PS R&D presentation: 25-05-05 Risk-bearing page 1 Risk-bearing in the Dutch health insurance...
41
R&D presentation: 25-05-05 Risk-bearing page 1 Risk-bearing in the Dutch health insurance Department of R&D AGIS Health Insurances Arnold van der Lee Head of Research
-
Upload
gervase-sims -
Category
Documents
-
view
213 -
download
0
Transcript of PS R&D presentation: 25-05-05 Risk-bearing page 1 Risk-bearing in the Dutch health insurance...

R&D presentation: 25-05-05Risk-bearing
page 1
Risk-bearingin the Dutch health insurance
Risk-bearingin the Dutch health insurance
Department of R&DAGIS Health Insurances
Arnold van der LeeHead of Research
Department of R&DAGIS Health Insurances
Arnold van der LeeHead of Research

R&D presentation: 25-05-05Risk-bearing
page 2
Market share of AGIS •AGIS Sickness funds: 1.4 miljon insured
•AGIS private insurance: 0.2 miljon insured
• Inhabitants: 16 miljon
1. AGIS Health Insurances, R&D

R&D presentation: 25-05-05Risk-bearing
page 3
Department of Research• Information and analyses of:
the insured persons, claims and insurance products not of the organizational costs
• cost containment analyses• health insurance financing system, risk-bearing• premium system, actuarial reserves• health care research
2 senior researcher
s
2 senior researcher
s
1. AGIS Health Insurances, R&D

R&D presentation: 25-05-05Risk-bearing
page 4
2. Presentation
• The risk-bearing in the dutch health insurance
• Are the main purposes of the financing system met?
• Spin-off for contracting of care, pay for performance
Presentation: subjects
R&D presentation: 25-05-05Risk-bearing
page 5
The main purposes of the financing system are:Stimulation of insurers to:• contract efficient providers• listen to the needs and wishes of the insurees
• insurees have equal access to good and affordable health insurance,
• level playing field for health insurance companies,
Important conditions are:
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
page 6
No charityNo charity

R&D presentation: 25-05-05Risk-bearing
page 7
3. Financing system: risk-bearing
Goal government:• Only competition based on quality and
price of contracted care
Therefore there are strong restrictions on the insurers:
• Accept everybody• one package• one flat rate premium per insurer
Goal government:• Only competition based on quality and
price of contracted care
Therefore there are strong restrictions on the insurers:
• Accept everybody• one package• one flat rate premium per insurer

R&D presentation: 25-05-05Risk-bearing
page 8
Therefore insurers need to be compensated for cost differences that they can’t influence, especially those caused by health status differences
• static dimension (compensate for existing losses and profits)
• dynamic dimension (also for future ones that will come because of the mobility of insurees)
Therefore insurers need to be compensated for cost differences that they can’t influence, especially those caused by health status differences
• static dimension (compensate for existing losses and profits)
• dynamic dimension (also for future ones that will come because of the mobility of insurees)
Because of the restriction to one flat rate premium: groups with predictable losses and profitsBecause of the restriction to one flat rate premium: groups with predictable losses and profits
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
Insured
Central Fund
Insurance company
Income-related premium
Risk adjusted capitation payments and risk sharing
Flat-rate premium
88 %
12 %
3. Financing system: risk-bearing
Standard insurance 50 %

R&D presentation: 25-05-05Risk-bearing
page 10
Risk adjusted capitation payments and risk sharing
At the individual level:• part 1: capitation payments• part 2: high risk compensation
At the sickness fund level:• part 3: risk sharing
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
Part 1: Capitation paymentsPart 1: Capitation payments• Ideally, capitation payments should reflect cost
differences resulting from health status differences
• However, health status differences are measured only indirectly by:• age and gender• region and employment status
and more directly by:
• Farmacy and diagnostic cost groups
• Ideally, capitation payments should reflect cost differences resulting from health status differences
• However, health status differences are measured only indirectly by:• age and gender• region and employment status
and more directly by:
• Farmacy and diagnostic cost groups
3. Financing system: risk-bearing
R&D presentation: 25-05-05Risk-bearing
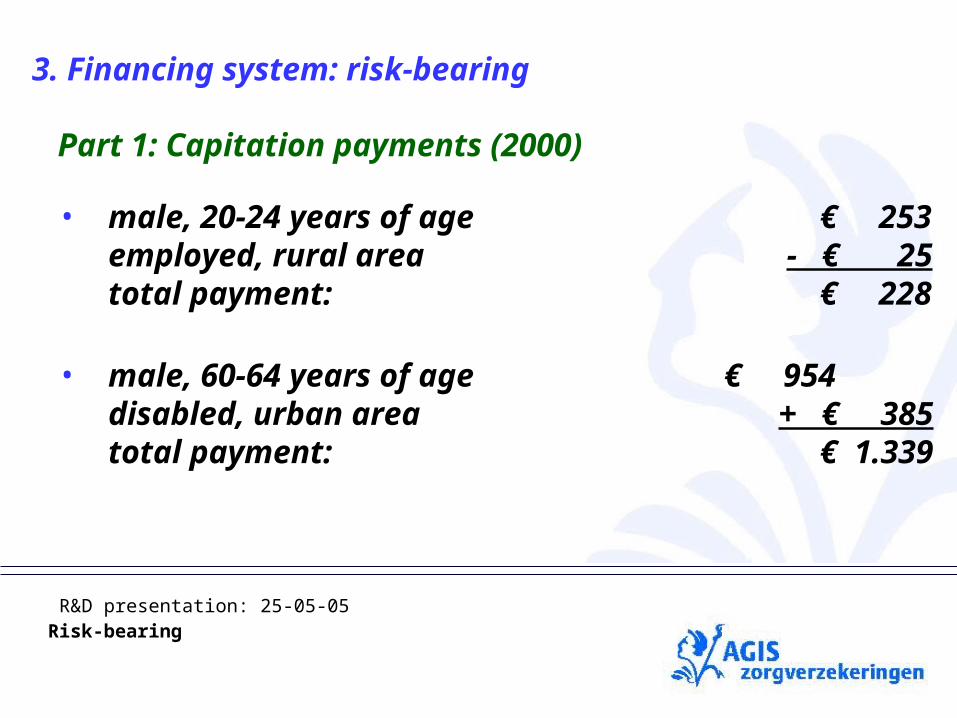
• male, 20-24 years of age € 253employed, rural area
- € 25total payment: € 228
• male, 60-64 years of age € 954disabled, urban area + € 385total payment: € 1.339
Part 1: Capitation payments (2000)Part 1: Capitation payments (2000)
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
page 13
Pharmacy Costs Groups (PCG)
228 700
2.900
12.900
10.200
• Male, 20-24 years
• employed
• rural area
1 = € 1
3. Financing system: risk-bearing
Part 1: Capitation payments (2000)Part 1: Capitation payments (2000)
R&D presentation: 25-05-05Risk-bearing
page 14
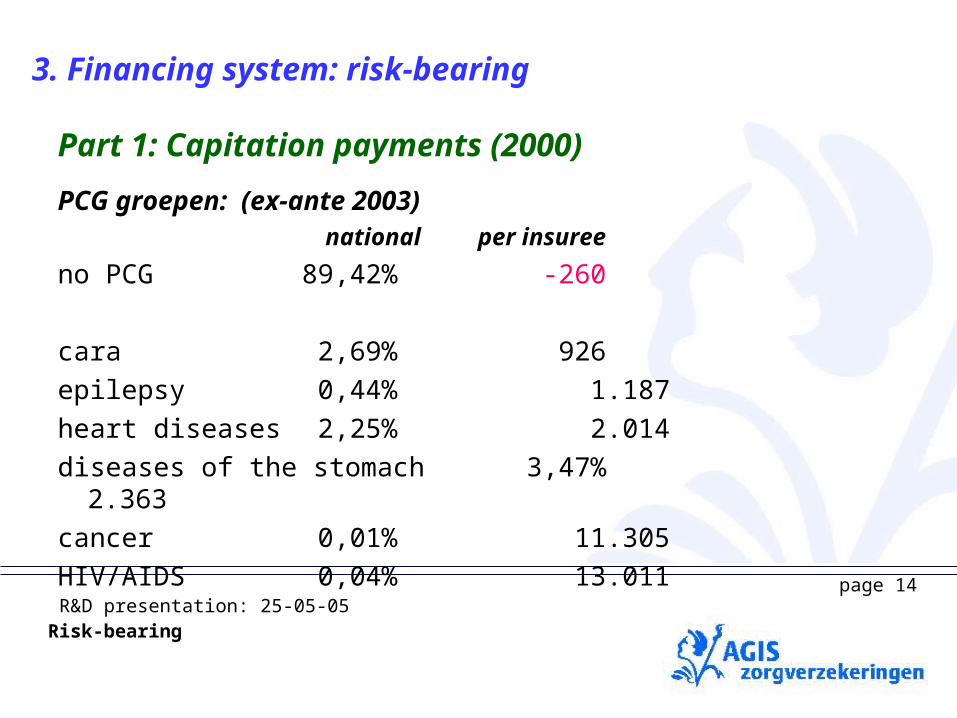
PCG groepen: (ex-ante 2003)
national per insuree
no PCG 89,42% -260
cara 2,69% 926epilepsy 0,44% 1.187heart diseases 2,25% 2.014diseases of the stomach3,47% 2.363cancer 0,01% 11.305HIV/AIDS 0,04% 13.011
3. Financing system: risk-bearing
Part 1: Capitation payments (2000)Part 1: Capitation payments (2000)

R&D presentation: 25-05-05Risk-bearing
Step 2: High Risk Compensation Step 2: High Risk Compensation
• Risk-adjusters are not sufficient to reach the goal of the payment system
• Add: High risk sharing at the individual level
• Costs above € 12.500 threshold are risk-shared (for 90%)
• Risk-adjusters are not sufficient to reach the goal of the payment system
• Add: High risk sharing at the individual level
• Costs above € 12.500 threshold are risk-shared (for 90%)
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
Step 3: Risk sharing Step 3: Risk sharing
• Remaining distributional flaws are risk-shared at the aggregate sickness fund level
• Reduces incentives for both selection and efficiency
• Ministry of Health goal:– Maximum amount of risk for insurers– Minimum size of risk sharing
• Remaining distributional flaws are risk-shared at the aggregate sickness fund level
• Reduces incentives for both selection and efficiency
• Ministry of Health goal:– Maximum amount of risk for insurers– Minimum size of risk sharing
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
• What determines the amount of risk sharing?
• Theory: preferences of regulator with regard to selection and efficiency (PhD dissertation Erik van Barneveld)
• Practice: effects at level of sickness funds (agreement sickness funds and regulator)
• What determines the amount of risk sharing?
• Theory: preferences of regulator with regard to selection and efficiency (PhD dissertation Erik van Barneveld)
• Practice: effects at level of sickness funds (agreement sickness funds and regulator)
3. Financing system: risk-bearing
Step 3: Risk sharing Step 3: Risk sharing

R&D presentation: 25-05-05Risk-bearing
Restrictions at the sickness fund level determine the size of the risk sharing pool:Restrictions at the sickness fund level determine the size of the risk sharing pool:
•Band width given capitation payments•Band width given capitation payments
•Band width after risk sharing
[ ]criteria
•Band width after risk sharing
[ ]criteria
3. Financing system: risk-bearing
Step 3: Risk sharing Step 3: Risk sharing

R&D presentation: 25-05-05Risk-bearing
The amount of insurance risk has increased as a consequence of lower risk sharing:1990: 0%
1995: 3%
2000: 40%
2003: 43%
2005: near 50%, goal government 70% in 20??
3. Financing system: risk-bearing
Step 3: Risk sharing Step 3: Risk sharing

R&D presentation: 25-05-05Risk-bearing
• Ministry of Health wants to control costs
therefore
• Health insurers must contain costs
• Incentive for insurers: win or loose insured
• Ministry of Health wants to control costs
therefore
• Health insurers must contain costs
• Incentive for insurers: win or loose insured
Step 3: Risk sharing and relation with cost containment Step 3: Risk sharing and relation with cost containment
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
Are there instruments to contain costs?Are there instruments to contain costs?• In the past the sickness funds had no instruments to
contain costs
• differences in costs per insured are not related to differences in efficiency
• more risk can only be introduced with more instruments for sickness funds to contain costs
• some are introduced with the new standard insurance
• In the past the sickness funds had no instruments to contain costs
• differences in costs per insured are not related to differences in efficiency
• more risk can only be introduced with more instruments for sickness funds to contain costs
• some are introduced with the new standard insurance
Step 3: Risk sharing and relation with cost containment Step 3: Risk sharing and relation with cost containment
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
page 22
Means of transport as seen by governmentMeans of transport as seen by government
How do we get there?How do we get there?

R&D presentation: 25-05-05Risk-bearing
page 23
Means of transport as seen by insurersMeans of transport as seen by insurers
How do we get there?How do we get there?

R&D presentation: 25-05-05Risk-bearing
What are the options of the sickness fund?What are the options of the sickness fund?
• Stimulation of efficient health care (positive effect)
• Mitigation of inefficient health care (positive effect)
• Cream skimming/quality skimping (negative effect)
• Stimulation of efficient health care (positive effect)
• Mitigation of inefficient health care (positive effect)
• Cream skimming/quality skimping (negative effect)
Step 3: Risk sharing and relation with cost containment Step 3: Risk sharing and relation with cost containment
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
system requirements:system requirements:
• Maximizes incentives for cost containment
• minimize incentives for cream skimming
• fair compensation of the unequal distribution of risks
• Maximizes incentives for cost containment
• minimize incentives for cream skimming
• fair compensation of the unequal distribution of risks
Step 3: Risk sharing and relation with cost containment Step 3: Risk sharing and relation with cost containment
3. Financing system: risk-bearing

R&D presentation: 25-05-05Risk-bearing
Committee on enhancement of capitation model (WOR)
• Ministry of Health (chairman)• Health Insurance Council (CVZ) • Branch Organization (ZN) • Participation Health Care Insurers (a.o. AGIS) • Research institutes
Committee on enhancement of capitation model (WOR)
• Ministry of Health (chairman)• Health Insurance Council (CVZ) • Branch Organization (ZN) • Participation Health Care Insurers (a.o. AGIS) • Research institutes
Consensus model, technical approachConsensus model, technical approach
4. Development of the financing system

R&D presentation: 25-05-05Risk-bearing
page 27
Development of the system: approach of AGIS
• participation in branche organisation at policy and technical levels
• participation in committee of Ministry of Health
• cooperation with expert group of prof. Van de Ven: PhD research project by Piet Stam: optimizing sick fund budget
• research projects e.g. results per region
4. Development of the financing system

R&D presentation: 25-05-05Risk-bearing
page 28
4. Development of the financing system
• Before 1989 sickness funds were administrative organisations which executed the rules and regulations. They were fully compensated for all the claims they paid.
• In 1989 the first step to a new system was taken. The insured had to pay a flat-rate premium themselves.
• Yearly new elements were introduced and the risk-bearing for insurers increased
from administration to risk-bearing

R&D presentation: 25-05-05Risk-bearing
page 29
System Changes:
• competition, • client orientation• free choice of “sickness funds”• insured may change sickfunds every year and
have to be accepted• selective contracting of providers• changes in coverage to and from AWBZ /
additonal health insurance• changes in groups that are compulsorily
covered
4. Development of the financing system

R&D presentation: 25-05-05Risk-bearing
page 30
4. Development of the financing system
• Tremendous changes: “culture shock”
• very dynamic: rapid succession of changes
• unpredictable: changes are introduced and reversed
System Changes:

R&D presentation: 25-05-05Risk-bearing
page 31
New developments:2005: Diagnoses Treatment Combination (DBC),
no-claim2006: system change to one insurance system
(risk-bearing from 9 milion to 16 milion insurees, change of definitions, higher reserves), better compensation for diabetes.
2007: Parts of Mental Health Care included.
4. Development of the financing system

R&D presentation: 25-05-05Risk-bearing
page 32
Insurers see warnings and opportunitiesInsurers see warnings and opportunities

R&D presentation: 25-05-05Risk-bearing
page 33
New developments:
4. Development of the financing system
• Government wants to increase the risk for insurers to 70%,
• but, the first years there is not enough data to base the capitation payments on,
• therefore less risk-bearing

R&D presentation: 25-05-05Risk-bearing
page 34
The main purposes of the financing system are:Stimulation of insurers to:• contract efficient providers• listen to the needs and wishes of the insurees
• insurees have equal access to good and affordable health insurance,
• level playing field for health insurance companies,
Important conditions are:
5. Are the goals of the financing system met?startsstarts
YesYesBut...But...
StillStillBut...But...
Not yetNot yet

R&D presentation: 25-05-05Risk-bearing
page 35
Problems with level playing field• Amsterdam and The Hague
• acknowledged by members WOR
uncompensated diseases• diabetes better compensation next year• many diseases lack specific medications or hospital
diagnoses for marker
5. Are the goals of the financing system met?

R&D presentation: 25-05-05Risk-bearing
page 36
• Possible ways to react on remaining problems:• Risk-selection (avoiding groups of insurees, be attratice to
certain groups and unattractive to other groups)• Contract efficient care• improve financing model
• Risk-selection denies equal access to health insurance, and on a national level ecoomist tell us it has unwanted effects on the economy
• Agis chooses to help improve the financing model and chooses to contract efficient care
5. Are the goals of the financing system met?

R&D presentation: 25-05-05Risk-bearing
page 37
6. Spin-off for contracting of care
• Knowledge about the risk-bearing is also usefull for contracting models with “pay for performance”.• In “pay for performance” the case-mix of the
population has to taken into account
• it also shows where the cost of care is higher than the national level• indicates where the care might be inefficient
R&D presentation: 25-05-05Risk-bearing
page 38
Te dekken kosten
Effect Verevening/nacalculatie
Effect HKV
Effect FKG totaal
Effect FKG insuline
Effect Regio/rechtsgrond
Effect Lftd/geslacht
Budget obv aantal verzekerden
Door verdeelmodel gedekt
6. Spin-off for contracting of care2006, solved?2006, solved?
Yes?
Than more insurees with diabetes
and better contracting of care
pays off
Yes?
Than more insurees with diabetes
and better contracting of care
pays off

R&D presentation: 25-05-05Risk-bearing
page 39
6. Spin-off for contracting of care
Is this caused by a few patients
with extreme high costs
or by inefficient care?
Is this caused by a few patients
with extreme high costs
or by inefficient care?

R&D presentation: 25-05-05Risk-bearing
page 40
Agis hopes for and helps to get a level playing field Agis hopes for and helps to get a level playing field

R&D presentation: 25-05-05Risk-bearing
page 41
Agis sees nice oppertunities Agis sees nice oppertunities We hope you enjoy Amersfoort We hope you enjoy Amersfoort