PSONews Summer 2013 Edition
12
The Center for Paent Safety is one of several PSOs across the naon working together to evaluate, beer understand and share learning about safety issues arising from the use of health informaon technology. Highlights come from informaon the Center and other parcipang PSOs are receiving from their parcipants. The following arcle represents Highlight Topic I of the Health IT Safety project. Please be sure to share in this learning by sending us informaon about your facility’s HIT related events, near misses and unsafe condions! From the Center for Patient Safety PSONEWS SUMMER 2013 EDITION IN THIS EDITION PSOs Collaborate Show Instead of Tell Paent Safety Culture Survey Second Vicms Webinar Series Center Tidbits A Fall Free Culture PSO Data Snapshot PSO Calendar 1 2 3 4 6 7 8 10 12 HIT and safety issues See PSO Data Snapshot, page 10 for more on HIT issues at “Contribung factors: Technology” PSOs collaborate to learn and share www.centerforpatientsafety.org Did You Know Links leading to many valuable resources and forms are available by clicking on the text in the electronic version of this newsletter. Using Personal Devices as a Workaround – Not an Uncommon Scenario One Case - In order to facilitate rapid communicaon of the progress of a wound, the bedside nurse took a picture of the wound with her personal cell phone and texted it to the physician. The hospital had no guidelines in place for use of personal cell phones for communicang paent informaon, but seemed unconcerned as long as there was no informaon that idenfied the paent. Neither the picture of the wound nor the communicaon was documented in the paent’s medical record. The Problem Healthcare workers report that using personal devices to communicate paent informaon (rather than an approved process) is easier and IT departments have been too slow to provide workers with new technology. These workers also report they felt workarounds were necessary to deliver efficient and effecve care to their paents. Such workarounds can lead to unintended consequences. They jeopardize the integrity of documentaon and communicaon of paent care, which can result in error and paent harm. And, protected health informaon (PHI) is at risk if transmied via an unencrypted form with a personal device. Suggesons for Prevenon 1. Provide staff with encrypted devices to deter reliance on personal devices. 2. Develop clear BYOD (bring your own device) policies and guidelines for the use of personal devices for communicaon of paent informaon. 3. Educate staff about the unintended consequences of such workarounds. 4. Ensure the IT department is agile and responsive in evaluang, securing and enabling mely use of new technology for frontline staff.
-
Upload
center-for-patient-safety -
Category
Documents
-
view
221 -
download
5
description
Â
Transcript of PSONews Summer 2013 Edition

The Center for Patient Safety is one of several PSOs across the nation working together to evaluate, better understand and share learning about safety issues arising from the use of health information technology. Highlights come from information the Center and other participating PSOs are receiving from their participants. The following article represents Highlight Topic I of the Health IT Safety project. Please be sure to share in this learning by sending us information about your facility’s HIT related events, near misses and unsafe conditions!
1w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
From the Center for Patient SafetyPSONEWS
SUMMER 2013 EDITION
IN THIS EDITIONPSOs CollaborateShow Instead of TellPatient Safety Culture SurveySecond VictimsWebinar Series Center TidbitsA Fall Free CulturePSO Data SnapshotPSO Calendar
12346781012
HIT and safety issuesSee PSO Data Snapshot, page 10 for more on HIT issues at “Contributing factors: Technology”
PSOs collaborate to learn and share
w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
Did You KnowLinks leading to many valuable resources and forms are available by clicking on the text in the electronic version of this newsletter.
Using Personal Devices as a Workaround – Not an Uncommon ScenarioOne Case - In order to facilitate rapid communication of the progress of a wound, the bedside nurse took a picture of the wound with her personal cell phone and texted it to the physician. The hospital had no guidelines in place for use of personal cell phones for communicating patient information, but seemed unconcerned as long as there was no information that identified the patient. Neither the picture of the wound nor the communication was documented in the patient’s medical record. The ProblemHealthcare workers report that using personal devices to communicate patient information (rather than an approved process) is easier and IT departments have been too slow to provide workers with new technology. These workers also report they felt workarounds were necessary to deliver efficient and effective care to their patients.
Such workarounds can lead to unintended consequences. They jeopardize the integrity of documentation and communication of patient care, which can result in error and patient harm. And, protected health information (PHI) is at risk if transmitted via an unencrypted form with a personal device. Suggestions for Prevention1. Provide staff with encrypted devices to deter
reliance on personal devices.2. Develop clear BYOD (bring your own device)
policies and guidelines for the use of personal devices for communication of patient information.
3. Educate staff about the unintended consequences of such workarounds.
4. Ensure the IT department is agile and responsive in evaluating, securing and enabling timely use of new technology for frontline staff.

CENTER FOR PATIENT SAFETY
SHOW TELL
2
instead of
R e S P O n d i n g t O m e d i a c R i t i c i S m S a b O u t S a f e t y
When unpleasant news coverage shines a bright light on an industry, it can go into a purely defensive mode, or it can use the opportunity to improve and redirect public focus. The long- term care (LTC) community’s reaction to the recent series, “Life and Death in Assisted Living,” brought out self-reflection among long-term care providers.
• Read the series on the ProPublica website at http://www.propublica.org/series/life-and-death-in-assisted-living. The site also has a link to the PBS Frontline TV program.
While some of the concerns addressed in the series (such as a spotty regulatory structure) are unique to assisted living, it also focused on issues like staffing and financial incentives to keep beds full, which are common to all levels of long-term care.
The series centered on a for-profit company, but the interface of financial and safety issues it addressed also arises in non-profit homes. All long-term care providers face the challenge of providing great care with resources that seem to shrink daily.
Ultimately, the series spoke to the ubiquitous fears of baby boomers about the safety of their elders in these communities. How can a home respond to fears about safety? By developing a culture that is all about safety.
Here’S HoW:
The Agency for Healthcare Research and Quality long-term care Survey of Safety Culture is a great start. It gets to the heart of many important issues.• Do staff believe that ownership and
management support safety? • Do staff work as a team for the benefit
of residents? • Does the home learn as it moves
forward to become even safer?
The survey identifies problem areas in the organization’s culture.
Resources now available from the Center for Patient Safety can help to address issues identified by the survey, including long-term care Patient Safety Organization (PSO) services dedicated to the collection and analysis of information about safety issues and working with participants to improve long-term care. Safety culture work, including the survey results and actions taken in response, can be fully protected and confidential for participants of the Center’s PSO.
The Center’s long-term care culture and PSO services are available to any long-term care provider and are available at no charge to Missouri’s licensed long-term care providers through a grant from the Missouri Foundation for Health.
Residents and their families want to know they have chosen a home where safety is a top priority. A strong safety culture speaks more loudly than any editorial response or advertising campaign. Let the Center help you!
w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
Did You Knowinterested in receiving the latest news and information from the center? click here to subscribe and receive updates direct to your inbox.

SUMMER 2013
CULTURE surveyIssues involving adverse events in healthcare settings have been surfacing in the news lately. The causes are being identified as a lack of safety culture.
When you hear the word culture, what comes to mind? A culture is often easiest to define if you consider “what happens when no one is looking.” To take the meaning a step further: culture is the thoughts, attitudes, and behaviors that staff consider “normal” at your organization.
To determine your organization’s patient safety culture, take the short quiz at right.
eacH UNiT/area HaS a cUlTUre of iTS oWN
The most valuable survey results are often derived when organizations survey their areas and units separately, analyzing the results on unit-to-unit basis.
If you have administered a survey on patient safety culture in the past and your scores were average, you may want to consider administering the survey at the department, unit, or office level rather than taking a “house-wide” approach. It has been found that many organizations distribute the survey to all staff without differentiating between units. This often results in the stronger units balancing out the weaker units resulting in unremarkable scores.
By surveying individual areas, you may be surprised to find several areas that have very high culture results. Use these valuable resources to lead action teams and let them determine and implement best practices throughout your organization. This option can save you time and money and expedite improvements in patient outcomes!
THe ceNTer caN HelP
The Center for Patient Safety can administer the Survey on Patient Safety (SOPS) for your long-term care home, hospital, physician clinics, or pharmacy. Surveys are available in English and Spanish. Learn more online, or request a quote from the Center for Patient Safety.
STaff focUS oN PaTieNT SafeTy
A culture of safety should be reflected in your organization’s mission, vision and values and have leadership commitment. Lack of executive leadership is quickly recognized by the frontline staff and the culture suffers accordingly.
Suggestion: Consider incorporating executive walkarounds as an interventional technique to engage executive leaders and supervisors with frontline staff in patient safety processes.
TUrNover
While high turnover can be attributed to multiple factors, remember that tenured staff members tend to be more engaged, and as a result, they are good facilitators to promote patient safety processes. Low turnover is often associated with a positive culture that supports and engages staff in open communication with supervisors and peers.
Suggestion: Administer the Survey On Patient Safety to individual departments and compare the results to turnover rates and employee and physician engagement scores.
The SOPS dimension results will indicate if your units are struggling with teamwork, communication, staffing, or handoffs. Your organization may be a candidate for the Comprehensive Unit-based Safety Program (CUSP) or Just Culture implementation.
vieW THe ceNTer’S SoPS ServiceS
eveNT rePorTiNg
A positive safety culture will encourage and promote reporting activities that lead to learning and improvements. If staff members are not reporting, consider whether there are apprehensions because of a current culture of blame. Remember to determine if events occur as a blatant disregard for the outcome, or are staff simply vulnerable to poor processes?
Suggestion: You may want to consider incorporating a “just” culture at your organization.1 Newman, Karin, Maylor, Uvanney, and Chansarkar, Bal. (2001), The nurse retention, quality of care and patient satisfaction chain, International Journal of Health care Quality Assurance 14, 2, 57-64.
3
The Center for Patient Safety recognizes your commitment to safety as a PSO participant. Therefore, we now offer a 20 percent discount to Center PSO participants that would like to use our services to
conduct the Survey on Patient Safety (SOPS). fiND oUT More!
“There is a clear interrelationship between employee satisfaction, the quality of care, and patient satisfaction” 1
WHaT’S yoUr cUlTUre?
Think of your long-term care home, hospital, pharmacy, or physician clinic and select the answer that best fits:
QUESTION #1: STAFF FOCUS ON PATIENT SAFETYA. Staff are always focused on patient safetyB. The focus on patient safety is highest when a supervisor is around
QUESTION #2: TURNOVERA. Turnover in our departments is better than averageB. All, or some, departments have very high turnover
QUESTION #3: EVENT REPORTINgA. Staff always report adverse events and near misses. Often, individuals report more than five per year.B. Staff members report few near misses and fewer unsafe conditions. On average, individuals report about 1 per year.
If you answered B to any of the questions above, your culture may require a more thorough assessment.

Being a health professional often requires putting emotions aside for the sake of patients. But despite the emotional resilience that allows health care providers to care for their patients under stressful, high-stakes circumstances, sometimes an unexpected clinical event or outcome can have a heavy emotional impact. Named ‘second victims’ by Albert Wu, these health care professionals often struggle alone through their emotions without an avenue to express and share them (Wu, 2000). In fact, the second victim response can take an immense professional and personal toll on the involved clinicians and can potentially lead to a career-altering experience (Scott, et al., 2010).
leSSoN learNeD
Wu’s editorial chronicled an experience from his early medical training in which a fellow resident failed to appreciate the significance of a patient’s test finding, which resulted in the patient requiring emergency surgery. The impact that clinical event had on this young resident and his colleague, Wu, would leave a lifelong impression regarding care for the caregiver in the aftermath of an unanticipated clinical event. Even though it’s been 13 years since Wu’s seminal editorial, there is now a growing appreciation regarding the emotional impact of the second victim phenomenon on the health care workforce.
TakiNg acTioN
In 2006, led by Sue Scott, PhD(c), RN, Manager-Patient Safety and Risk Management at University of Missouri Health Care and doctoral student at the Sinclair School of Nursing, a multidisciplinary research team at University of Missouri Health Care (MUHC) began studying the devastating impact that the second victim phenomenon can have on health care clinicians. Based on discussions with clinicians, the researchers defined a second victim as “health care providers who are involved in an unanticipated adverse patient event, a medical error and/or a patient-related injury and become victimized in the sense that the provider is traumatized by the event”
(Scott et. al., 2009). The MUHC patient safety researchers had two basic goals in mind – to help increase understanding and awareness of the second victim phenomenon in health care workers and to design an emotional “first aid” rapid response team for clinician support following an adverse event. The clinician rapid response system, staffed by trained colleagues/peers, would provide a “safe” zone of support within the natural working environment of the suffering clinician and would ideally occur immediately after the clinical event.
Second victims may exhibit a wide variety of physical and psychosocial symptoms. Signs and symptoms of this emotional aftershock may last days, a few weeks, a few months or even longer. Many second victims feel quite vulnerable by the wide ranging symptoms and frequently express that they have never experienced such an intense emotional response in their lives. It is estimated that the prevalence of second victims ranges between 30-50% (Edress et. Al., 2011, Scott et. al., 2009). Researchers also learned that second victims want to feel appreciated, be respected and understood, and most of all, remain a trusted member of their health care team!
THe forYOU TeaM iS eSTabliSHeD
After three years of researching the second victim phenomenon, MUHC formally deployed
a rapid response team to address the unique needs of clinicians who are experiencing the second victim phenomenon in 2009. MUHC’s group of multi-disciplinary individuals with specialized training in the second victim experience, known as the forYOU Team, provides a form of emotional first aid for the suffering clinician. A guiding principle of the forYOU Team is the understanding that each event is a unique experience with each clinician requiring individualized types and intensity of confidential social support to help facilitate the second victim’s transition through the six stages of emotional recovery.
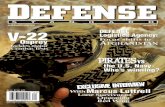
Based upon research findings, the team developed a framework of caring for future second victims. The comprehensive support network uses a three-tier intervention (refer to figure). Tier 1 provides basic emotional first aid at the “local” or departmental level. It is estimated that the vast majority of second victims receive adequate support at this level. This tier involves spreading awareness of the second victim phenomenon in an attempt to normalize the event for the caregiver. Local leaders monitor colleagues for signs/symptoms suggestive of the second victim experience and proactively approach colleagues following a critical clinical event that could potentially evoke a second victim response. Tier 2 offers guidance and support for identified second victims by their colleagues/peers. These individuals are embedded within clinical departments to continually monitor colleagues for signs
The SECOND victims a framework for caregiver suppor t
4 w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
CENTER FOR PATIENT SAFETY
Coming Soon! A dedicated LinkedIn group for
Second Victims trainers: Networking, sharing successes
and challenges and coaching from expert Second Victim faculty.
The Scott Three-Tiered interventional model of Second Victim Support

5
and symptoms suggestive of a second victim response. These “lifeguards” are equipped with special training to provide instantaneous basic one-on-one emotional support. As rapid response team members, peer supporters can activate group debriefings when an entire team is affected by an unanticipated clinical event. It is projected that this type of support and guidance meets the needs of an additional 30% of second victims. Tier 3 is utilized when peer supporters refer second victims to other internal resources who are available to assist in clinician recovery. This tier must ensure prompt availability and access to professional counseling support and guidance when a second victim’s emotional stress exceeds the expertise of the peer supporter. MUHC estimates that 10% of second victims require this level of support and guidance at some point after emotional trauma. An important element to Tier 3 support is the ability to provide a “fast-track” referral source to professional counselors. Examples of Tier 3 professionals include, but should not be limited to, clinical health psychologists, chaplains, employee assistance program personnel, wellness personnel, social workers and palliative care team members.
geTTiNg STarTeD
The nature of health care means that despite professionals’ best efforts, patients sometimes experience unanticipated clinical events. However, a strong peer-support program, such as MUHC’s forYOU Team, can help health professionals navigate the complex and potentially harmful emotions that accompany a second-victim response. Fortunately, the necessary building blocks of a comprehensive second victim response team already exist within most health care organizations.
With today’s tight health care financial environment, one might say “there is no way our hospital can afford to add a non-revenue producing program”. In fact, the support program is one you can’t afford not to offer your employees and medical staff members. MUHC’s experience has shown a peer-support program such as the forYOU Team has enhanced staff retention by preventing the resignation of talented, highly trained, and experienced professionals who are considering leaving their careers because of the emotional stress of a second-victim response. According to Scott, “saving one experienced ICU nurse from leaving his or her beloved care setting because of the anguish following an unanticipated clinical event will easily offset the nominal budget of a clinician’s support infrastructure. In fact it is projected to cost approximately $150,000 to
recruit, orient, and train a registered nurse to practice in an ICU setting.”
SUMMary
Every day health care professionals practice their art and science within complex environments and experience unexpected patient outcomes. Despite the increased understanding of the second victim phenomenon, many of today’s health care organizations are unaware of how to act on that knowledge to support their health professionals. Therefore, many clinicians still suffer alone after an unanticipated clinical event. Through proper social support and guidance, health care organizations can prevent excellent health care providers from experiencing long-term consequences such as prematurely leaving their chosen profession or experience prolonged professional and personal suffering. Health care facilities should proactively develop a plan which provides immediate support and assistance to clinicians who are experiencing the second victim phenomenon. Examples of interventional strategies to meet the unique needs of second victims include • building an environment of support and trust instead of blame • developing a process to immediately identify unanticipated events that could have an impact on clinicians • implementing formal support infrastructures utilizing current hospital resources (chaplains, social workers, Employee Assistance Programs, wellness personnel, etc.)• establishing an action plan to ensure that there is a rapid response plan in place to care for involved clinicians when a serious unanticipated event occurs
As an industry, we now know that second victim experience is common in almost every clinical setting. As health care entities, we have an obligation to our clinicians to ensure that constant surveillance and immediate ‘just in time’ emotional support strategies are developed to help mitigate second victim suffering and promote clinician recovery.
reSoUrceS are available
If you are interested in learning more about implementing a second victim support framework within your health care setting, there are several resources available. The forYOU Team has a website with information regarding the second victim phenomenon and the team structure (www.muhealth.org/secondvictim). An additional resource is the non-profit organization, the Medically Induced Trauma Support Services (MITSS), which was organized to support healing and restore hope to patients, families, and clinicians impacted by adverse events. Their website (www.mitsstools.org/tool-kit-for-staff-support-for-healthcare-organizations1.html) provides an extensive set of Tools for Building a Clinician and Staff Support Program, which includes a one-page assessment designed to serve as a roadmap for institutions interested in designing a comprehensive work plan for building a support system. In addition, the Center for Patient Safety (www.centerforpatientsafety.org) offers periodic webinars and live workshops relating to care of the second victim.
refereNceSEdrees, H.H., et al., Health care workers as second victims of medical errors. Pol Arch Med Wewn, 2011. 121(4): p. 101-8.
Medically Induced Trauma Support Services (MITSS). www.mitss.org.
Scott, S.D., Hirschinger, L.E., Cox, K.R., McCoig, M., Hahn-Cover, K., Epperly, K., Phillips, E., and Hall,L.W. (2010) Caring for our Own: Deployment of a Second Victim Rapid Response System. The Joint Commission Journal on Quality and Patient Safety. 36(5):233-240.
Scott, S.D., Hirschinger, L.E., Cox, K.R., McCoig, M., Brandt, J., and Hall, L.W. (2009). The natural history of recovery for the health care provider “second victim” after adverse patient events. Quality and Safety in Health Care. 18;325-330.
University of Missouri Health Care forYOU Team www.muhealth.org/secondvictim.
Wu, A.W., Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ, 2000. 320(7237): p. 726-7.
SUMMER 2013
Second Victims Defined…
“Healthcare team members involved in an unanticipated patient event, a medical error and/or a patient related injury and become victimized in the sense that they are traumatized by the event. Frequently, these individuals feel personally responsible for the patient outcome. Many feel as though they have failed the patient, second guessing their clinical skills and knowledge base.”

6 w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
PSO?PSES?PSWP?You have questions.
We have answers.
The Center for Patient Safety is excited to share its faculty’s expertise in the webinar series, “PSO? PSES? PSWP? You have questions, we have answers.” The series is a collaboration between the Center and VergeSolutions.
During these webinars the Center’s experts will address questions being raised by healthcare providers across the nation about:
• PSO participation and its benefits
• setting up a Patient Safety Evaluation System (PSES)
• defining Patient Safety Work Product (PSWP)
Center staff will share insights gained from our experience, plus tools and resources we’ve developed to assist others in gaining the most benefits from the sharing, learning and federal protections that are available from participating with a PSO.
The Webinar series is open to anyone interested in learning more about PSO participation, or just needing a refresher. Register here to join us for the September Webinar!
Center shares expertise nationally Free Webinar SerieS September 12 and october 16
CENTER FOR PATIENT SAFETY

7w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
ToolkiT for WorkiNg WiTH faMily caregiverSAn important part of improving patient safety is collaboration with family caregivers to provide education and increase their understanding of how they can help ensure safe care and environment for their family members as they transition from one care setting to another.
Next Step In Care offers a free Toolkit that includes numerous resources including printable materials and videos on topics such as: • how to engage family members• medication reconciliation and management• discharge planning• hand-off communication
Let’s work together to ensure a healthcare environment safe for all patients and healthcare providers, in all processes, all the time.
100 PaTieNT SafeTy beNcHMarkSUsing comparative data and searching for benchmark performance can be very time-consuming, but is necessary to assess performance and identify opportunities for improvement. Becker’s Hospital Review (August 12, 2013) published a list of 100 patient safety benchmarks from various sources. Measures include:• readmissions• mortality• complications• hospital-acquired conditions• number of safety events reported• care process measures• patient experience• patient safety culture comparisons
Bookmark this website for easy access.
cerTificaTeS available memberS-OnlY
Each PSO member can print a certificate that recognizes its participation with the Center for Patient Safety. Just answer a few questions on our PSO Participation Validation survey to confirm your participation and you’ll receive immediate access to a printable certificate. MeMberS oNly acceSS To MaTerialS
SafeTy alerT for feNTaNyl PaTcHeS Recently, the ingestion of Fentanyl patches has been identified as the cause of death for several toddlers and adults who either consumed them by mistake or in an attempt to seek opioids. In response, the Institute for Safe Medication Practices (ISMP) released a safety alert in August warning caregivers and family members about the potential danger involving the patches.
The patch is designed to release medication over 72 hours. Chewing the patch causes all the medication to be released at one time, often resulting in a fatal overdose. The ISMP is challenging “each and every healthcare professional, health system, community pharmacy, pharmaceutical company, public policy agency, and professional organization potentially associated with fentanyl patches and the patients who use them to accept personal responsibility for promoting safe use of this powerful opioid. We are exposing one of the most troubling examples of bystander apathy in healthcare.” Learn steps you can take to prevent this tragic situation in your facility, community or home.
HaTS off To cerTifieD ProfeSSioNalS iN PaTieNT SafeTyMore than 300 individuals have achieved the Certified Professional in Patient Safety (CPPS) credential since March, 2012. Congratulations to all, including those we work with closely: Mara Bollini –Washington University, St. LouisKaren Call – Mercy Health System, St. LouisLinda Maciejewski – BJC HealthCare, St. LouisRebecca Miller – Center for Patient Safety, Jefferson CityJanet Schaffner – Health Services group, Jefferson CityDeborah Smith – Phelps County Regional Medical Center, Rolla (recently retired)
For the full list, visit www.cbpps.org.
Certification requires a combination of education and experience, as well as successful completion of an evidence-based certification exam, which tests candidates on six core patient safety domains: Culture, Leadership, Risk Identification and Analysis, Data Management System Design, Mitigating Risk through Systems Thinking and Design and Human Factors Analysis, and External Influences on Patient Safety.
The CPPS credential is recommended for nurses, physicians, pharmacists, other clinicians, health care leaders, patient safety professionals, risk/quality managers and all others committed to the delivery of safe patient care. Additional information is available at www.cbpps.org. A discount on American Society for Professionals in Patient Safety (ASPPS) membership, the curriculum and certification exam are available through the Center.
Again, congratulations to all recipients!
SUMMER 2013
Center Tidbits
Did You Knowinterested in receiving the latest news and information from the center? click here to subscribe and receive updates direct to your inbox.

over 100 days without a fall on an Inpatient rehabilitation Unit?
Statistics would show that is a very difficult goal to reach, but Saint francis Medical center in Cape Girardeau, mO did just that. Patients on rehabilitation units are at high risk for falls with rates estimated to range between 2.92 to 15.9 falls per 1000 patient days. This rate is significantly higher than those for general inpatient units which range from 2.45 to 3.73 falls per 1000 patient days. rehabilitation units’ fall rates are higher due to the patients’ primary diagnoses, multiple comorbidities, and the fact that mobility and independence are promoted on these units.1 A patient at high risk for falling does not necessarily have to fall.
COmPlACenCY – everyone expects falls on a rehabilitation unit
Although standard fall-reduction interventions were in place on Inpatient Rehabilitation, falls continued to be a common occurrence. Existing interventions, including frequent risk assessments, bed enclosures, bed and chair alarms, patient and family education, and low beds did not seem to help prevent falls. Several staff members, working with the Saint Francis Fall Prevention Committee, attempted to identify why falls were happening on the unit, with no success. Additional research was performed to identify evidence-based precautions, additional equipment was purchased and staff members were reeducated, but falls still occurred. In fact, by April 1, 2013, there had been 12 falls on the unit, despite these interventions. Staff and Leadership were frustrated and decided to take a different approach to fall prevention.
WHaT cHaNgeD?
In December 2012, the CUSP (Comprehensive Unit-based Safety Program) model was introduced to Saint Francis’ Fall Prevention Committee, with the charge to utilize the concepts and tools to make a difference in the fall rate. The Inpatient Rehabilitation manager and staff embraced the model and moved ahead to lessen the number of falls. A Staff Safety Assessment was distributed early
in the year that asked staff for their opinions about how the next patient injury was most likely to occur. Leaders had identified falls as the No. 1 risk to patient safety, but they had never solicited specific input from staff. The assessment validated these concerns and led to the creation of a staff-level interdisciplinary CUSP team. The CUSP team is comprised of nurses, therapists, and even a senior executive within the organization. The team is committed to open and transparent discussions about falls. This openness helped the entire culture to evolve from “falls just happen on rehab units” to “I don’t want a fall to occur during my shift.” Transparent conversations include patients and family members so they too can be vigilant and do everything possible to avoid falls. The team is proud to report that they have gone 126 days without a fall and have had only one fall occur since beginning this program.
HoW Do THey Do iT?
Jessica Hanna, MSN, RN, patient care manager for Inpatient Rehabilitation, shared four changes that have contributed to the significant reduction of falls:
1) Fall prevention is led and owned by the staff – Hanna feels this is “a must” for success. “It’s amazing how fast staff can get their peers to buy into their own ideas. It works much better than having a mandate
On ThE CUSP:a FaLL FREE CULTURE
8 w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
CENTER FOR PATIENT SAFETY
“Our CUSP team has had tremendous success. Using a com-prehensive approach, we have had buy-in from all levels of the organization. This shows the dedication that the Saint Francis Medical Center patient care staff has for the patients and their safety.”
David C. Prather, CPA, controller, Saint francis Medical center

9
SUMMER 2013
from leadership. The frontline staff members of the CUSP team have done the research, implemented changes and communicated with their peers, medical staff members, patients and family members. They accept full responsibility and accountability for fall prevention, measuring their progress and celebrating their successes often. It’s been a win-win situation for patients and caregivers alike.”
2) Transparency and open discussion – One cannot walk onto the Rehabiliitation Unit without knowing that fall prevention is a top priority. A large sign placed in the middle of the unit hallway, shows the tally of days with no patient falls. The sign was not placed without controversy. Early on, it was taken down after a few days. Using scripted messages, providing additional one-on-one education and explaining the purpose to fellow caregivers and physicians turned the naysayers into supporters. The sign is now a welcome part of Inpatient Rehabilitation, constantly reminding staff, patients and family members to be keenly aware of the high potential of falls for all rehab patients.
3) C-suite champion support – David Prather, CPA, controller, Saint Francis Medical Center, is the team’s executive champion and actively supports the work of the team. He not only removes barriers, but is a “cheerleader” for the unit. He makes sure their learnings and successes are shared across the Medical Center. Prather encourages and thanks the team for their good work. Without active senior leader support, the CUSP team would not have the measure of success it has experienced. Prather’s participation proves that executive champions do not have to have a clinical background to influence patient safety.
4) Provide tools for caregivers –
a. Purposeful Hourly Rounding Checklist –The purposeful hourly rounding process was revamped, providing scripts on an hourly rounding checklist for all caregivers to consistently check for 4 Ps. The staff felt that the traditional 3 Ps (pain, positioning, and potty) were not sufficient; so an additional assessment regarding “possessions” was added. The staff now checks to make sure the patient’s phone, newspaper, glasses, or other personal possessions are within reach. An environmental scan is also completed to ensure furniture and cords are out of the way, and that there is a clear path to the bathroom. They also verify that lights are on when appropriate and there is no water or debris on the floor. MeMberS oNly acceSS To MaTerialS
b. Daily Activity Summary Sheet – Each patient takes this form with them to therapy. Notes and expectations are written on the form so everyone can easily see the patient’s goals and progress. This has resulted in improved communication and understanding of expectations between the nurses, therapists, patients and family members. MeMberS oNly acceSS To MaTerialS
SUcceSS – culture change!
Kim Penny, RN, chairperson of the CUSP team, said, “Creating a fall-free Rehab Unit was not easy, and we had our challenges. Our whole team was committed 100 percent to make our patients safer while they are in our care. Our team is stronger from overcoming a challenge as big as fall prevention.” Heidi
J. Hunter, MD, medical director for the Saint Francis Inpatient Rehabilitation Unit, said, “In rehabilitation, we spend our days helping our patients gain strength and independence through goal-setting and teamwork. This initiative helped a high functioning program set higher goals and work together to make the unit even safer for our patients.” The patient safety culture on Inpatient Rehabilitation is changing, and the results are worth celebrating. They have decreased their overall fall rate by 50 percent from the first quarter to the second quarter of 2013 and total falls per patient day have decreased by 18 percent. They have seen the additional benefits of decreased incontinence, increased patient satisfaction with nursing staff and overall likelihood of patients recommending the program to others. Congratulations to the caregivers on Saint Francis Medical Center’s Inpatient Rehabilitation Unit!
for More iNforMaTioN
For more information about the Saint Francis Medical Center’s Inpatient Rehabilitation CUSP initiative, contact Jessica Hanna, MSN, RN, Inpatient Rehabilitation manager, at 573-331-5335 or via email at [email protected].
For information about the overall fall reduction program at Saint Francis Medical Center, contact Vereline Johnson, MSN, RN, Patient Safety Officer, at (573) 331-5941 or via email at [email protected]. 1 Frisina, P., guellnitz, R., and Alvero, J. (2010). A time series analysis of falls and injuries in the inpatient rehabilitation setting. Rehabilitation Nursing, 35 (4), 141-148.
w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
Did You Knowfalls Prevention awareness day is September 22, 2013.

Some Patient Safety Organizations (PSOs) limit the collection of event information to specific types of events or specific levels of harm. Others may limit their scope to only pharmacies or hospitals.
The Center for Patient Safety PSO collects data on many kinds of healthcare events across the continuum of care. From Emergency Medical Services (EMS) agencies, to hospitals, to long-term care (LTC) settings, the Center achieves varied opportunities for learning as well the ability to distribute practical learnings to our participants.
The Center captures the following types of events and data from multiple healthcare providers: • medication- or other substance-related
events (hospital, EMS and LTC)• falls (hospital and LTC)• healthcare-associated infections
(hospital and LTC)• perinatal events (hospital)• stroke data (EMS) • pressure ulcers (hospital and LTC)• STEMI data (EMS)• airway events (EMS)• blood- or blood product-related events
(hospital, LTC, EMS)
• device, medical/surgical supply, and HIT-related events (hospital, EMS and LTC)
• ambulance crash events (EMS)• surgery and anesthesia events (hospital)• behavioral events (hospital and LTC)• diagnostic test-related events (hospital)
HoSPiTal DaTa:
The following data reflects event information submitted to the Center’s PSO during the period of July 2012 to May 2013. During this period, falls were again the most frequently reported event type (832), followed closely by medication events (716). Together, these two event types represent 42 percent of all hospital-reported events including those designated as “other”.
Deaths Reported: 28• 7 due to falls • 3 linked to device/medical-surgical
supplies• 2 medication errors • 2 healthcare-associated infections• 2 surgery/anesthesia- related events• 1 perinatal event• 1 suicide• 10 “other”
Of the 28 deaths reported, seven occurred
from falls linked to intracranial injuries occurring when ambulating without assistance or being transferred to or from a bed/chair, and severe injuries occurring as a result of toileting-related activities.
Read about a successful fall prevention strategy at Saint Francis Medical Center (page 8-9).
It is worth noting that more than 1500 events submitted to the PSO involved no harm to the patient. It is often these ‘no harm’ events and near misses that contribute to the greatest learning opportunities.
coNTribUTiNg facTor:TecHNology
A new type of event in healthcare is surfacing which includes the application of technology.
Remember, technological advances should not reduce the need for process checks. For example, a recent software vendor update caused the facility’s printer to offset the medication orders. Patients and their medications were incorrectly matched, causing the individual placing the orders to deliver prescriptions to the wrong patients. In this instance, two patients received one or more dose of
CENTER FOR PATIENT SAFETY
10 w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
PSODaTa SNAPSHOT
(Hospital-related events) (Hospital-related events)
Did You Knowinterested in receiving more information about PSO services available to you? Visit our website at www.centerforpatientsafety.org

In partnership with the National Patient Safety Foundation-
American Society of Professionals in Patient Safety
New Online Curriculum and Professional Certification also available• 10% discount on first year membership in the American Society of Professionals in Patient Safety (ASPPS)• $200 discount for National Patient Safety Foundation (NPSF) • Online Patient Safety Curriculum (including available CE & CME)• $50 discount toward certification from the Certification Board for Professionals in Patient Safety• And much more!
The Center for Patient Safetyis now offering a special 10% discount on membership in the
Visit www.centerforpatientsafety.org for more information.
SUMMER 2013
PSo ParTiciPaNTS memberS-OnlY
Watch for facility-specific data reports to arrive securely in your email soon!
11
the incorrect medication. Fortunately there were no adverse affects from the incorrectly administered medications.
eMS DaTa:
EMS agencies continue to join the Center’s PSO as an opportunity to share in the patient safety learnings, and receive the protections a PSO offers.
The majority of case data received from EMS agencies is related to Stroke and STEMI events. However, medication errors are reported often in EMS agencies, just as they are in hospitals.
Errors with like-name drugs, such as midazolam and morphine, have been reported. Prevention strategies put in place include additional labeling on the vials to denote the brand name of the drug Versed to help distinguish it from morphine. Other cases involved incorrect doses of Fentanyl administered when it was
drawn up by another paramedic and not double checked prior to administration. Another case involved a patient that was administered nitroglycerin in a clinical situation where it was contraindicated.
Information such as this is not currently
available in mass, aggregated volumes for EMS providers. The ability to share this important information is an invaluable example of the power of the data that PSOs can collect and analyze for EMS and all healthcare providers.
(Hospital-related events)

FOr mOre InFOrmATIOn, COnTACT AnY member OF OUr PSO TeAmExecutive Director, beCkY mIller, mHA CPHQ, FACHe, CPPS
Assistant Director, CArOl HAFleY, mHA, bSn, rn, [email protected]
Patient Safety Specialist, eUnICe HAlVerSOn, [email protected]
Project Manager, kATHrYn WIre, JD, mbA, CPHrm [email protected]
Program Manager and Analyst, alex [email protected]
Medical Director, mICHAel HAnDler, mD, mmm, FACPe
Contractor, AmY VOGelSmeIer, PHD, rn, GCnS-bC
For additional information on the Center’s PSO activities, resources, toolkits, upcoming events, safety culture resources, and more, visit our website at www.centerforpatientsafety.org or
follow us on Twitter @PtSafetyExpert for the most up-to-date news.
aboUT THe CenTer:The Missouri Center for Patient Safety, dba Center for Patient Safety, was founded by the Missouri Hospital Association, Missouri State Medical Association and Primaris as a private, non-profit corporation to serve as a leader to fulfill its vision of a healthcare environment safe for all patients and healthcare providers, in all processes, all the time.
CENTER FOR PATIENT SAFETY
12 w w w . c e n t e r f o r p a t i e n t s a f e t y . o r g
The information obtained in this publication is for informational
purposes only and does not constitute legal, financial, or other professional advice. The Center for
Patient Safety does not take any responsibility for the content of
information contained at links of third-party Websites.
NoTeSome articles contained within this newsletter may reference materials
available to Center for Patient Safety PSO participants only. If you have
questions about any Center-resources or articles within this newsletter,
please contact the Center for Patient Safety at [email protected] or call our
office at 888.935.8272.
2013SEPTEMBER
September 12 at 11 a.m. (CDT) - Free national webinar: • Part 1 of 2 - “PSO? PSES? PSWP? You have questions,
we have answers” REGISTERSeptember 22 - National Fall Awareness DaySeptember 25 at 1 p.m. (CDT) - Free webinar for Primaris’ Show Me Quality: QAPI in Action Learning and Action Network participants.
• Agency for Healthcare Research & Quality’s Resident Safety Culture Survey: Finding Your Way to Safety REGISTER
OCTOBEROctober 3 at 1 p.m. (CDT) - National webinar for EMS:
• Part 1 - “Safety Culture and Adverse Event Reporting in EMS – Why Participate and Report to a Patient Safety Organization?” (American Ambulance Association (AAA) members only) REGISTER
October 10 at 1 p.m. (CDT) - National webinar for EMS:• Session 2 - “The Nuts & Bolts of Participating with a
PSO – Developing Internal Policies to fit Your Processes” (American Ambulance Association (AAA) members only) REGISTER
October 16 at 1 pm (CDT) – Free national webinar:• Part 2 of 2 - “PSO? PSES? PSWP? You have questions,
we have answers” October 17 at 1 p.m. (CDT) - National webinar for EMS:
• Session 3 - “Getting the Most Out of PSO Participation – Stories from EMS Agencies” (American Ambulance Association (AAA) members only) REGISTER
October 24 - PSO Advisory Panel Meeting
2014April 29, 2014: PSO Day
MEMbErS-ONly
UPComing eVenTS..
Did You Knowinterested in reading
updates from the center? follow us on
twitter @PtSafetyexpert.
Did You Knowfalls Prevention awareness day is around the corner. click here for available resources to heighten awareness!