put little if any emphasis on
the use of assessment services in treatment planning and evalua-
tion. Whereas such guidelines have been highly controversial
within the mental health profession, the absence of assessment
services has not been a primary concern of mental health profes-
sionals at this time. Such guidelines strive to reflect best practices,
advocate empirically supported treatment, and improve the stan-
dard of care (Nathan, 1998). Objective and comprehensive assess-
ments are essential in aiding the profession and professionals in
guiding treatment and determining the efficacy of treatment. Pre-
and postassessment strategies can help practitioners objectivelydemonstrate the effect of treatment. The lack of attention to as-
sessment services in existing practice guidelines is troubling and
must be addressed if the influence of such guidelines increase.
Eisman et al. (1998) proposed a number of additional strategies
to reduce obstacles for reimbursement and precertification of as-
sessment services. These recommendations include enhanced leg-
islation and advocacy, public education to make customers and
patients aware of the benefits of psychological assessment, ex-
panded and continuing training of psychologists to ensure they are
skilled in assessment and aware of current practice standards and
ethical requirements, and criteria to help decision makers recog-
nize under what circumstances assessment is most helpful and
appropriate. Critics have argued that assessment is time consum-
ing, expensive, and not useful (Griffith, 1997), and it is clear that
until practitioners and the profession develop more effective em-
pirically based methods of advocacy the current misconceptions
about the utility of psychological and neuropsychological assess-
ments will remain.
References
Agranowhz, A., McKeown, M. R., & Nielsen, J. M. (1964). Aphasia
handbook for adults and children. Springfield, IL: Charles C Thomas.
American Psychiatric Association. (1994). Diagnostic and statistical man-
ual of mental disorders (4th ed.). Washington, DC: Author.
Ball. J. D., Archer, R. P., & Imhof, E. A. (1994). Time requirements of
psychological testing: A survey of practitioners. Journal of Personality
Assessment, 63(2), 239-249.

154 CAMARA, NATHAN, AND PUENTE
Barlow, D. H. (1994), Psychological intervention in the era of managedcompetition. Clinical Psychology: Science and Practice, I, 109-122.
Broskowski, A. T. (1995). The evolution of health care: Implications forthe training and careers of psychologists. Professional Psychology:Research and Practice, 26, 156-162.
Brown, W. R., & McGuire, J. M. (1976). Current psychological assessmentpractices. Professional Psychology, 7, 475-484.
Camara, W. J., Nathan, J., & Puente, A. (1998). Psychological test usagein professional psychology: Report to the APA Practice and ScienceDirectorates. Washington, DC: American Psychological Association.
Eisman, E. J., Dies, R. R., Finn, S. E., Eyde, L. D., Kay, G. G., Kubiszyn,T. W., Meyer, G. L, ftMoreland, K. L. (1998). Problems and limitationsin the use of psychological assessment in contemporary healthcaredelivery: Report of Board of Professional Affairs Psychological Assess-ment Working Group, Pan 11. Washington, DC: American PsychologicalAssociation.
Golden, C. J., Zillmer, E., & Spiers, M. (1992). Neuropsychologicalassessment and intervention. Springfield, IL: Charles C Thomas.
Griffith, L. (1997). Surviving no-frills mental health care: The future ofpsychological assessment. Journal of Practical Psychiatry and Behav-ioral Health, 3, 255-258.
Johnson, J. H., & Goldman, J. (1990). Developmental assessment inclinical child psychology: A handbook. New York: Pergamon Press.
Knoff, H. M. (1986). Identifying and classifying children and adolescentsreferred for personality assessment: Theories, systems, and issues. InH. M. Knoff (Ed.), The assessment of child and adolescent personality(pp. 3-31). New York: Guilford Press.
Lezak, M. D. (1995). Neuropsychological assessment (3rd ed.). New York:Oxford University Press.
Louttit, C. M., & Browne, C. G. (1947). Psychometric instruments inpsychological clinics. Journal of Consulting Psychology, I I , 49—54.
Liibin, B., Larsen, R. M., & Matarazzo, J. D. (1984). Patterns of psycho-
logical test usage in the United States: 1935-1982. American Psychol-ogist, 39, 451-454.
Lubin, B., Wallis, R. R., & Paine, C. (1971). Patterns of psychological testusage in the United States: 1935-1969. Professional Psychology, 2,70-74.
Meyer, G. I., Finn, S. E., Eyde, L. D., Kay, G. G., Kubiszyn, T., Moreland,K., Eisman, E., & Dies, R. (1998). Benefits and costs of psychologicalassessment in healthcare delivery: Report of Board of ProfessionalAffairs Psychological Assessment Working Group, Part II. Washington,DC: American Psychological Association.
Nathan, P. E. (1998). Practice guidelines: Not yet ideal. American Psy-chologist, 53, 290-299.
O'Roark, A. M., & Exner, J. E. (Eds.). (1989). History and directory:Society for personality assessment fiftieth anniversary. Hillsdale, NJ:Erlbaum.
Saltier, J. M. (1992). Assessment of children: Revised and updated (3rded.). San Diego, CA: Jerome M. Sattler.
Schneiderman, N., & Tapp, J. T. (1985). Behavioral medicine: The bio-psychosocial approach. New York: Erlbaum.
Spreen, E., & Strauss, C. (1991). Compendium of neuropsychological tests.New York: Oxford University Press,
Sundberg, N. D. (1961). The practice of psychological testing in clinicalservices in the United States. American Psychologist, 16, 79-83.
Watkins, C. E., Jr. (1991). What have surveys taught us about the teachingand practice of psychological assessment? Journal of Personality As-sessment, 56(3), 426-437.
Received April 6, 1999Revision received December 9, 1999
Accepted December 10, 1999
ORDER FORMStart my 2000 subscription to Professional Psychology:Research and Practice! ISSN: 0735-7028
$46.00, APA Member/Affiliate$92.00, Individual Nonmember$198.00, InstitutionIn DC add 5.75% sales tax
TOTAL AMOUNT ENCLOSED $
Subscription orders must be prepaid. (Subscriptions are ona calendar basis only.) Allow 4-6 weeks for delivery of thefirst issue. Call for international subscription rates.
SEND THIS ORDER FORM TO:American Psychological AssociationSubscriptions750 First Street, MEWashington, DC 20002-4242
AMERICANPSYCHOLOGICALASSOCIATION
Or call (800) 374-2721, fax (202) 336-5568.TDD/TTY (202)336-6123. Email: [email protected]
Send me a Free Sample Issue Q
Q Check Enclosed (make payable to APA)
Chargemy: Q VIS A Q MasterCard Q American ExpressCardholder NameCard No. Exp. date
Signature (Required for Charge)Credit CardBilling AddressCity State Zip.Daytime PhoneSHIP TO:Name
City. State .ZipAPA Customer #
GADOO
PLEASE DO NOT REMOVE - A PHOTOCOPY MAY BE USED


















